Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Stereotactic Accelerated Partial Breast Irradiation Using CyberKnife with Non-Invasive Skin Fiducial Marker Tracking in Early-Stage Breast Cancer: A Retrospective Study of Feasibility, Dosimetry, and Early Outcomes
Authors Wei CW ![]() , Cheng MC, Yeh HL
, Cheng MC, Yeh HL
Received 22 July 2025
Accepted for publication 23 October 2025
Published 29 October 2025 Volume 2025:17 Pages 997—1004
DOI https://doi.org/10.2147/BCTT.S555446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Chiao-Wen Wei,1 Mei-Chun Cheng,2 Hui-Ling Yeh1
1Department of Radiation Oncology, Taichung Veterans General Hospital, Taichung, Taiwan; 2Division of Medical Physics, Department of Radiation Oncology, Taichung Veterans General Hospital, Taichung, Taiwan
Correspondence: Hui-Ling Yeh, Department of Radiation Oncology, Taichung Veterans General Hospital, Taichung, Taiwan, Email [email protected]
Purpose: This study aimed to evaluate the feasibility, dosimetric characteristics, and early clinical outcomes of CyberKnife (CK)-based accelerated partial breast irradiation (APBI) using non-invasive skin fiducial marker tracking in an Asian population.
Materials and Methods: We retrospectively analyzed 74 female patients diagnosed with early-stage breast cancer who underwent APBI using the CK system between May 2019 and December 2024. Patient selection was based on the modified 2017 American Society for Radiation Oncology (ASTRO) consensus criteria. The total tumor doses were 30 Gy in 5 consecutive daily fractions. Non-invasive skin fiducial markers were used for respiratory motion tracking. Dosimetric parameters were recorded according to European Society for Radiotherapy and Oncology (ESTRO) and Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) recommendations. Primary clinical outcomes, acute and chronic toxicities were evaluated during a median follow-up period of 26.5 months. Predictive factors for toxicity were assessed using receiver operating characteristic (ROC) curve analysis.
Results: A total of 74 patients having a median age of 56 years were included in the study, with a median follow-up period of 26.5 months. Non-invasive skin fiducial markers demonstrated a strong correlation with internal surgical clips, validating their accuracy for motion tracking. The median conformity and homogeneity indexes were 1.15 and 1.20, respectively. Median mean heart doses were 1 Gy (left-sided) and 0.5 Gy (right-sided), while the ipsilateral lung mean dose was 2.34 Gy. Two patients (2.7%) developed ipsilateral breast tumor recurrence. There were no grade ≥ 2 toxicities or cardiopulmonary events observed. Radiation dermatitis represented the most common acute toxicity (48.6%), whereas breast fibrosis was the most frequent late toxicity (12.2%). Skin D0.03cc > 29.45 Gy and PTV-to-breast volume ratio > 14.5% were associated with grade 1 dermatitis, while a breast volume < 455.2 cm3 and PTV-to-breast volume ratio > 28.9% were predictive of breast fibrosis.
Conclusion: By retrospective reviewing, APBI using the CyberKnife system with non-invasive skin fiducial marker tracking is a safe, precise, and effective treatment option for early-stage breast cancer. Although this retrospective study with limited follow-up demonstrated favorable dosimetric outcomes and minimal acute toxicity, further prospective studies with larger cohorts and longer observation are needed to validate these findings.
Keywords: early breast cancer, cyberknife, accelerated partial breast irradiation, skin fiducial marker
Introduction
Breast cancer is the most commonly diagnosed malignancy amongst Taiwanese women and ranked fourth in cancer-related mortality in 2023. Advances in both imaging and diagnostic technologies have significantly improved the detection rate of early-stage breast cancer, contributing to an increasing number of patients eligible for breast-conserving surgery (BCS).
