Back to Journals » Risk Management and Healthcare Policy » Volume 16
Study on the Relationship Between the Number of Adverse Drug Reactions of Essential Drugs and Visits: Based on Vector Autoregressive Model
Authors Tang W ![]() , Chen H, Zhang Z, Wu G, Lin Y
, Chen H, Zhang Z, Wu G, Lin Y
Received 6 June 2023
Accepted for publication 5 December 2023
Published 14 December 2023 Volume 2023:16 Pages 2771—2778
DOI https://doi.org/10.2147/RMHP.S420407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Wan Tang,1,2 Hongdou Chen,1,2 Zixin Zhang,1,2 Gang Wu,1,2 Yanquan Lin1– 3
1Pharmacy, Suqian Hospital of Nanjing Drum-Tower Hospital Group, Suqian, People’s Republic of China; 2Pharmacy, Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, People’s Republic of China; 3Pharmacy, Xuzhou Medical University, Xuzhou, People’s Republic of China
Correspondence: Hongdou Chen, Email [email protected]
Objective: To analyse the relationship between the adverse drug reactions (ADRs) of essential drugs and visits, based on the recorded annual increase in ADRs associated with essential medicines in China, to provide a reliable theoretical basis for further analysis and optimization of the safety of essential drugs.
Methods: The data of adverse reactions of essential drugs in China from 2011 to 2020, time series analysis was conducted, and vector autoregressive (VAR) model was established. The relationship between the number of ADRs and visits was explored empirically through Granger causality test, impulse response function and variance decomposition.
Results: There was a long-term cointegration relationship and one-way causality between the number of visits and ADRs caused by essential medicines. In the initial stage, the ADR response to the number of visits increased sharply, but with an increase in the number of lag periods, the impact remained basically stable, even showing a slight decreasing trend.
Conclusion: The number of visits impacts ADRs caused by essential medicines, but this impact remains basically stable after reaching a certain level.
Keywords: essential medicines, adverse drug reactions, vector autoregressive model, time-series analysis
Background
The concept of essential medicines was proposed by the World Health Organization (WHO) in 1977.1 It refers to medicines needed to satisfy basic medical and health demand in suitable dosage form, at reasonable prices, and with guaranteed supply and fair access to the public.1,2 Since the implementation of a new medical reform in 2009,3 China has gradually established a national essential medicine system, which has played an important role in establishing and implementing the improvement of drug supply security systems, regulating the bulk of basic drugs, and reducing medical expense burdens. Currently, the study of basic drugs is concentrated on their affordability, accessibility and rationality.4,5 For example, the significant measures to implement the essential medicine system have impacted the affordability of primary medical institutions, patients and the government;6,7 accessibility issues in medical institutions and social pharmacies;8–11 and discussions of the rationality of basic drug prescriptions.12 However, from 2009 to 2020, the number of reported cases of ADRs associated with basic drugs collected by the National Center for the ADR Monitoring System increased year by year.13 In 2020, total ADRs reached 830 thousand, including 88 thousand serious reports, accounting for 10.6%.14 The reasons for this phenomenon merit further study and discussion. This study analysed the trend of ADRs caused by essential medicines in the past 10 years through a time-series analysis. To provide strong support to further guarantee the safety of basic drugs, we empirically analysed the related influencing factors of ADRs associated with basic drugs by using the VAR model, such as the number of visits.
Methods
Data Collection and Processing
Data were collected from the National Economic and Social Development Statistical Bulletin and the National Annual Report on Adverse Drug Reactions by the government agency.13,15 The indicators can be selected and included directly in this study, owing to the use of analyzed data in which participants were not identifiable. The variables analysed were the number of ADRs associated with basic drugs from 2011 to 2020, referred to as ADR_TOTAL, and the number of visitors, referred to as V. Simultaneously, data from 2014 to 2020 on ADRs caused by chemical drugs and biological preparations, denoted as ADR_CB, were extracted, as were data on ADRs caused by Chinese traditional patent medicine, written as ADR_TCM. Because the number of adverse reactions is in units of 10,000 cases and the number of visits in units of 100 million people, to facilitate the later modelling and statistical analysis, the number of ADRs and number of visits in 2011 were used as the bases, and the annual data were divided by the corresponding bases in 2011 to obtain the percentage value. The final obtained ADR sequence was recorded as EMADR_TOTAL and the number of visits as TV.
