Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Strategies for Managing Fluids and Electrolytes in High-Output Stomas: A Systematic Review and Evidence Summary
Authors Wen A ![]() , Jiao Y, Wang N, Xu J, Xu X, Du L, Lv L
, Jiao Y, Wang N, Xu J, Xu X, Du L, Lv L
Received 3 September 2025
Accepted for publication 24 January 2026
Published 10 February 2026 Volume 2026:19 564953
DOI https://doi.org/10.2147/JMDH.S564953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Anna Wen,1,* Yanxia Jiao,2,* Ning Wang,2 Jie Xu,1 Xinyue Xu,1 Li Du,1 Lin Lv3
1Evidence-Based Nursing Center, School of Nursing, Lanzhou University, Lanzhou, Gansu, People’s Republic of China; 2Wound and Ostomy Care Center, Outpatient Department, Gansu Provincial Hospital, Lanzhou, Gansu, People’s Republic of China; 3Evidence-Based Nursing Center, School of Nursing, Lanzhou University, Wound and Ostomy Care Center, Outpatient Department, Gansu Provincial Hospital, NHC Key Laboratory of Diagnosis and Therapy of Gastrointestinal Tumor, Lanzhou, Gansu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Lv, Evidence-Based Nursing Center, School of Nursing, Lanzhou University, Wound and Ostomy Care Center, Outpatient Department, Gansu Provincial Hospital, NHC Key Laboratory of Diagnosis and Therapy of Gastrointestinal Tumor, #28 Yanxi Road, Chenguan District, Lanzhou, Gansu, People’s Republic of China, Email [email protected]
Purpose: This study aimed to explore intervention strategies for fluid and electrolyte regulation in patients with high-output stomas, to optimize their clinical outcomes and quality of life.
Results: Fifteen experimental and semi-experimental studies were systematically reviewed. Interventions were categorized into five types by therapeutic purpose and route: gastrointestinal motility/anti-secretory agents, Glucagon-like Peptide-1/2 (GLP-1/2) analogs, rehydration/electrolyte supplements, micronutrient supplements, and dietary restriction. Key HOS complications included hyponatremia, hypomagnesemia, metabolic acidosis, hypokalemia, hypocalcemia, and kidney injury.
Conclusion: Hydro-electrolyte management in patients with HOS requires a multidisciplinary approach that integrates fluid management, pharmacotherapy, nutritional support, and surgical intervention. This framework may reduce dehydration-related readmission and improve outcomes. Future large-scale prospective studies are warranted to verify the efficacy, safety, and novel therapies, explore new therapeutic targets/drugs, and develop standardized guidelines, with an emphasis on individualized management for complex cases and prioritizing patient quality of life.
Keywords: dehydration prevention, hyponatremia, hypomagnesemia, pharmacotherapy, multidisciplinary team
Introduction
Enterostomy is a temporary measure in the clinical surgical treatment of abdominal emergencies, and also an auxiliary measure for radical surgery in the management of cancer, inflammatory bowel disease, and other related diseases. The number of people using colostomy stands at over one million in the United States and 102,000 in the United Kingdom.1,2 In China, more than 100,000 new ostomy patients are diagnosed every year, and the total number of ostomy patients has surpassed 1 million.3
The creation of a stoma directly disrupts the physiological continuity of the intestinal tract. Specifically, since ileostomies are situated in the intestinal region critical for absorptive function, the absorptive surface area is significantly reduced following surgery, leading to disorders in the transport and absorption of chyme and digestive juices. The human body secretes approximately 4 L of endogenous digestive fluids (including saliva, gastric juice, pancreaticobiliary juice, etc) daily, which are usually absorbed by the intestines, leaving only 1 to 2 L to enter the colon.4
High-output stomas (HOS) represent one of the most challenging postoperative complications of ostomy creation, with an overall incidence of 23%,5 significantly impeding postoperative recovery. It is characterized by increased stoma output and loss of water and electrolytes. Uncontrolled HOS over the long term can result in electrolyte imbalances, dehydration, and even complications like renal function impairment. Considering current studies, the diagnosis of HOS primarily relies on three following criteria, with variations across clinical guidelines and research: (1) a stoma output exceeding 2000 mL/d for three or more consecutive days;6 (2) a stoma output more than 1500 mL/d for two successive days;7 (3) a stoma output greater than 1000 mL/d for more than three consecutive days.8 These criteria reflect the heterogeneous definition of HOS in the literature, with no universal diagnostic standard currently established. Hydroelectrolyte management plays a crucial role in maintaining postoperative internal environment stability, as circulating blood volume, organ function, and metabolic status are all significantly influenced by the balance of hydroelectrolytes.
Currently, the management of HOS faces numerous challenges: medical personnel often lack systematic knowledge and practical experience.9 Globally, systematic evidence-based guidelines specifically addressing hydroelectrolyte management in HOS remain limited; current strategies primarily focus on etiological identification and symptomatic interventions, while a standardized multidisciplinary team (MDT) - driven comprehensive management framework has not yet been fully established. This can lead to delayed diagnosis or inappropriate management in some patients, thereby exacerbating their conditions. Thus, experienced multidisciplinary team care is crucial for patient education and management.10 This review contextualizes management of HOS within global guidelines (National Institute for Health and Care Excellence: www.nice.org.uk/guidance/mib286. European Society for Clinical Nutrition and Metabolism: https://doi.org/10.1136/gut.2006.091108), and aims to: (1) maintain fluid-electrolyte balance and prevent dehydration and electrolyte disorders; (2) offer a comprehensive reference for medical personnel to develop adequate fluid and electrolyte management protocols tailored to this patient population.
Materials and Methods
This evidence synthesis followed the PRISMA 2020 Statement. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (ID: CRD420251089227).
