Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Study on the Correlation of Skin Advanced Glycation End Products With Diabetic Cardiovascular Autonomic Neuropathy
Received 12 August 2024
Accepted for publication 15 January 2025
Published 3 February 2025 Volume 2025:18 Pages 335—343
DOI https://doi.org/10.2147/DMSO.S491158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Yucheng Fang, Wu Dai, Yonghong Cao
Department of Endocrinology, Hefei second People’s Hospital, Hefei, 230011, People’s Republic of China
Correspondence: Yucheng Fang, Email [email protected]
Aim: To investigate the correlation of advanced glycation end products (AGEs) with diabetic cardiovascular autonomic neuropathy (DCAN). Factors affecting DCAN and those related to skin AGE accumulation in patients with DCAN were analyzed.
Materials and Methods: A total of 192 patients with type 2 diabetes mellitus (T2DM) who were hospitalized in the Department of Endocrinology of Hefei Second People’s Hospital from November 2020 to December 2022 were included and divided into DCAN (n=121) and No_DCAN (n=71) groups based on the results of Ewing test. All patients completed the detection of skin AGEs accumulation. The clinical features of the two groups were analyzed; the factors affecting DCAN were analyzed by multiple logistic regression analysis, and those related to skin AGE accumulation in patients with DCAN were analyzed by Spearman correlation analysis and Pearson correlation analysis.
Results: Compared with the No_DCAN group, the combined DR ratio, fasting plasma glucose (FPG), and skin AGEs were increased in the DCAN group (all P< 0.05). Multivariate logistic regression analysis showed that FPG, combined DR, and skin AGEs all affected DCAN (P< 0.05). Spearman correlation analysis showed that skin AGE accumulation in patients with DCAN was correlated with sex (male or female) and the presence of vascular plaques (All P< 0.05). Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN was correlated with age, diabetes course, diastolic blood pressure, uric acid, creatinine and UACR levels (All P< 0.05).
Conclusion: Skin AGEs, combined DR and FPG affected DCAN, and skin AGEs, combined DR and FPG were closely related to the incidence of DCAN. Sex (male or female), presence of vascular plaques, age, diabetes course, diastolic blood pressure, uric acid levels, creatinine levels and UCAR levels were correlated with skin AGE accumulation in patients with DCAN.
Keywords: diabetic cardiovascular autonomic neuropathy, skin advanced glycation end products
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disease with a high incidence, mainly among the middle-aged and older adult groups, and is a common clinical disease.1 T2DM accounts for more than 90% of the incidence of diabetes.1 The onset of diabetic cardiac autonomic neuropathy (DCAN) is insidious, and its early symptoms are atypical.2 Most patients with T2DM tend to ignore symptoms in the early stages without treatment until DCAN progresses to a severe stage, with arrhythmia, severe orthostatic hypotension, painless myocardial infarction, and sudden cardiac death, increasing morbidity and mortality.2 Correct identification of high-risk patients with DCAN and early intervention can delay the progression of DCAN and play a key role in its treatment.2
Advanced glycation end products (AGEs) refer to the products formed by irreversible reaction of reducing sugars with proteins or lipids, which play an important role in the occurrence and development of diabetes mellitus and diabetes complications.3 AGEs can be classified by source into endogenous AGEs and dietary AGEs.4 Several studies have shown that high concentrations of AGEs in vivo may even induce diabetes by enhancing oxidative stress.5 During the decomposition of AGEs, reactive oxygen species (ROS) can produce and quickly oxidize plasma proteins. This process results in advanced oxidized protein products (AOPPs), which are tyrosine-containing cross-linked proteins that contribute to inflammation and various diseases including diabetes.6 AGEs have been linked to the microvascular complications of diabetes, and their accumulation in peripheral nerves has recently been recognized as another risk factor for the development of diabetic neuropathy (DN).7 Furthermore, a study has shown that AGEs can predict the occurrence of diabetic kidney disease (DKD).8 A study showed that diabetic peripheral neuropathy (DPN) is correlated with AGEs.9 AGEs are associated with cardiovascular autonomic neuropathy (CAN).7
This study aimed to explore the factors that affected DCAN development and those related to skin AGE accumulation in patients with DCAN to provide a clinical basis for the early diagnosis and prevention of AGE formation in patients with DCAN.
