Back to Journals » Lung Cancer: Targets and Therapy » Volume 16
Successful and On-going Long-Term Disease Control (>24 Months) with Gilteritinib in an ALK+ NSCLC Patient with Brain Metastasis Who Has Progressed on Multiple ALK TKIs. A Case Report and Review of Literature on Gilteritnib
Authors Ou SHI ![]() , Park CJ
, Park CJ ![]() , Arter ZL
, Arter ZL ![]() , Nagasaka M
, Nagasaka M ![]()
Received 14 June 2025
Accepted for publication 2 October 2025
Published 22 October 2025 Volume 2025:16 Pages 139—145
DOI https://doi.org/10.2147/LCTT.S547128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Joseph Locker
Sai-Hong Ignatius Ou,1,2 Cathleen June Park,1,2 Zhaohui Liao Arter,1,2 Misako Nagasaka1,2
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, 92868, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, 92868, USA
Correspondence: Sai-Hong Ignatius Ou, University of California Irvine School of Medicine, 200 South Manchester Ave, Suite 400, Orange, CA, 92868, USA, Email [email protected]
Background: Despite the approval to date of 3 generations of ALK tyrosine kinase inhibitors (TKIs) and the clinical development of a 4th-generation ALK TKI, neladalkib (NVL-655), patients still eventually progress on sequential treatment of various generations of ALK TKIs. Patients with advanced ALK+ NSCLC can survive many years with sequential use of various generations of ALK TKIs but will eventually exhaust all approved available ALK TKIs. Further options for these patients besides clinical trial could include the repurposing of approved multi-targeted TKIs for other oncologic indications. Gilteritinib, a multi-targeted FLT3 (and AXL, ALK, ROS1) TKI, is approved as monotherapy at 120 mg once daily for FLT3+ refractory/relapsed acute myelogenous leukemia (AML).
Case Description: Patient is currently an 82-year-old African-American female never-smoker who was diagnosed with stage 4 NSCLC at age 62. Almost 7.5 years after initial diagnosis and after disease progression on multiple chemotherapy regimens, her tumor was found to harbor an EML4-ALK v1 fusion. Since then, she has been treated with multiple ALK TKIs including crizotinib, alectinib, brigatinib, and lorlatinib sequentially (from age 75 to 80) but requiring dose reduction and interruption of lorlatinib due to neurocognitive toxicity from previous stereotactic brain radiation and resection and eventual discontinuation of lorlatinib. Repeat plasma genotyping after discontinuation of lorlatinib revelaed EML4-ALK v1 without known off-targeted resistances. With written consent from patient and family, she was started on gilteritinib 80 mg once daily with a quick dose increase to 120 mg and achieved stable disease with rapid clearance of ALK fusion from plasma, stability of the CNS metastasis, as well as a decrease in CEA and size of the left upper lesion. Patient is alive today and doing well without CNS effects while on full-dose gilteritinib.
Conclusion: This is the first patient case report with > 24 months on-going follow-up demonstrating that gilteritinib could be repurposed as a potent and tolerable ALK inhibitor based on previously reported pre-clinical activity and with potential CNS activity. A Phase 2 trial of gilteritnib in alectinib- or lorlatinib-refractory ALK+ NSCLC is being planned (NCT07140016).
Plain Language Summary: Key findings
Gilteritinib could be repurposed as a potent and tolerable ALK TKI with CNS activity.
What is known and what is new
Preclinically, gilteritinib has been demonstrated to possess potent ALK inhibitory activity with an IC50 similar to lorlatin (Figure 1) and can overcome certain acquired ALK mutations. Gilteritinib has also demonstrated activity in AML harboring an RANBP2-ALK fusion. This case report extends this pre-clinical observation to successfully treating one patient with advanced ALK+ NSCLC with progression on all three generations of ALK TKI and not eligible for clinical trial with neladalkib, demonstrating safety of full-dose gilteritinib 120 mg once daily with intracranial activity without CNS adverse events, unlike what this patient experienced with lorlatinib even at a very low dose.
What is the implication, and what should change now?