Index Selection
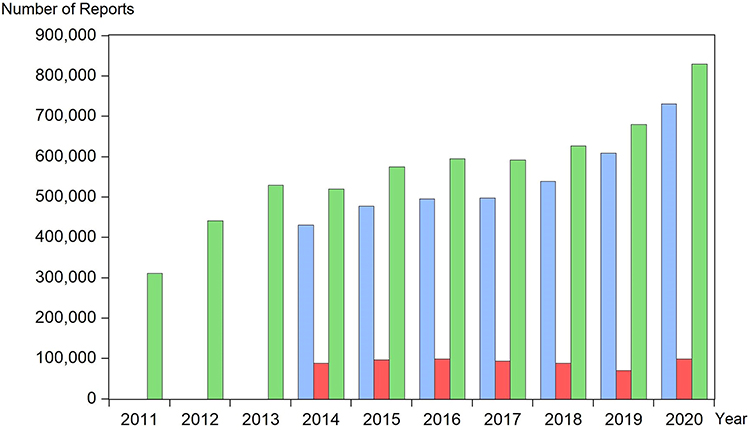
Theoretically, the number of ADRs is closely related to the number of varieties of basic drugs, ADRs reporting skills and structures, the usage of basic drugs and other factors, while the usage of basic drugs is influenced by factors such as the number of visits and relevant policies. Considering, the factors such as the monitoring system of ADRs and the policies for promoting the use of essential drugs are difficult to quantify for analysis. Meanwhile, we have the time-series analysis descriptive statistics for the ADRs associated with basic drugs was depicted with EViews 10 software (QMS, Irvine, CA, USA). An influence of the number of included varieties of basic drugs on ADRs can be ruled out because the descriptive analysis in the figure showed that while the number of ADRs associated with basic drugs increased year by year, the number of ADRs associated with Chinese traditional patent medicine tended to be stable (Figure 1). Therefore, this study attempts to explore the relationship between the ADRs associated with basic drugs and the number of visits based on time series analysis.

Statistical Analysis
A time-series analysis with vector autoregression (VAR) model was performed with EViews 10 software to examine the dynamic interaction between ADR and visits.16 First, the augmented Dickey–Fuller (ADF) stationarity test was employed to identify whether a unit root existed in the EMADR_TOTAL and TV series and determine the stationarity of the two series. The analysed time-series variables are all nonstationary series, and cointegration analysis can be performed on the original series variables. When the analysed variables for a time series are all nonstationary series (ADF, P>0.05), cointegration analysis can be performed on the original series variables. If there is a cointegration relationship between the two series (none and at most 1, P<0.05), then the VAR model can be further constructed, and the causal relationship between basic drug ADRs and the number of visits can be explored by means of Granger causality, impulse response analysis and variance decomposition. The optimal lag order of the VAR model is determined with the minimization principles of the Akaike information criterion (AIC) and Schwarz criterion (SIC). Next, the stationarity of the VAR model was tested. Only if a VAR model is stable can Granger analysis, impulse response analysis, and variance decomposition be carried out because these methods all require the VAR model to be a stationary system. A P value of <0.05 was considered to reject the null hypothesis.
Patient and Public Involvement
No patient involved
Results
Based on the data processed above, we performed statistical analysis on the two variables MEADR_TOTAL and TV. The processed data of the two groups showed a normal distribution (Jarque–Bera, P=0.989 and P=0.763, respectively); that is, the processing was reasonable and effective.
