")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Stress, Support, and Length of Diagnosis Among Women Living with HIV/AIDS in the Southern USA, During the COVID-19 Pandemic
Authors Montgomerie EK , Michel C , Sanchez-Covarrubias AP , Duthely LM
Received 1 September 2022
Accepted for publication 22 January 2023
Published 9 March 2023 Volume 2023:15 Pages 95—103
DOI https://doi.org/10.2147/HIV.S388307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Emily K Montgomerie,1 Cassandra Michel,2 Alex P Sanchez-Covarrubias,3 Lunthita M Duthely4,5
1Department of Neurology, Stroke Division, University of Miami Miller School of Medicine, Miami, FL, USA; 2School of Arts and Sciences, University of Miami, Coral Gables, FL, USA; 3Division of Gynecologic Oncology, Sylvester Comprehensive Cancer Center, University of Miami Miller School of Medicine, Miami, FL, USA; 4Department of Obstetrics, Gynecology and Reproductive Science, Division of Research and Special Projects, University of Miami Miller School of Medicine, Miami, FL, USA; 5Department of Public Health Sciences, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Lunthita M Duthely, University of Miami, Miller School of Medicine, Department of Obstetrics, Gynecology and Reproductive Sciences, 1120 NW 14th Street, CRB 1162, Miami, FL, 33136, USA, Tel +1-305-243-5800, Fax +1-305-243-1730, Email [email protected]
Background: Health-related challenges caused and worsened by the global COVID-19 pandemic have proven broad and multifaceted, particularly for racial/ethnic minority women living with HIV (WLWH). The 2020 pandemic has affected the wellbeing and access to care for WLWH in Southeastern Florida, a region that experienced simultaneous high rates of COVID-19 and HIV. WLWH, over a short- or long-term period, likely utilize different coping mechanisms as they face these challenges.
Methods: This analysis compared pandemic-related stress and support endorsed by participants attending an urban clinic in South Florida, from January through May 2021. Participants completed an adapted version of the Pandemic Stress Index (PSI). The items in the PSI assessed emotional distress, stigma, and support, and were dichotomized, as either “stress” or “support”. Mann–Whitney U-test assessed differences in distributions of PSI scores (stress and support) comparing long-term survivors (≥ 10 years with an HIV diagnosis) to those more recently diagnosed (< 10 years).
Results: The cohort consisted of 63 WLWH, aged 21– 71 (Mean = 42 years± 12.95). The group of WLWH were almost evenly split, with 50.8% having been diagnosed in the last 10 years (short-term survivors). The high-stress group endorsed lower levels of support, compared to the low-stress group. There was a non-significant trend of higher stress scores for short-term survivors, compared to long-term survivors; and, higher support scores for long-term survivors, compared to short-term survivors.
Conclusion: Results suggest a trend in long-term survivor WLWH endorsing lower stress and higher support; the contrary was found for their short-term survivor counterparts. Patterns in COVID-19 related stressors and maladaptive behaviors need further exploration to establish suitable interventions that address disparities within groups of WLWH.