Gilteritinib could be repurposed as a potent and tolerable ALK TKI in the refractory/relapsed setting against several single acquired ALK resistance mutations (but not ALK G1202R gate-keepr mutation) without off-target resistance mechanisms. Given its safety, tolerability, and similar IC50 to lorlatinib (IC50 = 0.78nM [gilteritinib]; IC50 = 1.2nM [lorlatinib]), gilteritinib should be investigated in earlier settings in the treatment of advanced ALK+ NSCLC. Currently, there is a Phase 1– 2 clinical trial of gilteritinib in ALK+ NSCLC ongoing at the University of Michigan (NCT06225427) and Astellas Pharma Inc, which owns gilteritinib, is planning phase 2 trial of gilteritinib in alectinib- and lorlatinib-refractory ALK+ NSCLC patients (NCT07140016).
Keywords: gilteritinib, lorlatinib, ALK fusion, non-small cell lung cancer
Introduction
Since the discovery of anaplastic lymphoma kinase (ALK) fusion in non-small cell lung cancer (NSCLC) in 2007,1,2 there are now 6 ALK TKIs approved in the US (crizotinib, ceritinib, alectinib, brigatinib, ensartinib, lorlatinib) and 8 ALK TKIs (the 6 ALK TKIs approved in US plus iruplialkib and envronalkib) approved in China as of early 2025. ALK fusion constitutes about 5% of actionable driver mutations in NSCLC.3 Sequential use of different generations of ALK TKIs has led to extended survival of patients with advanced ALK+ NSCLC4 but invariably lead to the emergence of compound resistance mutations5 where currently a fourth-generation ALK TKI, neladalkib (NVL-655) is being developed to overcome these compound mutations (ALKOVE-1, NCT05384626). However, the current developmental pathway for full approval of neladalkib is in the first line metastatic setting with the launch of the Phase 3 ALKAZAR trial (NCT06765109) comparing neladalkib to alectinib. Hence, in the future, many countries may not follow potential accelerated approval indications of neladalkib in the US and may not be able to use neladalkib in the refractory setting to overcome compound ALK resistance mutations. Hence, repurposing of approved TKIs that have wildtype ALK kinase activity is needed, given the rarity of these oncogenic drivers.
Gilteritinib (ASP2215) is a multi-targeted FLT3/AXL inhibitor6 that was approved as a single agent at 120 mg once daily on November 29, 2018, for the treatment of relapsed/refractory acute myelogenous leukemia (AML) with a FLT3 mutation based on the ADMIRAL trial.7 Gilteritinib achieved significant overall survival benefit over chemotherapy in relapsed/refractory AML (9.3 months vs 5.6 months; hazard ratio [HR] = 0.64; 95% confidence interval [CI], 0.49 to 0.83; P<0.001).7 This remains the only approved indication for gilteritinib to date.
Beginning in 2021, there were emerging preclinical data that gilteritinib could also be a very potent ALK TKI and as equipotent against wildtype EML4-ALK fusion as lorlatinib and far much more potent than second-generation ALK TKIs (Figure 1).8–10 Gilteritinib can overcome many acquired single ALK mutations, but it is projected to be ineffective against the solvent-from ALK G1202R mutation (IC50 = 168 nM).8 Importantly, however, in preclinical models, gilteritinib can overcome I1171N based and non G1202R compound mutations (ie IC50 = 3.2 nM against I1171N/F1174N)8,9 and has modest activity against G1202R/L1198F compound mutations.8 Furthermore, gilteritinib has been shown to inhibit NPM1-ALK fusion transcript and anaplastic large cell lymphoma cell lines,11 indicating preclinically that gilteritinib can function as a bonafide ALK TKI.
