Back to Journals » Journal of Pain Research » Volume 13
Stress and Self-Efficacy as Long-Term Predictors for Chronic Low Back Pain: A Prospective Longitudinal Study
Authors Puschmann AK ![]() , Drießlein D
, Drießlein D ![]() , Beck H, Arampatzis A, Moreno Catalá M, Schiltenwolf M, Mayer F, Wippert PM
, Beck H, Arampatzis A, Moreno Catalá M, Schiltenwolf M, Mayer F, Wippert PM ![]()
Received 19 July 2019
Accepted for publication 20 January 2020
Published 24 March 2020 Volume 2020:13 Pages 613—621
DOI https://doi.org/10.2147/JPR.S223893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Anne-Katrin Puschmann, 1 David Drießlein, 2 Heidrun Beck, 3 Adamantios Arampatzis, 4 Maria Moreno Catalá, 4 Marcus Schiltenwolf, 5 Frank Mayer, 6 Pia-Maria Wippert 1, 7
1Sociology of Health and Physical Activity, University of Potsdam, Potsdam, Germany; 2Statistical Consulting Unit, Ludwig-Maximilians-University Munich, Munich, Germany; 3University Center of Orthopedics and Surgery, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany; 4Department of Training and Movement Sciences, Humboldt-University of Berlin, Berlin, Germany; 5Conservative Orthopaedics and Pain Management, Center of Orthopaedics and Trauma Surgery, University Hospital Heidelberg, Heidelberg, Germany; 6University Outpatient Clinic, University of Potsdam, Potsdam, Germany; 7Department of Health Sciences and Technology, ETH Zürich, Zürich, Switzerland
Correspondence: Anne-Katrin Puschmann
University of Potsdam, Am Neuen Palais 10, House 12, Potsdam 14469, Germany
Tel +49 331 9771075
Email [email protected]
Purpose: Psychosocial variables are known risk factors for the development and chronification of low back pain (LBP). Psychosocial stress is one of these risk factors. Therefore, this study aims to identify the most important types of stress predicting LBP. Self-efficacy was included as a potential protective factor related to both, stress and pain.
Participants and Methods: This prospective observational study assessed n = 1071 subjects with low back pain over 2 years. Psychosocial stress was evaluated in a broad manner using instruments assessing perceived stress, stress experiences in work and social contexts, vital exhaustion and life-event stress. Further, self-efficacy and pain (characteristic pain intensity and disability) were assessed. Using least absolute shrinkage selection operator regression, important predictors of characteristic pain intensity and pain-related disability at 1-year and 2-years follow-up were analyzed.
Results: The final sample for the statistic procedure consisted of 588 subjects (age: 39.2 (± 13.4) years; baseline pain intensity: 27.8 (± 18.4); disability: 14.3 (± 17.9)). In the 1-year follow-up, the stress types “tendency to worry”, “social isolation”, “work discontent” as well as vital exhaustion and negative life events were identified as risk factors for both pain intensity and pain-related disability. Within the 2-years follow-up, Lasso models identified the stress types “tendency to worry”, “social isolation”, “social conflicts”, and “perceived long-term stress” as potential risk factors for both pain intensity and disability. Furthermore, “self-efficacy” (“internality”, “self-concept”) and “social externality” play a role in reducing pain-related disability.
Conclusion: Stress experiences in social and work-related contexts were identified as important risk factors for LBP 1 or 2 years in the future, even in subjects with low initial pain levels. Self-efficacy turned out to be a protective factor for pain development, especially in the long-term follow-up. Results suggest a differentiation of stress types in addressing psychosocial factors in research, prevention and therapy approaches.
Keywords: low back pain, psychosocial risk factors, stress, self-efficacy, MiSpEx
Plain Language Summary
The study reported on the influence of several types of stress on the development of chronic low back pain in a time frame of up to 2 years while respecting self-efficacy. The results point out the importance of stress experiences in social and work-related contexts as risk factors for pain chronification even in people presenting with low initial pain levels. Self-efficacy turned out to protect against the chronification of LBP. A differentiated view on those psychosocial factors should be part of low back pain management approaches aiming to prevent the chronification of this global pain disease.
Introduction
Low back pain is the most disabling health complaint with the world´s highest disability rate.1 Since at least one out of three patients with acute back pain experiences recurrent symptoms within the next 12 months,2 a better understanding of the underlying mechanisms is indispensable. The impact of psychological factors such as stress on pain development and chronification in subjects with low back pain (LBP) is already indisputable.3,4 However, the actual influence of each factor is difficult to investigate because of its dependence on the respective sample population and methodological issues.4–6 The presented analyses will focus on the influence of psychosocial stress on LBP, additionally including self-efficacy as a potential protective factor.
