Back to Journals » Orthopedic Research and Reviews » Volume 12
Sternoclavicular Joint Instability: Symptoms, Diagnosis And Management
Authors Garcia JA, Arguello AM ![]() , Momaya AM, Ponce BA
, Momaya AM, Ponce BA
Received 9 May 2020
Accepted for publication 13 July 2020
Published 28 July 2020 Volume 2020:12 Pages 75—87
DOI https://doi.org/10.2147/ORR.S170964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Jacob A Garcia,1 Alexandra M Arguello,2 Amit M Momaya,2 Brent A Ponce2
1University Of Alabama At Birmingham School Of Medicine, Birmingham, AL 35294, USA; 2University Of Alabama At Birmingham, Department Of Orthopedic Surgery, Birmingham, AL 35294, USA
Correspondence: Brent A Ponce
Department of Orthopaedic Surgery, University Of Alabama At Birmingham, Birmingham, AL 35294, USA
Tel +1 205-930-7081
Fax +1 205-930-8981
Email [email protected]
Abstract: Sternoclavicular joint (SCJ) instability is a rare condition and results from either a traumatic high energy impact, such as a motor vehicle crash or contact sports injury, or non-traumatically as a result of structural pathology. The infrequency of this injury has contributed to its diagnosis being missed as well as the paucity of literature on treatment and outcomes. Patients with SCJ instability often report diminished range of motion as well as shoulder girdle pain. The presentation of instability in the sternoclavicular joint can vary in severity and anterior or posterior directionality. Variation in severity of the instability changes the course of treatment regarding either operative or non-operative interventions to stabilize the SCJ. In general, anterior instability of the SCJ (the medial clavicle is displaced anterior to the sternum) is less urgent and generally manageable by symptom alleviation and rehabilitation, although some anterior instability cases require surgical intervention. In the case of posterior SCJ instability (the medial clavicle is displaced posterior to the sternum), patients require prompt joint reduction as they are at the greater risk of life-threatening injury due to the location of critical structures of the mediastinum posterior to the SCJ. Computed tomography visualization is useful to confirm dislocation or subluxation direction to better formulate a proper treatment plan. The purpose of this review is to report the clinical presentation and management of SCJ instability including pertinent symptoms, the diagnostic approaches to evaluating SCJ instability, as well as operative and non-operative management of the joint instability.
Keywords: sternoclavicular joint instability, SCJ dislocation, surgical techniques
Introduction
The sternoclavicular joint (SCJ) is an inherently unstable diarthrodial joint between the manubrium of the sternum and clavicle which obtains stability from ligamentous support.1–4 Injury to the SCJ is uncommon and generally presents from a high energy traumatic impact.5,6 SCJ injuries make up 5% of shoulder girdle injuries with dislocation of the SCJ being responsible for 3% of dislocations in the shoulder region.7,8 The direction of the medial clavicle subluxation or dislocation in relation to the sternum is used to define the direction of the instability or dislocation. In the more commonly encountered anterior SCJ dislocation, the medial clavicle is dislocated anterior to the sternum. As SCJ injuries generally occur in the setting of high energy collisions, it is not infrequent for injuries to be underdiagnosed due to the potentially low prevalence of clinical symptoms combined with concurrent distracting injuries.5 Atraumatic dislocation and instability of the SCJ are less frequent and can arise in patients who present with congenital malformations of the clavicle, generalized hypermobility syndrome, Ehler-Danlos, muscle patterning abnormalities, infection, and arthritis of the SCJ.8
Regardless of the mechanism of injury, the diagnosis and appropriate treatment of SCJ instability is necessary to preserve function and maintain quality of life.9 In the case of anterior SCJ instability, which is nearly nine times more common than posterior, a more conservative approach may be taken due to the lack of critical anatomic structures anteriorly.8 Anterior subluxations and dislocations may be treated through reduction and rehabilitation, though some instances may require stabilization through surgical intervention and management.8
SCJ injury leading to posterior subluxation or dislocation poses much greater risk to the patient. Posterior SCJ instability has life threatening implications due to the hilar and mediastinal anatomy that lies posterior to the SCJ.9 Thus, surgical intervention is usually required to not only reduce the dislocation but to also maintain stability and decrease likelihood of re-dislocation. The surgical approaches to stabilizing the sternoclavicular joint can involve the use of plates and screws or tendinous grafts depending upon what anatomical structures have been damaged resulting in instability. Due to the infrequency of SCJ instability, there is no gold standard treatment algorithm.5 This review article is aimed at detailing the approaches to diagnosis and management of SCJ instability.
Anatomical and Biomechanical Properties
Anatomical Properties
The SCJ is a diarthrodial joint which forms the union between the sternum and clavicle and is the only point of bony articulation between the clavicle and axial skeleton.5 The articulating surfaces of the SCJ are coated with a layer of hyaline cartilage and separated by a fibrocartilage disk. The SCJ is unique for its saddle shape and limited osseous restraint, which causes the joint to rely heavily upon ligamentous structures to maintain stability.1,2 The ligamentous structures stabilizing the SCJ include the anterior capsule, posterior capsule, intra-articular disk ligament, interclavicular ligament, and costoclavicular ligament (Figure 1).5
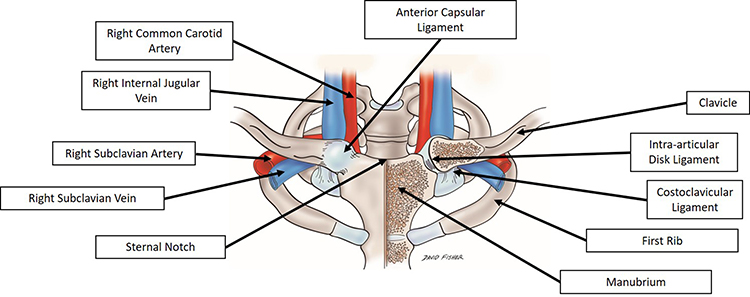 |
Figure 1 Anatomic depiction of the boney structures of the SCJ, ligamentous connections of the SCJ, as well as the major vessels that lie posterior to the SCJ. |
The capsular ligament, which is comprised of the anterior and posterior capsular ligamentous components, is visualized as thickenings around the joint capsule which enshrouds the external portion of the SCJ.10 The intra-articular disk ligament is dense and fibrous, originating from the chondral joint of the first rib and passing vertically through the SCJ, which allows for the creation of two distinct joint areas. Attachment for the intra-articular disk ligament occurs on both the superior and posterior portions of the clavicle and integrates within the capsular ligament.2 The interclavicular ligament is a band of thick fibrous material connecting the superior, medial portions of right and left capsular ligaments. The costoclavicular ligament or rhomboid ligament transects the synchondral joint formed by the manubrium and first rib and originates from the inferior border of the medial clavicle.1,2,10
It is imperative to appreciate that there are several critical anatomic structures which lie posterior to the SCJ. The innominate (also known as brachiocephalic) veins most often lie directly behind the SCJ.9 Other structures that are commonly found at the SCJ reconstruction drill holes include the common carotid arteries, subclavian veins, the superior vena cava, aortic arch, internal mammary arteries, and the trachea.9 These structures may be as close as 1mm to the SCJ and are susceptible to becoming impinged or damaged in posterior SCJ dislocations as well as during the reconstructive procedures (Figure 1).9 This relationship is the source of the general recommendation for cardiothoracic surgeons to be in close proximity when surgery on the SCJ is being performed with either a reduction (closed or open), plating, or reconstruction.