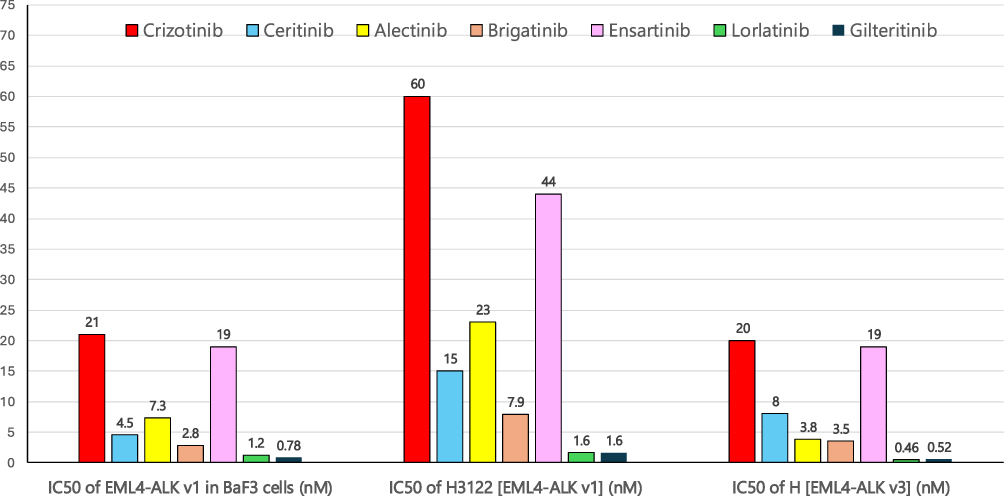 |
Figure 1 Comparison of reported IC50 of various generations of ALK TKIs with various background of EML4-ALK variants. Bar chart graph adopted from data from reference 4. |
Case Description
Patient is an 81-year-old life-long never-smoker African-American female. She was diagnosed with stage 4 non-small cell lung cancer at the age of 63, more than 18 years ago and was treated at an outside medical facility for 7.5 years until a second opinion consult at our institution in 2011. A previous ALK fluorescence in situ hybridization (FISH) performed in 2007 was reported as negative. Confirming her never-smoking status, at our institution, we performed a fine needle biopsy of a growing liver metastasis followed by next-generation sequencing which detected an EML4-ALK variant 1 fusion transcript (Foundation Medicine Inc, Cambridge, MA).
Patient was initially treated with multiple chemotherapy regimens during the 7.5 years prior to the ALK positivity diagnosis (Figure 2). After the diagnosis of ALK positivity, she received crizotinib x 16 months and started on alectinib upon progression on crizotinib. She received alectinib for 2 years and 4 months before developing brain metastases and received stereotactic radiation (SRS) twice over a period of 4 months to 4 and 6 separate lesions, respectively. With the loss of central nervous system (CNS) control, brigatinib was started but patient did not tolerate treatment well with emergent hypertension. Patient was then switched to lorlatinib through an expanded access program. One month after starting lorlatinib at 100 mg once daily, patient developed radiation necrosis requiring resection of the necrotic brain tissue. Lorlatinib was restarted at 75 mg once daily, but patient developed cognitive side effects including forgetfulness and personality changes and lorlatinib dose was eventually reduced to 25 mg once daily three months after starting lorlatinib. Patient continued lorlatinib 25 mg once daily for 36 months, but cognitive side effects again developed with memory loss and inability to perform selfcare. Lorlatinib was subsequently reduced to 25 mg every other day and then eventually held. After 3 months of interruption of lorlatinib, the patient’s cognitive status improved to be able to perform activities of daily living and selfcare but could not tolerate resuming lorlatinib 25 mg every other day and thus, lorlatinib was discontinued.
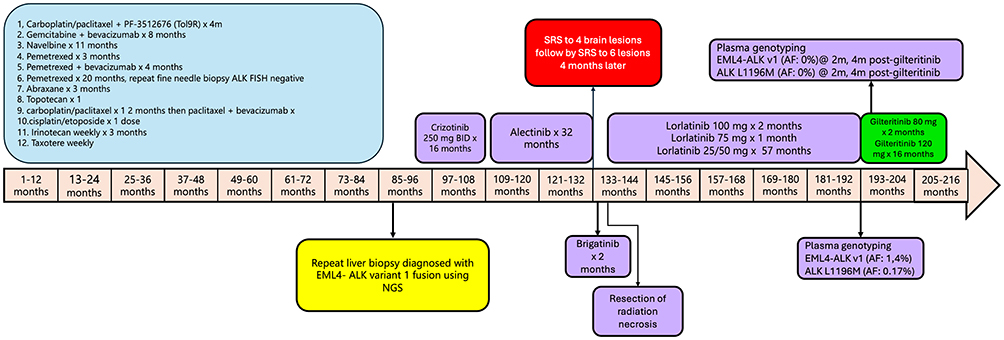 |
Figure 2 Timeline of the treatment history of patient over a period of 18.5 years. |
Patient’s mental status improved after discontinuation of lorlatinib. With patient’s improved performance status, the patient and her family desired further treatment. Given the sequalae of CNS effects, the patient was not eligible for participating in a clinical trial with fourth-generation ALK TKI NVL-655 (nedalalkib). We decided to start gilteritinib given its vigorous pre-clinical data of being a very potent ALK TKI and after discussions about the pre-clinical activity of gliteritinib with the patient and her family, full informed consent was obtained from patient and patient’s family. Pre-gilteritinib treatment plasma genotyping revealed EML4-ALK v1 at allele frequency (AF) of 1.4% with an acquired resistant ALK mutation of L1196M (AF of 0.7%). Other clinically significant co-mutations included TP53 G245A (AF of 0.33%), CHECK2 R117fs*1 (AF of 0.16%), DNMT3A R882P (AF of 0.17%). Gilteritinib was started at 80 mg once daily for 2 months and repeat plasma genotyping revealed disappearance of the EML4-ALK v1 and the ALK L1196M mutation. Radiographic imaging 3 months after starting gilteritinib revealed decrease in the left upper lobe mass (Figure 3). Patent tolerated treatment well with no side effects and the dose of gilteritinib was increased to the approved (in AML) full dose of 120 mg once daily and repeated plasma genotyping revealed continual clearance of both the EML4-ALK v1 and acquired resistance mutation.
