Back to Journals » International Journal of Nanomedicine » Volume 21
Strontium-Functionalized Biomaterials for Bone Regeneration: Mechanisms, Biological Functions, and Clinical Translational Progress
Authors Ning F, Wang X, Pan P, Liu W, Yan G, Wang X
Received 23 March 2026
Accepted for publication 7 June 2026
Published 18 June 2026 Volume 2026:21 611430
DOI https://doi.org/10.2147/IJN.S611430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jie Huang
Fengting Ning,1,* Xue Wang,2 Peng Pan,3 Wentao Liu,3,* Guangqi Yan,1 Xi Wang4
1Department of Oral and Maxillofacial Surgery, School of Stomatology, China Medical University, Liaoning Provincial Key Laboratory of Oral Diseases, Shenyang, People’s Republic of China; 2Department of Orthodontics, School of Stomatology, China Medical University, Liaoning Provincial Key Laboratory of Oral Diseases, Shenyang, People’s Republic of China; 3Shenyang National Laboratory for Materials Science, Institute of Metal Research, Chinese Academy of Sciences, Shenyang, People’s Republic of China; 4Department of Emergency and Oral Medicine, School and Hospital of Stomatology, China Medical University, Liaoning Provincial Key Laboratory of Oral Diseases, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xi Wang, Email [email protected] Guangqi Yan, Email [email protected]
Abstract: Strontium (Sr), a trace element with osteogenic, anti-resorptive, immunomodulatory, angiogenic, and antibacterial activities, has become an important functional component in biomaterials for bone regeneration. This review systematically summarizes Sr-functionalized biomaterials, with emphasis on Sr2⁺-mediated molecular mechanisms, concentration-dependent bioactivity, local delivery strategies, fabrication-dependent ion-release behavior, antimicrobial and antioxidant functions, and clinical translational potential. Particular attention is given to the physicochemical regulation of Sr incorporation, therapeutic-ion synergy, fabrication-related release characteristics, and key challenges affecting translational application. In addition, we discuss how Sr cooperates with other therapeutic ions, including Mg, Zn, Cu, Se, and Ga, to coordinate osteogenesis, angiogenesis, immunomodulation, and infection control within the bone-regeneration microenvironment. Current limitations include the lack of unified optimal Sr dosing across different material platforms, insufficient long-term release and biosafety data, limited large-animal and clinical evidence, and an incomplete understanding of Sr-associated antimicrobial mechanisms. Overall, this review provides mechanistic insights and practical guidance for the rational design of next-generation Sr-functionalized bone-repair biomaterials. The infographic outlines Sr²⁺ benefits across fields. In osteogenesis, it aids bone formation and cell differentiation. For angiogenesis, it enhances bone regeneration via VEGF and HIF-1α. Its antimicrobial effects reduce bacterial adhesion and biofilm formation, while increasing membrane disruption and ROS. Immune modulation includes macrophage M2 polarization and cytokine regulation, improving osteoimmune conditions. As an antioxidant, Sr²⁺ lowers ROS, oxidative stress, lipid peroxidation and DNA damage, restoring redox balance. Clinical uses include Sr-doped scaffolds, hydrogels, implant coatings and bone cements, enhancing biocompatibility. It works with ions like Mg²⁺, Zn²⁺, Cu²⁺, Se²⁻ and Ga³⁺. Sr²⁺ shows potential in treating osteoporosis, repairing bone defects, enhancing implants, regenerating infected tissues and personalizing tissue engineering.Sr² benefits: bone growth, blood vessels, antimicrobial, immune boost, antioxidant, biomaterials.
Keywords: strontium, osteoimmunomodulation, concentration-dependent bioactivity, local ion delivery, antibacterial bone regeneration, strontium-functionalized biomaterials
Introduction
Bone, as a key component of the human body, plays an indispensable role in life activities. The abundant cellular components in bones enable their self-repair and structural remodeling.1 When the balance between bone formation and bone resorption is disrupted, it leads to bone loss and degradation of the bone microarchitecture, eventually resulting in the development of systemic osteoporosis—a common and challenging bone disease worldwide.2 Data indicate that over 500 million people globally suffer from osteoarthritis (OA), and 43.5% of these patients typically experience limited joint movement due to the condition. According to the Global Burden of Disease Study (GBD) data from the U.S. Institute for Health Metrics and Evaluation (IHME), the prevalence of OA in the United States accounts for 10.5% of the total population, and this proportion increases significantly with age.3 Beyond inflammation, bone infections are often accompanied by bone loss. Common pathogens include Staphylococcus aureus (S. aureus), Streptococcus pneumoniae, and Escherichia coli (E. coli). Among these, S. aureus constitutes over 70% of the pathogenic flora due to its strong invasiveness, colonization ability, and proliferative capacity.4 For bone defects induced by chronic infections, conventional therapies often fail to achieve satisfactory outcomes. Another common issue affecting bone health is malignant tumors, such as bone cancer;5 additionally, oral and maxillofacial surgeries may cause severe bone defects.6 To repair bone defects larger than the critical size, autologous bone transplantation or bone graft substitutes are usually required.1,2 Therefore, a key challenge in bone tissue engineering (BTE) is to develop biodegradable bone substitutes with appropriate mechanical and biological properties, as well as anti-inflammatory and antibacterial effects.7
Strontium ranelate (SrR), a unique anti-osteoporotic drug, has been effectively used for the prevention and treatment of osteoporosis in postmenopausal women.8–10 Given the therapeutic efficacy of SrR in osteoporosis management, this has sparked growing interest in the application of Sr2⁺ in bone therapy.11 Sr2⁺ exhibits a marked tropism for bone tissues and possesses bidirectional regulatory properties: it activates osteoblastic bone matrix synthesis while inhibiting osteoclastic resorption. Additionally, it exerts antibacterial activity and promotes neovascularization—collectively facilitating bone regeneration.12–14 However, studies have shown that the oral absorption efficiency of Sr2⁺ is suboptimal, and concurrent calcium (Ca) intake or calcium-rich diets further impair its pharmacokinetic performance.10,15
Consequently, bone engineering strategies advocate the implantation of resorbable Sr2⁺-loaded matrices to achieve controlled ion release for bone defect repair. Recent advances have enabled the integration of Sr2⁺ into various orthopedic biomaterials, including titanium-based prostheses, orthopedic cements, bioglass composites, collagen matrices, regenerative scaffolds, and therapeutic release systems.16–20 The implantation of biomaterials triggers a cascade of immune responses through protein adsorption, involving macrophage phenotypic polarization and the dynamic regulation of cytokines (collectively referred to as the foreign body reaction, FBR).21 Bone integration is essentially a dynamic bone repair process regulated by the reprogramming of the immune microenvironment.22,23 Various cells in the bone immune microenvironment interact with bone marrow mesenchymal stem cells (BMSCs), continuously remodeling bone to maintain its mechanical strength and structural integrity.24,25 As the core cells of bone immunity, macrophages are crucial for organ development and inflammatory homeostasis, and their phenotypes and functions can be modulated by factors such as Sr2⁺.24 Modulating macrophage phenotypic polarization to ameliorate inflammatory conditions represents a promising therapeutic strategy for disease management.26,27
During bone remodeling, angiogenesis and bone formation are closely coupled.26 Vascularization of bone repair materials is also a key issue to be addressed in the bone repair process.27 In the early stage of angiogenesis, macrophages can exert vasculotrophic effects through physical contact and the secretion of potent angiogenic factors.28 Mesenchymal stem cells (MSCs) and immune cells also participate in important intercellular communication,29 guiding the host response and regulating the immune microenvironment.30
Although research on strontium-containing biomaterials for bone repair has been increasing, existing reviews still lack systematic integration of the intrinsic relationships among material design, ion release behavior, biological mechanisms, and clinical translation. Sr2⁺ can improve the physicochemical properties of biomaterials in a concentration-dependent manner and simultaneously regulate key processes of bone regeneration, including osteogenic differentiation, osteoclast inhibition, immune microenvironment modulation, and angiogenesis.31–33 Therefore, dose optimization, release regulation, and translational application of Sr-based materials have become important research directions. Previous reviews have mainly focused on strontium-containing bioactive glasses, Sr-related osteoimmunomodulation, or the general progress of recent Sr-functionalized materials, whereas the associations between material composition and fabrication methods, Sr2⁺ release, cellular behavior, and bone repair outcomes remain relatively underexplored. Based on this, this review systematically summarizes the dual regulatory mechanisms, concentration-dependent bioactivity, antibacterial properties, and clinical translational potential of Sr2⁺ in bone regeneration from an integrated perspective. In addition, by incorporating recent advances, this review further includes representative emerging materials such as Sr/Mg co-doped scaffolds, injectable Sr-based hydrogels, and Sr-based nanodelivery systems, aiming to further illustrate the developmental trends of Sr-functionalized bone repair materials in multi-ion synergy, local delivery, and precise regulation, and to provide references for the rational design and translational application of next-generation Sr-functionalized bone repair biomaterials.
