Back to Journals » Patient Preference and Adherence » Volume 17
Study of Adherence Level and the Relationship Between Treatment Adherence, and Superstitious Thinking Related to Health Issues Among Chronic Disease Patients in Southern Jordan: Cross-Sectional Study
Authors Al-Tarawneh F, Ali T, Al-Tarawneh A, Altwalbeh D ![]() , Gogazeh E, Bdair O, Algaralleh A
, Gogazeh E, Bdair O, Algaralleh A ![]()
Received 20 October 2022
Accepted for publication 27 January 2023
Published 9 March 2023 Volume 2023:17 Pages 605—614
DOI https://doi.org/10.2147/PPA.S390997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Fatima Al-Tarawneh,1 Tasneem Ali,1 Ahmad Al-Tarawneh,2 Diala Altwalbeh,1 Esraa Gogazeh,3 Ola Bdair,4 Abdulnaser Algaralleh5
1Department of Allied Medical Sciences, Karak University College, Al-Balqa Applied University, Karak, Jordan; 2Psychology Department, Faculty of Educational Sciences, Mutah University, Mutah, Jordan; 3Department of Allied Medical Sciences, Irbid University College, Al-Balqa Applied University, Irbid, Jordan; 4Department of Allied Medical Sciences, Salt University College, Al-Balqa Applied University, Salt, Jordan; 5Department of Counseling and Special Education, Faculty of Educational Sciences, Mutah University, Mutah, Jordan
Correspondence: Diala Altwalbeh, Email [email protected]
Background: For disease management, numerous drugs are prescribed. However, long-term treatment adherence is still unsatisfactory. Culture influences beliefs regarding medication, particularly irrational ideas that affect treatment adherence. The Middle East, notably Jordan, is affected by a lack of awareness of these attitudes with regard to treatment adherence.
Objective: Investigating the adherence level among patients with chronic diseases in southern Jordan. To determine whether certain demographic traits, different disease factors, and superstitions have any impact on treatment adherence.
Patients and Methods: A cross-sectional study that assessed treatment adherence and superstitious thinking-related health issues were conducted among chronic disease patients who had reviewed intrinsic medicine clinics at the Karak governmental hospital.
Results: For 314 participants, treatment adherence was categorized into three levels low-adherent patients made up 27.7% highly-adherent patients made up 49.4%, and the remaining adhered at a medium level. Treatment non-adherence was more common in the elderly and female, according to the chi-square analysis. Additionally, the classification of superstitious beliefs into three categories revealed that different percentages of the study population held low superstitious beliefs 21%, medium superstitions 54.1% and high superstitions 24.8% beliefs. The chi-square analysis revealed that the elderly, female, and low-educated patient groups were the highest in superstitious thinking. Multiple regression analysis revealed that educational level and superstitious thinking explained 0.223 of the treatment adherence variances. Treatment adherence is positively influenced by educational level β (0.244) value, but superstitious thinking is negatively influenced by β (− 0.302) value.
Conclusion: In conclusion, about half of the participants highly adhered. The results of the multiple-regression analysis indicate that superstition and education were two variables that impacted treatment adherence in this study. While superstitious beliefs lead to lower treatment adherence, education has the opposite effect. Finally, it is recommended to promote patient education to reduce superstitious beliefs, improve medication adherence.
Keywords: treatment adherence, treatment nonadherence, superstitious thinking, chronic diseases, Jordan
Introduction
Adherence to long-term pharmacotherapy in chronic disease therapy is considered crucial for treatment success.1 Adherence is defined as the process by which individuals take their medications as prescribed.2 Non-adherence is a global public health issue.3 However, numerous research have revealed that chronically diseased patients have a higher percentage of non-adherence to medication, at an average of 60%.4–6 Poor adherence leads to worse outcomes and an increased hospitalization rate.7
Poor adherence to long-term treatment is a multifactorial problem.8 These factors include the chronic condition of disease, therapy factors (complex medication regimen and polypharmacy, drug and food interactions, cost, adverse effects), patient factors (impaired memory and cognition, lack of familial and social support and care, beliefs and perceptions about the medicine).9,10
Medicine has a long history of being linked to superstitions, magic, and faith. Although scientific medicine contradicts the disease’s supernatural origins, several studies showed that many patients continue to believe in a superstitious manner toward disease causes and its treatment or have a significant misunderstanding about the disease’s origins and treatment efficacy.2,11,12 So false perceptions and beliefs play an important role in medication adherence.11,12
According to the researchers’ knowledge, this study is the first one to deal with the effects of superstition thinking on treatment adherence in Jordan. The objectives of the current study were to study the adherence level and the factor that might affect it. Also, to reveal the relationships between superstitious beliefs about prescription medications and treatment adherence in chronic disease patients in the South of Jordan.
