Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Stuck between a rock and a hard place: the work situation for nurses as leaders in municipal health care
Authors Nilsen E, Olafsen A, Steinsvåg A, Halvari H, Grov E
Received 17 November 2015
Accepted for publication 3 February 2016
Published 5 April 2016 Volume 2016:9 Pages 153—161
DOI https://doi.org/10.2147/JMDH.S100640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Etty R Nilsen,1 Anja H Olafsen,1 Anne Grethe Steinsvåg,2 Hallgeir Halvari,1 Ellen K Grov3
1Department of Strategy and Finance, School of Business, University College of Southeast-Norway, 2Department of Nursing Science, Faculty of Health Sciences, University College of Southeast-Norway, Kongsberg, 3Department of Nursing and Health Promotion, Faculty of Health Sciences, Oslo and Akershus University College, Oslo, Norway
Background: The paper aims to present how nursing leaders in the municipal health care perceive the interaction with and support from their superiors and peers. The paper further aims to identify the leaders’ vulnerability and strength at work in the current situation of shortage of manpower and other resources in the health care sector. This is seen through the lens of self-determination theory.
Methods: Qualitative interviews were conducted with nine nursing leaders in nursing homes and home-care services, which, in part, capture the municipal health care service in a time of reform.
Results: The nursing leaders are highly independent regarding their role as leaders. They act with strength and power in their position as superiors for their own staff, but they lack support and feel left alone by their leader, the municipal health director. The relation between the nursing leaders and their superiors is characterized by controlling structures and lack of autonomy support. As a consequence, the nursing leaders’ relations with subordinates and particularly peers, contribute to satisfy their needs for competence and relatedness, and, to some extent, autonomy. However, this cannot substitute for the lack of support from the superior level.
Conclusion: The paper maintains a need to increase the consciousness of the value of horizontal support and interaction with peers and subordinates for the municipal nursing leader. Also, the need for increased focus on “the missing link” upward between the municipal health director and the nursing leader is revealed. The impact of extensive controlling structures and lack of autonomy support from superiors might lead to reduced motivation and well-being.
Keywords: motivation, nursing leader, leadership, municipal health care service
A Letter to the Editor has been received and published for this article
Introduction
Nursing leaders in the municipal health care service have a lot of responsibility and are highly independent in their daily tasks. Home nursing leaders and nursing home leaders are top managers of nursing homes or managers of home-based services. They are senior executives in large organizations and, at the same time, they are middle managers in the wider municipal organization. A strained economy and a continuous flow of reforms characterize the municipal health care service, and the focus in this study is on how the nursing leaders stay afloat in their role as leaders, especially during the implementation of a new reform, coined as “the Coordination Reform” in Norway, which places increased demands on the leadership position.
The Coordination Reform represents a new health care structure in Norway, effectuated from 2012.1 The primary aim of this reform is to coordinate the health specialist service (given at the hospitals) and the health care service in Norwegian municipalities. The reform is also an attempt to meet the “resource challenge”, which alludes to the foreseen shortage of manpower in the health care sector in the future. One way of approaching the resource challenge is to enlarge the out-patient service, which means that the patients live at home, except during high-tech treatment. The intention is, to a higher extent, to move responsibility for advanced treatment and follow-up from the hospitals to the municipalities. So far, the health care services in the municipalities have dealt with caring for the elderly and those in need of low threshold services and treatment, rehabilitation, and follow-up, and prevention of diseases among infants and preschool children. For the elderly and for persons of all ages with disabilities, the medical and the social care services have become intertwined, especially in the home-care service.2 Due to earlier discharge from hospitals and greater responsibilities for advanced treatment and follow-up, the heads of municipalities have to prepare for new required activities and an unpredictable and challenging health care service. Due to this and other reforms, strongly influenced by New Public Management, responsibilities are being pushed “down” to the lowest level of the health care system.2
Taking into account the implementation of the Coordination Reform in Norway, the role of the nursing leader in municipal health care service is influenced. The nursing leaders are to allocate resources, or to recruit, for new tasks and more advanced medical and caring demands. Limited resources in terms of tight annual budgets and health care personnel not necessarily competent to face the new roles and obligations might leave the nursing leaders in a position described as “stuck between a rock and a hard place”. The consequences of balancing between the requests and demands, staff and cost limitations, and the ability to deliver quality care and satisfy the obligations may result in a squeeze for the nursing leaders.
