Back to Journals » Journal of Inflammation Research » Volume 18
Study on the Impact of Perioperative Application of Mindfulness - Based Motivational Care Combinations on Post - Operative Recovery and Negative Emotions of Endometriosis Patients
Received 22 April 2025
Accepted for publication 8 October 2025
Published 15 October 2025 Volume 2025:18 Pages 14343—14352
DOI https://doi.org/10.2147/JIR.S535948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Yao You, Yan Luo, Pengli Li
Department of Traditional Chinese Medicine Gynecology, Qinhuangdao Maternal and Child Health Hospital, Qinhuangdao, Hebei, People’s Republic of China
Correspondence: Pengli Li, Email [email protected]
Background: Endometriosis is a chronic gynecological condition characterized by the presence of endometrial tissue outside the uterine cavity, often leading to pain, infertility, and psychological distress. Effective perioperative care is crucial for promoting recovery and improving emotional well-being.
Objective: To explore the impact of the combined application of mindfulness-based motivational care during the perioperative period on postoperative recovery and negative emotions in patients with endometriosis.
Methods: A total of 103 patients were divided into a control group receiving conventional nursing (n=51) and an observation group receiving mindfulness-based motivational care in addition to conventional nursing (n=52). Postoperative recovery indicators, sleep quality (PSQI), pain (NRS), comfort (GCQ), negative emotions (SAS, SDS), ability of daily living (ADL), and quality of life (SF-36) were evaluated.
Results: Compared with the control group, the observation group showed significantly shorter times to first ambulation, first flatus, and hospitalization (P< 0.05). Improvements in PSQI, NRS, and GCQ scores were observed in both groups, but were more significant in the observation group (P< 0.05). Similarly, SAS and SDS scores decreased in both groups, with greater reductions in the observation group (P< 0.05), indicating superior efficacy in relieving anxiety and depression.
Conclusion: Compared with conventional nursing, the combined application of mindfulness-based motivational care during the perioperative period can more effectively promote postoperative recovery in patients with endometriosis, improve sleep quality and pain management, reduce negative emotions, enhance comfort, and improve quality of life.
Keywords: endometriosis, mindfulness-based motivational care, perioperative nursing, postoperative recovery, negative emotions
Introduction
Endometriosis is a common chronic gynecological disorder, typically occurring in women of reproductive age. It is characterized by the presence of endometrial tissue (including glands and stroma) outside the uterine cavity. Endometriosis primarily affects the pelvic organs, including the fallopian tubes, ovaries, bowel, and bladder, but rarely can affect more distant areas such as the abdominal wall, diaphragm, and pleura.1 The primary symptoms include chronic pelvic pain, dysmenorrhea, infertility, and menstrual irregularities, which not only severely affect patients’ physical health but also negatively influence their psychological well-being and overall quality of life.2,3 Surgical removal of ectopic endometrial tissue is often necessary for treatment, making perioperative care a crucial component for promoting postoperative recovery, pain management, emotional regulation, and quality of life improvement.4 However, conventional nursing interventions have certain limitations, such as insufficient management of patients’ negative emotions and pain.5 Therefore, there is an urgent need to explore more comprehensive and individualized nursing approaches to enhance postoperative outcomes.
In recent years, mindfulness therapy has attracted increasing attention in the fields of medicine and nursing due to its significant efficacy in alleviating anxiety, depression, and other negative emotional states.6–8 By focusing on present-moment awareness and cultivating acceptance of internal experiences, mindfulness therapy helps patients regulate emotions, reduce psychological stress, and improve tolerance to physical discomfort.9 Moreover, the motivational component of mindfulness care can strengthen patients’ positive emotions, increase treatment compliance, and ultimately promote recovery.10 Based on these considerations, the present study applies a mindfulness-based motivational care intervention model to the perioperative nursing of endometriosis patients, aiming to provide comprehensive support for postoperative recovery, pain control, and emotional well-being.
Subjects and Methods
Study Subjects
A retrospective analysis was conducted on the clinical data of 103 patients with endometriosis who underwent surgical treatment at our hospital from April 2022 to July 2024. The inclusion criteria were: ① Patients were clinically diagnosed with endometriosis through relevant tests11 and underwent elective surgery at our hospital; ② Patients were aged ≥18 years and <40 years; ③ Patients had good mental status at admission, with normal cognitive and communication abilities, and were willing to cooperate with the procedures required for this study; ④ Patients had not taken hormone medications in the past six months; ⑤ Patients had complete clinical data; ⑥ Patients underwent laparoscopic surgery for endometriotic lesions, with detailed records of lesion location (eg, ovaries, fallopian tubes, pelvic peritoneum, bowel, bladder, etc). The exclusion criteria were: ① Patients with other uterine diseases; ② Patients with severe abnormalities in organ function; ③ Patients with immune system diseases, hematological diseases, and/or severe infections; ④ Patients with malignant tumors; ⑤ Patients with cognitive impairment and/or psychiatric disorders; ⑥ Patients who had allergic reactions or contraindications to the treatment or intervention methods used in this study; ⑦ Patients who were unable to fully cooperate with the study for various reasons and/or had incomplete clinical data; ⑧ Patients with unclear or undocumented lesion location were excluded. Patients were retrospectively assigned into the control group (n=51) or the observation group (n=52) according to the actual nursing interventions they had received during hospitalization. Since this was a retrospective analysis, no random allocation was performed. To reduce potential bias, baseline characteristics were compared between groups and found to be comparable. It should be noted that patients in the observation group received additional mindfulness-based training and motivational guidance, which required active participation. This may have led to self-selection bias, which was minimized by including all eligible cases during the study period.This study was approved by the Qinhuangdao Maternal and Child Health Hospital Medical Ethics Committee (Approval No.: 24FKHL09) and conducted in strict accordance with the ethical principles of the Declaration of Helsinki. All participants provided informed consent and signed relevant informed consent forms.