Biomechanical Properties
Movement of the diarthrodial SCJ is crucial to the mobility of the shoulder girdle and heavily reliant on the ligamentous and capsular structures which stabilize the joint.11 The range of motion in the SCJ is significant as the ligamentous structures accommodate for 35 degree elevation change, 35 degree anterior-posterior flexion and extension, and 50 degree rotation about its linear plane.1,2 Additionally, during humeral elevation up to 90 degrees, there are 4 degrees of clavicular elevation about the SCJ for every 10 degrees of humeral elevation,12 an observation which established the notion that rigid fixation at the SCJ would result in inadequate mobility.
The capsular ligament, which is comprised of both an anterior and posterior segment, resists upward movement of the medial clavicle in response to axial load placed on the distal clavicle.10 Spencer et al,3 performed a biomechanical cadaver study to elucidate the individual stabilizing roles of the ligaments and capsules of the SCJ. They found that disruption of the posterior capsule resulted in significant posterior and anterior translation, and disruption of the anterior capsule affected anterior stability as well. This finding is the basis for the majority of surgical techniques seeking to reconstruct the posterior capsule/ligaments in cases of symptomatic chronic instability. The intra-articular disk ligament which passes through the articular joint and joins the capsular ligament resists medial displacement upon compressive forces applied to the clavicle.1,2 The interclavicular ligament connects both left and right medial clavicles to the sternum and functions to resist against upward movement of the medial clavicle in response to weight applied downward to the shoulder and distal clavicle. The costoclavicular ligament is considered the strongest of all the ligamentous structures of the SCJ with its twisted cord like appearance. The costoclavicular ligament has several anterior and posterior points of fusion which allow for a variety of structurally stabilizing features.1,5 The anterior portion of the costoclavicular ligament resists upward rotation and lateral movement of the clavicle while the posterior portion of the costoclavicular ligament resists downward rotation and medial movement of the clavicle.2
Classifications, Symptoms and Diagnosis
Classifications
Classification of SCJ instability can be broadly described by a set of parameters including acuity (acute or chronic), degree (subluxation or dislocation), directionality (anterior or posterior) and mechanism (atraumatic or traumatic) of the instability.1,13 Additionally, recent sources report utilizing the Stanmore triangle, classically used to describe glenohumeral instability, for evaluation of SCJ instability.5 The Stanmore triangle is based on three groupings of instability; type I is traumatic structural, type II is atraumatic structural, and type III is muscle patterning non-structural. In the case of type I instability there is clear trauma leading to structural change of the SCJ, such as dislocation or fracture. Type II instability is not related to any trauma but still shows clear structural changes in the SCJ causing instability possibly as a result from repetitive microtrauma. Type III instability occurs when the musculature, particularly the pectoralis major, contracts abnormally and causes instability of the SCJ.
Another system of numerically ranking SCJ ligamentous disturbance was developed by Allman et al,14 in 1967 and is traditionally used when staging the severity of the SCJ instability. A Type 1 SCJ instability rating reflects a sprain of the sternoclavicular ligaments without subluxation or dislocation. Type 2 instability indicates anterior or posterior clavicle subluxation from ligamentous injury. Type 3 SCJ instability indicates complete disruption of all ligamentous support with anterior or posterior clavicular dislocation.
Symptoms
Due to the ligamentous strength stabilizing the SCJ, often trauma resulting in a large force vector must be applied to result in SCJ instability. The extent of energy required to destabilize the SCJ frequently also causes injury to the chest wall and surrounding structures which may lead to a delayed or missed diagnosis.15 Part of the secondary survey of a trauma patient should include physical examination and advanced imaging of the SCJ if the mechanism was such that this injury is suspected.