The purpose of the present study is to investigate the role of nursing leaders in the municipal health care service, and we will use self-determination theory (SDT)3 as an analytical tool. We ask the following question: How are the nursing leaders supported in their role as leaders in a municipal health care setting?
The paper is organized as follows. We start by giving a short account of the theoretical framework, the SDT, introduced by Deci and Ryan,3 followed by an outline of our research design and methods. We then report and discuss the results and round off with the conclusion and implications for practice.
Motivation and management
The health care service in the municipalities is characterized by bureaucracy and, at the same time, by a steady flow of new reforms. These reforms are often inspired by redesigns already implemented and tested in the private sector,4 and they reinforce the emphasis on leadership.2,5 The public sector is often claimed to have a distinctive stamp also when it comes to the role of the leader and management, and the discussion of the importance of the leader for the goal attainment of the organization is ongoing.5 In addition, the leader role in public sector in Norway has traditionally been seen as neither visible nor very strong.5 The Coordination Reform introduces several new responsibilities for the nursing leaders, which further strains their situation and influences their motivation for reaching the goals of the health care service.
SDT6,7 is an organismic dialectical approach to human motivation, emotion, and personality in social contexts. Central to SDT is the postulation of the three basic psychological needs which are needs for autonomy, competence, and relatedness. Specifically, the need for autonomy concerns the feeling of choice making and of being the initiator of one’s own actions. The need for competence refers to the feeling of being effective in one’s interactions with the environment and of experiencing opportunities to both express and exercise one’s capacities. The need for relatedness concerns the feeling of a connection with other individuals and groups.3
Experiencing support of these needs leads to need satisfaction, while need frustration refers to the feeling that arises when the individuals perceive their needs to be undermined.8 Whether the basic needs are satisfied or not has implications for the quality of motivation and work-related outcomes such as goal attainment, competence, and health.6 Studies have shown that a controlling environment leading to frustration of the basic psychological needs undermines intrinsic and autonomous motivation and sets pressure toward specified outcomes.9,10 This is problematic as autonomous motivation is linked to optimal functioning. For example, recent research among employees in four Nordic companies has confirmed that both workplace need support and sufficient available resources are associated with high autonomous work motivation. In turn, the higher the autonomous motivation, the better the health among employees as indicated by low somatization, burnout, and sickness absenteeism scores.11,12 Other researchers indicate that need and resource supporting contexts and autonomous work motivation are important for competence development and goal attainment.6,13
Given the SDT framework, if leaders experience an environment that supports their needs for autonomy, competence, and relatedness, it will: 1) facilitate competence development among leaders and 2) improve the leaders’ health. Conversely, the feeling of need thwarting might lead to negative consequences related to goal attainment and health.
Methods
In order to answer the research question, a qualitative research design has been chosen. Qualitative research is characterized by description, realization, interpretation, or deconstruction of the qualities of human experience.14,15 The qualitative research interview is an appropriate tool for investigating individual experience.15,16 By interviewing nursing leaders from the municipal health care services, we were able to uncover the participants’ own perspectives on their work day, using an emic perspective.14 The goal is to capture the complexity of the services through the study of leadership in its natural context: the municipal health care service in a time of reform. As such, this study contributes to the assembling of theory about leadership within public health care.
Data collection
Data were collected using qualitative, individual interviews with nine municipal health care nursing leaders. The informants were selected due to their role as key personnel and largely responsible for practical interactions in the Coordination Reform. The informants in the study were purposefully and theoretically sampled.17,18 The unit of analysis was the nursing leader selected from six Norwegian municipalities. The goal of theoretical sampling was to choose data sources which were likely to replicate or extend the emergent theory in the field.17 The sample consisted of seven women and two men; five of them were leaders in nursing homes and four in home-care services. The participants represented both smaller and larger municipalities, as well as both rural and urban municipalities. They were all nurses by profession and had between 2 and 12 years of experience as leaders in the health care service. Through the individual qualitative interviews, we gained knowledge about how they experienced their position as nursing leader.
