Back to Journals » International Journal of Nanomedicine » Volume 21
Stimuli-Responsive Nanocarriers for Transdermal siRNA Delivery: Mechanisms, Challenges, and Therapeutic Strategies
Authors Jian Y, Ban M, Yan Z, Wang Y, Che Z, Ren W, Cao Y, Wang Z ![]() , Yuan Y
, Yuan Y ![]()
Received 12 January 2026
Accepted for publication 5 June 2026
Published 17 June 2026 Volume 2026:21 595572
DOI https://doi.org/10.2147/IJN.S595572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. RDK Misra
Yanmin Jian,1,* Minghui Ban,2,* Zhenyang Yan,1,* Yansui Wang,2 Ziyan Che,3,4 Wenwen Ren,5 Yuan Cao,1 Zao Wang,6 Yue Yuan7
1School of Life Science and Medicine, Shandong University of Technology, Zibo, 244000, People’s Republic of China; 2School of Medical Informational Engineering, Shandong University of Traditional Chinese Medicine, Jinan, 250355, People’s Republic of China; 3Co-Innovation Center for the Sustainable Forestry in Southern China and Department of Food Science and Technology, Nanjing, 210037, People’s Republic of China; 4College of Light Industry and Food Engineering, Nanjing Forestry University, Nanjing, 210037, People’s Republic of China; 5Department of Clinical Medicine, The First Clinical Medical College, Jinzhou Medical University, Jinzhou, 121001, People’s Republic of China; 6Department of Medical Laboratory Technology, School of Medicine, Hunan Normal University, Changsha, 410006, People’s Republic of China; 7Laboratory of Neurological Diseases and Brain Function, the Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Yuan, Email [email protected]
Background: Small interfering RNA (siRNA) holds therapeutic promise for dermatological diseases, but clinical translation is limited by the stratum corneum barrier and the instability of naked siRNA. Nanocarrier-based systems offer effective solutions by enhancing skin penetration, improving siRNA stability, and enabling targeted intracellular delivery.
Methods: This review synthesizes current evidence on nanocarrier-mediated transdermal siRNA delivery. Key design parameters: particle size, surface charge, degradability, and morphology are evaluated for their roles in skin permeation and intracellular trafficking. Stimuli-responsive nanocarriers (pH, enzymatic, light, temperature) and physical enhancement strategies, including microneedles, sonophoresis, and laser ablation, are also reviewed.
Results: Lipid-polymer hybrid nanoparticles demonstrate notable advantages in stability, biocompatibility, and co-delivery capability. Stimuli-responsive systems enable spatiotemporal control of siRNA release, while physical enhancement technologies significantly improve cutaneous permeability. Disease-specific delivery strategies tailored to pathological microenvironments including psoriasis, melanoma, and chronic wounds illustrate the feasibility of adapting material composition, structural parameters, and responsiveness to different therapeutic contexts.
Conclusion: Advances in intelligent nanomaterials, responsive carrier engineering, and physical facilitation approaches provide a solid foundation for clinically viable transdermal siRNA therapies. Future development will benefit from integrating precise release control with disease-tailored delivery strategies to overcome biological barriers and optimize therapeutic outcomes.
Keywords: siRNA, transdermal delivery, nanocarrier, lipid-polymer hybrid nanoparticles, stimuli-responsive systems
Introduction
Dermatological diseases impose a substantial global health burden and include chronic inflammatory disorders, chronic wounds, and cutaneous malignancies that often require long-term treatment and precise local intervention. Although conventional topical agents, systemic immunosuppressants, and biologics have improved disease control, their clinical utility remains limited by insufficient skin penetration, systemic adverse effects, high cost, and incomplete control of disease-driving molecular pathways.1,2 These limitations are especially evident in refractory skin disorders, where effective treatment requires both local delivery and precise regulation of pathogenic signaling networks.3
At the tissue level, the stratum corneum and the highly organized epidermal architecture severely restrict the penetration of macromolecules.3,4 Moreover, the physiological microenvironment at the skin surface can further compromise the stability of therapeutic agents and hinder their transdermal permeation.5
Small interfering RNA (siRNA) offers a highly sequence-specific strategy for silencing disease-relevant genes and therefore represents an attractive therapeutic modality for dermatological applications.6 By directing the RNA-induced silencing complex to complementary mRNA, siRNA enables programmable and potent post-transcriptional gene suppression.7 This mechanism is particularly appealing for skin diseases involving well-defined inflammatory, proliferative, or fibrotic pathways.8,9
However, despite the success of systemic siRNA therapeutics such as Patisiran, the clinical development of transdermal siRNA therapy remains largely at the preclinical stage. This translational gap reflects the unique difficulty of delivering fragile nucleic acid cargo across the skin barrier while preserving intracellular bioactivity.8,10 Unprotected “naked” siRNA is rapidly degraded by nucleases in biological environments, with a half-life ranging from minutes to hours.10 Its hydrophilicity and strong anionic character further limit transmembrane transport and hinder endosomal escape, leading to very low delivery efficiency.9 These coupled extracellular and intracellular constraints indicate that successful siRNA therapy cannot rely on formulation optimization at a single step, but instead requires delivery systems capable of protecting siRNA, enhancing cutaneous transport, promoting cellular internalization, and facilitating cytosolic release.
Nanocarriers have emerged as a central strategy for addressing these barriers because their physicochemical properties can be tuned to improve siRNA stability, regulate skin permeation, and support intracellular trafficking.11 In particular, stimuli-responsive nanocarriers and physically assisted transdermal technologies have created new opportunities for spatiotemporally controlled and disease-adapted delivery.5,8
Therefore, this review provides an integrated analysis of nanocarrier-mediated transdermal siRNA delivery from a multistage barrier perspective. Unlike earlier reviews that primarily catalog material types or general delivery platforms, we emphasize three interconnected dimensions: (i) how different nanocarriers are structurally designed to overcome sequential extracellular and intracellular barriers; (ii) how stimuli-responsive and physically assisted systems improve transdermal and intracellular delivery; and (iii) how carrier design can be tailored to representative pathological microenvironments, including psoriasis, skin tumors, and chronic wounds. Through this framework, we aim to clarify current design principles, identify translational bottlenecks, and outline future directions for clinically viable transdermal siRNA therapy.
Literature Search and Research Distribution
This review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (Figure 1).
 |
Figure 1 PRISMA flowchart. |
Inclusion Criteria
The study selection process followed by the Population, Intervention, Comparison, Outcomes, and Study (PICOS) framework.
(1) P: Studies involving in vitro (eg, cell lines), ex vivo (eg, excised skin), or in vivo (animal models or human subjects) models related to skin or cutaneous diseases.
(2) I: Transdermal or topical delivery of siRNA mediated by nanotechnology-based carriers, with particular focus on systems exhibiting stimuli-responsive properties (eg, pH-, enzyme-, or temperature-responsive).
(3) C: No specific comparator was required for inclusion. However, studies comparing stimuli-responsive systems with non-responsive carriers or conventional formulations were prioritized during synthesis.
(4) O: Studies reporting at least one of the following metrics: skin penetration depth/efficiency, cellular uptake mechanisms, endosomal escape efficacy, gene silencing levels (mRNA or protein), or therapeutic outcomes in disease models (eg, psoriasis, melanoma, skin fibrosis, wound healing).
(5) S: Original research articles, systematic reviews, clinical trials, and patents published in English or Chinese.
Information Sources and Search Strategy
A systematic search was conducted across six electronic databases: PubMed, Web of Science, Scopus, Embase, SciFinder, and CNKI, covering all publications from database inception to March 2024. The search strategy combined keywords and subject headings related to four core concepts: (1) siRNA therapeutics, (2) transdermal/topical administration, (3) nanocarrier technology and stimuli-responsive systems, and (4) relevant skin pathologies. Boolean operators “AND” and “OR” were used to construct the search queries. Reference lists of included articles and related reviews were also manually screened to identify additional eligible studies.
Study Selection and Data Extraction
After removing duplicates using EndNote X9, two independent reviewers (A.B. and C.D.) screened the titles and abstracts of all retrieved records according to the predefined eligibility criteria. Full texts of potentially relevant articles were then assessed in detail. Any discrepancies between the reviewers were resolved through discussion or, when necessary, consultation with a senior reviewer (E.F).
A standardized data extraction form was used to collect relevant information from each included study, including: (1) first author and publication year; (2) nanocarrier characteristics (eg, composition, size, stimuli-responsiveness); (3) siRNA target and sequence; (4) experimental model (cell line or animal species); and (5) key quantitative outcomes and main findings.
Data Synthesis
A narrative synthesis was employed to summarize and integrate the findings from the included studies. The results were structured thematically, focusing on the design principles of stimuli-responsive nanocarriers, their mechanisms for overcoming skin and cellular barriers, and their therapeutic applications in different skin diseases.
A two-stage screening process was employed. In the initial screening, studies were assessed based on titles and abstracts, followed by a full-text assessment of the preliminarily selected articles. The database search yielded 1847 records, after duplicate removal, 1203 remained. Following the initial screening, 268 articles were selected for full-text review, and 88 met the inclusion criteria and were included in this analysis (Figure 2). Among these, 63 articles (71.6%) focused directly on nanocarrier-mediated therapeutic applications. These comprise lipid-based systems (liposomes, ethosomes, solid lipid nanoparticles) in 18 articles (28.6%), polymeric systems (PLGA, PEI, chitosan, dendrimers) with 15 articles (23.8%), lipid-polymer hybrid nanoparticles (LPHNs) in 12 articles (19.0%), inorganic nanoparticles (gold, mesoporous silica, magnetic nanoparticles) in 13 articles (20.6%), and stimuli-responsive hybrid systems in 5 articles (7.9%).
 |
Figure 2 Trend analysis of research publication (1975–2025). Notes: Key findings in technology evolution: Lipid-based System: A cornerstone technology that has consistently led the field, accumulating 18 papers by 2024. It primarily targets inflammatory diseases like psoriasis, leveraging its excellent biocompatibility. Polymeric Systems: Experienced rapid development after 2010, totaling 15 papers by 2024, and has excelled in research on the treatment of chronic wounds and fibrotic disorders. Inorganic Nanoparticles: Have carved out unique application niches, with 13 papers by 2024. Gold nanoparticles target tumors via photothermal effects, while mesoporous silica is utilized for complex wound management. Lipid-Polymer Hybrid Nanoparticles (LPHNs): A research hotspot, accumulating 12 papers by 2024. They are regarded as a platform balancing biocompatibility and stability, showing potential in combination therapies. Stimuli-Responsive Hybrid: Have grown rapidly since 2018. The integration of multi-responsive systems with physical tools like microneedles signals a paradigm shift toward integrated delivery strategies in the field. |
Among the 88 included studies, 61 (69.3%) were experimental research articles, 21 (23.9%) were reviews or perspectives, and 6 (6.8%) were clinical or translational studies. Based on publication period, the studies were grouped into four stages: the foundational phase (1998–2010) with 5 publications, the mechanism exploration phase (2011–2017) with 17 publications, the intelligent systems development phase (2018–2022) with 38 publications, and the clinical translation acceleration phase (2023–2024) with 28 publications, indicating the rapid advancement of stimuli-responsive delivery technologies in this field.
Regarding disease distribution among therapeutic studies (n = 63) (Figure 3), 21 studies (33.3%) focused on chronic inflammatory disorders (psoriasis, atopic dermatitis), 18 (28.6%) on skin malignancies (melanoma, squamous cell carcinoma), 15 (23.8%) on chronic wounds (diabetic ulcers, burn wounds), and 9 (14.3%) on fibrotic disorders (keloids, systemic sclerosis). Notably, 75.0% of these publications were published after 2017, reflecting the rapid growth of intelligent nanocarrier-based delivery technologies in transdermal siRNA therapy.
 |
Figure 3 Disease research focus. Notes: Delivery System Distribution by Disease Category: Lipid-Based Systems: Enriched in chronic inflammatory disorders (n = 7), mainly for TNF-a/IL-17/IL-23 siRNA delivery. Polymeric Systems: Broadly distributed across inflammation, malignancies, wounds, and fibrosis, supporting sustained release. Inorganic Nanoparticles: Preferentially used in malignancies and chronic wounds (n = 4 each), enabling photothermal or antimicrobial functions. LPHNs: Used in inflammation and wounds (n = 4 each), suitable for siRNA-drug co-delivery. Optimal Delivery Combinations by Disease: Chronic Inflammatory Disorders: Lipid-based systems ± physical enhancers improve SC penetration and siRNA delivery. Skin Malignancies: Photothermal AuNPs and pH/MMP-responsive LPHNs support intratumoral release and TME modulation. Fibrotic Disorders: Lipid/polymer carriers dominate HSP47-siRNA delivery, with responsive inorganic systems underexplored. |
In terms of stimuli-responsive mechanisms, pH-responsive systems were the most frequently investigated (15 studies), followed by enzyme-responsive systems (8 studies), which were particularly effective in targeting tumor microenvironments and inflammatory lesions. Physical enhancement techniques were also increasingly incorporated into nanocarrier designs, with microneedle-assisted delivery reported in 6 studies, fractional laser in 3 studies, and iontophoresis in 2 studies. Multi-responsive systems combining two or more stimuli represented an emerging trend in advanced delivery platforms, offering distinct advantages for spatiotemporal control of siRNA release and enhanced therapeutic outcomes.