Methods
Surgical Methods
All patients underwent laparoscopic surgery after admission. The surgery was scheduled 3 to 7 days after the patient’s menstrual period ended, using tracheal intubation and general anesthesia. The specific surgical steps were as follows: First, a transverse incision was made above or below the umbilicus to ensure sufficient operating space. Through this incision, a pneumoperitoneum was established using carbon dioxide to create adequate surgical space in the abdominal cavity. Subsequently, a trocar was placed into the abdominal cavity to facilitate the laparoscopic operation. During the surgery, the surgeon conducted a comprehensive exploration of the patient’s pelvic and abdominal cavities to fully understand the distribution of lesions and any other possible pathological changes. For pelvic adhesions, blunt dissection and bipolar electrocoagulation techniques were used to separate them. The ectopic lesions were then treated with electrocautery to ensure thorough removal of the diseased tissue. To further evaluate the patency of the fallopian tubes, methylene blue solution (produced by Jiangsu Jichuan Pharmaceutical Group Co., Ltd., drug approval number: Guoyao Zhunzi H32024827) was injected into the uterus during the surgery, and its flow in the fallopian tubes was monitored laparoscopically to determine the patency of the tubes. After confirming the patency of the fallopian tubes, electrocoagulation was performed to prevent postoperative bleeding. To prevent postoperative adhesions, the pelvis was thoroughly irrigated during the surgery, and all surgical areas were carefully cleaned. Finally, the incision was sutured with fine threads, and the entire surgical procedure strictly adhered to aseptic principles. After the surgery, the patient was transferred to the recovery room for routine postoperative monitoring. The nursing care for both groups of patients commenced upon admission before surgery and continued throughout their hospital stay and for 5 weeks after discharge.
Control Group
The control group received routine nursing interventions, including health education, monitoring of vital signs, surgical assistance, medication adherence, daily care, and follow-up observation.
Observation Group
The observation group received the same routine nursing interventions as the control group, but with the addition of mindfulness-based motivational nursing interventions. The specific measures were as follows: (1) Training Part:12 ① Sitting Meditation: Sitting meditation is the core and most basic practice of mindfulness training, covering four aspects: mindful sound, mindful thoughts, mindful breathing, and mindful body. During the training, patients focused on their breathing, felt the rise and fall of their abdomen with each breath, observed the emergence, transition, and dissipation of thoughts in their mind, and were encouraged to practice self-awareness while paying attention to the sensation of pain in various parts of their body. ② Walking Meditation: Walking meditation is a form of mindfulness training conducted while walking. Patients were required to focus their attention on the movement of their feet, carefully feeling the process of lifting, moving, and placing their feet, and the sensation of their soles contacting the ground. During the entire training process, patients maintained a natural breathing rhythm, enhancing awareness of the present moment. ③ Mindful Yoga: During mindful yoga training, patients were guided to focus on their physical and mental experiences while performing yoga movements, feeling the motion and stretching of their bodies. This process helped patients deepen their body awareness and improve their self-awareness. ④ Body Scan: Body scan training required patients to lie down or sit with their eyes closed and sequentially become aware of the sensations in each part of their body from head to toe. This process helped patients shift their attention from complex thoughts to a detailed perception of their body, enhancing their awareness of each part of the body. ⑤ Three-Minute Breathing Space: In this exercise, patients sat with their eyes closed and focused on their current sensations, paying attention to the rise and fall of their abdomen and keeping their awareness on any abnormal sensations in their body. The training content was adjusted according to the patient’s recovery status. The initial training was conducted under the guidance and supervision of nursing staff, and once the patients were familiar with it, they could perform it on their own, at least once a day, for at least 2 hours each time. (2) Mindfulness-Based Motivational Guidance:13 ① Psychological Communication: Nursing staff proactively communicated with the patients daily, providing simple psychological counseling to help them relax, reduce anxiety, and alleviate tension. Through effective communication, nursing staff were able to understand the patients’ psychological states and provide corresponding emotional support. ② Physical Contact and Encouragement: During mindfulness training, nursing staff could appropriately approach the patients and provide warm touches to enhance their sense of security. Simultaneously, nursing staff should give positive feedback and encouragement to the patients through words to help boost their confidence. ③ Nutritional and Entertainment Support: The postoperative recovery of patients is closely related to adequate rest and good nutritional intake. Nursing staff should play relaxing music or movies according to the patients’ personal preferences to enrich their leisure experience. Additionally, personalized nutritional guidance should be provided to help the patients better meet the needs of their physical recovery.