The presentation of posterior SCJ dislocation is an emergent medical condition and should be dealt with as such. Thirty percent of patients who present with posterior dislocation of the SCJ sustained direct mediastinal injury from posterior displacement of the clavicle.16 A block of venous flow can occur as the clavicle impinges the brachiocephalic vein most commonly, and subclavian vein or jugular vein with sufficient displacement; posterior SCJ dislocation can also lead to dysphagia, cough, hoarseness, and choking sensation which all indicate superior mediastinal injury due to clavicular compression and pose a serious threat to the life of the patient.6,15,17-19
Patients presenting with a Allman type 2 or 3 SCJ injury generally present with chest and shoulder pain which is made worse by moving or lying flat on one’s back.1 Anterior type 2 or 3 SCJ instability may expose a protuberance of the clavicle medially, while posterior type 2 or 3 dislocations will be more subtle. A complete exam of the clavicle must be done in order to help identify a clavicle fracture or the possibility of a concomitant acromioclavicular (AC) joint dislocation, which would result in a “floating clavicle”.20 Due to the late ossification of the medial clavicle, patients up to 25 years of age are at risk for developing a physeal injury which can present with symptoms similar to SCJ dislocation, also known as “psuedodislocation”.5,21
Diagnosis
After sustaining trauma to the SCJ, an anteroposterior x-ray should be ordered to assess for clavicular injury. However, this diagnostic method is often hindered due to anatomic structures obstructing the view of the SCJ. The “serendipity view” allows for visualization of both SCJs and is used for comparative purposes as well as greater visibility of the clavicle and SCJ.22 In a “serendipity view” radiograph, the x-ray beam is oriented 40 degrees toward the head and centered on the SCJ.23,24
However, given the challenge of obtaining and interpreting radiographic evidence of SCJ injuries, computed tomography (CT) is recommended when SCJ injures are suspected (Figure 2). CT scans not only provide greater clarity of the SCJ but also help identify potential injury to mediastinal structures.23 CT scans are also useful for identifying associated fractures and the direction and degree of SCJ dislocation.1,25 Advanced imaging with either a CT, CT angiogram or magnetic resonance imaging (MRI) is recommended when planning for operative repair of the SCJ in order to better assess surrounding anatomy of the critical structures which may be encountered during surgery.26–31
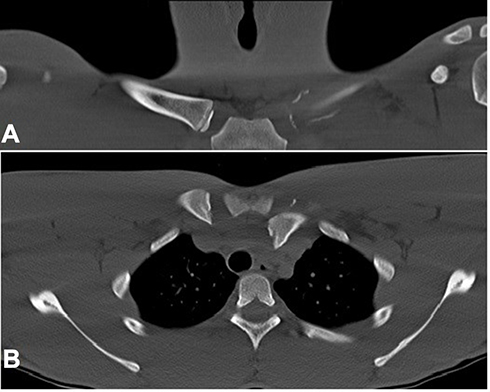 |
Figure 2 CT scan depicting coronal (A) and axial (B) views of a left posterior sternoclavicular physeal fracture dislocation. |
Management
Non-Operative Management
The type 1 sprain of the SCJ is accompanied with pain but the joint is stable. Management involves sling immobilization for a short period of time, ie 1–2 weeks, and concomitant anti-inflammatories, after which normal physical activity can resume.1 Slightly more severe sprains of the SCJ, ie a type 2 Allman injury, are usually associated with some form of subluxation instability of the clavicle in either the anterior or posterior direction.14 Treatment for type 2 injuries is similar to type 1 injuries but with longer sling immobilization, ie 4–6 weeks, with the goal of immobilization to provide a protected environment to allow ligament healing and prevent further injury.1 Great care must be taken with non-operative management of displaced physeal injuries so the treating surgeon must ensure he/she is dealing with an intact bone rather than a transphyseal injury.
For type 3 Allman injuries in which the SCJ is dislocated, the treatment is less well defined and is based primarily upon direction and acuity of injury. Regardless of direction, closed reduction is most often the first line of action. Closed reduction of anterior dislocation is accomplished through placing the patient in a supine position with a 4-inch foam pad beneath the back and between the scapulae of the patient, followed by continuous pressure in the posterior and lateral direction applied to the medial boarder of the clavicle where it meets the SCJ.6,32 The approach for closed reduction of a posterior dislocation usually involves the administration of anesthetic sedation due to severe pain and muscle spasm. The patient is oriented flat on their back with a foam pad centered underneath to pull back their shoulders. The arm is then positioned 90 degrees perpendicular to the body and the arm is pulled with constant pressure in order to gradually position the arm into full extension (Figure 3).6 While there is literature support for closed reductions, it is important to note that not all SCJ dislocations are amenable to closed reduction and they may not remain stable even after successful reduction. Anterior dislocations are more likely to re-dislocate than posterior dislocations after closed reduction and high risk contact sports should be avoided for 3 to 4 months in order to prevent repeated injury to the joint and chronic instability of the SCJ.5
 |
Figure 3 Illustration of closed reduction of a posterior SCJ dislocation. A foam pad or bolster is placed under the scapulae while lateral traction is applied as the arm is pulled into extension. |
There are very few longitudinal studies investigating non-operative outcomes. The recurrence rate of anterior SCJ dislocation after non-operative management has been reported around 50%.33 In a small cohort of anterior instability patients with a mean follow up time of 62.9 months, the outcomes of non-surgical treatment were assessed.34 In the study, 7 of 10 patients treated with analgesics and sling immobilization experienced good results, 2 reported fair results from treatment, and 1 reported a poor outcome from nonsurgical treatment. What is unclear in the literature are the variables of the subset of patients that have fair to poor outcomes from non-surgical treatment and that may benefit from early surgical stabilization.
Operative Management
Acute SCJ Dislocation
Traumatic posterior dislocations may need to be surgically reduced due to the critical structures that lie behind the manubrium.5 Use of a towel clamp or direct finger grasping of the clavicle is may be used to aid the reduction. It is recommended to consult a cardiothoracic surgeon prior to performing a closed or open reduction in the case that a vascular injury occurs or is revealed requiring surgical intervention.15 It is critical to assess the stability of the reduction at the time of reduction such that if you can re-dislocate the clavicle with minimal force, surgical reconstruction of the joint is necessary. After successful reduction of the posteriorly dislocated joint, the SCJ should be immobilized in a sling for 6 weeks with particular attention to avoid excessive anterior and posterior motion of the elbow which stresses the SCJ.