An interview guide was developed using sensitizing concepts19 from theories that together make up the researchers’ pre-established understanding.16 The interview guide emphasized four main topics related to leadership: perceived competence, learning, goal achievement, and the consequences of the Coordination Reform. We used semi-structured interviews in order to allow the informant to express him/herself in his/her own words.16 Memo writing20 was used during the interviews to ensure that these initial impressions would contribute to later interpretations. The interviews were taped and transcribed verbatim. The interviews took place during a period of 3 months. Six interviews were carried out just before implementing the “Collaboration Reform” and three just after. Lasting for about an hour, the interviews took place in the nursing leaders’ workplace.
Data analysis
Data from the interviews consisted of approximately 200 pages of text. Constant Comparative Method, which is a systematic scientific method21,22 suitable for getting an overview of large amounts of data, was chosen as the method of analysis. Our approach complemented the research question by using the theoretical framework developed by Deci and Ryan,6 to a process of deductive thematic analysis, while allowing for themes to emerge directly from the data using inductive coding, as recommended by Fereday and Muir-Cochrane.23
During the first reading of the interviews, important points that captured our interest were highlighted in order to reduce data to a manageable amount and codes providing an overview of the material were identified.21 Following this, the text in each interview was read with particular attention to these codes, while more overriding topics were identified. Through assembling codes, we became aware of patterns in the data.
In order to get a better overview of the categories, an analysis close to the original text that identified connections between units of meaning, subcategories, and categories was conducted. This was organized in a data matrix and the most informative among the informants’ quotes were included. In the phase of selective coding, we repeatedly went through the material in order to uncover the core processes, the main topic of the research, and systematically relate these to the other categories. We developed terms and a model that contributed to a better understanding of the phenomenon under study.21
Ethical considerations
The project has been approved by the Norwegian Data Service for Social Sciences (ethical approval no. 28709). The participants signed an informed consent form. The data are anonymized in the presentations.
Results
The model (Figure 1) that started as an analytical framework, however, turned into a descriptive map that captured the interactions and relations that the nursing leader has with superiors, subordinates, and peers.
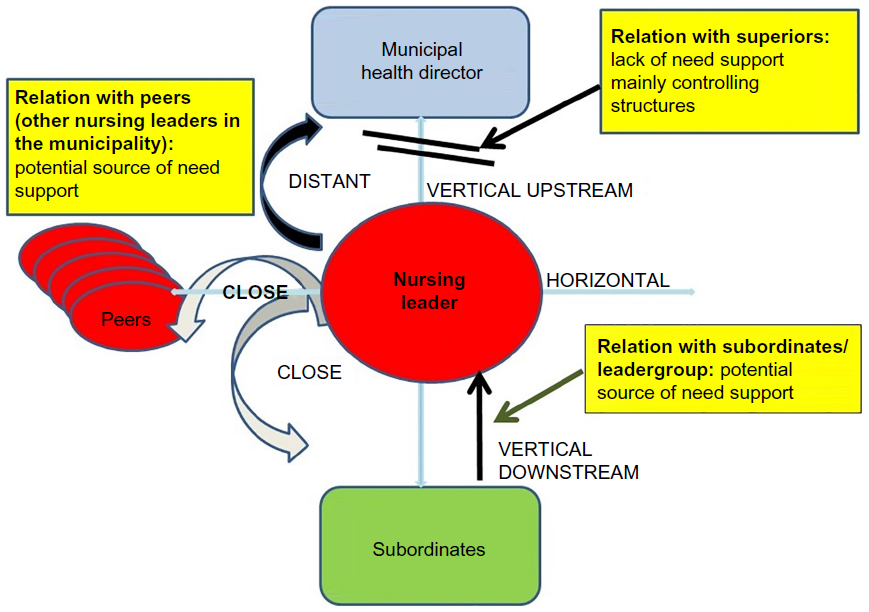 | Figure 1 Managing performance in a squeeze. |
The vertical line illustrates the vertical upstream relation to their superior, who in most cases is the municipal health director, and the vertical downstream relation to their subordinates, which also connects to the patients and the families of the patients. The vertical upstream connection is characterized as distant. The municipal health director is perceived by the nursing leaders as having a focus solely on budgets and pecuniary matters. The relation to subordinates is, on the contrary, characterized as close. Horizontally, there is also a close relation to peers, who are other nursing leaders and sometimes nursing leaders from other fields in the municipality. This horizontal interaction is described as supportive, and the support comes through interaction and collective reflection.
The distance to the subordinates is short physically, cognitively, and professionally. The relation in direction upward to the “manager of the manager”, the municipal health director, remains more fuzzy. The geographic and physical distance is typically long, and the municipal health director has a very wide area of responsibility, including responsibility across other municipal sectors, for example, education.