Observation Indicators
All questionnaires were part of the routine clinical evaluation forms or were retrospectively obtained from the patients’ medical records and follow-up records, rather than being newly administered during the study period.
Postoperative Recovery Indicators
These included the time of the first ambulation after surgery, the time of the first bowel movement after surgery, and the length of hospital stay. The information on these indicators was uniformly recorded by the relevant medical staff at our hospital.
Sleep Quality
Before and after the intervention, the Pittsburgh Sleep Quality Index (PSQI)14 was used to assess the sleep quality of patients before and after the intervention. The PSQI score ranges from 0 to 21 points, with lower scores indicating better sleep quality.
Pain
Before and after the intervention, the Numeric Rating Scale (NRS)15 was used to assess the pain levels of patients before and after the intervention. The NRS score ranges from 0 to 10 points, with higher scores indicating more severe pain.
Comfort
Before and after the intervention, the Kolcaba General Comfort Questionnaire (GCQ)16 was used to assess the comfort levels of patients before and after the intervention. The GCQ score ranges from 0 to 100 points, with higher scores indicating greater comfort.
Negative Emotional Status17
Before and after the intervention, the Self-Rating Anxiety Scale (SAS) was used to assess the anxiety levels of patients before and after the intervention. The total score of the scale is 100 points, with a cutoff score of 50 points, and higher scores indicating more severe anxiety. The Self-Rating Depression Scale (SDS) was used to assess the depression levels of patients before and after the intervention. The total score of the scale is 100 points, with a cutoff score of 53 points, and higher scores indicating more severe depressive emotions.
Self-Care Ability
Before and after the intervention, the Activities of Daily Living (ADL)18 was used to assess the self-care ability of patients before and after the intervention. The total score of ADL is 100 points, with higher scores indicating better self-care ability.
Quality of Life Level
Before and after the intervention, the patients’ quality of life was assessed using the Short Form Health Survey (SF-36).19 The SF-36 includes 8 dimensions and has a total score of 100 points, with higher scores indicating a better quality of life.
Satisfaction Level
After the intervention, the hospital’s self-made “Satisfaction Evaluation Scale”20 was given to the patients and their families for assessment. The scale includes five dimensions: treatment effect, service attitude of medical staff, professional level of medical staff, comfort of the treatment environment, and hygiene safety. The scale is scored from 0 to 100 points, with scores >85 indicating very satisfied, scores between 60 and 85 indicating basically satisfied, and scores <60 indicating dissatisfaction. The total satisfaction rate was calculated as 100% - (number of dissatisfied cases/total number of cases × 100%).
Occurrence of Adverse Event
This includes surgical adverse events (infection, bleeding, thrombosis, etc)., anesthesia-related adverse events (nausea and vomiting, dizziness and headache, abnormal blood pressure, etc), postoperative complications (intestinal obstruction, sexual dysfunction, etc), and self-management adverse events (poor compliance, incorrect self-management cognition and/or behavior), all of which were uniformly recorded by the relevant medical staff in our hospital.
Statistical Analysis
GraphPad Prism 8 software was used for charting, and SPSS 22.0 software was used for data processing. Categorical data were expressed as percentages (%), and the χ²-test was used for analysis. Measurement data were expressed as ( ). Independent samples t-test was used for comparisons between groups, and paired t-test was used for comparisons within the same group. A P-value < 0.05 was considered statistically significant.
). Independent samples t-test was used for comparisons between groups, and paired t-test was used for comparisons within the same group. A P-value < 0.05 was considered statistically significant.
Results
Patient Demographics and Surgical Characteristics
A total of 103 patients with endometriosis were included in the study, with 51 in the control group and 52 in the observation group. The two groups were comparable in baseline demographic characteristics, including age, disease duration, reproductive status, and educational level, with no statistically significant differences (P>0.05). In addition, the types of surgery performed (such as laparoscopic ovarian cystectomy, laparoscopic endometriotic lesion resection, and laparoscopic adhesiolysis) were also comparable between the two groups, with no significant differences observed (P>0.05). Detailed demographic and surgical characteristics are shown in Table 1.