Materials and Methods
Study Participants
A total of 192 patients with T2DM hospitalized in the Department of Endocrinology, Hefei Second People’s Hospital, from November 2020 to December 2022, including 119 males and 73 females, were selected as participants. Based on the Ewing test results, the patients were divided into the DCAN group (n=121) and the No_DCAN group (n=71). Inclusion criteria were: all patients aged 18–75 years who met the diagnostic criteria for diabetes established by the WHO Health Organization in 1999. Exclusion criteria were: pregnant and lactating women; patients with serious diseases of heart, brain, kidney, liver, and other important organs; mental or physical disability, inability to cooperate with the patient; suspected or confirmed history of alcohol or drug abuse; diabetic ketoacidosis, hypertonic coma, lactic acidosis and other acute complications associated with diabetes; patients who were using drugs that affect heart rate (beta-blockers, beta-agonists, epinephrine, dopamine, etc). 48 hours before the trial; thyroid function, blood potassium abnormalities; patients with severe hypertension or proliferative retinopathy who are at risk for Ewing test; patients with skin scars, lichens, vitiligo, malformed skin, and infectious skin diseases affected AGE detection. We acknowledged that our study complies with the Declaration of Helsinki.
General Clinical and Biochemical Measurements
Data on age, sex, and course of diabetes were collected; blood pressure, height, and weight were measured, and body mass index (BMI) was calculated. Carotid artery ultrasonography was used to determine whether patients had vascular plaques, and fundus radiography was used to determine whether patients had diabetic retinopathy (DR). After fasting for more than 8 hours, 3 mL of elbow venous blood was extracted from an empty stomach the next morning, and glycated hemoglobin A1c (HbA1c) was detected by high-performance liquid chromatography. Fasting plasma glucose (FPG) and 2-hour plasma glucose (2hPG) levels were measured using Johnson and Johnson blood glucose meters. A Beckman Coulter Model 5800 automatic biochemical analyzer was used to detect triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), blood uric acid (SUA), and serum creatinine (Scr). Fasting insulin (FINS) levels were detected using a Beckman DXI800 automatic chemiluminescence analyzer. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as = FPG×FINS/22.5 and HOMA β-cell function (HOMA-β) as = 20×FINS/ (FPG3.5). Urinary albumin and creatinine were detected using radioimmunoassay and enzymatic assays, and the urinary albumin/creatinine ratio (UACR) was calculated.
Measurement of CAN
Ewing tests were performed on all patients to determine the presence of DCAN. The following parameters were measured in the Ewing test: ① Resting heart rate. A resting heart rate >90 beats/min was classified as abnormal (excluding arrhythmia and cardiac insufficiency). ② Fist test. Blood pressure was measured immediately after 3 minutes of continuous hard clenching. A systolic blood pressure rise of > 16 mmHg was considered normal, and a systolic blood pressure rise of less than 10 mmHg was considered abnormal. ③ Poor blood pressure in the lying position. The patient’s blood pressure was measured in the supine position at rest; subsequently, the patient was asked to stand immediately, and blood pressure was measured within 1 min. A decrease in systolic blood pressure > 20 mmHg or diastolic blood pressure > 10 mmHg was considered abnormal. The difference in heart rate per minute in the lying position was determined. It was considered normal if the frequency was greater than 10 beats per minute. It was considered abnormal if the frequency was less than 10 times/min. Items 1, 2, and 4 were scored 1 point, and item 3 was scored 2 points. Those with more than 2 abnormal items and a total score ≥2 points were considered to have DCAN. Before the Ewing test, the subjects avoided strenuous exercise for 24 hours, avoided alcohol and tea consumption for 10 hours, and stopped using drugs that affect heart rate (β-blockers, angiotensin-converting enzyme inhibitors (ACEI), angiotensin-II receptor antagonists (ARB) and other drugs) for more than 48 hours. After each Ewing test, the participants rested for at least 2 min before performing the next Ewing test.
Detection of Skin AGEs
An AGEPro non-invasive detector for AGEs was used to measure their accumulation in the skin based on the obtained skin AGE fluorescence spectrum and skin diffuse reflectance spectrum. The skin was scanned 3 times to obtain the average value.
Statistical Analysis
The SPSS24.0 statistical software was used for analysis. The measurement data of normal distribution were expressed as x±s, and a t-test was used for comparison. Non-normally distributed measures were expressed as the median and interquartile range [M(QL, QU)] and compared using rank sum tests. Statistical data were expressed as n (%) and aχ2 test was used. Factors affecting DCAN were analyzed using multivariate logistic regression. Spearman and Pearson correlation analyses were used to analyze the factors correlated with skin AGE accumulation in patients with DCAN. P<0.05 indicated a statistically significant result.
