Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Sub-Optimal Chronic Obstructive Pulmonary Disease (COPD) Management in India: Findings from a Community-Based Study
Authors Jarhyan P, Hutchinson A ![]() , Khatkar R, Prabhakaran D, Mohan S
, Khatkar R, Prabhakaran D, Mohan S
Received 8 October 2024
Accepted for publication 6 April 2025
Published 30 June 2025 Volume 2025:20 Pages 2131—2142
DOI https://doi.org/10.2147/COPD.S499792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Prashant Jarhyan,1 Anastasia Hutchinson,2 Rajesh Khatkar,1 Dorairaj Prabhakaran,1,3,4 Sailesh Mohan1– 3
1Centre for Chronic Conditions and Injuries (CCCI), Public Health Foundation of India, Gurugram, India; 2Institute of Health Transformation, Faculty of Health, Deakin University, Burwood, Melbourne, Australia; 3Centre for Chronic Disease Control (CCDC), Delhi, India; 4London School of Hygiene and Tropical Medicine, London, UK
Correspondence: Sailesh Mohan, Public Health Foundation of India, 431A, 4th Floor Rectangle No. 1, Behind Saket Sheraton Hotel, Commercial Complex D4, Saket New Delhi, New Delhi, 110017, India, Email [email protected]
Background and Objective: Despite the second most common cause of disease burden, there are few studies reporting the prevalence, awareness, and treatment rates of COPD in India.
Methods: A community-based cross-sectional study was conducted among people aged ≥ 40 years residing in rural and urban areas of Sonipat district in North India using a multistage random sampling technique. COPD was defined as self-reported physician diagnosed COPD, emphysema, chronic bronchitis or being on treatment for COPD. Additional cases were detected using a validated sequential screening strategy, ie, administering the Lung Function Questionnaire (LFQ) followed by the pocket spirometry and confirmation by post-bronchodilation spirometry. Awareness was defined as self-reported diagnosed cases of COPD or self-reported treatment. Treatment was defined as self-reported intake of oral or inhalational corticosteroids and/or bronchodilators. Trained Community Health Workers interviewed the study participants using a paper-based validated questionnaire, screened for COPD with the LFQ and conducted the pocket spirometry. Confirmation of COPD using post-bronchodilation gold standard spirometry was conducted by trained physician researchers. Age-standardized estimates were calculated for the prevalence, awareness, and treatment of COPD.
Results: The overall age-standardised prevalence of COPD in our study was 8.6% (95% CI: 7.5– 9.8) with higher prevalence in men and rural population. The overall awareness of COPD was 75.1% (95% CI: 68.5– 80.7) with lower awareness among people who ever-smoked [33.9% (32.0– 35.8)], currently smoked [29.6% (27.8– 31.5)] and among those with post-bronchodilator confirmed diagnosis of mild COPD (4.8%). Less than half (45.7%) of participants with COPD reported taking bronchodilators and/or corticosteroids.
Conclusion: The awareness-treatment gap in COPD was high in the study population. There is a need to strengthen the public health system along with systematic training of health care providers to provide appropriate treatment to people with COPD.
Keywords: chronic obstructive pulmonary disease, COPD, public health, COPD management, lung health
Key Messages
What is already known on this topic?
In India, COPD is the second most prevalent cause of death. However, there is a dearth of data from community-based studies on the prevalence, awareness, and treatment rates to help improve public health policies for COPD management and control.
What this study adds?
This study gives a population-based estimate of the prevalence of COPD, together with information on treatment rates, awareness, and variations based on rural and urban status. It also employs a sequential technique to enable more precise detection of COPD prevalence.
How this study may affect research, practice or policy?
This study highlights the important gap in the utilisation of recommended inhalational treatments of COPD. The findings will help policy makers and researchers to focus on improving the access to inhalational drugs for people with COPD, especially in rural areas in India.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is one of the most common chronic respiratory diseases and has a worldwide prevalence of 10.1% in adults ≥40 years of age.1 It is also the third leading cause of death in the world and 90% of all COPD-related death occur in low and middle-income countries.2 India is undergoing rapid demographic and epidemiologic transitions which have contributed to an increasing prevalence of COPD.3 The global burden of disease study has estimated an increase from 28.1 million to 55.3 million, between 1990 and 2016 in India.4 COPD also contributed to 8.7% of total deaths and 4.8% of Disability Adjusted Life Years (DALYs), ranking as the second most common cause of disease burden after coronary artery disease in India.3
Internationally, substantial research has been conducted on COPD disease burden, its severity and clinical heterogeneity in different populations. However, there are limited data from India. Despite the huge burden, COPD largely remains undetected due to low awareness in the population and underdiagnosis in clinical practice.5 Population-level disease prevalence is essential to determine the baseline disease and risk factors burden.6,7 Enhancing disease awareness can improve the diagnosis, treatment and management of risk factors.8 Overall, there are very few published studies on the rural-urban and gender differentials in the prevalence of COPD, its awareness and treatment in India, which is crucial to framing policies for efficient allocation of resources for disease control.9,10 Therefore, the aim of this community-based cross-sectional study was to assess the prevalence, awareness, and treatment of COPD in rural and urban areas of Sonipat district of Haryana state in North India.