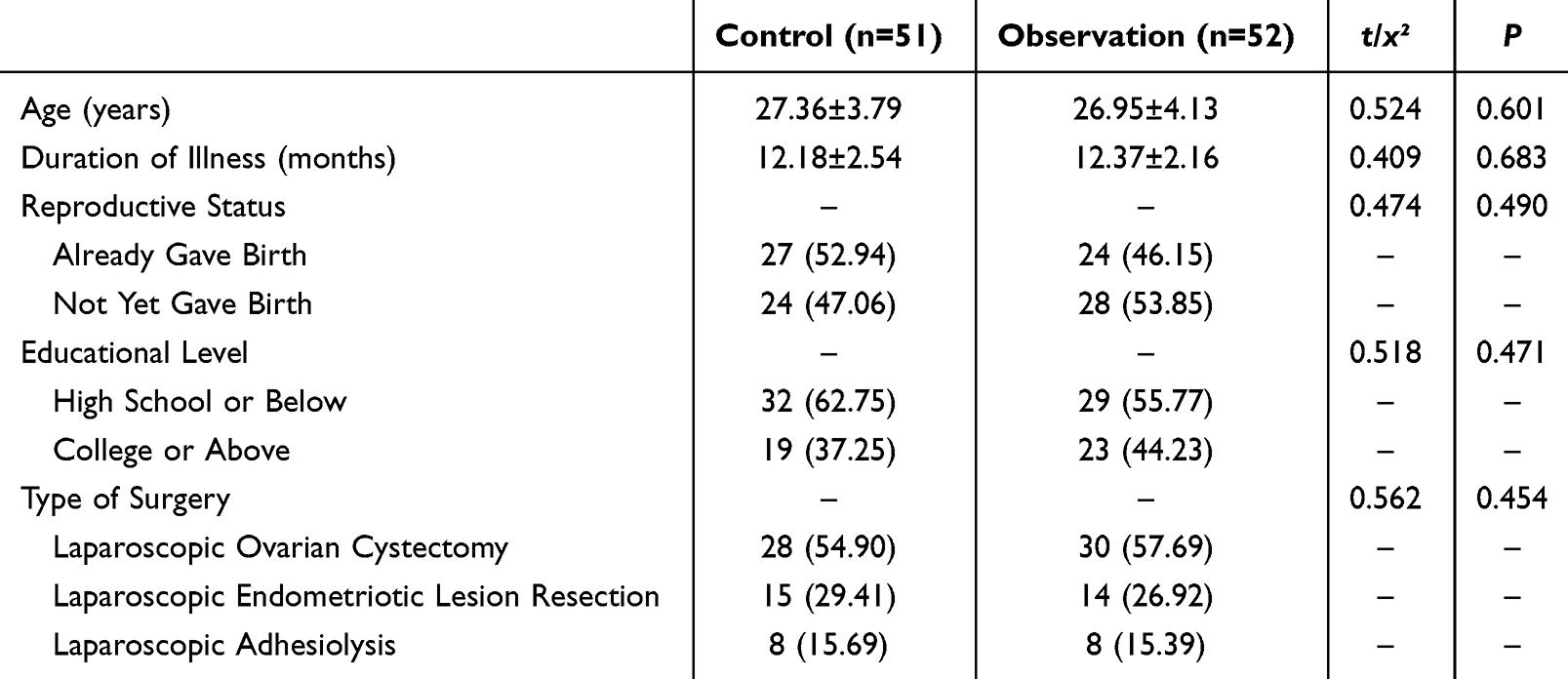 |
Table 1 Comparison of Patient Demographics and Surgical Characteristics [ |

Comparison of Postoperative Recovery
The time to first ambulation, time to first flatus, and length of hospital stay were all lower in the observation group compared to the control group (P<0.05), as shown in Table 2.
 |

Comparison of Sleep Quality, Pain, and Comfort
Compared with baseline (defined as preoperative assessment prior to nursing intervention), both groups exhibited decreased PSQI and NRS scores and increased GCQ scores after intervention. Improvements were significantly greater in the observation group (P<0.05), as shown in Figure 1.
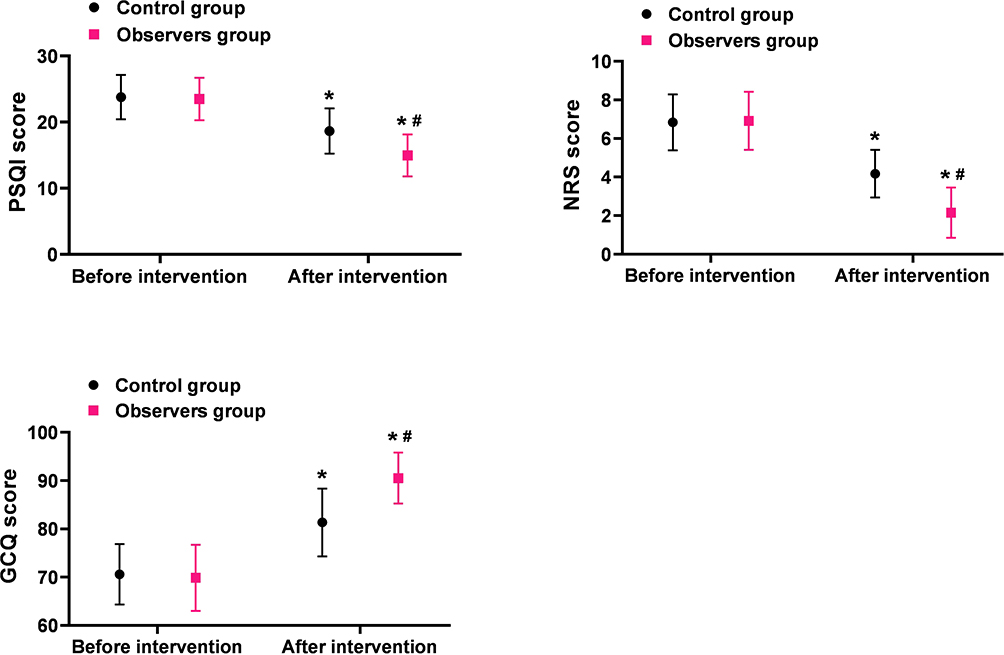 |
Figure 1 Comparison of Sleep Quality, Pain, and Comfort ( Note: Compared with before intervention, *P<0.05; Between groups comparison, #P<0.05. |

Comparison of Negative Emotional Status
After the intervention, both SAS scores and SDS scores decreased in both groups, with the observation group showing greater changes (P<0.05), as shown in Figure 2.