Results
Comparison of General Data and Biochemical Indexes Between the Two Groups
Compared with the No_DCAN group, combined DR Ratio, FPG, and skin AGEs were increased in the DCAN group (all P<0.05). There were no significant differences in sex, age, diabetes course, vascular plaques, BMI, systolic blood pressure, diastolic blood pressure, 2hPG, HbA1c, FINS, TG, TC, LDL-C, HDL-C, SUA, Scr, HOMA-β, HOMA-IR, and UACR between the two groups (All P>0.05) (Table 1).
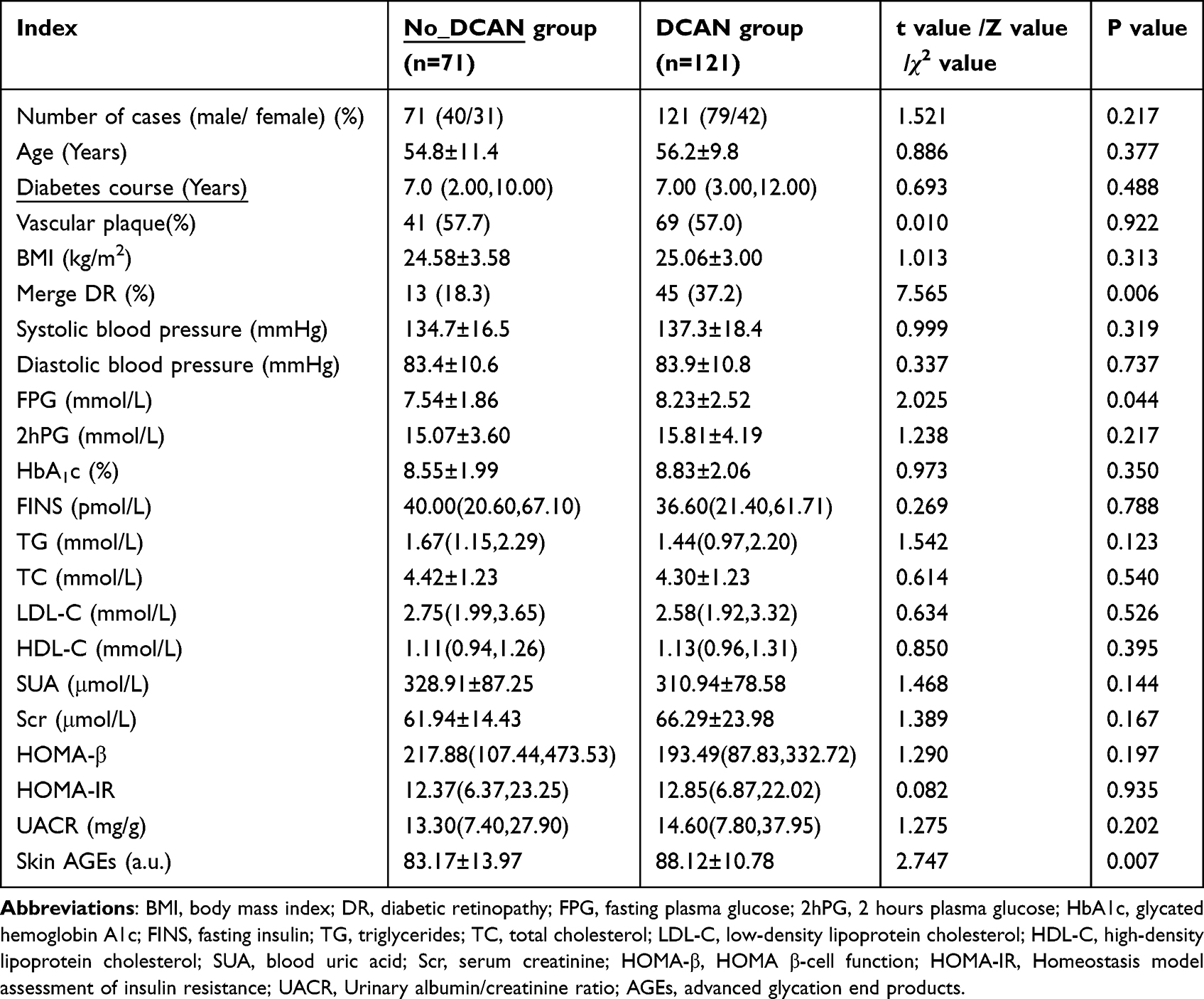 |
Table 1 Comparison of General Data and Biochemical Indices Between the Two Groups [x±s, M(QL, QU), n (%)] |
Factors Influencing DCAN Analyzed by Multivariate Logistic Regression
FPG, combined DR, and skin AGEs were independent variables, and DCAN was the dependent variable. Multivariate logistic regression was used to analyze the factors affecting DCAN. FPG, combined DR, and skin AGEs were risk factors for DCAN (all P<0.05) (Table 2).
