Back to Journals » Clinical Interventions in Aging » Volume 21
Subtype-Specific Associations Between Hyperlipidemia and Age-Related Cataract: A Clinic-Based Cross-Sectional Study
Authors Qin Y, Hong Y, Ning L, Zhang S, Xiao B, Ji Y ![]()
Received 22 January 2026
Accepted for publication 5 June 2026
Published 17 June 2026 Volume 2026:21 598237
DOI https://doi.org/10.2147/CIA.S598237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Yepei Qin,1– 3,* Yingying Hong,1– 3,* Li Ning,1– 3,* Shaohua Zhang,1– 3 Binghe Xiao,1– 3 Yinghong Ji1– 3
1Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, Shanghai, 200031, People’s Republic of China; 2NHC Key Laboratory of Myopia (Fudan University); Key Laboratory of Myopia, Chinese Academy of Medical Sciences, Shanghai, 200031, People’s Republic of China; 3Shanghai Key Laboratory of Visual Impairment and Restoration, Shanghai, 200031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yinghong Ji, Eye Institute and Department of Ophthalmology, Eye & ENT Hospital, Fudan University, No. 83 Fenyang Road, Shanghai, 200031, People’s Republic of China, Email [email protected]
Background: Age-related cataract (ARC) is the leading cause of global blindness in the elderly. An unbalanced metabolic state is known to contribute to lens epithelial cell dysfunction and ARC pathogenesis. However, the relationship between hyperlipidemia and ARC remains controversial.
Methods: In this cross-sectional study based in the Eye and Ears, Nose, and Throat Hospital, Fudan University, a total of 384 ARC subjects were included, and stratified by cataract morphology (cortical, nuclear, and posterior subcapsular cataract [PSC]). Detailed ocular and systemic evaluations were performed. Ordinal univariate and multivariate logistic regression analyses were used to identify associations between serum biochemical indices and ARC severity.
Results: After adjusting for potential confounders, multivariate analysis revealed that hyperlipidemia was independently associated with PSC severity. Specifically, elevated apolipoprotein B (APO-B; odds ratio [OR], 1.767; 95% confidence interval [CI], 1.297– 2.408) and triglycerides (TG; OR, 1.311; 95% CI, 1.014– 1.697) were significant risk factors, while high-density lipoprotein cholesterol (HDL-C; OR, 0.738; 95% CI, 0.572– 0.952) demonstrated an inverse association. In contrast, cortical cataract severity was independently associated with female sex (OR, 1.829; 95% CI, 1.147– 2.916), elevated APO-B (OR, 1.231; 95% CI, 1.012– 1.498) and lactate dehydrogenase (LDH; OR, 1.264; 95% CI, 1.040– 1.536). Nuclear cataract was primarily associated with older age (OR, 1.608; 95% CI, 1.301– 1.987) and longer axial length (OR, 1.310; 95% CI, 1.064– 1.611), with no independent links to serum lipids.
Conclusion: These cross-sectional findings demonstrate a significant and subtype-specific association between hyperlipidemia and ARC, particularly regarding PSC severity. While these associative results are exploratory, lipid biomarkers may generate hypotheses for future risk stratification and preventive strategies.
Keywords: cataract, dyslipidemias, triglycerides, lipoproteins, LOCS III
Introduction
Age-related cataract (ARC) remains the principal cause of blindness globally, posing a substantial burden on patients’ life quality and public healthcare systems.1 Its etiology is complex, involving a spectrum of risk factors such as aging,2 high myopia,3 uveitis, diabetes4 and so on. As a core component of metabolic syndrome, hyperlipidemia has been linked to the development of various age-related conditions, such as age-related macular degeneration5 and neurodegenerative diseases.6
However, its specific role in ARC remains inconclusive, with epidemiological evidence presenting considerable contradictions. First, a paradox exists between the overall and subtype-specific risk: elevated serum lipids are identified as independent risk factors for ARC in general, yet analyses reveal no significant variation in these levels across distinct morphological subtypes.7 Furthermore, the evidence for which lipids matter is inconsistent. Some studies point to total triglycerides as specifically linked to posterior subcapsular cataract (PSC) in males.8 Whereas others emphasize the combined effect of hyperglycemia and low HDL-cholesterol,9 indicating complex and potentially heterogeneous pathogenic pathways.
We hypothesize that the association between systemic dyslipidemia and the lens is not uniform but subtype-specific, dictated by the distinct metabolic microenvironments of different lens regions. To address these evidence gaps, this study aims to re-evaluate the relationship between systemic metabolic biomarkers with ARC, while accounting for the limitations of prior researches. To this end, we implemented a refined analytical approach in a carefully screened cohort, free from major comorbidities and history of long-term medication, to minimize confounding. Furthermore, all analyses were performed with respect to individual cataract subtypes and their severity grades. We hypothesize that this subtype-stratified framework will help uncover distinct biomarker profiles and provide deeper insights into the heterogeneous mechanisms underlying ARC. Clarifying these distinct associative pathways is of significant clinical interest. By isolating subtype-specific biomarkers, this exploratory research not only aims to resolve existing epidemiological paradoxes, but also generates targeted hypotheses for future longitudinal studies investigating personalized risk stratification and metabolic management.
Material and Methods
Study Population
This cross-sectional study enrolled 384 patients (with gender classified based on biological sex assigned at birth as recorded in medical documentation) diagnosed with ARC at the Eye and ENT Hospital of Fudan University between January 1st, 2023, and October 31th, 2024. An informed consent was received from all subjects. The study adhered to the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of the Eye and Ears, Nose, and Throat Hospital, Fudan University (No.2024215).
Data Collection
Two trained research staff conducted face-to-face interviews to collect comprehensive data on demographic characteristics, diseases history, medication history and family history.7 Clinical and demographic information was subsequently extracted from the hospital’s medical data platform by trained personnel following standardized data collection and quality control procedures to ensure the reliability of the analytical data. All participants underwent a thorough systemic medical evaluation at the Eye and ENT Hospital of Fudan University. This included: vital signs (blood pressure, heart rate, and body temperature); medical examinations (electrocardiogram (ECG), X-ray); laboratory tests (infectious diseases testing, comprehensive biochemical profiling, electrolyte panel, and complete blood and urine routine examinations). Each ARC patient received a set of standardized ophthalmic examinations performed by a skilled cataract specialist. These examinations included: visual acuity, slit-lamp examination under dilated pupils, fundus photography, and ocular B-mode ultrasound. Axial length (AL) was measured using the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany).
To be specific, lens opacity status was evaluated using the Lens Opacities Classification System III (LOCS III). To maximize internal consistency and eliminate inter-observer variability, all gradings were performed by one certified and experienced chief physician. A patient was considered to have a specific type of cataract if it was present in either eye, regardless of the coexistence of other opacity types.8 For patients presenting with mixed cataracts, the severity of each morphological component (Cortical, Nuclear, and PSC) was graded and analyzed independently. Therefore, a single patient could contribute data to multiple subtype-specific regression models based on their distinct regional opacities.
Blood samples were collected from all subjects after an 8-hour fast via standard venipuncture of the forearm vein. Ethylenediaminetetraacetic acid (EDTA) was used as an anticoagulant. The collected samples were centrifuged within 60 minutes of collection (3000 rpm, 10 minutes, 20°C). Serum biomarkers were measured using ZY-1200 fully automated biochemical analyzer (KeHua Biotech, Shanghai, China). The analyzed biomarkers included lipid metabolism (Total cholesterol, TC; total triglycerides, TG; high-density lipoprotein cholesterol, HDL-C; low-density lipoprotein cholesterol, LDL-C; apolipoproteins, APO-A, APO-B, APO-E; lipoprotein(a), LP(a); and small dense LDL, sdLDL), glucose metabolism (Fasting glucose, GLU; and glycated hemoglobin, HBA1c), liver function (Total bilirubin, T-BIL; direct bilirubin, D-BIL; and total bile acids, TBA), renal function (Blood urea nitrogen, BUN; creatinine, CR; uric acid, UA; and estimated glomerular filtration rate, eGFR), Cardiac marker (Lactate dehydrogenase, LDH), antioxidant enzymes and others (Superoxide dismutase, SOD; glutathione reductase, GR), and composite indices (Triglyceride-glucose index, TyG, atherogenic index of plasma, AIP; uric acid to high-density cholesterol ratio, UHR; and non-high-density lipoprotein cholesterol, nonHDL-C).
Inclusion and Exclusion Criteria
To ensure the intrinsic association between serum lipids and cataractogenesis was isolated from secondary metabolic influences, we implemented a highly-selective recruitment protocol. Participants were eligible if they met all of the following conditions: Aged 45 years or older; diagnosed with any type of ARC (cortical, nuclear, or posterior subcapsular) according to the Lens Opacities Classification System III (LOCS III). For patients suffered from bilateral cataracts, only the first eye scheduled for surgical intervention was included in analysis.
Exclusion criteria were rigorously applied to minimize confounding: Ocular conditions: presence of concomitant ocular diseases, including high myopia (axial length≥26 mm), uveitis, corneal pathologies, fundus diseases, congenital ocular diseases, history of ocular trauma, or any previous ocular surgery. Systemic comorbidities: history of specific systemic diseases, including diabetes mellitus, thyroid disease, hyperuricemia, Alzheimer’s disease, cancer, acute infectious diseases, kidney disease, autoimmune disorders, or significant cardiovascular abnormalities. Medication Use: Long-term use of medications known to influence systemic metabolism, such as lipid-lowering agents, antidiabetic drugs, anti-obesity medications, or thyroid hormone regulators.