The treatment of acute SCJ dislocation can involve a myriad of techniques and procedures. Traditionally, non-operative methods via closed reduction are used initially, however, there is evidence of recurrent or subsequent complications including instability, mediastinal injury, and fracture nonunion when taking this approach.22,32,35-38 Often the surgical options for reconstruction of the SCJ involve cannulated bone tunnels, grafted ligaments, suture anchors, and K-wires.36,39 These, however, have the possibility of loosening or failing over time, leading to revisions.40,41 Given the low density of the manubrium, anchor fixation may be less robust than in a long or weight bearing bone and should be tested vigorously at the time of insertion. In the acute setting where the healing process of the joint is still ongoing, it has been proposed that a surgical plate for short-term stabilization of the SCJ may lead to greater benefit.41
The use of a surgical plate for fixation of an unstable SCJ is referred to as an open reduction internal fixation (ORIF) (Figure 4). During an ORIF procedure, a locking compression plate, Balser plate, clavicular hook plate, or pre-contoured plate is used to provide fixation across the joint followed by sling immobilization for a minimum of two weeks.41–43 Hardware removal is recommended in order to avoid the possible migration of the hook in the manubrial or posterior direction.43 However, there have been cases where patients may have asymptomatic hardware and refuse its removal, such as in the case of locking compression plates which are smaller than the other plate options.42 Hardware removal prior to 3 months post-operation is avoided as it may lead to chronic SCJ instability.37
 |
Figure 4 AP radiograph status post ORIF of a left sternoclavicular joint dislocation. |
Recently, outcomes of a case series of first-time anterior SCJ dislocators who underwent capsular plication bolstered by internal bracing with suture tape were published.44 At a minimum of 2 year follow up, there were no recurrences of dislocation or any evidence of instability or subluxation. There were no reported complications with the procedure, and all patients returned to sport within 1 year of the procedure. Internal bracing is becoming more widely used by surgeons to treat knee, elbow, and ankle ligamentous instability.45–47 This technique could become especially useful for contact sport athletes who are more likely to have a recurrence of dislocation than the general public.
Chronic SCJ Instability
The majority of surgeons attempting closed reduction treatment for SCJ dislocations report over 50% of the patients have recurrent SCJ instability with dislocation or subluxation of the joint.33 This likely occurs because the injured ligamentous structures are torn or stretched and lose their ability to maintain stability of the SCJ after injury. The failure of closed reduction in the setting of persistent activity-limiting symptoms typically requires surgical treatment.5,23,24,26
SCJ surgical stabilization has evolved over time. Initially, rigid stabilization was attempted through wires and pins. This method was associated with a high mortality rate and significant complications and has since been discontinued.22,48,49 Stabilization of chronic injuries using suture fixation with reconstruction of the ligaments was then attempted, however this provided insufficient biomechanical stabilization.50 The utilization of a graft for reconstruction of the SCJ showed improved biomechanical properties.51 As the surgical techniques for SCJ stabilization progressed, a figure-8 method of reconstruction using various grafted tendons was adopted. The graft materials used for the figure-8 repair include semitendinosus, gracilis, sternocleidomastoid, palmaris longus, and hamstring tendons. The grafted tendons are passed through holes made in the medial clavicle and manubrium and are tied in a figure-8 fashion (Figure 5A).13,52,53 The biomechanical stability of each graft reconstruction technique has been shown to be reliable and sufficient to repair the unstable SCJ.51 From the figure-8 technique, multiple novel techniques have been created in order to avoid the dangers of drilling in the anterior-to-posterior fashion and utilizing additional materials including suture anchors and different configurations of graft material.54–58 Resection of the medial clavicle has also been explored in the setting of a chronically unstable and painful SCJ, with both open and arthroscopic techniques being described.56,59-64
 |
Figure 5 Summary of the surgical techniques for SCJ instability management. (5A) SCJ reconstruction using the Figure-8 surgical technique with grafted ligament or tendon. (5B) SCJ reconstruction using the suture anchor technique described by Bak et al (5C) SCJ reconstruction using the Roman numeral X technique described by Guan et al (5D) SCJ reconstruction using the Sternal Docking technique described by Sanchez-Sotelo et al. |
In a biomechanical study by Spencer and Kuhn,51 three different graft techniques of SCJ repair were examined. The study compared subclavius tendon stabilization,65 intramedullary tendon stabilization,62 and semitendinosus tendon figure-8 stabilization of the SCJ. The reconstructed joint was tested for percentage of stiffness compared to the stiffness of the normal, uninjured SCJ. For the anterior dislocation repair, there was a decrease in stiffness of 70.1%, 56.9%, and 36.9% in the intramedullary, subclavius, and figure-8 techniques respectively. In the posterior dislocation model, there was a decrease in stiffness compared to the native SCJ of 74.4%, 82.3%, and 3.8% in the intramedullary, subclavius, and figure-8 techniques respectively. The semitendinosus tendon figure-8 reconstruction method resulted in a peak load value three times that of the subclavius and intramedullary techniques. This demonstrated that the semitendinosus figure-8 technique for SCJ reconstruction yields better biomechanical properties compared to subclavius tendon stabilization and intramedullary tendon stabilization. More recently, a biomechanical study found that oblique drill holes, which aim to pose less risk to structures inferior to the SCJ during reconstruction, result in instability compared to straight drill holes. Additionally, suture tape augmentation provides additional stability compared with tendon graft alone.66
Surgical Techniques and Outcomes For SCJ Instability
Resection Arthroplasty
Techniques for resection or excision of the medial clavicle for chronic SCJ instability and pain include arthroscopic59,63 and open62 techniques. In general, these studies present good outcomes in that patients have return of function and decreased pain. Dekker et al,60 evaluated minimum five-year outcomes from a small cohort of 21 sternoclavicular joints for open resection arthroplasty. All post-operative outcomes scores increased significantly. The average patient reported success was a 9 out of 10 (range 2–10), and average pain after surgery improved significantly. Of the 14 patients which answered a return to sport questionnaire, 12 reported successful return to sports. Three patients required revision surgery due to recurrent SCJ pain after 5 year follow up. Finally, Panzica et al,56 also investigated outcomes of SCJ surgical management. Six of the 11 patients in this study underwent resection arthroplasty, while the others underwent some form of reconstruction. Two patients who underwent resection of the medial clavicle reported poor results due to persistent instability, though there were no significant differences in overall patient reported outcomes between the resection and reconstruction groups. It is important to note that resection arthroplasty outcomes are superior with preservation of the costoclavicular ligament and caution taken to not over-resect the medial clavicle.