Keywords: HIV, COVID-19, HIV-positive duration, Stress, Support
Introduction
The prolonged impact of the global COVID-19 pandemic (pandemic) and subsequent lifestyle changes on the mental health of the general population, is still under investigation;1 however, the burdens dealt by people living with HIV (PLWH) due to the pandemic are thought to have surpassed those of the general population.2–5 Health-related challenges caused and worsened by the pandemic are broad and multifaceted, particularly for racial/ethnic minority women living with HIV (WLWH).6 Increased stress and decreased well-being among WLWH have been attributed to social isolation, changes in routine, and economic instability.7–10 In Southeastern FL, a region that simultaneously experienced high infection rates of HIV and SARS-CoV-2, the virus that causes COVID-19, racial/ethnic minority women, compared to men, reported higher levels of stress and domestic instability during the height of the pandemic.11–13 The sustained impact of limited access to care for WLWH in Southeastern FL has been previously documented.14 Social support, which has the potential to mitigate risk factors such as stress and instability,15–17 may also be more abundant among long-term survivor WLWH.18,19
Previously published data from online surveys, disseminated at the beginning stages of the pandemic, documented stress and other negative subjective experiences among WLWH.7,14,20 Jones et al found that women in Southeastern FL experienced significantly higher levels of stress, compared to men, and reported losing mental health care and childcare support and services in the latter half of 2020. To our knowledge, the Pandemic Stress Index (PSI) was the only available vetted measure intended to identify the unique impacts of COVID-19 on HIV positive populations, and was previously implemented among vulnerable populations in Southeastern FL during the early stages of the pandemic. The PSI captures behavior changes and stressors, in response to COVID-19.21,22
Length of HIV diagnosis is an important factor to understand the mental health and HIV-related health challenges of those living with HIV. Prior to being under virologic control, newly diagnosed PLWH confront multiple barriers to care, as systemic failures throughout the health-care system prevent providers from allocating the proper resources to persons newly diagnosed with HIV.23
Newly diagnosed persons living with HIV predictably report higher levels of symptoms, opportunistic infections, and side effects from new use of antiretrovirals (ART).24 For those living with HIV for less than 10 years, severe fatigue, which is associated with a host of physiological and psychological challenges that come with a new chronic diagnosis,25–27 is common. Other studies reported that emotional distress caused by the pandemic affected adherence and retention, especially among newly diagnosed PLWH.28–30
Long-term survivors, or individuals who have lived with HIV for several years, are at higher risk of multiple co-morbidities31,32, more severe premature aging and cognitive dysfunction when living with HIV for longer than 10 years – independent of age in years.27 Among those living with HIV for longer than 10 years, higher levels of HIV stigma, and social isolation31,32 were reported, as well. The pandemic has led to changes in well-being, including disruptions in normal sleep patterns, increased anxiety and increased experiences of loneliness and depression.15 Other factors include a reduction in sexual activity and personal financial loss, among long-term survivors of HIV.15 It was reported that advanced physiological age, due to living with the virus and prolonged use of ART, accompanied by co-morbidities, psychosocial issues, and barriers to engagement to care, were exacerbated by the pandemic.18 It was also reported that long-term survivors experienced delayed access to ART medication during this time.7,33 Taken together, length of time living with HIV is an important factor to consider, when analyzing psycho-social data related to the COVID-19 pandemic.
Dichotomizing the duration of HIV diagnosis into acute (short-term) and chronic (long-term) cases may help reveal trends among subpopulations of WLWH and possible areas of intervention. A previous study investigating the association between years living with HIV and symptomology, using cumulative distribution among national citizens, found that long-term survivors did not experience more severe symptoms compared to short-term survivors.27 However, long-term survivors from this study were more likely to experience confusion, suggesting a greater need for cognitive resources.27 Previous research also distinguishes short and long duration HIV cutoffs with sample-specific medians or with the dependent variable in question. One study found amyloid deposition, which is implicated in Alzheimer’s disease, significantly increased after 15 years of living with HIV, revealing further the value in establishing HIV duration cutoffs for data analysis.34 Differences by subpopulations may inform interventions aimed at mitigating the effects of stress caused by the current or future pandemics.
This purpose of the study was to investigate the burden of the COVID-19 pandemic, by surveying levels of stress and support among WLWH, dichotomizing the data by duration of living with HIV, i.e., <10 years vs ≥10 years. Due to the exploratory nature of the analyses, formal hypotheses were not constructed; however, expected outcomes were based on the existing literature.15,18,35
Methods
Study Setting and Population
The authors’ institutional IRB (IRB#20170287) approved the study protocol, which was funded by several sources (see Funding). Women attending a women’s HIV clinic in a tertiary, safety net hospital in Southeastern Florida were surveyed between January and May 2021. Participants were approached and consented to complete the survey while waiting to be seen for primary care, gynecological care, or obstetrical services. All female participants attending the HIV clinics were approached by trained clinic staff who administered the survey. Approximately 750 women are seen at this HIV clinic annually.