Statistical Analysis
All statistical analyses were performed using the R statistical language version4.5.1 (R Core Team, 2025, Vienna, Austria).
Data preprocessing included handling missing values via k-nearest neighbors10 imputation (k=10) and outlier treatment using Tukey’s method. To ensure adequate sample size across severity subgroups for ordinal regression, cataract grading was transformed: PSC grades (originally 2~5) were recoded as 1~4, and cortical cataract grades (originally 1~5) were consolidated into three levels (1~2→1 level, 3→2 level, 4~5→3 level).
Continuous variables failing normality assumptions (Shapiro–Wilk test, P<0.05) underwent appropriate transformations (logarithmic, square root, or Box-Cox), followed by Z-score standardization.11
Descriptive statistics presented continuous variables as median (IQR) or mean ± SD, and categorical variables as frequencies (percentages). Group comparisons employed t-tests/ANOVA, Mann–Whitney U/Kruskal–Wallis tests, or chi-square/Fisher’s exact tests as appropriate.
To identify potential risk factors associated with cataract severity for each morphological subtype, univariate ordinal regression analyses were conducted using Jonckheere-Terpstra trend tests12 and Cochran-Armitage trend tests.13 A liberal significance threshold (P<0.1) was applied in the univariate analysis as an initial screening step.14 All variables meeting this criterion were then advanced for consideration in the multivariate analysis.
Three distinct multivariate proportional odds logistic regression models were developed for each cataract subtype.15 The proportional odds assumption was rigorously tested using the Brant test16 for all models (as shown in Supplementary Table S1). To address potential multicollinearity among the correlated lipid variables, a two-step approach was implemented. First, composite metabolic indices were a priori excluded from multivariable modeling to prevent inherent structural collinearity. Second, variance inflation factors (VIF) were calculated for the remaining individual covariates to evaluate multicollinearity. To prevent model instability, variables demonstrating high collinearity (VIF>5) were carefully evaluated. The detailed VIF values for all individual covariates are documented in Supplementary Table S2. Consequently, representative core lipid parameters (eg., APO-B and TG) were prioritized for inclusion in the final models to ensure maximum stability and clinical interpretability.
To ensure robustness, the three models were defined as follows:
Model 1: full model, which incorporated all potential covariates including demographic characteristics, ocular parameters, and comprehensive serum biomarkers.
Model 2: clinically important variables, which included only variables identified as clinically relevant or statistically significant in preliminary analyses.
Model 3: stepwise AIC-selected models, which employed stepwise variable selection using Akaike Information Criterion (AIC) minimization with bidirectional elimination.17
A strict analytical hierarchy was defined to interpret the results: Model 3 was designated as the primary analytical model, as it provides the optimal balance between model fit and parsimony by systematically eliminating redundant variables. Meanwhile, Model 1 and Model 2 served as supportive sensitivity analyses to verify the robustness and stability of our core findings across different covariate adjustment strategies.
Model performance was evaluated using AIC, BIC, pseudo R-squared and likelihood ratio tests. Statistical significance was defined as P<0.05 (two-tailed).
Results
Baseline Characteristics of the Study Population According to Cataract Subtypes