The RNA Interference Pathway and the siRNA Delivery Imperative
Although percutaneous siRNA therapy has shown promise in various skin disease models, current research on its mechanisms and delivery system design remains fragmented and lacks a unified framework. To translate these findings into practical design principles, it is necessary to return to the fundamentals of RNA interference and outline of process of siRNA-mediated gene silencing from both molecular structural and intracellular signaling pathways. Based on this understanding, the key delivery constraints and corresponding design requirements under transdermal administration should be clarified. Therefore, this section first provides an overview of the molecular structure and mechanism of action of siRNA. It then summarizes the major delivery challenges, skin barrier penetration, cellular uptake, and intracellular transport, based on the anatomical and physiological characteristics of the skin. This will form the mechanistic basis for subsequent discussions on nanocarrier selection and structural optimization.
Molecular Architecture and Mechanism of Action of siRNA
RNAi is a sequence-specific gene-silencing mechanism, first described by Fire and Mello in 1998 and later recognized with the 2006 Nobel Prize in Physiology or Medicine.12 As the key effector of the RNAi pathway, siRNA represents a cornerstone technology for precision gene regulation and next-generation therapeutic intervention.
Structurally, a canonical siRNA is a 21–23 nucleotides double-stranded RNA (dsRNA) composed of a guide strand and a passenger strand.13 Its defining physicochemical characteristics a perfectly complementary duplex, 2-nucleotide 3′ overhangs, a 5′-phosphate group, a molecular weight of ca. 13–15 kDa, and a high net negative charge,14 fundamentally dictate its biological fate, influencing both in vivo stability and cellular internalization.
The RNAi cascade begins when exogenous siRNAs or endogenous long dsRNAs are processed by the RNase III enzyme Dicer into 21–23 nucleotide siRNA duplexes15 (Figure 4). These duplexes are then loaded into the RISC, during which accessory factors recruit the key endonuclease Argonaute 2 (AGO2) to form a pre-RISC assembly.9 Within this complex, an ATP-dependent helicase unwinds the siRNA duplex. During the maturation step, the passenger strand is discarded, and the guide strand is retained to generate the active RISC.9 The mature complex then uses the guide strand to identify complementary target mRNA. Upon binding, the AGO2 catalytic domain cleaves the target mRNA, leading to its rapid degradation.16 Importantly, RISC functions catalytically; a single complex can mediate multiple rounds of cleavage, which contributes to the high potency of siRNA and enables sustained gene silencing at substoichiometric concentrations.17
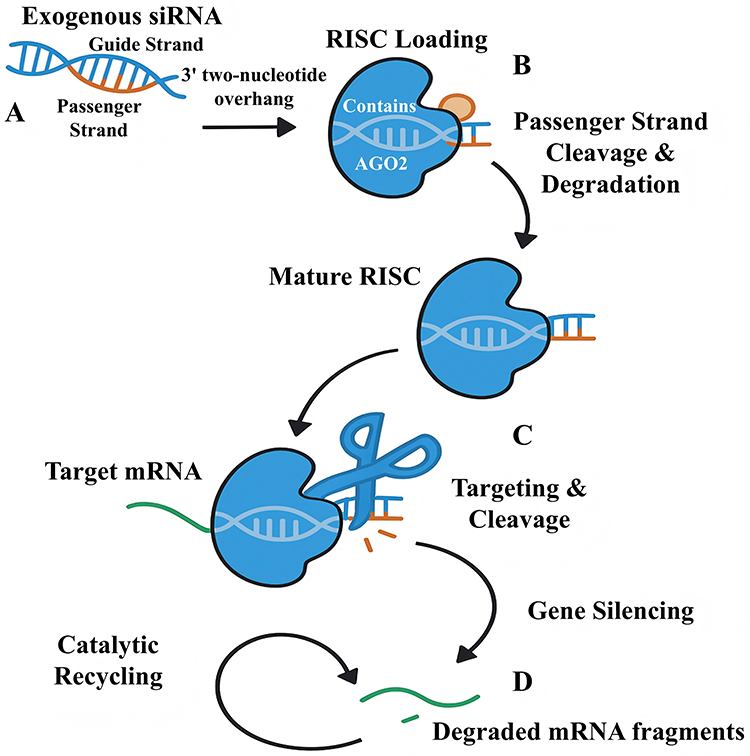 |
Figure 4 Cytoplasmic RNAi pathway mediated by exogenous siRNA. (A) Duplex siRNA with a 3′ two-nucleotide overhang enters the cytoplasm and is loaded into a pre-RNA-induced silencing complex (pre-RISC) containing the endonuclease AGO2. (B) AGO2 cleaves and releases the passenger strand, generating a mature RISC that retains the guide strand. (C) The active RISC binds to a fully complementary sequence on the target mRNA, and AGO2 catalyzes site-specific cleavage of the transcript. (D) The resulting mRNA fragments are rapidly degraded, while the intact RISC is recycled for multiple rounds of gene silencing. |
Compared with other RNAi effectors, such as microRNAs (miRNAs) and short hairpin RNAs (shRNAs), siRNA offers distinct advantages for therapeutic design. A key feature of siRNA is its requirement for perfect sequence complementarity to induce direct mRNA cleavage, in contrast to miRNAs, which typically bind with imperfect complementarity and mediate translational repression.18 Furthermore, unlike shRNAs that rely on nuclear processing and export, siRNAs act directly in the cytoplasm. This cytoplasmic mechanism makes siRNA particularly suitable for applications requiring rapid, transient, and tightly regulated gene modulation an essential characteristic for addressing dynamic pathological states in dermatological diseases where precise spatiotemporal control is needed.19
Principal Challenges in Transdermal siRNA Delivery
Despite its therapeutic potential, the clinical translation of siRNA for dermatological applications remains limited by multiple challenges spanning molecular design to in vivo performance. The primary barrier is the unique physiological architecture of the skin. As a macromolecular polyanion (13–15 kDa), siRNA shows poor penetration through the dual defense system formed by the stratum corneum’s “brick-and-mortar” lipid matrix and tight junctions beneath it.4 This barrier can become even more restrictive in pathological conditions such as psoriasis, where epidermal thickening and hyperkeratosis further limit the diffusion of therapeutic molecules to their target sites.
Naked siRNA is highly susceptible to degradation by endogenous nucleases in biological fluids. In serum-containing experimental systems, unmodified siRNA has often been reported to display a short half-life, in some cases of less than 30 minutes.20 Nuclease-rich environments at the skin surface and within interstitial tissues may further compromise siRNA integrity by accelerating phosphodiester backbone cleavage, thereby narrowing the therapeutic window. Furthermore, the strong anionic charge of siRNA leads to electrostatic repulsion with the similarly charged cell membrane, limiting cellular uptake.9 Even when internalized via endocytosis, most siRNA remains trapped in endo-lysosomal compartments instead of reaching the cytoplasm, where gene silencing occurs. This endosomal sequestration constitutes a major barrier to efficacy and can effectively eliminate the therapeutic activity of the delivered siRNA.21
Beyond physicochemical barriers, transdermal siRNA delivery also faces substantial biological challenges. Exogenous siRNA may be sensed by innate immune receptors, including Toll-like receptors such as TLR3 and TLR7/8, thereby triggering interferon signaling and pro-inflammatory cytokine production. However, this immunostimulatory risk can often be mitigated through rational sequence design and chemical modifications, such as 2′-O-methylation, 2′-fluoro substitution, and phosphorothioate backbone modification.22 In addition, conventional delivery approaches often lack sufficient cell-type specificity, which may reduce therapeutic efficiency and increase off-target exposure.23
We posit that these interlinked challenges necessitate a fundamental shift toward the design of advanced nanoparticle-based delivery systems. An ideal nanocarrier must integrate multiple functions within a single platform: protecting siRNA from enzymatic degradation, enhancing its penetration across the stratum corneum, promoting efficient internalization by target cells, and enabling robust endosomal escape. Only delivery systems that harmonize these functions are likely to achieve comprehensive optimization across the therapeutic pathway and improve the translational potential of siRNA for dermatological applications.24
Collectively, these sequential barriers indicate that transdermal siRNA therapy requires finely tunable delivery systems capable of integrating stabilization, barrier penetration, cellular uptake, and endosomal escape within a unified platform.
Types and Structural Design of Nanocarriers
The multistage limitations inherent to percutaneous siRNA delivery, including enzymatic degradation and protein adsorption on the skin surface, the physical barrier of the stratum corneum and epidermal architecture, as well as inadequate cellular uptake and insufficient endosomal escape, indicate that the in vivo fate of siRNA is shaped by a coupled sequence of delivery stages rather than by any single parameter. Thus, achieving stable and reproducible RNA interference under transdermal conditions requires delivery systems capable of integrating, within one platform, essential functions such as nucleic acid stabilization, transport across the cutaneous barrier, and efficient intracellular uptake and endosomal trafficking.3 Nanocarriers with tunable physicochemical properties, such as particle size, surface charge, and structural composition have therefore emerged as a central technological strategy for optimizing siRNA delivery behavior. Based on differences in material composition and structural configuration, nanocarrier systems used for transdermal siRNA delivery can be broadly grouped into three major categories: organic nanocarriers, inorganic nanocarriers, and organic-inorganic hybrid systems (Figure 5), each with distinct pharmacokinetic features and safety profiles.