Measures
Participants completed the Pandemic Stress Index (PSI), a three-item instrument, used to operationalize the effect of the pandemic.21,22 With the nature of COVID-19 and pandemic conditions taking a significant toll on research, there was an urgent need to find an efficient tool which captured sentiments toward the pandemic. The PSI served as a framework for future exploratory analysis encompassing psychosocial, financial, domestic, and physiological implications of the COVID-19 pandemic. The PSI assessed self-reported experiences during the pandemic and was available English, Spanish,21 and Haitian Creole.36
Scoring the PSI Scale
The PSI consisted of three items. This analysis included responses for the last item of the survey: “Which of the following are you experiencing (or did you experience) during COVID-19 (coronavirus).” This question was followed by a checklist of items, including fear during the pandemic, understanding the pandemic, stigma, discrimination, financial loss, substance use, sleep pattern changes, sexual activity changes, and social and financial support. Each item was dichotomized to “yes”/“no” responses, collapsed, and added to either the “stress” or “support” score. A point was allocated to the stress or support score if the participant selected the construct-specific item such that they could receive 0–14 points for stress and 0–3 points for support. To evaluate the effects of the pandemic on the patients attending the women’s clinics, the PSI was adapted to include questions related to pregnancy; however, these questions were excluded from the current analysis.
Statistical Analysis
We conducted statistical analysis in SPSS (v.26) and R (v 4.1). The median length of years living with HIV was 10 years for the current sample and analyses were executed at both 5-year and 10-year cutoffs. Scores from the stress and support constructs were compared, independently, between the two groups (short versus long-term HIV survivors), using the two-tailed, Mann–Whitney U-test, at alpha = 0.05.
Results
A total of 66 PSI surveys were administered. The mean age of women was 42 years (SD = 12.95). Three participants were excluded from the analysis due to missing dates of diagnosis. The majority (65.1%) were long-term survivors of HIV, with a diagnosis date of 5 years or more from the date of their visit. The group was nearly evenly split at 10 years since their HIV diagnosis; 54% of women had been living with HIV less than 10 years. Participant demographic information is detailed in Table 1.
 |
Table 1 Participant Demographic and Clinical Information |
A Mann–Whitney U-Test was run to determine if there were differences in stress and support scores, comparing long-term to shorter-term survivors of HIV. Distributions of the stress and support scores for both respective groups were not similar, as assessed by visual inspection. At the 10-year split, stress scores for short-term survivors (mean rank = 32.87) were slightly higher, compared to long-term survivors (mean rank = 31.16); the differences, however, were not significant (U = 469, z = −0.377, p = 0.706), using an exact sampling distribution for the U.37 The 10-year split for support scores showed the contrary, where support scores for short-term survivors were lower (mean rank = 30.82), compared to long-term survivors (mean rank = 33.14); the differences, however, were not significant (U = 532.5, z = 0.574, p = 0.566).37
The box plot in Figure 1 summarizes the Mann Whitney test, by comparing the two groups side by side. Figure 1A and B present stress scores for 10 year and 5 year cut offs of the sample, while panel C and D present support scores for 10 year and 5 year cut offs, respectively. In summary, women who are long-term survivors of HIV endorsed slightly lower stress and higher support, compared to short-term survivors of HIV—differences, however, were not significant.
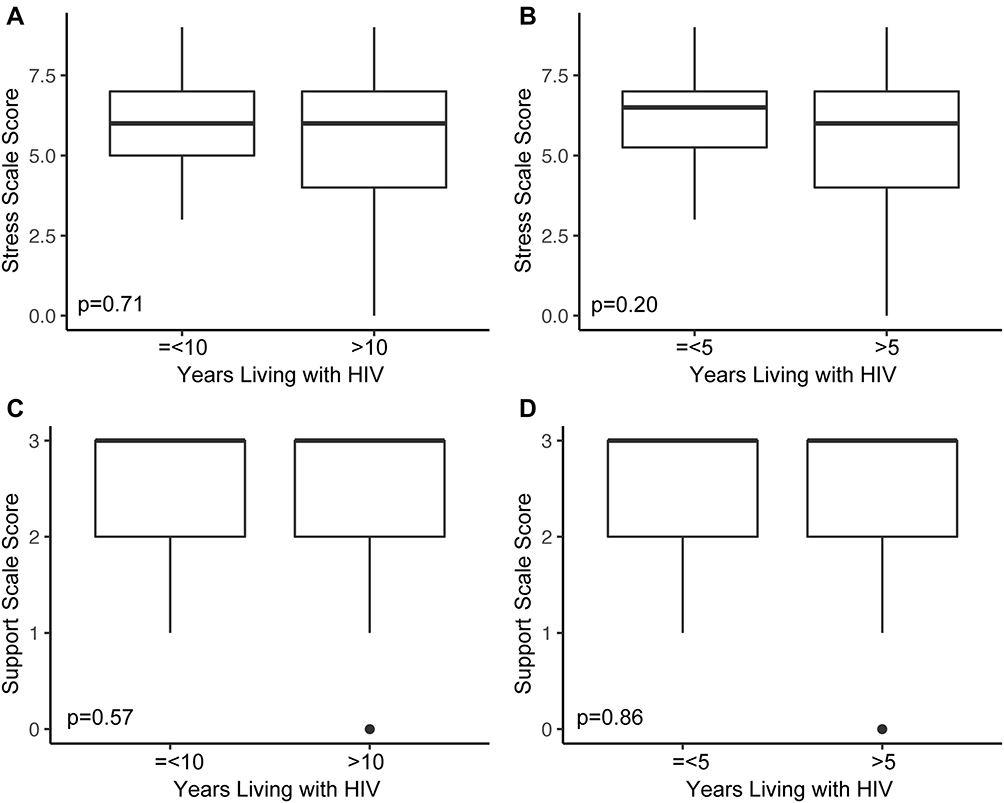 |
Figure 1 Box plots of PSI stress (A and B) and Support (C and D) scores, comparing 5 and 10-year Diagnosis Groups. |
Discussion
In a large cohort evaluating mental health among PLWH in Argentina and Southeastern FL, Jones et al found that social support and resilience contributed to lower depressive symptoms for PLWH in Argentina during the early stages of the pandemic.16 Comparatively, Wion et al reported increases in stress and decreases in social support, when comparing pre- and peri-pandemic symptoms for PLWH during April 2020. Algarin et al surveyed stress in older PLWH living in Southeastern FL during the period of social distancing. The average stress score reported by this sample was 4.4±3.3 out of 10 and, most often, stress was due to exposures to the SARS-CoV-2 virus, the adjustment to social distancing, and financial issues.33
