Back to Journals » Journal of Pain Research » Volume 15
Stress Mediates the Association Between Pain and Alcohol Use in College Students
Authors Bush NJ ![]() , Schick MR, Spillane NS, Boissoneault J
, Schick MR, Spillane NS, Boissoneault J
Received 30 November 2021
Accepted for publication 19 February 2022
Published 23 March 2022 Volume 2022:15 Pages 757—766
DOI https://doi.org/10.2147/JPR.S351837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Nicholas J Bush,1 Melissa R Schick,1 Nichea S Spillane,1 Jeff Boissoneault2
1Department of Psychology, University of Rhode Island, Kingston, RI, USA; 2Department of Clinical and Health Psychology, University of Florida, Gainesville, FL, USA
Correspondence: Nichea S Spillane, Department of Psychology, University of Rhode Island, 130 Flagg Road, Kingston, RI, 02881, USA, Tel +1 401-874-4252, Email [email protected]
Background: Alcohol use in young adults is highly prevalent and associated with numerous consequences, including academic difficulties and motor vehicle accidents. Pain is one factor that has been increasingly shown to be associated with higher rates of alcohol consumption and riskier patterns of drinking among undergraduate students. Although pain has traditionally been viewed as a lesser concern for young adults, current research demonstrates that pain may be more prevalent in younger populations than originally thought. However, little is known about how common psychosocial factors, such as stress and subjective social status (SSS), influence the association between pain and alcohol consumption in college students.
Objective: The study’s goal was to examine the effect of stress and SSS on the relationship between pain and alcohol consumption.
Participants and Methods: Participants (N = 445, 39.3% women, Mage= 22.98) were 18- to 25-year-old college students who completed an online questionnaire.
Results: Pain was significantly associated with total weekly alcohol consumption (r(445) = .22, p < 0.001); this association was significantly mediated by stress (b = 0.15, SE = 0.04, 95% CI = [.07,0.23]). SSS was significantly positively associated with alcohol consumption (r(445) = .22, p < 0.001) but was not found to significantly moderate the relationship between stress and alcohol use.
Conclusion: Results suggest that efforts to reduce college student alcohol use should include assessment of pain and stress given their association with alcohol consumption. Further, findings suggest that future studies are warranted to prospectively examine pain as an antecedent for alcohol use and to examine the utility of incorporating stress management techniques in pain-focused interventions to indirectly target alcohol use.
Keywords: alcohol, stress, pain, college students
Introduction
More than half of full-time college students in the United States report past-month alcohol consumption.1 Young adulthood is the time in life which represents the peak age of onset for alcohol use disorder.2 Perhaps even more concerning is that the high prevalence of alcohol use in this population is associated with numerous consequences, such as impaired driving, alcohol-related unintentional injuries and deaths, and trouble with residence hall or other college authorities.3–6 Moreover, research suggests that high-frequency drinking patterns that develop during college may persist for several years post-graduation.7
Pain has been found to be associated with alcohol use. In the United States, an estimated 50 million individuals experience chronic pain, defined as pain lasting for more than 3 months.8 While chronic pain is prototypically associated with older adults,9 research suggests college students may be at elevated risk for experiencing events that may lead to pain, such as athletic injuries.10 For instance, one study of 18- to 25-year-olds from general healthcare practices found that 66.9% of the sample endorsed experiencing pain within the previous six months. Further, 14.3% of respondents met criteria for chronic pain, with 3.0% reporting severely disabling chronic pain.11 In addition, a meta-analysis of population-level studies suggests that estimates of chronic pain in this age group, while lower than the general adult population (43.5%; 12), may be as high as 14.3%.12 While this estimate is lower than for other age groups, research suggests that the time course and length of duration of pain are important indicators of chronicity and functional outcomes.59,60 This is concerning, as inadequate pain treatment may impair physical functioning and sleep and is associated with high economic costs and deleterious health outcomes.13 For undergraduate students, pain may also result in significant interference with their education and ability to complete their schoolwork.14 Poorly controlled pain may lead some to find alternative ways to deal with the experience of pain. As such, a significant association has been demonstrated between pain and alcohol use.15,16 Research has found that pain is strongly and positively associated with substance use17 among college students, and students with chronic pain are much more likely to use alcohol and other analgesics.14 Further, pain has been shown to be an important predictor of heavy drinking episodes during alcohol use treatment,18 and decreased pain severity has been associated with decreased likelihood of alcohol use relapse following treatment.19 Given the positive association between pain and alcohol use in this population, it is important to understand psychosocial factors that may be underlying this relationship.