Search Strategy
Following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines,11 a comprehensive literature search was performed across various databases, including PubMed, Cochrane Library, Web of Science (WOS), Embase, China Biomedical (CBM), China National Knowledge Infrastructure (CNKI), Wanfang, and VIP databases. The search used keywords such as “Enterostomy/ Stoma”, “water/ fluid management”, “electrolyte management”, “medication/drug/pharmacologic therapy”, “diet*/nutrition/food/nutrition management/dietary management”, and “complication management”. Free-text terms and Medical Subject Headings (MeSH) terms were combined and adjusted according to the requirements of each database. Figure 1 outlines the literature search process. The search encompassed all available literature from the establishment of each database up to December 2025.
 |
Figure 1 PRISMA flow diagram of literature search and study selection. A total of 128,779 records were identified through database searching, including Cochrane Library (n=21,826), PubMed (n=47,696), Web of Science (n=59,202), CNKI (n=15), VIP (n=15), Wanfang (n=14), and CBM (n=11). After removing 106,938 duplicate records, 21,841 records were screened by title and abstract. A total of 21,483 irrelevant records were excluded based on population or topic, and 358 full-text articles were assessed for eligibility. Among these, 186 articles were excluded (134 for wrong study type, 14 for off-topic, and 9 for other reasons), with 15 studies finally included in the review. |
Study Population
The Population, Intervention, Comparison, Outcome, Study design (PICOS) framework is employed to clarify the scope of this systematic review and evidence synthesis. [P] The study population included adults (age >18 years) with a HOS (ileo-, jejuno-, and/or colostomy with residual small intestine, output >1500mL/day for ≥2 days) as defined by the original authors, regardless of underlying cause. [I] Interventions included fluid/electrolyte/drug/nutrition/complication treatment to manage HOS. [C] Interventions were compared with each other, placebos, and/or no interventions. [O] The primary outcome was correction of fluid and electrolyte balance disorder. Secondary outcomes included quality of life, mortality, morbidity, and complications. [S] Types of research design included Randomized Controlled Trials (RCTs), cohort studies, and case-control studies (n≥7).
Eligibility Criteria
Inclusion criteria: (1) Studies focusing on the management of fluid and electrolyte balance in adult HOS patients; (2) Evidence types including guidelines, clinical decisions, evidence summaries, randomized controlled trials(RCTs), expert consensus, or expert opinion; (3) Publications in Chinese or English.
Exclusion criteria: (1) Duplicate publications or updated versions of previously included studies; (2) Translated materials or interpretative documents based on guidelines; (3) Incomplete references or inaccessible full texts; (4) Studies with a quality evaluation grade of C or lower, indicating low-quality evidence; (5) Studies focusing on pure colostomies without residual small intestine.
Results
Search Results
A systematic review of 15 experimental and quasi-experimental studies was conducted in the present study. Interventions of the assessed studies included the following categories based on therapeutic purposes and administration routes: (1) Gastrointestinal motility regulators and anti-secretory agents: clonidine;12 budesonide;13 loperamide;14–16 codeine;14 omeprazole;17,18 and ranitidine.17 (2) GLP-1/2 analogs: liraglutide;19 and teduglutide.20 (3) Rehydration and electrolyte supplements: Pharmaniaga oral rehydration salts plus;21 Glucodrate® 500 mL administration;22 glucose electrolyte solution, glucose-polymer electrolyte solution, or salt capsules;23 and 0.9% saline + 5% dextrose + MgSO4.24 (4) Micronutrient supplements for electrolyte balance: 1-α-OH vitamin D3 or 1,25(OH)2 vitamin D3, with optional subsequent addition of magnesium oxide in cases of incomplete symptom resolution.25 (5) Dietary intervention: oral intake limitation to achieve stoma output at less than 1000 mL/day.26 The details of the interventions are presented in Table 1.
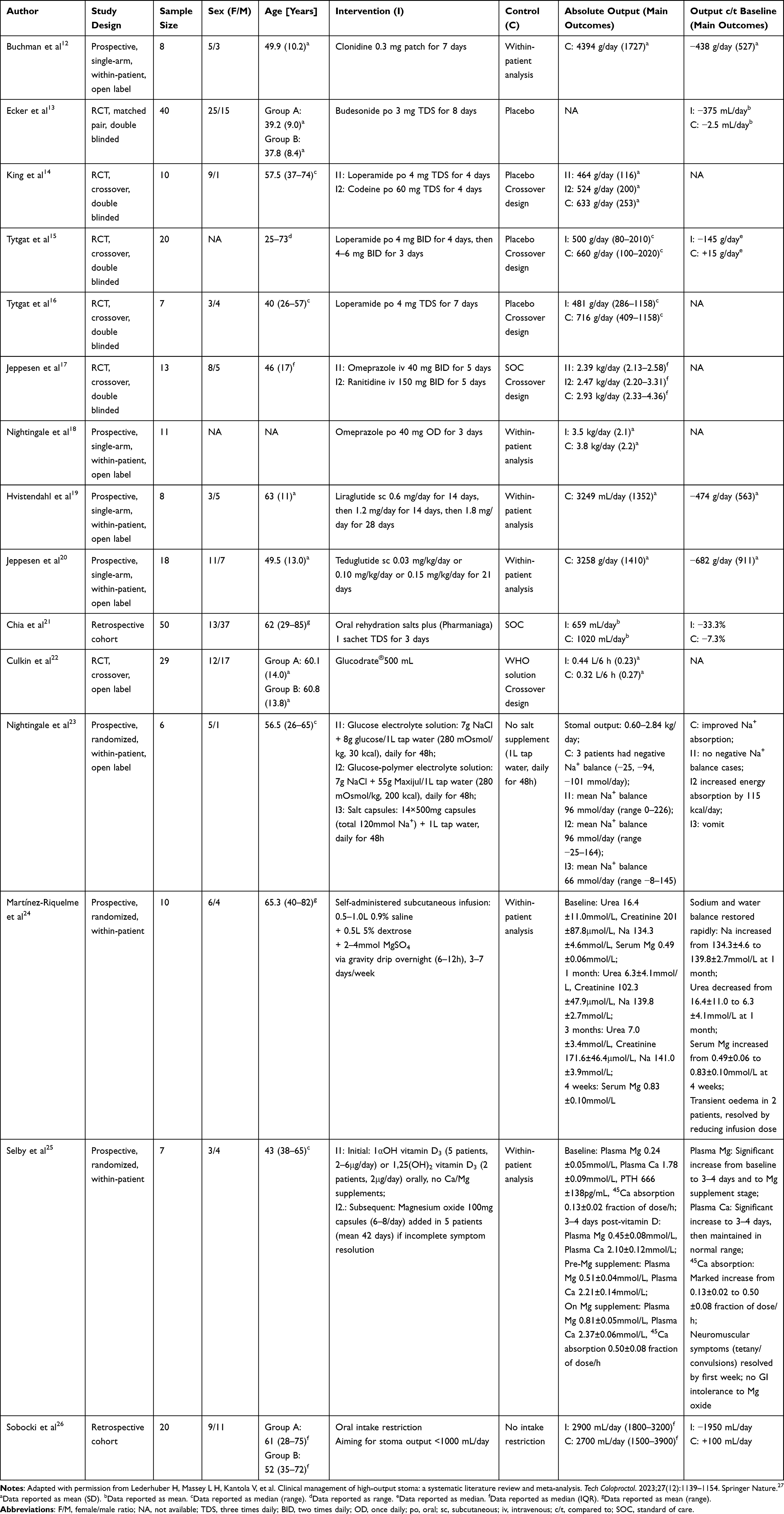 |
Table 1 Characteristics of the Included Studies |
Notably, a key limitation identified across the included studies is the lack of standardized protocols for oral food and fluid intake. Intestinal/stomal output is inherently dependent on the volume and composition of oral intake. Yet, most studies did not control for baseline dietary patterns, caloric intake, or consistency of fluid consumption among participants. Additionally, potential indirect effects of interventions on stoma output were observed: some pharmacological agents (such as GLP-1 analogs and high-dose loperamide) may modulate appetite, which could secondarily reduce oral intake and consequently lower stoma output, independent of their direct effects on intestinal motility or secretion.