 |
Figure 5 Comparative schematic of four representative nanocarrier platforms for siRNA delivery (schematic, not to scale). (A) Cationic liposome: a biomimetic bilayer vesicle composed of cationic lipids that electrostatically bind siRNA, with a PEG Corona providing steric stabilization. (B) PLGA nanoparticle: a solid polymer matrix that physically entraps siRNA, offering structural robustness and hydrolysis-driven sustained release. (C) LPHN: a core-shell architecture combining a high-loading polymer core with a biocompatible lipid shell and dense PEG corona, thereby extending circulation time. (D) MSN: a rigid inorganic carrier with high-surface-area mesopores for siRNA adsorption and stimuli-responsive gatekeeper enabling on-demand release. |
Organic Nanocarrier Systems
The excellent biocompatibility and compositional flexibility of lipid-based nanocarriers have established them as a central platform for siRNA delivery. Incorporating permeation enhancers such as ethanol or surfactants can further increase cutaneous deposition by 3- to 4-fold compared with conventional formulations.25,26 Among these systems, liposomes, one of the earliest and most widely used nanocarriers, facilitate siRNA transport by mimicking biological membranes. Typical liposomal formulations comprise structural lipids (eg, phosphatidylcholine, cholesterol), cationic lipids (eg, DOTAP), fusogenic lipids (eg, DOPE), and PEGylated lipids, which act synergistically to enhance siRNA binding and promote membrane fusion.20,27 Recent advances have yielded several important subclasses. Ionizable lipids that become protonated in the acidic endosomal environment are a key component of the integrated lipid nanoparticle platform used in Patisiran, the first FDA-approved siRNA therapeutic, where they contribute to siRNA encapsulation, stability, and endosomal release rather than acting as an isolated determinant of efficacy. Ultradeformable liposomes, whose membrane elasticity is enhanced by surfactant incorporation, can traverse pores substantially smaller than their own diameter under transdermal hydration or osmotic gradients, thereby improving transdermal delivery efficiency relative to conventional liposomes.28 Ethosomes, another vesicular platform, utilize high ethanol content (typically 20–45%) to perturb the ordered lipid lamellae of the stratum corneum and thereby enhance cutaneous penetration relative to conventional vesicular formulations.29
As a versatile alternative, polymeric nanoparticles provide advantages complementary to those of liposomes, particularly their structural robustness, sustained-release capability, and highly adaptable surface chemistry.30 The biodegradable polymer PLGA, enables controlled siRNA release through gradual hydrolysis of its ester backbone. In psoriasis-related experimental models, PLGA-based carriers have been reported to prolong local retention; however, the reported residence time of more than 96 hours should be interpreted in the context of the specific model and observation method used.31 PEI, a classical cationic polymer, is widely recognized for facilitating endosomal escape via the “proton sponge” effect; although the cytotoxicity of high-molecular-weight PEI remains a major translational concern. To address this limitation, strategies such as cross-linking low-molecular-weight PEI or grafting hydrophilic segments have been explored to improve biosafety while maintaining efficient transfection.21 Natural cationic polymers, including poly-L-lysine (PLL) and chitosan, have also been widely studied owing to their favorable biocompatibility. Importantly, the mode of siRNA association with the polymer matrix, whether through electrostatic binding, hydrophobic interaction, or physical entrapment plays a decisive role in determining the stability, protective capability, and release kinetics of the delivery system.11
LPHNs combine the advantages of distinct material systems and have shown promising therapeutic performance relative to single-component nanocarriers in multiple preclinical studies.32,33 These systems are commonly engineered into a core-shell configuration consisting of a polymeric core, an outer lipid bilayer, and a PEG-modified corona. The polymer core provides stable siRNA encapsulation and controlled release, the lipid shell enhances biocompatibility and membrane fusion capacity, and the PEG corona prolongs systemic circulation while reducing nonspecific protein adsorption. Empirical studies suggest that LPHNs can improve serum stability, cellular uptake, and endosomal escape relative to selected monocomponent comparators.34 Notably, the hybrid design also enables co-delivery of siRNA and small-molecule therapeutics, thereby producing synergistic therapeutic effects. For example, a lipid-PLGA hybrid nanoparticle co-loaded with anti-TNF-α siRNA and capsaicin achieved concurrent gene silencing and anti-inflammatory activity in a psoriasis model, with outcomes reported to be superior to the corresponding monotherapy groups.35
Inorganic and Hybrid Nanocarriers
Inorganic nanomaterials have expanded the design space for siRNA delivery because they provide properties that are difficult to obtain from purely organic carriers, including rigid structural control, high surface area, optical responsiveness, and versatile surface chemistry. Gold nanoparticles (AuNPs), for example, can be functionalized through thiol-gold bonding, electrostatic adsorption after cationic coating, or layer-by-layer assembly.36–38 These loading strategies influence siRNA binding stability, release behavior, and intracellular bioavailability, and therefore should be evaluated together with the biological model and comparator formulation used in each study.
A representative example is the use of spherical nucleic acid structures based on a 12-nm gold core. In the cited psoriasis-related study, anti-EGFR siRNA arranged densely on the AuNP surface penetrated reconstructed human epidermis and reached the basal layer, while reducing epidermal thickening in a psoriasis-like mouse model compared with the corresponding control treatment.39 This example supports the value of AuNPs as organized nucleic acid assemblies rather than simple passive carriers. In addition, AuNPs can provide photothermal responsiveness under near-infrared irradiation, which may transiently increase membrane permeability, assist endosomal escape, or trigger cargo release in selected experimental settings. These effects, however, depend strongly on irradiation parameters, particle size, surface coating, and tissue depth, and should not be generalized across all AuNP formulations.36,39
Mesoporous silica nanoparticles (MSNs) represent another inorganic platform with high surface area and tunable pore architecture. Their mesoporous structure allows adsorption or encapsulation of nucleic acids and can also support co-loading with small-molecule therapeutics.40–43 For example, mesoporous silica-coated silver nanoparticles co-delivering ciprofloxacin and siRNA have been reported to accelerate infected wound healing compared with corresponding control treatments, likely through combined antibacterial activity and gene-regulatory effects.42 This example illustrates the value of MSN-based systems for integrating antimicrobial therapy with RNA interference, but the magnitude of benefit should be reported together with the specific comparator group, model, and treatment duration.
Organic-inorganic hybrid carriers integrate the structural stability and multifunctionality of inorganic scaffolds with the biocompatibility and processability of organic components, providing a flexible strategy for nanocarrier design. Representative hybrid strategies include PLGA-cationic lipid hybrid nanoparticles, which combine polymeric structural support with lipid-mediated interaction with nucleic acids, and inorganic-organic composites such as polymer-capped MSNs or surface-modified AuNP-based vectors that improve siRNA loading, protection, and cellular delivery.43–45 Light-responsive inorganic-organic systems may further expand externally controlled siRNA release, but such claims should be linked to carrier-specific experimental evidence rather than generalized across all hybrid platforms. Overall, the core design principle of hybrid carriers is to combine complementary material functions, such as high loading capacity, structural stability, stimuli-responsive release, and improved biocompatibility. Future studies should define these advantages using standardized comparators and disease-relevant models before clinical translation can be realistically pursued.44–47
Critical Design Parameters and Their Impact on Delivery Efficiency
The physicochemical properties of nanocarriers fundamentally determine the efficiency of siRNA delivery, underscoring the need for precise tuning during the design phase.48 Among these parameters, particle size is particularly influential, dictating both the dominant route of transdermal penetration and the mechanism of cellular internalization. For transdermal delivery, an optimal size range of 10–200 nm has been identified. Nanocarriers smaller than 100 nm primarily traverse through follicular openings and the intercellular lipid matrix of the stratum corneum, whereas larger particles (> 100 nm) rely mainly on the follicular pathway.3 Particle size also strongly influences endocytosis uptake: carriers under 50 nm are mainly internalized via clathrin-mediated endocytosis, those between 50–200 nm preferentially enter through caveolae-mediated pathways, and particles larger than 200 nm are typically engulfed by macropinocytosis.9
Surface charge, another key design parameter, exerts multifactorial effects on siRNA complexation, cellular uptake, and biocompatibility. A moderately positive zeta charge (+10 to +30 mV) facilitates stable electrostatic association with anionic siRNA, whereas excessive cationic density increases the risk of nonspecific cytotoxicity and opsonization.17 Ionizable carriers provide an effective strategy to balance efficiency and safety: they remain nearly neutral at physiological pH but acquire a cationic charge within the acidic endosomal environment, thereby enabling stimulus-responsive activation and minimizing off-target interactions.11
Of paramount importance throughout the delivery cascade are the stability and degradation kinetics of the carrier. An ideal nanocarrier must maintain sufficient structural integrity during circulation to prevent premature siRNA release, yet be engineered to rapidly disassemble and liberate its payload in response to intracellular cues.10 Approaches such as adjusting cross-linking density, incorporating stabilizing excipients, and applying surface PEGylation have all been shown to enhance nanocarrier stability, thereby establishing a reliable foundation for clinical translation.49
A comprehensive analysis indicates that no single delivery platform is universally optimal for all therapeutic contexts. As summarized in Supplementary Table 1, each system presents a distinct balance of advantages and limitations. Consequently, the selection or rational design of an appropriate nanocarrier should be guided by the specific pathological microenvironment, therapeutic target, and intended route of administration.49 Future work should therefore focus on feedback-informed and disease-adapted nanocarriers that improve specificity, safety, and therapeutic efficacy while remaining experimentally reproducible and clinically manufacturable.
Among the available platforms, lipid-polymer hybrid nanoparticles (LPHNs) are particularly attractive because they combine complementary structural features within a modular architecture. The polymeric core can support siRNA encapsulation and controlled release, whereas the lipid shell may improve biocompatibility, membrane interaction, and formulation flexibility. This architecture also enables co-delivery of siRNA with small-molecule drugs, which may be useful for dermatological diseases driven by multiple inflammatory, proliferative, or malignant pathways. Nevertheless, the translational value of LPHNs should be evaluated against well-defined single-component comparators, disease-relevant models, and safety endpoints rather than assumed from the hybrid design alone.
Various nanocarriers, including liposomes, polymeric nanoparticles, gold nanoparticles, mesoporous silica, and organic-inorganic hybrid systems, provide a tunable physicochemical design space for transdermal siRNA delivery through their material composition and structural configurations. These platforms partially address key challenges such as nucleic acid instability, the dense skin barrier, and limited cellular uptake. However, material properties alone cannot fully explain, nor can they independently ensure, therapeutic efficacy. Practical performance depends more critically on whether these systems can sequentially overcome the hierarchical biological barriers from the skin surface to the cytoplasm and achieve adequate and sustained pharmacological exposure at essential stages, including skin penetration, intracellular trafficking, and cytosolic release. Therefore, after examining the major categories of nanocarriers and their structural attributes, a central question emerges: through which specific mechanisms do different material systems preserve siRNA stability, facilitate transport across the stratum corneum and epidermis, promote cellular internalization and endosomal escape, and achieve spatiotemporally controlled release (Figure 6)?
 |
Figure 6 Hierarchical barriers to effective transdermal delivery of siRNA-loaded nanocarriers. (A) Degradation of siRNA by extracellular nuclease on the skin surface; (B) Penetration of the stratum corneum via intercellular lipid pathways and transfollicular routes; (C) Cellular internalization of nanocarriers into viable epidermal/dermal cells via endocytosis; (D) Intracellular trafficking outcomes, including endosomal escape versus lysosomal degradation, culminating in cytosolic release of siRNA. |
Mechanisms of Transdermal Delivery: Deconstructing Multidimensional Barriers with Systematic Solutions
Preserving Molecular Integrity: Protection of siRNA from Degradation
Naked siRNA is readily degraded by nucleases before it reaches target cells, making molecular protection an early and essential step in transdermal delivery. If the duplex is degraded at the skin surface, within interstitial fluid, or during cellular uptake, later steps such as endosomal escape and RISC loading become ineffective. Current protective strategies generally fall into three categories: carrier-mediated binding or conjugation, chemical modification of the siRNA molecule, and surface shielding of the nanocarrier.
Carrier-mediated association is one direct way to reduce premature siRNA degradation. Electrostatic complexation is simple and widely used, but complexes formed only through charge interaction may dissociate in salt- or protein-rich environments. Covalent or reversibly crosslinked systems can provide stronger protection. For example, disulfide-containing linkers are designed to remain comparatively stable under extracellular oxidative conditions, but to be cleaved after exposure to the more reductive intracellular environment. In studies using disulfide-stabilized siRNA carriers, serum or nuclease stability was improved compared with the corresponding non-crosslinked or non-modified carrier systems, rather than compared with all delivery platforms in general. The reported degree of improvement therefore depends on the formulation, serum concentration, incubation time, and analytical method used in each study.50
Chemical modification of siRNA provides another layer of protection by reducing nuclease recognition and cleavage. Common modifications include 2′-O-methyl, 2′-fluoro, and phosphorothioate substitutions. These modifications have been reported to increase nuclease resistance compared with unmodified siRNA and may also reduce innate immune activation when appropriately incorporated into the sequence.51,52 Combined modification patterns, such as the use of 2′-fluoro, 2′-O-methyl, and phosphorothioate groups in selected positions, can further improve stability while preserving RNAi activity, although the final effect depends on the target sequence, modification site, and strand design.53
Surface modification of the carrier can also protect siRNA indirectly by stabilizing the nanoparticle and reducing nonspecific interactions with proteins. PEGylation is the most common example. A PEG layer can improve colloidal stability and reduce protein adsorption compared with non-PEGylated carriers.54 However, this benefit is not unlimited. Dense or high-molecular-weight PEG coatings may also reduce cellular interaction and slow endosomal uptake, which can weaken downstream gene silencing. For this reason, PEG molecular weight, grafting density, and linker chemistry need to be optimized rather than simply maximized.55 In the context of siRNA nanocarriers, changes in PEG molecular weight or grafting density should therefore be interpreted against clearly defined comparator formulations, such as non-PEGylated nanoparticles or nanoparticles with a different PEG chain length or surface density49,56 (Supplementary Table 2).
Overall, claims about improved siRNA stability should be linked to the exact baseline used in the original experiment, such as naked siRNA, unmodified siRNA, non-crosslinked carriers, non-PEGylated nanoparticles, or differently modified formulations. This clarification is important because “improved stability” does not describe a universal property of a carrier class, but a formulation-dependent result obtained under defined experimental conditions.