Table 1 gives an overview of how the data excerpts are categorized as subthemes and themes. The table highlights the relation between the nursing leaders and their superiors and subordinates, in addition to their interaction with peers.
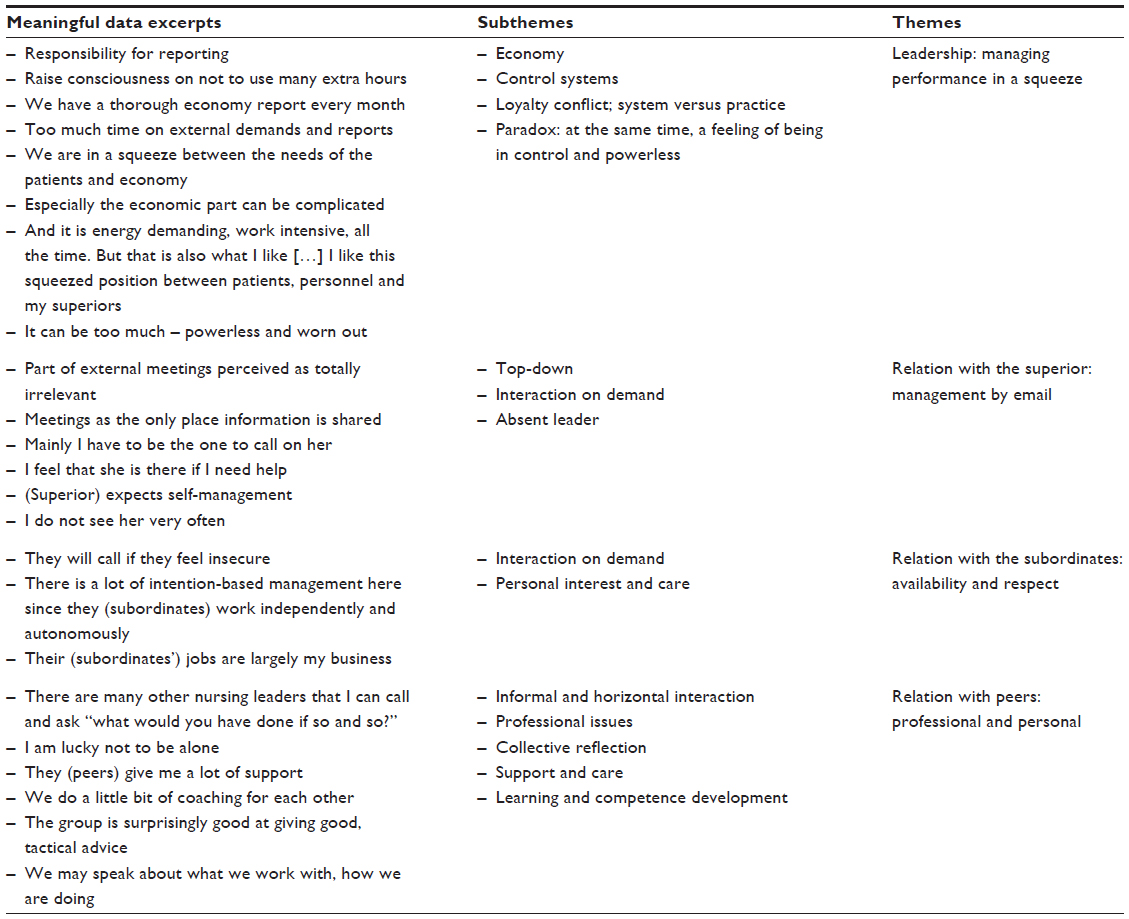 | Table 1 Data excerpts, subthemes, and themes |
Leadership: managing performance in a squeeze
The nursing leader perceives the demands from the municipal health director as pertaining to reporting routines and notifications of irregularities and describes the content of the interaction with the municipal health director: “[…] that’s what life is all about. Yes, money, money.” The nursing leaders use considerable time on their budget-control and economic issues, and one informant said: “[…] I use a lot of time on my subordinates in order to raise their consciousness on not to use many extra hours.” The same informant went on to describe the six objectives she is measured by – connected to the economic measures, for example, beds filled. Another informant confirmed this:
We have a thorough economy report every month. So we have to provide background for all prognosis and numbers in the world. [Informant C]
The informants emphasized the amount of time used on economical and mercantile tasks, for example, in this way:
I unfortunately use way too much time on external […] eh […] demands and reports. [Informant J]
The reporting systems make the municipality more transparent along the indicators that are measured and reported, and this also results in a better knowledge along these dimensions of what is going on in the units, but puts a lot of pressure on the nursing leaders. The nursing leaders’ role and function was expressed in the following way:
We are middle managers. In this way we are in a squeeze between the needs of the patients and economy. Very simple. And all areas are not always compatible, to put it that way. Especially the economic part can be complicated. [Informant A]
The nursing leaders’ background and experience as practicing nurses is considered to be important as a means of understanding her/his subordinates and what is going on in practice. They develop survival techniques in order to live with the stress:
I used to be much more worn out. I have probably acquired some techniques on “well, I cannot fix that right now”. [Informant H]
The nursing leaders are loyal to both their subordinates and superiors. This is a position that they like and perhaps have wanted. As one informant puts it:
And it is energy demanding, work intensive, all the time. But that is also what I like. That is the reason why I have chosen this. And I like having a position close to practice. I would not like to be further up in the system. To have a more superior position. I like this squeezed position between patients, personnel and my superiors […]. But you can experience that it can be too much. And then you can feel simply powerless and worn out. [Informant C]
When asked who looks after you, another informant replied:
That is my husband. [Informant J]
Relation with the superior: management by email
This relation refers to the interaction between the nursing leader and her/his superior, the municipal health director, and was expressed in different ways, for example:
But part of the external meetings, like the health director’s meeting, is perceived as totally irrelevant. [Informant A]
Another informant considers these meetings as opportunities for information sharing and that this is pretty much the only place information is shared (informant C). The emphasis is on transfer of information in a context characterized as “top-down”. One informant said that she meets her superior, the municipal health director, every fortnight in a meeting with 14 other nursing leaders:
So this is nothing personal. If I need to talk to her other than that, then I have to try to get the hold of her on the phone or send an e-mail: “management by outlook”. [Informant J]
The contact is very much based on “interaction on demand”, which was described as:
Mainly I have to be the one to call on her. Because her calendar is even fuller than mine. I do not have the need very often. I feel that she is there if I need help. And if I feel that I need to discuss something I will. And you can also pick up the phone. So I do not see her very often. I don’t. [Informant A]
The expectations from the municipal health director were perceived and described in the following way:
It appears she has an expectation, she just now expressed that, she expects that we are pretty self-managed. Since we have both applied for the position and been appointed. I heard she said that now, since she is also part of the management training. [Informant H]
In the same vein, another nursing leader expressed as follows when asked if she misses contact with her superior:
Sometimes I do. Sometimes it feels a bit sluggish. But when I ask for it, I get it. [Informant H]
The distance to the nursing leader’s superior is considerable, depending, of course, on the size of the municipality geographically and population wise. The contact is limited, and when they meet, it is often in larger meetings and meetings with a strict and full agenda. This relationship between the nursing leader and the municipal health director is characterized by structural frames and control mechanisms exercised by the municipal health director. We have labeled the dilemma that the nursing leader is in the middle of “strong and vulnerable”. This refers to the tension between the apparently confident nursing leader in full control, on one hand, and the vulnerable nursing leader, on the other, restricted by the municipal health director through tight budgeting and top-down demands, and scarce contact with the same.
Relation with subordinates: availability and respect
Interaction on demand seems to apply also to the interaction between the nursing leader and his/her subordinates, that is, within the organization, for example:
The framework for how people function in their jobs is largely my business, and has to be done as optimally as possible in order for them to succeed as often as possible. There is a lot of intention-based management here since they work independently and autonomous. [Informant A]
Also:
Yes, what I think is that they will call if they feel insecure, that they will call the coordinating day-nurse on duty. And ask for support from colleagues […] you have to be competent to know where to ask for help.