Postoperative whole-breast irradiation (WBI) has long been considered the standard of care following BCS. According to the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-17 trial, postoperative whole-breast irradiation reduces the risk of ipsilateral breast tumor recurrence (IBTR) by more than 50%.1 However, conventional WBI typically requires daily treatments over a period of 4 to 6 weeks, posing a burden for patients with geographic, occupational, or social barriers to undergo prolonged therapy.
Recently, accelerated partial breast irradiation (APBI) has emerged as a viable alternative for selected patients with low-risk early-stage breast cancer. APBI can be performed by either brachytherapy or external beam irradiation. The Florence trial demonstrated that external beam APBI using intensity-modulated radiotherapy (IMRT) in five once-daily fractions yielded comparable 10-year ipsilateral breast tumor recurrence rates to treatment involving whole breast irradiation, with reduced toxicity and improved cosmetic outcomes.2
CyberKnife (CK) is a form of stereotactic body radiotherapy (SBRT), which allows for a highly conformal delivery of radiation doses to the target with submillimeter precision and real-time motion tracking. A retrospective analysis of early-stage breast cancer treated with adjuvant stereotactic partial breast irradiation reported excellent disease control, favorable cosmetic outcomes, and minimal toxicity with CK treatment.3 Other studies in Western populations have also shown promising results using CK-based APBI in terms of both efficacy and toxicity.4–6 Typically, gold fiducials are commonly used for intra-fraction motion tracking.5,7–9 However, invasive fiducial implantation may be less acceptable or technically feasible in certain populations, including Asian women with smaller breast volumes.10,11 In this context, skin fiducial markers offer a non-invasive alternative for motion tracking during CK treatment. However, the use of skin fiducial markers presents unique challenges. Their reproducibility during treatment and their ability to accurately represent the tumor bed position must be carefully validated. Moreover, it remains critical to determine whether these external markers can be reliably detected by the CyberKnife imaging system and used by the Synchrony® respiratory tracking platform to correlate thoracic motion with tumor bed displacement. Despite the growing adoption of CK-based APBI in Western countries, its use remains limited in Taiwan. This retrospective study aims to report our institutional experience with APBI using CyberKnife. We evaluated treatment feasibility, dosimetric parameters, early clinical outcomes, and potential predictors of toxicity, before discussing the implications of this technique in an Asian population.
Materials and Methods
Patient Selection
This retrospective single-institution study included 74 female patients who underwent APBI using CyberKnife following breast-conserving surgery between the period of May 2019 and December 2024. Patient selection was based on the modified 2017 American Society for Radiation Oncology (ASTRO) consensus criteria.12 Eligible patients were over 45 years of age, diagnosed with ductal carcinoma in situ (DCIS) with tumor size <2.5 cm or invasive carcinoma (T1-T2) with tumor size <3 cm, had an estrogen receptor-positive status, were margin free (>2mm for invasive tumor and >3 mm for DCIS) and had a low to intermediate nuclear grade. Exclusion criteria included multifocal tumors, positive surgical margins, lymph node involvement, distant metastasis, or absence of surgical clips. Histopathological data, including tumor subtype, pathological size, lymphovascular invasion (LVI), perineural invasion (PNI), nodal status, and margin status, were all extracted from pathology reports. Treatment records were reviewed to document adjuvant therapies. Cancer staging was performed according to the 8th edition of the American Joint Committee on Cancer (AJCC). This retrospective study was approved by the Institutional Review Board of Taichung Veterans General Hospital (IRB No.: CE25198A). Patient consent was waived due to the retrospective design of the study. All data were obtained from the hospital’s legal biodatabase, which provided de-identified records to ensure patient confidentiality. The study was conducted in compliance with the Declaration of Helsinki.