One such factor that may be helpful in understanding the association between pain and alcohol consumption is perceived stress. Undergraduate students report experiencing high levels of stress, with approximately 75 to 80% of college students reporting moderate stress and 10 to 12% reporting severe stress.20,21 Previous work has found a strong significant positive association between perceived stress and intensity of pain.22 Stress also has been shown to be positively associated with alcohol use among college students. In laboratory studies, acute stress has been found to increase single-session alcohol intake.23 Similarly, cross-sectional research has shown that students are more likely to drink and drink more heavily on days that they endorse a greater number of life stressors.24 Despite robust evidence demonstrating the associations between pain and stress and alcohol and stress individually, little work has been done examining the potential relationship between pain and stress in college student samples.
Another important psychosocial factor may be socioeconomic status (SES), which has been shown to have a significant association with both alcohol use and perceived stress.25 Traditionally, SES has been measured using objective metrics, including income and educational level. Lower objective SES has also been shown to be associated with chronic stress and higher levels of stress-related hormones, such as cortisol.26,27 However, a limitation of this existing literature is that, in college populations, objective SES measures may be more sensitive to parents’ socioeconomic status rather than how the student perceives their own status within their college environment.28 An alternative measure is subjective social status (SSS), in which individuals rank themselves on a ladder in relation to where they perceive their position in their communities to be. Subjective metrics like SSS have been shown to capture youth perceptions of SES more comprehensively than objective measures.29,30 SSS has also been shown to be a robust and better predictor of health status and health decline than objective measures of SES.31,32 In adolescents, SSS was demonstrated to have a strong negative association with perceived stress.33 In addition, SSS is not only associated with stress but also with factors related to increased risk of using substances to self-manage pain, such as greater negative effect and utilization of fewer active coping strategies.34,35 While the literature on SSS in the college student population is limited, previous research suggests that higher levels of SSS are associated with higher levels of alcohol consumption and a greater likelihood of regular alcohol use.36,37
The goal of the current study was to assess the relationship between pain and alcohol consumption and to examine stress and SSS as potential moderators of this association in an online sample of 18 to 25-year-old college students. Understanding how these factors interact with each other will aid in the development of new approaches to target undergraduates’ alcohol consumption. We hypothesized there would be a relationship between average pain experienced and total weekly alcohol consumption, and that stress would mediate this association. Given SSS’s association with stress, self-medication for pain risk factors and alcohol use, we also expected that SSS would moderate the association between stress and alcohol consumption, such that students reporting higher stress and SSS would also report greater alcohol consumption.
Methods
Participants and Procedure
Respondents were recruited from Amazon’s Mechanical Turk (MTurk) platform, which has been shown to generate relatively reliable data38,39 and represent the general population in terms of demographics.40 Participants between the ages of 18 and 25 were screened for the larger study based upon three inclusionary criteria: (1) living in the United States; (2) able to read and answer questions in the English language; and (3) currently enrolled as an undergraduate student at a college or university. Participants who met eligibility criteria provided informed consent and completed the survey on Qualtrics. Participants were compensated $0.50 for study participation. All procedures were approved by the Institutional Review Board at the University of Rhode Island and complied with the Declaration of Helsinki of 1964 ethical guidelines prior to beginning data collection procedures.
Exclusions and Missing Data
Of the 2085 obtained responses to the screening, 135 potential participants did not complete the survey (remaining n=1950). Additionally, 1212 prospective participants were excluded for being over the age of 25, and 111 were excluded for not being currently enrolled in college (remaining n = 627). We then excluded one potential participant (remaining n = 626) who failed to pass at least one of the four validity checks placed throughout the survey to ensure attentive responding (two items; eg, participants being asked to rate “I have never brushed my teeth” on a three response option scale from “yes” to “no” to “strongly agree”) and comprehension (two items, asking participants to “please click yes” with response options “yes,” “no,” and “not sure”; 42–44). For the purpose of the present study, an additional 101 participants were excluded because they did not report any pain in the last month on the Medical Outcomes Survey – Short Form (MOS-SF 36, see Measures) (remaining n = 525) and 80 (remaining n = 445) were excluded for not responding to either question regarding typical alcohol consumption or frequency of drinking alcohol. Thus, the final sample used for the present study included 445 participants. See Table 1 for participant demographic characteristics.
 |
Table 1 Participant Demographics (N=445) |
Measures
Demographics
Participants were asked to report their age, gender, race, ethnicity, and student status (see Table 1).