Methods
Study Design
A community-based cross-sectional study was embedded within one of the sites of a large community-based research project entitled “UDAY: a comprehensive diabetes and hypertension prevention and management program in India”, the details which have been published previously.11 Briefly, UDAY was implemented in a population of about 100,000 each in rural and urban subsites in north India (Sonipat district in Haryana state) and south India (Visakhapatnam district in Andhra Pradesh state). In each rural and urban subsite, trained project staff referred to as Community Health Worker (CHW; 1 CHW per 5000 population), selected from the same area, conducted surveys and screened adults aged ≥30 years for the presence of diabetes and hypertension, subsequently linking those at high risk or with diabetes and/or hypertension to the healthcare system. CHWs also provided tailored health education to patients regarding non-pharmacological management of diabetes and hypertension and educated the general population about modification/reduction of risk factors.
Study Population
Inclusion criteria: The study population included individuals aged ≥40 years residing in the urban and rural areas within the study site of UDAY in Sonipat district. Exclusion criteria: We excluded individuals bedridden due to serious illness, those with cognitive impairment and those who did not provide the written informed consent to take part in the study.
Definitions
COPD
COPD was defined as the presence of self-reported physician diagnosed COPD/emphysema, or the presence of chronic bronchitis according to the Medical Research Council (MRC) definition12 or any self-reported treatment (bronchodilators and/or corticosteroids). Additional cases were diagnosed using the sequential strategy previously validated to detect COPD using the Lung Function Questionnaire (LFQ ≤ 18) followed by the pocket spirometry (FEV1/FEV6 <0.70) and subsequentconfirmation by post-bronchodilation spirometry.13
Awareness of COPD
Awareness of COPD was defined as self-reported diagnosed cases of COPD, emphysema, chronic bronchitis, or any self-reported treatment with bronchodilators and/or corticosteroids.
Treatment
Treatment was defined as self- reported intake of either oral or inhalational corticosteroids and/or bronchodilators.
Data Collection
Community Health Workers (CHWs, n=40) were trained to conduct interviews, screen individuals for the presence of COPD using the Lung Function Questionnaire (LFQ) and pocket spirometer. The study tools were pre-tested in rural and urban areas not selected for this study.
Eligible participants were recruited using a three-stage random sampling process. In the first stage, 30 clusters each were randomly selected in rural and urban sub-sites using the probability proportional to size method. In the second stage, 20 households were selected randomly within each cluster. Finally, one eligible man and one woman each were randomly selected among the eligible household members using the Kish table.14
Individuals within the selected households were interviewed by the CHWs using a questionnaire adapted from the Burden of Obstructive Lung Disease (BOLD) and UDAY study and screened using the Lung Function Questionnaire (LFQ) for the presence of COPD.11,15,16 The UDAY population survey questionnaire was used to collect the socio-demographic information and information on tobacco and alcohol consumption. The BOLD study questionnaires were used to collect the data on occupational exposures, biomass fuel smoke exposure, respiratory symptoms, comorbidities, medication and health care utilisation. Additionally, the COPD Assessment Test (CAT)17 was used to assess disease-specific quality of life among the study participants. The data collection was carried out from January to December 2018. CHWs also screened eligible individuals for the detection of COPD using the LFQ and the pocket spirometry for the study. Trained physician researchers conducted pre- and post-bronchodilation confirmatory spirometry using a diagnostic quality portable spirometer.
Statistical Analysis
Sample Size Calculation
We estimated that a sample size of 457 at one site would produce a two-sided 95% confidence interval with a width equal to 0.040 (0.03–0.07) when the sample proportion meeting the criteria for COPD is 0.050. It was anticipated that there would be between site differences in the prevalence of COPD and as we could not find the Intracluster Correlational Coefficient (ICC) to estimate the prevalence of COPD in studies from India, we used a design effect of 2. With an anticipated non-participation of 20%, we estimated that a final sample size of 1100 participants would be required, each from the urban and rural sub-sites, providing an overall sample size of 2200 for this study.18
Data Analysis
The study data were entered in the Microsoft excel spreadsheet by a data entry operator not involved in data collection or data analysis and data were cross checked for any discrepancies or missing data. Missing data or discrepancies were corrected by contacting participants telephonically. For those who could not be contacted by phone, an additional home visit was made by the trained field staff to collect the missing data. Data analyses were conducted using STATA 16 (StataCorp. 2012. Stata Statistical Software: Release 16. College Station, TX: StataCorp LP).
Population-level weights were calculated at the cluster and the household levels by calculating the probability of the selection of each cluster from the total number of clusters and the probability of selection of eligible households’ members within each household. We further created sample weights as the inverse of the multiplication of the population level weights. Age-standardised weights for the age categories were calculated using the weights obtained from the respective age categories from the Census of India population 2011.19 The overall age-standardised prevalence and awareness estimates along with their 95% confidence intervals (95% CI) were calculated.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics committee of PHFI (Reference no.: TRC-IEC-356/17) and Deakin University Human Research Ethics committee (DUHREC) (Reference no.: 2016–383). Written informed consent was obtained from each study participant by the CHWs. All participants diagnosed with COPD were referred to the nearest public health care facility for further evaluation and management. Patients with severe symptoms were provided with an additional referral linkage to the respiratory physician in the district hospital at Sonipat.