A total of 384 patients with ARC were enrolled in this study, with a median age of 68.65 (±8.42) years. The cohort comprised 125 males (32.6%) and 259 females (67.4%). The baseline characteristics of the participants, stratified by the morphological subtypes and severity of cataracts, are presented in Tables 1–3. While these main tables summarize the important or significantly different indicators across severity grades, the complete baseline data for all measured variables can be found in Supplementary Tables S3, S4, and S5.
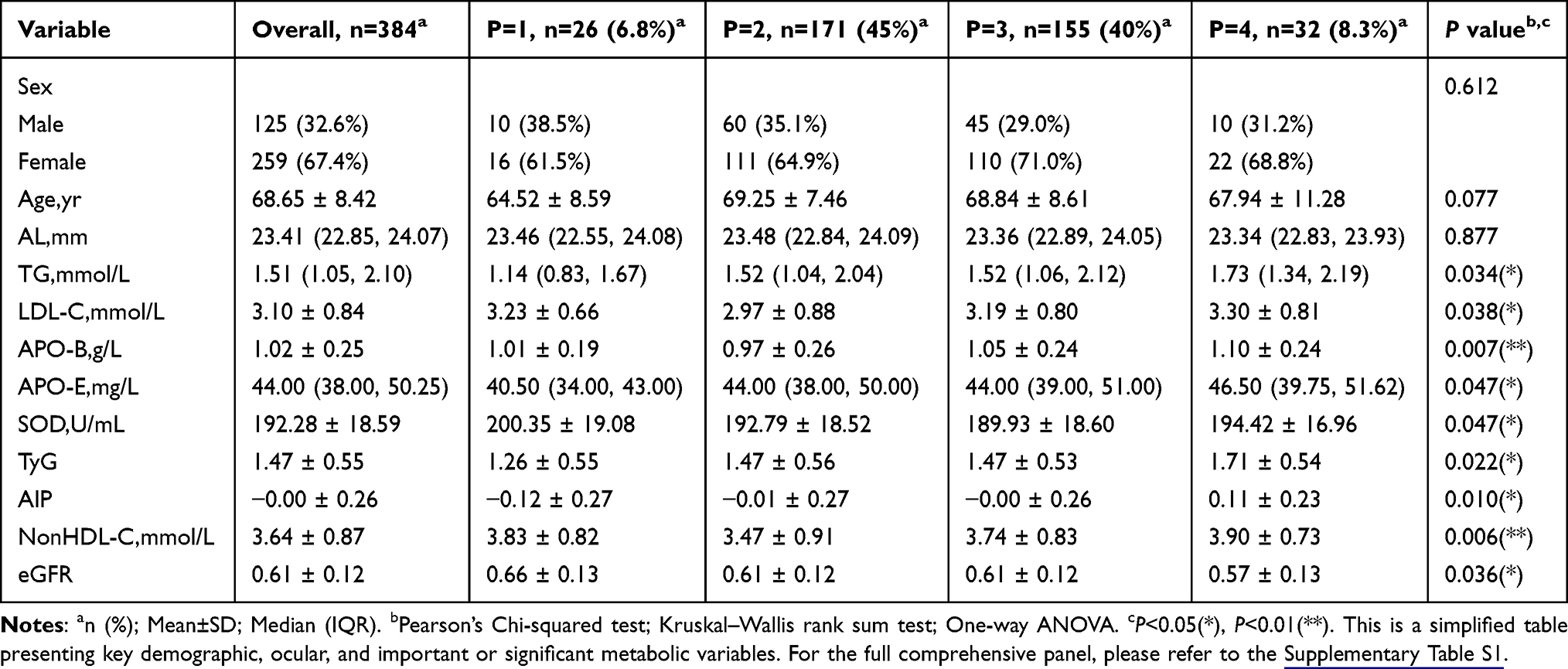 |
Table 1 Simplified Baseline Characteristics of the ARC Patients by the Severity of PSC |
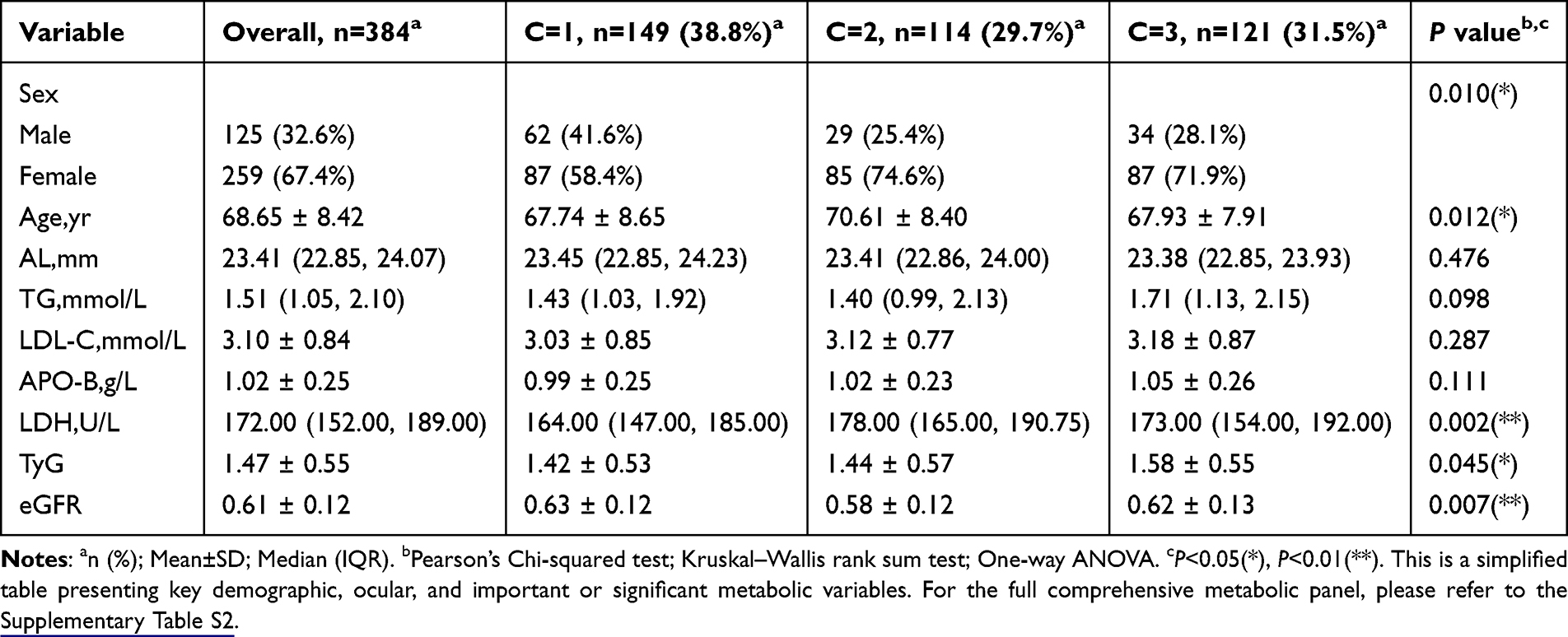 |
Table 2 Simplified Baseline Characteristics of the ARC Patients by the Severity of Cortical Cataract |
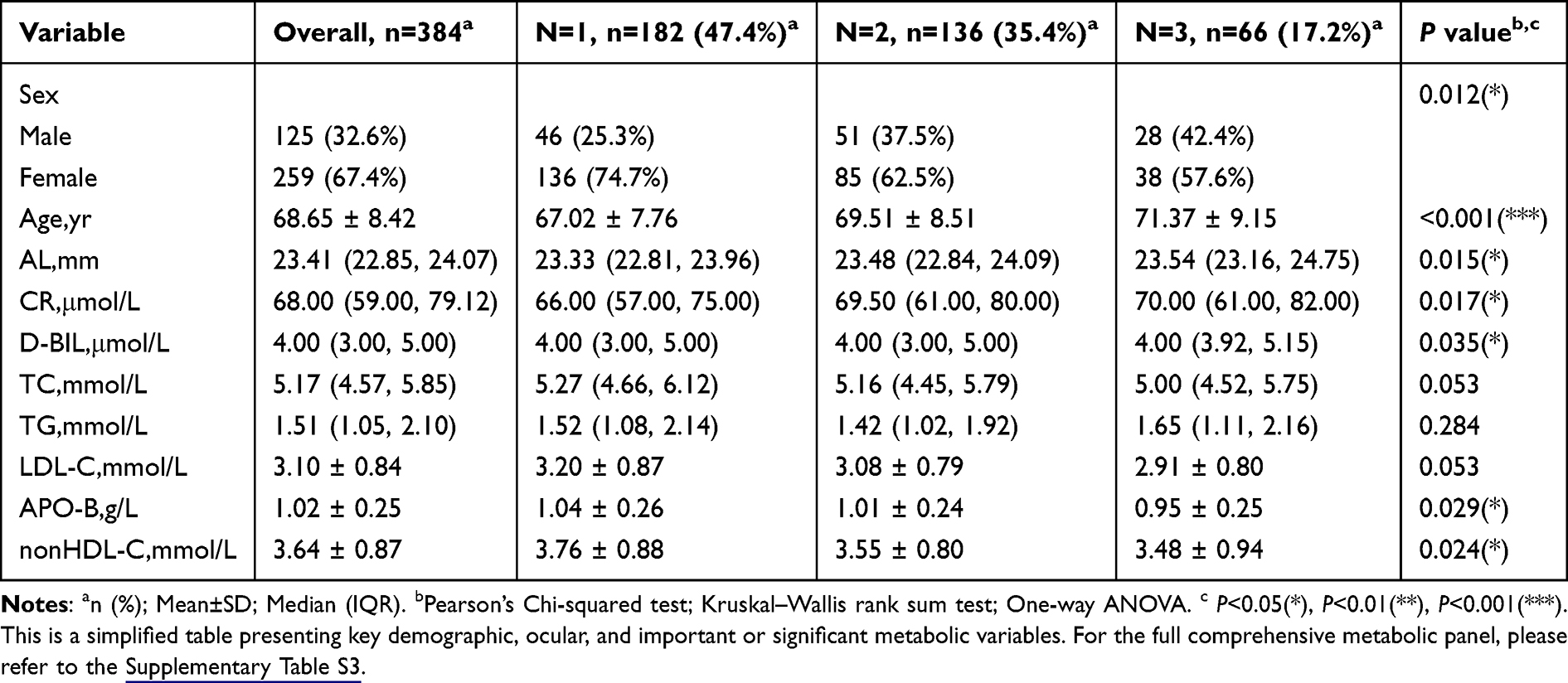 |
Table 3 Simplified Baseline Characteristics of the ARC Patients by the Severity of Nuclear Cataract |
Baseline Characteristics by Posterior Subcapsular Cataract (PSC) Grade
The participants were categorized into four groups based on the severity of PSC (equal to Grades 1 to 4). As shown in Table 1, the distribution across PSC grades was as follows: P1 (n=26, 6.8%); P2 (n=171, 45%); P3 (n=155, 40%); P4 (n=32, 8.3%). Sex distribution (P=0.612), age (P=0.077), most systemic biomarkers, and ocular length were comparable across groups. In contrast, several lipid metabolic indicators exhibited significant intergroup variations, including TG (P=0.034), LDL-C (P=0.038), APO-B (P=0.007), and APO-E (P=0.047). Statistically significant differences were also observed for the TyG index (P=0.022), AIP (P=0.010), nonHDL-C (P=0.006), and eGFR (P=0.036).
Baseline Characteristics by Cortical Cataract Grade
The baseline characteristics stratified by cortical (C) cataract grade (equal to Grade 1 to 3) are summarized in Table 2. The cohort was divided into C1 (n=149, 38.8%), C2 (n=114, 29.7%), and C3 (n=121, 31.5%). Sex distribution (P=0.010) and age (P=0.012) differed significantly among groups. Unlike the PSC analysis, most conventional lipid profiles (TC, TG, HDL-C, LDL-C) showed no significant association with cortical cataract grade. Instead, LDH levels (P=0.002) and eGFR (P=0.007) varied across groups. The TyG index (P=0.045) also showed a borderline significant association.
Baseline Characteristics by Nuclear Cataract Grade
Table 3 presents the characteristics of participants grouped by nuclear (N) cataract grade (equal to N1 to N3): N1 (n=182, 47.4%), N2 (n=136, 35.4%), and N3 (n=66, 17.2%). Significant intergroup disparities were observed for sex (P=0.012), age (P<0.001), AL (P=0.015), and CR (P=0.017). Among lipid metrics, APO-B (P=0.029) and nonHDL-C (P=0.024) levels also differed significantly. Additionally, D-BIL levels varied across nuclear cataract grades (P=0.035).
Univariate Ordinal Regression Analysis for Cataract Severity
Univariate ordinal regression analyses were performed to identify potential risk factors for the severity of each cataract subtype. The results, detailed in Table 4 revealed distinct and subtype-specific association profiles.
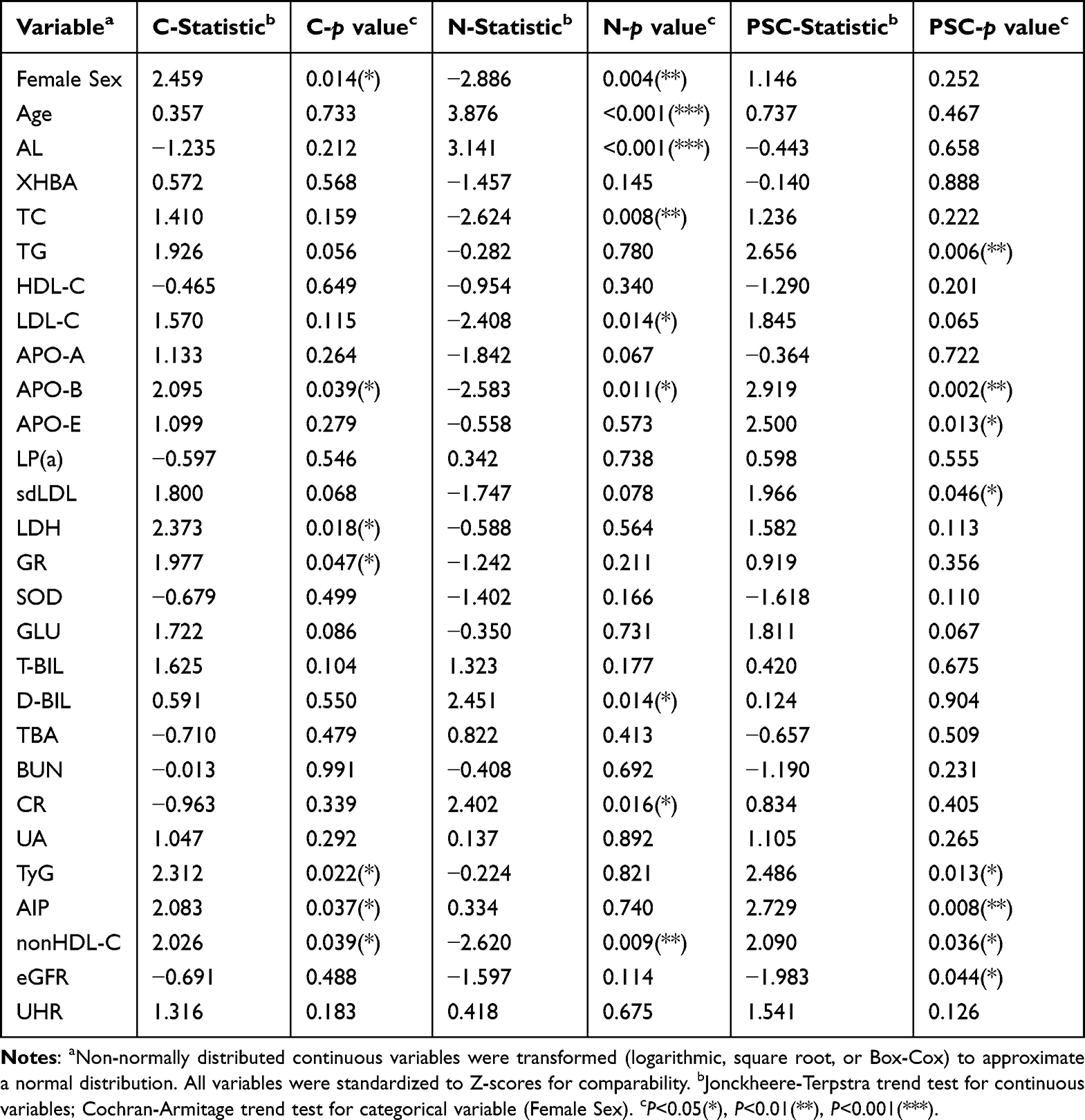 |
Table 4 Univariate Ordinal Analysis of Factors Associated with Severity of Cataract Subtypes |
Posterior Subcapsular Cataract: Strong Associations with Specific Lipid Components
The severity of PSC cataracts was strongly linked to several key lipid and metabolic factors. The most significant positive associations were observed for APO-B (statistic=2.919, P=0.002) and TG (statistic=2.656, P=0.006). This lipid-related risk was further evidenced by associations with APO-E (statistic=2,500, P=0.013), sdLDL (statistic=1.966, P=0.046), and composite measures including TyG (statistic=2.486, P=0.013), AIP (statistic=2.729, P=0.008), and non-HDL-C (statistic=2.090, P=0.036). In contrast, better renal function (eGFR; statistic=−1.983, P=0.044) was associated with lower risk of severe PSC cataract. Demographic factors such as age and sex distribution were not significant correlates. Figure 1 illustrates above significant associations in detail.