Medical Outcomes Survey – Short Form 36-Item (MOS-SF 36)
The MOS-SF 36 is a 36-item self-report measure that measures the generic health status across eight health-related areas.41 Pain was assessed as a screening measure using the item “how much bodily pain have you had during the past 4 weeks?” on a 6-point scale from “none” to “very severe.” Participants who selected the option “none” were screened out (see Exclusions and Missing Data).
Brief Pain Inventory – Short Form (BPI-SF)42
The BPI-SF is a 9-item self-report measure that assesses the location of pain in the body, severity of pain, and its impact on functioning.42 Pain on average was measured with one item, using a visual analog scale assessing severity of pain anchored on the left as “no pain” and on the right as “pain as bad as you can imagine.” The use of single-item VAS is consistent with recommendations by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT).45
Student-Life Stress Inventory (SLSI)43
The SLSI is a 51-item self-report measure that assesses stressors and reactions to stressors across 9 subscales: frustration, conflict, pressure, change, self-imposed, physiological, emotional, behavioral, and cognitive.43 Higher scores in each subscale, except for cognitive, indicate higher stress levels. In the cognitive subscale, lower scores indicate greater stress. Each item was rated on a Likert-type scale assessing how often the participant has experienced each item ranging from 1 = never to 5 = always. Items in the cognitive appraisal subscale were first reversed scored, then all items were added together to produce a total perceived stress score. The SLSI has good psychometric properties,43,44 including in the present study (α = 0.97).
MacArthur Subjective Social Status Scale34
The Subjective Social Status Scale is a single-item self-report measure that assesses subjective social status by asking participants to rank themselves on one of ten rungs of a visual ladder.34 Participants were provided a picture of a ladder on which they should select the point that best represented their standing within their community.
People define community in different ways; please define it in whatever way is most meaningful to you. At the top of the ladder are the people who have the highest standing in their community. At the bottom are the people who have the lowest standing in their community. Where would you place yourself on this ladder?
Assessment of SSS using the MacArthur scale has demonstrated moderate test-retest reliability45 and strong construct validity.46 In addition, Single-item SSS ladders have been shown to demonstrate moderate test-retest reliability and strong construct validity29,61 and good intraclass correlations (0.73–0.79) among American adolescents.62
NIAAA Six Question Set
The NIAAA Recommended Six Question Set47 is a 6-item self-report measure that assesses past-year frequency of alcohol use, quantity of drinks consumed, and frequency of binge drinking. Drinking frequency was measured by asking how often respondents consumed alcohol in the past year. Alcohol consumption quantity was measured by asking respondents to select how many drinks they consumed on a typical drinking day in the past year. A total alcohol consumption score was created by computing the product of quantity and frequency of alcohol consumption, which represented total number of drinks consumed per week, consistent with similar quantity-frequency alcohol measures used in extant research.48
Data Analysis
Analyses were conducted using IBM SPSS Statistics Version 25. First, Pearson product-moment correlations were calculated among relevant study variables to explore their bivariate associations. Next, mediation and moderation hypotheses were tested using the PROCESS macro developed by Hayes and Preacher.49 The PROCESS procedures use ordinary least squares regression and bootstrapping methodology, which confers more statistical power than do standard approaches to statistical inference. All variables were assessed for normality using skewness and kurtosis statistics. We determined an index violated normality if either skewness or kurtosis was greater than or equal to the absolute value of 2.63 Only the weekly alcohol consumption variable was considered non-normal (skewness = 2.32, kurtosis = 6.22). Due to the positive skewness, we used a square-root transformation on the raw values (skewness = 0.97, kurtosis = 0.58). First, we examined the mediating role of stress in the association between pain and alcohol consumption (PROCESS Model 4). Bootstrapping was done with 10,000 random samples generated from the observed covariance matrix to estimate the standard errors of parameter estimates and the bias-corrected 95% confidence intervals of the indirect effects. The indirect effect is significant if the 95% confidence interval does not contain zero.50 Then, we examined a second-stage moderated mediation model to examine SSS as a moderator of the association between stress and alcohol consumption. For moderation analyses, continuous predictor variables were mean-centered prior to the construction of the interaction term to aid in the interpretation of parameter estimates and to lessen the correlation between the interaction term and its component variables.