Wion et al measured stress, using the NIH Toolbox Item Bank Fixed Form v. 20, which corresponded to 10 items that were scored on a 1–5 Likert scale, where a total of 50 meant greater stress.38 The same survey measured social support using items comparing pre- and post-pandemic life.7 Jones et al used the Perceived Stress Scale, which is scored on a 5-point Likert scale, and surveyed social support, using one question on a similar 5-point Likert satisfaction scale.14,16 Algarin et al used a self-evaluation to measure stress from 1 to 10, based on an open-ended question on what was most stressful. The first published study that examined the impact of the COVID-19 pandemic, using the PSI, found that Latino sexual minority men living in Miami experienced stress due to being worried about family, friends, and personal financial loss, which was attributable to the pandemic.21 Regardless of whether individuals are directly impacted by HIV, feelings of stress were reported using this simple instrument. The PSI helped to reveal a possible disparity that exists between short- and long-term HIV diagnosis groups and their response to the COVID-19 pandemic.
The data in this analysis is derived from women who were surveyed in-person at their HIV clinic appointments from January through May of 2021. To provide context, this was around the time Florida Governor declared Phase 3 of the “Plan for Florida’s Recovery”, ie., Florida’s COVID response plan, which lifted all restrictions on businesses, ultimately rescinding the state of emergency in May 2021.39 The pandemic restrictions had since been challenged by the Governor, who openly criticized mask mandates as an infringement of personal freedoms.39 Perhaps this political climate, along with the early efforts to normalize the COVID situation in Florida, compared to the rest of the nation, allowed for most of the WLWH surveyed in this sample to exhibit signs of resilience even in the context of worsening mental health.40
Three quarters of the women in this sample identified as Black or more than one race; therefore, much, if not all, of this sample was vulnerable to preexisting health disparities due to genetic and biological risk factors.12,41 This susceptibility is compounded by the structural disparities faced by racial/ethnic minority women, such as augmenting power differentials, loss of agency at home, and increased chronic stress.9,11 The PSI documented stress, with items like fear of getting COVID-19, fear of giving it to someone else, and worry for other loved ones. Women, who are often ascribed structural roles within the home, like caregiving, are disproportionately affected by chronic stress due to their primary role as domestic caregivers.11,42
Previous findings on the associations between HIV-positive duration and health outcomes associated with the COVID-19 pandemic are inconclusive but more research exploring the outcomes of pandemic-related stress and support among these subgroups is warranted.26,27 Distress due to the disruption caused by the COVID-19 pandemic has been reported for both those newly diagnosed and PLWH for a longer-term.28 The nuanced experiences of PLWH over a short- or long-term, during, and long after, the COVID-19 pandemic has subsided, could inform tailored health interventions. The familiarity of living with HIV may provide a buffer during difficult times, even when control of the HIV epidemic is threatened, due to reduced treatment access and prevention services.15,43 Similarly, the mental health crisis experienced throughout the world, due to the COVID-19 pandemic in addition to loss of routine social support among PLWH, may have contributed to higher rates of chronic stress, regardless of length of diagnosis.44
It is important to mention that although stress has negative psycho-social consequences, it can also be a facilitator toward mental well-being for WLWH.45 In fact, Siegel et al used an explanatory model to examine stress-related growth among WLWH. They found that, despite its negative connotations, stress, in conjunction with social resources, specifically, emotional support, helped facilitate growth. Similarly, in the current study, long-term survivors endorsed higher levels of support, which may have led to lower perceived stress. This may be a product of having broader support networks, as long-term survivors have navigated living with HIV for a longer period of time than short-term survivors, who may still potentially be creating their support network and developing coping strategies related to their health.