Results
A total of 2334 participants (1215 in rural and 1119 in urban) were participated in the study. The mean (±SD) age of the study participants was 55.9 (10.9) years, 45.7% (95% CI: 43.6–47.7) were men and 52.2% (95% CI: 50.1–54.3) of the participants were from the rural area (Table 1).
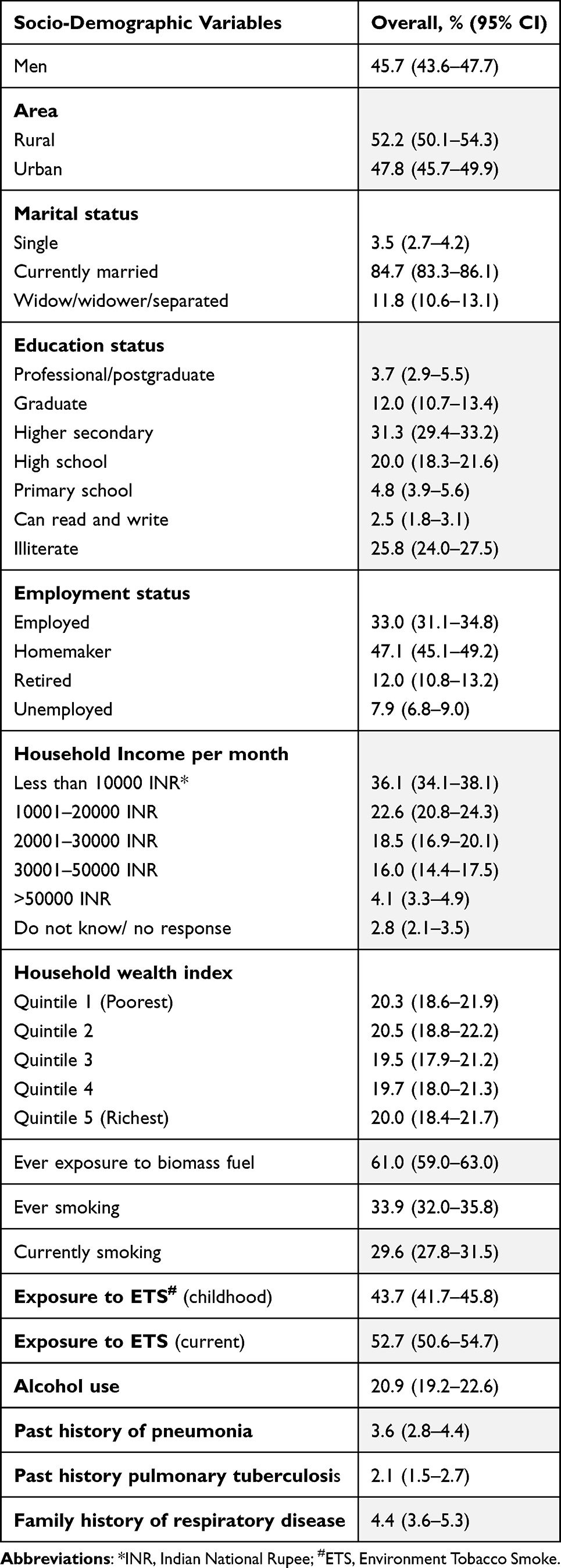 |
Table 1 Characteristics of the Study Participants (N = 2334) |
Prevalence
The overall age-standardised prevalence of COPD was 8.6% (95% CI: 7.5–9.8); the prevalence of COPD was higher among men [10.4% (8.8–12.3)] as compared to women [6.5% (5.6–8.5)] and among participants residing in the rural area [rural: 10.4% (8.8–12.2); urban area: 6.8% (5.4–8.4)].
Of the total 2334 participants, on using the validated sequential strategy to detect people with COPD, 438 (18.8%) had LFQ score of ≤18, 145 (6.2%) had a FEV1/FEV6 value <0.7 on pocket spirometry and 103 (4.4%) had a FEV1/FVC ratio <0.70 with gold standard post-bronchodilator spirometry confirmed COPD.