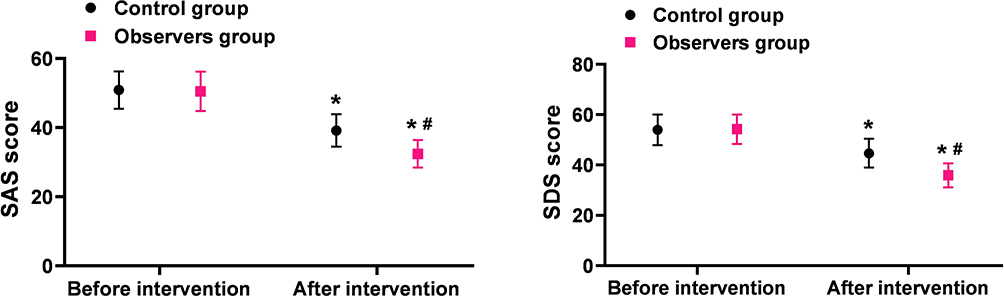 |
Figure 2 Comparison of Negative Emotional Status ( Note: Compared with before intervention, *P<0.05; Between groups comparison, #P<0.05. |

Comparison of Activities of Daily Living and Quality of Life
After the intervention, the ADL scores and SF-36 scores increased in both groups, with the observation group showing greater changes (P<0.05), as shown in Figure 3.
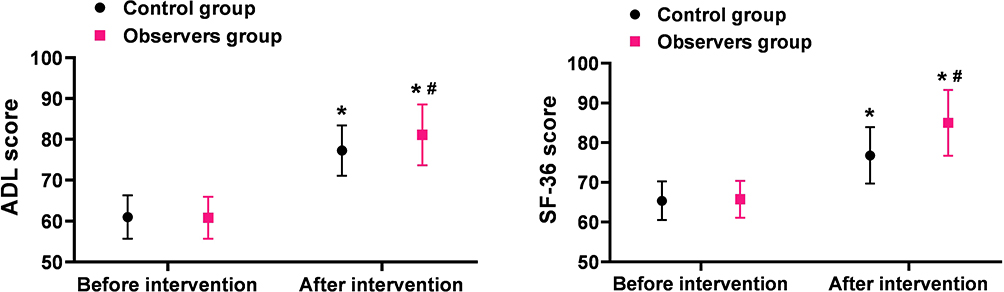 |
Figure 3 Comparison of Activities of Daily Living and Quality of Life ( Note: Compared with before intervention, *P<0.05; Between groups comparison, #P<0.05. |

Comparison of Satisfaction Levels
The overall satisfaction rate was higher in the observation group (94.23%) compared to the control group (80.39%) (P<0.05), as shown in Table 3.
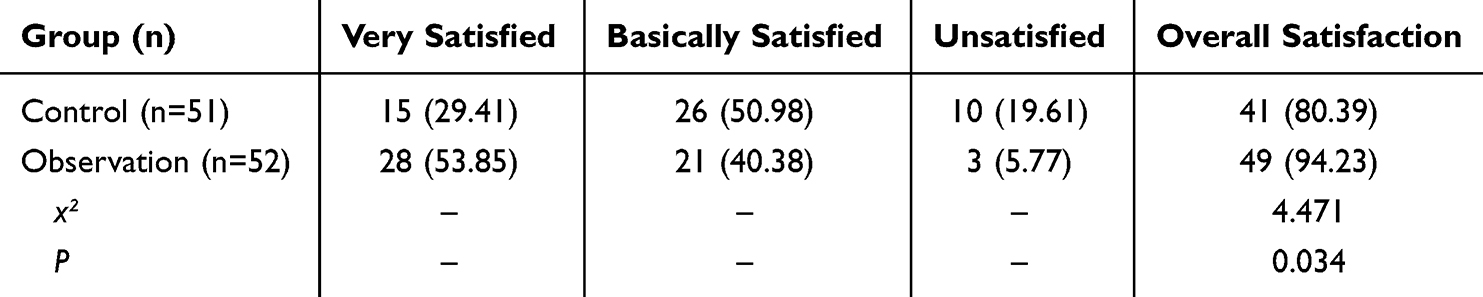 |
Table 3 Comparison of Satisfaction Levels [n (%)] |
Comparison of Adverse Event Incidence
The incidence rate of adverse events was lower in the observation group (7.69%) compared to the control group (21.57%) (P<0.05), as shown in Table 4.