Challenges and Solutions
The flexibility of assessing pandemic stress with the PSI, and the fact that this analysis was exploratory, revealed the challenge of scaling a new measure and finding the best method of analysis. There were some variables in the PSI that could have subjectively added to either the stress or support score. Changes to sleep patterns or sexual activity may have been interpreted as a positive or negative consequence of the pandemic. There was also nuance in whether financial support from others could be considered stressful due to the expectation of repayment. These answers could have been accounted for by adding a point to the stress measure for endorsing an objectively bad scenario and deducting a point if it was not selected. In the current analysis, a point was added to the stress construct if a change in finances was selected. The last question in the survey was open-ended and participants were asked to describe the challenges faced during the pandemic. Unequivocal responses to this question such as “things [got] better after moving in with mom”, and “COVID has not affected me negatively”, made categorizing them into the stress or support score more straightforward.
Other limitations were the small sample size, which limits the ability to generalize the results to experiences in other areas, as the results surveyed the experiences of WLWH in the Southeastern United States. The women in the sample were recruited from a health-care setting which may imply healthier outcomes compared to WLWH who are not linked to regular HIV care. Additionally, this survey provided only one open-ended question, which may not have been enough to provide a comprehensive scope of the causes of stress and support. Future efforts may pivot to including a qualitative piece to the PSI that captures more details of individual experiences. The PSI is generally subjective in its use of self-report to measure stress and support; nonetheless, the PSI provides a simple measure that easily assesses the impact of COVID-19, and may be useful as an efficient and comprehensive evaluation of stress and support during future pandemics.
Conclusion
To address the needs presented by the women who attended a women’s HIV clinic, participants were surveyed using pandemic-related stress instruments. The analysis revealed a pattern, though not statistically significant, of short-term survivors endorsing higher levels of stress, compared to their counterparts. As such, concomitant coping strategies that are common among this vulnerable community need further comparison. Similarly, the analysis contradicted the hypothesized levels of social support as endorsed by the women attending this clinic. We believed that there would be a significant difference found and short-term survivor WLWH would endorse less support than their counterparts. The data, though not significant, revealed a pattern: women who were long-term survivors had slightly lower levels of stress and slightly more support, compared to women who had been living with HIV for a shorter period.
Although the present findings do not allow causal conclusions, they add to the growing body of evidence investigating the complex impacts of the COVID-19 pandemic on racial/ethnic minority WLWH.46–48 Future aims would require a system-level evaluation of the COVID-19 pandemic on PLWH—specifically, the social, political, and economic influence of the pandemic on the HIV experience, and how inter-connected factors affect the health of racial/ethnic minority WLWH living in the United States.43 Examining how living with HIV for short- and long-term durations may influence stress and support levels can provide insight to future health needs and help address health disparities among WLWH. As such, the HIV population continues to age and if effective coping strategies, such as relying on support networks helps to maintain healthy outlooks, then support groups should be funded and prioritized.
As stated above, further exploration with the PSI is warranted to inform tailored support services and interventions to improve health and well-being, during this and future public health pandemics.