The ADF test revealed that the null hypothesis that there was a unit root could not be rejected for either the EMADR_TOTAL or the TV sequence (P=0.856 and P=0.319, respectively). Both sequences were thus nonstationary sequences, and cointegration analysis was required for them. A cointegration test was performed to determine whether there was a long-term equilibrium relationship between the two. The analysis of the cointegration test showed that there was a correlation between the EMADR_TOTAL and TV sets of sequences (none, P=0.001 and at most 1, P=0.002).
Based on the principle of AIC and SC minimization, the optimal lag order of the VAR model was determined to be 1. Then, the stationarity test of the VAR sequence was carried out (Figure 2). All the unit roots were inside the unit circle, which means that the VAR sequence was stationary. Therefore, the assumptions required for the Granger causality test, impulse response analysis and variance decomposition test for the two groups of variables EMADR_TOTAL and TV were satisfied. Through the Granger causality test, it could be concluded that the null hypothesis that TV is not the Granger-cause of EMADR_TAOTAL was rejected (P=0.034), indicating that the number of visits Granger-causes the number of ADRs associated with basic drugs. The null hypothesis that EMADR_TAOTAL is not the Granger-cause of TV was not rejected (P=0.674), which indicates that the number of ADRs caused by basic drugs does not Granger-cause the number of visits. Therefore, there is only a one-way relationship between the number of ADRs caused by the basic drugs and the number of visits.
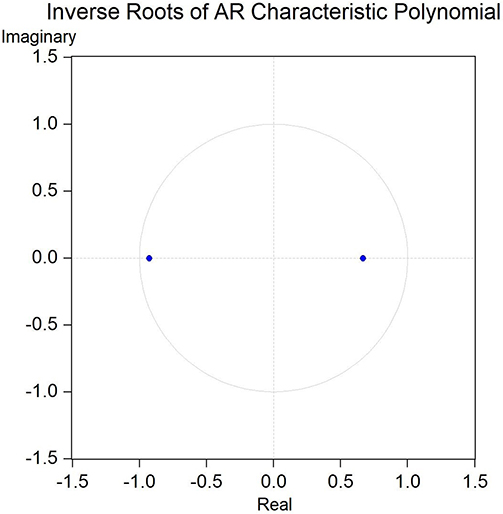 |
Figure 2 Stationarity test of VAR system. All the unit roots (blue dot) were inside the unit circle, which means that the VAR sequence was stationary. |
With the number of visits taken as the influencing factor and the number of ADRs caused by essential drugs taken as the response factor, the impulse responses of EMADR_TOTAL to a 1-standard-deviation shock to itself and to TV were analysed (Figures 3 and 4, respectively). The response of EMADR_TOTAL to a one-standard-deviation shock to TV showed a positive response in the initial stage, reached the maximum value in the second period, and then repeatedly fluctuated. After the fourth period, it fluctuated around the value of 0, and finally, the effect tended to disappear. At the same time, the response of EMADR_TOTAL to a one-standard-deviation shock to itself was negative in the initial stage and then fluctuated repeatedly, and the fluctuation range gradually flattened. The response direction of EMADR_TOTAL to a self-perturbation was opposite to that of a TV perturbation, and the response to the self-perturbation was larger. This showed that in the long run, the impact of the number of visits and basic drugs on the number of ADRs caused by the basic drugs becomes increasingly stable and that the basic drugs themselves have a greater impact on the number of ADRs.