Management of Electrolyte, Acid-Base, and Renal Complications in High-Output Stomas
Hyponatremia
In patients with HOS, the loss of sodium-rich secretions triggers a sensation of thirst, leading to the consumption of hypotonic fluids. This drives sodium from the plasma into the bowel, increasing stomal output and perpetuating a vicious cycle of acute kidney injury, dehydration, and further electrolyte loss.23,28–31
Hypomagnesemia
Hypomagnesemia, prevalent in up to 78% of jejunostomy patients,31 is a critical electrolyte disorder in the management of HOS. Its pathophysiology is multifactorial, primarily driven by the direct loss of magnesium-rich digestive fluids and secondary hyperaldosteronism,32,33 which enhances renal magnesium excretion. Contributing factors include a reduced intestinal absorptive surface area, malabsorption leading to magnesium soap formation (bicarbonate loss from high-output stoma effluent, which indirectly impairs magnesium absorption by altering intestinal pH),34,35 insufficient dietary intake, and the use of certain medications such as proton pump inhibitors(PPIs).36 This magnesium depletion often coexists with hypokalemia, though hypokalemia is relatively rare in HOS patients, and hypocalcemia, creating a synergistic electrolyte imbalance. Hypokalemia typically arises from secondary hyperaldosteronism induced by sodium depletion, where the body prioritizes sodium retention at the cost of increased renal excretion of potassium and magnesium.37 Furthermore, chronic hypomagnesemia, frequently accompanied by metabolic acidosis, disrupts calcium-magnesium homeostasis, leading to decreased bone density and an augmented risk profile for fractures and calciphylaxis.38
Metabolic Acidosis
The development of metabolic acidosis in individuals with HOS is attributable to two key factors: excessive loss of carbonate and the kidneys’ reduced ability to excrete acid loads when sodium depletion is present.39 The primary pathophysiological event is the depletion of the terminal ileum and right colon, the anatomical sites most responsible for the reabsorption of the approximately 70–80 mmol/day of luminal bicarbonate. Consequently, large volumes of alkaline intestinal fluid are lost, leading to a severe depletion of the body’s alkali reserve. Concurrently, the significant fluid loss results in volume depletion and secondary hyperaldosteronism. This creates a critical renal dilemma: while the kidneys strive to conserve sodium, this process inherently impairs their ability to excrete hydrogen ions and regenerate bicarbonate in the proximal tubule. Aldosterone itself further inhibits distal acid secretion. The combination of ongoing bicarbonate loss from the stoma and impaired renal compensation for daily metabolic acid loads induces persistent high-anion-gap metabolic acidosis.40
Hypokalemia
Jejunostomy discharge has low potassium (about 15 mmol/L), with net stoma loss only if residual jejunum < 50 cm.41 Hypokalemia mainly stems from sodium depletion-induced secondary aldosteronism or hypomagnesemia-impaired potassium transport.42
Hypocalcemia
Hypocalcemia in HOS stems from multiple mechanisms. Fat malabsorption leads to the formation of calcium soaps, preventing its absorption.43 Concurrently, damage to the intestinal mucosa and impaired renal hydroxylation hinder the activation and absorption of vitamin D, which is essential for calcium uptake.43 Furthermore, metabolic acidosis and volume depletion can increase renal calcium excretion, collectively disrupting calcium homeostasis.44,45
Kidney Injury & Renal Failure
Excessive stoma drainage and electrolyte disturbances predispose to dehydration and renal impairment, with stoma-related fluid loss linked to acute kidney injury (AKI) and a 17% 30-day readmission rate.46 Delayed fluid replacement causes renal ischemia, reduced glomerular filtration, and tubular injury, progressing to AKI; chronic imbalance induces irreversible chronic renal failure.47 High-output stomas are an independent risk factor for AKI,48 primarily driven by hypovolemia resulting from the loss of sodium-rich fluid.49 The prognosis is abysmal, with a 30 to 90 day mortality risk increased 2.7 fold, approaching 60%.49 Therefore, meticulous fluid and electrolyte management is crucial in preventing this fatal complication.
Discussion
Fluid Management
Optimal fluid management for patients with HOS demands an individualized approach based on the patient’s net secretor or absorber status. For net secretors, parenteral support is often essential to maintain balance, while net absorbers may be managed with optimized oral or enteral intake.50 Initial treatment of dehydration involves intravenous saline to achieve “oral zero”, followed by a cautious reintroduction of restricted fluids. The primary goals include stable body weight maintenance plus approximately 800 mL daily urine output that has sodium concentration above 20 mmol/L.51
Monitoring plays a critical role, with the most vital parameters including daily weight measurements, fluid balance assessments, and stoma output. In contrast to the potentially deceptive nature of plasma sodium, urinary sodium represents a far more reliable indicator of sodium depletion status, with a value below 10 mmol/L suggesting significant sodium loss.52 Serum creatinine and urinary sodium should be measured frequently during the initial phase and periodically thereafter.