Acknowledgments
The authors would like to acknowledge the patients who contributed to this survey and the individuals who contributed to data collection and data management, namely Mara Chavannes and William Billings. We would like to thank the University’s Writing Center for their assistance with editing this manuscript. This analysis was presented, in part, on October 13, 2021 at the San Francisco Center for AIDS Research (CFAR) virtual meeting.
Funding
Part of this study was financed by the Health Resources and Services Administrations (HRSA) Ryan White Part D funding stream, which pays in part for the care and treatment of patients whose data is included in this study. It was also funded by HRSA Ryan White Part C: COVID-19 Response Supplemental funding (H7CHA37137). HRSA funds the services provided by physicians, nurse practitioners, and nurses. Lunthita Duthely was partially funded through an Institutional KL2 (KL2TR002737), the Miami CFAR (P30AI073961), and an NIH NIDA (R34DA057150) award.
Disclosure
The author’s report no conflicts of interest related to this work.
References
1. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. 2020;52:102066. doi:10.1016/j.ajp.2020.102066
2. Spinelli MA, Brown LB, Glidden DV, et al. SARS-CoV-2 incidence, testing rates, and severe COVID-19 outcomes among people with and without HIV. AIDS. 2021;35(15):2545–2547. doi:10.1097/QAD.0000000000003075
3. Fields EL, Copeland R, Hopkins E. Same script, different viruses: HIV and COVID-19 in US Black communities. Lancet. 2021;397(10279):1040–1042. doi:10.1016/S0140-6736(20)32522-8
4. Millett GA. New pathogen, same disparities: why COVID-19 and HIV remain prevalent in U.S. communities of colour and implications for ending the HIV epidemic. J Int AIDS Soc. 2020;23(11):e25639. doi:10.1002/jia2.25639
5. Lesko CR, Bengtson AM. HIV and COVID-19: intersecting epidemics with many unknowns. Am J Epidemiol. 2021;190(1):10–16. doi:10.1093/aje/kwaa158
6. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
7. Wion RK, Miller WR. The impact of COVID-19 on HIV self-management, affective symptoms, and stress in people living with HIV in the United States. AIDS Behav. 2021;25(9):3034–3044. doi:10.1007/s10461-021-03335-4
8. Bigalke JA, Greenlund IM, Carter JR. Sex differences in self-report anxiety and sleep quality during COVID-19 stay-at-home orders. Biol Sex Differ. 2020;11(1):56. doi:10.1186/s13293-020-00333-4
9. Collins C, Landivar LC, Ruppanner L, Scarborough WJ. COVID-19 and the gender gap in work hours. Gend Work Organ. 2020;28(Suppl 1):101–112. doi:10.1111/gwao.12506
10. Sharma N, Vaish H. Impact of COVID - 19 on mental health and physical load on women professionals: an online cross-sectional survey. Health Care Women Int. 2020;1–18. doi:10.1080/07399332.2020.1825441
11. Connor J, Madhavan S, Mokashi M, et al. Health risks and outcomes that disproportionately affect women during the Covid-19 pandemic: a review. Soc Sci Med. 2020;266:113364. doi:10.1016/j.socscimed.2020.113364
12. Phillips N, Park IW, Robinson JR, Jones HP. The perfect storm: COVID-19 health disparities in US blacks. J Racial Ethn Health Disparities. 2020;8(5):1153–1160. doi:10.1007/s40615-020-00871-y
13. Waterfield KC, Shah GH, Etheredge GD, Ikhile O. Consequences of COVID-19 crisis for persons with HIV: the impact of social determinants of health. Bmc Public Health. 2021;21(1). doi:10.1186/s12889-021-10296-9
14. Jones DL, Rodriguez VJ, Salazar AS, et al. Sex differences in the association between stress, loneliness, and COVID-19 burden among people with HIV in the United States. AIDS Res Hum Retroviruses. 2021;37(4):314–321. doi:10.1089/AID.2020.0289