Results
Exploratory analyses were conducted assessing sex as a moderator along the pain to alcohol use pathway. Results indicated that sex was not a significant moderator (p>0.05). In addition, all models were also run using the MOS-SF pain subscale. This resulted in the same pattern of results and significance as the single item VAS from the BPI-SF.
Bivariate Correlations
Average pain was significantly positively associated with weekly alcohol consumption (r(445) = 0.26, p < 0.001) and perceived stress (r(445) = 0.56, p < 0.001). Additionally, perceived stress was significantly positively correlated with alcohol consumption (r(445) = 0.32, p < 0.001) and SSS (r(445) = 0.24, p < 0.001). SSS was also significantly positively correlated with alcohol consumption (r(445) = 0.21, p < 0.001). See Table 2 for bivariate correlations among all variables of interest.
 |
Table 2 Correlations Among Relevant Constructs |
Mediation Analysis
The overall model examining the role of perceived stress underlying the association between pain and alcohol consumption, controlling for the effects of age and gender, was significant (see Figure 1, F(4, 440) = 16.45, R2 = 0.13, p < 0.001). The relationship between pain and perceived stress was significant (b = 0.72, SE = 0.05, t = 13.95, p < 0.001), as was the association between stress and alcohol consumption (b = 0.02, SE = 0.004, t = 4.75, p < 0.001). Further, the indirect effect of pain on alcohol consumption through the pathway of perceived stress was also significant (b = 0.01, SE = 0.004, 95% CI [0.008, 0.022]), while the direct effect linking average pain with weekly alcohol consumption remained significant after controlling for the effect of perceived stress (b = 0.01, SE = 0.006, t = 2.20, p = 0.03).
 |
Figure 1 Summary of analyses explicating the role of stress in the relation between pain and weekly alcohol consumption. |
Moderated Mediation Analysis
The overall model examining the moderating effect of SSS on the pathway from stress to alcohol consumption, controlling for the effects of age and gender, was significant (see Figure 2, F(6, 438) = 12.51, R2 = 0.15, p < 0.001). There were significant main effects of stress (b = 0.02, SE = 0.004, t = 4.45, p < 0.001) and SSS (b = 0.16, SE = 0.07, t = 2.41, p = 0.016) on weekly alcohol consumption. However, the interaction of stress and SSS on alcohol consumption (b = 0.003, SE = 0.002, t = 1.56, p = 0.12) and the index of moderated mediation (b = 0.002, SE = 0.002, 95% CI [−.0006, 0.0051]) were not significant.
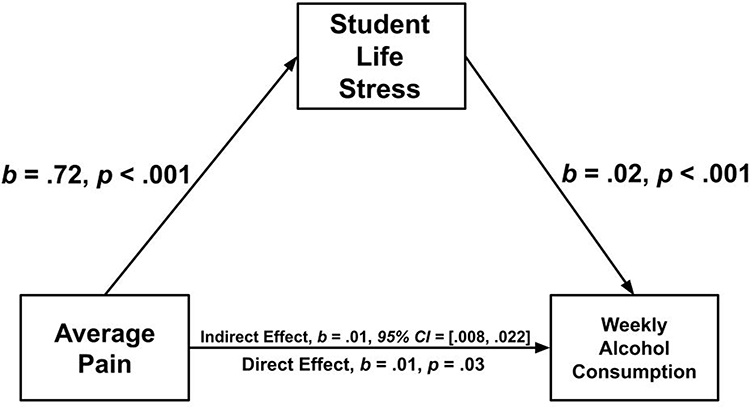 |
Figure 2 Summary of the analyses explicating the role of stress and subjective social status in the relation between pain and weekly alcohol consumption. |
Discussion
The goal of this study was to further our understanding of how pain, stress, and SSS are associated with alcohol consumption. Overall, the majority of the present sample reported moderate pain intensity and perceived stress, as well as high levels of alcohol consumption. Each of the factors were significantly interrelated, and stress significantly mediated the relationship between pain and alcohol consumption. Interestingly, subjective social status did not significantly moderate the association between stress and alcohol consumption but did demonstrate a significant main effect on alcohol consumption.