It is essential to emphasize that intestinal/stomal output is dynamically influenced by oral food and fluid intake—an important confounding factor that is rarely standardized in the reviewed studies. Variability in baseline dietary habits and ad libitum fluid consumption may have contributed to heterogeneous stoma output responses across interventions. For instance, patients with higher baseline oral intake may exhibit greater reductions in output following dietary restriction, independent of pharmacologic effects. In contrast, inconsistent fluid intake could mask or exaggerate the efficacy of rehydration strategies.
A cornerstone of management is the strict restriction of hypotonic fluid intake (water, tea, coffee) to below 500–1000 mL daily, as their intake promotes sodium efflux into the intestinal lumen, worsening dehydration.26 This finding is supported by Sobocki’s study,26 where oral intake limitation (aimed at < 1000 mL daily stoma effluent) resulted in a mean reduction of 1950 mL/day in stoma output, compared to a 100 mL/day increase in the non-restriction group—even though baseline output was slightly higher in the intervention group (2900 mL/day vs 2700 mL/day). When daily stoma discharge is under 1200 mL, patients can preserve fluid-electrolyte balance through dietary sodium intake, whereas those with higher outputs require glucose-saline solutions or salt capsules.23 Nightingale’s study23 demonstrated the efficacy of targeted sodium supplementation: glucose electrolyte solution (7g NaCl + 8g glucose/1L), glucose-polymer electrolyte solution (7g NaCl + 55g Maxijul/1L), and salt capsules (14×500mg capsules + 1L water) all achieved positive sodium balance, in contrast to the negative sodium balance observed in patients receiving only tap water. Notably, the glucose-polymer solution also increased energy absorption by 115 kcal/day, addressing the dual challenges of electrolyte balance and nutritional deficiency. An effective rehydration solution, such as St. Mark’s Electrolyte Mix, is formulated with 20g of glucose, 2.5g of sodium bicarbonate, and 3.5g of sodium chloride per liter of water and should be consumed in small, frequent sips.29 Sodium chloride capsules are an alternative, but they can cause gastrointestinal discomfort.23 For patients with very short remaining jejunum (<100 cm) or those who cannot be maintained on an oral regimen, regular subcutaneous or parenteral saline supplementation becomes necessary to prevent severe dehydration and renal failure.51
Medication
If oral fluid restriction and glucose-saline fail to maintain HOS fluid balance, multiple pharmacologic strategies can reduce stoma output, including antidiarrheals, antisecretory agents, as well as budesonide, clonidine, and GLP-1/2 agonists, with pre-meal dosing critical for postprandial secretion surges. Antidiarrheals like loperamide and codeine phosphate cut ileostomy volume by 20–30%.14,15,53–55 Loperamide is preferred due to its non-sedating, non-addictive properties and no fat malabsorption.14,16 High-dose liquid loperamide (caution with osmolality) or crushed/opened tablets (if intact in output) may be needed, especially in short bowel patients with disrupted enterohepatic circulation (12–24 mg/dose). A combination of 4 mg loperamide and 60 mg codeine phosphate, administered four times daily, is more effective.56 Oral budesonide (3mg thrice daily) reduces ileostomy output by ~30% via enhancing water absorption, with a higher response in patients with ≤20cm ileal resection.13 Transdermal clonidine (0.3mg patch) modestly lowers fecal weight/volume and reduces sodium loss in proximal jejunostomy patients.12
A crucial consideration when evaluating pharmacologic efficacy is the potential for appetite modulation. Some agents may reduce stoma output indirectly by suppressing appetite and subsequent oral intake, rather than solely via direct intestinal effects. For example, GLP-1 agonists (like liraglutide) are known to exert anorexigenic effects, which may contribute to the observed 13% reduction in jejunostomy output beyond their direct impact on intestinal absorption. Similarly, high-dose loperamide or codeine may cause nausea in some patients, inadvertently reducing oral intake and stoma output. This confounding effect is rarely quantified in the included studies, highlighting the need for standardized dietary protocols (such as controlled caloric intake, fixed fluid volume) in future research to isolate direct pharmacologic effects from indirect intake-related changes.
Antisecretory drugs reduce bowel secretions. Proton pump inhibitors (PPIs), such as omeprazole, 40 mg oral daily or intravenous (IV) administration twice daily, reduce jejunostomy output, particularly in net secretors with an output exceeding 2 L per day.17,18 IV PPIs are recommended due to impaired absorption;57 Histamine H2 Receptor Antagonists (400 mg cimetidine IV four times daily, 300 mg ranitidine oral twice daily) are alternatives for PPI-related hypomagnesemia.17,58 Studies show omeprazole (oral/IV) outperforms ranitidine in output reduction, with similar efficacy to octreotide (50 mg SC twice daily) but no impact on electrolyte absorption—requiring continued supplementation.17 Additionally, GLP-1 agonists —— liraglutide (escalated to 1.8mg/d SC) cuts jejunostomy output by ~13% and improves energy absorption;19 GLP-2 agonists —— teduglutide (0.03–0.15mg/kg/d SC) reduces faecal wet weight by 711g/day, boosts wet weight absorption by 22%, and increases jejunal villus height in short bowel patients.20
Nutrition Therapy
Regarding dietary intake, malnutrition risk is prevalent in HOS patients, as significant volumes of liquids and essential nutrients are depleted through the stoma; therefore, nutritional modifications are required.59 For most patients with HOS who depend exclusively on oral feeding, a 30% approximate rise in caloric intake is necessary to offset malabsorption-related losses;60 this goal can be attained via dietary modifications and oral nutritional formulas with dietitian oversight, but semi-factorial beverages and fiber-containing supplements are not recommended because they may increase stoma expulsion or are not easily tolerated.61 In terms of fat intake, for individuals undergoing jejunostomy, a dietary fat provision comprising 30–40% of the overall daily energy requirement is clinically recommended, as this does not increase stoma expulsion and does not interfere with mineral absorption.35 Carbohydrates should account for 40–50% of energy and should be based on low-fiber starchy foods, avoiding large amounts of simple sugars to prevent increased stoma discharge.62 It is recommended that protein contribute approximately 20% of the overall caloric content.62 A high-carbohydrate, low-fat diet is indicated for jejuno-colonic anastomosis patients, aiming at boosting colonic absorption as well as lowering steatorrhea risk.63 If enteral feeds are administered, sodium chloride supplementation is mandatory to titrate the total sodium concentration of the formula to roughly 90 mmol/L, with concurrent maintenance of an osmolality level of about 300 mOsm/kg.23 Two key scenarios warrant parenteral nutrition initiation: first, when oral energy absorption is less than 1/3 of total intake; second, when the small bowel segment remaining after jejunostomy measures under 75 cm.64