Materials and Methods
Design, Setting and Participants
The study population consisted of a group of patients who were visiting the internal clinics at Karak Governmental Hospital. Participants had to meet the inclusion criteria if they had a chronic illness for which they had received a diagnosis and were taking medication for more than three months. Pregnant women, patients with cognitive impairment and psychiatric disorders, as well as participants who worked in the medical field, were excluded. A face-to-face interview was conducted for approximately 10 minutes utilizing a structured questionnaire.
Ethical Considerations
The Institutional Review Board of Al-Balqa University gave its approval to the study protocol (Approval Number: 2/1/145). Also, the Director of Karak Governmental Hospital gave his approval for this study. Additionally, the participant’s verbal consent prior to completing the questionnaire and supplying the researchers with information. The use of verbal consent was fully disclosed and discussed in the research proposal submitted to the IRB of Al-Balqa University for review and approval. The Declaration of Helsinki was followed, all data were preserved, and they were only used for study purposes; hence, participants’ engagement was voluntary, and they were able to discontinue at any time.
Questionnaires Development and Data Collection
A research team consisting of doctors, clinical pharmacists, psychologists, and community members developed a list of questions. The research team also discusses the questions in order to integrate concepts that are consistent with the study’s goals and objectives and, if required, eliminate any repetitions. Arabic language was used to administer the questionnaire since it has a trustworthy sound in Jordan. The questionnaire consists of two sections.
The first section included demographic questions and disease characteristics. The second part comprises two scales: the superstitious thinking and beliefs related to the health issues scale and the Medication Adherence Report Scale-5 items (MARS-5).13,14 The first scale consisted of 25 items assessing thinking and beliefs concerning medication use and health issues. It’s graded on a five-point Likert scale, with 1 indicating strong disagreement and 5 indicating strong agreement. Then it’s subdivided into three levels (ie, highly superstitious thinking; moderate, and low superstitious thinking) according to the mean score. The total score is 125 (highest score × item number (5×25=125). The following equation was used to determine the level mark range: ((highest grade - lowest grade) ÷ levels number) = ((125–25) ÷3 =33.33)). Low superstitious beliefs (scoring 25–58.33 (25 + 33.33)), moderate superstitious beliefs (scoring 58.34–91.67), and highly superstitious beliefs (scoring 91.68–125) are the three kinds of superstition. The second scale, the MARS-5, was created by Horne and Weinman to gauge patient adherence.13,14 The MARS-5 instrument has five items designed to deal with non-adherent behavior. The first item on the scale measured unintentional non-adherence, whereas the other four measured intentional non-adherence.14 Using a five-point Likert scale it’s rated with a1 equaled always and a5 equaled never. The level of non-adherence increases as the point decreases. Following its translation into Arabic, this scale was reevaluated.14 Since the total scores (5×5) equaled 25, the level range was determined using the same equation as before ((25–5) ÷ 3=6.67) and divided into three categories. Low adherence (score 5–11.67), moderate adherence (scoring> 11.68–18.35), and highly adherent (score> 18.36–25) are the three levels of adherence.
Questionnaire Validation and Reliability
Face validity was employed to verify the validity of the superstitious thinking and beliefs related to the health issues scale. The scale was distributed to seven clinical pharmacists and clinical psychologist experts. They were asked to judge on the scale items’ validity and appropriateness. Their suggestions were taken into consideration. The criterion for accepting an item was the specialist’s agreement with an average of 80%. A thorough examination of the literature was conducted to make sure that all relevant criteria were taken into account while establishing the content validity. The paper and questionnaire were located using the source databases Science Direct, PubMed/Medline, and Google Scholar. Next, 100 patients were assessed using the scale. Since their data was gathered for the pilot, it was not included in the final analysis. Construct validity, Confirmatory Factor Analysis (CFA) validity was performed utilizing the principal components analysis, and extraction method, as described in Table 1.
 |
Table 1 Results of Principal Components Analysis for Superstitious Thinking and Beliefs Related to Health Issues Scale (Summary of Extraction Method) |
According to Table 1, there is only one component on which all scale items are loaded, and this component accounted for 79.057% of the entire variation. The values of (1–25) items, where item loading on one component with a value greater than 0.3, are verified in Table 1 according to the Guttmann criterion (0.451–0.931). That supports the scale validity since it only assesses one component, namely superstitious thinking and beliefs related to health issues.