Psychosocial stress has a direct impact on both people´s health and pain processing.3,7,8 Stress is an individual´s reaction to external or internal stressors activating psychological and physiological mechanisms, which prepare the individual to deal with an upcoming challenging situation.9–11 Stressors that combine social evaluative threat and uncontrollability are powerful in activating stress reactivity systems.12 Therefore, specific types of stress on the one hand and repeating stressful events or long-lasting challenging situations on the other hand can result in a permanently over-activated stress system.11,12 The ability to maintain homeostasis and therefore the body´s ability to restore energy and repair damages may be impaired due to an ongoing wear and tear of the body´s resources, as explained in the concept of allostatic load.10,11 The result can be dysfunctional reactions to acute stressors including symptoms of depression and fatigue.7,13 These mechanisms are highly interrelated to pain processing.7,8,11 For example, the occurrence of critical life events may elicit central changes in the limbic system and related neurotransmitters, which then alter descending signaling pathways and change pain inhibitory mechanisms. Chronic stress, on the other hand, and the resulting change of the body´s ability to maintain homeostasis may alter ascending signaling mechanisms and lead to decreased pain thresholds.14,15 Studies regarding stress as a risk factor for LBP maintenance and chronification often analyze stress in general or certain specific types of stress such as work-related stress. For example, a recent longitudinal study found stress as a predictor for long-term activity limitation in women with chronic LBP. However, in this study stress was not differentiated further.16
A major psychological construct influencing an individual´s management of both stress and pain is self-efficacy.17–19 It is defined as a person´s belief to be able to deal with upcoming challenges.20 The occurrence of pain could be such a challenging situation.21 Therefore, self-efficacy is regarded as a main psychological protective factor in the prevention of pain chronification. However, studies revealed conflicting results. While some authors state the influence of self-efficacy on reduced disability in subjects with chronic LBP,5,22,23 others could not find this relationship.6 It is discussed that the influence of self-efficacy in (chronic) LBP subjects may depend on the level of disability and pain status.6,23 Furthermore, several studies aimed to detect this relationship in cross-sectional designs, which do not allow the detection of prognostic influences.22,23 Although closely related to each other, psychosocial stress and self-efficacy have not been analyzed together in LBP research, yet.
Therefore, this study aims to compare different types of psychosocial stress to identify the most influential stress predictors for the development of chronic LBP including the influence of self-efficacy. Since long-term risk factors are especially relevant for preventive treatment approaches the analyses were conducted for a 1- and 2-years follow-up.
Materials and Methods
Procedure
Data were collected within a 2-year prospective observational longitudinal study conducted by the German research network ´Medicine in Spine Exercise (MiSpEx)`. Participants with intermittent LBP were recruited from the general population at four German study sites. After confirming that they met the inclusion criteria, participants received information about the study, signed informed consent. After baseline measurement, they took part in six follow-up measurements at 1 month, 3 months, 6 months, 12 months, 18 months and 24 months after baseline. At each measurement participants filled in comprehensive questionnaires administered digitally via computer by trained study nurses.24 For the presented analyses, data of measurements at baseline, at 12 months and at 24 months follow-up were used.
Measurements
Predictors
The different types of psychosocial stress were assessed using the following questionnaires:
Long-term chronic stress was assessed using the German short version of the Perceived Stress Scale (PSS).25,26 This questionnaire consists of four of the original 10 items, rated on a 5-point Likert scale (0 = “never” to 4 = “very often”). Items indicate how often individuals have experienced a described stressful situation within the previous 12 months (eg “In the last 12 months, how often have you felt that you were unable to control the important things in your life?”). Higher values indicate that stressful situations were experienced more often. Cronbach’s α for this sample was 0.74.
Stress experiences in the previous 3 months were assessed by the Trier Inventory of Chronic Stress (TICS),27 consisting of 57 items rated on a 5-point Likert scale (from 0 = “never” to 4 = “very often”). Items indicate how often an individual experienced a described stressful situation within the previous 3 months (eg “There is a lack of interesting tasks to fill my day”). The items are summed up to nine scales giving information about nine areas of potential stress experiences, with higher values meaning, that subjects had made the respective experience more often: work overload, pressure to perform, work discontent, excessive demands at work, social overload, lack of social recognition, social conflicts, social isolation and tendency to worry. In this sample, Cronbach´s α of the different scales ranged from 0.84 to 0.91.
Vital exhaustion (VE) was measured using the German short version,28 adapted from the original 21-item Maastricht VE Questionnaire.29 Nine items represent mental and physical consequences of stress such as excessive fatigue, disturbed sleep, general malaise, irritability, loss of mental and physical energy, and feelings of demoralization (eg “Do you lately feel more listless than before?”). Each item is rated accordingly, “no” (score = 0), “uncertain” (score = 1), and “yes” (score = 2), resulting in a summarized VE score between 0 and 18, with higher values indicating higher vital exhaustion. Cronbach's α for this sample was 0.81, indicating good internal reliability. Life-event stress was assessed using a singular item asking about the occurrence of major life-events during the previous 3 months, which could be answered on a dichotomous scale (“yes” or “no”). If yes, subjects could further specify the type of life-event.
Additionally, self-efficacy was measured using the original German version of the Inventory for the measurement of Self-Efficacy and Externality (I-SEE).30,31 The 32 items (eg “I can do a lot to protect myself from disease”) reflect four sub-factors: 1) general self-concept on personal skills and abilities (self-concept); 2) internal attribution in general control beliefs (internality); 3) socially caused externality (social externality); and 4) fatalistic externality. Of these, self-concept and internality build the scale self-efficacy, with higher values indicating stronger self-efficacy, ie stronger belief in the own ability to influence life and health. Higher values in social externality and fatalistic externality indicate a stronger belief in the influence of external factors on personal experiences. Cronbach’s α ranged between 0.70 and 0.76 for the scales in the sample of this study.