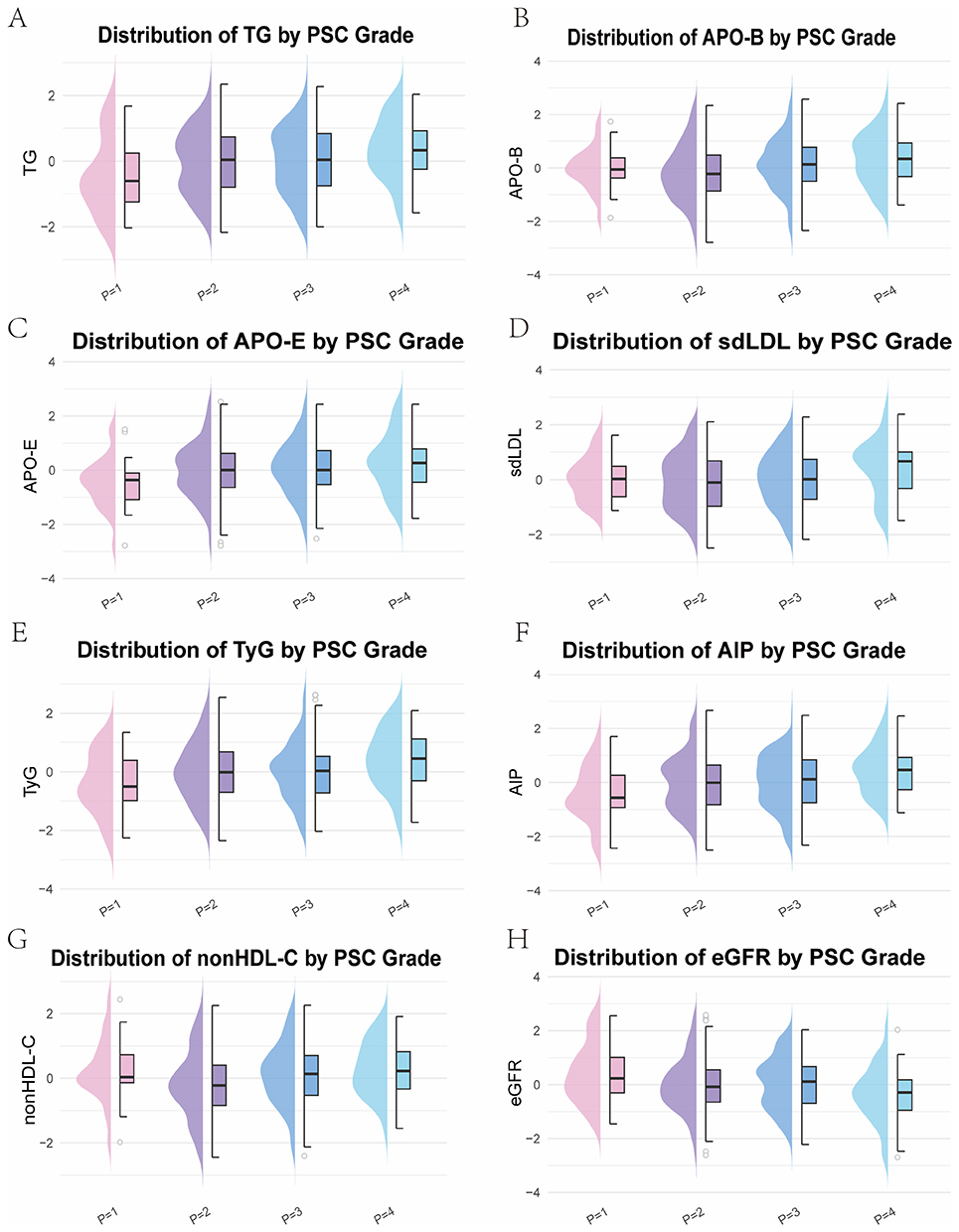 |
Figure 1 Distribution of Significant Biomarkers Across Severity Grades of PSC. Half−violin (density) and half−boxplot combination plots are shown for all variables significantly associated with PSC severity in univariate analysis (Jonckheere-Terpstra trend test). The panels represent: (A) TG (Triglycerides), (B) APO-B (Apolipoprotein B), (C) APO-E (Apolipoprotein E), (D) sdLDL (Small Dense Low-Density Lipoprotein), (E) TyG (Triglyceride-Glucose index), (F) AIP (Atherogenic Index of Plasma), (G) nonHDL-C (Non-High-Density Lipoprotein Cholesterol), and (H) eGFR (Estimated Glomerular Filtration Rate). Clinically, composite indices such as the TyG index serve as robust surrogate markers for systemic insulin resistance, while AIP and nonHDL-C comprehensively reflect atherogenic lipid burden and cardiovascular risk. Their inclusion highlights the potential role of systemic metabolic dysfunction in PSC progression. |
Cortical Cataract: A Heterogeneous Profile Involving Sex, Hemolysis, and Specific Lipids
Cortical cataract severity was associated with a diverse set of factors. Female sex (statistic=2.459, P=0.014) was a marked demographic risk. Biochemically, markers suggestive of hemolysis and oxidative stress were prominent, shown by the positive association with LDH (statistic=2.373, P=0.018) and the antioxidant enzyme GR (statistic=1.977, P=0.047). The lipid association was specific, with APO-B (statistic=2.095, P=0.039) and composite measures nonHDL-C (statistic=2.026, P=0.039) and AIP (statistic=2.083, P=0.037) reaching significance, alongside the TyG index (statistic=2.312, P=0.022). Figure 2 provides visual validation of these significant associations.
