Back to Journals » International Journal of General Medicine » Volume 14
Stroke Risk Factor Awareness Among Populations in Saudi Arabia
Authors Bakraa R, Aldhaheri R ![]() , Barashid M, Benafeef S, Alzahrani M
, Barashid M, Benafeef S, Alzahrani M ![]() , Bajaba R
, Bajaba R ![]() , Alshehri S, Alshibani M
, Alshehri S, Alshibani M ![]()
Received 19 June 2021
Accepted for publication 21 July 2021
Published 5 August 2021 Volume 2021:14 Pages 4177—4182
DOI https://doi.org/10.2147/IJGM.S325568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Reem Bakraa,1 Ruba Aldhaheri,1 Mada Barashid,1 Sarah Benafeef,1 Maram Alzahrani,1 Rasha Bajaba,2 Samah Alshehri,3 Mohannad Alshibani3
1College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 2Laboratory and Blood Bank Department, King Fahd General Hospital, Jeddah, Saudi Arabia; 3Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Mohannad Alshibani
Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, PO Box 22252, Jeddah, Saudi Arabia
Tel +966 126400000 ext. 21146
Fax +966 126951696
Email [email protected]
Background: Stroke is considered the second leading cause of death and the third leading cause of disability in the world. The incidence of stroke in Saudi Arabia is 43.8 per 100,000, due to the lack of knowledge and awareness of the population. This study intends to determine the level of stroke risk factor awareness among the Saudi population.
Methods: A cross-sectional study was conducted in Saudi Arabia on 898 participants older than 18 years old. The validated online survey was randomly distributed and consisted of 20 questions in both English and Arabic languages to evaluate the level of awareness of stroke risk factors among the population.
Results: A total of 898 participants completed the survey. The results showed that the median risk factor score was 5 (IQ 3– 8) out of 14. A total of 2.2% could recognize all 14 risk factors. Personal history of hypertension was chosen as a risk factor by the majority of the participants (81.7%) followed by personal history of stroke (74.1%) and personal history of dyslipidemia (57.2%).
Conclusion: This study showed that there is an insufficient level of stroke risk factor awareness in Saudi Arabia. More than half of the participants identified the term (stroke), while only 2.2% could recognize all 14 risk factors. Hence, public education is needed to identify people with stroke risk factors.
Keywords: stroke, awareness, risk factors, public education, Saudi Arabia
Introduction
Stroke is the second leading cause of death and the third leading cause of disability in the world.1 According to the recent statistics, nearly 15 million people experience a stroke each year, which resulted in more than 5 million deaths.2 Saudi Arabia is a rapidly developing country that evolved drastically in the past two decades, major lifestyle and environmental factors changed and increased the risk and incidence of stroke.3 The prevalence of stroke in the Kingdom of Saudi Arabia is 43.8 per 100,000 in which poor knowledge and awareness of the general public are contributing factors.4 Moreover, it is estimated that stroke constitutes 14,000 of total deaths in Saudi Arabia in 2012.2 A number of studies stated that the major risk factors for stroke are hypertension, diabetes mellitus, hyperlipidemia, smoking, ischemic heart diseases and obesity.3 It is well known that sedentary lifestyle including prolonged TV watching is also considered a risk factor that could lead to stroke.5 It is believed that stroke is a preventable disease if lifestyle and other modifiable risk factors were targeted by the community or on individual level.6
Globally, the incidence and prevalence of ischemic and hemorrhagic stroke events in 2013 were significantly greater in men than in women.7 In addition, a study conducted in Asser in 2018 reported a significant difference in the incidence of stroke among both males and females. The incidence of stroke in male is dominant in all age groups except in age group from 45 to 49, where females showed a higher incidence.8 Globally, individuals aged 25 years and above have approximately 25% tendency to develop a stroke.9 A study in the United States declared that there is a direct relationship between age and stroke, where the incidence of stroke doubles each decade after the age of 55 years.10 Moreover, a study in Asser stated that the incidence of stroke is 851.81 per 100,000 for patients aged 70 years or more.8 However, the level of stroke awareness in the community could potentially improve stroke outcome and improve public behavior.