In order to, assess the Medication Adherence Report Scale-5 (MARS-5) validity. Face validity was used; since it is a widely used scale, as was previously mentioned, all seven arbitrators accepted it’s without change. Cronbach’s alpha reliability coefficient was used in a pilot sample in order to evaluate the reliability of the scales used in this study. The Cronbach’s alpha reliability coefficient for the superstitious thinking related to health issues scale was 0.96. While the Cronbach’s alpha reliability coefficient for the MARS-5 scale was 0.86 as well.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS, version 22) software was used to analyze the data. Descriptive statistics were computed to describe all items of the questionnaire; mean and standard deviation for continuous variables while frequency and percent for categorical ones. The Chi-square test was performed to check the portion of individuals in the study sample who were classified as having a high, medium, or low level of adherence based on the demographic characteristics in this study. Chi-square was also utilized to verify the proportion of the study sample classified as high, medium, or low in terms of superstitious thinking. Multiple regression analysis was used to explain the effects of the study variables on treatment adherence.
Results
The study questionnaire was completed by 314 individuals, yielding an 86.5% response rate. Between the first of March and the tenth of October 2021, data were gathered. About 60% of participants are females. Approximately two-thirds had cardiovascular disease (CVD) and took two to five medications (66.88%, and 66.2% respectively). Table 2 describes more details.
 |
Table 2 Demographic and Disease Characteristics of Participants (N=314) |
Table 3 shows treatment adherence levels, according to demographic characteristics. Nearly half of the participants had a high adherence level 49.9%. The majority of the non-adherent participants were females 77%. Those with a bachelor’s degree have a high adherence level 43.9% With regard to education level. Non-adherence was higher among those over the age of 60, accounting for around 31% of those who did not adhere.
 |
Table 3 The Chi-Square Results for Distributing Study Sample Members to the Treatment Adherence Level and the Superstitious Thinking Level Based on Demographics of the Study Sample N (314) |
Additionally, 54.1% of people, as seen in Table 3, exhibit a moderate level of superstition. In terms of gender and educational attainment, a majority of those with a high degree of superstitious thinking were female (76.9%) and had only completed secondary school or less (71.8%).Differences in superstitious beliefs could be attributed to age as well. Participants above the age of 60 were the most engaged in superstitious thinking.
A multiple linear regression analysis was carried out to determine the effects of the study variables (patient age, educational level, number of medications taken by the patient, disease number, disease duration and superstitious thinking) on treatment adherence. The model’s validity in assessing the study hypothesis was checked, the high value of the computed F (16.181) and the statistically significant degrees of freedom (6, 307) demonstrates the model’s appropriateness for testing the hypothesis.
A multiple linear regression analysis was performed, Adjusted R Square 0.225 shows that all model indicators explain 22.5% of the variance in treatment adherence, which is small when compared to the number of forecasters, so the transactions of each of these variables were extracted to see their respective contributions to the prediction of treatment adherence, as shown in Table 4.