Consistent with earlier research,14 we identified a significant positive association between pain and alcohol use. This is consistent with research among adults in the United States, which has found greater pain to be associated with greater alcohol use.16 The present study expands this finding to a younger population and suggests the importance of assessing pain as a motivator for alcohol use when planning interventions. Specifically, students who use alcohol to help manage their pain may benefit from pain management interventions in an effort to reduce their alcohol consumption. Additionally, pain has been found to be related to alcohol consumption at the bivariate level and this association was remained significant after accounting for perceived stress. Pain has been shown to be positively associated with stress and is a stressor in its own right, which may explain their strong association.51–53 This is an important consideration as research has shown that higher levels of stress are associated with drinking to cope among college students54 and that 39% of college students reported drinking to cope with stress.20 This finding suggests that students in groups at high risk for pain, such as collegiate athletes and students with pre-existing conditions, may also be at increased risk for stress and therefore drink more alcohol. Efforts to reduce substance use in these students should consider targeting stress and pain as treatment targets using interventions such Cognitive Behavioral Therapy for Pain (CBT-P) and mindful awareness and acceptance-based treatments.55,56
Our finding that SSS was positively correlated at the bivariate level with alcohol consumption is consistent with previous research amongst adolescents.57,58 Interestingly, perceived stress was also significantly positively associated with SSS. However, in contrast to study hypotheses, SSS did not significantly moderate the pathway between stress and alcohol consumption. One potential explanation for the non-significance of the interaction may be that since stress is highly prevalent amongst college students, the expectation that alcohol will have a stress response dampening effect may exist across SSS groups. Secondly, the majority of our sample reported a SSS higher than 6, which may have limited our ability to characterize effects for those with lower SSS. Future research in this area should include a wider distribution of SSS and consider additional factors such as coping and negative affect when assessing for SSS and alcohol use.
While the findings of this study contribute important knowledge regarding the associations among pain, stress, and subjective social status on alcohol consumption in undergraduate students, they should be considered within the study’s limitations. First, the results are cross-sectional and correlational in nature, which limits the ability to determine the directionality of the associations. To address this, future research should examine these relationships through direct experimental manipulations and in a prospective longitudinal framework. In addition, research utilizing ecological momentary assessment may be a useful approach for understanding interindividual dynamics between these variables and provide a prospective framework. Second, our inclusion of the terms “pain” and “alcohol” in the MTurk project title may have resulted in oversampling of students with higher levels of pain or alcohol use; thus, findings may not reflect undergraduate students as a whole. Further, the use of an online sampling platform may introduce limitations resulting from the loss of control over the research environment (eg, because there is no opportunity to clarify questions or limit distractions). In addition, our sample demographics are primarily non-Hispanic White male students which may not generalize the student body as a whole. Thus, future research that integrates other data collection methods (eg, interviewing) and diverse groups of students is warranted. Lastly, future research in this area should consider other potentially relevant moderators, such as sex and race, which may provide additional insight on the role of stress and subjective social status in the association between pain and alcohol consumption.
Taken together, our results extend knowledge of psychosocial factors on the relationship between pain and alcohol consumption among undergraduate students. These findings suggest that psychosocial factors, including pain, stress, and SSS, should be considered when assessing students presenting for prevention or treatment programs targeting alcohol consumption or when college students present to campus health centers seeking attention for pain. In particular, alcohol use should be assessed among students who are at-risk for developing pain, and pain should be assessed among students referred to treatment due to alcohol use. Additionally, findings of this study suggest that stress reduction and pain management are important foci for targeted interventions to reduce alcohol consumption in college student populations.
Acknowledgments
The authors would like to acknowledge the participants who volunteered for this study. This work was supported by the University of Rhode Island Undergraduate Research & Innovation Office’s Undergraduate Research Grant.
Funding
Work on this paper was supported by the University of Rhode Island Undergraduate Research & Innovation Office’s Undergraduate Research Grant awarded to the first author (NB).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Substance Abuse and Mental Health Services Administration (SAMHSA). Key Substance use and mental health indicators in the United States: results from the 2018 national survey on drug use and health; 2018:82.