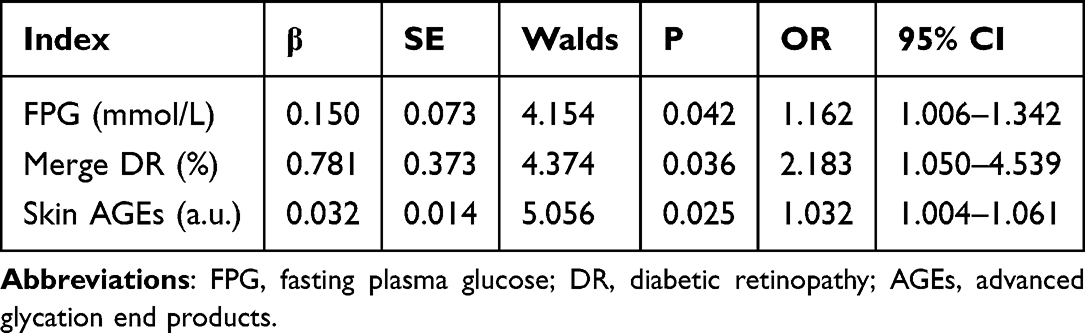 |
Table 2 Multi-Factor Logistic Regression Analysis of DCAN Influencing Factors |
Spearman Correlation Analysis of the Correlation Factors of Skin AGE Accumulation in Patients With DCAN
Spearman correlation analysis showed that the skin AGE accumulation in patients with DCAN correlated negatively with sex (P<0.05). Skin AGE accumulation in patients with DCAN correlated positively with the presence of vascular plaques (P<0.05) (Table 3).
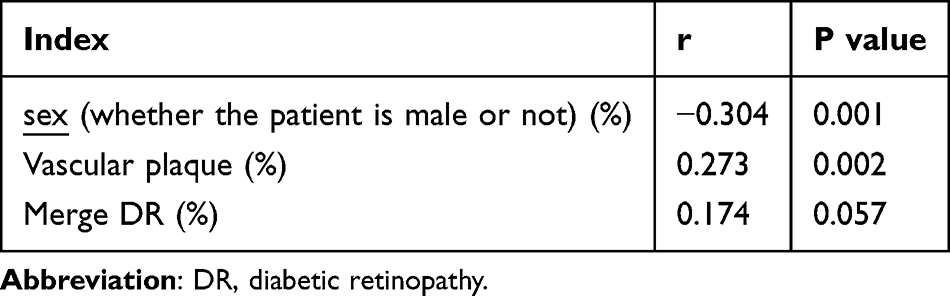 |
Table 3 Correlation Between Related Indicators and Skin AGEs Accumulation in DCAN Patients |
Pearson Correlation for Factors Associated With Skin AGE Accumulation in Patients With DCAN
Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with age, diabetes course, uric acid, creatinine and UACR levels (all P<0.05). Skin AGE accumulation with DCAN correlated negatively with diastolic blood pressure (P<0.05) (Table 4, Figures 1–6).