 |
Table 4 Multiple Regression Coefficients, to Verify the Effects of (Patient Age, Educational Level, Number of Medications Taken by the Patient, Disease Number, Disease Duration and Superstitious Thinking) on the Treatment Adherence Level |
The T-value demonstrates that there are just two variables (education levels and superstitious thinking) that can be confidently predicted. Because the remaining variable’ coefficients were not significant, they were removed from the regression equation, and the regression analysis of the extent of adherence to the variables (educational level and superstitious thinking) was re-analyzed stepwise. That revealed that the proportion of variance described by the variables (educational level and superstitious thinking) was 22.3%, which is quite close to the percentage of variation explained by all factors, implying that the remaining variables are negligible. Their respective transactions were extracted for use in the forecast equation to predict the level of adherence using only the two variables. Using Table 5, which provides the regression equation coefficients, the regression equation can be represented as follows:
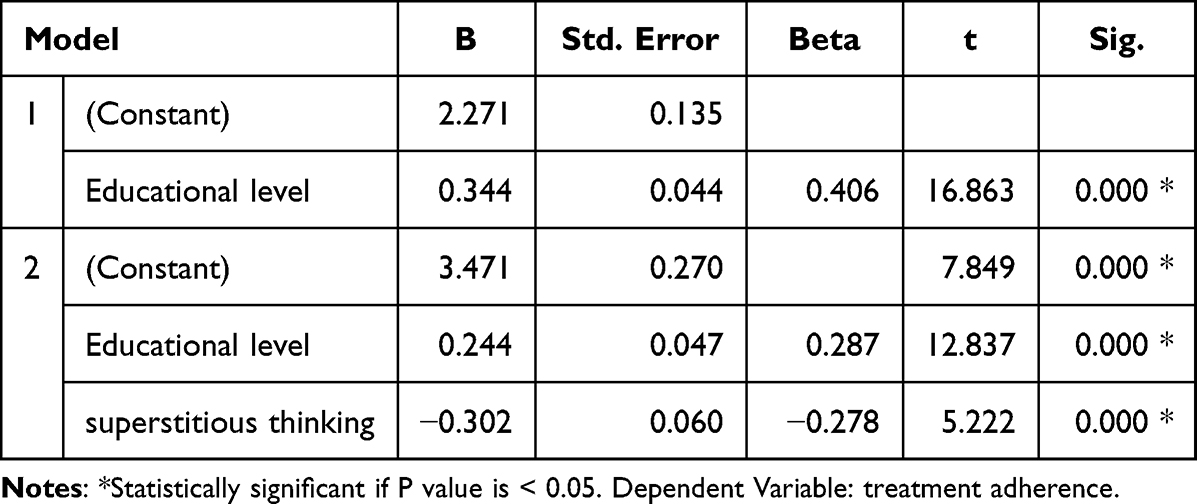 |
Table 5 Multiple Regression Coefficients, to Verify the Effects of (Educational Level, Superstitious Thinking) on the Treatment Adherence |
A = 0.244E - 0.302T + 3.471.
A: Adherence; E: Education level; T: Superstitious thinking.
According to Table 5, within this model, education level and superstitious thinking explain 0.223 of the variance in the dependent variable treatment adherence. So it turns out that the standard regression B value for educational level is 0.244, which is statistically significant. That shows if educational level values increase by one, the treatment adherence variable will increase 0.244. In addition, the model shows that the superstitious thinking variable’s standard regression B value is (−0.302), a statistical function, implying that if the value of superstitious thinking changes by one, the treatment adherence variable changes by 0.302 in the negative direction.
Discussion
This study, which included 314 people with chronic conditions, found that 49.4% of patients had high levels of adherence, 27.7% had low levels, and the remaining group had a medium level. Noted that patients’ adherence varies among patients in different groups.
The majority of non-adherent patients (77%), according to the current study, were female. Additional research supported this finding.15–17 Even though there are no proven gender variations in adherence, women were noted to exhibit low compliance to multiple doses, and non-adherence to healthcare professional advice is also a factor in women’s refusal to take recommended medications. On the other hand, according to some studies, women are more likely than males to seek preventive care and treatment.15,16
The present study’s findings showed that non-adherence was higher among those over the age of 60. Some Studies among patients with chronic diseases reported similar results to this study.18,19 That can be explained by the characteristics of chronic diseases and their management, impairment of cognitive and physical function in the elderly population may lead to more frequent cases of omitted drug use as well as diminished interactions between the elderly and their health care providers, were recognized as the key factors contributing to a decrease in adherence to treatment among the elderly.7,15,18,19 In addition, this group in the study sample had a higher level of superstitious thinking, which led to lower adherence, according to the study findings.