2. Delker E, Brown Q, Hasin DS. Alcohol consumption in demographic subpopulations. Alcohol Res. 2016;38(1):7–15.
3. Hingson R, Zha W, Smyth D. Magnitude and trends in heavy episodic drinking, alcohol-impaired driving, and alcohol-related mortality and overdose hospitalizations among emerging adults of college ages 18–24 in the United States, 1998–2014. J Stud Alcohol Drugs. 2017;78(4):540–548. doi:10.15288/jsad.2017.78.540
4. Beck KH, Kasperski SJ, Caldeira KM, Vincent KB, O’Grady KE, Arria AM. Trends in alcohol-related traffic risk behaviors among college students. Alcohol Clin Exp Res. 2010;34(8):1472–1478. doi:10.1111/j.1530-0277.2010.01232.x
5. Jackson KM, Sokolovsky AW, Gunn RL, White HR. Consequences of alcohol and marijuana use among college students: prevalence rates and attributions to substance-specific versus simultaneous use. Psychol Addict Behav. 2020;34(2):370–381. doi:10.1037/adb0000545
6. Presley CA, Pimentel ER. The introduction of the heavy and frequent drinker: a proposed classification to increase accuracy of alcohol assessments in postsecondary educational settings. J Stud Alcohol. 2006;67(2):324–331. doi:10.15288/jsa.2006.67.324
7. Arria AM, Caldeira KM, Allen HK, Vincent KB, Bugbee BA, O’Grady KE. Drinking like an adult? Trajectories of alcohol use patterns before and after college graduation. Alcohol Clin Exp Res. 2016;40(3):583–590. doi:10.1111/acer.12973
8. Dahlhamer J. Prevalence of chronic pain and high-impact chronic pain among adults — United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
9. Thielke S, Sale J, Reid MC. Aging: are these 4 pain myths complicating care? J Fam Pract. 2012;61(11):666–670.
10. Amoako AO, Pujalte GGA. Osteoarthritis in young, active, and athletic individuals. Clin Med Insights Arthritis Musculoskelet Disord. 2014;7:27–32. doi:10.4137/CMAMD.S14386
11. Mallen C, Peat G, Thomas E, Croft P. Severely disabling chronic pain in young adults: prevalence from a population-based postal survey in North Staffordshire. BMC Musculoskelet Disord. 2005;6(1):42. doi:10.1186/1471-2474-6-42
12. Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. doi:10.1136/bmjopen-2015-010364
13. Sinatra R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010;11(12):1859–1871. doi:10.1111/j.1526-4637.2010.00983.x
14. Thomas M, Roy R, Cook A, Marykuca S. Chronic pain in college students: issues of management. Can Fam Physician. 1992;38:2597–2601.
15. Stennett B, Anderson MB, Vitus D, et al. Sex moderates the effects of experimentally induced musculoskeletal pain on alcohol demand in healthy drinkers. Drug Alcohol Depend. 2021;219:108475. doi:10.1016/j.drugalcdep.2020.108475
16. Zale EL, Maisto SA, Ditre JW. Interrelations between pain and alcohol: an integrative review. Clin Psychol Rev. 2015;37:57–71. doi:10.1016/j.cpr.2015.02.005
17. Ferrer E, Marks R, Midlarsky E, Hutz-Midgett A. Substance abuse and pain in a cohort of college students. Res J Drug Abuse. 2015;2(1):1. doi:10.7243/2057-3111-2-1
18. Witkiewitz K, Vowles KE, McCallion E, Frohe T, Kirouac M, Maisto SA. Pain as a predictor of heavy drinking and any drinking lapses in the COMBINE study and the UK Alcohol Treatment Trial. Addiction. 2015;110(8):1262–1271. doi:10.1111/add.12964
19. Jakubczyk A, Ilgen MA, Kopera M, et al. Reductions in physical pain predict lower risk of relapse following alcohol treatment. Drug Alcohol Depend. 2016;158:167–171. doi:10.1016/j.drugalcdep.2015.11.020
20. Pierceall EA, Keim MC. Stress and coping strategies among community college students. Community Coll J Res Pract. 2007;31(9):703–712. doi:10.1080/10668920600866579
21. Saleh D, Camart N, Romo L. Predictors of stress in college students. Front Psychol. 2017;8. doi:10.3389/fpsyg.2017.00019.