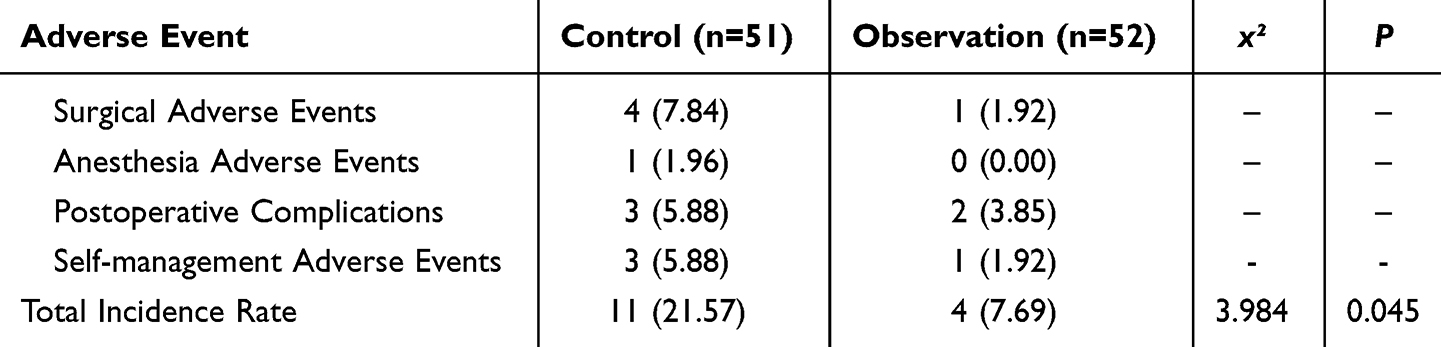 |
Table 4 Comparison of Adverse Event Incidence [n (%)] |
Discussion
Endometriosis is a common chronic inflammatory disease characterized by the presence of functional endometrial tissue outside the uterine cavity, such as in the ovaries, fallopian tubes, and peritoneum, resulting in a variety of complex clinical manifestations.21 From an etiological perspective, the pathogenesis of endometriosis remains incompletely understood, but multiple mechanisms may act synergistically, including retrograde menstruation, immune dysfunction, hormonal imbalance, genetic susceptibility, and abnormal inflammatory responses, which may promote the implantation and survival of ectopic endometrial tissue in pelvic sites and occasionally in extra-pelvic regions. Epidemiological studies indicate that the prevalence of endometriosis in women of reproductive age can reach 10–15%, with approximately 30–50% of patients experiencing infertility, making it a major cause of female infertility.22 Patients often present with recurrent chronic pelvic pain, menorrhagia, dyspareunia, and other symptoms, which severely affect their daily life and psychological well-being. In the present study, the included patients mainly underwent laparoscopic ovarian cystectomy, lesion excision, or adhesiolysis, which are standard surgical procedures for moderate to severe endometriosis, reflecting the clinical representativeness and relevance of the study sample. Although surgery is the primary treatment for moderate to severe cases—aimed at removing ectopic endometrial tissue, alleviating symptoms, and improving fertility23—it still carries risks of postoperative pain, recurrence, and complications, and surgery alone cannot completely cure the disease. Therefore, perioperative nursing interventions are crucial, as they not only provide preoperative support and postoperative guidance but also address patients’ psychological well-being, quality of life, and overall recovery. Traditional perioperative nursing models often focus primarily on physiological care, overlooking patients’ emotional and psychological needs, which may lead to suboptimal postoperative recovery, increased negative emotions, and reduced quality of life.
In recent years, mindfulness therapy has gained attention in the field of medical care, especially for its unique advantages in alleviating psychological stress and negative emotions in patients with chronic diseases.24 The core of mindfulness therapy is to cultivate patients’ focus and awareness of the present experience, helping them maintain a calm and accepting attitude when facing pain and anxiety, thereby enhancing psychological resilience.25 The application of mindfulness therapy extends beyond psychological treatment to overall health management, such as improving sleep quality, increasing pain tolerance, and reducing anxiety and depression.26 Compared to traditional nursing models, mindfulness-based motivational care interventions combine mindfulness therapy with motivational factors to create a more comprehensive and personalized care model. This intervention model not only focuses on physiological recovery but also aims to enhance patients’ psychological adaptation and positive emotions, promoting comprehensive rehabilitation. Therefore, applying mindfulness-based motivational care interventions in the perioperative care of endometriosis patients holds significant clinical potential and may offer a new path to improving postoperative recovery, reducing negative emotions, and enhancing quality of life. Regarding the timing of intervention, in our design, perioperative nursing began immediately upon hospital admission before surgery, continued throughout hospitalization, and extended to 5 weeks after discharge. Baseline assessments were conducted preoperatively, prior to the initiation of nursing intervention. This ensures transparency in study design and provides consistency when interpreting the improvements in postoperative recovery and psychosocial outcomes. The results of this study show that the observation group had significantly lower times for the first out-of-bed activity, first flatus, and hospital stay compared to the control group (P < 0.05). This indicates that the combined application of mindfulness-based motivational care interventions can effectively promote postoperative recovery in endometriosis patients. The reasons for this may be that mindfulness-based motivational care interventions actively guide patients to change negative behavior patterns, enhance self-management abilities, and further stimulate their recovery confidence and intrinsic motivation. Additionally, mindfulness training helps patients achieve deep physical relaxation by adjusting their physical and mental states and breathing rhythms postoperatively, thereby improving lung function, alleviating postoperative pain, and helping patients better adapt to the recovery process, ultimately enhancing recovery outcomes.