Asking colleagues for help, in small and larger matters, seem to be a salient feature of the work environment. [Informant B]
Relation with peers: professional and personal
The nursing leaders made repeated references to meetings with other nursing leaders in the municipality, through ongoing or new projects, and through courses and training programs. This interaction has an aura of informality and care, although the content of the conversations tends to be work related:
Yes, sometimes we go out and have a bite, a Danish or something like that. There are many other nursing leaders that I can call and ask, “What would you have done if so and so?” [Informant J]
When asked about where they get their support, the nursing leader’s immediate response had to do with the horizontal relations to other nursing leaders:
Well I am lucky not to be alone in the position that I have. There are five others who are on the same level, as unit-leaders for home-based services. So they give me a lot of support. [Informant D]
Furthermore, another one said:
[…] we have some other unit-leaders, we do a little bit of coaching for each other. [Informant J]
This relationship is characterized by collective reflection on professional issues and they are also open to discuss specific (although depersonalized) cases:
Yes, in the homecare services-group we can do that. There we can discuss cases […] the group is surprisingly good at giving good, tactical advice. [Informant D]
And a third one said:
Yes, we did a round around the table where we may speak about what we work with, how we are doing, what we are right in the middle of. [Informant E]
The municipalities are apparently aware of the particular need to address leadership issues, in general, and one informant referred to an interdisciplinary network of leaders in the municipality with middle managers from all sectors in the municipality, such as principals, nursing leaders, etc. She said:
This is not, however, where I take out my frustrations. [Informant F]
They have tried to create a professional and narrow arena of leaders at the same level in the organization. This is, however, not prioritized by its potential members and the informant said it makes her feel alone at times. The nursing leaders find the interaction with peers from the health care field useful, but this is not the case with the interdisciplinary gatherings.
Discussion
Our main findings regarding descriptions of the nursing leaders’ role and interactions can be categorized as managing performance in a squeeze, and relations with superiors, with subordinates, and with peers (see Figure 1). The leaders have a vertical relation upstream with their superiors, vertically downstream with their subordinates, the patients and their relatives, and horizontally through interaction with their team of leaders and with peers. These work-related interactions are potential sources of satisfaction of the basic psychological needs, that is, autonomy, competence, and relatedness for the nursing leaders. These sources, however, comply only to a certain extent with the psychological needs. This is discussed subsequently.
Controlling structures
The relation with the superior is scarce and to a high degree characterized by controlling mechanisms like focus on budgets. These mechanisms are extensive and are at the core of the operations and services, since they are almost solely connected to pecuniary issues. In addition, the pressure for specific and new outcomes represented by the new reform seems to challenge the nursing leaders in terms of the extreme focus on efficiency to perform advanced tasks, support and educate the staff, as well as keep within the budget frames. Furthermore, the relation is characterized by ad hoc interaction and interaction on demand. The distance to their superior (municipal health director) is long geographically, but is also perceived as long due to the scarce contact and the character of the relation. It is more a lack of support than thwarting from their superior – an empty space above the nursing leader. On the other hand, the municipal structure itself can be characterized as controlling due to the character of the relation between the health director and the nursing leaders, which almost solely concerns keeping the budgets and cuts in budgets. This appears to lead to need thwarting, which, in turn, might limit the nursing leaders’ experience of being autonomous. However, the nursing leaders’ superiors may not be the only sources of need satisfaction. Subsequently, we discuss how support from peers and subordinates can be relevant for the nursing leaders’ need satisfaction.
Admiration from the subordinates and support from peers
Interaction between the nursing leader and subordinates brings together heterogeneous actors in terms of occupations, positions in the hierarchy, departmental affiliation, and so on. The relation is characterized by supervision and care on the nursing leader’s part, but the nursing leader also expressed that interaction with subordinates represents a “home” for her. This interaction is frequent, and is similar to what Grill et al24 found in a study of the use of dialogue for first-line leaders. This frequent interaction strongly contrasts the lack of interaction that the nursing leader has with the municipal health director. We suggest that the support they receive from the subordinates may give the nursing leaders a feeling of being competent and related at work. This is supported by studies by Vie25 and Tengblad,26 who asserted that managers spend more time than before with their subordinates.
Furthermore, the contact and interaction they have with their peers, here the nursing leaders in other health care services and institutions in the municipality, is perceived to substitute the lack of contact with their superiors. This interaction and peer support, where the nursing leaders learn together and share personal and professional experiences, resembles “peer group supervision”.27,28 Even if they are in separate physical spaces during the work day, they feel close to their peers and this interaction appears to fill the need for relatedness.3 Furthermore, it contributes to satisfy the need for competence and partly for autonomy, since the nursing leaders have overlapping knowledge29 and they give each other support in their role as managers, as illustrated in Figure 1.