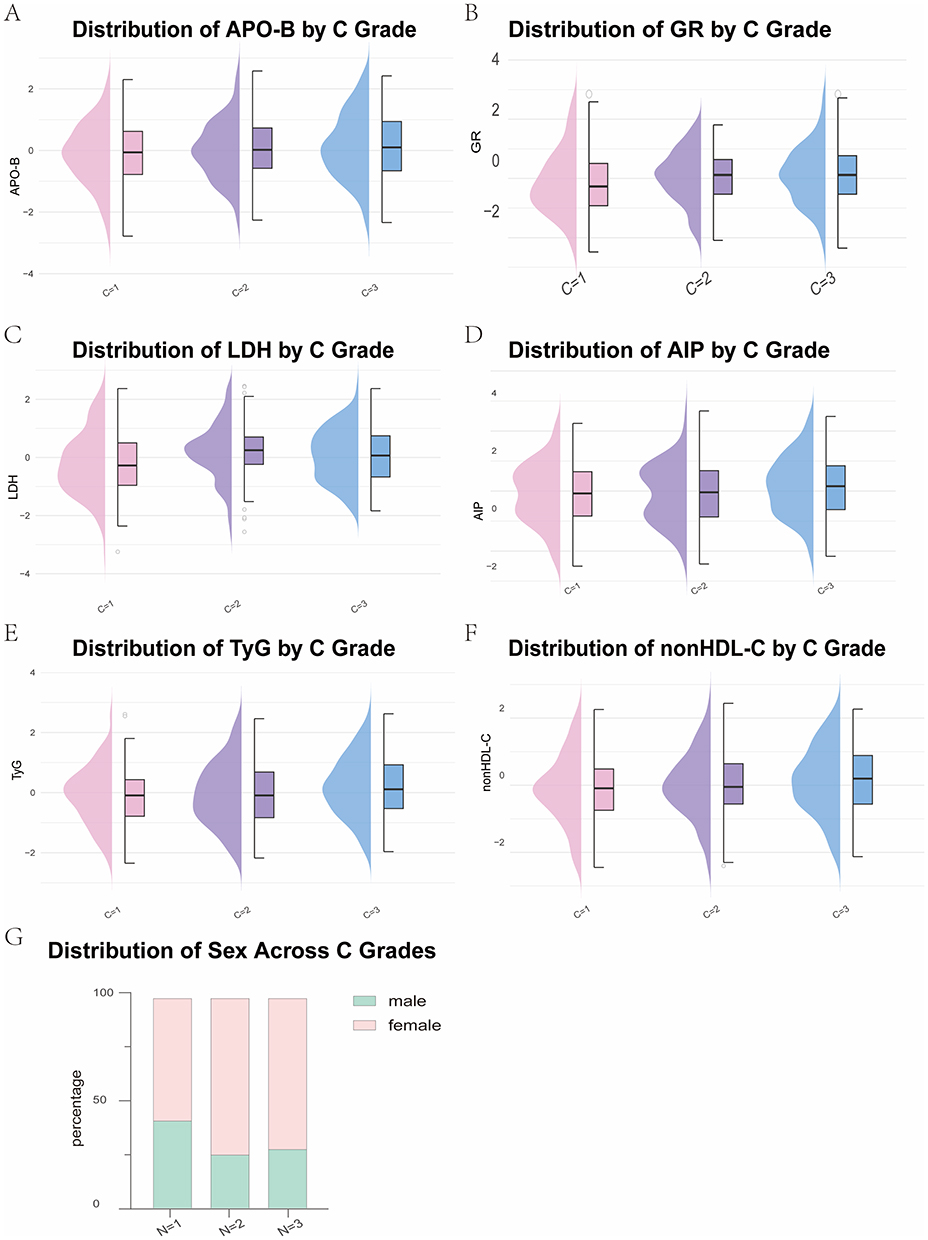 |
Figure 2 Distribution of Significant Biomarkers Across Severity Grades of Cortical (C) cataract. Half−violin (density) and half−boxplot combination plots are shown for all variables significantly associated with cortical cataract severity in univariate analysis (Jonckheere-Terpstra trend test). The panels represent: (A) APO-B, (B) GR (Glutathione Reductase), (C) LDH (Lactate Dehydrogenase), (D) AIP, (E) TyG, (F) nonHDL-C, and (G) Sex. The display of composite metabolic indices (TyG, AIP, nonHDL-C) alongside tissue metabolism markers (LDH) illustrates the cumulative impact of insulin resistance, systemic oxidative stress, and dyslipidemia on the severity of cortical cataract. |
Nuclear Cataract: Primarily Associated with Aging and Axial Length Elongation
The severity of nuclear cataract was predominantly determined by demographic and ocular structural factors. Older age (statistic=3.876, P<0.001) and longer axial length (statistic=3.141, P<0.001) were the most powerful strongest correlates, with female sex (statistic=−2.886, P=0.004) also associated with lower odds. A distinctive and counterintuitive finding was the consistent inverse relationship with conventional lipid parameters; higher levels of TC (statistic=−2.624, P=0.008), LDL-C (statistic=−2.408, P=0.014), APO-B (statistic=−2.583, P=0.011), and nonHDL-C (statistic=−2.620, P=0.009) were all associated with a lower odds of severe nuclear cataract. Other significant factors included CR (statistic=2.402, P=0.016) and D-BIL (statistic=2.451, P=0.014). The distributions of these significant variables are detailed in Figure 3.
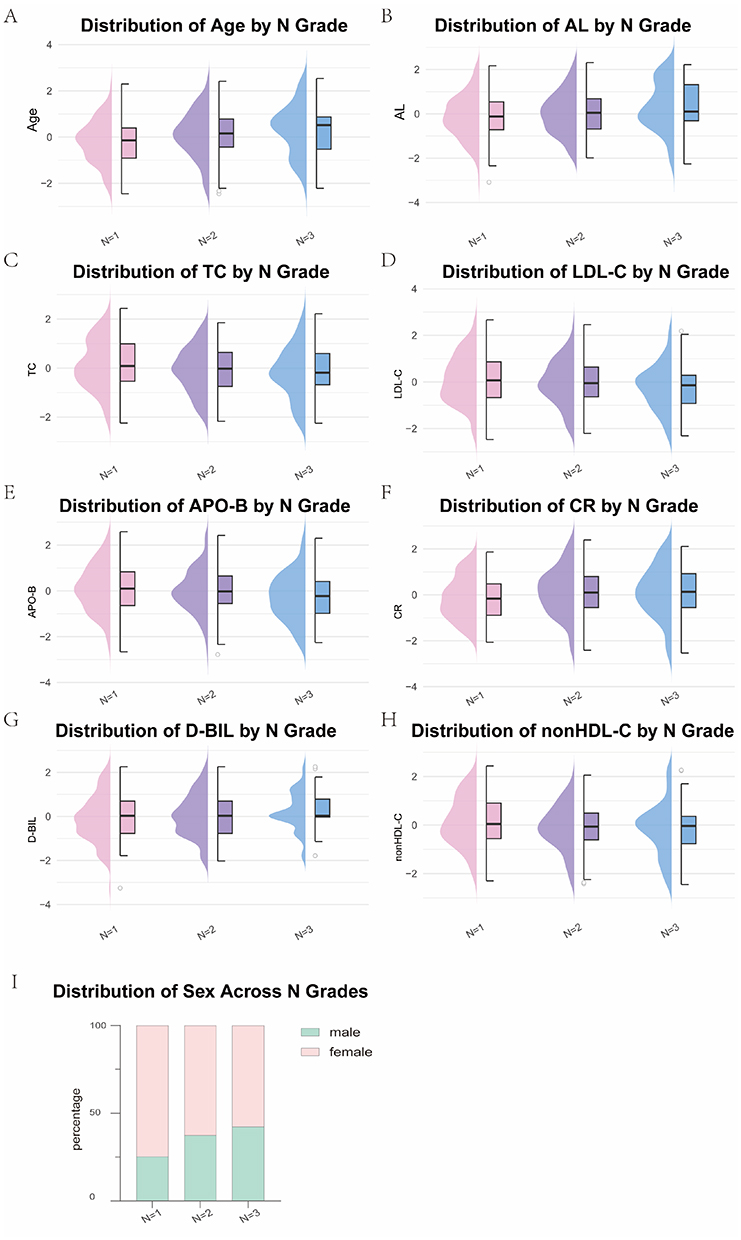 |
Figure 3 Distribution of Significant Biomarkers Across Severity Grades of Nuclear (N) cataract. Half−violin (density) and half−boxplot combination plots (for continuous variables) and column chart (for categorical variable-female sex) are shown for all variables significantly associated with nuclear cataract severity in univariate analysis (Jonckheere-Terpstra trend test and Cochran-Armitage trend test). The panels represent: (A) Age, (B) AL (Axial Length), (C) TC (Total Cholesterol), (D) LDL-C (Low-Density Lipoprotein Cholesterol), (E) APO-B, (F) CR (Creatinine), (G) D-BIL (Direct Bilirubin), (H) nonHDL-C, and (I) Sex. These variables capture a broad clinical profile: AL reflects ocular biometry strongly linked to nuclear sclerosis, while systemic markers such as nonHDL-C and D-BIL highlight the complex interplay between total atherogenic lipid load, oxidative stress, and age-related nuclear cataract severity. |
Multivariate Ordinal Regression Analysis for Cataract Severity
To discern the independent associations distinct from the univariate findings, multivariate ordinal regression analyses were employed, rigorously adjusting for a comprehensive set of demographics, ocular, and systemic confounders. This approach allowed for the isolation of the most robust and subtype-specific risk factors, revealing a clear divergence in the clinical and biochemical profiles associated with different cataract morphologies.
Systemic Hyperlipidemia as an Independent Risk Factor for PSC
Multivariable ordinal logistic regression analyses (Figure 4) robustly identified systemic hyperlipidemia as a primary factor associated with PSC severity. APO-B demonstrated a consistent and independent positive association with PSC severity across all adjusted models (Model 1: OR, 1.516; 95% CI, 1.114–2.063; Model 2: OR, 1.404; 95% CI, 1.060–1.861; Model 3: OR, 1.767; 95% CI, 1.297–2.408), highlighting its role as a core biomarker reflecting the concentration of atherogenic lipoproteins.