Fiducial Placement and Simulation
APBI was initiated 4–6 weeks postoperatively after adequate wound healing. Patients were positioned supine with the ipsilateral arm raised and then immobilized using a customized vacuum bag. Scout images at 0° and 90° were obtained to guide the placement of five to six skin fiducial markers (SureMark™ SL-20). The distance from each fiducial to the tumor bed was measured on these images to ensure placement within 5 cm. If a fiducial exceeded this distance, it was repositioned and the scout images were re-acquired. Additional scout images at both 45° and 315° were used for verification. CT simulation was performed under expiration breath-hold with a 1.25 mm slice thickness, as recommended by the manufacturer, to optimize visualization of fiducial markers. Patients were instructed to breathe normally during treatment, while the Synchrony® image tracking system continuously monitored skin fiducial positions to compensate for respiratory motion. For the first 18 patients, both inspiratory and expiratory CT scans were acquired in order to evaluate the motion of the skin fiducials and internal surgical clips. The target centers of the skin fiducials and internal clips were calculated, and the correlation between their displacements was assessed.
Treatment Planning
Gross tumor volume (GTV) was defined as the tumor bed according to surgical clips, seroma and postoperative changes. Based on the ASTRO guideline for partial breast irradiation,13 the clinical target volume (CTV) is generally contoured with a 1–1.5 cm margin around the GTV, with adjustments to respect anatomical boundaries. In our protocol, a 1.5–2 cm margin extension from GTV in all directions was performed, with the posterior margin limited by the ribs and the anterior margin limited by 4 mm from the skin surface, so as to generate the CTV. The planning target volume (PTV) is 5mm extension of CTV except 3mm with limitations on the ribs and the skin. The radiation doses were delivered with the CyberKnife M6 system using the InCise2™ multileaf collimator. The prescribed dose was 30 Gy in 5 consecutive daily fractions.14 Treatment plans were created using the MultiPlan® v5.3.0 system and the finite-size pencil beam (FSPB) algorithm. The Synchrony® respiratory tracking system was used for real-time tumor motion compensation. Dose constraints followed modified QUANTEC criteria and the AAPM Task Group 101 recommendations: PTV coverage ≥95% of the prescription dose; D0.03cc of PTV <39 Gy; ipsilateral breast V15Gy <40%, V30Gy <20%; contralateral breast V1Gy <7%; ipsilateral lung V9Gy <10%; contralateral lung V1.5Gy <10%; heart V1.5Gy <40%; D0.03cc for skin and ribs <33 Gy.15–18
Dosimetric Evaluation
Dosimetric quality was assessed according to ESTRO recommendations. Parameters included ipsilateral breast V50%, mean heart dose, heart V1.5Gy, ipsilateral lung V9Gy, contralateral lung V1.5Gy, skin D0.03cc, and rib D0.03cc. The new conformity index (nCI) was defined as nCI = Prescription isodose volume (PIV) / [Tumor isodose volume (TIV) * Coverage]. The homogeneity index (HI) was defined as HI = Maximum dose/ Prescription dose.
Follow-Up and Toxicity Evaluation
The patients were followed up at 2 weeks, 3 months, and every 6 months thereafter. Toxicities were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) v4.0. Clinical evaluations and annual imaging studies, including mammography and ultrasonography, were all performed. Cardiovascular events were also reviewed from medical records.
Statistical Analysis
Numerical data were summarized as median with interquartile range (IQR). Kaplan–Meier analysis was used to estimate local recurrence-free survival (LRFS) and overall survival (OS). Candidate dosimetric and anatomical parameters were selected a priori based on clinical relevance and biological plausibility. For example, for radiation dermatitis, variables related to skin exposure and breast size (eg, breast volume, PTV-to-breast volume ratio, and skin D0.03cc) were considered, while for fibrosis, parameters reflecting irradiated breast volume were prioritized. Parameters without clinical justification (eg, heart or lung dose for dermatitis) were not included. Due to small sample size, receiver operating characteristic (ROC) curve analyses were performed and using its AUC to predict probabilities derived from logistic regression models. Optimal cut-off values were determined by maximizing the Youden index (sensitivity + specificity − 1). Statistical significance was defined as p < 0.05. All analyses were performed using SPSS version 22.0 (IBM Corp).