The current study found that education level was a significant predictor of medication adherence. According to various research’s, participants education play role in high levels of adherence to treatment protocols.20,21 Higher educated people have a tendency to grasp the importance of medications, which has a significant impact on adherence. Sweileh W.et al study’s revealed that patients who were illiterate and unable to distinguish between their prescriptions were more likely to make mistakes, be non-adherent, and have poorer medical knowledge.22
77% of study participants, or those with a high level of superstitious thinking, were female. This findings can be attributed to the observed gender differences in cognitive style, specifically the greater prevalence of intuitive and experiential thinking in females compared to the more prevalent use of rational and analytical thinking styles among males.23 This finding completely agrees with Torgler’s research, which revealed that women are more likely than men to believe in pseudoscience and spirituality.24 In addition, a 2016 survey in northern Germany found that 68% of women and just 38% of males believe in superstitions.25
The results showed that patients with secondary scientific education and below had the highest levels of superstitious beliefs. People with adequate education are less prone to believe in accidental magical abilities.24 Less-educated people are more susceptible to shallow thinking, false religion, irrational notions, hereditary behavioral tendencies, and other views that do not seem to fit with reality. That might be caused by the information’s cognitive complexity, according to Wiseman and Watt.26
According to the study’s results, patients 60 years of age and older exhibited the highest level of superstitious thinking. That could be related to a feeling of helplessness, in which the person tends to assign the origins of their illness to superstitious explanations that allow them to solve problems imaginary rather than logically solve.24
Multiple regression analysis revealed two factors that affect treatment adherence (Educational level and superstitious thinking). A high educational level improves treatment adherence, which is consistent with other studies that demonstrate this relationship.6,27–29
However, multiple-regression results revealed superstition thinking decreases adherence. That may be because of the idea that people believe medications have more negative effects than positive ones. And as shown by the scale items, these superstitious beliefs encourage people to adopt other regimens based on traditional medicine rather than their prescribed medications.30 These superstitious beliefs are present in the study sample; this may be the result of an intersection of superstitious thinking and scientific manifestations, as in medicine, where folk medicine myths are widely in the Arab world in the form of prescriptions and herbs provided by charlatans, some of which accidentally cured, and the patient believes in the efficacy of these recipes. Additionally, superstitious beliefs serve an emotional purpose in a person’s life by giving him a sense of security and comfort in the face of the danger that threatens his life, as a spirit of hope and apparent optimism.12,31 Superstitious people, in the opinion of some specialists, have beliefs that limit their flexibility and prevent them from changing. These ideas affect how people respond to treatments, health, and psychological needs.25
Study Implications
The study results are helpful and crucial in providing insight into the extent of treatment adherence among patients with chronic disease and some factors that may affect it. Also, it highlights factors that may affect treatment associated with superstitious thinking. Additionally, the results of this study are also helpful within the field of health care, health care directors, and policymakers in designing educational programs for patients with chronic diseases. That will be helpful for health care and economic purposes.
Also, this study provides some basic information associated with the Jordanian patients within the region with a restricted variety of studies, which may encourage researchers to conduct additional research during this relevance confirms these results. Additionally, this study constructs a new scale to measure superstitious thinking and beliefs associated with health issues. So, it can be used by other researchers to explore many health issues that may be affected by patient thought.
Study Limitations
The current study has several limitations. Since it was conducted in the southern part of Jordan, the results might not be generalizable to other areas. Additionally, social desirability bias may have affected participant responses. Moreover, the hospital environment restricted the interviewing time between the researcher and participants, thus limiting the information exchange process.
Conclusion
In conclusion, the study’s participants reported a high level of adherence in almost half the cases. High-adherence participants were either male, had bachelor’s degrees or above, and were between the ages of 40 and 50. Additionally, superstitious thinking significantly influences about 25% of the study participants. In addition, females, the elderly, and individuals with low levels of education had elevated levels of superstitions.
The multiple-regression analysis results show that the degree of education and superstitions were two factors that affected treatment adherence in this study. On treatment adherence, education has a favorable effect. While superstitious thinking decrease adherence.
Therefore, it is recommended to implement continuing education programs for patients, particularly about their notions and superstitions, to ensure optimal medication adherence. It also calls for more research about treatment adherence issues and how to address them.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jüngst C, Gräber S, Simons S, Wedemeyer H, Lammert F. Medication adherence among patients with chronic diseases: a survey-based study in pharmacies. QJM. 2019;112(7):505–512. doi:10.1093/qjmed/hcz058
2. Shahin W, Kennedy GA, Stupans I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: a systematic review. Patient Prefer Adherence. 2019;13:1019.
3. Costa E, Giardini A, Savin M, et al. Interventional tools to improve medication adherence: review of literature. Patient Prefer Adherence. 2015;9:1303.
4. Menditto E, Cahir C, Aza-Pascual-Salcedo M, et al. Adherence to chronic medication in older populations: application of a common protocol among three European cohorts. Patient Prefer Adherence. 2018;12:1975.
5. Giardini A, Martin MT, Cahir C, et al. Toward appropriate criteria in medication adherence assessment in older persons: position Paper. Aging Clin Exp Res. 2016;28(3):371–381.
6. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: a cross-sectional study in a low-income country. Biomed Res Int. 2020;2020:548.
7. Jin H, Kim Y, Rhie SJ. Factors affecting medication adherence in elderly people. Patient Prefer Adherence. 2016;10:2117.
8. Maffoni M, Traversoni S, Costa E, et al. Medication adherence in the older adults with chronic multimorbidity: a systematic review of qualitative studies on patient’s experience. Eur Geriatr Med. 2020;11(3):369–381.