Effect of Sr Incorporation on the Physicochemical Properties and Biological Performance of Bone Restorative Materials
Effect of Sr Incorporation on Crystal Structure, Physicochemical Properties, and Degradation Behavior
As a mineral, Sr2⁺ is absorbed in the body similarly to calcium ions (Ca2⁺). In Ca-based bioceramics, Sr2⁺ has been widely used as a substitute for Ca2⁺. Because the ionic radius of Sr2⁺ (118 pm) is larger than that of Ca2⁺ (99 pm), the substitution of Ca2⁺ by Sr2⁺ disrupts the structural arrangement and symmetry of the hydroxyapatite (HA) lattice, induces lattice strain, and expands the HA unit cell size.34,35 X-ray diffraction (XRD) analyses demonstrated that increasing Sr2⁺ incorporation in HA reduced crystallinity and broadened the characteristic diffraction peaks with a shift toward lower angles, indicating the successful incorporation of Sr2⁺ into the HA crystal structure. Moreover, the Sr2⁺ doping amount may be a dominant factor affecting crystal size.31 In contrast, replacing larger-radius Ba2⁺ with smaller-radius Sr2⁺ results in unit cell shrinkage and reduced particle size.36 Additionally, because Sr2⁺ possesses lower electronegativity (0.95) than Ca2⁺ (1.0), Sr2⁺ incorporation can alter the surface charge of HA and increase its positive surface potential.34
The lattice distortion and reduced crystallinity induced by Sr2⁺ further influence the degradation behavior of biomaterials. Sr2⁺ substitution decreases the crystallinity of Ca-based bioceramics, thereby accelerating degradation and increasing ion release, which may contribute to enhanced material bioactivity.37 In apatite structures, Sr2⁺ substitution for Ca2⁺ also promotes phosphate degradation, potentially generating an ion-rich microenvironment favorable for bone formation.38 In hydrogel systems, increasing Sr2⁺ concentration improves structural stability and lowers the swelling rate during the early swelling stage, likely due to the increased cross-linking density caused by the chelation reaction between -COOH groups and Sr2⁺.39
In addition, Sr2⁺ significantly affects the phase stability of calcium phosphate materials. Tovani et al developed a bioinspired physical confinement strategy for fabricating Sr-doped apatite [Sr(CaP)] nanotubes. In the absence of Sr2⁺, poorly crystalline apatite resembling bone mineral preferentially nucleated within the pores of polymeric membranes. However, introducing 10% Sr2⁺ induced lattice distortion in the apatite crystalline framework and caused broadened diffraction bands in XRD patterns.38 Another study demonstrated that the biomimetic precipitation of Sr-doped amorphous calcium phosphate (Sr-ACP) in homogeneous media initiated only when 25% of Ca2⁺ in the apatite lattice was substituted by Sr2⁺. Furthermore, the amorphous phase remained stable only at higher Sr2⁺ substitution levels, such as 50% and 75%.38 Xu et al further showed that incorporating 2.5 wt% Sr2⁺ into the ACP framework prolonged the persistence of the amorphous state under dehydrated conditions for at least 3.5 years. Compared with pure ACP, Sr-ACP may serve as a more favorable component for medical devices with enhanced bone repair potential.40
Regulation of Osteogenesis and Biomineralization by Sr Concentration
The biological effects of Sr2⁺ on bone restorative materials exhibit a clear concentration-dependent manner. Appropriate Sr2⁺ release can generate an ion-rich microenvironment favorable for bone formation and promote osteogenic cellular responses. However, excessive Sr2⁺ concentrations may negatively affect both material stability and osteogenesis. For example, incorporating 50% Sr2⁺ may destabilize the apatite lattice structure, distort crystal symmetry, and impair osteogenesis.41
Studies on amorphous strontium calcium phosphate (Sr-Ca-ACP) particles with low Sr2⁺ content identified 10% as a relatively optimal proportion of Sr2⁺ for bone tissue application.38 Increasing Sr2⁺ content from 10% to 50% destabilized collagen assembly, hindered the crystallization of bone apatite-like platelets, and generated Sr2⁺-enriched micrometer-sized ACP particles within collagen scaffolds. These changes disrupted the typical three-dimensional bone structure and impaired preosteoblast adhesion.42 At a concentration of 10 mol% Sr2⁺, the absorption peaks associated with the vibrational modes of OH− groups in HA disappeared, which was likely caused by structural distortion induced by the larger Sr2⁺ ions.31
Notably, HA composites containing 10 mol% Sr substitution exhibited biomechanical properties similar to those of natural bone and supported bone formation, vascularization, and osseointegration in a sheep model of severe bone defects.43 These findings further demonstrated that 10% Sr2⁺-enriched scaffolds possess considerable efficacy in stimulating the osteogenic differentiation of mesenchymal stem cells (MSCs) (Figure 1).44 Therefore, higher Sr2⁺ incorporation is not necessarily associated with superior osteogenic performance, and maintaining a balance between structural stability and osteogenic bioactivity is essential (Table 1).
 |
Figure 1 Effect of Sr2⁺ substitution for Ca2⁺ on the physicochemical and biological properties of biomaterials. Sr2⁺ substitution within hydroxyapatite alters crystallinity, crystalline phase stability, ion release behavior, surface positive charge, unit cell size, and degradability. Upward arrows indicate enhancement or increase, whereas downward arrows indicate reduction or decrease following Sr2⁺ incorporation. |
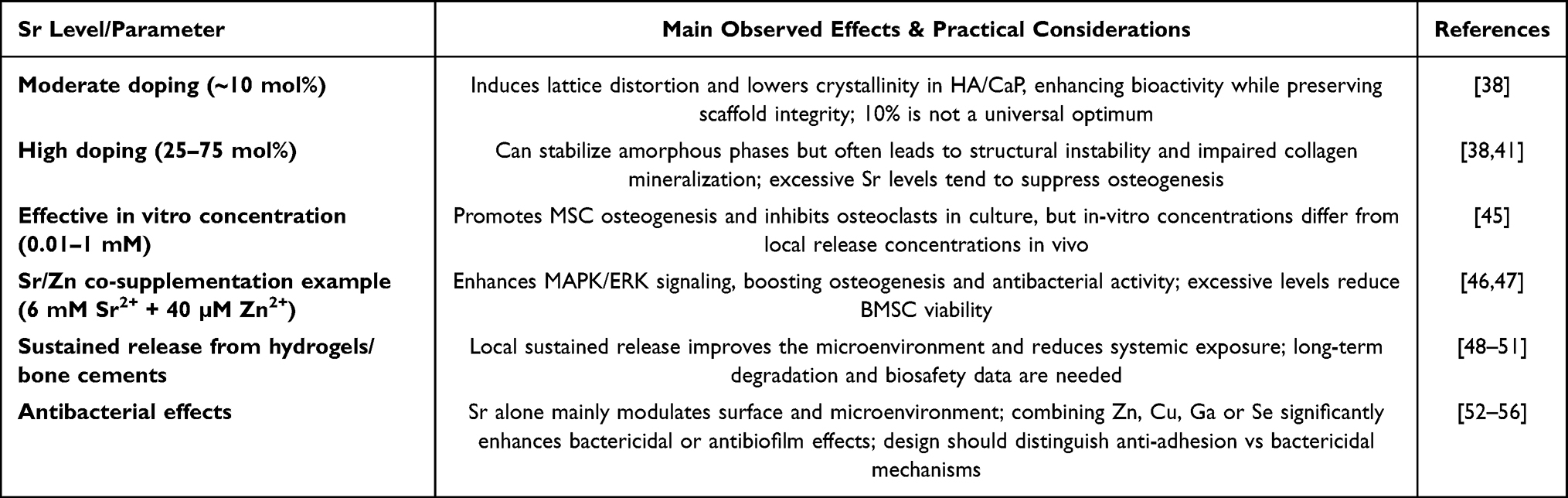 |
Table 1 Effects of Sr Dose, Incorporation Level, and Release Behavior on Physicochemical Properties and Biological Responses |
Design Strategies and Clinical Translation of Sr-Based Composite Biomaterials
Compared with other therapeutic ions, Sr is characterized by its dual regulatory effects on bone metabolism, including promotion of osteoblast-lineage activity and suppression of osteoclast-mediated bone resorption. In contrast, Mg mainly contributes to mineral metabolism, degradation regulation, and angiogenesis;57 Zn is closely associated with antibacterial activity and osteogenic enzyme regulation;46 Cu exhibits prominent angiogenic and antibacterial properties but requires careful cytotoxicity control;58 while Se and Ga are commonly introduced to enhance antimicrobial or antitumor functions.59,60 Therefore, Sr is particularly suitable as a core osteoimmunomodulatory ion, whereas Mg, Zn, Cu, Se, or Ga may be combined with Sr to compensate for the limitations of single-ion systems.
In strontium-based composite biomaterials, the focus of multi-ion design is not to simply increase the total ion loading, but to align the release profiles of Sr2⁺ and other functional ions with different stages of bone healing.61 Early-stage release may emphasize anti-inflammatory and antibacterial effects, intermediate-stage release may promote angiogenesis, and late-stage release may sustain osteogenesis and bone remodeling, thereby enabling complementary effects between Sr2⁺ and ions such as Mg, Zn, Cu, Se, or Ga. Meanwhile, fabrication techniques directly determine the distribution, release behavior, degradation profile, and mechanical performance of Sr2⁺.62 Ion substitution within calcium phosphate or HA lattices can achieve stable Sr2⁺ incorporation, although it may affect crystallinity and phase stability.38 Sol–gel methods and mesoporous bioactive glasses are advantageous for regulating ion release, but require precise control of pore structure and dissolution kinetics.63 Ti and PEEK surface coatings are suitable for enhancing local Sr2⁺ activity at the bone–implant interface, whereas 3D printing, injectable hydrogels, and bone cements are more appropriate for individualized bone defects, spatial multi-ion distribution, and minimally invasive delivery, respectively.48–50 Therefore, the fabrication strategy of strontium-based biomaterials should be selected according to defect morphology, load-bearing requirements, degradation period, and infection risk (Table 2).