Results
A total of 74 patients having a median age of 56 years were included, with a median follow-up of 26.5 months. Most tumors were invasive ductal carcinoma, staged as Tis or T1–T2N0 with a luminal subtype. Lymphovascular invasion and perineural invasion were absent in 93% and 90.1% of patients, respectively. The majority (93.2%) received adjuvant hormonal therapy. The characteristics of the patients are described in detail in Table 1.
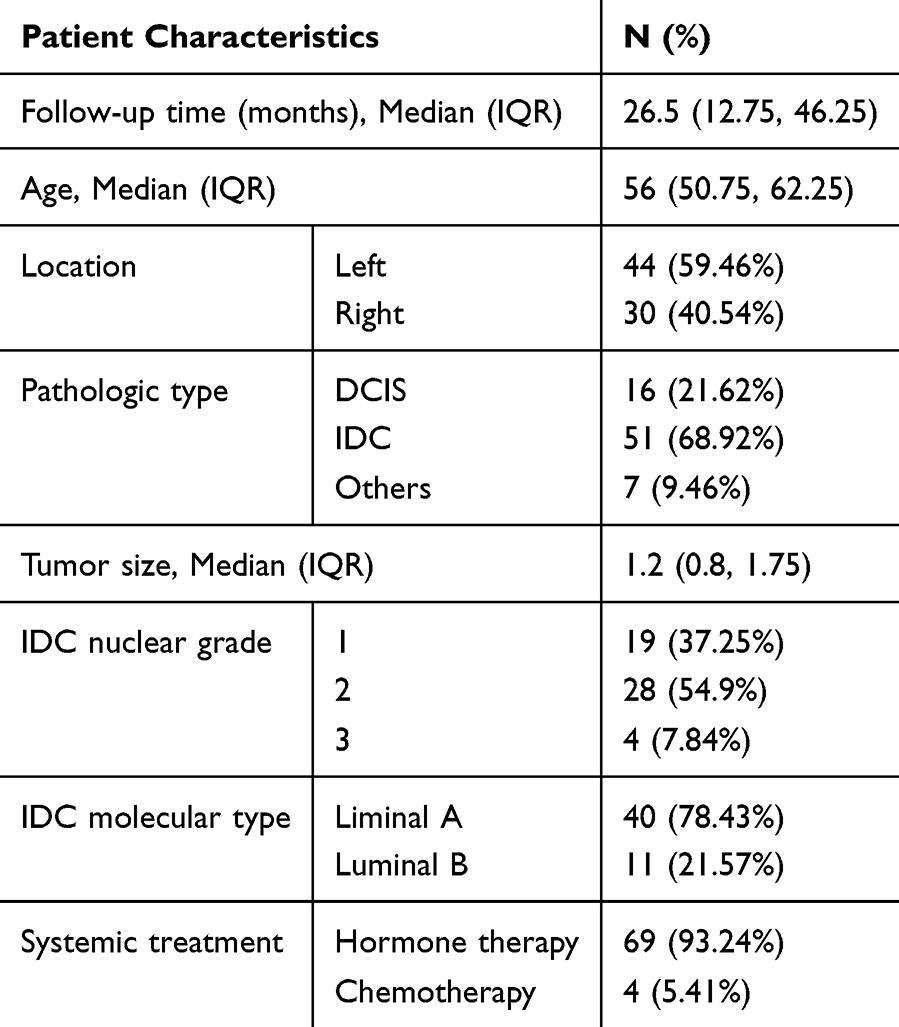 |
Table 1 Patient Characteristics (n=74) |
In the first 18 patients, respiratory-phase CT scans demonstrated a strong correlation between the target centers of skin fiducials and surgical clips, confirming skin fiducial reliability. Median motion between inspiratory and expiratory phases was 0 mm (X-axis), 2.5 mm (Y-axis), and 3.3 mm (Z-axis) for skin fiducials; and −0.4 mm, 0.7 mm, and 2.8 mm respectively for clips. The median displacement between fiducials and clips in the expiratory phase was minimal (X: 0 mm, Y: −0.5 mm, Z: 0 mm), with the correlation coefficient being close to 1. The details are presented in Table 2. The median PTV was 78.98 cm3; median ipsilateral breast volume was 485.35 cm3, with a median PTV-to-breast volume ratio of 18.96%. The median ipsilateral breast V50% was 17.15%. Regarding OARs, the median heart dose was 1 Gy for left-sided and 0.5 Gy for right-sided cancers. Median heart V1.5Gy was 18.95% (left) and 1.70% (right). Ipsilateral lung mean dose was 2.34 Gy, and V9Gy was 4.55%. Skin and rib D0.03cc were 29.07 Gy and 29.98 Gy, respectively. Plan quality metrics showed a median nCI of 1.15 and an HI of 1.20. Details regarding dosimetry characteristics are provided in Table 3.