22. Boglut A, Codreanu D. Gender, positive and negative emotions predictors for the self-perceived pain at undergraduate students at psychology – a pilot study. Procedia Soc Behav Sci. 2015;187:723–727. doi:10.1016/j.sbspro.2015.03.135
23. Magrys SA, Olmstead MC. Acute stress increases voluntary consumption of alcohol in undergraduates. Alcohol Alcohol. 2015;50(2):213–218. doi:10.1093/alcalc/agu101
24. Russell MA, Almeida DM, Maggs JL. Stressor-related drinking and future alcohol problems among university students. Psychol Addict Behav. 2017;31(6):676–687. doi:10.1037/adb0000303
25. Keyes KM, Hatzenbuehler ML, Grant BF, Hasin DS. Stress and alcohol. Alcohol Res. 2012;34(4):391–400.
26. Baum A, Garofalo JP, Yali AM. Socioeconomic status and chronic stress: does stress account for SES effects on health? Ann N Y Acad Sci. 1999;896(1):131–144. doi:10.1111/j.1749-6632.1999.tb08111.x
27. Cohen S, Doyle WJ, Baum A. Socioeconomic status is associated with stress hormones. Psychosom Med. 2006;68(3):414–420. doi:10.1097/01.psy.0000221236.37158.b9
28. Svedberg P, Nygren JM, Staland-Nyman C, Nyholm M. The validity of socioeconomic status measures among adolescents based on self-reported information about parents occupations, FAS and perceived SES; implication for health related quality of life studies. BMC Med Res Methodol. 2016;16(1). doi:10.1186/s12874-016-0148-9
29. Goodman E, Adler NE, Kawachi I, Frazier AL, Huang B, Colditz GA. Adolescents’ perceptions of social status: development and evaluation of a new indicator. Pediatrics. 2001;108(2):E31. doi:10.1542/peds.108.2.e31
30. Joffer J, Flacking R, Bergström E, Randell E, Jerdén L. Self-rated health, subjective social status in school and socioeconomic status in adolescents: a cross-sectional study. BMC Public Health. 2019;19(1):785. doi:10.1186/s12889-019-7140-3
31. Nobles J, Ritterman Weintraub M, Adler N. Subjective socioeconomic status and health: relationships reconsidered. Soc Sci Med. 2013;82:58–66. doi:10.1016/j.socscimed.2013.01.021
32. Singh-Manoux A, Marmot MG, Adler NE. Does subjective social status predict health and change in health status better than objective status? Psychosom Med. 2005;67(6):855–861. doi:10.1097/01.psy.0000188434.52941.a0
33. Steen PB, Poulsen PH, Andersen JH, Biering K. Subjective social status is an important determinant of perceived stress among adolescents: a cross-sectional study. BMC Public Health. 2020;20(1):396. doi:10.1186/s12889-020-08509-8
34. Adler NE, Epel ES, Castellazzo G, Ickovics JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy, White women. Health Psychol. 2000;19(6):586–592. doi:10.1037/0278-6133.19.6.586
35. Ferguson E, Zale E, Ditre J, et al. CANUE: a theoretical model of pain as an antecedent for substance use. Ann Behav Med. 2020. doi:10.1093/abm/kaaa072
36. D’Hooge L, Achterberg P, Reeskens T. Mind over matter. The impact of subjective social status on health outcomes and health behaviors. PLoS One. 2018;13(9):e0202489. doi:10.1371/journal.pone.0202489
37. Hamilton HA, van der Maas M, Boak A, Mann RE. Subjective social status, immigrant generation, and cannabis and alcohol use among adolescents. J Youth Adolesc. 2014;43(7):1163–1175. doi:10.1007/s10964-013-0054-y
38. Buhrmester M, Kwang T, Gosling SD. Amazon’s mechanical turk: a new source of inexpensive, yet high-quality, data? Perspect Psychol Sci. 2011;6(1):3–5. doi:10.1177/1745691610393980
39. Shapiro DN, Chandler J, Mueller PA. Using mechanical turk to study clinical populations. Clin Psychol Sci. 2013;1(2):213–220. doi:10.1177/2167702612469015
40. Mishra S, Carleton RN. Use of online crowdsourcing platforms for gambling research. Int Gambl Stud. 2017;17(1):125–143. doi:10.1080/14459795.2017.1284250
41. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
42. Daut RL, Cleeland CS, Flanery RC. Development of the Wisconsin brief pain questionnaire to assess pain in cancer and other diseases. Pain. 1983;17(2):197–210. doi:10.1016/0304-3959(83)90143-4
43. Gadzella BM. Student-life stress inventory: identification of and reactions to stressors. Psychol Rep. 1994;74(2):395–402. doi:10.2466/pr0.1994.74.2.395
44. Gadzella BM. Three stress groups on their stressors and reactions to stressors in five studies. Psychol Rep. 2004;94(2):562–564. doi:10.2466/pr0.94.2.562-564
45. Giatti L, Camelo LDV, Rodrigues JFDC, Barreto SM. Reliability of the MacArthur scale of subjective social status - Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). BMC Public Health. 2012;12(1):1096. doi:10.1186/1471-2458-12-1096
46. Cundiff JM, Smith TW, Uchino BN, Berg CA. Subjective social status: construct validity and associations with psychosocial vulnerability and self-rated health. Int J Behav Med. 2013;20(1):148–158. doi:10.1007/s12529-011-9206-1
47. National Institute on Alcohol Abuse and Alcoholism. Recommended Alcohol Questions | National Institute on Alcohol Abuse and Alcoholism (NIAAA). Recommended Alcohol Questions; 2003. Available from: https://www.niaaa.nih.gov/research/guidelines-and-resources/recommended-alcohol-questions.