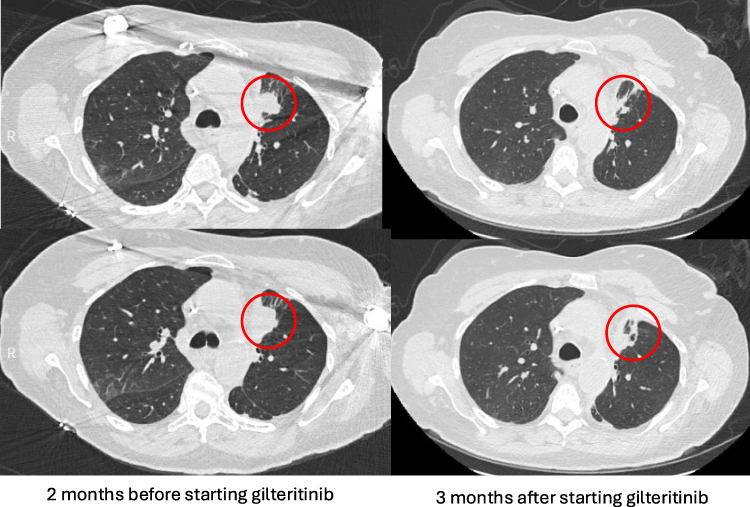 |
Figure 3 Radiographic response to gilteritinib 120 mg once daily after 3 months of treatment. Decrease in the left upper lobe mass was noted. The red circles denoted the tumor responses to gilteritinib treatment. |
Patient continued on gilteritintib and remained well through telemedicine visits, but due to social factors (long travel distance from home to UCI, old age, the long duration of treatment, patient and family preference), surveillance scans were obtained sparingly. Repeat plasma genotyping 18 months after starting gilteritinib revealed continued clearance of EML4-ALK v1. Repeat CT scans showed stable disease in the primary tumor and CEA remained low. The CEA level was monitored throughout her treatment at our institution (Figure 4). To date, the patient has not encountered any laboratory abnormalities, including myelosuppression, while on full dose of gilteritinib treatment.
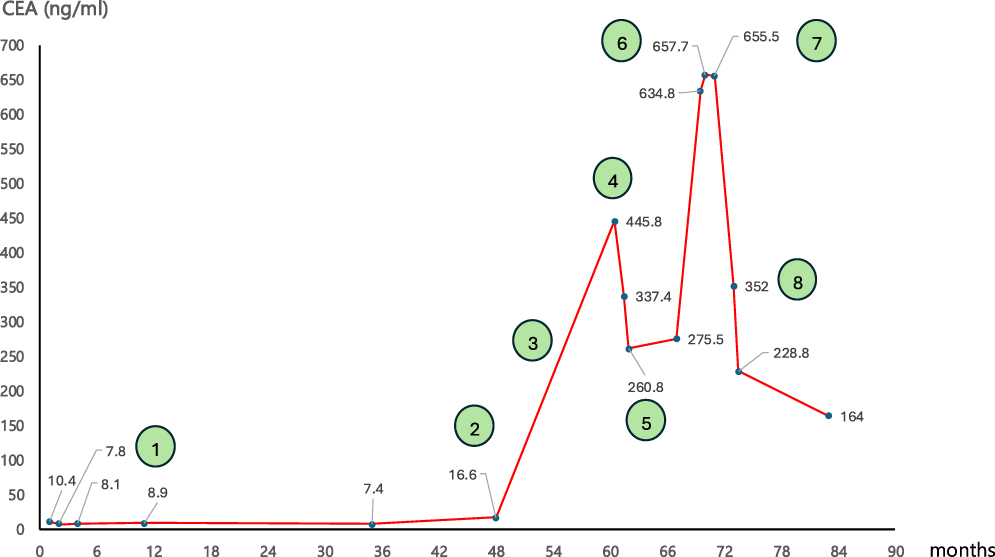 |
Figure 4 Graph of carcinoembryonic antigen (CEA) during treatment history of patient after EML4-ALK fusion was diagnosed at our institution throughout various treatments. Circle 1. Start of alectinib treatment. Circle 2. Start of lorlatinib 100 mg treatment with dose reduction to 75 mg after 1 months of treatment and reduction to 25 mg 3 months later after resection of radiation necrosis. Circle 3. Lorlatinib at 25 mg once daily. Circle 4. Lorlatinib 25 mg every other day to eventual discontinuation. Circle 5. Restarted lorlatinib 25 mg every other day. Circle 6. Permanent discontinuation of lorlatinib. Circle 7. Gilteritinib at 80 mg once daily. Circle 8. Gilteritinib at 120 mg once daily. |
Discussion
We believe our patient case provides the first ever long-term clinical evidence that gilteritinib can be repurposed as a potent and tolerable ALK inhibitor. Granted that patient has survived stage 4 ALK+ NSCLC for more than 18 years, her tumor may have an indolent biology although TP53 mutation, which is a poor prognostic factor,12 was detected immediately prior to the start of gilteritinib. That being said, our case report has provided objective evidence of tumor shrinkage observed in CT scans. Further supportive evidence includes disappearance of circulating EML4-ALK v1 fusion for the duration of gilteritinib treatment and decrease in the level of the