The age-standardised prevalence of COPD among those who had undergone gold standard post-bronchodilator spirometry, was 4.2% (3.5–5.1%) with higher prevalence among men [men: 6.9% (5.6–8.5%); women: 1.5% (95% CI: 1.0–2.3%)] and among those residing in the rural area [5.9% (4.7–7.3%)] as compared to those residing in the urban area [2.5% (1.8–3.7%)] (Table 2). Among those with gold standard post-bronchodilator spirometry confirmed COPD, 12.7% (8.3–18.9) had mild, 43.0% (28.0–59.4) had moderate, 38.7% (24.3–55.5) had severe and 5.5% (2.8–11.0) had very severe COPD according to the GOLD severity category.20
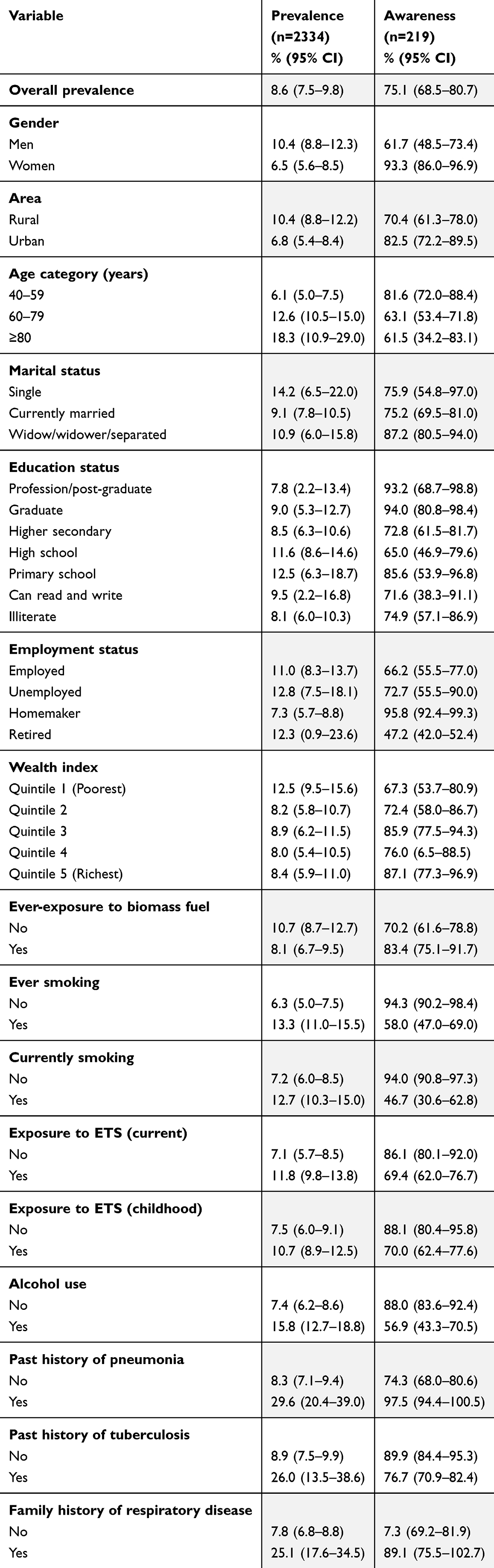 |
Table 2 Age Standardized Estimates of Prevalence and Awareness of COPD |
Awareness
Overall, 75.1% (68.5–80.7) of the participants were aware that they had COPD. COPD awareness was significantly higher among women [93.3% (95% CI: 86.0–96.9)] than men [61.7% (48.7–73.4)], and younger participants [40–49 years: 81.6% (72.0–88.4); 60–79 years: 63.1% (53.4–71.8); ≥80years: 61.5% (34.2–83.1)]. The awareness was lower among those who ever smoked and were currently smoking [ever smoked: 33.9% (32.0–35.8); currently smoking: 29.6% (27.8–31.5)]. Though, the awareness of COPD was low among those with post-bronchodilator confirmed diagnosis of COPD [38.7% (95% CI: 24.9–54.8%)], it was higher among those with very severe disease (77.8%) as compared to those with moderate (47.5%) and severe disease (45.2%) (Table 2).
Treatment
Less than half of the total participants with COPD (45.7%) reported that they were using bronchodilators and/or corticosteroids for treatment. The proportion receiving treatment was even lower [32.0% (95% CI: 23.7–41.7%)] among those with post-bronchodilator confirmed diagnosis of COPD. Most participants 29 (35.3%) were taking oral bronchodilators, (oral methylxanthines: 62% and oral salbutamol: 34.5% participants) while inhaled corticosteroids (IC) or their combination with other respiratory drugs were reported taken only by 23.2% participants. A higher percentage of urban participants reported taking inhalational Short Acting Beta Agonists (SABA) in combination with another inhalational drugs (SABA+:19.4%) and Inhalational Corticosteroids (IC) in combination with other inhalational drugs (IC+:51.6%) as compared to their rural counterparts (SABA+: 5.9%, IC+: 5.9%). Use of short and long-acting muscarinic agonists (SAMA, LAMA) was even lower (4.9%) (Table 3).