9. Shruthi R, Jyothi R, Pundarikaksha H, Nagesh G, Tushar T. A study of medication compliance in geriatric patients with chronic illnesses at a tertiary care hospital. J Clin Diagnostic Res. 2016;10(12):FC40.
10. Waari G, Mutai J, Gikunju J. Medication adherence and factors associated with poor adherence among type 2 diabetes mellitus patients on follow-up at Kenyatta National Hospital, Kenya. Pan Af Med J. 2018;29(1):1–15.
11. Kretchy I, Owusu-Daaku F, Danquah S. Spiritual and religious beliefs: do they matter in the medication adherence behaviour of hypertensive patients? Biopsychosoc Med. 2013;7(1):1–7.
12. Taher M, Pashaeypoor S, Cheraghi MA, Karimy M, Hoseini ASS. Superstition in health beliefs: concept exploration and development. J Family Med Primary Care. 2020;9(3):1325.
13. Horne R, Weinman J. Self-regulation and self-management in asthma: exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol Health. 2002;17(1):17–32.
14. Lemay J, Waheedi M, Al-Sharqawi S, Bayoud T. Medication adherence in chronic illness: do beliefs about medications play a role? Patient Prefer Adherence. 1687;2018(12):21.
15. Al-Noumani H, Al-Harrasi M, Jose J, Al-Naamani Z, Panchatcharam SM. Medication Adherence and Patients’ Characteristics in Chronic Diseases: a National Multi-Center Study. Clin Nurs Res. 2022;31(3):426–434.
16. Beatty L, Binnion C. A systematic review of predictors of, and reasons for, adherence to online psychological interventions. Int J Behav Med. 2016;23(6):776–794.
17. Angadi NB, Kavi A, Torgal SS. Therapeutic Adherence among Elderly with Chronic Diseases Residing in Urban Area of South India–A Descriptive Cross Sectional Study. Biomed Pharmacol J. 2020;13(4):2109–2116.
18. Kim SJ, Kwon OD, Han EB, et al. Impact of number of medications and age on adherence to antihypertensive medications: a nationwide population-based study. Medicine. 2019;98:49.
19. Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155.
20. Uchmanowicz B, Chudiak A, Uchmanowicz I, Rosińczuk J, Froelicher ES. Factors influencing adherence to treatment in older adults with hypertension. Clin Interv Aging. 2018;13:2425.
21. Damiani G, Basso D, Acampora A, et al. The impact of level of education on adherence to breast and cervical cancer screening: evidence from a systematic review and meta-analysis. Prev Med. 2015;81:281–289.
22. Sweileh W, Aker O, Hamooz S. Rate of compliance among patients with diabetes mellitus and hypertension. Natural Sci. 2004;19(1):1–11.
23. Maqsood A, Jamil F, Khalid R. Thinking Styles and Belief in Superstitions: moderating Role of Gender in Young Adults. Pakistan J Psychol Res. 2018;33.
24. Mocan N, Pogorelova L. Compulsory schooling laws and formation of beliefs: education, religion and superstition. J Econ Behav Organ. 2017;142:509–539.
25. Graeupner D, Coman A. The dark side of meaning-making: how social exclusion leads to superstitious thinking. J Exp Soc Psychol. 2017;69:218–222.
26. Neubauer A, Wammerl M, Benedek M, Jauk E, Jaušovec N. The influence of transcranial alternating current stimulation (tACS) on fluid intelligence: an fMRI study. Pers Individ Dif. 2017;118:50–55.
27. Awwad O, Akour A, Al-Muhaissen S, Morisky D. The influence of patients’ knowledge on adherence to their chronic medications: a cross-sectional study in Jordan. Int J Clin Pharm. 2015;37(3):504–510.
28. Alkatheri AM, Albekairy AM. Does the patients’ educational level and previous counseling affect their medication knowledge? Ann Thorac Med. 2013;8(2):105.
29. Romero‐Sanchez J, Garcia‐Cardenas V, Abaurre R, Martínez‐Martínez F, Garcia‐Delgado P. Prevalence and predictors of inadequate patient medication knowledge. J Eval Clin Pract. 2016;22(5):808–815.
30. Andersson Sundell K, Jönsson AK. Beliefs about medicines are strongly associated with medicine‐use patterns among the general population. Int J Clin Pract. 2016;70(3):277–285.
31. Putzi S. A to Z World Lifecycles: 175 Countries-Birth, Childhood, Coming of Age, Dating and Courtship, Marriage, Family and Parenting, Work Life, Old Age and Death. World Trade Press; 2008.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.