Figure-8 Surgical Reconstruction
The figure-8 weave using an allograft tendon is commonly utilized for SCJ reconstruction based on the biomechanical study of Spencer and Kuhn.51 Bae et al,7 reported outcomes of 11 patients treated with a figure-8 surgical reconstruction for chronic anterior instability in a pediatric patient population with a mean follow-up of 4 years. The outcomes of the 11 patients treated with the ligamentous reconstruction were compared to 4 patients who had a resection of the medial clavicle and demonstrated to be 17% better according to the Simple Shoulder Test (SST). The mean SST score for patients who underwent medial clavicle resections was 9.8, while the mean SST score for patients who underwent SCJ reconstruction was 11.4. This result, although higher for the reconstruction cohort, does not hold clinical significance as the value of SST discrepancy is less than 2.4.67 Two of the patients in this cohort reported SCJ instability post-operatively. Overall the patients had an average ASES score over 90% of healthy individuals’ mean values, and there were no surgical revisions. Over 85% of the patients recorded having physical limitations post-surgery, in which 13 of the 15 stated they had some residual physical limitation in recreational sports and activities. Thus, orthopedic surgeons should be cognizant and inform patients that surgery aims to relieve pain and stabilize the joint, but residual functionality deficits may persist.
Sabatini et al,58 also performed a study regarding figure-8 surgical reconstruction of the SCJ. All 10 patients included in the study underwent figure-8 allograft reconstruction augmented by 2 tenodesis screws and were evaluated at a mean follow-up time of 38 months. Before reconstruction the mean ASES score was 35.3 and after surgical reconstruction the mean ASES score was 84.7. Additionally, the Visual Analog Scale (VAS) score decreased from an average of 7 preoperatively to a value of 1.2 postoperatively. In this cohort, 67% of patients reported stability considered good most of the time but with some limitations. Two patients had minor postoperative complications.
Recently, Lacheta et al,68 published five-year outcome data from their case series of 22 patients who underwent a figure-8 SCJ reconstruction utilizing a hamstring autograft. They reported 90% construct survivorship at minimum five years post-operatively, and of the patients that answered an optional sport questionnaire, 94% of them returned to their previous level of play.
It is worth mentioning that synthetic ligaments are being utilized in chronic SCJ reconstruction. In a recent case series, surgically stabilized SCJ’s using artificial weave ligaments revealed significant improvement at 29 months post-operatively and all patients returned to sport.57 No revisions were performed on any of the patients.57
Finally, there was a systematic review published by Willinger et al,69 which details the outcomes associated with reconstruction of anterior SCJ instability using a graft. This study included a review of 5 manuscripts compiling 80 patients. Of the cohort of patients 10% reported excellent outcomes, 89% reported good outcomes, and 1% reported fair outcomes. Ten percent reported recurrent instability and 5% required revision surgery. Overall, the rate of revision surgery was low and 10% reported recurrent instability, supporting that the use of autologous grafts in SCJ stabilization is reliable and safe for patients with chronic instability.
Novel Approaches
Because of the rare nature of the pathology and lack of long-term outcomes with a high volume of patients, there is no current consensus of best surgical technique for SCJ instability. For this reason, surgeons continue to create new techniques that aim to be technically reproducible, safe for the patient, and have excellent long-term outcomes. The following techniques from the last seven years add unique facets to the figure-8 technique.
Bak et al,70 created a suture anchor graft technique combining principles of the figure-8 described by Spencer and Kuhn51 as well as the non-augmented suture anchor technique from Abiddin et al.54 In their study, Bak et al,68 proposed a technique utilizing a self-tapping metallic anchor to be inserted at a 20-degree angle with the horizontal into the lateral aspect of the manubrium. Additionally, two holes were drilled into the oblique side of the clavicle entering on the medial clavicular articular facet and exiting through the anterior surface of the medial clavicle to allow for the suture passage (Figure 5B). The Western Ontario Shoulder Instability (WOSI) score, which is one of the most reliable patient-reported outcomes measures for SCJ instability, was used to evaluate instability preoperatively and postoperatively at a mean follow-up time of 55 months in 27 patients with anterior SCJ instability.71 The overall WOSI score improved from a mean value of 44% preoperatively to a mean value of 75% postoperatively. The suture anchor technique is proposed to be superior to that of the figure-8 approach due to the reduction of risk associated with drilling holes anterior to posterior through the manubrium. Some risk of posterior puncture remains with the anchor approach based on angle of placement and anatomy of the patient. Additionally, Bak et al,70 reported a concern regarding the age of the cohort of patients within their study: over half of the patients from the study were aged under 25. Because the medial epiphysis of the clavicle can remain open until age 26, there is a question of passage of an autograft through the medial clavicular epiphysis having deleterious long-term effects. Aside from the possible complications, Bak et al demonstrated an innovative anchoring strategy to avoid drilling holes posterior to the SCJ, while retaining the positive stabilizing result of the figure-8 reconstruction.
Guan et al,13 explored another innovative surgical technique, which aimed to avoid the risky dissection and drilling posterior to the manubrium. A similar infero-superior drilling technique has been in two studies utilizing sternocleidomastoid tendon for SCJ reconstruction.55,72 Unicortical drill holes were made 15 mm lateral to the SCJ on the clavicle and the sternum in the superior to inferior, and inferior to superior directions followed by connection of the tunnel using a curette. An autograft tendon (eg Gracilis, semitendinosus tendon, or palmaris longus) was passed through the bone tunnels of the clavicle and sternum in order to reconstruct the SCJ. The result of the reconstruction was a complete figure-8 component along with inferior and superior transverse graft supports, which combine to form a Roman numeral X configuration for the complete surgical reconstruction with the graft (Figure 5C). In the study, 6 patients underwent reconstruction with the Roman numeral X technique. All 6 patients reported symptomatic relief after surgery with full range of motion and all returned to activities they engaged in prior to SCJ instability. In addition, 5 patients reported a 0 out of 10 on the VAS pain score, while only 1 reported slight discomfort at a 1–3 out of 10 on the VAS pain score. One patient did return with recurrent pain at 4 years follow up and the reconstruction was revised with amelioration of pain after the revision. The study notes that the patient who experienced reconstructive failure at 4 years was the first patient on which the procedure was performed and the joint was reduced more than necessary causing posterior displacement of the medial clavicle. Through modifying the Spencer and Kuhn51 figure-8 technique via utilization of superior to inferior bone tunnels and fashioning the graft in a Roman numeral X pattern, equal or greater stabilization can be achieved with less risk to the patient.