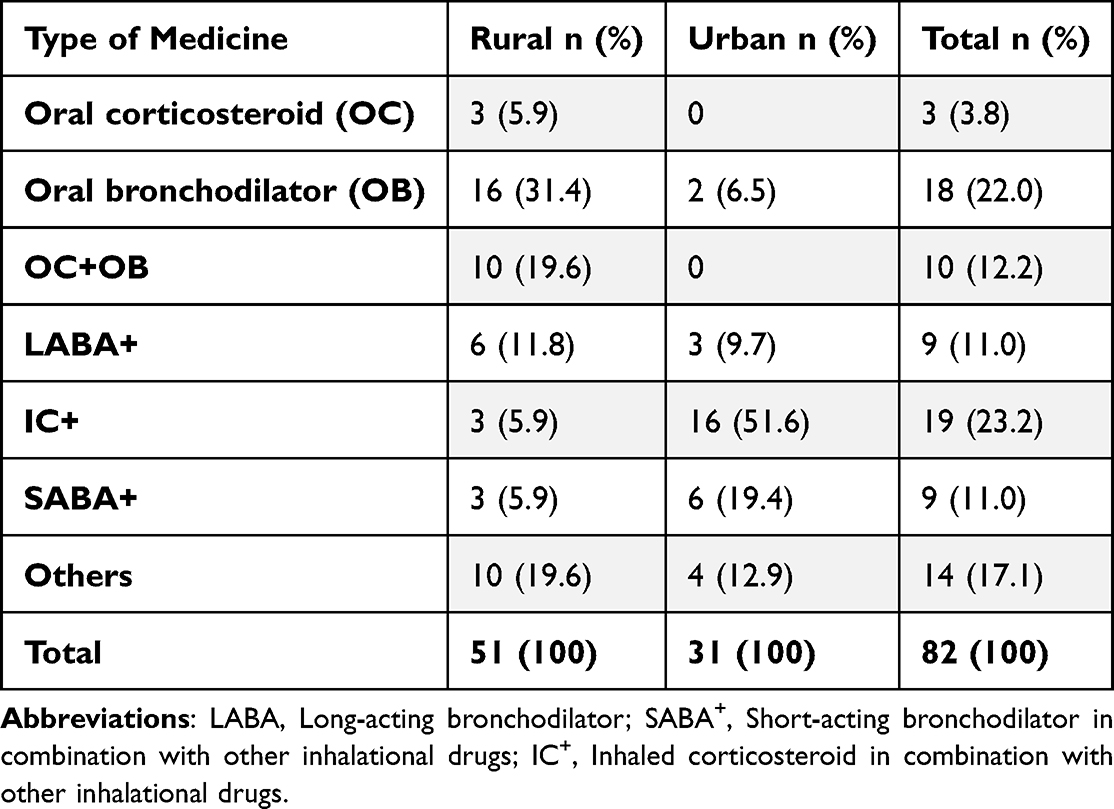 |
Table 3 Type of Respiratory Medications Used by Participants with COPD |
Impact of COPD on the Disease Specific Quality of Life
Respiratory symptoms had a substantial effect on day-to-day activities of participants with COPD. COPD was responsible for very high impact level (CAT score > 30) on the disease-specific quality of life among 8.0% (3.7–12.3), high impact level (CAT score > 20) in 20.4% (1.4–2.6), medium impact level (CAT score 10–20) in 35.2% (27.9–42.4) and low impact level (CAT score > 10) in 36.4% (29.3–43.6) of the participants with COPD. There were no significant rural-urban differences in the CAT scores.
COPD Control
Most of the participants with COPD reported 0–1 exacerbation [74.0% (67.2–80.8)] in the past 12 months and ≥2 exacerbations were reported by 26.0% (19.2–32.8) of the participants. Among those with spirometry confirmed COPD, 24.6% (14.2–39.2%) were in GOLD A Stage, 50.0% (34.3–65.8%) in B stage, 2.7% (1.0–7.4%) in C Stage and 22.6% (11.2–40.6%) in GOLD D stage of GOLD ABCD assessment of COPD. The GOLD stage D participants were higher in rural area [31.4% (23.2–41.0)] as compared to urban [9.6% (4.6–18.8)] area (Table 4).
 |
Table 4 Estimates of COPD GOLD Severity, Dyspnoea, Disease Specific Quality of Life, Exacerbations, Hospitalisations and GOLD ABCD Stages |
Discussion
We conducted a comprehensive population-based cross-sectional survey to assess the prevalence of COPD, its awareness, treatment, disease-specific quality of life, and prevalence of disease severity and control using the GOLD criteria among the rural and urban population in Sonipat district of Haryana state in Northern India.
Our study revealed a prevalence of COPD [8.6% (95% CI: 7.5–9.8)] which is similar to the regional and global COPD prevalence and previous studies conducted in the same region.1,9,21,22 However, previously many studies in India have reported the prevalence of chronic bronchitis to report the prevalence of COPD and few studies have assessed the prevalence of COPD with post-bronchodilation spirometry.9 Though, conducting post-bronchodilation spirometry to detect COPD is the gold-standard method to detect COPD, it requires tremendous resources in terms of time, trained manpower and funds.9 Therefore, new strategies need to be developed and tested to assess the accurate burden of COPD especially in low and low middle income countries.9 In this study, we used self-reported diagnosis of chronic bronchitis, emphysema and COPD to define COPD and additionally conducted a validated sequential strategy to detect additional COPD cases.