 |
Table 2 Therapeutic Ions Combined with Sr in Bone-Regenerative Composites |
Osteogenic Functions and Mechanisms of Sr2⁺
Sr2+ Can Be Directly Involved in Bone Regeneration and Its Regulatory Mechanisms
Ca is the fundamental element composing the mineral component of bone, and Sr2⁺ share similar chemical and physical properties as well as ionic size with Ca2⁺.64 Sr2⁺ can substitute for Ca in hydroxyapatite, endowing bone graft substitutes with excellent osteogenic capabilities and upregulating the expression of osteogenic-related genes such as RUNX2 (runt-related transcription factor 2), Osterix, alkaline phosphatase (ALP), and collagen type 1 (COL-1).65–67 Sr-coated biomaterials have been widely applied due to their superior tissue integration ability and osteogenic effects; various Sr-coated materials enhance the expression of osteogenic markers, including bone morphogenetic protein-2 (BMP2), osteocalcin (OCN), osteopontin (OPN), osteoprotegerin (OPG), osteoblast-specific transcription factor (OSX, also known as Osterix), ALP, RUNX2, and COL-1. This promotes the differentiation of osteogenic genes in bone defect regions and stimulates bone formation.48–50,63–67
The differentiation of MSCs into other cell lineages is precisely regulated by signaling pathways,68–70 and Sr2⁺ acts as one of the key factors governing this differentiation process.10 During bone remodeling, Sr2⁺ uniquely exerts both catabolic and anabolic effects by inducing prostaglandin (PG) synthesis and cyclooxygenase (COX) expression, thereby promoting the differentiation of MSCs into osteoblasts.13 Sr2⁺ helps maintain more cells in the cell cycle by increasing the proportions of S-phase and G2/M-phase cell populations. It also regulates the asymmetric stem cell division (ACD) of the Par complex via activating the atypical Wnt5a signaling pathway, and promotes bone formation by inducing the asymmetric distribution of Par3 and aPKC (atypical protein kinase C).71 The activation of the Wnt signaling pathway requires Wnt ligands to bind to Frizzled (FZD) receptors and cooperate with co-receptors LRP5/6 to initiate downstream signaling events.72 Sr2⁺ enhances the phosphorylation of glycogen synthase kinase-3β (GSK-3β), which in turn inhibits its enzymatic activity and stabilizes β-catenin.49,73,74 This stabilization facilitates the translocation of β-catenin into the nucleus, where it binds to T-cell factor/lymphoid enhancer factor (TCF/LEF) transcription factors, activating downstream genes such as c-myc and osteogenic markers.72
Cui et al demonstrated that Sr2⁺ promotes the osteoblastic differentiation of human bone marrow mesenchymal stromal cells (hBMSCs) via the Wnt/β-catenin pathway, as evidenced by the increased expression of signaling components including Axin-2 and β-catenin.49,73,74 Furthermore, Sr2⁺ stimulates the expression of c-myc, a β-catenin-dependent transcriptional target, which reinforces osteogenic signaling.49,73,74 Mechanistically, Sr2⁺ interacts with the calcium-sensing receptor (CaR) on the cell membrane, thereby upregulating the expression of osteogenic transcription factors such as RUNX2, ALP, and OPN, and promoting the proliferation and differentiation of MSCs (Figure 2).75 Additionally, Sr2⁺ promotes the proliferation and osteogenic differentiation of MSCs; it also enables treated human osteosarcoma cells (MG-63) to acquire mature cellular functions via the canonical Wnt signaling pathway, regulating cell proliferation, migration, and growth.76
 |
Figure 2 Schematics of nHA/CS@PDA-Sr.75 (A) Schematic overview of the synthesis of nHA/CS@PDA-Sr and bone defect repair. (B) Sustained release of Sr2+ from nHA/CS@PDA-Sr promotes mesenchymal stem cell osteogenesis and endothelial cell angiogenesis. Arrows in the figure indicate activation, promotion, release, differentiation, migration, or process direction. |
Peroxisome proliferator-activated receptor-γ (PPAR-γ) acts as the master regulator of adipogenesis.10,71 This process is also regulated by a series of transcription factors, including CCAAT/enhancer-binding proteins (C/EBPs), signal transducers and activators of transcription (STATs), and adipocyte determinant and differentiation-dependent factor 1/sterol regulatory element-binding protein 1c (ADD1/SREBP1c).77 Some researchers have proposed that knockdown of the adhesion molecule CDH2 in MSCs leads to increased mRNA expression of DLX5, SP7, and ALP, along with decreased PPAR-γ expression—this in turn reduces cell viability and concurrently impairs osteogenic differentiation.49
Sr2⁺ acts as a pivotal modulator of MSC differentiation, mediating the downregulation of PPARγ2 to attenuate adipogenesis while directing cellular commitment toward osteoblastic phenotypes.10 Aimaiti et al demonstrated that Sr2⁺ can reactivate the extracellular signal-regulated kinase (ERK) signaling pathway to antagonize the inhibitory effect of dexamethasone (DEX) on osteogenesis, enhance ERK phosphorylation, and thereby inhibit adipogenesis by downregulating the expression levels of PPAR-γ and adipocyte fatty acid-binding protein (aP2), ultimately promoting osteogenic differentiation and matrix mineralization.78 The molecular target of Sr2⁺ may be located between signal transducer and activator of transcription 3 (STAT3) and PPAR-γ; it significantly reduces the protein expression levels of PPAR-γ and STAT1 in BMSCs.77
Most scholars believe that Sr2⁺ promotes osteogenesis by regulating the differentiation direction of MSCs or precursor cells, rather than acting on already differentiated adipocytes. Ataie et al also confirmed this, showing that Sr2⁺ significantly upregulates the expression of osteogenic genes (RUNX2 and OCN) in human adipose-derived stem cells (hADSCs).79
Shimizu et al demonstrated that the surface micro/nanostructure of implants promotes cell adhesion and enables the sustained release of Sr2⁺ from the coating.80 This stimulated cellular adhesion results in enhanced expression of integrin β, coordination of intrinsic signaling pathways, and activation of the FAK/MAPK and PI3K/Akt signaling cascades.80 Activation of the FAK/MAPK cascade increases the phosphorylation levels of FAK, ERK1/2, and p38 in BMSCs.76,81 FAK, an intracellular non-receptor tyrosine kinase, plays a pivotal role in adhesion-mediated signaling mechanisms.82
Sr2⁺ can activate integrins, which in turn block the activity of glycogen synthase kinase 3 (GSK3) via the CaSR/PI3K/Akt signaling pathway, thereby enhancing nuclear transcription.83 Researchers exposed MC3T3-E1 cells to ion release extracts from SrHPO4-coated JDBM (Mg-Nd-Zn-Zr alloy), which significantly increased the expression of PI3K and phosphorylated Akt (at Ser 473 and Thr 308) in the cells.84 Treatment with a TLR4 inhibitor (CLI-095) resulted in a significant decrease in these protein levels, highlighting the TLR4/PI3K/Akt signaling pathway as a potential mechanism regulating the osteogenic response (Figure 3).84
 |
Figure 3 Osteogenic effects of SrHPO4-coated JDBM extracts on MC3T3-E1 cells via the TLR4/PI3K/Akt signaling pathway.84 (A) ALP, OCN and TLR4 expression after treatment with Ti6Al4V, JDBM, SrHPO4-coated JDBM, and SrHPO4-coated JDBM + CLI-095 extracts. (B) pan-Akt, p-Akt (Ser473), p-Akt (Thr308), p-PI3K (p85), and PI3K expression after the same treatments. (C) Alizarin Red S staining after 21 days of incubation. Data are presented as mean ± SD. Statistical significance is indicated as follows: *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001. |
Effects of Sr2⁺ Concentration on Bone Tissue Engineering Repair
Sr2⁺ exhibits a marked concentration-dependent influence on various cell types.45 It was shown that low amounts of Sr2+ induced osteogenic responses in human MSCs, increasing the expression of transcription factors (including RUNX2 and OSR) and osteogenic markers including ALP, OPN, OSP, OSC, and bone salivary proteins (BSP).85 Whereas excessive concentrations of Sr2+ were unfavorable for cellular activity.39 Nevertheless, with rising strontium ion levels, the quantity of TRAP+ cells exhibited a progressive reduction, and even trace Sr2+ concentrations (under 0.2 mg/L) effectively suppressed osteoclastic function and maturation,38 falling within the range of Sr2+ positive concentrations (0.01–1mM) that stimulate osteogenesis and inhibit osteoclastogenesis.86 The highest osteogenic potential was noted in BMSCs grown in 2% Sr2+-enriched medium, characterized by markedly upregulated levels of BMP-2, OCN, Col-I and VEGF, along with significantly increased ALP activity and Ca deposition. Additionally, assessments for cartilaginous tissue development, vascular neotissue formation, and tendon integration with surrounding tissues demonstrated superior outcomes compared to other concentration groups.31
From the previous section, it is known that Sr2+ can trigger a variety of signaling pathways and promote osteogenesis.87 At very low doses of Sr2⁺, Sr-incorporated carbon nitride nanosheets (CNS) can activate the FAK/RhoA/ROCK1 signaling pathway, promote stress fiber formation, and enhance intracellular mechanical tension, thereby facilitating osteogenic differentiation.87 Submicromolar Sr2⁺ doses (0.1 μg/mL, ie., ~1.14 μM) reprogrammed SMAD phosphorylation equilibria, enhancing cell proliferation while suppressing chondrogenic differentiation in articular chondrocytes by biasing the TGFβ1 pathway toward SMAD3 activation, concomitantly at the expense of SMAD1/5/9 signaling axes.88 Additionally, the MAPK/ERK pathway is an important osteogenic mechanism.51 With increasing concentrations of Zn2⁺ and Sr2⁺ in co-supplemented cultures, the osteogenesis-related gene expression of BMSCs increases initially and then declines gradually. When the concentration of Sr2⁺ exceeds 10 mM and that of Zn2⁺ exceeds 80 μM, BMSC viability is significantly impaired. At the optimal concentrations of 6 mM Sr2⁺ and 40 μM Zn2⁺, Sr2⁺ significantly enhances the phosphorylation of Erk1/2 and p38, while Zn2⁺ specifically promotes p38 phosphorylation; additionally, Zn2⁺ markedly enhances Erk1/2 phosphorylation.51 Furthermore, researchers can regulate the surface charge by modulating Sr2+ concentrations.89 The data shows that changes in the membrane potential of cells treated with Sr2+ barium titanate (nBa2+: nSr2+ = 7.9:0.1) enhance the elevated expression of the L-type voltage-gated Ca2⁺ channel Cav1.2.89 This channel governs cytosolic Ca2⁺ levels by altering its gating state or modulating its abundance on the plasma membrane.39 Consequently, increased intracellular Ca2⁺ acts as a secondary signaling molecule, initiating downstream signaling through the calcium-dependent calmodulin/calcineurin-NFAT cascade to stimulate bone formation processes.36,89
The results of some studies showed that Sr2+ concentration promoted MSCs proliferation at ion release accumulation levels of 0.5 and 1 mM, while the opposite effect was observed for ion release accumulation levels ranging from 1 to 10 mM.90 In addition, the CCK-8 assay demonstrated that elevated SrR levels (0.5, 1.0, and 2.0 mM) markedly suppressed cellular viability (P<0.05), whereas lower doses (0.125, 0.25, and 0.5 mM) exerted no notable influence on BMSC growth, suggesting that Sr2⁺ concentrations of 0.5 and 1 mM significantly restricted MSC proliferative capacity.45 However, low concentrations of SrR (0.125, 0.25, and 0.5 mmol/L) did not affect the proliferation of BMSCs, which suggests that different concentrations of Sr2+ will have different effects on cells. Literature has shown that concentrations of Sr2+ between 1.9 mg/L and 7.3 mg/L have beneficial effects on osteoblast activity and proliferation, with 16.4 wt%-Sr2+ substituted magnesium phosphate (MgP) scaffolds having the best physical and osteogenic properties.91 Ding et al reported that the optimal Sr2+ concentration (25–500 µm) for promoting osteogenic differentiation of stem cells was 500 µm, and that this Sr100nHA/hydroxypropyl chitosan/aldehyde dextran hydrogel (CDH) group also promoted osteogenesis in vivo and accelerated the reconstruction of bone defects.41
In addition, quantitative analysis of Von Kossadye solution staining and alizarin red S staining demonstrated that mineralization of the extracellular matrix inside and outside the hydrogel increased dramatically with increasing Sr2+ concentration (P<0.05).39 3D-printed alginate-collagen composite hydrogels seeded with MC3T3-E1 osteoblasts were crosslinked using varying concentrations of 1% strontium-enriched calcium polyphosphate (SCPP). The optimal Sr2+ concentration for cell proliferation and mineralization, as well as the concentration of 1% SCPP that minimized cytotoxic effects (0.3–0.5 mg/mL), were determined. Additionally, 0.5 mg/mL SCPP was found to produce sufficient amounts of Ca nodules.92
Sr2+ May Indirectly Promote Osteogenesis by Inhibiting Osteoclasts
In the research process of osteogenesis, Wang et al have proposed a novel central mechanism: Sr2⁺ induces autophagy, thereby leading to rapid osseointegration by activating the time-dependent regulation of the Akt/mTOR signaling pathway. Additionally, increased secretion of OPG by osteoblasts alters the RANK/RANKL/OPG axis (receptor activator of nuclear factor-κB/receptor activator of nuclear factor-κB ligand/osteoprotegerin axis), indirectly inhibiting osteoclastogenesis.93 An elevated LC3II/LC3-I ratio and high expression levels of Beclin1 (autophagy-related protein Beclin1) demonstrated that Sr2⁺ activates both the early and late stages of autophagy. As a critical regulator in autophagosome nucleation, Beclin1 triggers this process by mobilizing other autophagy-related proteins to the phagophore assembly site.93–95
Furthermore, Sr2⁺ inhibits bone resorption by decreasing the osteoclastogenic factor ratio of RANKL to OPG.68,96 Sr2⁺ also suppresses RANKL-induced osteoclastogenesis by promoting the expression of nuclear factor kappa-B inhibitory protein (IκB-α), significantly inhibiting the phosphorylation of the NF-κB subunit P65, and downregulating the NF-κB signaling pathway.72 Simultaneously, it increases the expression level of OPN, thereby limiting the interaction between the receptor activator of NF-κB (RANK) and its ligand RANKL, and consequently inhibiting osteoclast activity.97 Moreover, enhanced OPG expression and inactivated nuclear factor of activated T-cells cytoplasmic 1 (NFATc1) block RANKL binding and further suppress osteoclast formation.98
Zeng et al found that supplementation with Sr2⁺ significantly inhibits NFATc1, a key transcription factor regulating the expression of multiple genes associated with osteoclast differentiation and function.99 As a core transcription factor, NFATc1 regulates the expression of various genes related to osteoclast differentiation and function, thereby downregulating target genes such as c-FOS, OSCAR (osteoclast-associated receptor), TRAP (tartrate-resistant acid phosphatase), MMP-9 (matrix metalloproteinase-9), and TRAF6 (tumor necrosis factor receptor-associated factor 6) to inhibit osteoclast differentiation and activity.72,100 The results are summarized as follows (Figure 4).