Surgical Options
Surgical strategies for individuals with HOS demand a comprehensive evaluation of reconstructive potential and individual anatomical variance. It has been proven that restoration of intestinal continuity markedly enhance nutritional status in individuals who develop short bowel syndrome that arises as a consequence of extensive intestinal resection, enabling 77% of individuals to wean off parenteral nutrition within five years.65 However, any surgical intervention involving intestinal bypass or reconstruction must be predicated on a personalized anatomical assessment, given the profound individual variation in human small intestinal length. Consequently, precise measurement of the remaining small bowel is a critical step when planning corrective or metabolic procedures, as it is essential for preventing postoperative short bowel syndrome and severe malnutrition.66 Furthermore, to address adaptive dilation of the intestinal remnant, autologous gastrointestinal reconstruction techniques, such as the Serial Transverse Enteroplasty Procedure (STEP) or Longitudinal Intestinal Lengthening and Tailoring (LILT), present surgical options to augment absorptive surface area, though their application requires stringent adherence to indications.67 Ultimately, when all conservative and reconstructive measures prove futile, intestinal transplantation emerges as the definitive consideration for end-stage intestinal failure.68
Hypomagnesemia
Hypomagnesemia secondary to HOS requires a multifaceted approach, starting with correcting underlying water and sodium depletion.69 Oral magnesium oxide (12–24 mmol per day) is frequently prescribed nocturnally for mild cases, leveraging slower intestinal transport to enhance absorption.42 However, gastrointestinal side effects like nausea and diarrhea are common due to poor salt absorption. Selby’s study demonstrated that combining magnesium oxide (6–8 capsules/day) with vitamin D achieved significant improvements in plasma magnesium: from a baseline of 0.24 ± 0.05 mmol/L to 0.81 ± 0.05 mmol/L with supplementation. Plasma calcium also increased from 1.78 ± 0.09 mmol/L to 2.37 ± 0.06 mmol/L, and 45Ca absorption nearly quadrupled (from 0.13 ± 0.02 to 0.50 ± 0.08 fraction of dose/h), with neuromuscular symptoms (tetany/convulsions) resolving within the first week—highlighting the synergistic benefits of combined vitamin D and magnesium supplementation.25
If oral intake fails, intravenous magnesium sulfate—typically four mmol diluted in 500–1000 mL saline—is recommended for rapid correction. Martínez-Riquelme’s study further supported the role of parenteral supplementation: subcutaneous infusion of 0.9% saline + 5% dextrose + 2–4mmol MgSO4 (3–7 days/week) restored serum magnesium from 0.49±0.06 mmol/L to 0.83±0.10 mmol/L at 4 weeks, along with improvements in sodium (134.3±4.6 to 139.8±2.7 mmol/L) and urea (16.4±11.0 to 6.3±4.1 mmol/L) levels. Transient edema occurred in 2 patients but resolved with dose reduction, indicating a favorable safety profile.24
A unique therapeutic option involves administering oral 1-α-hydroxycholecalciferol gradually (0.25–9.00 μg/day every 2–4 weeks) to improve magnesium balance.25,70 Crucially, this condition rarely exists in isolation; concurrent hypokalemia and hypocalcemia are frequent. Potassium supplementation alone is ineffective without magnesium correction, as low magnesium impedes cellular uptake.71 Monitoring is critical. Serum magnesium levels should be checked every 1–2 days initially, then weekly as stability improves.72 Patients with severe absorption disorders may require home infusions or outpatient monitoring.
Kidney Injury & Renal Failure
Avoid the use of drugs that are detrimental to the kidneys, such as non-steroidal anti-inflammatory drugs. Kidney-protecting drugs, such as angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor antagonists (ARBs), can be used when necessary. In the case of severe renal failure and ineffective conservative treatment, renal replacement therapy, such as hemodialysis and peritoneal dialysis, may be required.73
International Guideline Framework for Management of HOS
International guidelines, such as National Institute for Health and Care Excellence (NICE), European Society for Clinical Nutrition and Metabolism (ESPEN), and British Association for Parenteral and Enteral Nutrition (BAPEN: https://www.bapen.org.uk/pdfs/bifa/bifa-top-tips-series-1-updated.pdf) demonstrate a highly synergistic, evidence-based framework for managing HOS, centered on individualized risk assessment stratified by remaining small bowel length to inform tiered treatment protocols. A cornerstone across all recommendations is the limitation to hypotonic liquid ingestion, supplemented by electrolyte solutions with sodium concentration matched to stoma losses. Pharmacologically, there is a consensus recommendation for antimotility and antisecretory agents; however, guidelines also caution against the risk of PPI-induced hypomagnesemia, proposing H2 receptor antagonists as a feasible substitute in those with parenteral nutrition dependence. Novel therapies such as GLP-2 analogues are incorporated into recommendations, with a strong emphasis on their administration within specialized centers.
Furthermore, these guidelines collectively advocate for a service model centered on multidisciplinary teams and specialized centers, a strategy designed to ensure both quality of care and cost-effectiveness while providing essential emergency support pathways. This model transcends purely technical interventions by recognizing the patient as an expert in their own management, integrating a philosophy of psychosocial support. In doing so, it constructs a comprehensive management system that spans from foundational fluid management to cutting-edge therapies, and from individualized assessment to systemic support, thereby securing the scientific rigor and advanced nature of clinical practice on a global scale.
Conclusion
Based on the findings of this study, fluid and electrolyte management of HOS demands a multidisciplinary approach that integrates precise fluid and electrolyte strategies with targeted pharmacologic and nutritional interventions. The clinical significance of this comprehensive framework is profound, directly translating into improved patient outcomes by mitigating life-threatening complications. By implementing evidence-based protocols—ranging from restricting hypotonic fluids to utilizing advanced therapies like GLP-2 analogues—clinicians can substantially reduce hospital readmissions related to dehydration. The ultimate goal is not merely to correct biochemical imbalances but to empower patients for self-management, thereby reducing the long-term burden of care and enhancing functional independence.