There are many stroke risk factors known and reported in the literature. However, some of them are related to our daily life routine which is modifiable by increasing the knowledge about these practices. Due to the high prevalence of stroke in Saudi Arabia, there could be a lack of awareness among the community about the risk factors of stroke. This study aims to investigate the level of stroke risk factor awareness among the Saudi population.
Methods
A cross-sectional study was carried out at King Abdulaziz University Hospital. Ethical approval was obtained from the Institutional Review Board (IRB) at King Abdulaziz University Hospital, Jeddah, Saudi Arabia in accordance with the Declaration of Helsinki. The questionnaire was adopted from a previous study and validated on 12 people randomly.11 The study was conducted by distributing an online survey consisting of 20 questions in both English and Arabic languages to all individuals who were 18 years and older with no sex restriction, during a period of one week. Participants were selected through volunteer sampling. Information about the survey purpose and the expected time to finish was provided for each participant and an informed consent was signed before taking the survey. A contact email was provided for the participants in case any inquiries were needed regarding the survey. The questionnaire consisted of two sections: one to collect demographic characteristics and another for assessment of stroke risk factor awareness.
The demographic variables included were age, gender, nationality, province, marital status, level of education, occupation, and total income. Participants were asked regarding their health problems which included high blood pressure, cardiovascular disorder, diabetes mellitus, high cholesterol level and current smoking. Awareness of stroke risk factors was assessed by giving 14 risk factors to choose from. One point was assigned for awareness of each of the 14 previously mentioned risk factors; thus, the total score ranged from 0 to 14, with 0 being the lowest and 14 being the highest score. The 14 risk factors were smoking, lack of physical activity at least 3 minutes of walking 5 days per week, fast-food intake, soft drink intake, watching TV 4 hours or more per day, using computer devices for 4 hours or more per day, personal history of diabetes, personal history of stroke, personal history of heart attack diagnosed by a physician, family history of diabetes, personal history of hypertension, family history of hypertension, family history of hyperlipidemia, high cholesterol or triglyceride level, family history of coronary artery disease diagnosed by a physician. Participants were asked which gender and age groups are more susceptible to develop a stroke.
Data Analysis
Data were entered and analyzed using SPSS version 21. The analysis included qualitative data that were presented as frequency and percentage. The total risk factor score presented as median and interquartile range.
Results
A total of 898 participants completed the questionnaire. The demographic variables of the population surveyed are presented in (Table 1). Most of the respondents were females representing 69.3% of the total participants and 30.7% were males. Nearly half of the respondents aged between 20 and 30 years, represented by (48.8%), other participants were divided into 18–19 years (7.2%), 31–40 years (17.7%), 41–50 years (17.6%), 51–65 years (8.5%) and 66 years and above (0.1%). The majority of the participants were Saudi Arabian (93.0%), and only (7.0%) were non-Saudi. Most of the participants were from Makkah, Riyadh and Al-Sharqiyah regions (60.2%,16.2%, and 8.9%), respectively, and the remaining were from Al-Madinah (8.8%), Al-Bahah (1.3%), Asser (1.3%), Tabuk (1.3%), Qassim (0.9%), Hail (0.3%), Northern borders (0.2%), Jizan (0.2%) and Al-Jouf (0.2%). Regarding the marital status of the study population, 49.8% were married, 46.8% were single, and 3.3% were separated or divorced. The majority of the participants has a bachelor’s degree (65.3%), and the minority had a primary level of education (0.2%). Others had secondary level (16.8%), Masters or PhD (10.5%), and intermediate level (1.1%). The greater part of the participants was students representing (34.0%) of the total sample, followed by housewife (14.8%), education sector (14.8%), administrative sector (9.7%), health care sector (8.5%), retired not working (6.9%), engineering and industry sector (2.6%), business sector (2.6%), army and police sector (2.6%), technical and computer sector (1.6%), commerce sector (1.3%), research sector (0.7%). Participants total income was as follows: 35.8% receive >10,000 Saudi Riyals, almost equivalent to the participants who receive <3000 Saudi Riyals (35.2%), and 19.2% receive 5000–10,000 Saudi Riyals, while 9.8% of the participants receive 3000–5000 Saudi Riyals (Table 1).