 |
Figure 4 Sr2⁺ inhibits bone resorption by regulating the RANKL/OPG ratio, inhibiting the NF-κB signaling pathway, and downregulating the NFATc1 transcription factor. |
Sr2+ May Influence Bone Repair by Participating in Immune Modulation
Modulation of the immune milieu has emerged as a promising therapeutic focus for osseous repair,101 with immune cells interacting with osteoblasts through direct contact or paracrine mechanisms.102 The effect of macrophages on osteoblasts depends on their polarization profiles and the paracrine factors they secrete.103 As a highly plastic cell population,104 macrophages exhibit diverse roles throughout inflammatory responses and tissue repair, serving as a key regulatory cell population that modulates subsequent phases of bone-implant integration.105
Sr2⁺-doped implants inhibit the expression of the pro-inflammatory cytokines tumor necrosis factor α (TNF-α) and interleukin-1β (IL-1β) by attenuating the activation of nuclear factor-κB (NF-κB).106 In RAW264.7 macrophages, the expression levels of IL-1β and matrix metalloproteinase 9 (MMP9) are downregulated by approximately 0.6-fold, while the mRNA levels of cathepsin K (CTSK), macrophage colony-stimulating factor (MCSF), and interleukin-6 (IL-6) are also reduced.107 BMP2, a potent osteoinductive cytokine involved in skeletal regeneration, is significantly upregulated by Sr2⁺, and it plays a pivotal role in initiating fracture repair and enhancing the expression of osteogenic markers—including ALP, RUNX2, OCN and collagen-related proteins.106 This process fosters an immunomodulatory microenvironment that suppresses RANKL-mediated osteoclastogenesis.106
Additionally, Sr2⁺ can induce neutrophils to play an important role in bone immunity. By suppressing the NF-κB signaling pathway and increasing the phosphorylation level of STAT3, Sr2⁺ induces the polarization of neutrophils toward the N2 phenotype and promotes neovascularization.108
Macrophage cytoarchitecture and catalase (CAT)/superoxide dismutase (SOD) activity are influenced by oxidative stress (OS) and inflammation.102,103 In early inflammatory environments, Sr2⁺ upregulates the expression of OMSR/IL6st/STAT3—key genes in the oncostatin M (OSM) pathway—to promote osteogenesis.46 Through the ERK signaling pathway, Sr2⁺ polarizes macrophages from the M1 to the M2 phenotype. Subsequently, M2 macrophages overexpress osteogenesis-related cytokines such as transforming growth factor-β (TGF-β), platelet-derived growth factor-BB (PDGF-BB), and BMP2; they also stimulate the expression of the anti-inflammatory genes arginase and interleukin 10 (IL-10), reducing the inhibitory effect of the pro-inflammatory factor TNF-α on BMP, OSX, ALP, and RUNX2. Sr2⁺ downregulates the expression of inflammation-related genes (IL-1β, TNF-α, and IL-6) in macrophages.102,103,105 The upregulated IL-10 can suppress the production of pro-inflammatory cytokines (including IL-1β, TNF-α, and IL-6), thereby exerting anti-inflammatory effects and enhancing tissue repair (Figure 5).109
 |
Figure 5 Sr2⁺ induces M2 polarization of macrophages through the ERK pathway, upregulates osteogenic factor TGF-β1/PDGF-BB/BMP2 and inhibits inflammatory factors (IL-1β, TNF-α, IL-6), and activates IL-10 to enhance anti-inflammatory effect, thereby promoting bone regeneration. |
Macrophage paracrine signaling activated by Sr-containing implants promotes the proliferation of osteoblasts and the osteogenic differentiation of MSCs.110 Additionally, biomaterials containing mixed metal ions—such as the slow-release Cu2⁺/Sr2⁺ bone cement designed by Li et al and the sustained-release Zn2⁺/Sr2⁺ composite scaffolds prepared by Qian et al via selective laser sintering—upregulate the expression of anti-inflammatory genes (IL-10, Arg-1 (arginase-1), IL-1Ra (interleukin-1 receptor antagonist), and TGF-β1) while downregulating the pro-inflammatory genes (TNF-α, IL-1β, and IL-6) when co-cultured with macrophages.111,112
This immunomodulatory effect further regulates bone healing and suggests superior bone-enhancing effects compared to using Sr2⁺ alone.111,112 This favorable osteogenic microenvironment prompts macrophages to significantly upregulate the expression of osteogenesis-related genes involved in cellular development, including ALP, OSM, RUNX2, BMP-2, Wnt10b, and OSX. This, in turn, increases ALP activity and promotes the formation of mineralized nodules.112 Notably, during the late stages of NFATc1/Maf and Wnt signaling pathway activation, Sr2⁺ can significantly elevate the expression of osteogenic factors in BMSCs by stimulating macrophages to establish an appropriate bone immune microenvironment.46
Effects of Sr2+ on Angiogenesis
Bone is highly vascularized, with blood vessels playing an integral role in maintaining bone and bone marrow homeostasis.113 The vascular network acts as a multifunctional circulatory structure, exerting pivotal functions in organ morphogenesis, tissue renewal, and stem cell dynamics. Within osseous microenvironments, specific vascular niches sustain perivascular stem cells or osteoprogenitors, thereby orchestrating osteogenic processes.114
Slowly released Sr2⁺ can upregulate the expression of miR-146a (microRNA-146a),115 and angiogenic genes (vascular endothelial growth factor, VEGF; basic fibroblast growth factor, bFGF).111 It also inhibits the expression of Smad4 and NF2 proteins,115 as well as the pro-inflammatory factor IL-6, in HUVECs.22 This combined regulatory effect, in turn, promotes developmental vascularization and vascularized bone regeneration.115
Xing et al demonstrated that Sr2⁺ can inhibit apoptosis in rat cardiomyocytes (CMs) by decreasing caspase-3 activity and promote angiogenesis by enhancing cell proliferation, strengthening paracrine capacity, and regulating interactions among cardiac cells.116 Sr2⁺ stimulates the release of myogenic regulatory factors (myogenin, MyoG; myoblast determination protein, MyoD) and angiogenic factors (VEGF; hypoxia-inducible factor-1α, HIF-1α), which directly protect injured muscle tissues and facilitate microvascular repair.105,109 Additionally, Sr2⁺ facilitates the M2 polarization of macrophages and suppresses their M1 polarization, indirectly protecting muscle tissues and promoting angiogenesis.117
In bone defect regions, Sr2⁺ activates the platelet-derived growth factor-BB (PDGF-BB)/phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT) signaling pathway to enhance angiogenesis, leading to increased AKT phosphorylation and PDGF-BB expression in HUVECs.118 Furthermore, due to their immunomodulatory effects, HUVECs can polarize macrophages from the M1 to the M2 phenotype and secrete high levels of VEGF and PDGF-BB. These factors promote vascular development in defect regions, accelerate new bone formation, and ultimately improve bone repair outcomes.27
Sr2+ Elements Function in Other Ways
Antimicrobial Effects of Sr2+
It has been reported that 6 mM Sr2⁺ can significantly inhibit the growth of Streptococcus mutans (S. mutans), halting its proliferation within 10 hours. However, its inhibitory effect is weaker than that of 40 μM Zn2⁺, which can arrest S. mutans growth within 8 hours.51 A high-Sr content nanomaterial (15 wt% Sr-CaP, strontium-doped calcium phosphate) exerts significant antibacterial activity against Pseudomonas aeruginosa (P. aeruginosa; the original term “Mycobacterium glauciobacterium” was incorrect), and can completely inhibit P. aeruginosa growth. This effect is associated with Sr2⁺-mediated alterations in the zeta potential of the material surface.119 Strontium-containing hydroxyapatite (Sr-HA) coatings indirectly inhibit bacterial adhesion by alleviating zinc-based degradation and Zn2⁺ cytotoxicity. Their surface properties, such as smoothness, are superior to those of single-layer Zn(OH)2 or HA coatings, further reducing the risk of bacterial colonization.120
The combined release of multiple ions (eg., Zn2⁺/Sr2⁺/Mg2⁺) disrupts bacterial metabolism by creating an alkaline microenvironment. It also induces bacterial membrane potential differences and triggers reactive oxygen species (ROS) production, achieving synergistic antimicrobial effects.52–54 The combination of gallium ions (Ga3⁺) and Sr2⁺ significantly inhibits S. aureus on implant surfaces; this synergistic effect enhances both osteogenic and antimicrobial properties.55 Selenium ions (Se2⁺)/Sr2⁺ co-doped HA exhibits broad-spectrum antibacterial activity against E. coli (a Gram-negative bacterium) and Gram-positive bacteria (eg., S. aureus). The addition of Se neutralizes the cytotoxicity of Sr-HA.34 The Sr2⁺/Zn2⁺/Se2⁺ ternary composite scaffold integrates antimicrobial, antitumor, and osteogenic functions.51 Calcium-aluminate cement (CA) composites containing 20 wt% strontium borosilicate glass (SrBG) exhibit the optimal biofilm inhibitory effect against E. coli and S. aureus. However, antimicrobial activity is negatively correlated with surface porosity: high Sr2⁺ content enhances surface smoothness, inhibiting biofilm formation via physical barrier effects rather than direct bactericidal action.56 Other studies have shown that Sr-doped materials can inhibit biofilm formation but exert no direct killing effect on specific strains (eg., S. aureus and E. coli), suggesting that their antimicrobial mechanism may be primarily mediated by indirect regulation (eg., microenvironmental changes or material surface modification).56
Antioxidant Effects of Sr2⁺
Sr2⁺-doped modified amino-functional mesoporous bioactive glass (MBG) has been developed as a bioactive scaffold. This scaffold not only facilitates superior bone regeneration and vascularization but also reduces ROS levels in BMSCs by activating the cyclic adenosine monophosphate/protein kinase A (cAMP/PKA) signaling pathway, thereby counteracting OS.9
Notably, Sr2⁺ itself can also downregulate ROS levels via activating the cAMP/PKA signaling pathway. Furthermore, Sr2⁺ modulates the behaviors of osteoblasts and osteoclasts by enhancing the activities of antioxidant enzymes (catalase, CAT; superoxide dismutase, SOD), increasing local oxygen tension, and scavenging excessive endogenous ROS in osteoblasts. These effects endow Sr-containing samples with excellent osteoinductive and antioxidant properties.121,122 Kaur et al also confirmed that Sr-doped bioceramic materials exert favorable protective effects against oxidative stress, among which the 5 mol% Sr-doped bioceramic exhibits the strongest protective effect against hydrogen peroxide (H2O2)-induced oxidative stress.123
Clinical Applications of Sr-Containing Biomaterials
The clinical translation of strontium-containing biomaterials requires a comprehensive evaluation of material forms, defect indications, ion release characteristics, mechanical requirements, surgical applicability, and risk-benefit balance.124 Accumulated evidence has verified that strontium acts as a promising functional ion for the fabrication of bone cements, hydrogels, porous scaffolds, and surface-modified coated implants.125 Nevertheless, most current studies remain confined to in vitro experiments and small-animal models.124 Local strontium delivery strategy is particularly critical throughout the clinical translation process. This approach can construct a favorable therapeutic microenvironment at the bone defect and implant interface, reduce systemic strontium exposure, and circumvent the pharmacokinetic limitations of oral administration.62 For load-bearing skeletal sites, the fatigue resistance of strontium-modified ceramics and 3D-printed scaffolds should be assessed to ensure matched material degradation and bone ingrowth behavior. In terms of irregular craniofacial and jaw defects, injectable strontium-doped hydrogels and cements exhibit superior defect adaptability and enable minimally invasive implantation.126
A variety of strontium-containing biomaterials have been fabricated in recent years, including strontium-doped hydroxyapatite/silk fibroin (SrHA/SF) nanospheres,127 strontium-incorporated biocomposite scaffolds,128 phase-change lysozyme-modified strontium-containing titanium implants (Ti-Ly-Sr),129 strontium carbonate-based composite bioceramics (SrC-SrP), strontium-containing phosphate glass (SrP),130 and strontium-releasing nanoscale bone cement.98 Over the past several years, numerous studies have systematically summarized the classification and clinical application potential of strontium-based bioactive materials, covering bone repair scaffolds, bone cements, hydrogels, and surface-modified implants (Table 3).