Enhancing Skin Penetration: Nanotechnological and Physical Strategies
Once siRNA stability is preserved, the next challenge is to move the nanocarrier across the stratum corneum and into viable skin layers. The stratum corneum consists of corneocytes embedded in a dense intercellular lipid matrix, commonly described as a “brick-and-mortar” structure, and it restricts the penetration of most hydrophilic macromolecules and nanoparticle systems.57–59 Current approaches to improve skin penetration can be broadly divided into passive nanocarrier optimization and physically assisted delivery.
Particle size is one of the most practical parameters for regulating skin penetration. In general, smaller nanocarriers are more likely to enter the intercellular lipid domain or appendageal routes, whereas larger particles tend to remain closer to the skin surface or accumulate around hair follicles. Reported size thresholds vary among skin models and formulations, but particles below approximately 100 nm are often associated with better penetration than larger particles.57 For example, in an ex vivo porcine skin model, 65-nm siRNA-loaded lipid nanoparticles reached a penetration depth of approximately 255 μm after 12 h, whereas 125-nm nanoparticles reached about 150 μm under the same experimental conditions. In the corresponding EGFR-silencing experiment, the smaller nanoparticles achieved 68% gene silencing compared with 42% in the larger-particle group.60
Surface charge also influences the balance between skin adhesion, penetration, and cellular uptake. A moderately positive surface charge may enhance interaction with the negatively charged skin surface, but excessive cationic density can increase nonspecific adhesion, cytotoxicity, and retention in superficial layers.48 Charge-conversion systems have therefore been explored to reduce this trade-off. In these formulations, the carrier may initially present a mildly positive surface to support skin contact and then shift toward a neutral or less adhesive state after entering the skin. In the cited study, this strategy increased penetration depth by 1.8-fold and improved gene-silencing efficiency by 56% compared with fixed-charge control formulations.48
Vesicular flexibility is another important factor in topical and transdermal delivery. The standard terms commonly used in this context are ultradeformable vesicles and transfersomes. Transfersomes are generally regarded as ultradeformable lipid vesicles containing edge activators, such as surfactants, that increase bilayer elasticity. Compared with conventional liposomes, these vesicles can deform more readily and pass through narrow intercellular spaces under hydration or osmotic gradients.28,61–63 Ethosomes represent a related but distinct vesicular system. Their high ethanol content, commonly around 20–45%, can fluidize stratum corneum lipids and increase vesicle flexibility, thereby improving skin deposition relative to conventional liposomes in reported cutaneous delivery models.29 Where quantitative improvements are reported, such as several-fold increases in penetration depth or flux, these values should be interpreted according to the specific comparator used, usually conventional liposomes or non-deformable vesicular formulations.28,29,61–63
Physical enhancement methods can further improve siRNA delivery by creating temporary pathways through the stratum corneum or by increasing lipid disorder within the barrier layer.64,65 Microneedles form micron-scale channels that allow nanocarriers or nucleic acid formulations to reach the viable epidermis or superficial dermis more directly66 (Figure 7). Fractional laser treatment works through controlled microablation. In one reported study, Er: YAG laser pretreatment increased the penetration depth of siRNA nanoparticles from 85 μm to 217 μm and improved gene-silencing efficiency by nearly threefold compared with the non-laser control group.60 Sonophoresis can also enhance permeation by cavitation-mediated disruption of lipid organization; in the cited model, low-frequency sonophoresis increased nanoparticle permeation flux by up to 4.2-fold relative to untreated skin controls.67 These physical methods are best viewed as complementary tools rather than universal solutions, because their effectiveness depends on device parameters, skin condition, carrier properties, and treatment duration (Supplementary Table 3).
 |
Figure 7 Schematic illustration of microneedle-assisted transdermal delivery (not to scale). (A) Apply: a drug-loaded microneedle (MN) patch is gently pressed onto the skin, in contrast to conventional topical application, which is blocked by the ~10-20 µm stratum corneum (SC). (B) Penetrate: MNs ≈ 500 µm in length painlessly traverse the SC, creating transient microchannels that typically close within ≈ 30 min while avoiding underlying nerves and blood vessels. (C) Deliver: coated solid MNs provide a rapid burst release of siRNA nanocarriers, whereas dissolving MNs gradually disintegrate to provide sustained release, together enabling efficient epidermal deposition for subsequent cellular uptake. |
Overcoming Intracellular Barriers: Cellular Uptake and Endosomal Escape
After crossing the stratum corneum and reaching viable epidermal or dermal cells, siRNA-loaded nanocarriers must still be internalized and release their cargo into the cytosol. This step is important because siRNA must access the cytoplasmic RNA-induced silencing complex to mediate mRNA cleavage. If the payload remains trapped in endosomes or is transferred to lysosomes, gene-silencing activity can be substantially reduced.21 Therefore, intracellular delivery design generally focuses on two related processes: promoting cellular uptake and improving endosomal escape.
Nanoparticles may enter cells through several endocytic routes, including clathrin-mediated endocytosis, caveolae-mediated endocytosis, macropinocytosis, and clathrin-/caveolae-independent pathways.9 These pathways can lead to different intracellular trafficking outcomes, but they should not be interpreted as fixed or mutually exclusive routes. In many studies, more than one uptake mechanism contributes to internalization, and the dominant pathway may vary with cell type, particle size, surface charge, ligand modification, and incubation conditions. Therefore, size and surface chemistry should be viewed as factors that bias uptake behavior rather than as absolute determinants of a single endocytic route.9
Surfactant protein B-functionalized liposomes provide one example of how surface modification can alter intracellular trafficking. In the cited study, these liposomes showed evidence of caveolae-associated uptake and reduced lysosomal colocalization compared with the matched control formulation. The same study reported an approximately 60% increase in gene-silencing efficacy relative to that control group.68 This finding suggests that directing carriers away from degradative trafficking routes may improve cytosolic siRNA availability, although the effect is likely formulation- and cell-model-dependent.
One commonly used strategy for endosomal escape is the proton sponge effect, which is associated with polymers containing protonatable amine groups, such as PEI and poly(amidoamine) dendrimers.21 These polymers can buffer endosomal acidification, leading to proton accumulation, chloride influx, osmotic swelling, and partial destabilization of the endosomal membrane. In reported siRNA delivery studies, PEI-containing formulations showed higher endosomal escape or transfection efficiency than the corresponding non-PEI or less-buffering control formulations, with some studies reporting approximately 3- to 5-fold improvement.21,69 However, this benefit must be balanced against the well-known cytotoxicity of high-molecular-weight or highly cationic PEI.
To reduce PEI-associated toxicity, alternative biodegradable buffering materials have been explored. Histidine-rich peptides and poly(β-amino ester)s (PBAEs) are representative examples. PBAEs are better described as materials that facilitate endosomal escape through pH-dependent protonation, buffering capacity, and membrane interaction, while their ester bonds allow hydrolytic degradation that can reduce long-term polymer accumulation. Thus, their main contribution in siRNA delivery should be discussed in terms of improving endosomal escape and cytosolic release, rather than as a general claim of improved clinical viability.70
Other strategies aim to destabilize the endosomal membrane more directly. Fusogenic lipids or peptides can promote interaction between the carrier membrane and the endosomal membrane, whereas lytic or membrane-active peptides may transiently disrupt the endosomal bilayer. Many of these components are designed to become more active under acidic endosomal pH, which helps restrict membrane-disruptive activity to the intracellular compartment.33 For example, pH-sensitive fusogenic peptide-modified siRNA nanocarriers have been reported to enhance endosomal escape and gene silencing compared with the corresponding non-fusogenic or less-responsive control formulations.71 Together, these approaches show that intracellular delivery depends not only on how efficiently carriers enter cells, but also on whether they can avoid lysosomal degradation and release siRNA into the cytosol.
Stimuli-Responsive Nanocarriers for Controlled siRNA Release
Stimuli-responsive nanocarriers are designed to adjust their structure, surface properties, or release behavior in response to disease-associated signals or externally applied triggers. In transdermal siRNA delivery, this design is useful because the carrier must remain sufficiently stable during skin penetration but release siRNA after reaching the lesion microenvironment or intracellular compartment. Common triggers include acidic pH, overexpressed enzymes, redox gradients, light, temperature, and intracellular metabolites72 (Figure 8).
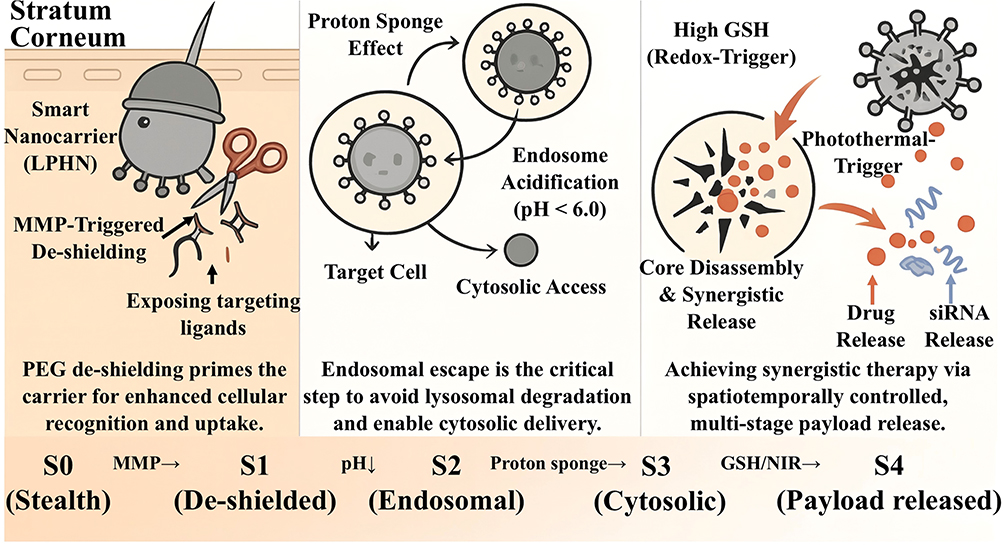 |
Figure 8 Cascade-of-activation pathway for a stimuli-responsive LPHN. Note: S0→S1: Barrier Penetration & Extracellular Priming. S1→S3: Cellular Internalization & Endosomal Escape. S3→S4: Synergistic Firepower & Strike. |
pH-responsive systems exploit pH differences between normal skin, inflamed or tumor tissues, and endo-lysosomal compartments. In general, these carriers are designed to remain relatively stable under physiological or near-neutral pH, but to undergo protonation, bond cleavage, charge conversion, swelling, or structural loosening under mildly acidic conditions.73,74 This behavior can support two delivery requirements: preserving carrier integrity before reaching the target site and promoting siRNA release after exposure to a pathological or intracellular acidic environment.5,74
Enzyme-responsive systems use disease-associated enzymatic activity as a trigger for carrier activation or payload release. Matrix metalloproteinases (MMPs), including MMP-2 and MMP-9, are frequently discussed in inflammatory lesions, tumors, and wound-remodeling environments because their expression or activity can be altered during extracellular matrix remodeling.75,76 In this context, enzyme-responsive designs may incorporate enzyme-cleavable linkers or coatings to expose targeting ligands, remove shielding layers, or accelerate siRNA release in enzyme-rich microenvironments. It is therefore important to distinguish general MMP-associated pathological activity from evidence derived from specifically designed MMP-cleavable nanocarrier systems.
Light- and thermo-responsive systems provide externally controlled approaches for modulating siRNA delivery. Near-infrared (NIR) irradiation, laser treatment, or photochemical activation can be used to increase local permeability, promote endosomal escape, or trigger carrier destabilization in selected models.77,78 For example, photochemical internalization has been investigated as a way to enhance intracellular siRNA release in topical psoriasis-related delivery systems.78 Because light penetration, local heating, and intracellular release are highly dependent on wavelength, irradiation dose, photosensitizer, and tissue depth, these systems should be interpreted according to the exact experimental setting.
Multi-responsive systems combine two or more triggers, such as acidic pH, enzymatic activity, redox gradients, intracellular glutathione (GSH), adenosine triphosphate (ATP), or externally applied light. These systems are intended to achieve stepwise activation, for example, surface de-shielding in the extracellular lesion microenvironment followed by intracellular release after endosomal acidification or exposure to high cytosolic GSH. Reported examples include ATP-responsive lipid nanoparticles for melanoma-related siRNA delivery and cascade-responsive nanocomplexes for psoriasis-related RNA interference.79,80 Because the mechanisms and disease models differ substantially across studies, multi-responsive systems should be described as a developing strategy rather than as a uniformly validated clinical solution (Supplementary Table 4).