15. Gwadz M, Campos S, Freeman R, et al. Black and latino persons living with HIV evidence risk and resilience in the context of COVID-19: a mixed-methods study of the early phase of the pandemic. AIDS Behav. 2021;25(5):1340–1360. doi:10.1007/s10461-021-03177-0
16. Jones DL, Ballivian J, Rodriguez VJ, et al. Mental health, coping, and social support among people living with HIV in the Americas: a comparative study between Argentina and the USA during the SARS-CoV-2 pandemic. AIDS Behav. 2021;25(8):2391–2399. doi:10.1007/s10461-021-03201-3
17. Friedman MR, Coulter RWS, Silvestre AJ, et al. Someone to count on: social support as an effect modifier of viral load suppression in a prospective cohort study. AIDS Care. 2017;29(4):469–480. doi:10.1080/09540121.2016.1211614
18. Gwadz M, Cleland CM, Freeman R, et al. Stopping, starting, and sustaining HIV antiretroviral therapy: a mixed-methods exploration among African American/Black and Latino long-term survivors of HIV in an urban context. Bmc Public Health. 2021;21(1):419. doi:10.1186/s12889-021-10464-x
19. Buscher AL, Giordano TP. Gaps in knowledge in caring for HIV survivors long-term. JAMA. 2010;304(3):340–341. doi:10.1001/jama.2010.870
20. Parisi CE, Varma DS, Wang Y, et al. Changes in mental health among people with HIV during the COVID-19 pandemic: qualitative and quantitative perspectives. AIDS Behav. 2022;26(6):1980–1991. doi:10.1007/s10461-021-03547-8
21. Harkness A, Behar-Zusman V, Safren SA. Understanding the impact of COVID-19 on latino sexual minority men in a US HIV hot spot. AIDS Behav. 2020;24(7):2017–2023. doi:10.1007/s10461-020-02862-w
22. Harkness A, Weinstein ER, Mayo D, Rodriguez-Diaz C, Safren SA. Latinx sexual minority men’s behavioral, psychosocial, and medical experiences during COVID-19: differences across immigration statuses. Ann LGBTQ Public Popul Health. 2021;2(2):104–115. doi:10.1891/lgbtq-2020-0054
23. Pinto RM, Park S. COVID-19 pandemic disrupts HIV continuum of care and prevention: implications for research and practice concerning community-based organizations and frontline providers. AIDS Behav. 2020;24(9):2486–2489. doi:10.1007/s10461-020-02893-3
24. Zhu Z, Zhao R, Hu Y. Symptom clusters in people living with HIV: a systematic review. J Pain Symptom Manage. 2019;58(1):115–133. doi:10.1016/j.jpainsymman.2019.03.018
25. Huang Y, Luo D, Chen X, Zhang D, Huang Z, Xiao S. HIV-related stress experienced by newly diagnosed people living with HIV in China: a 1-year longitudinal study. Int J Environ Res Public Health. 2020;17(8). doi:10.3390/ijerph17082681
26. Xiao X, Reynolds NR, Saligan L, Lei Y, Wang M, Wang H. Effectiveness of non-pharmacological interventions to decrease fatigue in people living with HIV/AIDS: a protocol of systematic review and meta-analysis. BMJ Open. 2020;10(9):e040996. doi:10.1136/bmjopen-2020-040996
27. Zhu Z, Wen H, Yang Z, et al. Evolving symptom networks in relation to HIV-positive duration among people living with HIV: a network analysis. Int J Infect Dis. 2021;108:503–509. doi:10.1016/j.ijid.2021.05.084
28. Brown LB, Spinelli MA, Gandhi M. The interplay between HIV and COVID-19: summary of the data and responses to date. Curr Opin HIV AIDS. 2021;16(1):63–73. doi:10.1097/COH.0000000000000659
29. Devlin SA, Johnson AK, McNulty MC, Joseph OL, Hall A, Ridgway JP. ”Even if I’m undetectable, I just feel like I would die”: a qualitative study to understand the psychological and socioeconomic impacts of the COVID-19 pandemic on women living with HIV (WLWH) in Chicago, IL. BMC Womens Health. 2022;22(1):218. doi:10.1186/s12905-022-01812-z
30. Ogueji IA. People newly diagnosed with HIV during the COVID-19 pandemic: a focus group study on the associated early biopsychosocial reactions. J HIV AIDS Soc Serv. 2021;20(3):209–227. doi:10.1080/15381501.2021.1955800