Looking forward, the current evidence base, while robust in its principles, reveals critical gaps that must be addressed to refine and standardize care. Priority areas for future research include the rigorous evaluation of novel therapies, such as teduglutide and other GLP-2 analogues, through well-designed, large-scale clinical trials with standardized oral intake protocols to control for confounding variables and ascertain their long-term effectiveness, their safety profile, as well as their ideal positioning within treatment algorithms. Concurrently, there is an urgent need to develop universally accepted, standardized management guidelines that can harmonize practices across different healthcare systems. Until such data are available, a wealth of practical insights can be gleaned from meticulously documented case reports and case series. These narratives are invaluable for capturing innovative or highly individualized management approaches, particularly for rare or complex patient populations where large-scale trials remain infeasible. This ensures that every patient, regardless of the complexity of their condition, can benefit from the collective evolution of clinical expertise.
Abbreviations
HOS, high-output stomas; RCTs, Randomized Controlled Trials; MDT, Multidisciplinary Team; PROSPERO, International Prospective Register of Systematic Reviews; WOS, Web of Science; CBM, China Biomedical Database; CNKI, China National Knowledge Infrastructure; MeSH, Medical Subject Headings; PICOS, Population, Intervention, Comparison, Outcome, Study design; IV, intravenous; GLP-1/2, Glucagon-like Peptide-1/2; PPI, Proton Pump Inhibitors; AKI, Acute Kidney Injury; ACEIs, Angiotensin-Converting Enzyme Inhibitors; ARBs, Angiotensin II Receptor Antagonists; STEP, Serial Transverse Enteroplasty Procedure; LILT, Longitudinal Intestinal Lengthening and Tailoring; NICE, National Institute for Health and Care Excellence; ESPEN, European Society for Clinical Nutrition and Metabolism; BAPEN, British Association for Parenteral and Enteral Nutrition.
Data Sharing Statement
Data is available on request from the corresponding author.
Ethics Approval and Informed Consent
The study protocol (reference number LZUHLXY20250103) was approved by the Ethics Committee of Lanzhou University, ensuring compliance with the Declaration of Helsinki and its amendments.
Funding
This study has been funded by “The Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (grant number 2019PT320005)” and “In-hospital Scientific Research Fund Project of Gansu Provincial Hospital (24GSSYF-2, 24GSSYF-7)”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agarwal S, Ehrlich A. Stoma dermatitis: prevalent but often overlooked. Dermatitis. 2010;21(3):138–15. doi:10.2310/6620.2010.09103
2. Burch J. Caring for peristomal skin: what every nurse should know. Br J Nurs. 2010;19(3):166, 168, 170 passim. doi:10.12968/bjon.2010.19.3.46538
3. Li R, Wu W, Sun X, Ju M. Current status of health beliefs and their influencing factors in patients with permanent enterostomy. J China Med Univ. 2024;53(04):373–378.
4. Kiela PR, Ghishan FK. Physiology of intestinal absorption and secretion. Best Pract Res Clin Gastroenterol. 2016;30(2):145–159. doi:10.1016/j.bpg.2016.02.007
5. Shen Y, Dai Z, Li J, Wu X, Wang S, Wang Q. Incidence and influencing factors of high-output ileostomy in adults: a meta-analysis. Chin J Gen Pract. 2023;21(02):324–328. doi:10.16766/j.cnki.issn.1674-4152.002874
6. Takeda M, Takahashi H, Haraguchi N, et al. Factors predictive of high-output ileostomy: a retrospective single-center comparative study. Surg Today. 2019;49(6):482–487. doi:10.1007/s00595-018-1756-2
7. Adaba F, Vaizey CJ, Warusavitarne J. Management of intestinal failure: the high-output enterostomy and enterocutaneous fistula. Clin Colon Rectal Surg. 2017;30(3):215–222. doi:10.1055/s-0037-1598163
8. Seifarth C, Augustin LN, Lehmann KS, et al. Assessment of risk factors for the occurrence of a high-output ileostomy. Front Surg. 2021;8:642288. doi:10.3389/fsurg.2021.642288
9. Zhang Q, Sun J, Wang D, Wang Q, Hu H. Knowledge, attitudes, practices and associated factors regarding high output stoma of ileostomy among colorectal surgical nurses: a multicenter cross-sectional study. Support Care Cancer. 2023;32(1):12. doi:10.1007/s00520-023-08228-x
10. Medlin S. Nutritional and fluid requirements: high-output stomas. Br J Nurs. 2012;21(6):S22–5. doi:10.12968/bjon.2012.21.Sup6.S22
11. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
12. Buchman AL, Fryer J, Wallin A, Ahn CW, Polensky S, Zaremba K. Clonidine reduces diarrhea and sodium loss in patients with proximal jejunostomy: a controlled study. JPEN J Parenter Enteral Nutr. 2006;30(6):487–491. doi:10.1177/0148607106030006487
13. Ecker KW, Stallmach A, Seitz G, Gierend M, Greinwald R, Achenbach U. Oral budesonide significantly improves water absorption in patients with ileostomy for Crohn disease. Scand J Gastroenterol. 2003;38(3):288–293. doi:10.1080/00365520310000645a
14. King RF, Norton T, Hill GL. A double-blind crossover study of the effect of loperamide hydrochloride and codeine phosphate on ileostomy output. Aust NZ J Surg. 1982;52(2):121–124. doi:10.1111/j.1445-2197.1982.tb06083.x