CEA tumor marker (Figure 4). Furthermore, the clearance of ALK L1196M is consistent with pre-clinical gilteritinib data (IC50 = 20 nM against ALK L1196M)6 and reflected in the long survival (>24 months) of our patient with single-agent gilteritinib. Additionally, full-dose gilteritinib 120 mg once daily was well tolerated, and there were no cognitive side effects per patient and patient’s family as compared to even the lowest possible dosing of lorlatinib 25 mg every other day. Given patient’s history of progressive CNS metastasis, the absence of new neurocognitive symptoms for >24 months further indicates that gilteritinib may have CNS activity as well.
Our patient had experienced all three generations of ALK TKIs with twice stereotactic radiation and brain resection and given her age had significant CNS adverse events to lorlatinib. The cognitive effect exhibited by this patient on even very low-dose lorlatinib is correlated to the presence of brain metastasis (P = 0.008) and previous brain radiation (P = 0.033) as previously reported.13 Based on the 5-year CROWN data update,14 lorlatinib should be considered the preferred first-line treatment of advanced ALK+ NSCLC.15,16 Given the excellent activity of lorlatinib against CNS metastasis,13 a similar situation with our patient with progressive CNS metastasis on sequential ALK TKIs is unlikely to occur if her ALK+ NSCLC is diagnozed today with lorlatinib as first-line treatment.
It took a second opinion consult 7.5 years after the initial diagnosis to diagnose this patient as having an ALK+ NSCLC, despite the knowledge that patient was a lifelong never-smoker. Patient was initially diagnosed in 2007 during the dawn of a new era of molecular targeted therapies, with the adaptation of regular testing for EGFR mutation and the initial development of the diagnostic test for ALK fusion with ALK FISH which was technically challenging.17 Indeed, the initial ALK FISH of the patient’s tumor was read as negative. However, as we now fully appreciate life-long never-smokers with NSCLC of having a prolonged survival and their tumors of almost always harboring an actionable driver mutation, repeated biopsy should be performed using both DNA and RNA next-generation sequencing to identify any actionable driver mutation as the pre-test probablity of an actionable driver mutation is high.