Taken together, Preserving Molecular Integrity: Protection of siRNA From Degradation–Stimuli-Responsive Nanocarriers for Controlled siRNA Release outline the major barriers and design strategies involved in transdermal siRNA delivery, including siRNA protection, stratum corneum penetration, cellular uptake, endosomal escape, and controlled release. These principles are broadly useful, but their practical relevance depends on the disease microenvironment. Psoriatic plaques, skin tumors, and chronic wounds differ in barrier structure, pH, enzyme activity, oxidative stress, vascular remodeling, and microbial burden. Therefore, the next section maps these general delivery principles onto representative cutaneous disease settings and discusses how carrier design can be adapted to psoriasis, skin tumors, and chronic wounds.
Tailoring Carrier Design to Cutaneous Pathological Microenvironments
The performance of siRNA nanocarriers is strongly influenced by the pathological microenvironment in which they are applied. For transdermal therapy, carrier design should therefore be considered not only in terms of material properties, but also in relation to lesion-specific barriers, inflammatory signals, enzyme activity, vascular changes, and release requirements. A formulation that performs well under idealized in vitro conditions may behave differently in thickened epidermis, tumor stroma, or protease-rich wound fluid. Thus, disease-adapted design requires matching carrier structure, responsiveness, and release kinetics to the biological context of each lesion.
To illustrate this disease-adapted design concept, this section focuses on three representative cutaneous settings: psoriasis, which is characterized by epidermal thickening and immune activation; skin tumors, which often show acidic, hypoxic, and matrix-remodeled tumor microenvironments; and chronic wounds, which are associated with persistent inflammation, protease-rich exudate, microbial burden, and impaired tissue repair (Supplementary Figure 1).
Delivery Strategies within the Psoriatic Microenvironment
Psoriasis is an immune-mediated inflammatory skin disease in which epidermal thickening, keratinocyte hyperproliferation, vascular remodeling, and immune-cell infiltration occur together.81,82 These features create both physical barriers and biological cues for transdermal siRNA delivery. On the one hand, the thickened and hyperkeratotic epidermis can reduce passive diffusion of nucleic acid formulations. On the other hand, the inflammatory microenvironment, including elevated cytokines such as interleukin-17 (IL-17), interleukin-23 (IL-23), and tumor necrosis factor-α (TNF-α), provides disease-relevant molecular targets for local gene silencing.82,83
For psoriatic lesions, the first design requirement is improved penetration through the remodeled epidermal barrier. Flexible vesicular systems, such as transfersomes or other ultradeformable lipid vesicles, may be useful because their membrane elasticity allows them to move through narrow intercellular spaces more readily than conventional rigid vesicles.29,62 Particle size and surface properties should also be selected according to the lesion context. Increased vascular permeability in inflamed psoriatic lesions may support lesion-associated accumulation of appropriately sized nanocarriers in some experimental settings. For example, carriers within the 70–150 nm range have been discussed in relation to enhanced deposition in inflamed skin, although this process should be interpreted as inflammation-associated vascular permeability rather than as a tumor-like enhanced permeability and retention (EPR) effect.84
The biochemical features of psoriatic plaques can also be used to guide responsive release. Oxidative stress, altered local pH, inflammatory cytokine activity, and upregulated enzymes such as matrix metalloproteinase-9 (MMP-9) have been reported in psoriasis-related lesions.85,86 In psoriasis-related or psoriasis-mimicking models, stimuli-responsive carriers have been reported to increase siRNA release under lesion-associated conditions compared with healthy-skin or non-stimulated control conditions. When quantitative differences are reported, such as an approximately 2.3-fold increase in release, the value should be interpreted according to the specific stimulus, model system, and comparator used in the original study.87
Active targeting provides another way to improve cell-specific delivery within the psoriatic inflammatory network. Macrophages, dendritic cells, T cells, and keratinocytes all contribute to disease progression, but they may require different targeting strategies. For example, hyaluronic acid has been used to enhance interaction with CD44-expressing inflammatory cells, while arginine-glycine-aspartic acid (RGD) peptides may facilitate interaction with integrin-expressing cells.31 In relevant experimental models, ligand-functionalized carriers have been reported to increase intracellular siRNA accumulation in target cells compared with non-targeted or unmodified counterparts, with some studies reporting approximately 3- to 5-fold enhancement.88 These findings suggest that ligand modification can improve local and cellular delivery, although the effect depends on receptor expression, lesion stage, and carrier formulation.
The siRNA payload should also be selected according to the inflammatory pathway being targeted. Candidate targets include TNF-α, signal transducer and activator of transcription 3 (STAT3), and components of the IL-23/IL-17 axis, as well as the Fn14-TWEAK pathway.86,88,89 In principle, combining siRNAs against multiple inflammatory mediators may produce broader immunomodulatory effects than single-target silencing. However, such multi-target approaches should be evaluated carefully for dose requirements, off-target effects, and potential innate immune activation. Overall, psoriasis-adapted siRNA delivery requires coordinated optimization of epidermal penetration, inflammatory-cell targeting, responsive release, and payload selection.
Adaptive Strategies for the Skin Tumor Microenvironment
Cutaneous malignancies, such as melanoma and cutaneous squamous cell carcinoma, often develop microenvironmental features that influence nanocarrier delivery, including abnormal vasculature, regional hypoxia, extracellular matrix remodeling, immune suppression, and heterogeneous interstitial pressure.11,90 These factors may affect tumor accumulation, intratumoral distribution, cellular uptake, and intracellular release of siRNA-loaded nanocarriers. Therefore, tumor-adapted carrier design should treat the tumor microenvironment (TME) not only as a therapeutic target, but also as a delivery barrier.
The TME is often mildly acidic compared with surrounding normal tissues, and the endo-lysosomal compartment is even more acidic after cellular uptake. This pH gradient provides a rationale for pH-responsive siRNA carriers, although the degree of acidity and release selectivity varies among tumor models and formulations.11 In general, pH-sensitive carriers are designed to remain relatively stable at physiological pH, but to undergo protonation, charge conversion, bond cleavage, or structural destabilization in acidic tumor or endosomal environments. Such changes may improve local release and endosomal escape, but their effectiveness should be assessed in relation to the specific tumor model and control formulation used.
Many studies have also explored combined passive and active targeting strategies. Passive tumor accumulation may be influenced by abnormal vasculature and impaired lymphatic drainage, whereas active targeting relies on ligand-receptor interactions on tumor cells or tumor-associated stromal cells.91,92 This combined approach is intended to improve multiple delivery steps, including tumor deposition, cellular recognition, internalization, and intracellular release. However, active targeting should not be interpreted as absolute tumor specificity, because receptor expression can also occur in normal tissues and may vary across tumor stages.
In a melanoma-related experimental model, ligand-modified lipid-polymer hybrid nanoparticles showed higher cellular uptake and antitumor activity than non-targeted nanoparticles. These data support the potential value of ligand modification, but they should be interpreted within the corresponding experimental context, including the tumor model, ligand density, dosing schedule, and comparator formulation.48
The stromal structure of skin tumors is another important consideration. Dense extracellular matrix (ECM), elevated interstitial fluid pressure, and abnormal vascular architecture can restrict nanoparticle penetration and produce uneven intratumoral distribution.93,94 Effective tumor-adapted siRNA nanocarrier design should therefore consider both payload potency and stromal penetration, as limited intratumoral distribution may reduce therapeutic exposure even when the siRNA target is biologically relevant.
Combination therapy is also frequently explored in tumor-adapted delivery systems. siRNA-mediated gene silencing can be integrated with chemotherapy, photothermal therapy, photodynamic therapy, or immunotherapy to address multiple aspects of tumor progression. For example, NIR-responsive photothermal systems may promote local hyperthermia and triggered siRNA release, while immune-modulating formulations may reduce checkpoint-related immunosuppression in preclinical models.95,96 These combination approaches are promising, but their interpretation should distinguish between improved delivery, direct cytotoxicity, immune modulation, and true synergistic therapeutic effects. Overall, skin tumor-adapted siRNA delivery requires integration of tumor accumulation, stromal penetration, intracellular release, and rational therapeutic combination.
Optimizing Delivery Systems for the Chronic Wound Microenvironment
Chronic wounds present a distinct delivery environment compared with inflammatory plaques or tumors. Their microenvironment is characterized by persistent inflammation, excessive wound exudate, elevated protease and nuclease activity, microbial biofilm formation, impaired angiogenesis, hypoxia, and altered pH.97,98 These factors can destabilize siRNA, interfere with carrier retention, and delay tissue repair. Therefore, chronic wound-adapted siRNA delivery systems must be designed not only to protect nucleic acids, but also to function in a protease-rich, fluid-rich, and microbiologically complex lesion environment.
Because wound exudate contains proteases, nucleases, inflammatory mediators, salts, and reactive species, maintaining carrier stability is a primary requirement. Structural crosslinking, multilamellar encapsulation, and protective polymer or lipid coatings have been explored to reduce premature degradation and improve retention in wound-related models. In reported wound-related delivery settings, reinforced or coated nanocarriers have shown improved stability compared with corresponding non-reinforced formulations. Where values such as a 3.6-fold increase are reported, they should be interpreted according to the simulated wound fluid, incubation period, and analytical method used.99
Responsive release is also important because chronic wound healing proceeds through overlapping inflammatory, proliferative, and remodeling phases. A carrier that releases siRNA too rapidly may fail to maintain therapeutic levels, whereas excessive retention may delay adaptation to later repair stages. Representative responsive systems have been designed to react to wound-associated signals such as pH changes, protease activity, reactive oxygen species, or bacterial biofilm-related cues.40,100 These systems may allow siRNA release to be better matched with local pathological activity, although the effectiveness of each trigger depends on the wound model and disease stage.
Chronic wounds usually require multi-target intervention. Reducing inflammation alone may not be sufficient if bacterial burden, impaired angiogenesis, and extracellular matrix dysfunction persist. For this reason, multifunctional nanocarriers capable of co-delivering anti-inflammatory siRNA, antibacterial agents, and pro-regenerative molecules have attracted attention.101 Such systems may help reduce microbial load, suppress excessive inflammatory signaling, and support angiogenesis or matrix remodeling. However, the contribution of each component should be evaluated with appropriate controls, such as siRNA-only, antibacterial-only, carrier-only, and combined-treatment groups.
Stage-matched release is particularly relevant for chronic wounds. A practical design may involve early release of anti-inflammatory or antibacterial components, followed by sustained delivery of pro-angiogenic or matrix-remodeling signals during the proliferative and remodeling phases. Matching release profiles with biological stages may reduce dosing frequency and improve local therapeutic continuity, but this concept still requires validation in wound models that adequately reproduce chronic inflammation, biofilm burden, vascular impairment, and delayed re-epithelialization.
Sections 6.1–6.3 show that transdermal siRNA delivery cannot rely on a single universal carrier design. Psoriasis, skin tumors, and chronic wounds differ in barrier structure, inflammatory status, enzymatic activity, vascular remodeling, microbial burden, and release requirements. Disease-adapted delivery should therefore match carrier composition, particle properties, targeting ligands, responsiveness, and release kinetics to the specific pathological context. Nevertheless, these strategies remain largely preclinical and require further validation in models that better reproduce human skin pathology, long-term safety, and clinically relevant dosing conditions.
Discussion
Nanocarrier-mediated transdermal siRNA delivery has demonstrated considerable potential in preclinical research. However, translating these complex nanosystems into standardized clinical therapies requires solving problems that extend beyond biological efficacy. Key challenges include scalable manufacturing, quality control, long-term safety evaluation, and the predictive validity of preclinical models.
Challenges in Production Scalability and Standardization
A major obstacle to clinical translation is the gap between small-scale laboratory preparation and reproducible large-scale manufacturing. Nanocarrier self-assembly is sensitive to raw-material attributes, solvent composition, mixing rate, temperature, and purification conditions. Small process variations can alter critical quality attributes (CQAs), including particle size distribution, polydispersity index, surface charge, encapsulation efficiency, drug loading, residual solvent content, and release behavior.102,103
Quality-by-design (QbD) and process analytical technology (PAT) approaches are therefore increasingly important for nanomedicine development. For lipid- and polymer-based nanosystems, defined relationships among critical material attributes, critical process parameters, and final product performance are needed to support batch-to-batch reproducibility and regulatory comparability.102 Continuous or microfluidic manufacturing platforms may improve process control for some liposomal and lipid nanoparticle systems, but their suitability must still be validated for each formulation and payload.103 Establishing Good Manufacturing Practice (GMP)-compatible production and release-testing workflows is thus a prerequisite for clinical translation.