This study also revealed higher prevalence of COPD with increasing age, among men, those residing in rural areas, ever or currently smoking status, exposure to environmental tobacco smoke, alcohol use, previous history of pneumonia and previous history of tuberculosis. The higher prevalence of COPD with increasing age, among men as compared to women in our study is consistent with the findings from other studies in India which probably results from higher prevalence of tobacco smoking among men.9 Increasing age is a known risk factor for developing COPD.23 We also found a higher age-standardised prevalence of COPD in age groups >50 years as compared to 40–49 years of age which was also found by other studies.22,24
This study also showed higher age-adjusted prevalence of past pneumonia among those with COPD than those without COPD. Pneumonia is a known risk factor for and complication of COPD.25,26 The risk of pneumonia increases with treatment of COPD with inhaled corticosteroids (IC),26 however IC were not widely used in this study population with only 19 participants reporting that they were using these inhalers. It is therefore relatively unlikely that IC use was associated with increased risk in the study population. The high prevalence of a history of pneumonia among those with COPD does highlight that if inhaled medications became more widely available in low resources settings, then the introduction of IC treatment may need to be implemented with caution and adequate patient follow-up.
There was a significantly high prevalence of COPD among those with a past history of treatment for tuberculosis in our study. In a systematic review, Allwood et al found a positive association between a past history of tuberculosis and COPD.27 They suggested several mechanisms resulting in structural damage of airways and increased emphysematous changes related to recurrent or chronic inflammation for the development of COPD among those with history of past tuberculosis.27 Gupte et al found a high burden of lung function defects and COPD among recently treated tuberculosis patients in two tertiary care institutions in India and recommended screening for chronic lung diseases and linkage of treated patients to respiratory health clinics in the routine management plan.28 High burden of tuberculosis may contribute to high burden of COPD in India. This necessitates the need to strengthen the existing primary health care system and training of physician and non-physician health personnel for appropriate screening, diagnosis and treatment of COPD.
Another important finding in our study was the lower awareness of the disease among ever smoking and currently smoking individuals and those with moderate and severe COPD. Lower awareness of COPD among tobacco smoking individuals and those with comparatively advanced stage, especially severe disease is worrisome as tobacco smoking is the most important risk factor for the development of COPD. This needs population-based strategies to generate awareness, timely COPD detection and appropriate management. There is also an urgent need to evaluate strategies to increase the screening of tobacco smoking individuals for COPD and strengthening the public health infrastructure for initiation of appropriate pharmacological and non-pharmacological management to decrease the disease progression.3,29
Our study also highlighted the lower utilisation of inhalational drugs and higher reliance on oral treatment of COPD, especially in rural area. Despite the high awareness, only about half of those with COPD were taking treatment and use of inhalational drugs was low in our study. Use of oral bronchodilators for treating COPD, which was prevalent especially in rural areas, has not been reported by previous studies in India. Poor availability of inhalational drugs in the public health system in India and their higher costs, patient’s discomfort and poor training in taking inhalational drugs are widely known factors that decrease the acceptability of inhalational therapies.30 This requires the strengthening of the current public health system and capacity building of health providers and pharmacists to educate patients regarding correct inhalational techniques.
In our study, there was high symptom burden of COPD (dyspnoea, higher CAT scores and number of exacerbations) among those residing in the rural area. A study among people with COPD, consulting for routine care from respiratory disease-specific programmes in Europe, USA and China found that high symptom burden was particularly pronounced in China, where treatment with oral xanthines was common.31 In our study, common use of oral bronchodilators for COPD treatment in rural area may be contributing to higher symptom burden and reflects poor access to quality care, including inhalational medications. Improving access to inhalational drugs along with education on inhalational techniques at primary health care level is required for better control of symptoms and reducing COPD-related morbidity.
About one-fourth of the participants with COPD reported ≥2 exacerbations, poor control of COPD, in this study. There are limited data on exacerbations from community-based studies in India. As COPD exacerbations are associated with higher mortality rates and poor quality of life, prolonged use of appropriate inhalational drugs and training for guideline-based treatment is required.32 There was poor control of COPD among those residing in the rural area which may be due to the higher use of oral bronchodilators and exposure to risk factors. Improving access to inhalational drugs along with pulmonary rehabilitation especially in rural area is required for better control of symptoms and prevention of exacerbations and related hospitalisations.
The major strength of this study is that it highlights the differential COPD burden, awareness, treatment and disease-specific quality of life according to socio-demographic characteristics (rural-urban differences) in India. This study also underlines the need to further investigate the attributable risk of COPD in individuals with previous history of pneumonia and pulmonary tuberculosis. Larger epidemiological studies representing different representative regions of India are required to generate the evidence on COPD burden, awareness, treatment and disease-specific quality of life to guide COPD control policy in India.