48. Sobell L, Sobell M. Alcohol consumption measures. In: Assessing Alcohol Problems.
49. Hayes AF, Preacher KJ. Conditional process modeling: using structural equation modeling to examine contingent causal processes. In: Structural Equation Modeling: A Second Course. Quantitative Methods in Education and the Behavioral Sciences: Issues, Research, and Teaching.
50. Abdallah CG, Geha P. Chronic pain and chronic stress: two sides of the same coin? Chronic Stress. 2017;1. doi:10.1177/2470547017704763.
51. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
52. Blackburn-Munro G, Blackburn-Munro RE. Chronic pain, chronic stress and depression: coincidence or consequence? J Neuroendocrinol. 2001;13(12):1009–1023. doi:10.1046/j.0007-1331.2001.00727.x
53. Vierck CJ, Green M, Yezierski R. Pain as a stressor: effects of prior nociceptive stimulation on escape and lick/guard responding of rats to thermal stimulation. Eur J Pain. 2010;14(1):11–16. doi:10.1016/j.ejpain.2009.01.009
54. Rice KG, Van Arsdale AC. Perfectionism, perceived stress, drinking to cope, and alcohol-related problems among college students. J Couns Psychol. 2010;57(4):439–450. doi:10.1037/a0020221
55. Davis MC, Zautra AJ, Wolf LD, Yeung EW. Mindfulness and cognitive-behavioral interventions for chronic pain: differential effects on daily pain reactivity and stress reactivity. J Consult Clin Psychol. 2015;83(1):24–35. doi:10.1037/a0038200
56. Regehr C, Glancy D, Pitts A. Interventions to reduce stress in university students: a review and meta-analysis. J Affect Disord. 2013;148(1):1–11. doi:10.1016/j.jad.2012.11.026
57. Piko B, Fitzpatrick KM. Does class matter? SES and psychosocial health among Hungarian adolescents. Soc Sci Med. 2001;53(6):817–830. doi:10.1016/s0277-9536(00)00379-8
58. Ritterman ML, Fernald LC, Ozer EJ, Adler NE, Gutierrez JP, Syme SL. Objective and subjective social class gradients for substance use among Mexican adolescents. Soc Sci Med. 2009;68(10):1843–1851. doi:10.1016/j.socscimed.2009.02.048
59. Boersma K, Linton SJ. How does persistent pain develop? An analysis of the relationship between psychological variables, pain and function across stages of chronicity. Behav Res Ther. 2005;43(11):1495–1507. doi:10.1016/j.brat.2004.11.006
60. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
61. Operario D, Adler NE, Williams DR. Subjective social status: reliability and predictive utility for global health. Psychol Health. 2004;19(2):237–246. doi:10.1080/08870440310001638098
62. Walston Z, McLester C, McLester J. Effect of low back pain chronicity on patient outcomes treated in outpatient physical therapy: a retrospective observational study. Arch Phys Med Rehabil. 2020;101(5):861–869. doi:10.1016/j.apmr.2019.11.009
63. George D, Mallery M. SPSS for Windows Step by Step: A Simple Guide and Reference, 17.0 Update.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.