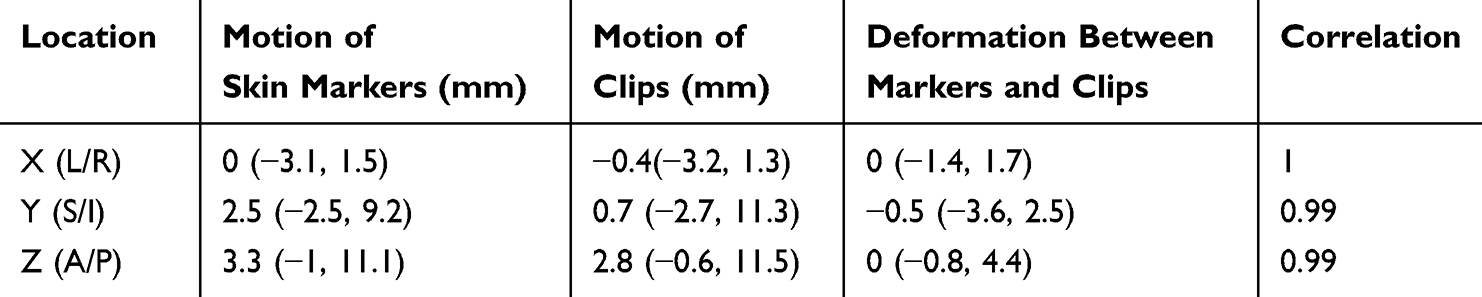 |
Table 2 The Motion of Surgical Clips and Skin Markers in Breast Cancer |
 |
Table 3 Dosimetry Characteristics |
Two patients experienced ipsilateral breast tumor recurrence after 16 months and 46 months of follow-up, respectively. One of these patients experienced an out-field recurrence and received salvage surgery with simple mastectomy, with the state of her disease currently being stable The other one was an in-field recurrence; however, the patient was later lost to follow-up after the diagnosis was confirmed. No deaths from breast cancer or cardiac disease occurred during follow-up. At the median follow-up time of 26.5 months (IQR: 12.75–46.25), the IBTR rate was 2.7%. Radiation dermatitis was the most common acute toxicity (36 patients, 48.65%), all grade 1. Grade 1 fibrosis occurred in 9 patients (12.16%), while fat necrosis and telangiectasia each being seen in 1 patient (1.35%). No grade ≥2 toxicities, pneumonitis, or cardiovascular events were observed. Logistic regression identified skin D0.03cc and PTV-to-breast volume ratio as significantly associated with grade 1 dermatitis, while breast volume and PTV-to-breast volume ratio were significantly associated with grade 1 fibrosis. ROC analysis is shown in Figure 1 and identifies skin D0.03cc >29.45 Gy (AUC = 0.711, p < 0.001) and PTV-to-breast volume ratio >14.5% (AUC = 0.653, p = 0.02) as predictors of grade 1 dermatitis. Similarly, a breast volume <455.2 cm3 (AUC = 0.728, p = 0.007) and PTV-to-breast volume ratio >28.9% (AUC = 0.713, p = 0.039) were both associated with grade 1 fibrosis. The optimal thresholds, derived by maximizing the Youden index were used to define the cut-offs reported above. Sensitivity and specificity were moderate: skin D0.03cc >29.45 Gy (55.56%, 78.59%), PTV/breast >14.5% (83.33%, 50%), breast volume <455.2 cm3 (77.78%, 61.54%), and PTV/breast >28.9% (44.44%, 93.85%).