Lastly, Sanchez-Sotelo et al,73 explored an innovative stabilization procedure while limiting exposure and risk to the patient. This study involved 15 patients and 16 unstable SC joints, as well as 3 others suffering from osteoarthritis. The 18 patients underwent reconstruction of the SCJ through a semitendinosus tendon allograft in a sternal docking configuration. The procedure entailed drilling two holes, one on the anterior, superior portion of the medial clavicle and one on the anterior, inferior portion of the medial clavicle, followed by removal of residual bone tissue in the canal with a curette until exiting out through the articular facet of the clavicle. Next an oblong hole was made into the sternal facet, as well as two holes on the anterior sternum inferiorly and superiorly. The semitendinosus tendon graft was then passed through both bone tunnels in the clavicle and simultaneously run through the bone tunnels on the sternum, followed by suturing the two ends of the graft together on the anterior portion of the sternum (Figure 5D). At a mean follow-up time of three years, 16/18 patients had resolution of their pain or instability.
A summary of the outcomes from all surgical approaches for SCJ reconstruction can be found in Table 1. Additionally, a flow chart depicting the different approaches to management of SCJ instability is shown in Figure 5.
 |
Table 1 Summary Of Surgical SCJ Repair Outcomes |
Conclusion
The diagnosis and management of SCJ instability remains challenging and without a true gold standard treatment algorithm. The techniques to reconstruct the SCJ are variable and may be partially due to provider preference for open or arthroscopic and allograft or autograft. Although the biomechanical strength of the figure-8 is superior, multiple groups have worked to determine the safest technique with regard to posterior structures while maintaining biomechanical stability.13,13,70,70,73,73 Long-term outcomes and multi-center studies are needed to determine whether these novel approaches result in improved patient outcomes after operative management of SCJ instability.
Disclosure
Dr. Brent Ponce reports personal fees from Wright Medical Inc, personal fees from ODi, personal fees from Mitek, personal fees from Stryker, outside the submitted work. Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connections with the submitted article. Additionally, there was no grant support or other funding methods associated with this article.
References
1. Iannotti JP, Williams GR. Disorders of the Shoulder: Diagnosis & Management. 1. Lippincott Williams & Wilkins; 2007.
2. Renfree KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003;22(2):219–237. doi:10.1016/S0278-5919(02)00104-7
3. Spencer EE, Kuhn JE, Huston LJ, Carpenter JE, Hughes RE. Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg. 2002;11(1):43–47. doi:10.1067/mse.2002.119394
4. Sewell MD, Al-Hadithy N, Le Leu A, Lambert SM. Instability of the sternoclavicular joint: current concepts in classification, treatment and outcomes. Bone Joint J. 2013;95-B(6):721–731. doi:10.1302/0301-620X.95B6.31064
5. Martetschlager F, Warth RJ, Millett PJ. Instability and degenerative arthritis of the sternoclavicular joint: a current concepts review. Am J Sports Med. 2014;42(4):999–1007. doi:10.1177/0363546513498990
6. Groh GI, Wirth MA. Management of traumatic sternoclavicular joint injuries. JAAOS. 2011;19(1):1–7. doi:10.5435/00124635-201101000-00001
7. Bae DS, Kocher MS, Waters PM, Micheli LM, Griffey M, Dichtel L. Chronic recurrent anterior sternoclavicular joint instability: results of surgical management. J Pediatr Orthop. 2006;26(1):71–74.
8. Morell DJ, Thyagarajan DS. Sternoclavicular joint dislocation and its management: A review of the literature. World J Orthop. 2016;7(4):244–250. doi:10.5312/wjo.v7.i4.244
9. Ponce BA, Kundukulam JA, Pflugner R, et al. Sternoclavicular joint surgery: how far does danger lurk below? J Shoulder Elbow Surg. 2013;22(7):993–999. doi:10.1016/j.jse.2012.10.037
10. Bearn J. Direct observations on the function of the capsule of the sternoclavicular joint in clavicular support. J Anat. 1967;101(Pt 1):159.
11. Bontempo NA, Mazzocca AD. Biomechanics and treatment of acromioclavicular and sternoclavicular joint injuries. Br J Sports Med. 2010;44(5):361–369. doi:10.1136/bjsm.2009.059295
12. Inman VT, Abbott LC. Observations of the function of the shoulder joint. Clin Orthopaedics Related Research®. 1996;330:3–12. doi:10.1097/00003086-199609000-00002
13. Guan JJ, Wolf BR. Reconstruction for anterior sternoclavicular joint dislocation and instability. J Shoulder Elbow Surg. 2013;22(6):775–781. doi:10.1016/j.jse.2012.07.009
14. Allman FL
15. Chaudhry FA, Killampalli VV, Chowdhry M, Holland P, Knebel R. Posterior dislocation of the sternoclavicular joint in a young rugby player. Acta Orthop Traumatol Turc. 2011;45(5):376–378. doi:10.3944/AOTT.2011.2359
16. Bicos J, Nicholson GP. Treatment and results of sternoclavicular joint injuries. Clin Sports Med. 2003;22(2):359–370. doi:10.1016/S0278-5919(02)00112-6
17. Chotai PN, Ebraheim NA. Posterior sternoclavicular dislocation presenting with upper-extremity deep vein thrombosis. Orthopedics. 2012;35(10):e1542e1547. doi:10.3928/01477447-20120919-27
18. Groh GI, Wirth MA, Rockwood CA
19. Waters PM, Bae DS, Kadiyala RK. Short-term outcomes after surgical treatment of traumatic posterior sternoclavicular fracture-dislocations in children and adolescents. J Pediatric Orthopaedics. 2003;23(4):464–469. doi:10.1097/01241398-200307000-00010
20. Eni-Olotu D, Hobbs N. Floating clavicle: simultaneous dislocation of both ends of the clavicle. Injury. 1997;28(4):319–320. doi:10.1016/S0020-1383(97)00009-0
21. El Mekkaoui M, Sekkach N, Bazeli A, Faustin J. Proximal clavicle physeal fracture-separation mimicking an anterior sterno-clavicular dislocation. Orthopaedics Traumatol. 2011;97(3):349–352.