 |
Table 3 Representative Sr-Containing Biomaterials in Bone Tissue Engineering |
Meanwhile, multi-ion composite systems have further expanded the functional scope of Sr-based biomaterials.142 Within multi-ion composite systems, strontium serves as a functional component to construct coordinated therapeutic ion systems. Sr/Mg co-doping synergistically enhances osteogenesis and angiogenesis and improves the deposition of mineralized matrices.62 Sr/Zn composite systems can strengthen antibacterial capacity and regulate the activity of osteogenesis-related enzymes.46 Sr/Cu composites are applicable for bone defects requiring simultaneous vascularization and anti-infection performance, while the dose-dependent cytotoxicity induced by copper ions needs strict control.47 Additionally, Sr/Se and Sr/Ga composites are suitable for specialized repair scenarios requiring antibacterial and even antitumor properties.59,60 Collectively, the clinical applicability of strontium-containing composites depends on whether the ion combination matches specific clinical demands, including osteoporotic osseointegration, infected bone defects, vascularized bone regeneration, and craniofacial bone reconstruction.62,143–145
Conclusion
Sr-functionalized biomaterials have shown substantial potential for bone regeneration by integrating osteogenesis, osteoclast inhibition, osteoimmunomodulation, angiogenesis, antioxidant activity and antimicrobial protection. Mechanistically, Sr2+ regulates multiple pathways, including CaSR/Wnt/beta-catenin, MAPK/ERK, PI3K/Akt, RANKL/OPG/NF-kappaB/NFATc1 and macrophage-related inflammatory signaling. From a materials perspective, Sr incorporation modifies crystallinity, surface charge, degradation and local ion-release behavior; therefore, the biological outcome is closely linked to material chemistry and fabrication strategy. Multi-ion composites further broaden the functional spectrum of Sr-containing biomaterials, especially when Sr is combined with Mg, Zn, Cu, Se or Ga to address angiogenesis, infection control and immune regulation.
Future research should place greater emphasis on optimizing Sr-based biomaterials for different clinical applications. Since material systems such as ceramics, coatings, hydrogels, bone cements, and 3D-printed scaffolds differ in their structural characteristics and degradation behaviors, their optimal Sr concentrations and release profiles may also vary. Therefore, more stable and controllable therapeutic parameters still need to be established. Meanwhile, before broad clinical application, long-term biosafety, degradation behavior, and the potential risk of systemic Sr accumulation should be systematically evaluated through animal studies. In addition, current fabrication strategies should gradually shift from simple ion doping toward more precise local release systems in order to improve therapeutic efficiency while reducing side effects. The antimicrobial mechanisms of Sr also remain insufficiently understood, particularly regarding reactive oxygen species generation, membrane interference, and biofilm regulation. Future translational studies may focus on challenging clinical conditions such as osseointegration in osteoporotic implants, infected bone defects, craniofacial reconstruction, and vascularized bone regeneration. Overall, Sr-functionalized biomaterials show promising potential in bone repair; however, their successful clinical translation will still depend on further advances in material design, ion-controlled release strategies, and high-quality preclinical and clinical investigations.
Author Contributions
Fengting Ning and Wentao Liu should be considered co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Applied Basic Research Programs of Liaoning Province (No. 2025JH2/101300029 to W.L.), the Provincial Nature Science Foundation of Liaoning (No.2023-MS-174 to X.W.), the Horizontal Project of China Medical University (No. 2900024040 to G. Y.), and the Provincial Nature Science Foundation of Liaoning (No.2025-MSLH-801 to G. Y.).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Tam WL, Freitas Mendes L, Chen X, et al. Human pluripotent stem cell-derived cartilaginous organoids promote scaffold-free healing of critical size long bone defects. Stem Cell Res Ther. 2021;12(1):513. doi:10.1186/s13287-021-02580-7
2. Yan C, Zhang P, Qin Q, et al. 3D-printed bone regeneration scaffolds modulate bone metabolic homeostasis through vascularization for osteoporotic bone defects. Biomaterials. 2024;311:122699. doi:10.1016/j.biomaterials.2024.122699
3. Lo J, Chan L, Flynn S. A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the united states: a 2019 update. Arch Phys Med Rehabil. 2021;102(1):115–21. doi:10.1016/j.apmr.2020.04.001
4. Qin L, Yang S, Zhao C, et al. Prospects and challenges for the application of tissue engineering technologies in the treatment of bone infections. Bone Res. 2024;12(1):28. doi:10.1038/s41413-024-00332-w
5. Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002;2(8):584–593. doi:10.1038/nrc867
6. Zorrón M, Cabrera AL, Sharma R, et al. Emerging 2D nanomaterials-integrated hydrogels: advancements in designing theragenerative materials for bone regeneration and disease therapy. Adv Sci. 2024;11(31):2403204. doi:10.1002/advs.202403204
7. Golafshan N, Vorndran E, Zaharievski S, et al. Tough magnesium phosphate-based 3D-printed implants induce bone regeneration in an equine defect model. Biomaterials. 2020;261:120302. doi:10.1016/j.biomaterials.2020.120302
8. Feng Y, Zhu S, Mei D, et al. Application of 3D printing technology in bone tissue engineering: a review. Current Drug Delivery. 2021;18(7):847–861. doi:10.2174/1567201817999201113100322
9. Wu Q, Hu L, Yan R, et al. Strontium-incorporated bioceramic scaffolds for enhanced osteoporosis bone regeneration. Bone Res. 2022;10(1):55. doi:10.1038/s41413-022-00224-x
10. Kołodziejska B, Stępień N, Kolmas J. The influence of strontium on bone tissue metabolism and its application in osteoporosis treatment. Int J Mol Sci. 2021;22(12):6564. doi:10.3390/ijms22126564
11. De Bonis A, Uskoković V, Barbaro K, et al. Pulsed laser deposition temperature effects on strontium-substituted hydroxyapatite thin films for biomedical implants. Cell Biol Toxicol. 2020;36(6):537–551. doi:10.1007/s10565-020-09527-3
12. You J, Zhang Y, Zhou Y. Strontium functionalized in biomaterials for bone tissue engineering: a prominent role in osteoimmunomodulation. Front Bioeng Biotechnol. 2022;10:928799. doi:10.3389/fbioe.2022.928799
13. Martín-Del-Campo M, Sampedro JG, Flores-Cedillo ML, et al. Bone regeneration induced by strontium folate loaded biohybrid scaffolds. Molecules. 2019;24(9):1660. doi:10.3390/molecules24091660
14. Li Z, Peng S, Pan H, et al. Microarchitecture and nanomechanical properties of trabecular bone after strontium administration in osteoporotic goats. Biol Trace Elem Res. 2012;145(1):39–46. doi:10.1007/s12011-011-9158-y
15. Bharadwaz A, Jayasuriya AC. Recent trends in the application of widely used natural and synthetic polymer nanocomposites in bone tissue regeneration. Mater Sci Eng C. 2020;110:110698. doi:10.1016/j.msec.2020.110698
16. Liu X, Wang D, Wang S, et al. Promoting osseointegration by in situ biosynthesis of metal ion-loaded bacterial cellulose coating on titanium surface. Carbohydr Polym. 2022;297:120022. doi:10.1016/j.carbpol.2022.120022
17. Sheng X, Li C, Wang Z, et al. Advanced applications of strontium-containing biomaterials in bone tissue engineering. Mater Today Bio. 2023;20:100636. doi:10.1016/j.mtbio.2023.100636
18. Du J, Fan L, Razal JM, et al. Strontium-doped mesoporous bioglass nanoparticles for enhanced wound healing with rapid vascularization. J Mat Chem B. 2023;11(31):7364–7377. doi:10.1039/D3TB01256E
19. Huang H, Qiang L, Fan M, et al. 3D-printed tri-element-doped hydroxyapatite/polycaprolactone composite scaffolds with antibacterial potential for osteosarcoma therapy and bone regeneration. Bioact. Mater. 2024;31:18–37. doi:10.1016/j.bioactmat.2023.07.004
20. Kargozar S, Baino F, Sutter J-M. Multiple and promising applications of strontium (Sr)-Containing bioactive glasses in bone tissue engineering. Front Bioeng Biotechnol. 2019;7:7. doi:10.3389/fbioe.2019.00161
21. Li R, Feng D, Han S, et al. Macrophages and fibroblasts in foreign body reactions: how mechanical cues drive cell functions? Mater Today Bio. 2023;22:100783. doi:10.1016/j.mtbio.2023.100783
22. Ma F, Zhang Y, Hu L, et al. Strontium Laminarin polysaccharide modulates osteogenesis-angiogenesis for bone regeneration. Int J Biol Macromol. 2021;181:452–461. doi:10.1016/j.ijbiomac.2021.03.136
23. Arthur A, Gronthos S. Clinical application of bone marrow mesenchymal stem/stromal cells to repair skeletal tissue. Int J Mol Sci. 2020;21(24):9759. doi:10.3390/ijms21249759
24. Mass E, Nimmerjahn F, Kierdorf K, et al. Tissue-specific macrophages: how they develop and choreograph tissue biology. Nat Rev Immunol. 2023;23(9):563–579. doi:10.1038/s41577-023-00848-y
25. Yunna C, Mengru H, Lei W, et al. Macrophage M1/M2 polarization. Eur J Pharmacol. 2020;877:173090. doi:10.1016/j.ejphar.2020.173090
26. Lu GD, Cheng P, Liu T, et al. BMSC-Derived exosomal miR-29a promotes angiogenesis and osteogenesis. Front Cell Develop Biol. 2020;8:608521. doi:10.3389/fcell.2020.608521
27. Miao Q, Yang X, Diao J, et al. 3D printed strontium-doped calcium phosphate ceramic scaffold enhances early angiogenesis and promotes bone repair through the regulation of macrophage polarization. Mater Today Bio. 2023;23:100871. doi:10.1016/j.mtbio.2023.100871