Outcome Variables
Pain in the past 3 months was assessed using the Chronic Pain Grade Questionnaire (CPG;32 German version33) with its subscales characteristic pain intensity (CPI) and pain-related disability (Disability Score, DISS). It consists of three items on a 11-point numerical self-rating scale ranging from 0 = “no interference” to 10 = “unable to carry on any activities”, building DISS (eg “In the past 3 months, how much has back pain interfered with your daily activities?”) with a range of 0 to 100, and three items (eg “In the past 3 months, how intense was your worst pain?”) rated from 0 = “no pain” to 10 = “pain as bad as could be”, building CPI ranging from 0 to 100, respectively. Higher values in CPI indicate higher intensity of pain in the past 3 months; higher values of DISS indicate that there was more interference in daily life due to pain. Further, the number of days of disability during the previous 3 months was assessed. Cronbach’s α was 0.85 for CPI and 0.91 for DISS.
Control Variables
Baseline pain was used as a control variable (CPI, DISS) as well as other pain-related factors such as gender and age. Further, lifestyle status (satisfaction with health and sleep, medication, smoking, alcohol consumption, physical activity, monthly net income), was assessed using singular items (eg “How satisfied are you with your health? Do you smoke regularly? Do you drink alcohol regularly? If you exercise on a regular basis, how many hours per week?”) comparable to other studies.34
Statistical Analyses
The selection of the most predictive stress types was executed using least absolute shrinkage and selection operator regression (Lasso). This technique provides a possibility to deal with problems arising when highly correlated predictors are analyzed together in the same regression model weakening the resulting prediction. The statistical analyses were conducted using IBM SPSS Statistics 24.0 and the software R,35 packages glmnet and penalized.36 The applied two-step procedure resulted in four models – one for each outcome variable (CPI and DISS) and follow-up (1-year, 2-years).
In the first step, the most influential sub-scales were identified using Lasso with 10-fold cross-validation resulting in an optimal degree of penalization.37,38 Data from participants with complete cases for each model and measurement point were used for this selection. Therefore, observation numbers differ between the models. Variables without predictive strength as well as redundant – ie highly correlated – variables were penalized and shrinked to zero, resulting in a reduced number of predictors in the final Lasso model. All subscales of the baseline predictors (TICS: tendency to worry, social isolation, social conflicts, work discontent, lack of social recognition, work overload, pressure to succeed, excessive demands at work, social overload, I-SEE: internality, self-concept, social externality, fatalistic externality, VE: vital exhaustion, PSS: perceived long-term stress) were included penalized into the analyses and therefore can be selected. Possible confounders such as pain at baseline (DISS or CPI, respectively), as well as lifestyle-related factors (medication, smoking, alcohol consumption, physical activity, monthly net income) and satisfaction with health and sleep were included penalized, too. Age, gender, and study center were included unpenalized, therefore kept stable as control variables in all final models, which means, these variables could not be shrinked to zero and thus removed from the model.
As a second step, to obtain unbiased regression coefficients, the selected subscales and variables were put together into a linear regression model (refit model). To evaluate the predictive quality of these models, an independent data subset was used consisting of subjects not included into the selection analysis of the first steps due to missing values. Therefore, sample numbers differ from each other. For each model, the root-mean-squared error (RMSE) was calculated.
For the interpretation of RMSE, it has to be compared to the outcome scales. In this case, DISS and CPI which range from 0 to 100. RMSE is calculated at the same scale, and therefore can range from 0 to 100, too. Additionally, the percentage of explained variance is reported using adjusted R2, which adjusts for the number of predictors in the model.
Results
Sample
Initially, a total of n = 1071 subjects were enrolled in the study. Of those, n = 1048 completed the baseline measurement. At 1-year follow-up 677 (64.7%) and at 2-year follow-up 626 (51.7%) participants remained. Reasons for dropout were, eg upcoming pregnancy, illness or relocation. For further analyses, data from subjects with complete data in the outcome variables at baseline and at the respective follow-up are reported (n = 588 at baseline).
Descriptives
Participants' mean age was 39.2 years (±13.4), and 56% were female. At baseline, they reported a mean CPI score of 27.8 (±18.4) and DISS of 14.3 (±17.9), reflecting low levels of intermittent pain at baseline. Furthermore, stress levels, vital exhaustion, and self-efficacy were on normal to moderate range representing a distribution comparable to the general German population. Further characteristics of the participants are displayed in Table 1. The correlations of the predictors used are displayed in supplementary Tables S1 and S2.