Long-Term Biocompatibility, Immunogenicity, and Immune Recognition
Long-term biocompatibility and immunological safety remain central issues for the clinical translation of transdermal siRNA nanocarriers. Although many preclinical studies evaluate short-term cytotoxicity, skin irritation, or acute inflammatory responses, fewer studies systematically examine repeated administration, chronic exposure, delayed immune activation, and long-term tissue retention. This concern is particularly relevant for slowly degradable or non-degradable inorganic and organic-inorganic hybrid carriers, whose long-term behavior may involve local tissue retention, persistent inflammation, foreign-body responses, or fibrotic remodeling.
Once exposed to biological fluids, interstitial fluid, inflammatory exudate, or wound fluid, nanocarriers may adsorb proteins, lipids, and other biomolecules, forming a dynamic biomolecular or protein corona. This corona can change the apparent biological identity of the carrier and influence colloidal stability, cellular recognition, tissue distribution, immune clearance, and even ligand-mediated targeting.104 Both the carrier and the siRNA cargo can also contribute to immune activation through complement activation, cytokine release, macrophage uptake, or recognition by innate RNA-sensing pathways.
Repeated administration introduces additional concerns. PEGylated carriers may induce or interact with anti-polyethylene glycol (anti-PEG) antibodies in some settings, and repeated exposure to PEGylated nanocarriers has been linked to accelerated blood clearance (ABC) or altered biodistribution.105,106 At the same time, immune recognition is not an unavoidable limitation of siRNA therapy. Rational sequence design, avoidance of immunostimulatory motifs, and chemical modifications such as 2′-O-methyl, 2′-fluoro, and phosphorothioate substitutions can improve nuclease resistance and reduce activation of Toll-like receptors and other RNA-sensing pathways when appropriately incorporated into the duplex. Carrier-level strategies, including ionizable materials, charge-conversion systems, optimized PEGylation, degradable lipids, biodegradable polymers, and biomimetic coatings, may further reduce nonspecific protein adsorption and inflammatory recognition.
These advances reduce, but do not eliminate, the need for systematic safety evaluation. Future studies should combine repeated-dose toxicity testing, chronic immunotoxicity assessment, protein-corona profiling, complement activation assays, cytokine profiling, and local skin histopathology. Such evaluation is particularly important for chronic dermatological diseases, where repeated or long-term topical administration may be required.
Limitations in the Predictive Validity of Preclinical Models
The translation of transdermal nanomedicine findings remains limited by the predictive validity of available models. Rodent skin differs from human skin in stratum corneum organization, thickness, hair follicle density, immune composition, and repair dynamics, which can affect the apparent penetration, retention, and therapeutic performance of nanocarriers. Ex vivo skin, reconstructed human skin, and animal models each provide useful information, but none fully reproduces the dynamic microenvironment of chronic human skin disease.
Human-relevant models are therefore needed to bridge the gap between conventional assays and clinical conditions. Three-dimensional reconstructed human skin equivalents can provide a more relevant epidermal barrier than monolayer culture, while microfluidic skin-on-a-chip systems can incorporate perfusion, tissue-tissue interfaces, and real-time monitoring of barrier function or toxicity.107 These models are not replacements for all in vivo testing, but they can improve early-stage screening and help identify formulations that warrant more intensive preclinical evaluation.
Future Research Directions
Future development should emphasize high-fidelity evaluation systems and clearer structure-function relationships. Reconstructed human skin equivalents, diseased skin models, and skin-on-a-chip platforms can be used to assess nanocarrier penetration, cellular uptake, inflammatory responses, and toxicity under more physiologically relevant conditions.107 Integrating these models with quantitative imaging, transcriptomic or proteomic readouts, and computational simulations may improve prediction of dose-exposure-response relationships.
A second priority is to deepen mechanistic understanding of nano-bio interactions in skin environments. Protein-corona formation, ligand shielding, endocytic route selection, endosomal escape, and local immune recognition should be studied as dynamic processes rather than as fixed material properties.104 These questions are especially important for ligand-targeted and stimuli-responsive systems, where biological fluids or lesion exudates may alter surface identity before the carrier reaches target cells.
Finally, next-generation systems may integrate multiple stimuli-responsive modules, including pH-, enzyme-, redox-, light-, or metabolite-responsive components.108 Logic-gated or feedback-regulated nanocarriers remain an attractive long-term direction, but they should be developed with equal attention to manufacturability, safety, and disease-relevant validation. For transdermal siRNA therapy, clinical progress will likely depend less on adding more functions to a carrier and more on matching the necessary functions to a well-defined pathological context.
Conclusion
This review summarizes current advances in stimuli-responsive nanocarrier-mediated transdermal siRNA delivery for skin diseases from the perspectives of molecular mechanism, carrier design, barrier negotiation, and disease-oriented application. Although siRNA offers highly specific therapeutic potential, its successful transdermal use remains constrained by sequential extracellular and intracellular barriers, including nuclease degradation, poor skin permeation, limited cellular uptake, and inefficient endosomal escape.
Collectively, current evidence suggests that clinically meaningful transdermal siRNA therapy will most likely emerge not from a universal carrier, but from rationally engineered systems tailored to specific pathological microenvironments. In this context, lipid-polymer hybrid nanoparticles appear particularly promising because they combine structural stability, biocompatibility, and co-delivery capacity within a modular platform. At the same time, stimuli-responsive designs and physical enhancement technologies further expand the feasibility of precise and localized siRNA delivery.
Future progress in this field will depend on integrating disease-specific design, reliable manufacturing, long-term safety evaluation, and more predictive preclinical models. With continued advances in intelligent materials and translational nanomedicine, transdermal siRNA delivery has strong potential to evolve from a promising experimental strategy into a clinically relevant therapeutic modality.
Abbreviations
AGO2, Argonaute 2; AMF, Alternating magnetic field; ATP, Adenosine triphosphate; AuNP, Gold nanoparticle; AuNPs, Gold nanoparticles; BRAF, B-Raf proto-oncogene, serine/threonine kinase; CME, Clathrin-mediated endocytosis; COVID-19, Coronavirus disease 2019; CTLA-4, Cytotoxic T-lymphocyte-associated protein 4; DMA, N, N-dimethylacetamide; DNA, Deoxyribonucleic acid; DODAX, Dioleoyldimethylammonium halide (X = Br, Cl); DOPE, 1,2-dioleoyl-sn-glycero-3-phosphoethanolamine; DOTAP, 1,2-dioleoyl-3-trimethylammonium-propane; DLS, Dynamic light scattering; ECM, Extracellular matrix; EGF, Epidermal growth factor; EGFR, Epidermal growth factor receptor; EJNMMI, European Journal of Nuclear Medicine and Molecular Imaging; EPR, Enhanced permeability and retention (effect); ESBL, Extended-spectrum β-lactamase; FTIR, Fourier-transform infrared spectroscopy; GSH, Glutathione; HEPES, 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid.
H2O2, Hydrogen peroxide; HPLC, High-performance liquid chromatography; IL-6, Interleukin-6; LPHN, Lipid-polymer hybrid nanoparticle; MAIT, Mucosal-associated invariant T; miRNA, microRNA; miRNAs, microRNAs; MN, Microneedle; MMP, Matrix metalloproteinase; MMPs, Matrix metalloproteinases; MMP-2, Matrix metalloproteinase-2 (gelatinase A); MMP-9, Matrix metalloproteinase-9 (gelatinase B); MSN, Mesoporous silica nanoparticle; MSNs, Mesoporous silica nanoparticles; mRNA, messenger RNA; NIR, Near-infrared; NMR, Nuclear magnetic resonance; PAGE, Polyacrylamide gel electrophoresis; PAMAM, Poly(amidoamine); PBAE, Poly(beta-amino ester); PBAEs, Poly(beta-amino ester)s; PBS, Phosphate-buffered saline; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; PDI, Polydispersity index; PEG, Polyethylene glycol; PEI, Polyethylenimine; PLGA, Poly(lactic-co-glycolic acid); RGD, Arginine-glycine-aspartic acid; RISC, RNA-induced silencing complex; RNAi, RNA interference; RNase, Ribonuclease; SC, Stratum corneum; SECosome, Cationic liposomal complex for siRNA delivery; SDS, Sodium dodecyl sulfate; SEM, Scanning electron microscopy; siRNA, small interfering RNA; SPR, Surface plasmon resonance; TEM, Transmission electron microscopy; TGI, Tumor growth inhibition; TLR, Toll-like receptor; TLRs, Toll-like receptors; TME, Tumor microenvironment; TNF, Tumor necrosis factor; VEGF, Vascular endothelial growth factor; YAG, Yttrium aluminum garnet.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study does not require ethical approval or patient consent.