Finally, gilteritinib has been shown to induce a complete morphological response in RANBP2-ALK AML.18 Gilteritinib also has pre-clinical activity as a ROS1 TKI with IC50 of 11.1 nM against wildtype CD74-ROS1 but importantly IC50 of <1 nM against the ROS1 (Cβ6) L2086F mutation19 which confers resistance to all current type I ROS1 TKIs.11 Additionally, pre-clinically gilteritinib is a potent LTK TKI with IC50 = 0.3 nM against CLIP1-LTK fusion.20 Thus, our successful case report based on published pre-clinical data on gilteritinib can also serve as supporting evidence for “repurposing” gilteritinb in ROS1+ NSCLC patients with a ROS1 L2018F mutation21 and even rarer molecular alteration of LTK+ NSCLC.22 Already, Astella Pharma is planning a phase 2 study of gilteritinib in alectinib- or lorlatinib-refractory ALK+ NSCLC patients (NCT07140016). However, we need to be aware gilteritinib is not effective against ALK G1202R solvent-front mutation, based on pre-clinical data; hence patient selection in alectinib-refractory patients is important not to enroll patients with ALK G1202R or with off-target resistance mechanism that gilteritnib is not expected to overcome, such as MET amplification, commonly found in certain subgroup of alectinib- or lorlatinib-refractory patients23 although inhibiting FLT3 and AXL pathway may be able to circumvent resistance driven by MET amplification given the extensive cross-talk among human receptor tyrosine kinases.24 Given the exceedingly long PFS acheivied by lolratinib in the CROWN study, it is a long shot in next decade that gilteritinib can replace lorlatinib as first-line treatment but can be useful in certain clinical situation if the resistance mechanisms are known.
Acknowledgment
We thank our patient and her family for enrolling in several ALK TKI clinical trials and always having close clinic follow ups despite the travel distance and social challenges and placing their trust on the treating clinicians. A signed informed consent for her case history to be published and presented has been obtained (and scanned into our EPIC electronic medical record). Institution approval for this case report is not required since this is case report is not considered research.
Disclosure
Dr Sai-Hong Ignatius Ou reports stock ownership from MB Therapeutics, Blossom Hill Therapeutics, Nuvalent, Nuvation Bio, Lilly; personal fees from Pfizer, during the conduct of the study. Dr Zhaohui Arter is on the advisory board for Catalyst, J & J, Rigel, outside the submitted work. Dr Misako Nagasaka reports personal fees from AstraZeneca, Daiichi Sankyo, Pfizer, Lilly, Genentech, Regeneron, Johnson and Johnson, Mirati/BMS, Takeda; non-financial travel support from AnHeart/ Nuvation Bio, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561–566. doi:10.1038/nature05945
2. Rikova K, Guo A, Zeng Q, et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell. 2007;131(6):1190–1203. doi:10.1016/j.cell.2007.11.025
3. Harada G, Yang SR, Cocco E, Drilon A. Rare molecular subtypes of lung cancer. Nat Rev Clin Oncol. 2023;20(4):229–249. doi:10.1038/s41571-023-00733-6
4. Arnaoutakis K, Wan Y, Elliott J, et al. Real-World treatment patterns and outcomes across three lines of therapy in patients with ALK+ NSCLC. Adv Ther. 2024;41(8):3217–3231. doi:10.1007/s12325-024-02899-6
5. Zhu VW, Nagasaka M, Madison R, Schrock AB, Cui J, Ou SI. A novel sequentially evolved EML4-ALK variant 3 G1202R/S1206Y double mutation in cis confers resistance to lorlatinib: a brief report and literature review. JTO Clin Res Rep. 2020;2(1):100116. doi:10.1016/j.jtocrr.2020.100116
6. Mori M, Kaneko N, Ueno Y, et al. Gilteritinib, a FLT3/AXL inhibitor, shows antileukemic activity in mouse models of FLT3 mutated acute myeloid leukemia. Invest New Drugs. 2017;35(5):556–565. doi:10.1007/s10637-017-0470-z
7. Perl AE, Martinelli G, Cortes JE, et al. Gilteritinib or chemotherapy for relapsed or refractory FLT3-mutated AML. N Engl J Med. 2019;381(18):1728–1740. doi:10.1056/NEJMoa1902688