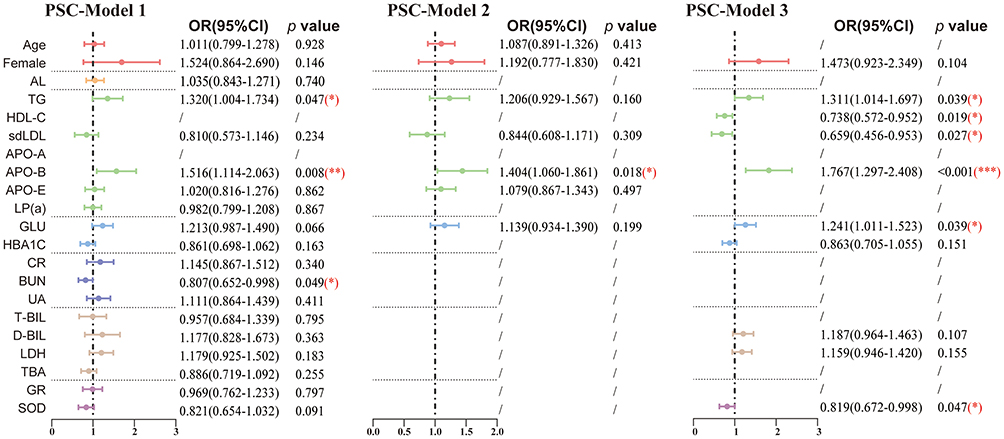 |
Figure 4 Multivariate Ordinal Regression Analysis of Factors Associated with PSC Severity. Three multivariate proportional odds models were constructed to identify factors independently associated with PSC severity. Forest plots depict odds ratios and 95% confidence intervals for variables retained in three multivariate models (Full, Clinically-important, and stepwise-selected models). Detailed model construction criteria are provided in the Methods section. Statistical significance was defined as *P<0.05, **P<0.01 and ***P<0.001. |
Furthermore, elevated TG (OR, 1.311; 95% CI, 1.014–1.697) and GLU (OR, 1.241; 95% CI, 1.011–1.523) also emerged as significant independent risk factors in the final stepwise model. The convergence of high APO-B, TG, and GLU suggests a synergistic contribution of atherogenic dyslipidemia and impaired glucose metabolism to PSC risk.
Conversely, HDL-C (Model 3: OR, 0.738; 95% CI, 0.572–0.952) demonstrated an independent inverse association. Notably, a higher level of the antioxidant enzyme SOD (Model 3: OR, 0.819; 95% CI, 0.672–0.998) was also associated with reduced odds of severe PSC, underscoring the importance of oxidative stress in its pathogenesis. An unexpected inverse association was observed for sdLDL (Model 3: OR, 0.659; 95% CI, 0.456–0.953), indicating a potential complex role for specific lipoprotein subfractions that warrants further investigation.
Independent Correlates of Cortical Cataract Severity
In contrast to other subtypes, the pathogenesis of cortical cataracts demonstrates significant heterogeneity and multifactorial complexity. Multivariate ordinal regression analyses (Figure 5) reveal that its severity is independently associated with a combination of demographic characteristics, specific lipid components, hepatic metabolism markers, and indicators of cellular damage, collectively painting a complex pathophysiological picture.
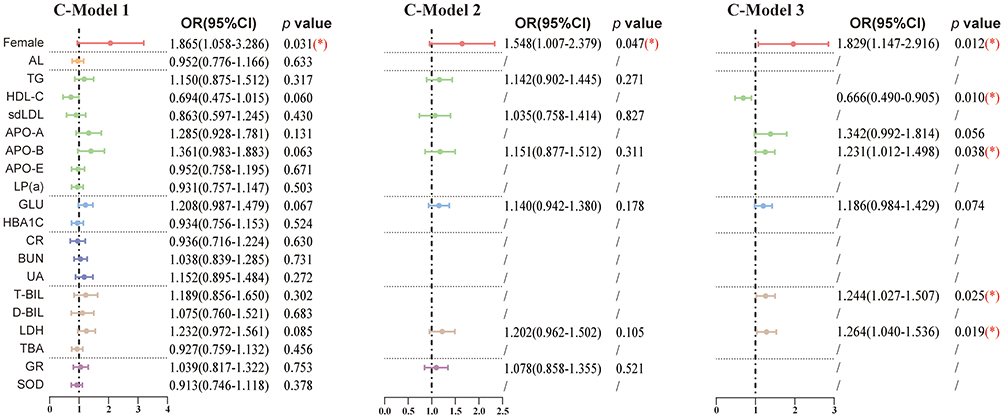 |
Figure 5 Multivariate Ordinal Regression Analysis of Factors Associated with C Severity. Three multivariate proportional odds models were constructed to identify factors independently associated with C severity. Forest plots depict odds ratios and 95% confidence intervals for variables retained in three multivariate models (Full, Clinically-inportant, and stepwise-selected models). Detailed model construction criteria are provided in the Methods section. Statistical significance was defined as *P<0.05. |
Among demographic factors, female sex emerged as a consistent and significant independent risk factor. Across all three adjusted models, females (Model 1: OR, 1.865; 95% CI, 1.058–3.286; Model 2: OR, 1.548; 95% CI, 1.007–2.379; Model 3: OR, 1.829; 95% CI, 1.147–2.916) exhibited a significantly higher risk than males. Lipid metabolism exhibits a “selective association” pattern rather than generalized dyslipidemia. Elevated APO-B was identified as an independent risk factor (Model 3: OR, 1.231; 95% CI, 1.012–1.498), while HDL-C (Model 3: OR, 0.666; 95% CI, 0.490–0.905) demonstrated a clear inverse association.
Markers of hepatic function and hemolysis showed independent association. Elevated T-BIL (Model 3: OR, 1.244; 95% CI, 1.027–1.507) was identified as a risk factor. Notably, elevated LDH (Model 3: OR, 1.264; 95% CI, 1.040–1.536) emerged as a strong independent associated factor. LDH is a marker of cell membrane integrity loss and active glycolysis, and its elevation often indicates tissue ischemia, hypoxia, or hemolytic damage. Therefore, elevated systemic LDH levels may reflect corresponding changes in LDH concentration within the ocular microenvironment or indicate a state of widespread cellular metabolic stress in the body. Such a systemic state may be associated with the development of cataracts.
Nuclear Cataract: Predominance of Age and Axial Length Independent of Systemic Lipids
The severity of nuclear cataract was clearly distinguished from the other subtypes, being predominantly associated with inherent demographic and ocular structural factors, with no independent role for systemic metabolism. As shown in Figure 6, older age (OR=1.616, 1.458, 1.608 in Model 1, 2, 3, respectively) and longer axial length (OR=1.318, 1.315, 1.310 in Model 1, 2, 3, respectively) were the most powerful and consistent independent correlates. Female sex was also confirmed as an independent inversely associated factor (Model 3: OR, 0.582; 95% CI, 0.376–0.899).
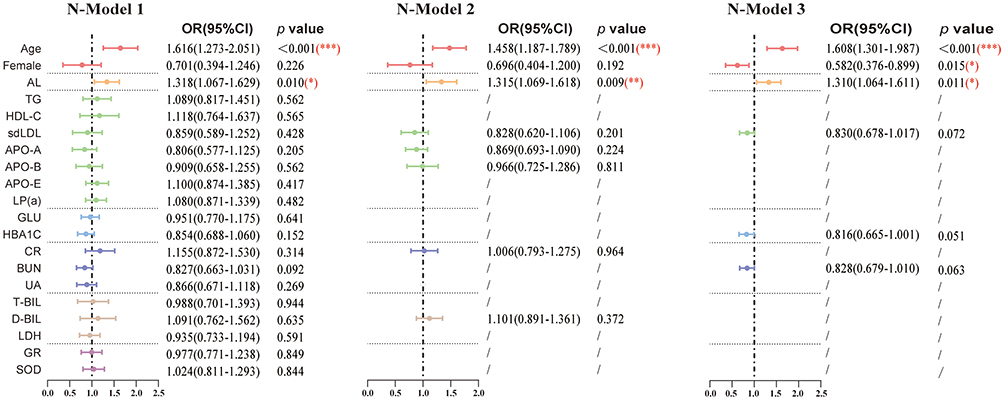 |
Figure 6 Multivariate Ordinal Regression Analysis of Factors Associated with N Severity. Three multivariate proportional odds models were constructed to identify factors independently associated with N severity. Forest plots depict odds ratios and 95% confidence intervals for variables retained in three multivariate models (Full, Clinically-inportant, and stepwise-selected models). Detailed model construction criteria are provided in the Methods section. Statistical significance was defined as *P<0.05, **P<0.01 and ***P<0.001. |
Crucially, after comprehensive adjustment for confounders, no serum lipid variable remained significantly associated with nuclear cataract severity in the final stepwise multivariate model. This clear finding strongly suggests that the severity of nuclear opacification is linked to factors largely independent of systemic metabolic status, centering instead on intrinsic ocular anatomical features and the cumulative effects of aging.
Discussion
In this cross-sectional study, we systematically evaluated the association between systemic metabolic biomarkers and the severity of ARC, with a particular focus on subtype-specific relationships. By recruiting a relatively healthy cohort free from major comorbidities and chronic medication history, and by employing rigorous subtype-stratified ordinal regression analyses, we were able to minimize confounding and clarify the distinct associative patterns characterized by different cataract morphologies.
Our principal finding is that hyperlipidemia exhibits a significant and morphology-dependent association with ARC. Specifically, elevated APOB and TG were identified as independent risk factors for PSC severity, while HDL-C demonstrated an inverse association. In contrast, cortical cataract severity was independently associated with female sex and elevated APOB, but not with the broader lipid profile. Notably, nuclear cataract severity was primarily driven by older age and longer axial length, with no independent association with systemic lipid levels.