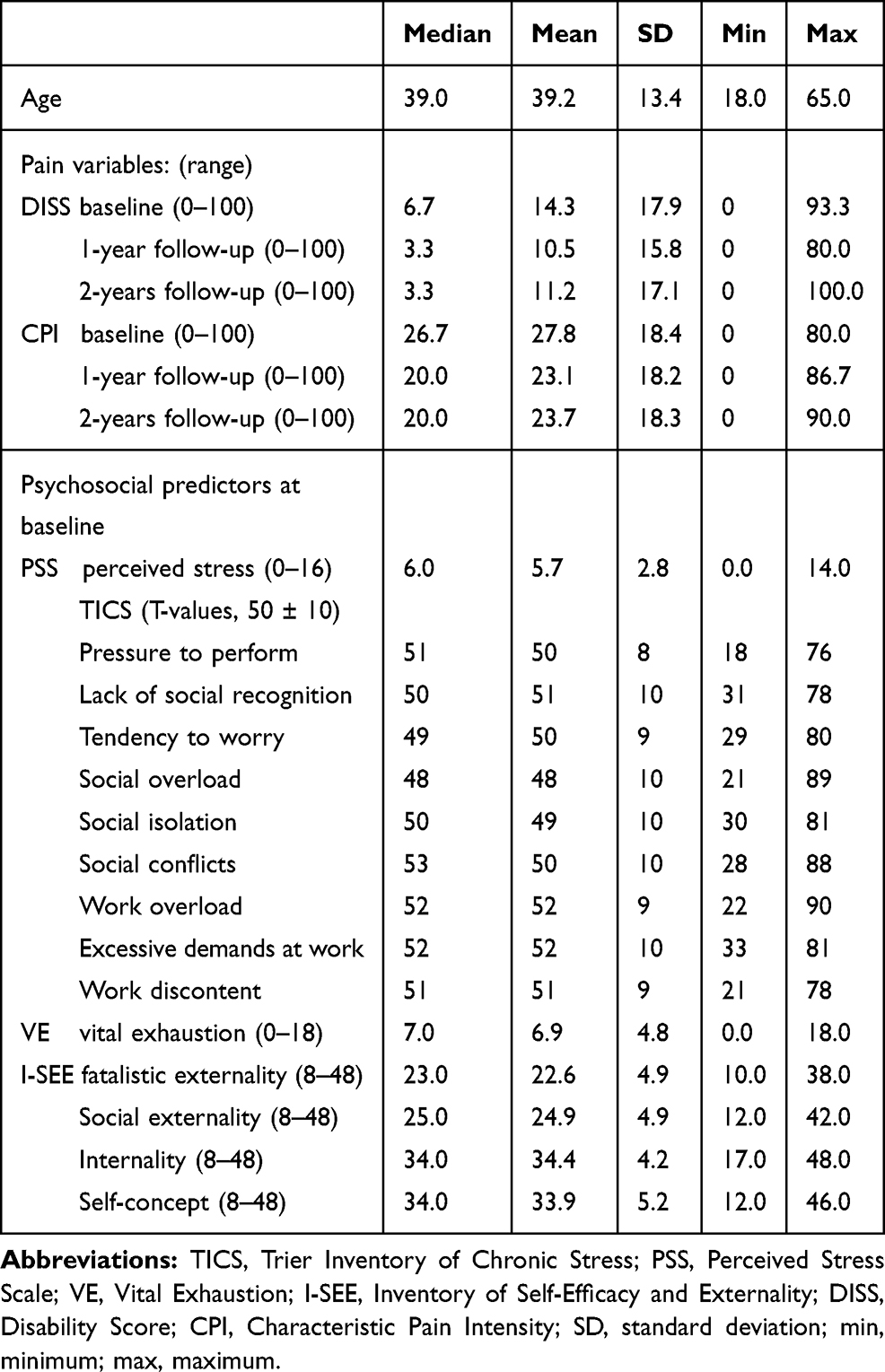 |
Table 1 Participant Characteristics of the Subset Used for Analyses (n = 588) |
Lasso Selection
A summary of the results of the Lasso selection is displayed in Table 2. The results are based on the paths of penalization of the coefficients and not on the p-values in the refit models. Because of incorrectness of standard p-values after a selection procedure, p-values based on the work of Zhang and Zhang39 were calculated.
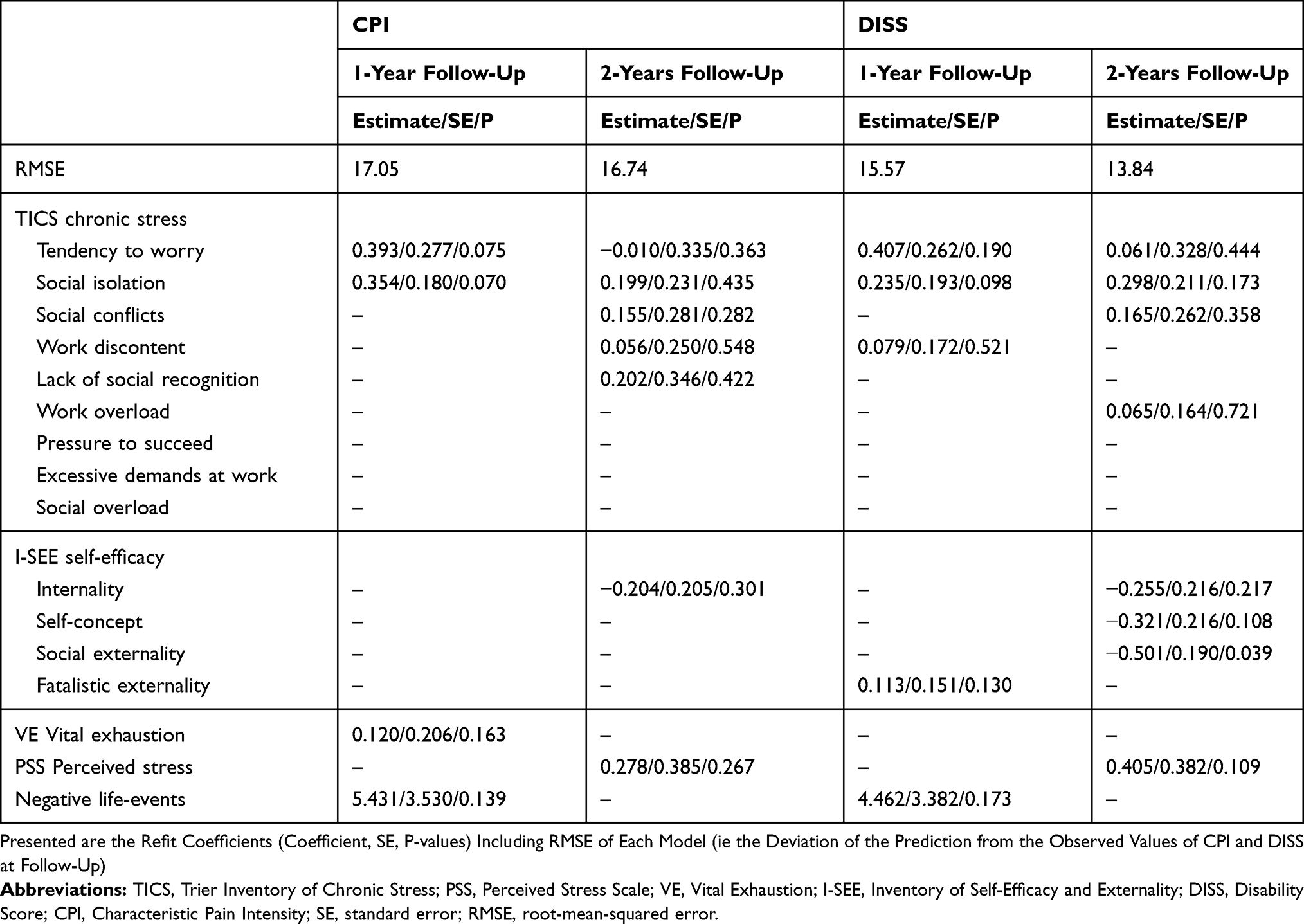 |
Table 2 Stress-Related Predictors for Characteristic Pain Intensity (CPI) and pain-related disability (DISS) at 1-Year and 2-Years Follow-Up Selected by the Lasso |
One-Year Follow-Up
Lasso selected the TICS subscales tendency to worry, and social isolation; life events as well as vital exhaustion as influential in predicting CPI at 1-year follow up. The model refit (n = 166) resulted in RMSE of 17.05 (Table 2), which means, the predicted values of CPI differed 17.05 points from the observed values (on the 0 to 100 scale of CPI). The overall prediction model explained 38.4% of the variance of CPI (adjusted R2 = 0.384).
For DISS Lasso selected the TICS subscales tendency to worry, social isolation and work discontent as well as the I-SEE-subscale fatalistic externality and life events as predictors. The model refit (n = 55) resulted in RMSE of 16.74 (Table 2), which means, the predicted values of DISS differed 16.74 points from the observed values (on the 0 to 100 scale of DISS). The overall prediction model explained 21.9% of the variance of DISS (adjusted R² = 0.219).
2 Years Follow-Up
Lasso selected the TICS subscales work discontent, lack of recognition, social isolation, social conflicts and tendency to worry, perceived stress (PSS) as well as the I-SEE subscale internality as predictors for CPI at 2-years follow-up. The model refit (n = 113) resulted in RMSE of 15.57 (Table 2), which means, the predicted values of CPI differed 15.57 points from the observed values (on the 0 to 100 scale of CPI). The overall prediction model explained 27.9% of the variance of CPI (adjusted R² = 0.279).
For DISS Lasso selected the TICS subscales tendency to worry, social isolation and social conflicts, the I-SEE subscales internality, self-concept (ie self-efficacy) as well as social externality, and perceived stress (PSS) as predictors. The model refit (n = 104) resulted in RMSE of 13.84 (Table 2), which means the predicted values differed 13.84 points from the observed values of DISS (on the 0 to 100 scale of DISS). The overall prediction model explained 15.7% of the variance of DISS (adjusted R² = 0.157).
Discussion