8. Mizuta H, Okada K, Araki M, et al. Gilteritinib overcomes lorlatinib resistance in ALK-rearranged cancer. Nat Commun. 2021;12(1):1261. doi:10.1038/s41467-021-21396-w
9. Liang S, Wang Q, Qi X, et al. Deciphering the mechanism of gilteritinib overcoming lorlatinib resistance to the double mutant I1171N/F1174I in anaplastic lymphoma kinase. Front Cell Dev Biol. 2021;9:808864. doi:10.3389/fcell.2021.808864
10. Ando C, Ichihara E, Nishi T, et al. Efficacy of gilteritinib in comparison with alectinib for the treatment of ALK-rearranged non-small cell lung cancer. Cancer Sci. 2023;114(11):4343–4354. doi:10.1111/cas.15958
11. Kuravi S, Cheng J, Fangman G, et al. Preclinical evaluation of gilteritinib on NPM1-ALK-driven anaplastic large cell lymphoma cells. Mol Cancer Res. 2021;19(5):913–920. doi:10.1158/1541-7786.MCR-20-0738
12. Zhang SS, Nagasaka M, Zhu VW, Ou SI. Going beneath the tip of the iceberg. Identifying and understanding EML4-ALK variants and TP53 mutations to optimize treatment of ALK fusion positive (ALK+) NSCLC. Lung Cancer. 2021;158:126–136. doi:10.1016/j.lungcan.2021.06.012
13. Dagogo-Jack I, Abbattista A, Murphy JF, et al. Factors associated with developing neurocognitive adverse events in patients receiving lorlatinib after progression on other targeted therapies. J Thorac Oncol. 2023;18(1):67–78. doi:10.1016/j.jtho.2022.09.219
14. Solomon BJ, Liu G, Felip E, et al. Lorlatinib versus crizotinib in patients with advanced ALK-Positive non-small cell lung cancer: 5-Year outcomes from the phase III CROWN study. J Clin Oncol. 2024;42(29):3400–3409. doi:10.1200/JCO.24.00581
15. Nagasaka M, Ou SI. Lorlatinib should be considered as the preferred First-Line option in patients with advanced ALK-rearranged NSCLC. J Thorac Oncol. 2021;16(4):532–536. doi:10.1016/j.jtho.2020.12.021
16. Ou SI, Lee ATM, Nagasaka M. From preclinical efficacy to 2022 (36.7 months median follow -up) updated CROWN trial, lorlatinib is the preferred 1st-line treatment of advanced ALK+ NSCLC. Crit Rev Oncol Hematol. 2023;187:104019. doi:10.1016/j.critrevonc.2023.104019
17. Ou SH, Bartlett CH, Mino-Kenudson M, Cui J, Iafrate AJ. Crizotinib for the treatment of ALK-rearranged non-small cell lung cancer: a success story to usher in the second decade of molecular targeted therapy in oncology. Oncologist. 2012;17(11):1351–1375. doi:10.1634/theoncologist.2012-0311
18. Adashek JJ, Brodsky M, Levis MJ. Complete morphologic response to gilteritinib in ALK-rearranged acute myeloid leukemia. NPJ Precis Oncol. 2024;8(1):197. doi:10.1038/s41698-024-00701-y
19. Ou SI, Hagopian GG, Zhang SS, Nagasaka M. Comprehensive review of ROS1 Tyrosine Kinase Inhibitors-Classified by structural designs and mutation spectrum (Solvent front mutation [G2032R] and central beta-sheet 6 [Cbeta6] mutation [L2086F]). J Thorac Oncol. 2024;19(5):706–718. doi:10.1016/j.jtho.2023.12.008
20. Mori S, Izumi H, Araki M, et al. LTK mutations responsible for resistance to lorlatinib in non-small cell lung cancer harboring CLIP1-LTK fusion. Commun Biol. 2024;7(1):412. doi:10.1038/s42003-024-06116-6
21. Thawani R, Repetto M, Keddy C, et al. TKI type switching overcomes ROS1 L2086F in ROS1 fusion-positive cancers. NPJ Precis Oncol. 2024;8(1):175. doi:10.1038/s41698-024-00663-1
22. Izumi H, Matsumoto S, Liu J, et al. The CLIP1-LTK fusion is an oncogenic driver in non-small-cell lung cancer. Nature. 2021;600(7888):319–323. doi:10.1038/s41586-021-04135-5
23. Dagogo-Jack I, Yoda S, Lennerz JK, et al. MET alterations are a recurring and actionable resistance mechanism in ALK-Positive lung cancer. Clin Cancer Res. 2020;26(11):2535–2545. doi:10.1158/1078-0432.CCR-19-3906
24. Blume-Jensen P, Hunter T. Oncogenic kinase signalling. Nature. 2001;411(6835):355–365. doi:10.1038/35077225
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
ALESIA 5-Year Update: Alectinib at 600 mg Twice Daily Gives Lorlatinib a Run for Its Money in Asia
Lee AT, Ou SI
Lung Cancer: Targets and Therapy 2023, 14:71-78
Published Date: 7 July 2023