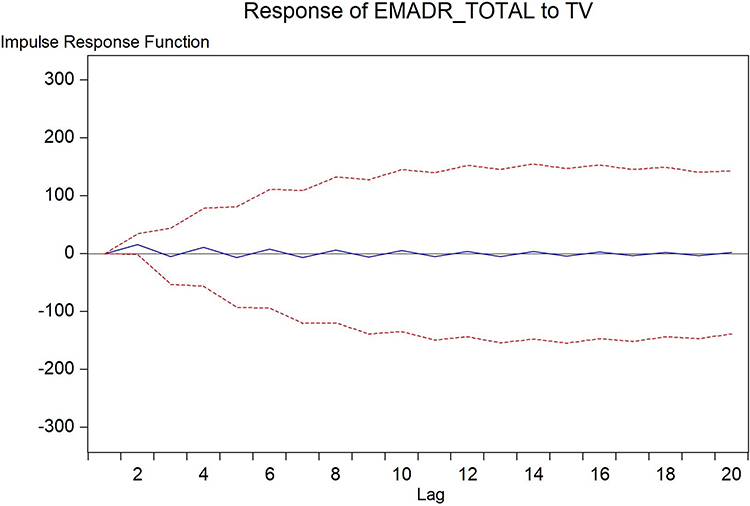 |
Figure 3 Response of EMADR_TOTAL to TV perturbation. Blue line is trace of impulse response values, between the red dotted lines are the response standard errors. |
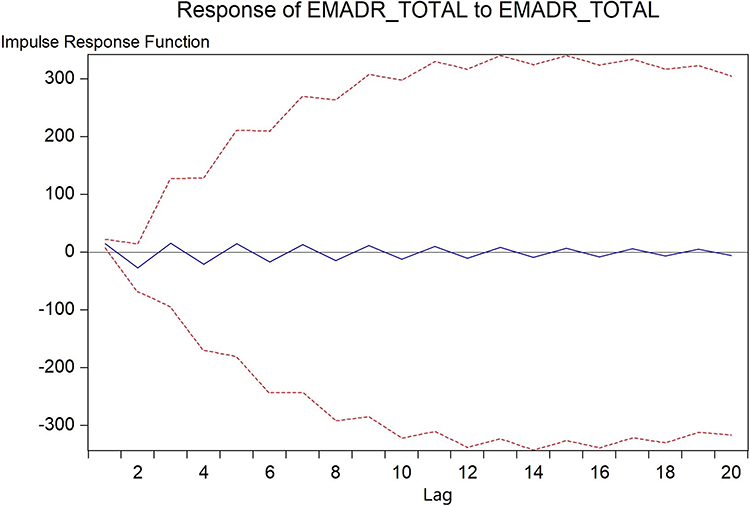 |
Figure 4 Response of EMADR_TOTAL to self-disturbance. Blue line is trace of impulse response values, between the red dotted lines are the response standard errors. |
The variance decomposition provided the relative degree of influence of each disturbance factor on each variable in the VAR model. The part of the variance in the EMADR_TOTAL variable explained by a self-change showed a sharp downwards trend in the early stage, slight fluctuations in the third and fourth periods, and then a slight increasing trend, while the part explained by the TV change showed a sharp increase in the early stage and then a slight downwards trend (Figure 5). Approximately 80% of the variance in the EMADR_TOTAL variable was explained by the self-disturbance, and the remaining 20% was explained by the TV perturbation. This means that in the initial stage, the number of visits had a greater impact on ADRs caused by basic drugs but that in the long run, this impact was basically stable and relatively small.
 |
Figure 5 |

Discussion
ADRs refer to harmful reactions unrelated to the purpose of the drug when normal doses of qualified drugs are used for the prevention, diagnosis and treatment of diseases.17 At present, reports relevant to the ADRs associated with essential medicines focus on the analysis of the drugs’ safe use, rational clinical application, and interactions to reduce the occurrence of ADRs.18,19 Simple statistics are available on ADR-susceptible populations, affected systems, Chinese traditional patent medicine injections, antibacterial drugs, etc.20–22 There are also related discussions on ADR monitoring models and monitoring signals for basic drugs by Liu Cuili et al23 and research on related genes and proteins for predicting ADRs by Kuhn, M et al24,25 Currently, there are no macro time-series analyses on the long-term trend of the basic drug ADR series and related influencing factors. This study makes up for the lack of comprehensive safety evaluation from a macro perspective, and can provide references for similar studies in the future.