However, there were some limitations also. Firstly, the definition of COPD included self-reported history of COPD, emphysema and chronic bronchitis which may introduce some misclassification bias for determining COPD prevalence in this study. In India, patients may not be able to differentiate between COPD and asthma.33 To overcome this bias, we specifically trained our research staff to differentiate between COPD and asthma and provided the definitions of each condition in the questionnaire along with the options to minimize the misclassification bias. The inclusion of self-reported cases of COPD, chronic bronchitis and emphysema in the case definition of COPD besides the spirometry confirmed cases contributed to the overall prevalence of COPD in this study. This included participants as cases who were missed as they could not undergo the pocket spirometry and diagnostic spirometry due to various reasons (medically unfit, unable to perform the spirometry or refused) and those participants who might have been classified as false negative by the two-step screening strategy, contributing to a lower prevalence estimate in our study. In India, many people use informal health care providers (practitioners who do not have a qualification to treat and prescribe allopathic medicines) for availing outpatient and inpatient health care,34 which may have compensated for the number of hospitalisations during acute exacerbations in people with COPD in our study. However, we used ‘seeking medical care’ as a proxy for exacerbation as a measure for hospitalisation and did not find a difference in the proportions of control according to the GOLD ABCD approach. Another major limitation of this study is that it was conducted before the COVID-19, also known as severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) pandemic. The prevalence estimates may have increased since a huge proportion of population have been affected by SARS-COV-2. The long-term effects of SARS-COV-2 on the lung function and its attributable risk for COPD development need to be further assessed.9
Conclusion
Despite the high prevalence, the awareness of COPD among high-risk population, especially smokers, is low. Additionally, there is a huge treatment gap and underutilisation of recommended inhalational treatments. There is an urgent need to generate awareness about COPD and its risk factors, especially in rural areas and concomitantly strengthen the public health system along with capacity building of physician and non-physician healthcare workers for the timely detection and appropriate management COPD.
Acknowledgment
This study was supported by a PhD scholarship grant under the Deakin India Research Initiative to Prashant Jarhyan. Prashant Jarhyan was also partly supported by the Public Health Foundation of India and by a VECD Global Health Fellowship, funded by the Fogarty International Center (FIC) of the NIH (3D43TW009337-09S3). Prashant Jarhyan and Sailesh Mohan were also partly supported by grants from the UK NIHR (NIHR203257) and European Commission under EU Horizon CORONA 2021 programme.The funders had no role in the design, conduct, analysis of the research or manuscript writing.
Disclosure
The authors report no conflict of interest in this work.
References
1. Buist AS, McBurnie MA, Vollmer WM, et al. BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4.
2. WHO. Chronic obstructive pulmonary disease (COPD); 2023 [cited November 11, 2023]. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
3. India State-Level Disease Burden Initiative CRD Collaborators. The burden of chronic respiratory diseases and their heterogeneity across the states of India: the Global Burden of Disease Study 1990-2016, Lancet Glob Health. 2018;6(12):e1363–e1374. PMID: 30219316; PMCID: PMC6227385. doi:10.1016/S2214-109X(18)30409-1
4. Soriano JB, Kendrick PJ, Paulson KR; GBD Chronic Respiratory Disease Collaborators, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3.
5. Lamprecht B, BOLD Collaborative Research Group, the EPI-SCAN Team, the PLATINO Team, and the PREPOCOL Study Group, et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest. 2015;148:971–985.
6. Lopez AD, Mathers CD, Ezzati M, et al. Measuring the global burden of disease and risk factors, 1990–2001. In: Lopez AD, Mathers CD, Ezzati M, editors. Global Burden of Disease and Risk Factors. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006. https://www.ncbi.nlm.nih.gov/books/NBK11817/.
7. Stansfield SK, Walsh J, Prata N, et al. Information to improve decision making for health. In: Jamison DT, Breman JG, Measham AR, et al. editors. Disease Control Priorities in Developing Countries.
8. Almuzaini AS, Algeffari M, Alsohaibani A, et al. Awareness of chronic obstructive pulmonary disease and its risk factors among the adult population of the Qassim Region, Saudi Arabia. Cureus. 2023;15(9):e44743. PMID: 37809115; PMCID: PMC10555947. doi:10.7759/cureus.44743
9. Jarhyan P, Hutchinson A, Khaw D, et al. Prevalence of chronic obstructive pulmonary disease and chronic bronchitis in eight countries: a systematic review and meta-analysis. Bull World Health Organ. 2022;100(3):216–230. PMID: 35261410; PMCID: PMC8886252. doi:10.2471/BLT.21.286870
10. McKay AJ, Mahesh PA, Fordham JZ, Majeed A. Prevalence of COPD in India: a systematic review. Prim Care Respir J. 2012;21(3):313–321. doi:10.4104/pcrj.2012.00055
11. Mohan S, Jarhyan P, Ghosh S, et al. UDAY: a comprehensive diabetes and hypertension prevention and management program in India. BMJ Open. 2018;8(6):e015919. doi:10.1136/bmjopen-2017-015919
12. Stuart-Harris CH, Crofton J, Gilson JC, et al. Definition and classification of chronic bronchitis for clinical and epidemiological purposes. A report to the medical research council by their committee on the aetiology of chronic bronchitis. Lancet. 1965;1(7389):775–779.