Research27 indicates that one reason for the ineffective improvement in psychological status and quality of life of endometriosis patients under conventional nursing models is that traditional care often neglects the psychological needs and emotional states of patients. Patients undergoing surgery and postoperative recovery often experience negative emotions such as anxiety and depression, which not only exacerbate their psychological burden but may also adversely affect the postoperative recovery process.28 The results of this study show that the PSQI scores, NRS scores, SAS scores, and SDS scores in the observation group after intervention were lower than those in the control group, while the GCQ scores, ADL scores, and SF-36 scores in the observation group were higher than those in the control group (P < 0.05). These results indicate that mindfulness-based motivational care interventions can effectively improve patients’ sleep quality and pain management, significantly reduce negative emotions, and further enhance their comfort and quality of life. The reason may be that mindfulness-based motivational care interventions encourage patients to actively participate in postoperative rehabilitation activities and provide positive feedback and continuous support, thereby enhancing patients’ confidence and enthusiasm for recovery. Additionally, mindfulness training helps patients by regulating breathing rhythms, alleviating anxiety and stress, and reducing tension, which contributes to improved physical and mental comfort. These measures help patients better adapt to postoperative recovery, reduce pain and sleep disturbances, and further enhance their daily living abilities and overall quality of life. In terms of adverse event rates and patient satisfaction, this study also yielded positive conclusions. Data show that the overall satisfaction in the observation group was as high as 94.23%, compared to 80.39% in the control group (P < 0.05); meanwhile, the adverse event rate in the observation group was only 7.69%, lower than the 21.57% in the control group (P < 0.05). This indicates that mindfulness-based motivational care interventions not only improve patient satisfaction but also effectively reduce the risk of related adverse events. The reason may be that mindfulness-based motivational care interventions comprehensively promote postoperative recovery, alleviate negative emotions, and improve quality of life, thereby enhancing the overall effectiveness of care and patient experience.
Despite these positive conclusions, the study has certain limitations. Firstly, this study is a retrospective analysis, which may involve selection bias and information bias, and the sample size is relatively small, including only 103 patients, which may affect the generalizability of the results. Secondly, due to the lack of long-term follow-up data, the impact of mindfulness-based motivational care interventions on patients’ long-term quality of life and recurrence rates could not be assessed. Finally, the study did not explore the differences in responses to mindfulness-based motivational care interventions among patients with varying degrees of endometriosis. Future research should consider stratified analysis to further optimize care plans. In conclusion, to further validate the reliability and clinical application value of this study’s results, it is recommended to conduct prospective studies with larger sample sizes, different clinical settings, and longer follow-up periods. Additionally, individualized mindfulness-based motivational care intervention models for different patient populations should also be a focus of future research to achieve more precise and effective care interventions.
Conclusion
This study demonstrates that mindfulness-based motivational care interventions have significant clinical benefits for patients with endometriosis in the perioperative period. Compared with conventional care, this intervention model effectively promotes postoperative recovery, enhances sleep quality, alleviates pain, and reduces negative emotions such as anxiety and depression. In addition, it significantly improves patients’ self-care abilities, quality of life, and overall comfort, resulting in higher patient satisfaction and a lower incidence of adverse events. These findings provide evidence supporting the incorporation of mindfulness-based motivational care into perioperative nursing protocols for endometriosis patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Awad Hegazy A. A new look at the theoretical causes of endometriosis: narrative review. Int J Reprod Biomed. 2024;22(5):343–356. doi:10.18502/ijrm.v22i5.16433
2. Bulun SE, Yildiz S, Adli M, et al. Endometriosis. Endocr Rev. 2019;40(4):1048–1079.
3. Rolla E. Endometriosis: advances and controversies in classification, pathogenesis, diagnosis, and treatment. F1000Res. 2019;8. doi:10.12688/f1000research.17047.1
4. Koninckx PR, Fernandes R, Ussia A, et al. Pathogenesis based diagnosis and treatment of endometriosis. Front Endocrinol. 2021;12:745548. doi:10.3389/fendo.2021.745548
5. Chen Y, Mo Z, Cao J, et al. Application of doctor-nurse-patient integration management mode in patients with endometriosis. Iran J Public Health. 2018;47(10):1546–1551.