 |
Figure 1 Sensitivity and specificity between dosimetry and adverse events. (A) ROC curve for sensitivity and specificity between skin D0.03cc and dermatitis (B) ROC curve for sensitivity and specificity between PTV/breast volume ratio and dermatitis (C) ROC curve for sensitivity and specificity between ipsilateral breast volume and fibrosis (D) ROC curve for sensitivity and specificity between PTV/breast volume ratio and fibrosis. |
Discussion
This study demonstrates that APBI using the CyberKnife system with skin fiducial tracking is a feasible and well-tolerated treatment modality for early-stage breast cancer. The observed clinical outcomes and dosimetric parameters suggest that this approach can deliver highly conformal radiation with minimal toxicity. Our findings show a high treatment plan quality, with a median nCI of 1.15 and a HI of 1.20. These values are comparable to those reported in previous studies, such as the ACCEL trial,19 which conducted APBI by a five-field inverse-planned IMRT, and reported a median conformity index of 1.1.
For the dose constraint of OAR, the IMPORT-HIGH trial documented a median mean lung dose of 5.3 Gy, and median mean heart doses of 2.5 Gy for left-sided and 1.1 Gy for right-sided breast cancer.20 Compared to WBI delivered in the prone position with 5000 cGy in 25 fractions,21 APBI using CK in our study also resulted in lower mean lung and heart doses. Additionally, the mean heart dose in our cohort was lower (1 Gy for left-sided cancers) than that reported for hypofractionated whole-breast irradiation,22 supporting the dosimetric advantage of CK-based APBI in reducing cardiac exposure. We also reviewed other APBI techniques. Compared to invasive approaches such as multicatheter interstitial brachytherapy (MIBT), CK-based APBI offers a non-invasive alternative while maintaining low radiation doses to the OARs. In our previous study, an HI of 0.73 and CI of 0.88 for MIBT were reported, with a mean heart dose of 1.06 Gy and an ipsilateral lung dose of 1.57 Gy.23 In our APBI study involving CK, the corresponding values were comparable or better without the need for catheter implantation.
Our results are consistent with international studies taken from institutions in New York, Hungary, and Korea,3,7,9 demonstrating similar dosimetric outcomes and toxicity profiles. The retrospective study conducted in New York reported a median mean lung dose of 3.3 Gy and median mean heart dose of 1.3 Gy for left-sided and 1.1 Gy for right-sided breast cancer. In our study, we achieved comparable or more favorable dose constraints. Notably, while the study conducted in Hungary employed a lower total dose of 25 Gy in 4 fractions and reported favorable dosimetry, our protocol of 30 Gy in 5 fractions achieved comparable results.
To the best of our knowledge, this is one of the first clinical studies to evaluate the use of non-invasive skin fiducial markers for respiratory motion tracking in CyberKnife-based APBI. In contrast to invasive fiducials, which may be difficult to place in patients with smaller breast volumes, skin fiducial markers offer a non-invasive, patient-friendly alternative. The strong correlation observed between skin fiducial markers and internal surgical clips from our study suggests that surface tracking may be sufficient for accurate target localization in this population. This approach simplifies treatment preparation, reduces procedural risks, and enhances overall treatment experience. Given the limited prior evidence, our study provides early validation for the use of skin fiducial markers in breast SBRT and may support a broader adoption of non-invasive tracking in clinical practice.