28. Lu W, Zhou C, Ma Y, et al. Improved osseointegration of strontium-modified titanium implants by regulating angiogenesis and macrophage polarization. Biomater Sci. 2022;10(9):2198–2214. doi:10.1039/D1BM01488A
29. Maruyama M, Rhee C, Utsunomiya T, et al. Modulation of the inflammatory response and bone healing. Front Endocrinol. 2020;11:386. doi:10.3389/fendo.2020.00386
30. Deng Y, Ma F, Ruiz-Ortega LI, et al. Fabrication of strontium Eucommia ulmoides polysaccharides and in vitro evaluation of their osteoimmunomodulatory property. Int J Biol Macromol. 2019;140:727–735. doi:10.1016/j.ijbiomac.2019.08.145
31. Ma P, Chen T, Wu X, et al. Effects of bioactive strontium-substituted hydroxyapatite on osseointegration of polyethylene terephthalate artificial ligaments. J Mat Chem B. 2021;9(33):6600–6613. doi:10.1039/D1TB00768H
32. Pontremoli C, Izquierdo-Barba I, Montalbano G, et al. Strontium-releasing mesoporous bioactive glasses with anti-adhesive zwitterionic surface as advanced biomaterials for bone tissue regeneration. J Colloid Interface Sci. 2020;563:92–103. doi:10.1016/j.jcis.2019.12.047
33. Wang X, Liu W, Jiang C, et al. Research progress on the osteogenic properties of tantalum in the field of medical implant materials. J Mater Res Technol. 2024;30:1706–1715. doi:10.1016/j.jmrt.2024.03.200
34. Maqbool M, Nawaz Q, Atiq Ur Rehman M, et al. Synthesis, characterization, antibacterial properties, and in vitro studies of selenium and strontium co-substituted hydroxyapatite. Int J Mol Sci. 2021;22(8):4246. doi:10.3390/ijms22084246
35. Dai LL, Nudelman F, Chu CH, et al. The effects of strontium-doped bioactive glass and fluoride on hydroxyapatite crystallization. J Dentistry. 2021;105:103581. doi:10.1016/j.jdent.2021.103581
36. Wang P, Zhou X, Lv C, et al. Modulating the surface potential of microspheres by phase transition in strontium doped barium titanate to restore the electric microenvironment for bone regeneration. Front Bioeng Biotechnol. 2022;10:988300. doi:10.3389/fbioe.2022.988300
37. Nadi A, Khodaei M, Javdani M, et al. Fabrication of functional and nano-biocomposite scaffolds using strontium-doped bredigite nanoparticles/polycaprolactone/poly lactic acid via 3D printing for bone regeneration. Int J Biol Macromol. 2022;219:1319–1336. doi:10.1016/j.ijbiomac.2022.08.136
38. Tovani CB, Oliveira TM, Soares MPR, et al. Strontium calcium phosphate nanotubes as bioinspired building blocks for bone regeneration. ACS Appl Mater Interfaces. 2020;12(39):43422–43434. doi:10.1021/acsami.0c12434
39. Zhao D, Wang X, Tie C, et al. Bio-functional strontium-containing photocrosslinked alginate hydrogels for promoting the osteogenic behaviors. Mater Sci Eng C. 2021;126:112130. doi:10.1016/j.msec.2021.112130
40. Xu J, Vecstaudza J, Wesdorp MA, et al. Incorporating strontium enriched amorphous calcium phosphate granules in collagen/collagen-magnesium-hydroxyapatite osteochondral scaffolds improves subchondral bone repair. Mater Today Bio. 2024;25:100959. doi:10.1016/j.mtbio.2024.100959
41. Ding X, Li X, Li C, et al. Chitosan/Dextran hydrogel constructs containing strontium-doped hydroxyapatite with enhanced osteogenic potential in rat cranium. ACS Biomater Sci Eng. 2019;5(9):4574–4586. doi:10.1021/acsbiomaterials.9b00584
42. Bussola Tovani C, Divoux T, Manneville S, et al. Strontium-driven physiological to pathological transition of bone-like architecture: a dose-dependent investigation. Acta Biomater. 2023;169:579–588. doi:10.1016/j.actbio.2023.07.043
43. Akshata CR, Murugan E, Harichandran G. Alginate templated synthesis, characterization and in vitro osteogenic evaluation of strontium-substituted hydroxyapatite. Int J Biol Macromol. 2023;252:126478. doi:10.1016/j.ijbiomac.2023.126478
44. Prabha RD, Ding M, Bollen P, et al. Strontium ion reinforced bioceramic scaffold for load bearing bone regeneration. Mater Sci Eng C. 2020;109:110427. doi:10.1016/j.msec.2019.110427
45. Yu H, Liu Y, Yang X, et al. Strontium ranelate promotes chondrogenesis through inhibition of the Wnt/β-catenin pathway. Stem Cell Res Ther. 2021;12(1):296. doi:10.1186/s13287-021-02372-z
46. Zhong Z, Wu X, Wang Y, et al. Zn/Sr dual ions-collagen co-assembly hydroxyapatite enhances bone regeneration through procedural osteo-immunomodulation and osteogenesis. Bioact. Mater. 2022;10:195–206. doi:10.1016/j.bioactmat.2021.09.013
47. Pang S, Wu D, Yang H, et al. Enhanced mechanical performance and bioactivity in strontium/copper co-substituted diopside scaffolds. Biomat Adv. 2023;145:213230. doi:10.1016/j.bioadv.2022.213230
48. Mengdi Z, Jiayi L, Canfeng L, et al. Surface modification of polyetheretherketone (PEEK) to enhance osteointegration by grafting strontium Eucommia ulmoides polysaccharides. Int J Biol Macromol. 2022;211:230–237. doi:10.1016/j.ijbiomac.2022.05.048
49. Zhou C, Ge Z, Song L, et al. Strontium-modified titanium substrate promotes osteogenic differentiation of
50. Liu Z, Zhang H, Gan J, et al. Black phosphorus tagged responsive strontium hydrogel particles for bone defect repair. Adv Sci. 2025;12(1):2408284. doi:10.1002/advs.202408284
51. Yin S, Sun N, Jiang F, et al. The translation from in vitro bioactive ion concentration screening to in vivo application for preventing peri-implantitis. ACS Appl Mater Interfaces. 2021;13(4):5782–5794. doi:10.1021/acsami.0c19698
52. Hou HH, Lee BS, Liu YC, et al. Vapor-Induced pore-forming atmospheric-plasma-sprayed zinc-, strontium-, and magnesium-doped hydroxyapatite coatings on titanium implants enhance new bone formation—an in vivo and in vitro investigation. Int J Mol Sci. 2023;24(5):4933. doi:10.3390/ijms24054933
53. Mao Z, Li Y, Yang Y, et al. Osteoinductivity and antibacterial properties of strontium ranelate-loaded Poly(Lactic-co-glycolic acid) microspheres with assembled silver and hydroxyapatite nanoparticles. Front Pharmacol. 2018;9:368. doi:10.3389/fphar.2018.00368
54. Baheiraei N, Eyni H, Bakhshi B, et al. Effects of strontium ions with potential antibacterial activity on in vivo bone regeneration. Sci Rep. 2021;11(1):8745. doi:10.1038/s41598-021-88058-1
55. Gao Z, Song M, Liu RL, et al. Improving in vitro and in vivo antibacterial functionality of Mg alloys through micro-alloying with Sr and Ga. Mater Sci Eng. 2019;104:109926. doi:10.1016/j.msec.2019.109926
56. Abd El-Hamid HK, El-Kheshen AA, Abdou AM, et al. Incorporation of strontium borosilicate bioactive glass in calcium aluminate biocement: physicomechanical, bioactivity and antimicrobial properties. J Mech Behav Biomed Mater. 2023;144:105976. doi:10.1016/j.jmbbm.2023.105976
57. Liu YC, Lee YT, Huang TC, et al. In vitro bioactivity and antibacterial activity of strontium-, magnesium-, and zinc-multidoped hydroxyapatite porous coatings applied via atmospheric plasma spraying. ACS Appl Bio Mater. 2021;4(3):2523–2533. doi:10.1021/acsabm.0c01535
58. Wu Y, Shi X, Wang J, et al. A surface metal ion-modified 3D-printed Ti-6Al-4V implant with direct and immunoregulatory antibacterial and osteogenic activity. Front Bioeng Biotechnol. 2023;11:1142264. doi:10.3389/fbioe.2023.1142264
59. Li K, Tian H, Guo A, et al. Gallium (Ga)–strontium (Sr) layered double hydroxide composite coating on titanium substrates for enhanced osteogenic and antibacterial abilities. J Biomed Mater Res Part A. 2022;110(2):273–286. doi:10.1002/jbm.a.37284
60. Marcello E, Maqbool M, Nigmatullin R, et al. Antibacterial composite materials based on the combination of polyhydroxyalkanoates with selenium and strontium co-substituted hydroxyapatite for bone regeneration. Front Bioeng Biotechnol. 2021;9:647007. doi:10.3389/fbioe.2021.647007
61. Luo Y, Zhang H, Wang Z, et al. Strategic incorporation of metal ions in bone regenerative scaffolds: multifunctional platforms for advancing osteogenesis. Regenerat Biomat. 2025;12:rbaf068. doi:10.1093/rb/rbaf068
62. Ho CC, Hsu TT, Chiu YC, et al. 3D-printed magnesium/strontium-co-doped calcium silicate scaffolds promote angiogenesis and bone regeneration through synergistic bioactive ion stimulation. J Biol Eng. 2025;19(1):58. doi:10.1186/s13036-025-00528-6
63. Gómez-Cerezo N, Lozano D, Salinas AJ, et al. Mesoporous bioactive glasses: a powerful tool in tissue engineering and drug delivery. Adv Healthcare Mater. 2026;15(2):e02201. doi:10.1002/adhm.202502201
64. Wu Y, Adeeb SM, Duke MJ, et al. Compositional and material properties of rat bone after bisphosphonate and/or strontium ranelate drug treatment. J Pharm Pharm Sci. 2013;16(1):52. doi:10.18433/J3C59H
65. Chan WCW, Tan Z, To MKT, et al. Regulation and role of transcription factors in osteogenesis. Int J Mol Sci. 2021;22(11):5445. doi:10.3390/ijms22115445
66. Liu Q, Li M, Wang S, et al. Recent advances of osterix transcription factor in osteoblast differentiation and bone formation. Front Cell Develop Biol. 2020;8:601224. doi:10.3389/fcell.2020.601224
67. Sartoretto SC, Calasans-Maia MD, Alves ATNN, et al. The role of apoptosis associated speck-like protein containing a caspase-1 recruitment domain (ASC) in response to bone substitutes. Mater Sci Eng C. 2020;112:110965. doi:10.1016/j.msec.2020.110965
68. Liu R, Wu S, Liu W, et al. microRNAs delivered by small extracellular vesicles in MSCs as an emerging tool for bone regeneration. Front Bioeng Biotechnol. 2023;11:1249860. doi:10.3389/fbioe.2023.1249860
69. Kim P, Park J, Lee DJ, et al. Mast4 determines the cell fate of MSCs for bone and cartilage development. Nat Commun. 2022;13(1):3960. doi:10.1038/s41467-022-31697-3