Based on this discussion, the relation the nursing leaders have with their subordinates and peers tends to make them feel that they can manage without the support from above. However, although the nursing leaders have support through this relation with peers, they might feel their autonomy thwarted, as discussed above in the “Controlling structures” section. This autonomy thwarting might be impossible for peers to relieve. This leaves the nursing leader strong in one sense, but vulnerable in another.
Stuck between a rock and a hard place
Based on our findings, we assert that autonomy support from subordinates and peers cannot fully compensate for lack of support from a higher organizational level, the municipal health director. Although one study has shown that autonomy support from a higher organizational level compensated for the lack of autonomy support from a lower organizational level,30 our findings do not indicate support for the opposite in the context of our study.
At work, one is always tied to some structural guidelines based on the hierarchy that the organization represents, and peers are not able to give the same permissions, and so on as a boss. This may be particularly salient for the nursing leaders in this study, who are tied to budget in almost everything they do. As such, based on this definition of managerial autonomy support, horizontal support may not be sufficient in terms of satisfying all the three basic needs. For the municipal health care service, our findings suggest that the need for autonomy is thwarted, or at least not satisfied. This does not necessarily stem from the management style of the superiors, but rather from the organizational structure and the character of the relationship, which hinder communication and diminish the opportunity to perform one’s task autonomously. When the support from superiors consists more or less solely of controlling structures, the way our data show, this will influence the quality of motivation of the nursing leaders negatively. Specifically, thwarting of autonomy from their leaders may reduce autonomous motivation, and as SDT contends, the satisfaction of the need for autonomy ultimately determines the quality of one’s motivation.31 This may, in turn, lead to health consequences such as burnout, somatization, and absenteeism, and result in sick leave or turnover.12
Furthermore, goal attainment may be affected negatively,13 which is unfortunate for the municipality and the aims of the new reform. Especially when the need for autonomy is thwarted, the nursing leaders may not perceive that they have the ability or the resources needed to obtain their goals, and will find themselves stuck between a rock and a hard place. The reason why the nursing leaders still continue in their positions may be that they are used to not being supported. However, our data imply that this is not a situation that they regard as positive.
Although this study is based on a qualitative design and we cannot generalize from this data, there is reason to believe that these results are transferable to other contexts, for example, to educational contexts on different levels. These issues would benefit from being studied using a larger sample.
Conclusion
The relation between the nursing leader and their superiors is characterized by controlling structures and lack of autonomy support. The nursing leader’s relations with subordinates and, in particular, with peers contribute to support their needs for competence and relatedness, and, to some extent, autonomy. However, this cannot substitute for the lack of support from the superior level. Even though autonomy support can be obtained by peers in, for example, personal relationships, the work context may operate differently. In light of the SDT framework, it appears that the horizontal interaction with peers and downstream with subordinates contributes to fulfill the need for competence and relatedness. Findings indicate that lack of leader support will fail to fulfill the need for autonomy for the nursing leaders.
Implications for practice
Based on the findings from this study, we suggest routines for one-to-one interaction between superior and the nursing leader. There is a missing link upward between the nursing leader and the “leader of the leader”, and structural measures can be taken in order to improve this interaction and, hence, the support. This is also a political issue on the municipal level as to the design of the municipal health care organization. Furthermore, we suggest increased consciousness on the value of the horizontal support and interaction that the nursing leaders find useful, both inter- and intraorganizationally. Fragmented organizations, like municipalities, could benefit from facilitation of horizontal interaction.
Disclosure
The authors report no conflicts of interest in this work.