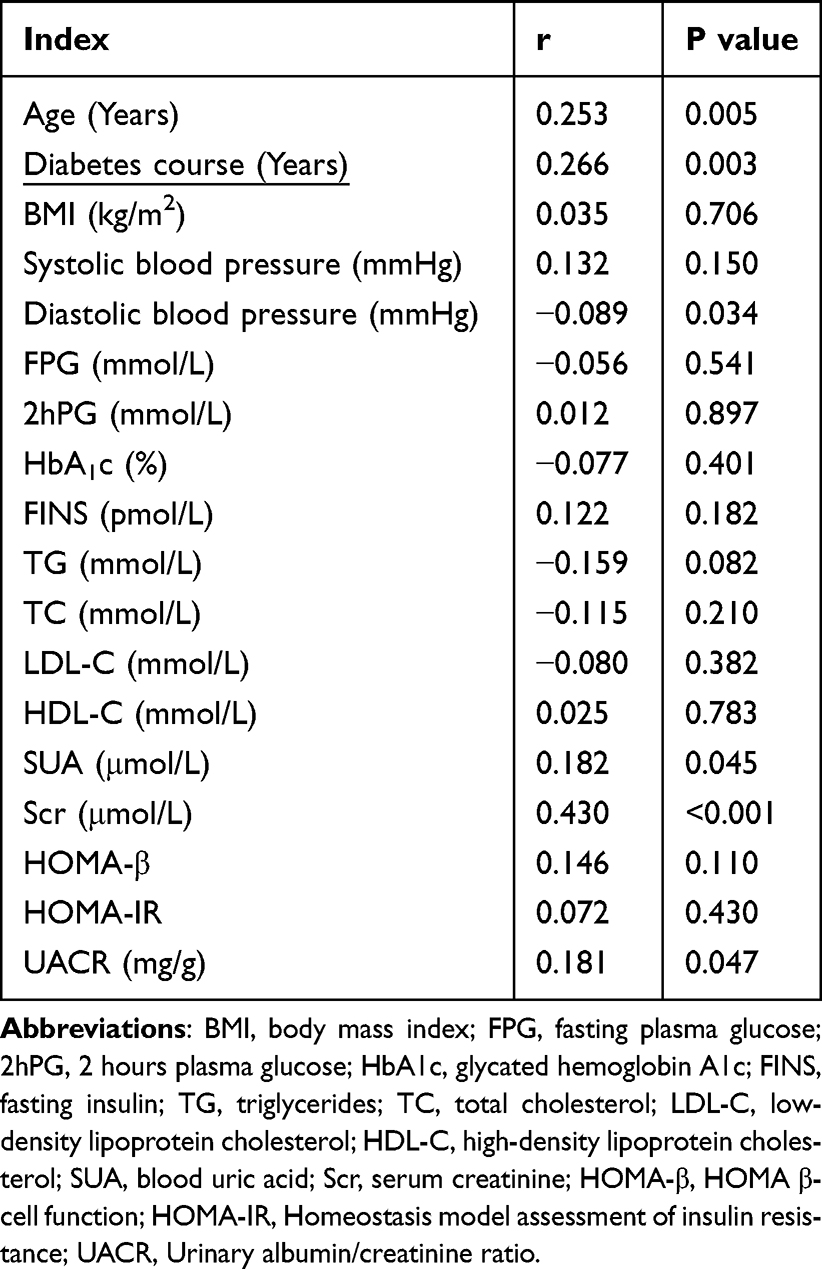 |
Table 4 Linear Correlation Between Related Indicators and Skin AGEs Accumulation in DCAN Patients |
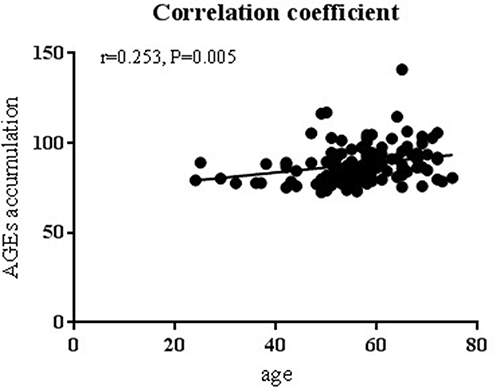 |
Figure 1 Scatter plot of the correlation between age and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with age (P<0.05). |
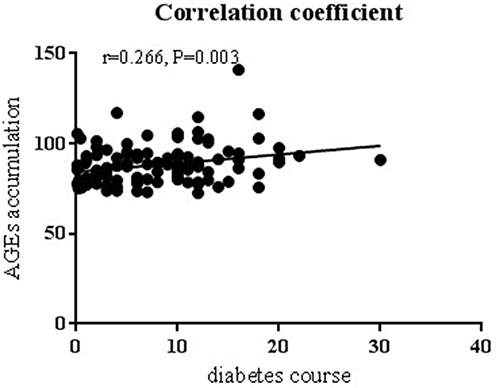 |
Figure 2 Scatter plot of the correlation between diabetes course and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with diabetes course (P<0.05). |
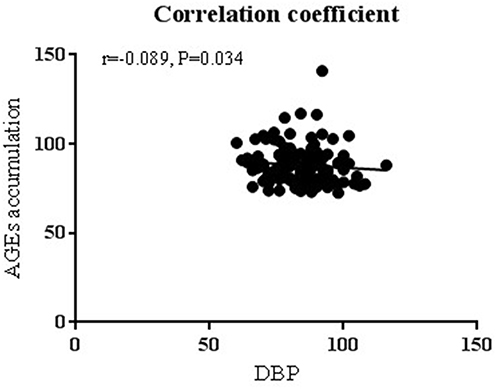 |
Figure 3 Scatter plot of the correlation between diastolic blood pressure and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated negatively with diastolic blood pressure (P<0.05). |
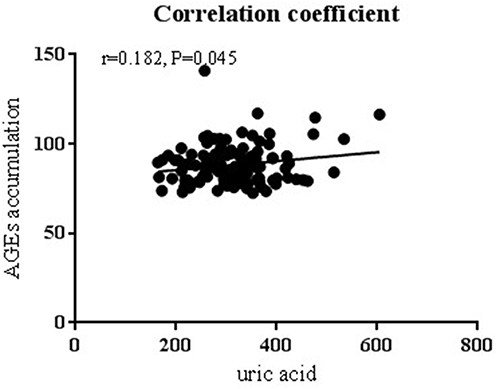 |
Figure 4 Scatter plot of the correlation between uric acid and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with uric acid (P<0.05). |
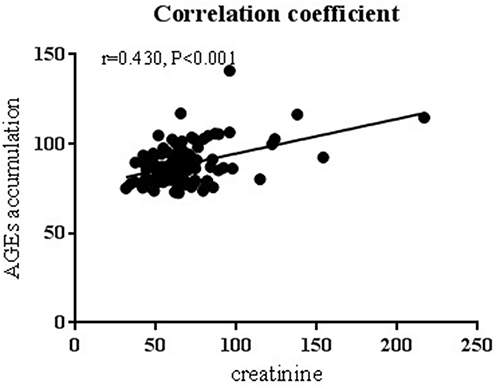 |
Figure 5 Scatter plot of the correlation between creatinine and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with creatinine (P<0.05). |
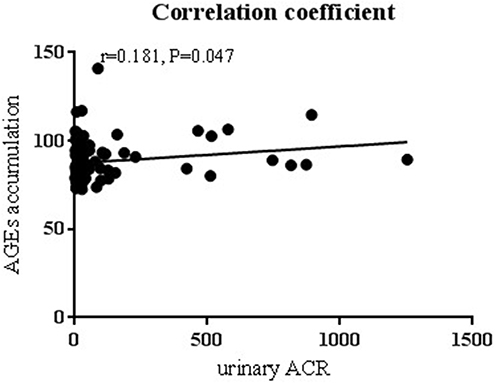 |
Figure 6 Scatter plot of the correlation between UACR and skin AGEs accumulation in patients with DCAN. Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN correlated positively with UACR (P<0.05). |
Discussion
AGEs are the products of an irreversible reaction between reducing sugars, proteins, and lipids.3 They are crucial in the occurrence and development of diabetes and related complications.3 AGEs show moderate production under normal physiological conditions, which is accelerated under hyperglycemic conditions due to an increased glucose supply.10 AGEs are key for the pathophysiology of diabetic