The VAR model is to construct the model by taking each endogenous variable in the system as a function of the lag value of all endogenous variables in the system, so as to extend the univariate autoregressive model to the “vector” autoregressive model composed of multiple time series variables.26–29 The model does not care whether the regression coefficient of the equation is significant or not, but focuses on the stability level of the whole model. Only on the basis of the stability of the VAR system can impulse response and variance decomposition be used to study the dynamic impact of random disturbance on the variable system.30,31 In this study, ADF balance test and cointegration analysis were used to determine that there is a long-term equilibrium relationship between the two groups of variables “EMADR_TOTAL” and “TV”, so the VAR model can be established and run. The stationarity test of the overall model found that all the unit roots were in the circle, that is, the VAR model was stable and could carry out subsequent analysis, and the subsequent analysis results were reasonable.
The VAR model was constructed with the time-series data of the number of medical visits and the number of ADRs caused by basic drugs in China from 2011 to 2020. Through the methods of Granger causality tests and impulse response and variance decomposition analyses, we discussed the dynamic relationship between the number of visits and the number of ADRs caused by basic drugs, improve the safety analysis of basic drugs from a macro perspective. From each test, it could be concluded, first, that there was a long-term stable relationship and one-way Granger causality between the two series, which showed that the number of visits had a certain influence on the number of ADRs. Then, through the impulse response and variance decomposition analyses, it was found that the impact of the number of visits showed a sharp increase only in the initial stage and that upon reaching a threshold of approximately 20%, the impact basically remained stable and even showed a slight declining trend. Thus, the impact of visits on the number of ADRs caused by basic drugs may decrease in the long run.
There are many factors that affect the number of ADRs, such as the list of essential medicines, usage, the monitoring system of ADRs, and number of patients, and other factors.32,33 This study analyses of the total number of ADRs associated with basic drugs in China from 2011 to 2020 and the ADRs caused by Chinese traditional patent medicines, chemical drugs and biological preparations of basic drugs found that the number of ADRs caused by Chinese traditional patent medicines tended to be stable and that the dynamic trend in the number of ADRs caused by chemical drugs and biological preparations was basically the same as that for the overall ADR number. In the past 10 years, China has successively updated the 2012 version (with 520 drugs) and the 2018 version (with 685 drugs) of its essential drug list.34 So that, our tests allowed us to rule out an influence of the number of catalogue varieties.
The usage of basic drugs is affected by factors such as diagnosis and treatment plan, disease degree, and the number of visits. Currently, most factors, such as diagnoses and treatment plans, reporting skills of ADRs, disease severity, are difficult to collect or quantify except for the number of visits. Which makes them impossible be directly applied to statistical analysis. Therefore, this paper studied mainly the time series relationship between the ADRs associated with basic drugs and the number of visits. However, there are only nearly 10 years of relevant data for basic drugs, which imposes certain limitations on the VAR analysis of dynamic changes. The main influencing factor of ADRs caused by basic drugs may be itself. which is not discussed in this paper because it needs to be explored in many directions and further excavation.
For discussions of the influencing factors of the time-series increase in ADRs caused by basic drugs, the relevant data in this paper can provide reference for the safety evaluation of the national essential drug system, and further improve the safety guarantee of basic drugs. At the same time, it also provides a reference for the safety and effect evaluation of the implementation of essential drugs policy and provides a scientific basis for the management of essential drugs in the country. Following, we will further exploration and analysis will be conducted from multiple perspectives, such as the optimization of the quality of basic drug preparations, improvement to basic drug safety evaluation models, pharmacovigilance, and improvement and strengthening of the ADR monitoring system.