These findings help reconcile some of the inconsistencies in the existing literature. For instance, the Framingham studies reported an association between elevated TG and PSC in men,8 while the Blue Mountains Eye Study found no link between TG and cataract subtypes.18 Moreover, analysis based on the Beaver Dam Eye Study further revealed sex-specific differences in the relationship between blood lipids and cataract,19 which adds complexity when comparing findings across studies. Such discrepancies may arise from the common practice of treating ARC as a homogeneous entity, as well as the inclusion of populations with significant metabolic comorbidities, which can obscure subtype-specific risk factors. By excluding participants with diabetes mellitus, thyroid disorders, cardiovascular abnormalities, and other chronic metabolic conditions, this study reduced confounding from comorbidities and related medications, thereby allowing a clearer assessment of the intrinsic relationship between blood lipids and cataractogenesis.
The robust and independent association of APOB and TG with PSC severity highlights the potential relevance of atherogenic dyslipidemia in its related pathophysiological processes. APO-B, as the core structural protein of LDL-C, signifies an elevated circulating burden of lipid-rich particles.20 Anterior lens epithelium exists in a state of metabolic activity21 and is persistently exposed to high oxidative stress from UV light.22 This unique environment may potentiate the pathogenic effects of infiltrating lipids. It has been reported that elevated levels of APO-B-containing lipoproteins and TG-rich particles could contribute to a pro-oxidative23 and pro-inflammatory24 state through several plausible mechanisms. These lipids are susceptible to oxidation,25 leading to generating lipid peroxidation products (LOPs) that can activate inflammatory signaling pathways, such as NF-κB26—a mechanism well-documented in the pathogenesis of atherosclerosis,27 diabetes,28 Alzheimer’s diseases,29 and so on.
The significance of systemic lipid transport is further highlighted by the finding that the concentration of free fatty acid (FFA)/albumin complexes in aqueous humor increases with age in cataract patients.30 This observation suggests a potential link between systemic lipid profiles and ocular lipotoxicity, which may, in turn, increase the susceptibility of lens epithelial cells to mitochondrial dysfunction and apoptosis, the critical event in cataractogenesis. This concept of “lipotoxic cascade” is further supported by interventional evidence; in streptozotocin-induced diabetic animals, high fat diet accelerated cataract onset independently of plasma glucose levels.31 Therefore, we hypothesize that the convergence of elevated APO-B and TG may contribute to a synergistic pathogenic microenvironment of lipotoxicity, oxidative stress, and chronic inflammation within the anterior ocular segment, potentially rendering the lens epithelium particularly vulnerable to the formation of opacity. This vulnerability could be most pronounced at the anterior and posterior capsules, which are in directly bathed in aqueous humor and vitreous humour, respectively. Accounting for the diffusion gradient characteristic of the vitreous body32 —where lipid-soluble components can accumulate and slowly diffuse anteriorly— the posterior capsule, being proximate to the retina, might consequently be exposed to a higher and more sustained concentration of lipotoxic metabolites, thereby potentially incurring a greater risk of lipid-induced damage and opacification.
The finding that nuclear severity is independent of systemic lipid profiles, being primarily driven by older age and longer axial length, aligns with established clinical observations. It is well-recognized that patients with high myopia (often defined as AL ≥ 26 mm) exhibit a marked predisposition to nuclear cataract.33 This strong association suggests shared pathogenic mechanisms between axial elongation and lens nuclear aging that operate independently of systemic metabolic dysregulation. One plausible explanation involves that they may share common underlying signaling pathways. For instance, transforming growth factor-beta (TGF-β), a key mediator in fibrotic and stress responses, has been implicated in both the development of high myopia through its effects on scleral remodeling34 and in the pathogenesis of cataracts by influencing proliferation, migration, and polarity formation.35 Therefore, our results reinforce the concept that nuclear cataract, particularly in the context of high myopia, constitutes a distinct disease entity whose progression is governed more by intrinsic ocular anatomical factors and shared local pathogenic pathways than by systemic lipid levels.
These findings have direct implications for clinical practice and risk stratification. We suggest that APO-B and TG should be integrated into the systemic evaluation of cataract patients. Elevated levels of these atherogenic lipids may serve as biomarkers for identifying patients at higher risk for severe PSC, allowing clinicians to optimize the timing of surgical intervention. The independent role of APO-B in PSC suggests that lipid-lowering therapies (eg., statins) could potentially delay the onset or progression of this specific subtype. This provides a rationale for future clinical trials to evaluate the efficacy of metabolic management in cataract prevention.
Several limitations of our study should be acknowledged. First, the inherent limitations of a cross-sectional design preclude any causal or mechanistic inferences. Our findings represent strictly associative relationships. Second, to isolate the intrinsic metabolic effects of physiological lens aging, we employed highly stringent exclusion criteria to eliminate confounding from comorbidity-induced chronic systemic inflammation and oxidative stress. While this maximized internal validity, it inevitably introduced a “healthy survivor” bias, limiting the generalizability of our findings to the typical comorbid elderly population. Third, while the total sample size was adequate for ordinal regression analysis, the distribution of patients across certain extreme subgroups (eg., PSC grade 1 and grade 4) was relatively unbalanced and small. Although our multivariate models successfully passed the Brant test—confirming that the proportional odds assumption was met and ensuring mathematical validity—this sample imbalance may still affect the ultimate stability and robustness of the regression estimates. Fourth, we excluded patients with total cataract due to difficulties in grading, which may have led to an underestimation of metabolic influences on PSC progression. Fifth, although we controlled for a wide range of confounders, residual confounding from unmeasured factors (eg., dietary habits, genetic predispositions) cannot be ruled out. Finally, the external validity of our findings may be constrained by the single-center, ethnically homogeneous (Han Chinese) nature of our cohort, necessitating future validation across broader geographic and ethnic populations. Finally, given the large number of serum biomarkers tested, formal corrections for multiple comparisons were not applied. Consequently, our univariate screening results carry a risk of Type I error, and these subtype-specific associations should be interpreted as exploratory and hypothesis-generating.
Future longitudinal and interventional studies are needed to validate the causal role of lipid biomarkers in ARC progression. Mechanistic investigations exploring the role of APO-B and TG in lens epithelial cell dysfunction, mitochondrial impairment, and oxidative stress are also warranted. Additionally, the potential utility of lipid-lowering therapies in preventing or delaying PSC warrants clinical evaluation.
Conclusions
In summary, our study demonstrates that systemic hyperlipidemia—particularly elevated APO-B and TG—is independently associated with the severity of PSC, whereas cortical and nuclear cataracts exhibit distinct associative profiles involving demographic, structural, and sex-specific factors. These findings highlight the importance of subtype-specific analyses. While our stringent exclusion criteria minimized major systemic confounders, they inherently limit the generalizability of these findings to broader, comorbid elderly populations. Although our results highlight the importance of subtype-specific analyses, the cross-sectional design precludes causal inference; therefore, the potential utility of lipid biomarkers for risk stratification and targeted prevention remains strictly exploratory and requires future validation in prospective, longitudinal cohorts.
Use of AI and AI-Assisted Technologies Statement
During the preparation of this work, the authors used Deepseek (version: DeepSeek-V3.2-Exp, developed by DeepSeek) in order to improve English grammar. The AI-assisted writing and editing process was conducted during September 2025. After using this tool, the authors carefully reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Abbreviation
ARC, Age Related Cataract; AIC, Akaike Information Criterion; AIP, Atherogenic index of Plasma; AL, Axial Length; APO-A, Apolipoprotein A; APO-B, Apolipoprotein B; APO-E, Apolipoprotein E; BUN, Blood Urea Nitrogen; C, Cortical (cataract); CR, Creatinine; D-BIL, direct Bilirubin; ECG, Electrocardiogram; EDTA, Ethylenediaminetetraacetic Acid; eGFR, Estimated Glomerular Filtration Rate; FFA, Free Fatty Acid; GLU, Fasting Glucose; GR, Glutathione Reductase; HBA1c, Glycated Hemoglobin; HDL-C, High-density Lipoprotein Cholesterol; LDH, Lactate Dehydrogenase; LDL-C, Low-density Lipoprotein Cholesterol; LOCS III, Lens Opacities Classification System III; LOPs, Lipid Peroxidation Products; LP(a), Lipoprotein(a); N, Nuclear (cataract); nonHDL-C, non-High-Density Lipoprotein Cholesterol; PSC, Posterior Subcapsular Cataract; sdLDL, Small Dense LDL; SOD, Superoxide Dismutase; TBA, Total Bile Acids; T-BIL, Total Bilirubin; TC, Total Cholesterol; TG, Triglycerides; TGF-β, Transforming Growth Factor-beta; TyG, Triglyceride-glucose Index; UA, Uric Acid; UHR, Uric Acid to High-density Cholesterol Ratio; VIF, Variance Inflation Factors.
Data Sharing Statement
On reasonable request, data supporting these findings can be obtained from the corresponding author.
Ethical Approval
This study was reviewed and approved by the Eye and Ears, Nose, and Throat Hospital Medical Ethics Committee of Fudan University (No.2024215).
Funding
This work was supported by the National Natural and Science Foundation of China (No.82070942) and Shanghai Oriental Talents Program-Top-notch Talent (BJWS2024015).
Disclosure
The authors declare that no conflict of interest exists.