complications.10 Pathophysiological mechanisms underlying AGE-induced diabetes include direct capture and cross-linking of proteins and binding to cell surface receptors.10 The receptor for advanced glycation end products (RAGE) is the most important cell surface receptor.10 Harmful effects of AGEs include crosslinking proteins, changing protein conformation and enzyme activity, and reduced protein degradation and clearance capacity.11 In patients with T2DM, chronic hyperglycemia leads to increased production and accumulation of AGEs.12 The binding of AGEs and RAGE activates signaling pathways such as MAPK/ERK, transforming growth factor-β, JNK, and nuclear factor-KB, enhancing oxidative stress and inflammatory responses.10 The AGE/RAGE axis is associated with oxidative stress, inflammation, RAGE-induced islet beta cytotoxicity, epigenetic modifications, and diabetic complications.10
The poorer the glycemic control, the higher the prevalence of DCAN in patients with T2DM, and HbA1c correlates well with the severity of DCAN.13 In an analysis of the correlation between glycemic profiles and beta cell function in patients with DCAN, 455 diabetic patients were included in a community-based cross-sectional study of a Chinese population.14 In this study, glycemic indices such as FPG and HbA1c were significantly and independently correlated with DCAN, respectively, and β cell function parameters, such as HOMA-β were significantly and negatively correlated with DCAN.14 Compared with the No_DCAN group, FPG in the DCAN group was increased (P<0.05). Multivariate logistic regression analysis showed that the FPG level was a risk factor for DCAN (P<0.05), suggesting its association with the incidence of DCAN, consistent with the results of this study.