To get insight into the relationship between different types of psychosocial stress and the chronification of LBP, several types of stress were analyzed simultaneously regarding their predictive power in a 2-year prospective observational study. In order to deal with typical statistical problems (multiple testing, multicollinearity) arising when multidimensional constructs are analyzed and assessed with several instruments, the Lasso regression analysis was applied, a statistical approach that still is rarely used in social science.37 With Lasso, a priori assessed psychosocial stress variables were selected that served as predictors for pain intensity and pain-related disability32 in participants with LBP at 1-year and 2-year follow-up. Due to the highly varying number of selected predictors during the cross-validation procedure, especially in the 2-years follow-up model, the results were interpreted using the coefficient paths of the predictors. If a predictor was selected even at a high degree of penalization, it was interpreted as stable.
The particular influences of the selected stress types decreased with time while the influence of resources such as self-efficacy increased from 1-year follow-up to 2-years follow-up. The stress types add to the already existing pain at baseline, which for both time courses revealed influences on future pain.40
The retrieved prediction models had RMSE between 13.84 and 17.05. This means, the predicted values of CPI and DISS at follow-up deviated from the observed values between 13.84 and 17.05 points on the 0 to 100 scale. These moderate prediction errors show that the selected predictors are able to predict pain intensity and disability to certain extend, but that there is still information missing to retrieve a more accurate prediction. This is also shown by the amount of explained variance of the models (from 15.7% to 38.4%). Further variables like depression,5 pain-related beliefs and other yellow flags would offer additional information.4,41,42
Stress
As expected, several psychosocial stress predictors influencing pain intensity and pain-related disability at 1-year or 2-years follow-up could be selected in participants with initial intermittent LBP. This effect was found especially at the 1-year follow-up, where tendency to worry, social isolation, vital exhaustion and the occurrence of life events predicted CPI, whereas the tendency to worry, social isolation, work discontent and life events predicted DISS. CPI at 2-years follow-up was predicted by work discontent, social stress (social isolation, lack of recognition, social conflicts), tendency to worry and perceived stress. DISS after 2 years was predicted by tendency to worry, social stress (social isolation, social conflicts) and perceived stress.