70. Huang Y, Wu Q, Tam PKH. Immunomodulatory mechanisms of mesenchymal stem cells and their potential clinical applications. Int J Mol Sci. 2022;23(17):10023. doi:10.3390/ijms231710023
71. Li Y, Yue J, Liu Y, et al. Strontium regulates stem cell fate during osteogenic differentiation through asymmetric cell division. Acta Biomater. 2021;119:432–443. doi:10.1016/j.actbio.2020.10.030
72. Zeng J, Guo J, Sun Z, et al. Osteoblastic and anti-osteoclastic activities of strontium-substituted silicocarnotite ceramics: in vitro and in vivo studies. Bioact. Mater. 2020;5(3):435–446. doi:10.1016/j.bioactmat.2020.03.008
73. Fenbo M, Sijing L, Ruiz-Ortega LI, et al. Effects of alginate/chondroitin sulfate-based hydrogels on bone defects healing. Mater Sci Eng C. 2020;116:111217. doi:10.1016/j.msec.2020.111217
74. Liu X, Sun Y, Shen J, et al. Strontium doped mesoporous silica nanoparticles accelerate osteogenesis and angiogenesis in distraction osteogenesis by activation of Wnt pathway. Nanomed Nanotechnol Biol Med. 2022;41:102496. doi:10.1016/j.nano.2021.102496
75. Cheng D, Ding R, Jin X, et al. Strontium ion-functionalized nano-hydroxyapatite/chitosan composite microspheres promote osteogenesis and angiogenesis for bone regeneration. ACS Appl Mater Interfaces. 2023;15(16):19951–19965. doi:10.1021/acsami.3c00655
76. Hassani A, Avci ÇB, Kerdar SN, et al. Interaction of alginate with nano-hydroxyapatite-collagen using strontium provides suitable osteogenic platform. J Nanobiotechnol. 2022;20(1):310. doi:10.1186/s12951-022-01511-9
77. Zhou C, Chen YQ, Zhu YH, et al. Antiadipogenesis and osseointegration of strontium-doped implant surfaces. J Dental Res. 2019;98(7):795–802. doi:10.1177/0022034519850574
78. Aimaiti A, Wahafu T, Keremu A, et al. Strontium ameliorates glucocorticoid inhibition of osteogenesis via the ERK signaling pathway. Biol Trace Elem Res. 2020;197(2):591–598. doi:10.1007/s12011-019-02009-6
79. Ataie M, Nourmohammadi J, Seyedjafari E. Carboxymethyl carrageenan immobilized on 3D-printed polycaprolactone scaffold for the adsorption of calcium phosphate/strontium phosphate adapted to bone regeneration. Int J Biol Macromol. 2022;206:861–874. doi:10.1016/j.ijbiomac.2022.03.096
80. Shimizu Y, Fujibayashi S, Yamaguchi S, et al. Bioactive effects of strontium loading on micro/nano surface Ti6Al4V components fabricated by selective laser melting. Mater Sci Eng C. 2020;109:110519. doi:10.1016/j.msec.2019.110519
81. Liu C, Xiong Q, Li Q, et al. CHD7 regulates bone-fat balance by suppressing PPAR-γ signaling. Nat Commun. 2022;13(1):1989. doi:10.1038/s41467-022-29633-6
82. Dawson JC, Serrels A, Stupack DG, et al. Targeting FAK in anticancer combination therapies. Nat Rev Cancer. 2021;21(5):313–324. doi:10.1038/s41568-021-00340-6
83. Li L, Yao L, Wang H, et al. Magnetron sputtering of strontium nanolayer on zirconia implant to enhance osteogenesis. Mater Sci Eng C. 2021;127:112191. doi:10.1016/j.msec.2021.112191
84. Wang Z, Wang X, Pei J, et al. Degradation and osteogenic induction of a SrHPO4-coated Mg–Nd–Zn–Zr alloy intramedullary nail in a rat femoral shaft fracture model. Biomaterials. 2020;247:119962. doi:10.1016/j.biomaterials.2020.119962
85. Naruphontjirakul P, Tsigkou O, Li S, et al. Human mesenchymal stem cells differentiate into an osteogenic lineage in presence of strontium containing bioactive glass nanoparticles. Acta Biomater. 2019;90:373–392. doi:10.1016/j.actbio.2019.03.038
86. Wu T, Liu W, Huang S, et al. Bioactive strontium ions/ginsenoside Rg1–incorporated biodegradable silk fibroin-gelatin scaffold promoted challenging osteoporotic bone regeneration. Mater Today Bio. 2021;12:100141. doi:10.1016/j.mtbio.2021.100141
87. Liu L, Zhang Z, Aimaijiang M, et al. Strontium-Incorporated carbon nitride nanosheets modulate intracellular tension for reinforced bone regeneration. Nano Lett. 2022;22(23):9723–9731. doi:10.1021/acs.nanolett.2c04078
88. Liu S, Shen B, Loor JJ, et al. Strontium regulates the proliferation and differentiation of isolated primary bovine chondrocytes via the TGFβ/SMAD pathway. Front Pharmacol. 2022;13:925302. doi:10.3389/fphar.2022.925302
89. Kameyama M, Minobe E, Shao D, et al. Regulation of cardiac Cav1.2 channels by calmodulin. Int J Mol Sci. 2023;24(7):6409. doi:10.3390/ijms24076409
90. Lourenço AH, Torres AL, Vasconcelos DP, et al. Osteogenic, anti-osteoclastogenic and immunomodulatory properties of a strontium-releasing hybrid scaffold for bone repair. Mater Sci Eng. 2019;99:1289–1303. doi:10.1016/j.msec.2019.02.053
91. Meininger S, Moseke C, Spatz K, et al. Effect of strontium substitution on the material properties and osteogenic potential of 3D powder printed magnesium phosphate scaffolds. Mater Sci Eng. 2019;98:1145–1158. doi:10.1016/j.msec.2019.01.053
92. Tharakan S, Khondkar S, Lee S, et al. 3D Printed osteoblast–alginate/collagen hydrogels promote survival, proliferation and mineralization at low doses of strontium calcium polyphosphate. Pharmaceutics. 2022;15(1):11. doi:10.3390/pharmaceutics15010011
93. Wang H, Ma Y, Li J, et al. Modulating autophagy by strontium-doped micro/nano rough titanium surface for promotion of osteogenesis and inhibition of osteoclastogenesis. Colloids Surf B. 2022;210:112246. doi:10.1016/j.colsurfb.2021.112246
94. Zhang X, Cui J, Cheng L, et al. Enhancement of osteoporotic bone regeneration by strontium-substituted 45S5 bioglass via time-dependent modulation of autophagy and the Akt/mTOR signaling pathway. J Mat Chem B. 2021;9(16):3489–3501. doi:10.1039/D0TB02991B
95. Wang X, Li X, Xia Y, et al. Hernandezine regulates proliferation and autophagy-induced apoptosis in melanoma cells. J Natural Prod. 2022;85(5):1351–1362. doi:10.1021/acs.jnatprod.2c00098
96. Xing H, Li R, Wei Y, et al. Improved osteogenesis of selective-laser-melted titanium alloy by coating strontium-doped phosphate with high-efficiency air-plasma treatment. Front Bioeng Biotechnol. 2020;8:367. doi:10.3389/fbioe.2020.00367
97. Ullah I, Zhang W, Yang L, et al. Impact of structural features of Sr/Fe co-doped HAp on the osteoblast proliferation and osteogenic differentiation for its application as a bone substitute. Mater Sci Eng C. 2020;110:110633. doi:10.1016/j.msec.2020.110633
98. Lee NH, Kang MS, Kim TH, et al. Dual actions of osteoclastic-inhibition and osteogenic-stimulation through strontium-releasing bioactive nanoscale cement imply biomaterial-enabled osteoporosis therapy. Biomaterials. 2021;276:121025. doi:10.1016/j.biomaterials.2021.121025
99. Zhong Z, Zhang C, Ni S, et al. NFATc1-mediated expression of SLC7A11 drives sensitivity to TXNRD1 inhibitors in osteoclast precursors. Redox Biol. 2023;63:102711. doi:10.1016/j.redox.2023.102711
100. Geng Z, Ji L, Li Z, et al. Nano-needle strontium-substituted apatite coating enhances osteoporotic osseointegration through promoting osteogenesis and inhibiting osteoclastogenesis. Bioact. Mater. 2021;6(4):905–915. doi:10.1016/j.bioactmat.2020.09.024
101. Xiong Y, B MB, Lin Z, et al. The role of the immune microenvironment in bone, cartilage, and soft tissue regeneration: from mechanism to therapeutic opportunity. Military Med Res. 2022;9(1):65. doi:10.1186/s40779-022-00426-8
102. Fischer V, Haffner-Luntzer M. Interaction between bone and immune cells: implications for postmenopausal osteoporosis. Semin Cell Dev Biol. 2022;123:14–21. doi:10.1016/j.semcdb.2021.05.014
103. Yao Y, Cai X, Ren F, et al. The macrophage-osteoclast axis in osteoimmunity and osteo-related diseases. Front Immunol. 2021;12:664871. doi:10.3389/fimmu.2021.664871
104. Schlundt C, Fischer H, Bucher CH, et al. The multifaceted roles of macrophages in bone regeneration: a story of polarization, activation and time. Acta Biomater. 2021;133:46–57. doi:10.1016/j.actbio.2021.04.052
105. Xu AT, Xie YW, Xu JG, et al. Effects of strontium-incorporated micro/nano rough titanium surfaces on osseointegration via modulating polarization of macrophages. Colloids Surf B. 2021;207:111992. doi:10.1016/j.colsurfb.2021.111992
106. Fenbo M, Xingyu X, Bin T. Strontium chondroitin sulfate/silk fibroin blend membrane containing microporous structure modulates macrophage responses for guided bone regeneration. Carbohydr Polym. 2019;213:266–275. doi:10.1016/j.carbpol.2019.02.068
107. Xu L, Ma F, Leung FKL, et al. Chitosan-strontium chondroitin sulfate scaffolds for reconstruction of bone defects in aged rats. Carbohydr Polym. 2021;273:118532. doi:10.1016/j.carbpol.2021.118532
108. Li T, He H, Yang Z, et al. Strontium-doped gelatin scaffolds promote M2 macrophage switch and angiogenesis through modulating the polarization of neutrophils. Biomater Sci. 2021;9(8):2931–2946. doi:10.1039/D0BM02126A
109. Saraiva M, Vieira P, O’Garra A. Biology and therapeutic potential of interleukin-10. J Exp Med. 2020;217(1):e20190418. doi:10.1084/jem.20190418
110. Wang D, Chen M, Wei Y, et al. Construction of wogonin nanoparticle-containing strontium-doped nanoporous structure on titanium surface to promote osteoporosis fracture repair. Adv Healthcare Mater. 2022;11(21):2201405. doi:10.1002/adhm.202201405
111. Li S, Zhang L, Liu C, et al. Spontaneous immunomodulation and regulation of angiogenesis and osteogenesis by Sr/Cu-borosilicate glass (BSG) bone cement to repair critical bone defects. Bioact Mater. 2023;23:101–117. doi:10.1016/j.bioactmat.2022.10.021
112. Qian G, Mao Y, Shuai Y, et al. Enhancing bone scaffold interfacial reinforcement through in situ growth of metal–organic frameworks (MOFs) on strontium carbonate: achieving high strength and osteoimmunomodulation. J Colloid Interface Sci. 2024;655:43–57. doi:10.1016/j.jcis.2023.10.133