The incidence of acute toxicities in our study was low and mostly limited to grade 1 events. No grade ≥2 toxicities or cardiopulmonary complications were observed. ROC analysis revealed that higher skin D0.03cc (>29.45 Gy) and PTV-to-breast volume ratio (>14.5%) were predictive of grade 1 dermatitis. Similarly, smaller breast volume (<455.2 cm3) and a higher PTV-to-breast volume ratio (>28.9%) were both associated with grade 1 fibrosis. Since these thresholds demonstrated only moderate sensitivity and specificity, validation in larger cohorts will be necessary before definitive clinical implementation.
Limitations within this study include its retrospective nature, single-institution setting, relatively small sample size, and limited follow-up period. Furthermore, only low-risk patients were included. Prospective studies with larger cohorts and longer follow-up periods remain warranted in order to confirm these preliminary findings.
Conclusions
In conclusion, APBI using the CyberKnife system with skin fiducial marker tracking is a precise, non-invasive, and effective treatment option for selected patients with early-stage breast cancer. It provides excellent target conformity and homogeneity while minimizing radiation exposure to surrounding normal tissues. Acute toxicities were minimal and predictable based upon dosimetric parameters. Nevertheless, this study is limited by its retrospective design, modest sample size, and intermediate follow-up period. Moreover, while the ROC-derived thresholds for predicting toxicity are novel, they should be regarded as preliminary and require validation in larger datasets. Further prospective studies involving larger cohorts and extended follow-up periods are still warranted to help better validate these findings and establish long-term safety and efficacy protocols.
Acknowledgment
The authors would like to thank the Biostatistics Task Force of Taichung Veterans General Hospital for their statistical assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wapnir IL, Dignam JJ, Fisher B, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103(6):478–488. doi:10.1093/jnci/djr027
2. Meattini I, Marrazzo L, Saieva C, et al. Accelerated partial-breast irradiation compared with whole-breast irradiation for early breast cancer: long-term results of the randomized Phase III APBI-IMRT-florence trial. J Clin Oncol. 2020;38(35):4175–4183. doi:10.1200/JCO.20.00650
3. Jaysing A, Lischalk JW, Sanchez A, et al. Robotic stereotactic body radiation therapy for the adjuvant treatment of early-stage breast cancer: outcomes of a large single-institution study. Adv Radiat Oncol. 2022;8(2):101095. doi:10.1016/j.adro.2022.101095
4. Haas JA, Witten MR, Cotrutz C, et al. Stereotactic body radiation therapy for early-stage breast cancer using a robotic linear accelerator. Int J Radiat Oncol Biol Phys. 2017;99(2):S7. doi:10.1016/j.ijrobp.2017.06.033
5. Obayomi-Davies O, Kole TP, Oppong B, et al. Stereotactic accelerated partial breast irradiation for early-stage breast cancer: rationale, feasibility, and early experience using the cyberknife radiosurgery delivery platform. Front Oncol. 2016;6:129. doi:10.3389/fonc.2016.00129
6. Rahimi A, Thomas K, Spangler A, et al. Preliminary results of a Phase 1 dose-escalation trial for early-stage breast cancer using 5-fraction stereotactic body radiation therapy for partial-breast irradiation. Int J Radiat Oncol Biol Phys. 2017;98(1):196–205.e2. doi:10.1016/j.ijrobp.2017.01.020
7. Lee WH, Chang JS, Kim MJ, et al. First experience in Korea of stereotactic partial breast irradiation for low-risk early-stage breast cancer. Front Oncol. 2020;10:672. doi:10.3389/fonc.2020.00672
8. Lozza L, Fariselli L, Sandri M, et al. Partial breast irradiation with CyberKnife after breast conserving surgery: a pilot study in early breast cancer. Radiat Oncol. 2018;13(1):49. doi:10.1186/s13014-018-0991-4
9. Mészáros N, Smanykó V, Major T, et al. Implementation of stereotactic accelerated partial breast irradiation using cyber-knife - technical considerations and early experiences of a Phase II clinical study. Pathol Oncol Res. 2020;26(4):2307–2313. doi:10.1007/s12253-020-00821-3
10. Maskarinec G, Meng L, Ursin G. Ethnic differences in mammographic densities. Int J Epidemiol. 2001;30(5):959–965. Erratum in: Int J Epidemiol. 2003 Jun;32(3):479. doi:10.1093/ije/30.5.959
11. Maskarinec G, Lyu LC, Meng L, Theriault A, Ursin G. Determinants of mammographic densities among women of Asian, Native Hawaiian, and Caucasian ancestry. Ethn Dis. 2001;11(1):44–50.