22. Wirth MA, Rockwood CA
23. Carmichael KD, Longo A, Lick S, Swischuk L. Posterior sternoclavicular epiphyseal fracture-dislocation with delayed diagnosis. Skeletal Radiol. 2006;35(8):608–612. doi:10.1007/s00256-005-0076-y
24. Ono K, Inagawa H, Kiyota K, Terada T, Suzuki S, Maekawa K. Posterior dislocation of the sternoclavicular joint with obstruction of the innominate vein: case report. J Trauma Acute Care Surgery. 1998;44(2):381–383. doi:10.1097/00005373-199802000-00027
25. Van Holsbeeck M, Van Melkebeke J, Dequeker J, Pennes D. Radiographic findings of spontaneous subluxation of the sternoclavicular joint. Clin Rheumatol. 1992;11(3):376–381. doi:10.1007/BF02207196
26. Rajaratnam S, Kerins M, Apthorp L. Posterior dislocation of the sternoclavicular joint: a case report and review of the clinical anatomy of the region. Clin Anatomy. 2002;15(2):108–111. doi:10.1002/ca.1104
27. Franck WM, Siassi RM, Hennig F. Treatment of posterior epiphyseal disruption of the medial clavicle with a modified Balser plate. J Trauma Acute Care Surgery. 2003;55(5):966–968. doi:10.1097/01.TA.0000090756.65556.97
28. Asplund C, Pollard ME. Posterior sternoclavicular joint dislocation in a wrestler. Mil Med. 2004;169(2):134–136. doi:10.7205/MILMED.169.2.134
29. Salgado R, Ghysen D. Post-traumatic posterior sternoclavicular dislocation: case report and review of the literature. Emerg Radiol. 2002;9(6):323–325. doi:10.1007/s10140-002-0247-2
30. Allen JB, Zielinski C. Posterior fracture through the sternoclavicular physis associated with a clavicle fracture: a case report and literature review. Am j orthopedics. 1999;28(10):598–600.
31. Hidalgo Ovejero AM, Garcia Mata S, Sanchez Villares JJ, Martinez de Morentin J, Martinez Grande M. Posterior sternoclavicular dislocation. Report of two cases. Acta Orthop Belg. 2003;69(2):188–192.
32. Yeh GL, Williams GR
33. VAn TOnGEL A, McRae S, Gilhen A, LEiTER J, MACDOnALD P. Management of anterior sternoclavicular dislocation: a survey of orthopaedic surgeons. Acta Orthop Belg. 2012;78(2):164–169.
34. de Jong KP, Sukul DM. Anterior sternoclavicular dislocation: a long-term follow-up study. J Orthop Trauma. 1990;4(4):420–423. doi:10.1097/00005131-199012000-00010
35. Nettles JL, Linscheid RL. Sternoclavicular dislocations. J Trauma Acute Care Surgery. 1968;8(2):158–164. doi:10.1097/00005373-196803000-00004
36. Brinker MR, Bartz RL, Reardon PR, Reardon MJ. A method for open reduction and internal fixation of the unstable posterior sternoclavicular joint dislocation. J Orthop Trauma. 1997;11(5):378–381. doi:10.1097/00005131-199707000-00016
37. Stahel PF, Barlow B, Tepolt F, Mangan K, Mauffrey C. Safe surgical technique: reconstruction of the sternoclavicular joint for posttraumatic arthritis after posterior sternoclavicular dislocation. Patient Saf Surg. 2013;7(1):38. doi:10.1186/1754-9493-7-38
38. Worman L, Leagus C. Intrathoracic injury following retrosternal dislocation of the clavicle. J Trauma. 1967;7(3):416–423. doi:10.1097/00005373-196705000-00006
39. Thut D, Hergan D, Dukas A, Day M, Sherman OH. Sternoclavicular joint reconstruction. Bull NYU Hosp Jt Dis. 2011;69(2):128–135.
40. Deren ME, Behrens SB, Vopat BG, Blaine TA. Posterior sternoclavicular dislocations: a brief review and technique for closed management of a rare but serious injury. Orthop Rev. 2014;6:1. doi:10.4081/or.2014.5245
41. Shuler FD, Pappas N. Treatment of posterior sternoclavicular dislocation with locking plate osteosynthesis. Orthopedics. 2008;31(3):273. doi:10.3928/01477447-20080301-35
42. Quispe JC, Herbert B, Chadayammuri VP, et al. Transarticular plating for acute posterior sternoclavicular joint dislocations: a valid treatment option? Int Orthop. 2016;40(7):1503–1508. doi:10.1007/s00264-015-2952-y
43. Franck WM, Jannasch O, Siassi M, Hennig FF. Balser plate stabilization: an alternate therapy for traumatic sternoclavicular instability. J Shoulder Elbow Surgery. 2003;12(3):276–281. doi:10.1016/S1058-2746(02)86802-1
44. Tytherleigh-Strong G, Pecheva M, Titchener A. Treatment of first-time traumatic anterior dislocation of the sternoclavicular joint with surgical repair of the anterior capsule augmented with internal bracing. Orthopaedic j Sports Med. 2018;6(7):2325967118783717. doi:10.1177/2325967118783717
45. van Eck CF, Limpisvasti O, ElAttrache NS. Is there a role for internal bracing and repair of the anterior cruciate ligament? a systematic literature review. Am J Sports Med. 2018;46(9):2291–2298. doi:10.1177/0363546517717956
46. Scheiderer B, Imhoff FB, Kia C, et al. LUCL internal bracing restores posterolateral rotatory stability of the elbow. Knee Surg Sports Traumatol Arthrosc. 2019.
47. Ulku TK, Kocaoglu B, Tok O, Irgit K, Nalbantoglu U. Arthroscopic suture-tape internal bracing is safe as arthroscopic modified Brostrom repair in the treatment of chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2020;28(1):227–232. doi:10.1007/s00167-019-05552-w
48. Smolle-Juettner F, Hofer P, Pinter H, Friehs G, Szyskowitz R. Intracardiac malpositioning of a sternoclavicular fixation wire. J Orthop Trauma. 1992;6(1):102–105.