31. Brown MJ, Weissman SB. The impact of COVID-19 on older adults living with HIV: HIV care and psychosocial effects. J Gerontol Soc Work. 2020;63(6–7):602–606. doi:10.1080/01634372.2020.1799281
32. Villar-Loubet OM, Illa L, Echenique M, et al. Prenatal and mental health care among trauma-exposed, HIV-infected, pregnant women in the United States. J Assoc Nurses AIDS Care. 2014;25(1 Suppl):S50–61. doi:10.1016/j.jana.2013.06.006
33. Algarin AB, Varas-Rodriguez E, Valdivia C, et al. Symptoms, stress, and HIV-related care among older people living with HIV during the COVID-19 pandemic, Miami, Florida. AIDS Behav. 2020;24(8):2236–2238. doi:10.1007/s10461-020-02869-3
34. Morgello S, Cortes EP, Gensler G, et al. HIV disease duration, but not active brain infection, predicts cortical amyloid beta deposition. AIDS. 2021;35(9):1403–1412. doi:10.1097/QAD.0000000000002893
35. Freeman R, Gwadz M, Wilton L, et al. Understanding long-term HIV survivorship among African American/Black and Latinx persons living with HIV in the United States: a qualitative exploration through the lens of symbolic violence. Int J Equity Health. 2020;19(1):146. doi:10.1186/s12939-020-01253-w
36. Duthely LM, Wagner L, Thomas TES. Endis Estrès Pandemi –Haitian Creole Version of the Pandemic Stress Index. University of Miami; 2020.
37. Dinneen LC, Blakesley BC. A generator for the sampling distribution of the Mann‐Whitney U statistic. J R Stat Soc C. 1973;22(2):4. doi:10.2307/2346934
38. Salsman JM, Butt Z, Pilkonis PA, et al. Emotion assessment using the NIH Toolbox. Neurology. 2013;80(11 Suppl 3):S76–86. doi:10.1212/WNL.0b013e3182872e11
39. Weissert CS, Uttermark MJ, Mackie KR, Artiles A. Governors in control: executive orders, state-local preemption, and the COVID-19 pandemic. Publius. 2021;51(3):396–428. doi:10.1093/publius/pjab013
40. Ballivian J, Alcaide ML, Cecchini D, Jones DL, Abbamonte JM, Cassetti I. Impact of COVID-19-related stress and lockdown on mental health among people living with HIV in Argentina. J Acquir Immune Defic Syndr. 2020;85(4):475–482. doi:10.1097/QAI.0000000000002493
41. McKnight-Eily LR, Okoro CA, Strine TW, et al. Racial and ethnic disparities in the prevalence of stress and worry, mental health conditions, and increased substance use among adults during the COVID-19 pandemic - United States, April and May 2020. MMWR Morb Mortal Wkly Rep. 2021;70(5):162–166. doi:10.15585/mmwr.mm7005a3
42. Thibaut F, van Wijngaarden-Cremers PJM. Women’s mental health in the time of Covid-19 pandemic. Front Glob Womens Health. 2020;1:588372. doi:10.3389/fgwh.2020.588372
43. Brown LL, Martin EG, Knudsen HK, Gotham HJ, Garner BR. Resilience-focused HIV care to promote psychological well-being during COVID-19 and other catastrophes. Front Public Health. 2021;9:705573. doi:10.3389/fpubh.2021.705573
44. Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJG. COVID stress syndrome: concept, structure, and correlates. Depress Anxiety. 2020;37(8):706–714. doi:10.1002/da.23071
45. Siegel K, Schrimshaw EW, Pretter S. Stress-related growth among women living with HIV/AIDS: examination of an explanatory model. J Behav Med. 2005;28(5):403–414. doi:10.1007/s10865-005-9015-6
46. Boes S, Sabariego C, Bickenbach J, Stucki G. How to capture the individual and societal impacts of syndemics: the lived experience of COVID-19. BMJ Glob Health. 2021;6(10):e006735. doi:10.1136/bmjgh-2021-006735
47. Shiau S, Krause KD, Valera P, Swaminathan S, Halkitis PN. The burden of COVID-19 in people living with HIV: a syndemic perspective. AIDS Behav. 2020;24(8):2244–2249. doi:10.1007/s10461-020-02871-9
48. Chenneville T, Gabbidon K, Hanson P, Holyfield C. The impact of COVID-19 on HIV treatment and Research: a call to action. Int J Environ Res Public Health. 2020;17(12). doi:10.3390/ijerph17124548
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.