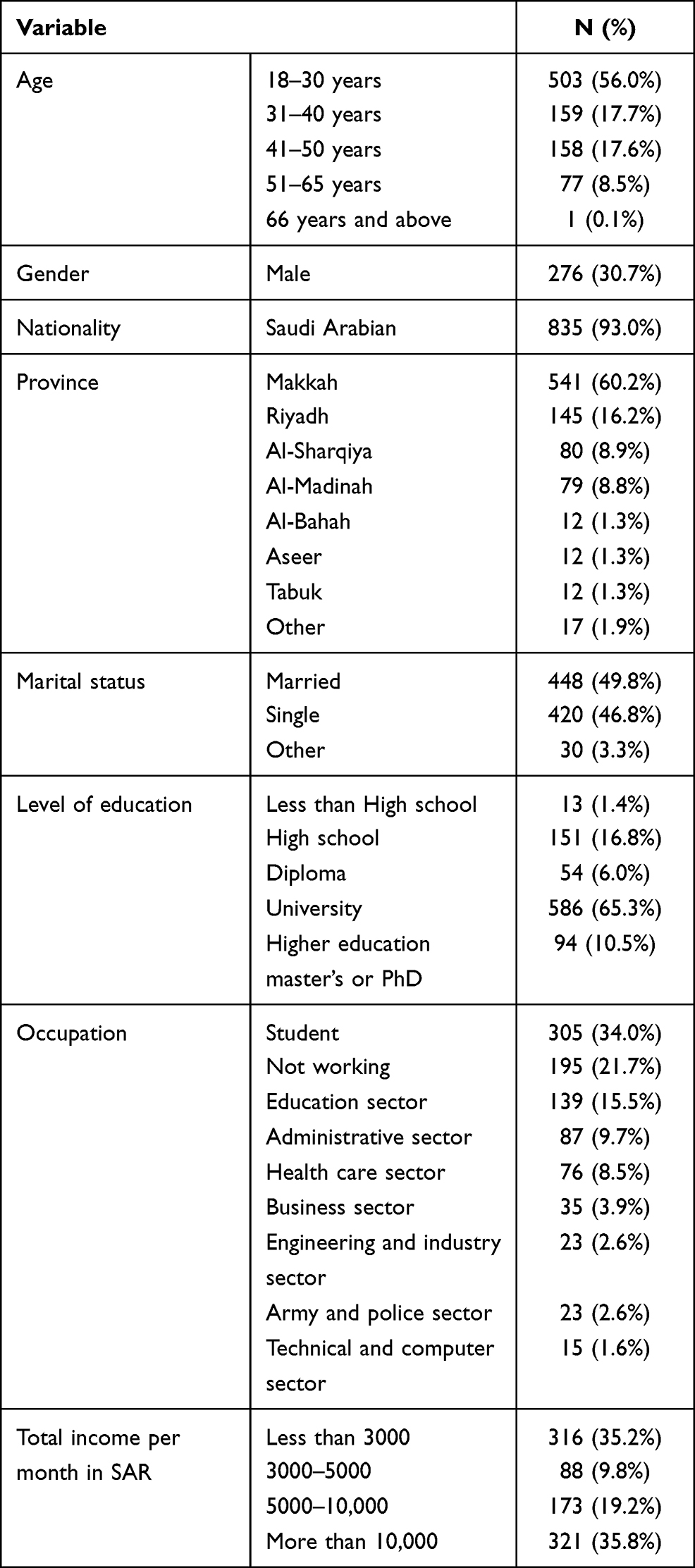 |
Table 1 Demographic Characteristics of Participants |
High blood pressure was determined as the major health problem of the participant representing (17.9%), followed by high cholesterol level (16.5%), diabetes mellitus (9.9%), cardiovascular disorder (4.9%) (Table 2). Concerning regular smoking for more than one year 83.5% of the participants did not smoke regularly, while 16.5% smoked regularly. The majority of the respondents (69.8%) had no family history of stroke, while only 20.2% of the respondents know a family member who has had a stroke, and 10.0% did not know if a family member has suffered a stroke before.