13. Jarhyan P, Hutchinson A, Khatkar R, et al. Diagnostic accuracy of a two-stage sequential screening strategy implemented by community health workers (CHWs) to identify individuals with COPD in Rural India. Int J Chron Obstruct Pulmon Dis. 2021;16:1183–1192. PMID: 33958862; PMCID: PMC8096419. doi:10.2147/COPD.S293577
14. Kish L. A procedure for objective respondent selection within the household. Journal of the American Statistical Association. 1949;44(247):380–387. doi:10.1080/01621459.1949.10483314
15. Buist AS, Vollmer WM, Sullivan SD, et al. The burden of obstructive lung disease initiative (BOLD): rationale and design. COPD. 2005;2(2):277–283. PMID: 17136954. doi:10.1081/COPD-57610
16. Hanania NA, Mannino DM, Yawn BP, et al. Predicting risk of airflow obstruction in primary care: validation of the lung function questionnaire (LFQ). Respir Med. 2010;104(8):1160–1170. doi:10.1016/j.rmed.2010.02.009
17. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34:248–654.
18. Fleiss JL, Levin B, Paik MC. Statistical Inference for a Single Proportion. In: Shewart WA, Wilks SS, Fleiss JL, Levin B, Paik MC, editors Statistical Methods for Rates and Proportions. 3rd ed. Hooboken, New Jersey: John Wiley and Sons; 2003:34.
19. Census (2011). Census of India website: Office of the Registrar General & Census Commissioner, India; 2023 [cited November 13, 2023]. Available from: https://censusindia.gov.in/census.website.
20. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2021 report [Internet]. Global Initiative for Chronic Obstructive Lung Disease; 2021. Available from: https://goldcopd.org/.
21. Mukhmohit S, Bhardwaj A, Saini S, Mukherjee AK. COPD–prevalence and risk study among females of rural area, district Ambala, Haryana. India. J Evol Med Dent Sci. 2014;3(16):4183–4192.
22. Sinha B, Singla R, Chowdhury R. An epidemiological profile of chronic obstructive pulmonary disease: a community-based study in Delhi. J Postgrad Med. 2017;63(1):29–35.10.4103/0022–3859.194200.
23. Brandsma CA, de Vries M, Costa R, Woldhuis RR, Königshoff M, Timens W. Lung ageing and COPD: is there a role for ageing in abnormal tissue repair? Eur Respir Rev. 2017;26(146):170073. PMID: 29212834; PMCID: PMC9488745. doi:10.1183/16000617.0073-2017
24. Koul PA, Hakim NA, Malik SA, et al. Prevalence of chronic airflow limitation in Kashmir, North India: results from the BOLD study. Int J Tuberc Lung Dis. 2016;20(10):1399–1404. doi:10.5588/ijtld.15.0968
25. Hayden LP, Hobbs BD, Cohen RT, et al. COPDGene Investigators. Childhood pneumonia increases risk for chronic obstructive pulmonary disease: the COPDGene study. Respir Res. 2015;16(1):115. PMID: 26392057; PMCID: PMC4578796. doi:10.1186/s12931-015-0273-8
26. Restrepo MI, Mortensen EM, Pugh JA, et al. COPD is associated with increased mortality in patients with community-acquired pneumonia. Eur Respir J. 2006;28(2):346–351. PMID: 16611653. doi:10.1183/09031936.06.00131905
27. Allwood BW, Myer L, Bateman ED. A systematic review of the association between pulmonary tuberculosis and the development of chronic airflow obstruction in adults. Respiration. 2013;86(1):76–85. PMID: 23652030. doi:10.1159/000350917
28. Gupte AN, Paradkar M, Selvaraju S, et al. Assessment of lung function in successfully treated tuberculosis reveals high burden of ventilatory defects and COPD. PLoS One. 2019;14(5):e0217289. PMID: 31120971; PMCID: PMC6532904. doi:10.1371/journal.pone.0217289
29. Salvi S, Agarwal A. India needs a national COPD prevention and control program. J Assoc Physicians India. 2012;60:5–7.
30. Patil S, Patil R, Bhise M, Jadhav A. Respiratory questionnaire-based analysis of awareness of COPD in a large multicenter rural population-based study in India. Chronic Dis Transl Med. 2022;8(4):322–330. PMID: 36420173; PMCID: PMC9676131. doi:10.1002/cdt3.47
31. Ding B, Small M, Bergström G, Holmgren U. COPD symptom burden: impact on health care resource utilization, and work and activity impairment. Int J Chron Obstruct Pulmon Dis. 2017;12:677–689. PMID: 28260874; PMCID: PMC5327905. doi:10.2147/COPD.S123896
32. Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. PMID: 10806163. doi:10.1164/ajrccm.161.5.9908022
33. Daniel J, Gupta R, Thangakunam B, Christopher DJ. Undiagnosed Asthma-COPD overlap among patients diagnosed as Asthma and COPD in a referral hospital, India. Heliyon. 2023;9(4):e14711. PMID: 37025820; PMCID: PMC10070599. doi:10.1016/j.heliyon.2023.e14711
34. Jarhyan P, Singh B, Rai SK, Nongkynrih B. Private rural health providers in Haryana, India: profile and practices. Rural Remote Health. 2012;12:1953.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.