Conclusion
In summary, through the analysis of the current, limited ADR data for basic drugs, it is found that the number of visits has a certain impact on ADRs but that after this impact reaches a certain level, it basically remains stable Indeed, in the long run, it may become increasingly small. We also found that the basic drugs themselves had a greater impact than the number of visits on ADRs. It is suggested that it is worth focusing more on basic drugs themselves in the future—for example, through comprehensive evaluations of their quality—to further explore the reasons for the increase in ADRs associated with basic drugs year by year and improve the overall safety of basic drugs. In view of the limitations of our current research data, we welcome all research and regulatory teams to provide advice and support in identifying influencing factors and collecting data to study various aspects of essential medicine ADRs.
Abbreviations
WHO, World Health Organization; NCADRM, National Center for ADR Monitoring, China; ADR, adverse drug reaction.
Data Sharing Statement
The datasets used and/or analysed in the current study were collected from the National Health and Family Planning Development Statistical Bulletin and the National Annual Report on Adverse Drug Reaction Monitoring. These data are also available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was certified as exempt from the ethical review by the Research Ethics Committee of Suqian Hospital of Nanjing Drum-Tower Hospital Group. This is because the study was based on open source data, users can download relevant data for free for research and publish relevant articles, so there are no ethical issues and other conflicts of interest.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by The Fifth Phase 333 High-Level Talents Training Research Funding Project of Jiangsu Province (BRA2020234) and Jiangsu Pharmaceutical Association–Chia Tai Tianqing (Lianyungang) Hospital Pharmaceutical Research Project (Q202043).
Disclosure
The authors declare that they have no competing interests.
References
1. The central people`s government of the people`s republic of China. What does essential drugs mean?[EB/OL]. Available from: https://www.gov.cn/ztzl/ygzt/content_1661317.htm.
2. Zhao Y. Research on the national essential drugs list of China in 2018[D]. Zhengzhou University. 2019.
3. National medical products administration. Implementation Opinions on Establishing a national Essential drugs system[EB/OL]. Available from: https://www.nmpa.gov.cn/directory/web/nmpa/zhuanti/lshzht/shhwshgg/20090818151301303.html.
4. Rossdegnan D, Ball D, Ewen M, et al. Medicine Prices, Availability, and Affordability in 36 Developing and Middle-Income Countries: a Secondary Analysis. Lancet. 2009;373(9659):240–249.
5. Sheikh K, Gilson L, Agyepong IA, et al. Building the Field of Health Policy and Systems Research: framing the Questions. PLoS Med. 2011;8(8):e1001073. doi:10.1371/journal.pmed.1001073
6. Ye L, Hu SL, Ewen M, et al. Evidence-base study on the affordability of essential drugs in Shanghai. Chine Health Resources. 2008;11(4):195–196.
7. Zhang Y, Li X. Investigation and analysis of availability and affordability of essential medicine in Nanjing based on WHO/ HAI standard survey method. China Pharm. 2015;26(30):4188–4191.
8. Gong SW, Xu Y, Zhang L. Study on evaluation indicator system of drug accessibility. Chin Health Economics. 2011;30(5):72–74.
9. Guan XD, Shi LW. Study on evaluation method for the accessibility of essential medicine in China based on WHO/HAI standardized approach. China Pharm. 2013;24(24):2212–2215.
10. Wu YX, Xu W, Cai GJ, et al. Study on the factors affecting the availability of essential drugs——An empirical analysis based on data from 25 provinces. Health Economics Research. 2018;4(12):37–39.
11. Yao Q, Luo F, He LY, et al. Effectiveness evaluation of national essential medicine system in China from the perspective of drug access. Chinese Hospital Management. 2014;34(3):60–62.
12. Shang JX, Lin QM, Li L, et al. Analysis of rational use of essential medicine in Beijing. Chine Pharm Affairs. 2015;29(10):1006–1012.
13. National center for ADR monitor. China, Center for drug reevaluation. NIMPA. Drugs-Safety Alert-Data release. Available from: https://www.cdr-adr.org.cn/drug_1/aqjs_1/drug_aqjs_sjbg/.