References
The Norwegian Ministry of Health and Care Services. Meld. St. nr. 47 (2008–2009) Samhandlingsreformen [Report to the Storting (White Paper). Coordination reform]. Oslo: Norwegian Ministry of Health and Care Services; 2009. | |
Vabø M. Home care in transition: The complex dynamic of competing drivers of change in Norway. J Health Organ Manag. 2009; 23(3):346–358. | |
Deci EL, Ryan RM. Handbook of Self-Determination Research. Rochester: University of Rochester Press; 2002. | |
McNulty T. Reengineering as knowledge management – A case of change in UK healthcare. Manage Learn. 2002;33(4):439–458. | |
Lotsberg DØ. Ledelsesteori – hva slags ledere passer i kommunene [Management theory – what type of managers are suitable for the municipalities]? In: Baldersheim H, Rose L, editors. Det kommunale laboratorium. Teoretiske perspektiver på lokal politikk og organisering [The municipal laboratory. Theoretical perspectives on local politics and organizing]. Bergen: Fagbokforlaget; 2000:137–161. Norwegian. | |
Deci EL, Ryan RM. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. | |
Deci EL, Ryan RM. Intrinsic Motivation and Self-Determination in Human Behavior. New York: Plenum Press; 1985. | |
Bartholomew K, Ntoumanis N, Ryan R, Thøgersen-Ntoumani C. Psychological need thwarting in the sport context: assessing the darker side of athletic experience. J Sport Exerc Psychol. 2011;33(1):75–102. | |
Deci EL. Effects of externally mediated rewards on intrinsic motivation. J Pers Soc Psychol. 1971;18:105–115. | |
Deci EL, Betley G, Kahle J, Abrams L, Porac J. When trying to win. Pers Soc Psychol Bull. 1981;7:79–83. | |
Olafsen A, Westbye C. R-MAWS in Norwegian[Master]. Hønefoss: Department of Business and Strategy, Buskerud University College; 2010. | |
Williams GC, Halvari H, Niemiec CP, Sørebø Ø, Olafsen AH, Westbye C. Managerial support for basic psychological needs, somatic symptom burden and work-related correlates: A self-determination theory perspective. Work Stress. 2014;28(4):404–419. | |
Sheldon KM, Elliot AJ. Goal striving, need satisfaction, and longitudinal well-being: the self-concordance model J Pers Soc Psychol. 1999;76(3):482–497. | |
Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. Los Angeles, Calif: SAGE; 2014. | |
Brinkmann S, Tanggaard L. Kvalitative metoder. Empiri og teoriutvikling [Qualitative methods. Empirical data and theory development]. Oslo: Gyldendal Norsk Forlag; 2012. Norwegian. | |
Kvale S, Brinkmann S. Det kvalitative forskningsintervjuet [The qualitative research interview]. 2. utgave. Oslo: Gyldendal Akademisk; 2009. Norwegian. | |
Eisenhardt KM. Building theories from case study research. Acad. Manage. Rev. 1989;14(4):532–550. | |
Miles MB, Huberman AM, Saldaña J. Qualitative Data analysis: A Methods Sourcebook. Los Angeles: Sage; 2014. | |
Charmaz K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. London: Sage; 2006. | |
Glaser BG. Theoretical Sensitivity. Mill Valley, Calif.: Sociology Press; 1978. | |
Corbin J, Strauss A. Basics of Qualitative Research. Techniques and Procedures for Developing Grounded Theory 3rd edition. Calif: Sage Publications Inc.; 2007. | |
Guvå G, Hylander I. Grounded theory. Et teorigenererende forskningsperspektiv [Grounded theory. A Theory Generating Research Perspective]. København: Hans Reitzels forlag; 2005. Norwegian. | |
Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):80–92. | |
Grill C, Ahlborg G, Lindgren EC. Valuation and handling of dialogue in leadership. A grounded theory study in Swedish hospitals. J Health Organ Manag. 2011;25(1):34–54. | |
Vie OE. Have post-bureaucratic changes occurred in managerial work? Eur Manag J. 2010;28(3):182–194. | |
Tengblad S. Is there a ‘new managerial work’? a comparison with Henry Mintzberg’s Classic Study 30 years later. J Manage Stud. 2006;43(7):1437–1461. | |
Kuipers P, Pager S, Bell K, Hall F, Kendall M. Do structured arrangements for multidisciplinary peer group supervision make a difference for allied health professional outcomes? J Multidiscip Healthc. 2013; 6:391–397. | |
Ducat WH, Kumar S. A systematic review of professional supervision experiences and effects for allied health practitioners working in non-metropolitan health care settings. J Multidiscip Healthc. 2015;8:397–407. | |
Nonaka I. A dynamic theory of organizational knowledge creation. Organ Sci. 1994;5(1):14–37. | |
Liu D, Chen X-P, Yao X. From autonomy to creativity: a multilevel investigation of the mediating role of harmonious passion. J Appl Psychol. 2011;96(2):294–309. | |
Gagné M, Deci EL. Self-determination theory and work motivation. J Organ Behav. 2005;26(4):331–362. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.