113. Prisby RD. Bone Marrow Microvasculature[M/OL]//TERJUNG R. In:Comprehensive Physiology. Wiley;2020:1009–1046.
114. Zhao Y, Xie L. Unique bone marrow blood vessels couple angiogenesis and osteogenesis in bone homeostasis and diseases. Ann NY Acad Sci. 2020;1474(1):5–14. doi:10.1111/nyas.14348
115. Liu L, Yu F, Li L, et al. Bone marrow stromal cells stimulated by strontium-substituted calcium silicate ceramics: release of exosomal miR-146a regulates osteogenesis and angiogenesis. Acta Biomater. 2021;119:444–457. doi:10.1016/j.actbio.2020.10.038
116. Xing M, Jiang Y, Bi W, et al. Strontium ions protect hearts against myocardial ischemia/reperfusion injury. Sci Adv. 2021;7(3):eabe0726. doi:10.1126/sciadv.abe0726
117. Yuan Y, Zhang Z, Mo F, et al. A biomaterial-based therapy for lower limb ischemia using Sr/Si bioactive hydrogel that inhibits skeletal muscle necrosis and enhances angiogenesis. Bioact. Mater. 2023;26:264–278. doi:10.1016/j.bioactmat.2023.02.027
118. Sun Y, Li Y, Zhang Y, et al. A polydopamine-assisted strontium-substituted apatite coating for titanium promotes osteogenesis and angiogenesis via FAK/MAPK and PI3K/AKT signaling pathways. Mater Sci Eng C. 2021;131:112482. doi:10.1016/j.msec.2021.112482
119. Anwar A, Kanwal Q, Sadiqa A, et al. Synthesis and antimicrobial analysis of high surface area strontium-substituted calcium phosphate nanostructures for bone regeneration. Int J Mol Sci. 2023;24(19):14527. doi:10.3390/ijms241914527
120. Wang B, Li Y, Wang S, et al. Electrodeposited dopamine/strontium-doped hydroxyapatite composite coating on pure zinc for anti-corrosion, antimicrobial and osteogenesis. Mater Sci Eng C. 2021;129:112387. doi:10.1016/j.msec.2021.112387
121. Shen X, Fang K, Ru Yie KH, et al. High proportion strontium-doped micro-arc oxidation coatings enhance early osseointegration of titanium in osteoporosis by anti-oxidative stress pathway. Bioact. Mater. 2022;10:405–419. doi:10.1016/j.bioactmat.2021.08.031
122. Lin SJ, Huang CC. Strontium peroxide-loaded composite scaffolds capable of generating oxygen and modulating behaviors of osteoblasts and osteoclasts. Int J Mol Sci. 2022;23(11):6322. doi:10.3390/ijms23116322
123. Kaur P, Singh KJ, Kaur S, et al. Sol-gel derived strontium-doped SiO2–CaO–MgO–P2O5 bioceramics for faster growth of bone like hydroxyapatite and their in vitro study for orthopedic applications. Mater Chem Phys. 2020;245:122763. doi:10.1016/j.matchemphys.2020.122763
124. Tang X, Xu H, Liu X, et al. Advances in 3D-Printed scaffolds for bone defect repair: material strategies and synergistic functional performance. Front Bioeng Biotechnol. 2025;13:1707406. doi:10.3389/fbioe.2025.1707406
125. Shan Y, Bai Y, Zhao L, et al. Three-dimensional-printed strontium-incorporated β-TCP bioceramic triply periodic minimal surface scaffolds with enhanced angiogenic and osteogenic properties. Regenerat Biomat. 2025;12:rbaf080. doi:10.1093/rb/rbaf080
126. Huang K, Li Q, Liu Y, et al. 3D-printed functionalized strontium-silk fibroin-hydroxyapatite scaffolds facilitate bone regeneration via immunomodulatory and sequential angiogenic-osteogenic coupling. Bioact. Mater. 2026;55:271–289. doi:10.1016/j.bioactmat.2025.09.033
127. Wang L, Pathak JL, Liang D, et al. Fabrication and characterization of strontium-hydroxyapatite/silk fibroin biocomposite nanospheres for bone-tissue engineering applications. Int J Biol Macromol. 2020;142:366–375. doi:10.1016/j.ijbiomac.2019.09.107
128. Zhang XY, Chen YP, Han J, et al. Biocompatiable silk fibroin/carboxymethyl chitosan/strontium substituted hydroxyapatite/cellulose nanocrystal composite scaffolds for bone tissue engineering. Int J Biol Macromol. 2019;136:1247–1257. doi:10.1016/j.ijbiomac.2019.06.172
129. Ding Y, Yuan Z, Liu P, et al. Fabrication of strontium-incorporated protein supramolecular nanofilm on titanium substrates for promoting osteogenesis. Mater Sci Eng C. 2020;111:110851. doi:10.1016/j.msec.2020.110851
130. Huang C, Zhou J, Rao J, et al. Fabrication of strontium carbonate-based composite bioceramics as potential bone regenerative biomaterials. Colloids Surf B. 2022;218:112755. doi:10.1016/j.colsurfb.2022.112755
131. Dai J, Fu Y, Chen D, et al. A novel and injectable strontium-containing hydroxyapatite bone cement for bone substitution: a systematic evaluation. Mater Sci Eng C. 2021;124:112052. doi:10.1016/j.msec.2021.112052
132. Sasaki JI, Kiba W, Abe GL, et al. Fabrication of strontium-releasable inorganic cement by incorporation of bioactive glass. Dent. Mater. 2019;35(5):780–788. doi:10.1016/j.dental.2019.02.019
133. No YJ, Xin X, Ramaswamy Y, et al. Novel injectable strontium-hardystonite phosphate cement for cancellous bone filling applications. Mater Sci Eng C. 2019;97:103–115. doi:10.1016/j.msec.2018.11.069
134. Li H, Liao J, Zhang Y, et al. Strontium hydroxyapatite/magnesium oxychloride cement with high strength and high osteogenic activity for bone defect repair. Biomed Mater. 2023;18(2):025023. doi:10.1088/1748-605X/acbd07
135. Cui X, Zhang Y, Wang J, et al. Strontium modulates osteogenic activity of bone cement composed of bioactive borosilicate glass particles by activating Wnt/β-catenin signaling pathway. Bioact. Mater. 2020;5(2):334–347. doi:10.1016/j.bioactmat.2020.02.016
136. Richter RF, Ahlfeld T, Gelinsky M, et al. Composites consisting of calcium phosphate cements and mesoporous bioactive glasses as a 3D plottable drug delivery system. Acta Biomater. 2023;156:146–157. doi:10.1016/j.actbio.2022.01.034
137. Zhang W, Shi W, Wu S, et al. 3D printed composite scaffolds with dual small molecule delivery for mandibular bone regeneration. Biofabrication. 2020;12(3):035020. doi:10.1088/1758-5090/ab906e
138. Sutthavas P, Tahmasebi Birgani Z, Habibovic P, et al. Calcium phosphate-coated and strontium-incorporated mesoporous silica nanoparticles can effectively induce osteogenic stem cell differentiation. Adv Healthcare Mater. 2022;11(4):2101588. doi:10.1002/adhm.202101588
139. Li Y, Wang W, Yu F, et al. Characterization and cytocompatibility of hierarchical porous TiO2 coatings incorporated with calcium and strontium by one-step micro-arc oxidation. Mater Sci Eng C. 2020;109:110610. doi:10.1016/j.msec.2019.110610
140. Sun Y, Liu X, Tan J, et al. Strontium ranelate incorporated 3D porous sulfonated PEEK simulating MC3T3-E1cell differentiation. Regenerat Biomat. 2021;8(1):rbaa043. doi:10.1093/rb/rbaa043
141. Zheng Z, Hu L, Ge Y, et al. Surface modification of Poly(ether ether ketone) by simple chemical grafting of strontium chondroitin sulfate to improve its anti-inflammation, angiogenesis, osteogenic properties. Adv Healthcare Mater. 2022;11(13):2200398. doi:10.1002/adhm.202200398
142. Akobundu UU, Ifijen IH, Duru P, et al. Exploring the role of strontium-based nanoparticles in modulating bone regeneration and antimicrobial resistance: a public health perspective. RSC Adv. 2025;15(14):10902–10957. doi:10.1039/D5RA00308C
143. Xu B, Zhao J, He JM, et al. An injectable multi-functional strontium based gentiopicroside hydrogel accelerates bone regeneration via immunomodulation and promoting osteo-/angiogenesis effects. Adv Compos Hybrid Mater. 2026;9(2):151. doi:10.1007/s42114-026-01719-5
144. Chen B, Zhang L, Zhong Z, et al. Strontium/magnesium-doped coralline hydroxyapatite for bone regeneration. Regenerat Biomat. 2025;12:rbaf036. doi:10.1093/rb/rbaf036
145. Chen YY, Ma TL, Chang PJ, et al. Synergistic effect of strontium doping and surfactant addition in mesoporous bioactive glass for enhanced osteogenic bioactivity and advanced bone regeneration. Polymers. 2025;17(2):187. doi:10.3390/polym17020187
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.