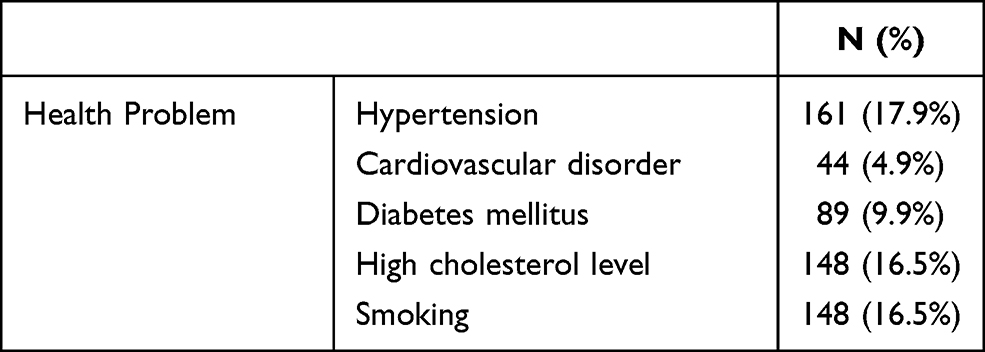 |
Table 2 Health Problems Among the Participants |
A large number of respondents thought that the risk of stroke was higher in individuals who are older than 50 years old (54.1%), while the rest chose the following: 30–50 years old (23.2%), did not know (18.7%), and older than 20 years old (4.0%). When asked which gender is more prone to stroke, 42.8% did not know which gender is more prone to develop stroke, 39.4% chose males as the higher risk group, 4.3% chose females and 13.5% thought that the risk is equal in both genders (Table 3). The participants were asked about 14 risk factors that could lead to stroke, personal history of hypertension was the most chosen factor (81.7%) followed by personal history of stroke (74.1%), family history of hyperlipidemia, high cholesterol or triglyceride level (57.2%), smoking (55.1%) (Table 4). The median (interquartile) of the total risk factor score was 5 (3–8) out of 14 (Figure 1).
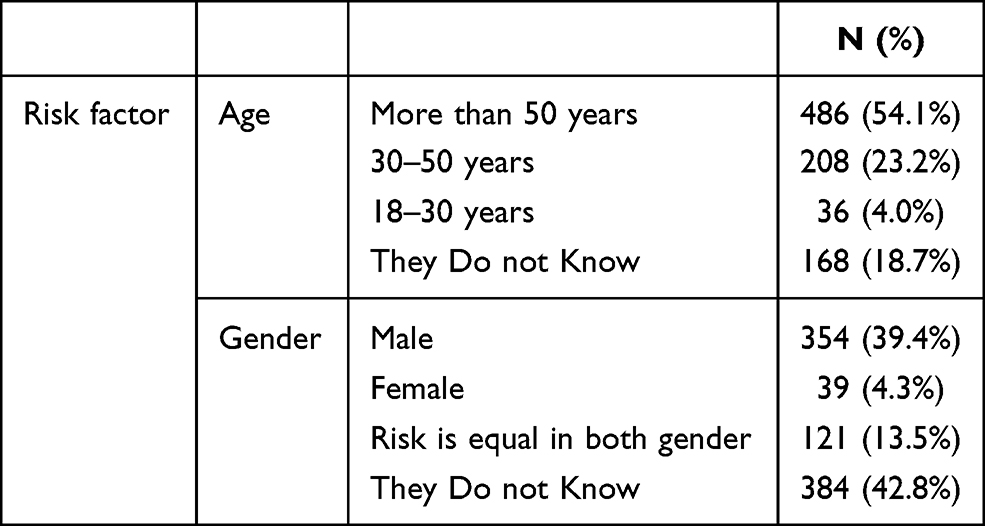 |
Table 3 Age and Gender Group at High Risk of Stroke |
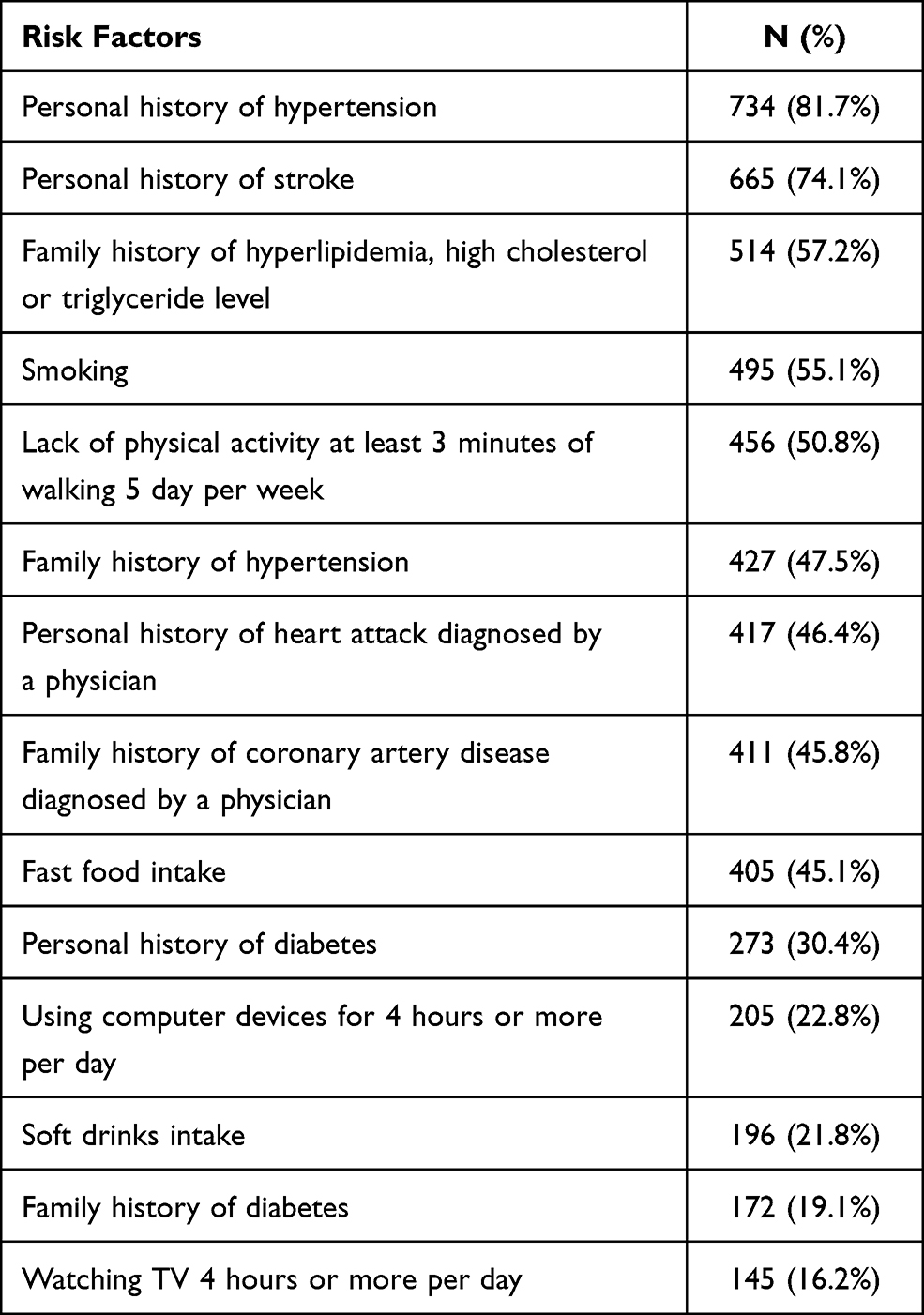 |
Table 4 Stroke Risk Factor Frequency |
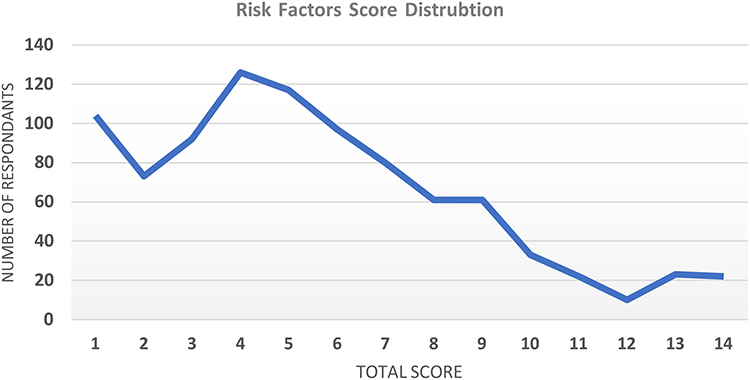 |
Figure 1 Frequency of risk factor score. |
Discussion