Author Contributions
Conceptualization: Yanmin Jian, Minghui Ban, Zhenyang Yan, Zao Wang, and Yue Yuan; Methodology: Yanmin Jian, Minghui Ban, Zhenyang Yan, Zao Wang, and Yue Yuan; Formal analysis and investigation: Yansui Wang, Ziyan Che, Wenwen Ren, and Yuan Cao; Writing-original draft preparation: Yanmin Jian, Minghui Ban, Zhenyang Yan, Zao Wang, and Yue Yuan; Writing-review and editing: Yanmin Jian, Minghui Ban, Zhenyang Yan, Zao Wang, and Yue Yuan; Resources: Zao Wang and Yue Yuan; Supervision: Yanmin Jian, Minghui Ban, Zhenyang Yan, Zao Wang, and Yue Yuan. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. The funding body had no role in the design of the study, collection, analysis, interpretation of data, or writing of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects of topical glucocorticosteroids. J Am Acad Dermatol. 2006;54:
2. Lebwohl M. Advances in biologic therapy of psoriasis. J Eur Acad Dermatol Venereol. 2023;37:1689–26. doi:10.1111/jdv.19287
3. Sufianov A, Beilerli A, Kudriashov V, Ilyasova T, Wenjie B, Beylerli O. Advances in transdermal siRNAs delivery: a review of current research progress. Noncoding RNA Res. 2023;8:392–400. doi:10.1016/j.ncrna.2023.05.008
4. Zhang L, Dong Z, Liu W, et al. Novel pharmaceutical strategies for enhancing skin penetration of biomacromolecules. Pharmaceuticals. 2022;15:877. doi:10.3390/ph15070877
5. Berillo D, Zharkinbekov Z, Kim Y, Raziyeva K, Temirkhanova K, Saparov A. Stimuli-responsive polymers for transdermal, transmucosal and ocular drug delivery. Pharmaceutics. 2021;13:2050. doi:10.3390/pharmaceutics13122050
6. Thakur S, Sinhari A, Jain P, Jadhav HR. A perspective on oligonucleotide therapy: approaches to patient customization. Front Pharmacol. 2022;13:1006304. doi:10.3389/fphar.2022.1006304
7. Zhang C, Zhang B. RNA therapeutics: updates and future potential. Sci China Life Sci. 2023;66:12–30. doi:10.1007/s11427-022-2171-2
8. Silvestrini AVP, Morais MF, Debiasi BW, Praça FG, Bentley MVLB. Nanotechnology strategies to address challenges in topical and cellular delivery of siRNAs in skin disease therapy. Adv Drug Deliv Rev. 2024;207:115198. doi:10.1016/j.addr.2024.115198
9. Zhang J, Chen B, Gan C, Sun H, Zhang J, Feng L. A comprehensive review of small interfering RNAs (siRNAs): mechanism, therapeutic targets, and delivery strategies for cancer therapy. Int J Nanomed. 2023;18:7605–7635. doi:10.2147/IJN.S436038
10. Kim B, Park J-H, Sailor MJ. Rekindling RNAi therapy: materials design requirements for in vivo siRNA delivery. Adv Mater. 2019;31:e1903637. doi:10.1002/adma.201903637
11. Wang Y, Deng T, Liu X, et al. Smart nanoplatforms responding to the tumor microenvironment for precise drug delivery in cancer therapy. Int J Nanomed. 2024;19:6253–6277. doi:10.2147/IJN.S459710
12. Fire A, Xu S, Montgomery MK, Kostas SA, Driver SE, Mello CC. Potent and specific genetic interference by double-stranded RNA in caenorhabditis elegans. Nature. 1998;391:806–811. doi:10.1038/35888
13. Elbashir SM, Harborth J, Lendeckel W, Yalcin A, Weber K, Tuschl T. Duplexes of 21-nucleotide RNAs mediate RNA interference in cultured mammalian cells. Nature. 2001;411:494–498. doi:10.1038/35078107
14. Ito S, Nagata K. Roles of the endoplasmic reticulum-resident, collagen-specific molecular chaperone Hsp47 in vertebrate cells and human disease. J Biol Chem. 2019;294:2133–2141. doi:10.1074/jbc.TM118.002812
15. du Halgouet A, Darbois A, Alkobtawi M, et al. Role of MR1-driven signals and amphiregulin on the recruitment and repair function of MAIT cells during skin wound healing. Immunity. 2023;56:78–92.e6. doi:10.1016/j.immuni.2022.12.004
16. Blagbrough IS, Metwally AA, Blagbrough IS, Metwally AA. siRNA and gene formulation for efficient gene therapy. In: Gene Therapy - Tools and Potential Applications. IntechOpen; 2013. doi10.5772/55518
17. Zhang Y, Almazi JG, Ong HX, et al. Nanoparticle delivery platforms for RNAi therapeutics targeting COVID-19 disease in the respiratory tract. Int J Mol Sci. 2022;23:2408. doi:10.3390/ijms23052408
18. Yeung ML, Jeang K-T. MicroRNAs and cancer therapeutics. Pharm Res. 2011;28:3043–3049. doi:10.1007/s11095-011-0526-2
19. Ahn I, Kang CS, Han J. Where should siRNAs go: applicable organs for siRNA drugs. Exp Mol Med. 2023;55:1283–1292. doi:10.1038/s12276-023-00998-y
20. Xia Y, Tian J, Chen X. Effect of surface properties on liposomal siRNA delivery. Biomaterials. 2016;79:56–68. doi:10.1016/j.biomaterials.2015.11.056
21. Xia T, Kovochich M, Liong M, et al. Polyethyleneimine coating enhances the cellular uptake of mesoporous silica nanoparticles and allows safe delivery of siRNA and DNA constructs. ACS Nano. 2009;3:3273–3286. doi:10.1021/nn900918w
22. Kang MS, Kwon M, Jang HJ, Jeong SJ, Han D-W, Kim KS. Biosafety of inorganic nanomaterials for theranostic applications. Emergent Mater. 2022;5:1995–2029. doi:10.1007/s42247-022-00426-3
23. Petrovic SM, Barbinta-Patrascu M-E. Organic and biogenic nanocarriers as bio-friendly systems for bioactive compounds’ delivery: state-of-the art and challenges. Materials. 2023;16:7550. doi:10.3390/ma16247550
24. Hattab D, Gazzali AM, Bakhtiar A. Clinical advances of siRNA-based nanotherapeutics for cancer treatment. Pharmaceutics. 2021;13:1009. doi:10.3390/pharmaceutics13071009
25. Teixeira MC, Carbone C, Souto EB. Beyond liposomes: recent advances on lipid based nanostructures for poorly soluble/poorly permeable drug delivery. Prog Lipid Res. 2017;68:1–11. doi:10.1016/j.plipres.2017.07.001
26. Gomes-da-silva LC, Fonseca NA, Moura V, de Lima MCP, Simões S, Moreira JN. Lipid-based nanoparticles for siRNA delivery in cancer therapy: paradigms and challenges. Acc Chem Res. 2012;45:1163–1171. doi:10.1021/ar300048p
27. Clarke D, Idris A, McMillan NAJ. Development of novel lipidic particles for siRNA delivery that are highly effective after 12 months storage. PLoS One. 2019;14:e0211954. doi:10.1371/journal.pone.0211954
28. Khan S, McCabe J, Hill K, Beales PA. Biodegradable hybrid block copolymer - lipid vesicles as potential drug delivery systems. J Colloid Interface Sci. 2020;562:418–428. doi:10.1016/j.jcis.2019.11.101
29. Bracke S, Carretero M, Guerrero-Aspizua S, et al. Targeted silencing of DEFB4 in a bioengineered skin-humanized mouse model for psoriasis: development of siRNA SECosome-based novel therapies. Exp Dermatol. 2014;23:199–201. doi:10.1111/exd.12321
30. Luther DC, Huang R, Jeon T, et al. Delivery of drugs, proteins, and nucleic acids using inorganic nanoparticles. Adv Drug Deliv Rev. 2020;156:188–213. doi:10.1016/j.addr.2020.06.020
31. Yang S-C, Alalaiwe A, Lin Z-C, Lin Y-C, Aljuffali IA, Fang J-Y. Anti-inflammatory microRNAs for treating inflammatory skin diseases. Biomolecules. 2022;12:1072. doi:10.3390/biom12081072
32. Dave V, Yadav RB, Kushwaha K, Yadav S, Sharma S, Agrawal U. Lipid-polymer hybrid nanoparticles: development & statistical optimization of norfloxacin for topical drug delivery system. Bioact Mater. 2017;2:269–280. doi:10.1016/j.bioactmat.2017.07.002
33. Zhang L, Chan JM, Gu FX, et al. Self-assembled lipid--polymer hybrid nanoparticles: a robust drug delivery platform. ACS Nano. 2008;2:1696–1702. doi:10.1021/nn800275r
34. Pramual S, Lirdprapamongkol K, Atjanasuppat K, Chaisuriya P, Niamsiri N, Svasti J. PLGA-lipid hybrid nanoparticles for overcoming paclitaxel tolerance in anoikis-resistant lung cancer cells. Molecules. 2022;27:8295. doi:10.3390/molecules27238295
35. Desai PR, Marepally S, Patel AR, Voshavar C, Chaudhuri A, Singh M. Topical delivery of anti-TNFα siRNA and capsaicin via novel lipid-polymer hybrid nanoparticles efficiently inhibits skin inflammation in vivo. J Control Release. 2013;170:51–63. doi:10.1016/j.jconrel.2013.04.021
36. Ramadon D, McCrudden MTC, Courtenay AJ, Donnelly RF. Enhancement strategies for transdermal drug delivery systems: current trends and applications. Drug Deliv Transl Res. 2022;12:758–791. doi:10.1007/s13346-021-00909-6
37. Rizvi SMD, Lila ASA, Moin A, et al. Antibiotic-loaded gold nanoparticles: a nano-arsenal against ESBL producer-resistant pathogens. Pharmaceutics. 2023;15:430. doi:10.3390/pharmaceutics15020430
38. Shinn J, Lee J, Lee SA, et al. Oral nanomedicines for siRNA delivery to treat inflammatory bowel disease. Pharmaceutics. 2022;14:1969. doi:10.3390/pharmaceutics14091969
39. Nemati H, Ghahramani M-H, Faridi-Majidi R, et al. Using siRNA-based spherical nucleic acid nanoparticle conjugates for gene regulation in psoriasis. J Control Release. 2017;268:259–268. doi:10.1016/j.jconrel.2017.10.034
40. Ugalde-Arbizu M, Aguilera-Correa JJ, Sebastian ES, et al. Antibacterial properties of mesoporous silica nanoparticles modified with fluoroquinolones and copper or silver species. Pharmaceuticals. 2023;16:961. doi:10.3390/ph16070961
41. Janjua TI, Cao Y, Kleitz F, Linden M, Yu C, Popat A. Silica nanoparticles: a review of their safety and current strategies to overcome biological barriers. Adv Drug Deliv Rev. 2023;203:115115. doi:10.1016/j.addr.2023.115115
42. Liu Q, Zhang Y, Huang J, et al. Mesoporous silica-coated silver nanoparticles as ciprofloxacin/siRNA carriers for accelerated infected wound healing. J Nanobiotechnology. 2022;20:386. doi:10.1186/s12951-022-01600-9
43. Möller K, Müller K, Engelke H, Bräuchle C, Wagner E, Bein T. Highly efficient siRNA delivery from core-shell mesoporous silica nanoparticles with multifunctional polymer caps. Nanoscale. 2016;8:4007–4019. doi:10.1039/c5nr06246b
44. Arruda DC, Lachagès A-M, Demory H, et al. Spheroplexes: hybrid PLGA-cationic lipid nanoparticles, for in vitro and oral delivery of siRNA. J Control Release. 2022;350:228–243. doi:10.1016/j.jconrel.2022.08.030
45. Elizarova TN, Antopolsky ML, Novichikhin DO, et al. A straightforward method for the development of positively charged gold nanoparticle-based vectors for effective siRNA delivery. Molecules. 2023;28:3318. doi:10.3390/molecules28083318
46. Azlan AYHN, Katas H, Busra MFM, Salleh NAM, Smandri A. Metal nanoparticles and biomaterials: the multipronged approach for potential diabetic wound therapy. Nanotechnol Rev. 2021;10:653–670. doi:10.1515/ntrev-2021-0046
47. Jiang X, Lin M, Huang J, et al. Smart responsive nanoformulation for targeted delivery of active compounds from traditional Chinese medicine. Front Chem. 2020;8:559159. doi:10.3389/fchem.2020.559159
48. Campora S, Ghersi G. Recent developments and applications of smart nanoparticles in biomedicine. Nanotechnol Rev. 2022;11:2595–2631. doi:10.1515/ntrev-2022-0148
49. Ge X, Chen L, Zhao B, Yuan W. Rationale and application of PEGylated lipid-based system for advanced target delivery of siRNA. Front Pharmacol. 2020;11:598175. doi:10.3389/fphar.2020.598175
50. Zheng N, Song Z, Liu Y, et al. Redox-responsive, reversibly-crosslinked thiolated cationic helical polypeptides for efficient siRNA encapsulation and delivery. J Control Release. 2015;205:231–239. doi:10.1016/j.jconrel.2015.02.014
51. Saneyoshi H, Ono A. Development of protecting groups for prodrug-type oligonucleotide medicines. Chem Pharm Bull. 2018;66:147–154. doi:10.1248/cpb.c17-00696
52. Ni S, Yao H, Wang L, et al. Chemical modifications of nucleic acid aptamers for therapeutic purposes. Int J Mol Sci. 2017;18:1683. doi:10.3390/ijms18081683
53. Osborn MF, Khvorova A. Improving siRNA delivery in vivo through lipid conjugation. Nucleic Acid Ther. 2018;28:128–136. doi:10.1089/nat.2018.0725
54. Catani M, De Luca C, Alcântara JMG, et al. Oligonucleotides: current trends and innovative applications in the synthesis, characterization, and purification. Biotechnol J. 2020;15:e1900226. doi:10.1002/biot.201900226