The results of this study point out a major influence of different stress experiences on pain maintenance in subjects with initial intermittent LBP. In addition to the known literature,14,15,43,44 not only work-related stress experiences are related to LBP maintenance but also factors related to social stress as reflected by the TICS subscales social isolation and social conflicts.27 This is supported by findings of earlier studies identifying poor social relationships being a risk factor for pain chronification.41,45
Vital exhaustion as a sign of stress-related fatigue turned out to predict pain intensity at 1-year follow-up, but not disability. At 2-years follow-up, this link was not found. Although still rare in LBP research, there are findings supporting this relationship of fatigue and pain in subjects with chronic LBP.46 It could be argued that the relationship is a more complex one including depression, and multiple interactions rather than linear relations may play a role.46,47 These were not addressed in the present design but warrant further attention.
The experience of negative life-events before baseline measurement has additional influence on LBP chronification in our sample, leading to higher pain intensity and disability at 1-year follow-up. This effect could not be detected at 2-years follow-up. Since life-events were measured as a dichotomous variable only (occurrence yes or no), the impact of cumulative critical life-events48 or their intensity49 should be addressed in future research.
Self-Efficacy
At 1-year follow-up only the I-SEE-subscale internality showed a small influence on pain intensity or disability. However, at 2-years follow-up, three of four subscales (internality, self-concept, social externality) showed predictive strength, especially in the prediction of pain-related disability. The subscales internality and self-concept form the scale self-efficacy of the I-SEE questionnaire. In our sample, higher self-efficacy at baseline was related to lower pain-related disability after 2 years. Self-efficacy is known to be a major component in dealing with stress and pain, as well as chronic illness.18,19 In line with recently published studies50–52 the results indicate a potential long term buffering effect of self-efficacy and control beliefs on the development of disability due to LBP, which should be studied further. The influence of the potential buffering factor self-efficacy was not present in the prediction of pain intensity. This finding underlines the importance of self-efficacy in back pain research. Back pain interventions addressing this aspect of patient´s personality have revealed positive effects.50,53
Limitations
Some limitations are to be considered when interpreting the results of the study. First, despite the large sample size, there is still a dropout rate of 48.3% at 2-years follow-up. One reason may be the follow-up procedures which included the presence of the subjects at the study sites at each measurement day over the 2 years. Still, for this analysis, it was possible to use an initial complete case sample of n = 588. Second, the usage of several similar scales reflecting overlapping dimensions of the same construct (TICS and PSS) should be questioned in further research or analyses. Although Lasso is a robust method for this purpose due to the penalization procedure, highly linked predictors still may lead to less precise interpretations.37 It should also be noted that the majority of the subjects reported low initial levels of pain intensity or disability as well as low initial levels of stress. The impact of psychosocial stress as a precursor of chronic pain should therefore be analyzed further in samples with chronic pain patients.
Conclusion
The presented results of this longitudinal study on subjects with intermittent LBP confirm the importance of stress in a social and work context for pain chronification in the time course of 1 and 2 years. It was not possible to identify one predominant factor. In contrast, the influencing factors varied depending on the time course and whether pain intensity or pain-related disability was addressed. In turn, self-efficacy could be identified as a personal resource factor potentially buffering stress effects on pain disability in the long run. Our results highlight the influence of psychosocial factors including stress experiences and self-efficacy. They also underline the importance to differentiate between stress types such as social stress or work-related stress since these may have different influences on LBP development. These issues should be addressed in a differentiated manner not only in the treatment of patients with chronic LBP but also in preventive treatment approaches for subjects presenting low initial back pain levels but not yet chronic pain complaints.
Abbreviations
CPG, Chronic pain grade questionnaire; CPI, CPG scale characteristic pain intensity; DISS, CPG scale disability due to pain; I-SEE, Inventory of self-efficacy and externality; Lasso, least absolute shrinkage selection operator; LBP, low back pain; PSS, perceived stress scale; RMSE, root mean squared error; TICS, Trier inventory for chronic stress; VE, vital exhaustion.
Ethics Approval
All clinical investigations were conducted according to the Declaration of Helsinki. Final ethical approval was provided on January 25, 2012, by the major institutional ethics review board of the University of Potsdam, Germany (number 36/2011).