12. Correa C, Harris EE, Leonardi MC, et al. Accelerated partial breast irradiation: executive summary for the update of an ASTRO evidence-based consensus statement. Practical Radiation Oncol. 2017;7(2):73–79. ISSN 1879-8500. doi:10.1016/j.prro.2016.09.007
13. Shaitelman SF, Anderson BM, Arthur DW, et al. Partial breast irradiation for patients with early-stage invasive breast cancer or ductal carcinoma in situ: an ASTRO clinical practice guideline. Pract Radiat Oncol. 2024;14(2):112–132. Erratum in: Pract Radiat Oncol. 2024 Nov-Dec;14(6):613. doi: 10.1016/j.prro.2024.06.011. doi:10.1016/j.prro.2023.11.001
14. Viani GA, Arruda CV, Faustino AC, De Fendi LI. Partial-breast irradiation versus whole-breast radiotherapy for early breast cancer: a systematic review and update meta-analysis. Brachytherapy. 2020;19(4):491–498. doi:10.1016/j.brachy.2020.03.003
15. Vicini FA, Cecchini RS, White JR, et al. Long-term primary results of accelerated partial breast irradiation after breast-conserving surgery for early-stage breast cancer: a randomised, Phase 3, equivalence trial. Lancet. 2019;394(10215):2155–2164. doi:10.1016/S0140-6736(19)32514-0
16. Emami B. Tolerance of normal tissue to therapeutic radiation. Rep Radiother Oncol. 2013;1:123–127.
17. Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: the report of AAPM task group 101. Med Phys. 2010;37(8):4078–4101. doi:10.1118/1.3438081
18. Vermeulen S, Cotrutz C, Morris A, et al. Accelerated partial breast irradiation: using the cyberknife as the radiation delivery platform in the treatment of early breast cancer. Front Oncol. 2011;1:43. doi:10.3389/fonc.2011.00043
19. Quirk S, Grendarova P, Craighead P, et al. Results of the ACCEL trial: dosimetry in accelerated partial breast irradiation. Radiother Oncol. 2020;147:50–55. doi:10.1016/j.radonc.2020.03.004
20. IMPORT Trial Management Group; Coles CE, Haviland JS, Kirby AM, et al. Dose-escalated simultaneous integrated boost radiotherapy in early breast cancer (IMPORT HIGH): a multicentre, phase 3, non-inferiority, open-label, randomised controlled trial. Lancet. 2023;401(10394):2124–2137. doi:10.1016/S0140-6736(23)00619-0
21. Gao Y, Wang L, Bai H, et al. Comparative analysis of dosimetry and predictive somatotype parameters of prone and supine whole-breast irradiation among Chinese women after breast-conserving surgery. Front Oncol. 2022;12:1011805. doi:10.3389/fonc.2022.1011805
22. Chhatui B, Roy N, Chakrabarty S, et al. An observational study comparing the dosimetry and clinical effects of conventional versus hypofractionated radiotherapy in elderly patients of early breast cancer. J Cancer Res Ther. 2025;21(1):118–123. doi:10.4103/jcrt.jcrt_2491_23
23. Cheng HS, Hung CC, Wang KC, Tsai IC, Lin JF, Yeh HL. Preliminary outcomes of accelerated partial breast irradiation by interstitial multicatheter brachytherapy with intraoperative free-hand catheter implantation in early breast cancer. J Chin Med Assoc. 2023;86(4):381–387. doi:10.1097/JCMA.0000000000000893
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.