Diabetic retinopathy (DR) and CAN are both diabetic microvascular complications associated with CAN.15 In a study on the correlation between DR and CAN in patients with T2DM, 174 patients with T2DM were included.16 The Composite Autonomic Scoring Scale (CASS) was used to grade the severity of autonomic nerve damage, and CAN was defined as a CASS score of >2.16 The results of this study showed a significant correlation between DR and CASS.16 The study concluded that DR is the most important risk factor for predicting the presence of CAN in patients with T2DM.16 In this study, compared with the No_DCAN group, the proportion of patients with DCAN combined with DR was higher (P<0.05). Multivariate logistic regression analysis showed that combined DR was a risk factor for DCAN (P<0.05), suggesting that combined DR is associated with the incidence of DCAN, similar to the results of this study.
AGEs are correlated with DCAN. Previous studies have shown that the increase of AGEs in tissues caused by the increase of protein glycosylation caused by the rise of blood glucose is one of the pathogenesis of CAN.17 High blood sugar can cause increased glycosylation of proteins, leading to the accumulation of AGEs.18 These AGEs form intracellular and extracellular proteins, lipids, and nucleic acids through complex arrangements and cause cross-linking.18 The accumulation of AGEs is associated with the severity of peripheral and autonomic nerve abnormalities in diabetes, and this process is mediated by the receptor for advanced glycation end products (RAGE), a structurally expressed but known pattern recognition receptor for AGEs that induces inflammation.18 In addition, the interaction of AGEs and RAGE causes a chronic cascade of inflammation and tissue damage.18
Accumulation of AGEs in the skin increases in patients with T2DM with CAN.19 Compared with the No_DCAN group, skin AGEs in the DCAN group were increased (P<0.05). Multiple Logistic regression analysis showed that skin AGEs were a risk factor for DCAN (P<0.05), suggesting that skin AGEs were associated with the incidence of DCAN. Spearman correlation analysis showed that skin AGE accumulation in patients with DCAN was negatively correlated with sex (P<0.05), and positively correlated with the presence of vascular plaque (P<0.05). Pearson correlation analysis showed that skin AGE accumulation in patients with DCAN was positively correlated with age, diabetes course, uric acid, creatinine and UACR levels (all P<0.05), indicating that skin AGEs and DCAN incidence were related and that sex (male), vascular plaques, age, diabetes course, uric acid, creatinine and UACR levels are associated with the formation of AGEs in patients with DCAN. We did not discuss the mechanism of these factors affecting the accumulation of skin AGE and we think it is a limitation of the paper. But we will discuss the intrinsic link between these factors and cutaneous metabolism in our further research. This suggests that early monitoring of cutaneous AGEs can help identify people at high risk of DCAN and intervene to address the factors affecting AGE accumulation, thus providing a new strategy for the prevention and treatment of DCAN. This study provides an important basis for understanding the pathogenesis of DCAN and improving clinical diagnosis and treatment. The sample size of this study is small, and future prospective studies should be expanded to verify the causal relationship between AGEs and DCAN.
Conclusions
In summary, DCAN was correlated with skin AGEs. FPG, combined DR, and skin AGEs were risk factors for DCAN. Sex (male or female), presence of vascular plaques, age, diabetes course, uric acid level, creatinine level and UACR level were correlated with skin AGE accumulation in patients with DCAN. Therefore, for patients with T2DM, controlling blood sugar and other metabolic disorders along with early detection of DCAN by regularly monitoring skin AGEs is necessary. Early screening for skin AGEs should be performed in patients with T2DM showing poor glycemic control and DR to reduce the risk of cardiovascular disease. Patients with DCAN should be treated for vascular plaques and lower uric acid, creatinine and UACR levels to prevent AGE formation and associated complications.