Acknowledgments
The authors thank Juliane Müller, Steffen Müller, Josephine Stoll, Hannes Kaplick, Tilmann Engel, Philipp Flößel, Daniela Schubert, Simone Gantz, Jessica de Witt Huberts, Anja Weiffen, Michael Fliesser, and all local principal investigators for the invaluable support in study design. We also thank both the technical and medical staff at the study sites for their investment during study conduction.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The present study was funded by the German Federal Institute of Sport Science on behalf of the Federal Ministry of the Interior of Germany. It was realized within MiSpEx – the National Research Network for Medicine in Spine Exercise (grant number: 080102A/11-14). All sources of funding for the research reported are declared. The funder did not influence data collection, analysis, interpretation, or writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. doi:10.1136/annrheumdis-2013-204428
2. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–147. doi:10.1016/j.mayocp.2014.09.010
3. Nicholas MK, Linton SJ, Watson PJ, Main CJ, Group DFW. Early identification and management of psychological risk factors (“yellow flags”) in patients with low back pain: a reappraisal. Phys Ther. 2011;91(5):737–753. doi:10.2522/ptj.20100224
4. Pincus T, Kent P, Bronfort G, Loisel P, Pransky G, Hartvigsen J. Twenty-five years with the biopsychosocial model of low back pain-is it time to celebrate? A report from the twelfth international forum for primary care research on low back pain. Spine (Phila Pa 1976). 2013;38(24):2118–2123. doi:10.1097/BRS.0b013e3182a8c5d6
5. Glattacker M, Heyduck K, Jakob T. Yellow flags as predictors of rehabilitation outcome in chronic low back pain. Rehabil Psychol. 2018;63(3):408–417. doi:10.1037/rep0000200
6. Jegan NR, Brugger M, Viniol A, et al. Psychological risk and protective factors for disability in chronic low back pain - a longitudinal analysis in primary care. BMC Musculoskelet Disord. 2017;18(1):114. doi:10.1186/s12891-017-1482-8
7. McEwen BS, Kalia M. The role of corticosteroids and stress in chronic pain conditions. Metabolism. 2010;59(Suppl. 1):S9–15. doi:10.1016/j.metabol.2010.07.012
8. Wippert PM, Wiebking C. Stress and alterations in the pain matrix: a biopsychosocial perspective on back pain and its prevention and treatment. Int J Environ Res Public Health. 2018;15(4). doi:10.3390/ijerph15040785
9. Juster R-P, McEwen BS, Lupien SJ. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev. 2010;35(1):2–16. doi:10.1016/j.neubiorev.2009.10.002
10. Korte SM, Koolhaas JM, Wingfield JC, McEwen BS. The Darwinian concept of stress. Benefits of allostasis and costs of allostatic load and the trade-offs in health and disease. Neurosci Biobehav R. 2005;29(1):3–38. doi:10.1016/j.neubiorev.2004.08.009
11. McEwen BS. Physiology and neurobiology of stress and adaptation: central role of the brain. Physiol Rev. 2007;87(3):873–904. doi:10.1152/physrev.00041.2006
12. Dickerson SS, Kemeny ME. Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychol Bull. 2004;130(3):355–391. doi:10.1037/0033-2909.130.3.355
13. Fries E, Hesse J, Hellhammer J, Hellhammer DH. A new view on hypocortisolism. Psychoneuroendocrino. 2005;30(10):1010–1016. doi:10.1016/j.psyneuen.2005.04.006
14. Truchon M, Cote D, Schmouth ME, Leblond J, Fillion L, Dionne C. Validation of an adaptation of the stress process model for predicting low back pain related long-term disability outcomes: a cohort study. Spine (Phila Pa 1976). 2010;35(13):1307–1315. doi:10.1097/BRS.0b013e3181c03d06
15. Truchon M, Cote D, Fillion L, Arsenault B, Dionne C. Low-back-pain related disability: an integration of psychological risk factors into the stress process model. Pain. 2008;137(3):564–573. doi:10.1016/j.pain.2007.10.019
16. Nordeman L, Thorselius L, Gunnarsson R, Mannerkorpi K. Predictors for future activity limitation in women with chronic low back pain consulting primary care: a 2-year prospective longitudinal cohort study. BMJ Open. 2017;7(6):e013974. doi:10.1136/bmjopen-2016-013974
17. Schönfeld P, Preusser F, Margraf J. Costs and benefits of self-efficacy: differences of the stress response and clinical implications. Neurosci Biobehav Rev. 2017;75:40–52. doi:10.1016/j.neubiorev.2017.01.031
18. Jackson T, Wang Y, Wang Y, Fan H. Self-efficacy and chronic pain outcomes: a meta-analytic review. J Pain. 2014;15(8):800–814. doi:10.1016/j.jpain.2014.05.002
19. Lee H, Hubscher M, Moseley GL, et al. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain. 2015;156(6):988–997. doi:10.1097/j.pain.0000000000000146
20. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
21. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. 2007;11(2):153–163. doi:10.1016/j.ejpain.2005.12.008
22. Duray M, Yagci N, Ok N. Determination of physical parameters associated with self-efficacy in patients with chronic mechanic low back pain. J Back Musculoskelet Rehabil. 2018;31(4):743–748. doi:10.3233/bmr-170993
23. Koenig AL, Kupper AE, Skidmore JR, Murphy KM. Biopsychosocial functioning and pain self-efficacy in chronic low back pain patients. J Rehabil Res Dev. 2014;51(8):1277–1286. doi:10.1682/jrrd.2014.02.0047
24. Wippert P-M, Puschmann A-K, Drießlein D, et al. Development of a risk stratification and prevention index for stratified care in chronic low back pain. Focus: yellow flags (MiSpEx Network). PAIN Reports. 2017;e623. DOI: 10.1097/PR9.0000000000000623.
25. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
26. Büssing A. Translation of Cohen´s 10 Item PERCEIVED STRESS SCALE (PSS). University of Witten/Herdecke; 2011.
27. Schulz P, Schlotz W, Becker P. Trierer Inventar zum chronischen Stress (TICS). Göttingen: Hofgrefe; 2004.
28. Schnorpfeil P, Noll A, Wirtz P, et al. Assessment of exhaustion and related risk factors in employees in the manufacturing industry: a cross-sectional study. Int Arch Occup Environ Health. 2002;75(8):535–540. doi:10.1007/s00420-002-0369-6
29. Appels A, Hoppener P, Mulder P. A questionnaire to assess premonitory symptoms of myocardial infarction. Int J Cardiol. 1987;17(1):15–24. doi:10.1016/0167-5273(87)90029-5
30. Krampen G. Fragebogen zu Kompetenz- und Kontrollüberzeugungen (FKK). [Inventory on Competence and Control Beliefs]. Göttingen: Hofgrefe; 1991.