14. National Medical Products Administration. National adverse drug reaction monitoring annual report(2020) [EB/OL]. Available from: https://www.nmpa.gov.cn/xxgk/fgwj/gzwj/gzwjyp/20210325170127199.html.
15. National Bureau of Statistics. National Economic and Social Development Statistical Bulletin[BE/OL]. Available from: http://www.stats.gov.cn/tjsj/tjgb/ndtjgb/.
16. Ma HH. EViews Statistical Analysis and Application (Third Edition). Beijing: Publishing house of electronics industry; 2016:159–176.
17. Fossouo Tagne J. Measures for the management of adverse drug reaction reporting and monitoring. China Pharm. 2011;5:68–75.
18. Jiang C, Shen J, Shou D, et al. Identification of high-risk patients for ADR induced by traditional Chinese medicine injection: a nested case-control study. Sci Rep. 2019;9(1):16721. doi:10.1038/s41598-019-53267-2
19. Sugioka M, Tachi T, Mizui T, et al. Effects of the number of drugs used on the prevalence of adverse drug reactions in children. Sci Rep. 2020;10(1):21341. doi:10.1038/s41598-020-78358-3
20. Huang P, Wang J. Analysis of 30399 cases of national essential medicine adverse reaction reports. Anhui Med Pharmaceutial J. 2012;16(11):1708–1710.
21. Chang HH, Chiang SY, Chen PC, et al. A system for reporting and evaluating adverse drug reactions of herbal medicine in Taiwan from 1998 to 2016. Sci Rep. 2021;11(1):21476. doi:10.1038/s41598-021-00704-w
22. Yan Z, Feng Z, Jiao Z, et al. The severity of adverse drug reactions and their influencing factors based on the ADR monitoring center of Henan Province. Sci Rep. 2021;11(1):20402. doi:10.1038/s41598-021-99908-3
23. Liu CL, Xia DS. Discussion on the monitoring of the adverse reaction and the risk management of essential medicines. Chine J Pharmacovigilance. 2014;11(10):614–617.
24. Kuhn M, Al. Banchaabouchi M, Campillos M, et al. Systematic identification of proteins that elicit drug side effects. Mol Sys Biol. 2013;9(1):663. doi:10.1038/msb.2013.10
25. Yan S, Xiong H, Shao F, et al. HLA-C*12:02 is strongly associated with Xuesaitong-induced cutaneous adverse drug reactions. Pharmacogenomics J. 2019;19(3):277–285. doi:10.1038/s41397-018-0051-3
26. Gao TM, Chen F, Kong XL, et al. Econometric Analysis Methods and Modeling: Eviews Applications and Examples. Beijing: Tsinghua University Press; 2020.
27. Yu D, Li Y, Tian GC. Empirical analysis of RMB exchange rate based on vector autoregressive model. Modern Business Trade Industry. 2011;23(03):161.
28. Allen PG, Morzueh BJ. Twenty-five years of progress, problems, and conflicting evidence in econometric forecasting. What about the next 25 years? Int J Forecasting. 2006;22(3):475–492. doi:10.1016/j.ijforecast.2006.03.003
29. Han JP, Shao ZX, Wu HZ. Analysis on the Economic Efficiency and Its Influencing Factors of General Hospitals in China Based on VAR Model. Chin Health Economics. 2020;39(1):80–82.
30. Cheng Y. A study on factors affect China`s price fluctuation in open economy[D]. Xiamen University. 2009:31.
31. Zhu HM, Liu ZW. Bayesian inference theory of time-series vector autoregressive models. Statistics Decision. 2004;1:11–12.
32. Su GH, Jiang H. Factors affecting adverse drug reactions. Heilongjiang Sci Tech Information. 2009;7:176.
33. Jia YL. Briefly discuss the influencing factors and countermeasures of adverse drug reactions. J Front Med. 2016;6(1):384–385.
34. Zhang SS, Wu T, Zhang R, et al. Interpretation of the 2018 edition of the national essential drugs list. Health Economics. 2019;36(6):47–50.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.