The results of this study showed that the Saudi Arabian population had limited information about the risk factors that could lead to a stroke. Although a larger number of the respondents were from either younger age and educated or students, the most health condition reported among them was hypertension. Importantly, the majority of participants were aware about hypertension as a risk factor to develop stroke.
More than half of the participants confirmed the US study results by declaring that the risk of stroke was higher in individuals who are older than 50 years old.10 This article found that 39.4% of the participants chose males as being more susceptible to having a stroke, while 4.3% chose females as being more susceptible. Notably, the majority of the participants in this study were females. Likewise, a study in Asser investigated the incidence of stroke and found that it was dominant in males.8 Unfortunately, the greater percentage of the participants (42.8%) did not know which gender is more prone to develop a stroke.
The participants were asked about 14 risk factors that could lead to stroke, personal history of hypertension was the most chosen factor (81.7%) which confirmed studies in Egypt and Italy that found hypertension was the most common risk factor recognized (73.0%) and (67.6%), respectively,7 whereas a study in Jeddah about coronary artery disease awareness used the same risk factors and the most chosen risk factor was fast-food intake (74.8%).12 However, the variation between the two results might be due to the difference between the two topics. Most of the participants (12.6%) recognized 5 out of 14 risk factors, while only 2.2% recognized all the 14 risk factors. This indicates an alarmingly low level of stroke risk factor knowledge. This is an unfortunate outcome due to the fact that almost all the risk factors of stroke are preventable. In a study done in New Zealand, both Asian and Pacific Island respondents were less likely to consider smoking as a risk factor, while in this study smoking was well recognized as a risk factor.11 Surprisingly, only (16.5%) of the participants smoked regularly for more than one year which was not expected, this could be due to the confusing character of the term “smoking”, since some individuals do not consider shisha/hookah and the newly emerged vaping devices (electronic cigarettes) as smoking.
The recognition of stroke risk factors is equally important to the knowledge of unified emergency number. This is to ensure rapid assessment and to reduce the delay in patient transportation time. Currently, Saudi Arabia has established unified emergency number 911 only in Makkah region.