6. Simkin DR, Black NB. Meditation and mindfulness in clinical practice. Child Adolesc Psychiatr Clin N Am. 2014;23(3):487–534. doi:10.1016/j.chc.2014.03.002
7. Öztürk A, Hüseyin TG, Ömer FK, Öztekin MF, Esen Z. Investigation of the relationship between mindfulness, social media addiction and psychological resilience levels in nursing students. J Mod Nurs Pract Res. 2024;4(3):17. doi:10.53964/jmnpr.2024017
8. Aldridge M, Gallegos C, Bailey M. Parent experiences using a mindfulness app for mental health wellbeing. J Mod Nurs Pract Res. 2024;5(2):4. doi:10.53964/jmnpr.2025004
9. Serrat M, Sanabria-Mazo JP, Almirall M, et al. Effectiveness of a multicomponent treatment based on pain neuroscience education, therapeutic exercise, cognitive behavioral therapy, and mindfulness in patients with fibromyalgia (FIBROWALK study): a randomized controlled trial. Phys Ther. 2021;101(12). doi:10.1093/ptj/pzab200
10. Knoerl R, Mazzola E, Woods H, et al. Exploring the feasibility of a mindfulness-music therapy intervention to improve anxiety and stress in adolescents and young adults with cancer. J Pain Symptom Manage. 2022;63(4):e357–e363. doi:10.1016/j.jpainsymman.2021.11.013
11. Allaire C, Bedaiwy MA, Yong PJ. Diagnosis and management of endometriosis. Cmaj. 2023;195(10):E363–e371. doi:10.1503/cmaj.220637
12. Gu C, Peng Y, Peng Y, Lin S, Yao J, Chen X. Effects of a 4-week internet-delivered mindfulness-based cancer recovery program on anxiety, depression, and mindfulness among patients with breast cancer. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024;49(7):1130–1142. doi:10.11817/j.issn.1672-7347.2024.240028
13. Duan D, Wang H, Tong L, et al. Online mindfulness-based stress reduction improves anxiety and depression status and quality of life in caregivers of patients with severe mental disorders. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2024;53(1):108–115. doi:10.3724/zdxbyxb-2023-0555
14. Zitser J, Allen IE, Falgàs N, et al. Pittsburgh sleep quality index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS One. 2022;17(6):e0270095. doi:10.1371/journal.pone.0270095
15. Karcioglu O, Topacoglu H, Dikme O, et al. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
16. Gonzalez-Baz MD, Pacheco Del Cerro E, Ferrer-Ferrándiz E, et al. Psychometric validation of the Kolcaba general comfort questionnaire in critically ill patients. Aust Crit Care. 2023;36(6):1025–1034. doi:10.1016/j.aucc.2022.12.013
17. Yue T, Li Q, Wang R, et al. Comparison of hospital anxiety and depression scale (HADS) and Zung self-rating anxiety/depression scale (SAS/SDS) in evaluating anxiety and depression in patients with psoriatic arthritis. Dermatology. 2020;236(2):170–178. doi:10.1159/000498848
18. Alsubiheen AM, Choi W, Yu W, et al. The effect of task-oriented activities training on upper-limb function, daily activities, and quality of life in chronic stroke patients: a randomized controlled trial. Int J Environ Res Public Health. 2022;19(21):14125. doi:10.3390/ijerph192114125
19. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Medicine. 2016;4:2050312116671725. doi:10.1177/2050312116671725
20. Mattisson M, Börjeson S, Lindberg M, et al. Psychometric evaluation of the telenursing interaction and satisfaction scale. Scand J Caring Sci. 2023;37(3):687–697. doi:10.1111/scs.13149
21. Koninckx PR, Ussia A, Adamyan L, et al. Pathogenesis of endometriosis: the genetic/epigenetic theory. Fertil Steril. 2019;111(2):327–340. doi:10.1016/j.fertnstert.2018.10.013
22. Pirtea P, Vulliemoz N, de Ziegler D, et al. Infertility workup: identifying endometriosis. Fertil Steril. 2022;118(1):29–33. doi:10.1016/j.fertnstert.2022.03.015
23. Nezhat C, Vang N, Tanaka PP, et al. Optimal management of endometriosis and pain. Obstet Gynecol. 2019;134(4):834–839. doi:10.1097/AOG.0000000000003461
24. Beerse ME, Van Lith, T, Pickett, SM, et al. Biobehavioral utility of mindfulness-based art therapy: neurobiological underpinnings and mental health impacts. Exp Biol Med. 2020;245(2):122–130. doi:10.1177/1535370219883634
25. Lee SH, Cho SJ. Cognitive behavioral therapy and mindfulness-based cognitive therapy for depressive disorders. Adv Exp Med Biol. 2021;1305:295–310. doi:10.1007/978-981-33-6044-0_16
26. Rusch HL, Rosario, M, Levison, LM, et al. The effect of mindfulness meditation on sleep quality: a systematic review and meta-analysis of randomized controlled trials. Ann NY Acad Sci. 2019;1445(1):5–16. doi:10.1111/nyas.13996
27. Segal ZV, Dimidjian S, Beck A, et al. Outcomes of online mindfulness-based cognitive therapy for patients with residual depressive symptoms: a randomized clinical trial. JAMA Psychiatry. 2020;77(6):563–573. doi:10.1001/jamapsychiatry.2019.4693
28. Alio L, Angioni S, Arena S, et al. Endometriosis: seeking optimal management in women approaching menopause. Climacteric. 2019;22(4):329–338. doi:10.1080/13697137.2018.1549213
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.