49. Clark R. Fatal aortic perforation and cardiac tamponade due to a Kirschner wire migrating from the right sternoclavicular joint. South Med J. 1974;67:316. doi:10.1097/00007611-197403000-00017
50. Thomas D, Williams P, Hoddinott H. A’safe’surgical technique for stabilisation of the sternoclavicular joint: a cadaveric and clinical study. Ann R Coll Surg Engl. 2000;82(6):432.
51. Spencer EE
52. Castropil W, Ramadan LB, Bitar AC, Schor B, de Oliveira D’Elia C. Sternoclavicular dislocation–reconstruction with semitendinosus tendon autograft: a case report. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):865–868. doi:10.1007/s00167-008-0527-9
53. Singer G, Ferlic P, Kraus T, Eberl R. Reconstruction of the sternoclavicular joint in active patients with the figure-of-eight technique using hamstrings. J Shoulder Elbow Surgery. 2013;22(1):64–69. doi:10.1016/j.jse.2012.02.009
54. Abiddin Z, Sinopidis C, Grocock C, Yin Q, Frostick S. Suture anchors for treatment of sternoclavicular joint instability. J Shoulder Elbow Surgery. 2006;15(3):315–318. doi:10.1016/j.jse.2005.07.005
55. Armstrong A, Dias J. Reconstruction for instability of the sternoclavicular joint using the tendon of the sternocleidomastoid muscle. J Bone Joint Surg Br. 2008;90(5):610–613. doi:10.1302/0301-620X.90B5.20293
56. Panzica M, Zeichen J, Hankemeier S, Gaulke R, Krettek C, Jagodzinski M. Long-term outcome after joint reconstruction or medial resection arthroplasty for anterior SCJ instability. Arch Orthop Trauma Surg. 2010;130(5):657–665. doi:10.1007/s00402-009-0911-z
57. Quayle JM, Arnander MW, Pennington RG, Rosell LP. Artificial ligament reconstruction of sternoclavicular joint instability: report of a novel surgical technique with early results. Tech Hand Up Extrem Surg. 2014;18(1):31–35. doi:10.1097/BTH.0000000000000027
58. Sabatini JB, Shung JR, Clay TB, Oladeji LO, Minnich DJ, Ponce BA. Outcomes of augmented allograft figure-of-eight sternoclavicular joint reconstruction. J Shoulder Elbow Surgery. 2015;24(6):902–907. doi:10.1016/j.jse.2014.10.001
59. Warth RJ, Lee JT, Campbell KJ, Millett PJ. Arthroscopic sternoclavicular joint resection arthroplasty: a technical note and illustrated case report. Arthroscopy Techniques. 2014;3(1):e165e173. doi:10.1016/j.eats.2013.09.019
60. Dekker TJ, Lacheta L, Goldenberg BT, Horan MP, Pogorzelski J, Millett PJ. Minimum 5-year outcomes and return to sports after resection arthroplasty for the treatment of Sternoclavicular Osteoarthritis. Am J Sports Med. 2020;48(3):715–722. doi:10.1177/0363546519897892
61. Katthagen JC, Tahal DS, Menge TJ, Horan MP, Millett PJ. Minimum 2-year outcomes and return to sport following resection arthroplasty for the treatment of sternoclavicular osteoarthritis. J Shoulder Elbow Surgery. 2017;26(2):e37e43. doi:10.1016/j.jse.2016.07.008
62. Rockwood CA
63. Tavakkolizadeh A, Hales PF, Janes GC. Arthroscopic excision of sternoclavicular joint. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):405–408. doi:10.1007/s00167-008-0692-x
64. Pingsmann A, Patsalis T, Michiels I. Resection arthroplasty of the sternoclavicular joint for the treatment of primary degenerative sternoclavicular arthritis. J Bone Joint Surg Br. 2002;84(4):513–517. doi:10.1302/0301-620X.84B4.0840513
65. Burrows HJ. Tenodesis of subclavius in the treatment of recurrent dislocation of the sterno-clavicular joint. J Bone Joint Surg Br. 1951;33(2):240–243. doi:10.1302/0301-620X.33B2.240
66. Martetschläger F, Reifenschneider F, Fischer N, et al. Sternoclavicular joint reconstruction fracture risk is reduced with straight drill tunnels and optimized with tendon graft suture augmentation. Orthop J Sports Med. 2019;7(4):2325967119838265. doi:10.1177/2325967119838265
67. Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American shoulder and elbow surgeons score, simple shoulder test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(1):144–148. doi:10.1016/j.jse.2016.06.007
68. Lacheta L, Dekker TJ, Goldenberg BT, et al. Minimum 5-year clinical outcomes, survivorship, and return to sports after hamstring tendon autograft reconstruction for sternoclavicular joint instability. Am J Sports Med. 2020;48(4):939–946. doi:10.1177/0363546519900896
69. Willinger L, Schanda J, Herbst E, Imhoff AB, Martetschläger F. Outcomes and complications following graft reconstruction for anterior sternoclavicular joint instability. Knee Surg Sports Traumatol Arthrosc. 2016;24(12):3863–3869. doi:10.1007/s00167-015-3770-x
70. Bak K, Fogh K. Reconstruction of the chronic anterior unstable sternoclavicular joint using a tendon autograft: medium-term to long-term follow-up results. J Shoulder Elbow Surg. 2014;23(2):245–250. doi:10.1016/j.jse.2013.05.010
71. Plancher KD, Lipnick SL. Analysis of evidence-based medicine for shoulder instability. Arthroscopy. 2009;25(8):897–908. doi:10.1016/j.arthro.2009.03.017
72. Uri O, Barmpagiannis K, Higgs D, Falworth M, Alexander S, Lambert SM. Clinical outcome after reconstruction for sternoclavicular joint instability using a sternocleidomastoid tendon graft. J Bone Joint Surg Am. 2014;96(5):417–422. doi:10.2106/JBJS.M.00681
73. Sanchez-Sotelo J, Baghdadi Y, Nguyen NTV. Sternoclavicular joint allograft reconstruction using the sternal docking technique. JSES Open Access. 2018;2(4):190–193. doi:10.1016/j.jses.2018.08.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.