The main limitations of this article were the inadequacy of the sample size, unequal distribution of the online survey across Saudi Arabia’s province, age groups and education levels, since the participants were not equal among the variables (age group, education level). As well as the predominance of female participants and students. Another limitation could be the fact that the data collection was conducted in a very short period of time. Moreover, no similar countrywide studies have been conducted in Saudi Arabia in terms of stroke risk factor knowledge. Hence, the results cannot be generalized to the entire population. Furthermore, the association between the level of education, income or occupation and the stroke risk factor awareness was not investigated in this paper.
The recommendation for future papers should include a well-distributed survey across both genders, age groups, provinces and different occupations. It is important to mention that the sample was small for the fact that it was a countrywide paper. Therefore, it should have included a larger group that is distributed among different provinces. There is a seemingly shortage in level of knowledge about stroke risk factors. Participants must be empowered with suitable education programs, campaigns, organization of national stroke training programs could improve the level of awareness. This article wishes to mention the urgent need to conduct more studies on stroke to determine a more recent percentage occurrence.
Conclusion
This study highlights the insufficient level of stroke risk factor awareness in Saudi Arabia. Limited number of participants could identify all the 14 risk factors. Stroke awareness should be implemented in our country due to its alarming level of incidence and preventable behavior.
Author Contributions
MAlshibani and SA designed the study. RB, RA, MB, SB, MA and RBajaba collected the data. MAlshibani, and SA double-checked the data collection. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare no conflicts of interest for this work.
References
1. Johnson W, Onuma O, Owolabi M, Sachdev S. Stroke: a global response is needed. Bull World Health Organ. 2016;94(9):634–A. doi:10.2471/BLT.16.181636
2. Al-Senani F, Al-Johani M, Salawati M, et al. An epidemiological model for first stroke in Saudi Arabia. J Stroke Cerebrovasc Dis. 2020;29(1):104465. doi:10.1016/j.jstrokecerebrovasdis.2019.104465
3. Alhijji B, Almahlawi A, Youssef M. Awareness of stroke symptomatology, risk factors, significance of acute management and prevention in AL-Madinah community. World J Pharm Res. 2018;7(15):33–46. doi:10.20959/wjpr201815-12978
4. Alaqeel A, AlAmmari A, AlSyefi N, Al-Hussain F, Mohammad Y. Stroke awareness in the Saudi community living in Riyadh: prompt public health measures must be implemented. J Stroke Cerebrovasc Dis. 2014;23(3):500–504. doi:10.1016/j.jstrokecerebrovasdis.2013.04.011
5. Pinto VJ, George P. Awareness on risk factors and warning signs of stroke among individuals with hypertension. J Evol Med Dent Sci. 2017;6(30):2410–2415. doi:10.14260/jemds/2017/520
6. Boehme AK, Esenwa C, Elkind MSV. Stroke risk factors, genetics, and prevention. Circ Res. 2017;120(3):472–495. doi:10.1161/CIRCRESAHA.116.308398
7. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
8. Alhazzani AA, Mahfouz AA, Abolyazid AY, et al. Study of stroke incidence in the Aseer Region, Southwestern Saudi Arabia. Int J Environ Res Public Health. 2018;15(2):215. doi:10.3390/ijerph15020215
9. Feigin VL, Nguyen G, Cercy K, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379(25):2429–2437. doi:10.1056/NEJMoa1804492
10. Ovbiagele B, Nguyen-Huynh MN. Stroke epidemiology: advancing our understanding of disease mechanism and therapy. Neurotherapeutics. 2011;8(3):319–329. doi:10.1007/s13311-011-0053-1
11. Kamran S, Bener AB, Deleu D, et al. The level of awareness of stroke risk factors and symptoms in the Gulf Cooperation Council countries: Gulf Cooperation Council stroke awareness study. Neuroepidemiology. 2007;29(3–4):235–242. doi:10.1159/000112856
12. Almalki MA, AlJishi MN, Khayat MA, et al. Population awareness of coronary artery disease risk factors in Jeddah, Saudi Arabia: a cross-sectional study. Int J Gen Med. 2019;12:63–70. doi:10.2147/IJGM.S184732
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.