31. Greve W, Anderson A, Krampen G. Self-efficacy and externality in adolescence: theoretical conceptions and measurement in New Zealand and German secondary school students. int J Theor Phys. 2001;1(4):321–344. doi:10.1207/S1532706XID0104_02
32. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133–149. doi:10.1016/0304-3959(92)90154-4
33. Klasen BW, Hallner D, Schaub C, Willburger R, Hasenbring M. Validation and reliability of the German version of the Chronic Pain Grade questionnaire in primary care back pain patients. Psychosoc Med. 2004;1:Doc07.
34. Keil U. The worldwide WHO MONICA project: results and perspectives. Gesundheitswesen. 2005;67(S1):S38–45. doi:10.1055/s-2005-858240
35. R Development Core Team RF. R: A Language and Environment for Statistical Computing. [computer program]. Vienna, Austria: R Foundation for Statistical Computing; 2017.
36. Goeman JJ. L1 penalized estimation in the Cox proportional hazards model. Biometer J. 2010;52(1):70–84. doi:10.1002/bimj.200900028
37. Tibshirani R. Regression shrinkage and selection via the Lasso. J R Stat Soc B. 1996;58(1):267–288. doi:10.1111/j.2517-6161.1996.tb02080.x
38. Driesslein D, Küchenhoff H, Tutz G, Wippert PM. Variable selection and inference in a follow-up study on back pain. Technical Report, No 206, Department of Statistics, University of Munich. 2017. DOI: 10.5282/ubm/epub.40387.
39. Zhang CH, Zhang SS. Confidence intervals for low dimensional parameters in high dimensional linear models. J R Stat Soc B. 2014;76(1):217–242. doi:10.1111/rssb.12026
40. Papageorgiou AC, Croft PR, Thomas E, Ferry S, Jayson MI, Silman AJ. Influence of previous pain experience on the episode incidence of low back pain: results from the South Manchester Back Pain Study. Pain. 1996;66(2–3):181–185. doi:10.1016/0304-3959(96)03022-9
41. McKillop AB, Carroll LJ, Jones CA, Battie MC. The relation of social support and depression in patients with chronic low back pain. Disabil Rehabil. 2017;39(15):1482–1488. doi:10.1080/09638288.2016.1202335
42. Pinheiro MB, Ferreira ML, Refshauge K, et al. Symptoms of depression and risk of new episodes of low back pain: a systematic review and meta-analysis. Arthritis Care Res (Hoboken). 2015;67(11):1591–1603. doi:10.1002/acr.22619
43. Gheldof EL, Vinck J, Vlaeyen JW, Hidding A, Crombez G. Development of and recovery from short- and long-term low back pain in occupational settings: a prospective cohort study. Eur J Pain. 2007;11(8):841–854. doi:10.1016/j.ejpain.2006.12.012
44. Gheldof EL, Vinck J, Vlaeyen JW, Hidding A, Crombez G. The differential role of pain, work characteristics and pain-related fear in explaining back pain and sick leave in occupational settings. Pain. 2005;113(1–2):71–81. doi:10.1016/j.pain.2004.09.040
45. Villumsen M, Holtermann A, Samani A, Madeleine P, Jorgensen MB. Social support modifies association between forward bending of the trunk and low-back pain: cross-sectional field study of blue-collar workers. Scand J Work Environ Health. 2016;42(2):125–134. doi:10.5271/sjweh.3549
46. Snekkevik H, Eriksen HR, Tangen T, Chalder T, Reme SE. Fatigue and depression in sick-listed chronic low back pain patients. Pain Med. 2014;15(7):1163–1170. doi:10.1111/pme.12435
47. Sturgeon JA, Darnall BD, Kao MC, Mackey SC. Physical and psychological correlates of fatigue and physical function: a Collaborative Health Outcomes Information Registry (CHOIR) study. J Pain. 2015;16(3):291–298.e291. doi:10.1016/j.jpain.2014.12.004
48. Young Casey C, Greenberg MA, Nicassio PM, Harpin RE, Hubbard D. Transition from acute to chronic pain and disability: a model including cognitive, affective, and trauma factors. Pain. 2008;134(1–2):69–79. doi:10.1016/j.pain.2007.03.032
49. Wippert PM, Fliesser M, Krause M. Risk and protective factors in the clinical rehabilitation of chronic back pain. J Pain Res. 2017;10:1569–1579. doi:10.2147/jpr.S134976
50. Fordham B, Ji C, Hansen Z, Lall R, Lamb SE. Explaining how cognitive behavioral approaches work for low back pain: mediation analysis of the back skills training trial. Spine (Phila Pa 1976). 2017;42(17):E1031–e1039. doi:10.1097/brs.0000000000002066
51. Karayannis NV, Jull GA, Nicholas MK, Hodges PW. Psychological features and their relationship to movement-based subgroups in people living with low back pain. Arch Phys Med Rehabil. 2017. doi:10.1016/j.apmr.2017.08.493
52. Skidmore JR, Koenig AL, Dyson SJ, Kupper AE, Garner MJ, Keller CJ. Pain self-efficacy mediates the relationship between depressive symptoms and pain severity. Clin J Pain. 2015;31(2):137–144. doi:10.1097/ajp.0000000000000094
53. Michalski D, Roick C, Hinz A. Zusammenhang der Veränderungen psychologischer und subjektiv-beschwerdebezogener Parameter durch Training der Rumpfmuskulatur bei Rückenschmerzpatienten. Manuelle Medizin. 2007;45(3):175–182. doi:10.1007/s00337-007-0498-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.