55. Lim SB, Banerjee A, Önyüksel H. Improvement of drug safety by the use of lipid-based nanocarriers. J Control Release. 2012;163:34–45. doi:10.1016/j.jconrel.2012.06.002
56. Yu H-P, Liu F-C, Chung Y-K, Alalaiwe A, Sung CT, Fang J-Y. Nucleic acid-based nanotherapeutics for treating sepsis and associated organ injuries. Theranostics. 2024;14:4411–4437. doi:10.7150/thno.98487
57. Agrawal R, Jurel P, Deshmukh R, et al. Emerging trends in the treatment of skin disorders by herbal drugs: traditional and nanotechnological approach. Pharmaceutics. 2024;16:869. doi:10.3390/pharmaceutics16070869
58. Zakrewsky M, Mitragotri S. Therapeutic RNAi robed with ionic liquid moieties as a simple, scalable prodrug platform for treating skin disease. J Control Release. 2016;242:80–88. doi:10.1016/j.jconrel.2016.09.003
59. Dharamdasani V, Mandal A, Qi QM, Suzuki I, Bentley MVLB, Mitragotri S. Topical delivery of siRNA into skin using ionic liquids. J Control Release. 2020;323:475–482. doi:10.1016/j.jconrel.2020.04.038
60. Lee W-R, Lin Y-K, Alalaiwe A, Wang P-W, Liu P-Y, Fang J-Y. Fractional laser-mediated siRNA delivery for mitigating psoriasis-like lesions via IL-6 silencing. Mol Ther Nucleic Acids. 2020;19:240–251. doi:10.1016/j.omtn.2019.11.013
61. Dorrani M, Garbuzenko OB, Minko T, Michniak-Kohn B. Development of edge-activated liposomes for siRNA delivery to human basal epidermis for melanoma therapy. J Control Release. 2016;228:150–158. doi:10.1016/j.jconrel.2016.03.010
62. Boakye CHA, Patel K, Doddapaneni R, Bagde A, Marepally S, Singh M. Novel amphiphilic lipid augments the co-delivery of erlotinib and IL36 siRNA into the skin for psoriasis treatment. J Control Release. 2017;246:120–132. doi:10.1016/j.jconrel.2016.05.017
63. Chhibber T, Scherzer MT, Prokofyeva A, et al. Transdermal delivery of ultradeformable cationic liposomes complexed with miR211-5p (UCL-211) stabilizes BRAFV600E+ melanocytic nevi. J Control Release. 2025;381:113586. doi:10.1016/j.jconrel.2025.113586
64. Lee W-R, Chou W-L, Lin Z-C, Sung CT, Lin C-Y, Fang J-Y. Laser-assisted nanocarrier delivery to achieve cutaneous siRNA targeting for attenuating psoriasiform dermatitis. J Control Release. 2022;347:590–606. doi:10.1016/j.jconrel.2022.05.032
65. Fukuta T, Oshima Y, Michiue K, Tanaka D, Kogure K. Non-invasive delivery of biological macromolecular drugs into the skin by iontophoresis and its application to psoriasis treatment. J Control Release. 2020;323:323–332. doi:10.1016/j.jconrel.2020.04.044
66. Lahiji SF, Dangol M, Jung H. A patchless dissolving microneedle delivery system enabling rapid and efficient transdermal drug delivery. Sci Rep. 2015;5:7914. doi:10.1038/srep07914
67. Bolton CJW, Howells O, Blayney GJ, et al. Hollow silicon microneedle fabrication using advanced plasma etch technologies for applications in transdermal drug delivery. Lab Chip. 2020;20:2788–2795. doi:10.1039/d0lc00567c
68. Guagliardo R, Herman L, Penders J, et al. Surfactant protein B promotes cytosolic SiRNA delivery by adopting a virus-like mechanism of action. ACS Nano. 2021;15:8095–8109. doi:10.1021/acsnano.0c04489
69. Kou L, Wang Y, Li J, et al. Mitochondria-lysosome-extracellular vesicles axis and nanotheranostics in neurodegenerative diseases. Exp Neurol. 2024;376:114757. doi:10.1016/j.expneurol.2024.114757
70. Guk K, Lim H, Kim B, Hong M, Khang G, Lee D. Acid-cleavable ketal containing poly(β-amino ester) for enhanced siRNA delivery. Int J Pharm. 2013;453:541–550. doi:10.1016/j.ijpharm.2013.06.021
71. Hatakeyama H, Ito E, Akita H, et al. A pH-sensitive fusogenic peptide facilitates endosomal escape and greatly enhances the gene silencing of siRNA-containing nanoparticles in vitro and in vivo. J Control Release. 2009;139:127–132. doi:10.1016/j.jconrel.2009.06.008
72. Kumar N, Singh S, Sharma P, Kumar B, Kumar A. Single-, dual-, and multi-stimuli-responsive nanogels for biomedical applications. Gels. 2024;10:61. doi:10.3390/gels10010061
73. Zakrewsky M, Kumar S, Mitragotri S. Nucleic acid delivery into skin for the treatment of skin disease: proofs-of-concept, potential impact, and remaining challenges. J Control Release. 2015;219:445–456. doi:10.1016/j.jconrel.2015.09.017
74. Wang M-Z, Niu J, Ma H-J, et al. Transdermal siRNA delivery by pH-switchable micelles with targeting effect suppress skin melanoma progression. J Control Release. 2020;322:95–107. doi:10.1016/j.jconrel.2020.03.023
75. Tiwari N, Osorio-Blanco ER, Sonzogni A, Esporrín-Ubieto D, Wang H, Calderón M. Nanocarriers for skin applications: where do we stand? Angew Chem Int Ed Engl. 2022;61:e202107960. doi:10.1002/anie.202107960
76. Li N, Luo H-C, Yang C, et al. Cationic star-shaped polymer as an siRNA carrier for reducing MMP-9 expression in skin fibroblast cells and promoting wound healing in diabetic rats. Int J Nanomed. 2014;9:3377–3387. doi:10.2147/IJN.S66368
77. Huang Y, Yu F, Park Y-S, et al. Co-administration of protein drugs with gold nanoparticles to enable percutaneous delivery. Biomaterials. 2010;31:9086–9091. doi:10.1016/j.biomaterials.2010.08.046
78. Suzuki IL, de Araujo MM, Bagnato VS, Bentley MVLB. TNFα siRNA delivery by nanoparticles and photochemical internalization for psoriasis topical therapy. J Control Release. 2021;338:316–329. doi:10.1016/j.jconrel.2021.08.039
79. Xiong L, Chen S, Li S, et al. ATP-responsive tumor targeted lipid nanoparticle for enhanced siRNA delivery and improved treatment efficacy in melanoma. J Control Release. 2025;382:113622. doi:10.1016/j.jconrel.2025.113622
80. Zhang M, Qin X, Gao Y, et al. Transcutaneous immunotherapy for RNAi: a cascade-responsive decomposable nanocomplex based on polyphenol-mediated framework nucleic acid in psoriasis. Adv Sci. 2023;10:e2303706. doi:10.1002/advs.202303706
81. Xu L, Shao Z, Fang X, et al. Exploring precision treatments in immune-mediated inflammatory diseases: harnessing the infinite potential of nucleic acid delivery. Exploration. 2025;5:20230165. doi:10.1002/EXP.20230165
82. Zhou X, Chen Y, Cui L, Shi Y, Guo C. Advances in the pathogenesis of psoriasis: from keratinocyte perspective. Cell Death Dis. 2022;13:81. doi:10.1038/s41419-022-04523-3
83. Funding AT, Johansen C, Kragballe K, et al. Mitogen- and stress-activated protein kinase 1 is activated in lesional psoriatic epidermis and regulates the expression of pro-inflammatory cytokines. J Invest Dermatol. 2006;126:1784–1791. doi:10.1038/sj.jid.5700252
84. M S, A E, H F. Advances in psoriasis physiopathology and treatments: up to date of mechanistic insights and perspectives of novel therapies based on innovative skin drug delivery systems (ISDDS). J Control Release. 2016;239. doi:10.1016/j.jconrel.2016.07.003
85. Morry J, Ngamcherdtrakul W, Gu S, et al. Dermal delivery of HSP47 siRNA with NOX4-modulating mesoporous silica-based nanoparticles for treating fibrosis. Biomaterials. 2015;66:41–52. doi:10.1016/j.biomaterials.2015.07.005
86. Marepally S, Boakye CHA, Patel AR, et al. Topical administration of dual siRNAs using fusogenic lipid nanoparticles for treating psoriatic-like plaques. Nanomedicine. 2014;9:2157–2174. doi:10.2217/nnm.13.202
87. Xu J, Chen H, Qian H, Wang F, Xu Y. Advances in the modulation of ROS and transdermal administration for anti-psoriatic nanotherapies. J Nanobiotechnology. 2022;20:448. doi:10.1186/s12951-022-01651-y
88. Li L, Wu X, Wu J, et al. Transdermal delivery of Fn14 siRNA using a novel composite ionic liquid for treatment of psoriasis-like skin lesions. J Control Release. 2024;365:818–832. doi:10.1016/j.jconrel.2023.12.009
89. Ma X, Cong R, Cui X, et al. Dendritic lipopeptide-based transdermal siRNA delivery systems for effective non-invasive therapy in psoriasis. J Control Release. 2025;381:113581. doi:10.1016/j.jconrel.2025.113581
90. Tran MA, Gowda R, Sharma A, et al. Targeting V600EB-raf and Akt3 using nanoliposomal-small interfering RNA inhibits cutaneous melanocytic lesion development. Cancer Res. 2008;68:7638–7649. doi:10.1158/0008-5472.CAN-07-6614
91. Chen Y, Bathula SR, Yang Q, Huang L. Targeted nanoparticles deliver siRNA to melanoma. J Invest Dermatol. 2010;130:2790–2798. doi:10.1038/jid.2010.222
92. Li L, Hou J, Liu X, et al. Nucleolin-targeting liposomes guided by aptamer AS1411 for the delivery of siRNA for the treatment of malignant melanomas. Biomaterials. 2014;35:3840–3850. doi:10.1016/j.biomaterials.2014.01.019
93. Arms L, Smith DW, Flynn J, et al. Advantages and limitations of current techniques for analyzing the biodistribution of nanoparticles. Front Pharmacol. 2018;9:802. doi:10.3389/fphar.2018.00802
94. Zhang C, Zhu X, Hou S, Pan W, Liao W. Functionalization of nanomaterials for skin cancer theranostics. Front Bioeng Biotechnol. 2022;10:887548. doi:10.3389/fbioe.2022.887548
95. Zhang X, Cai A, Gao Y, Zhang Y, Duan X, Men K. Treatment of melanoma by nano-conjugate-delivered Wee1 siRNA. Mol Pharm. 2021;18:3387–3400. doi:10.1021/acs.molpharmaceut.1c00316
96. Wang Y, Luo Y-L, Chen Y-F, et al. Dually regulating the proliferation and the immune microenvironment of melanoma via nanoparticle-delivered siRNA targeting onco-immunologic CD155. Biomater Sci. 2020;8:6683–6694. doi:10.1039/d0bm01420f
97. Serra R, Grande R, Butrico L, et al. Chronic wound infections: the role of pseudomonas aeruginosa and staphylococcus aureus. Expert Rev Anti Infect Ther. 2015;13:605–613. doi:10.1586/14787210.2015.1023291
98. Guan H, Dong W, Lu Y, et al. Distribution and antibiotic resistance patterns of pathogenic bacteria in patients with chronic cutaneous wounds in China. Front Med. 2021;8:609584. doi:10.3389/fmed.2021.609584
99. Matei A-M, Caruntu C, Tampa M, et al. Applications of nanosized-lipid-based drug delivery systems in wound care. Appl Sci. 2021;11:4915. doi:10.3390/app11114915
100. Xu X, Wang L, Bi X, et al. Targeted silencing of engrailed-1 reprograms profibrotic fibroblast lineage for scarless wound healing. Mol Ther. 2025;33:4889–4903. doi:10.1016/j.ymthe.2025.07.031
101. Zhang G-Y, Langan EA, Meier NT, Funk W, Siemers F, Paus R. Thyroxine (T4) may promote re-epithelialisation and angiogenesis in wounded human skin ex vivo. PLoS One. 2019;14:e0212659. doi:10.1371/journal.pone.0212659
102. Cunha S, Costa CP, Moreira JN, Lobo JMS, Silva AC. Using the quality by design (QbD) approach to optimize formulations of lipid nanoparticles and nanoemulsions: a review. Nanomedicine. 2020;28:102206. doi:10.1016/j.nano.2020.102206
103. Sheybanifard M, Guerzoni LPB, Omidinia-Anarkoli A, et al. Liposome manufacturing under continuous flow conditions: towards a fully integrated set-up with in-line control of critical quality attributes. Lab Chip. 2023;23:182–194. doi:10.1039/D2LC00463A
104. Monopoli MP, Åberg C, Salvati A, Dawson KA. Biomolecular coronas provide the biological identity of nanosized materials. Nat Nanotechnol. 2012;7:779–786. doi:10.1038/nnano.2012.207
105. Lila ASA, Kiwada H, Ishida T. The accelerated blood clearance (ABC) phenomenon: clinical challenge and approaches to manage. J Control Release. 2013;172:38–47. doi:10.1016/j.jconrel.2013.07.026
106. Verhoef JJF, Carpenter JF, Anchordoquy TJ, Schellekens H. Potential induction of anti-PEG antibodies and complement activation toward PEGylated therapeutics. Drug Discov Today. 2014;19:1945–1952. doi:10.1016/j.drudis.2014.08.015
107. Zoio P, Oliva A. Skin-on-a-chip technology: microengineering physiologically relevant in vitro skin models. Pharmaceutics. 2022;14:682. doi:10.3390/pharmaceutics14030682
108. Mura S, Nicolas J, Couvreur P. Stimuli-responsive nanocarriers for drug delivery. Nat Mater. 2013;12:991–1003. doi:10.1038/nmat3776
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.