Funding
This work was supported by the Medical Application Research Project of Hefei ([2019] No. 172,Hwk2023zd003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wei Y, Juan J, Su R. et al. Risk of gestational diabetes recurrence and the development of type 2 diabetes among women with a history of gestational diabetes and risk factors: a study among 18 clinical centers in China. Chin Med J. 2022;135(6):665–671. doi:10.1097/CM9.0000000000002036
2. Liu Y, Peng Y, Jin J, et al. Insulin resistance is independently associated with cardiovascular autonomic neuropathy in type 2 diabetes. J Diabetes Investig. 2021;12(9):1651–1662. doi:10.1111/jdi.13507
3. Chiu CJ, Rabbani N, Rowan S, et al. Studies of advanced glycation end products and oxidation biomarkers for type 2 diabetes. Biofactors. 2018;44(3):281–288. doi:10.1002/biof.1423
4. Li Y, Peng Y, Shen Y, Zhang Y, Liu L, Yang X. Dietary polyphenols: regulate the advanced glycation end products-RAGE axis and the microbiota-gut-brain axis to prevent neurodegenerative diseases. Crit Rev Food Sci Nutr. 2023;63(29):
5. Chen Q, Li Y, Dong L, et al. Quantitative determination of Nε-(carboxymethyl)lysine in sterilized milk by isotope dilution UPLC-MS/MS method without derivatization and ion pair reagents. Food Chem. 2022;15(385):132697. doi:10.1016/j.foodchem.2022.132697
6. Shi B, Guo X, Liu H, et al. Dissecting Maillard reaction production in fried foods: formation mechanisms, sensory characteristic attribution, control strategy, and gut homeostasis regulation. Food Chem. 2024;16(438):137994. doi:10.1016/j.foodchem.2023.137994
7. Papachristou S, Pafili K, Papanas N. Skin AGEs and diabetic neuropathy. BMC Endocr Disord. 2021;21(1):
8. Koska J, Gerstein HC, Beisswenger PJ, Reaven PD. Advanced glycation end products predict loss of renal function and high-risk chronic kidney disease in type 2 diabetes. Diabetes Care. 2022;45(3):684–691. doi:10.2337/dc21-2196
9. Zhao XW, Yue WX, Zhang SW, Chen Q. Correlation between the accumulation of skin glycosylation end products and the development of type 2 diabetic peripheral neuropathy. BMC Endocr Disord. 2022;22(1):106. doi:10.1186/s12902-022-00997-6
10. Khalid M, Petroianu G, Adem A. Advanced Glycation End Products and Diabetes Mellitus: mechanisms and Perspectives. Biomolecules. 2022;12(4):542. doi:10.3390/biom12040542
11. Stirban A, Gawlowski T, Roden M. Vascular effects of advanced glycation end products: clinical effects and molecular mechanisms. mol Metab. 2014;3(2):
12. de la Cruz-Ares S, Cardelo MP, Gutiérrez-Mariscal FM, et al. Endothelial dysfunction and advanced glycation end products in patients with newly diagnosed versus established diabetes: from the CORDIOPREV Study. Nutrients. 2020;12(1):238. doi:10.3390/nu12010238
13. Dhumad MM, Hamdan FB, Khudhair MS, Al-Matubsi HY. Correlation of staging and risk factors with cardiovascular autonomic neuropathy in patients with type II diabetes mellitus. Sci Rep. 2021;11(1):3576. doi:10.1038/s41598-021-80962-w
14. Fang P, Dong J, Zeng F, Tang Z. Analysis of the association between glucose profiles and β-cell function for diabetic cardiovascular autonomic neuropathy in China. J Diabetes Investig. 2017;8(3):354–362. doi:10.1111/jdi.12584
15. Sacchetta L, Chiriacò M, Nesti L, et al. Synergistic effect of chronic kidney disease, neuropathy, and retinopathy on all-cause mortality in type 1 and type 2 diabetes: a 21-year longitudinal study. Cardiovasc Diabet. 2022;21(1):233. doi:10.1186/s12933-022-01675-6
16. Huang CC, Lee JJ, Lin TK, et al. Diabetic retinopathy is strongly predictive of cardiovascular autonomic neuropathy in type 2 diabetes. J Diabetes Res. 2016;2016:6090749. doi:10.1155/2016/6090749
17. Agashe S, Petak S. Cardiac autonomic neuropathy in diabetes mellitus. Methodist Debakey Cardiovasc J. 2018;14(4):251–256. doi:10.14797/mdcj-14-4-251
18. Vinik AI, Erbas T, Casellini CM. Diabetic cardiac autonomic neuropathy, inflammation and cardiovascular disease. J Diabetes Investig. 2013;4(1):4–18. doi:10.1111/jdi.12042
19. Papachristou S, Pafili K, Trypsianis G, Papazoglou D, Vadikolias Κ, Papanas N. Correlation between skin advanced glycation end products and cardiac autonomic neuropathy among subjects with type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. 2022;130(12):767–772. doi:10.1055/a-1831-0991
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.