15. Tytgat GN, Huibregtse K. Loperamide and ileostomy output--placebo-controled double-blind crossover study. Br Med J. 1975;2(5972):667. doi:10.1136/bmj.2.5972.667
16. Tytgat GN, Huibregtse K, Dagevos J, van den Ende A. Effect of loperamide on fecal output and composition in well-established ileostomy and ileorectal anastomosis. Am J Dig Dis. 1977;22(8):669–676. doi:10.1007/bf01078345
17. Jeppesen PB, Staun M, Tjellesen L, Mortensen PB. Effect of intravenous ranitidine and omeprazole on intestinal absorption of water, sodium, and macronutrients in patients with intestinal resection. Gut. 1998;43(6):763–769. doi:10.1136/gut.43.6.763
18. Nightingale JM, Walker ER, Farthing MJ, Lennard-Jones JE. Effect of omeprazole on intestinal output in the short bowel syndrome. Aliment Pharmacol Ther. 1991;5(4):405–412. doi:10.1111/j.1365-2036.1991.tb00044.x
19. Hvistendahl M, Brandt CF, Tribler S, et al. Effect of liraglutide treatment on jejunostomy output in patients with short bowel syndrome: an open-label pilot study. JPEN J Parenter Enteral Nutr. 2018;42(1):112–121. doi:10.1177/0148607116672265
20. Jeppesen PB, Sanguinetti EL, Buchman A, et al. Teduglutide (ALX-0600), a dipeptidyl peptidase IV resistant glucagon-like peptide 2 analogue, improves intestinal function in short bowel syndrome patients. Gut. 2005;54(9):1224–1231. doi:10.1136/gut.2004.061440
21. Chia CLK, Tai YS, Tan KY. A preliminary study of the use of oral rehydration salts in decreasing ileostomy output. Tech Coloproctol. 2017;21(7):587–588. doi:10.1007/s10151-017-1646-4
22. Culkin A, Gabe SM, Nightingale JMD. A new palatable oral rehydration solution: a randomised controlled cross-over study in patients with a high output stoma. J Hum Nutr Diet. 2022;35(1):94–101. doi:10.1111/jhn.12935
23. Nightingale JM, Lennard-Jones JE, Walker ER, Farthing MJ. Oral salt supplements to compensate for jejunostomy losses: comparison of sodium chloride capsules, glucose electrolyte solution, and glucose polymer electrolyte solution. Gut. 1992;33(6):759–761. doi:10.1136/gut.33.6.759
24. Martínez-Riquelme A, Rawlings J, Morley S, Kendall J, Hosking D, Allison S. Self-administered subcutaneous fluid infusion at home in the management of fluid depletion and hypomagnesaemia in gastro-intestinal disease. Clin Nutr. 2005;24(1):158–163. doi:10.1016/j.clnu.2004.09.016
25. Selby PL, Peacock M, Bambach CP. Hypomagnesaemia after small bowel resection: treatment with 1 alpha-hydroxylated vitamin D metabolites. Br J Surg. 1984;71(5):334–337. doi:10.1002/bjs.1800710504
26. Sobocki J, Zaczek Z, Jurczak P, et al. Restricted v. unrestricted oral intake in high output end-jejunostomy patients referred to reconstructive surgery. Br J Nutr. 2021;125(10):1125–1131. doi:10.1017/s0007114520003360
27. Lederhuber H, Massey L H, Kantola V E, Siddiqui M R, Sayers A E, McDermott F D, Daniels I R and Smart N J. Clinical management of high-output stoma: a systematic literature review and meta-analysis. Tech Coloproctol. 2023;27(12):1139–1154. doi:10.1007/s10151-023-02830-1
28. Newton CR, Drury P, Gonvers JJ, McIntyre P, Preston DM, Lennard-Jones JE. Incidence and treatment of sodium depletion in ileostomists. Scand J Gastroenterol Suppl. 1982;74:159–160.
29. Newton CR, Gonvers JJ, McIntyre PB, Preston DM, Lennard-Jones JE. Effect of different drinks on fluid and electrolyte losses from a jejunostomy. J R Soc Med. 1985;78(1):27–34. doi:10.1177/014107688507800106
30. Griffin GE, Fagan EF, Hodgson HJ, Chadwick VS. Enteral therapy in the management of massive gut resection complicated by chronic fluid and electrolyte depletion. Dig Dis Sci. 1982;27(10):902–908. doi:10.1007/bf01316574
31. Nightingale JM, Lennard-Jones JE, Gertner DJ, Wood SR, Bartram CI. Colonic preservation reduces need for parenteral therapy, increases incidence of renal stones, but does not change high prevalence of gall stones in patients with a short bowel. Gut. 1992;33(11):1493–1497. doi:10.1136/gut.33.11.1493
32. Hanna S, Mac II. The influence of aldosterone on magnesium metabolism. Lancet. 1960;2(7146):348–350. doi:10.1016/s0140-6736(60)91487-2
33. Horton R, Biglieri EG. Effect of aldosterone on the metabolism of magnesium. J Clin Endocrinol Metab. 1962;22:1187–1192. doi:10.1210/jcem-22-12-1187
34. Hessov I, Andersson H, Isaksson B. Effects of a low-fat diet on mineral absorption in small-bowel disease. Scand J Gastroenterol. 1983;18(4):551–554. doi:10.3109/00365528309181636
35. Ovesen L, Chu R, Howard L. The influence of dietary fat on jejunostomy output in patients with severe short bowel syndrome. Am J Clin Nutr. 1983;38(2):270–277. doi:10.1093/ajcn/38.2.270
36. Pisani LF, Filippi E, Vavassori S, Munizio N, Vecchi M, Pastorelli L. Effect of proton pump inhibitors on magnesium balance: is there a link to cardiovascular risk? Magnes Res. 2016;29(1):1–10. doi:10.1684/mrh.2016.0397
37. Elisaf M, Milionis H, Siamopoulos KC. Hypomagnesemic hypokalemia and hypocalcemia: clinical and laboratory characteristics. Miner Electrolyte Metab. 1997;23(2):105–112.
38. Richette P, Ayoub G, Lahalle S, et al. Hypomagnesemia associated with chondrocalcinosis: a cross-sectional study. Arthritis Rheum. 2007;57(8):1496–1501. doi:10.1002/art.23106
39. Bower TR, Pringle KC, Soper RT. Sodium deficit causing decreased weight gain and metabolic acidosis in infants with ileostomy. J Pediatr Surg. 1988;23(6):567–572. doi:10.1016/s0022-3468(88)80370-1