References
1. Yeo D, Hwang SH, Lee S, et al. Global, regional and national burden of major blindness-associated ophthalmologic conditions, 1990-2021, with forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Br J Ophthalmol. 2025:bjo–2025–16. doi:10.1136/bjo-2025-327917
2. Asbell PA, Dualan I, Mindel J, Brocks D, Ahmad M, Epstein S. Age-related cataract. Lancet. 2005;365(9459):599–609. doi:10.1016/S0140-6736(05)17911-2
3. Tang Y, Wang X, Wang J, et al. Prevalence of age-related cataract and cataract surgery in a Chinese adult population: the taizhou eye study. Invest Ophthalmol Vis Sci. 2016;57(3):1193–1200. doi:10.1167/iovs.15-18380
4. Sabanayagam C, Wang JJ, Mitchell P, et al. Metabolic syndrome components and age-related cataract: the Singapore malay eye study. Invest Ophthalmol Vis Sci. 2011;52(5):2397–2404. doi:10.1167/iovs.10-6373
5. Reynolds R, Rosner B, Seddon JM. Serum lipid biomarkers and hepatic lipase gene associations with age-related macular degeneration. Ophthalmology. 2010;117(10):1989–1995. doi:10.1016/j.ophtha.2010.07.009
6. García-Zamora M, García-Lluch G, Moreno L, Pardo J, Cháfer-Pericás C. Influence of statin potency and liposolubility on Alzheimer’s disease patients: a population-based study. Pharmacol Res. 2024;209:107446. doi:10.1016/j.phrs.2024.107446
7. Li S, Li D, Zhang Y, Teng J, Shao M, Cao W. Association between serum lipids concentration and patients with age-related cataract in China: a cross-sectional, case-control study. BMJ open. 2018;8(4):e021496. doi:10.1136/bmjopen-2018-021496
8. Hiller R, Sperduto RD, Reed GF, D’Agostino RB, Wilson PWF. Serum lipids and age-related lens opacities: a longitudinal investigation. Ophthalmology. 2003;110(3):578–583. doi:10.1016/S0161-6420(02)01762-1
9. Jee D, Park S. Hyperglycemia and hypo-HDL-cholesterolemia are primary risk factors for age-related cataract, and a Korean-style balanced diet has a negative association, based on the korean genome and epidemiology study. J Korean Med Sci. 2021;36(23):e155. doi:10.3346/jkms.2021.36.e155
10. Shariati MM, Eslami S, Shoeibi N, et al. Development, comparison, and internal validation of prediction models to determine the visual prognosis of patients with open globe injuries using machine learning approaches. BMC Med Inform Decis Mak. 2024;24(1):131. doi:10.1186/s12911-024-02520-4
11. Palmrich P, Kalafat E, Schirwani-Hartl N, et al. Prognostic value of maternal N-terminal pro-B-type natriuretic peptide for prediction of severe maternal adverse outcome in women with pre-eclampsia. Ultrasound Obstet Gynecol. 2025. doi:10.1002/uog.70129
12. Zhu Y, Wu J, Zhao S, et al. Environmentally relevant concentrations of polystyrene nanoplastics induce Parkinson’s-like neurotoxicity in C. elegans via oxidative stress. Environ Int. 2025;206:109926. doi:10.1016/j.envint.2025.109926
13. Liu L, Zhuang S, Zheng J, et al. Treatment patterns and prognosis of cervical cancer patients aged 65 and older: a population-based cohort study. Ann Surg Oncol. 2025. doi:10.1245/s10434-025-18687-7
14. Chang Y, Kim J, Woo HG, Ryu DR, Oh HJ, Song TJ. Plasma fibroblast growth factor 23 concentration is associated with intracranial cerebral atherosclerosis in acute ischemic stroke patients. J Clin Neurol. 2020;16(1):29–36. doi:10.3988/jcn.2020.16.1.29
15. Li Y, Zhang L, Zhai L, et al. Association between triglyceride-glucose index and obstructive sleep apnea severity in hypertensive patients with co-existing OSA: a cross-sectional study. Front Endocrinol. 2025;16:1669661. doi:10.3389/fendo.2025.1669661
16. Dires AA, Workie DL, Teklie AK. Exploring factors influencing childhood immunization status in east Africa using multilevel ordinal logistic regression analysis. Front Public Health. 2024;12:1508303. doi:10.3389/fpubh.2024.1508303
17. La Sala L, Busetto L, Carlini V, et al. Body mass index (BMI) associates with frequency of arterial hypertension and type 2 diabetes in obese patients candidates for bariatric surgery. Cardiovasc Diabetol. 2025;24(1):445. doi:10.1186/s12933-025-02989-x
18. Ghaem Maralani H, Tai BC, Wong TY, et al. Metabolic syndrome and risk of age-related cataract over time: an analysis of interval-censored data using a random-effects model. Invest Ophthalmol Vis Sci. 2013;54(1):641–646. doi:10.1167/iovs.12-10980
19. Klein BEK, Klein R, Lee KE, Gangnon RE. Incidence of age-related cataract over a 15-year interval the beaver dam eye study. Ophthalmology. 2008;115(3):477–482. doi:10.1016/j.ophtha.2007.11.024
20. Ghodsi S, Meysamie A, Abbasi M, et al. Non–high-density lipoprotein fractions are strongly associated with the presence of metabolic syndrome independent of obesity and diabetes: a population-based study among iranian adults. J Diabetes Metab Disord. 2017;16:25. doi:10.1186/s40200-017-0306-6
21. Hejtmancik JF, Riazuddin SA, McGreal R, Liu W, Cvekl A, Shiels A. Lens biology and biochemistry. Prog Mol Biol Transl Sci. 2015;134:169–201. doi:10.1016/bs.pmbts.2015.04.007
22. Øsnes-Ringen O, Azqueta AO, Moe MC, et al. DNA damage in lens epithelium of cataract patients in vivo and ex vivo. Acta Ophthalmol. 2013;91(7):652–656. doi:10.1111/j.1755-3768.2012.02500.x
23. Zabłocka-Słowińska K, Płaczkowska S, Skórska K, et al. Oxidative stress in lung cancer patients is associated with altered serum markers of lipid metabolism. PLoS One. 2019;14(4):e0215246. doi:10.1371/journal.pone.0215246
24. Coelewij L, Waddington KE, Robinson GA, et al. Serum metabolomic signatures can predict sub-clinical atherosclerosis in patients with SLE. Arterioscler Thromb Vasc Biol. 2021;41(4):1446–1458. doi:10.1161/ATVBAHA.120.315321
25. Matsumoto RLT, Mendonça S, De Oliveira DM, Souza MF, Bastos DHM. Effects of maté tea intake on ex vivo LDL peroxidation induced by three different pathways. Nutrients. 2009;1(1):18–29. doi:10.3390/nu1010018
26. Tanaka M, Sato A, Kishimoto Y, Mabashi-Asazuma H, Kondo K, Iida K. Gallic acid inhibits lipid accumulation via AMPK pathway and suppresses apoptosis and macrophage-mediated inflammation in hepatocytes. Nutrients. 2020;12(5):1479. doi:10.3390/nu12051479
27. Ren R, Hashimoto T, Mizuno M, et al. A lipid peroxidation product 9-oxononanoic acid induces phospholipase A2 activity and thromboxane A2 production in human blood. J Clin Biochem Nutr. 2013;52(3):228–233. doi:10.3164/jcbn.12-110
28. Oyenihi AB, Chegou NN, Oguntibeju OO, Masola B. Centella asiatica enhances hepatic antioxidant status and regulates hepatic inflammatory cytokines in type 2 diabetic rats. Pharm Biol. 2017;55(1):1671–1678. doi:10.1080/13880209.2017.1318293
29. Jakubek P, Parchem K, Wieckowski MR, Bartoszek A. The interplay between endogenous and foodborne pro-oxidants and antioxidants in shaping redox homeostasis. Int J Mol Sci. 2024;25(14):7827. doi:10.3390/ijms25147827
30. Glaesser D, Iwig M. Increased molar ratio of free fatty acids to albumin in blood as cause and early biomarker for the development of cataracts and Alzheimer’s disease. Exp Eye Res. 2024;243:109888. doi:10.1016/j.exer.2024.109888
31. Tsutsumi K, Inoue Y, Yoshida C. Acceleration of development of diabetic cataract by hyperlipidemia and low high-density lipoprotein in rats. Biol Pharm Bull. 1999;22(1):37–41. doi:10.1248/bpb.22.37
32. Shui YB, Holekamp NM, Kramer BC, et al. The gel state of the vitreous and ascorbate-dependent oxygen consumption. Arch Ophthalmol. 2009;127(4):475–482. doi:10.1001/archophthalmol.2008.621
33. Tan Y, Liu L, Li J, Qin Y, Sun A, Wu M. Evaluation of preoperative corneal astigmatism using swept-source optical biometry in Chinese cataract surgery candidates with high myopia: a prospective, comparative observational study. Ann Transl Med. 2021;9(8):618. doi:10.21037/atm-20-6757
34. Liu S, Chen T, Chen B, Liu Y, Lu X, Li J. Lrpap1 deficiency leads to myopia through TGF-β-induced apoptosis in zebrafish. Cell Commun Signal. 2022;20(1):162. doi:10.1186/s12964-022-00970-9
35. Wei L, Du Y, Gao S, et al. TGF-β1-induced m6A modifications accelerate onset of nuclear cataract in high myopia by modulating the PCP pathway. Nat Commun. 2025;16(1):3859. doi:10.1038/s41467-025-58995-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.