40. Adrogué HJ. Metabolic acidosis: pathophysiology, diagnosis and management. J Nephrol. 2006;19(Suppl 9):S62–9.
41. Jeppesen PB, Mortensen PB. Intestinal failure defined by measurements of intestinal energy and wet weight absorption. Gut. 2000;46(5):701–706. doi:10.1136/gut.46.5.701
42. Nightingale J, Woodward JM. Guidelines for management of patients with a short bowel. Gut. 2006;55(Suppl 4):iv1–12. doi:10.1136/gut.2006.091108
43. Knight JO, Cotten LF, Ziegler TR, Vellanki P. A case of severe hypocalcemia caused by malabsorption due to partial gastrectomy and small bowel resection. AACE Clin Case Rep. 2021;7(5):323–326. doi:10.1016/j.aace.2021.04.002
44. Lemann J, Litzow JR, Lennon EJ. Studies of the mechanism by which chronic metabolic acidosis augments urinary calcium excretion in man. J Clin Invest. 1967;46(8):1318–1328. doi:10.1172/jci105624
45. Alexander RT, Cordat E, Chambrey R, Dimke H, Eladari D. Acidosis and urinary calcium excretion: insights from genetic disorders. J Am Soc Nephrol. 2016;27(12):3511–3520. doi:10.1681/asn.2016030305
46. Li L, Lau KS, Ramanathan V, et al. Ileostomy creation in colorectal cancer surgery: risk of acute kidney injury and chronic kidney disease. J Surg Res. 2017;210:204–212. doi:10.1016/j.jss.2016.11.039
47. Barbar SD, Clere-Jehl R, Bourredjem A, et al. Timing of renal-replacement therapy in patients with acute kidney injury and sepsis. N Engl J Med. 2018;379(15):1431–1442. doi:10.1056/NEJMoa1803213
48. Pencovich N, Silverman JS, Horesh N, et al. Readmission with acute kidney injury following ileostomy: patterns and predictors of a common phenomenon. Langenbecks Arch Surg. 2023;408(1):96. doi:10.1007/s00423-023-02842-3
49. Gómez-Fregoso JA, Zaragoza JJ, González-Duarte JA, et al. Severe acute kidney injury associated with intestinal ostomies. Kidney Med. 2025;7(10):101093. doi:10.1016/j.xkme.2025.101093
50. Nightingale JM, Lennard-Jones JE, Walker ER, Farthing MJ. Jejunal efflux in short bowel syndrome. Lancet. 1990;336(8718):765–768. doi:10.1016/0140-6736(90)93238-k
51. Nightingale JMD. How to manage a high-output stoma. Frontline Gastroenterol. 2022;13(2):140–151. doi:10.1136/flgastro-2018-101108
52. Rondon H, Badireddy M. Hyponatremia. In: StatPearls. StatPearls Publishing LLC.; 2025.
53. Fordtran JS. Stimulation of active and passive sodium absorption by sugars in the human jejunum. J Clin Invest. 1975;55(4):728–737. doi:10.1172/jci107983
54. Avery ME, Snyder JD. Oral therapy for acute diarrhea. The underused simple solution. N Engl J Med. 1990;323(13):891–894. doi:10.1056/nejm199009273231307
55. Newton CR. Effect of codeine phosphate, Lomotil, and Isogel on iileostomy function. Gut. 1978;19(5):377–383. doi:10.1136/gut.19.5.377
56. Nightingale JM, Lennard-Jones JE, Walker ER. A patient with jejunostomy liberated from home intravenous therapy after 14 years; contribution of balance studies. Clin Nutr. 1992;11(2):101–105. doi:10.1016/0261-5614(92)90019-m
57. Pironi L, Cuerda C, Jeppesen PB, et al. ESPEN guideline on chronic intestinal failure in adults - Update 2023. Clin Nutr. 2023;42(10):1940–2021. doi:10.1016/j.clnu.2023.07.019
58. Epstein M, McGrath S, Law F. Proton-pump inhibitors and hypomagnesemic hypoparathyroidism. N Engl J Med. 2006;355(17):1834–1836. doi:10.1056/NEJMc066308
59. Vasilopoulos G, Makrigianni P, Polikandrioti M, et al. Pre- and post-operative nutrition assessment in patients with colon cancer undergoing ileostomy. Int J Environ Res Public Health. 2020;17(17):6124. doi:10.3390/ijerph17176124
60. Sturm A, Layer P, Goebell H, Dignass AU. Short-bowel syndrome: an update on the therapeutic approach. Scand J Gastroenterol. 1997;32(4):289–296. doi:10.3109/00365529709007674
61. McIntyre PB, Fitchew M, Lennard-Jones JE. Patients with a high jejunostomy do not need a special diet. Gastroenterology. 1986;91(1):25–33. doi:10.1016/0016-5085(86)90434-8
62. Byrne T, Veglia L, Camelio M, et al. Clinical observations: beyond the prescription: optimizing the diet of patients with short bowel syndrome. Nutr Clin Pract. 2000;15:306–311. doi:10.1177/088453360001500606
63. Matarese LE, O’Keefe SJ, Kandil HM, Bond G, Costa G, Abu-Elmagd K. Short bowel syndrome: clinical guidelines for nutrition management. Nutr Clin Pract. 2005;20(5):493–502. doi:10.1177/0115426505020005493
64. Rodrigues CA, Lennard-Jones JE, Thompson DG, Farthing MJ. Energy absorption as a measure of intestinal failure in the short bowel syndrome. Gut. 1989;30(2):176–183. doi:10.1136/gut.30.2.176
65. Adaba F, Rajendran A, Patel A, et al. Mesenteric infarction: clinical outcomes after restoration of bowel continuity. Ann Surg. 2015;262(6):1059–1064. doi:10.1097/sla.0000000000001100
66. Tacchino RM. Bowel length: measurement, predictors, and impact on bariatric and metabolic surgery. Surg Obes Relat Dis. 2015;11(2):328–334. doi:10.1016/j.soard.2014.09.016
67. Iyer KR. Surgical management of short bowel syndrome. JPEN J Parenter Enteral Nutr. 2014;38(1 Suppl):53s–59s. doi:10.1177/0148607114529446
68. Kaufman SS, Avitzur Y, Beath SV, et al. New Insights Into the Indications for Intestinal Transplantation: consensus in the Year 2019. Transplantation. 2020;104(5):937–946. doi:10.1097/tp.0000000000003065
69. Makowsky MJ, Bell P, Gramlich L. Subcutaneous magnesium sulfate to correct high-output ileostomy-induced hypomagnesemia. Case Rep Gastroenterol. 2019;13(2):280–293. doi:10.1159/000501121
70. Fukumoto S, Matsumoto T, Tanaka Y, Harada S, Ogata E. Renal magnesium wasting in a patient with short bowel syndrome with magnesium deficiency: effect of 1 alpha-hydroxyvitamin D3 treatment. J Clin Endocrinol Metab. 1987;65(6):1301–1304. doi:10.1210/jcem-65-6-1301
71. Solomon R. The relationship between disorders of K+ and Mg+ homeostasis. Semin Nephrol. 1987;7(3):253–262.
72. Seelig MS. Magnesium requirements in human nutrition. J Med Soc N J. 1982;79(11):849–850.
73. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–84. doi:10.1159/000339789
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.