Back to Journals » Patient Preference and Adherence » Volume 19
Status and Influencing Factors of Dyadic Appraisals Differences Between Patients with COPD and Their Spousal Caregivers
Authors Xu J ![]() , Chang M, Chen H, Chen L, Luo T, Cheng X
, Chang M, Chen H, Chen L, Luo T, Cheng X
Received 13 August 2025
Accepted for publication 26 November 2025
Published 5 December 2025 Volume 2025:19 Pages 3901—3912
DOI https://doi.org/10.2147/PPA.S560407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Jing Xu,1,2 Mengting Chang,1,2 Hongxin Chen,1 Lixia Chen,2 Tiantian Luo,2 Xirong Cheng2
1School of Nursing, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2Department of Nursing, The Second Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xirong Cheng, Department of Nursing, The Second Affiliated Hospital of Nanjing University of Chinese Medicine, 23 Nanhu Road, Jianye District, Nanjing, Jiangsu, 210017, People’s Republic of China, Tel +15365150199, Email [email protected]
Background: The dyadic management of COPD and the dyadic health status are profoundly affected by the dyadic appraisals of disease symptoms between patients and their caregivers. However, existing research has not adequately explored the discrepancies in these dyadic appraisals or their underlying determinants.
Methods: A cross-sectional study was conducted between February and March 2025 using convenience sampling. A total of 142 pairs of clinically stable patients with COPD and their spousal caregivers were recruited from the Department of Pulmonary Diseases at a tertiary Grade A hospital of traditional Chinese medicine in Jiangsu Province. Data were collected using the Memorial Symptom Assessment Scale, Mutuality Scale, Social Support Rating Scale, Self-Concealment Scale, and a general information questionnaire. SPSS 26.0 was used for data analysis, and linear regression was employed to identify the factors influencing the differences in symptom appraisal.
Results: High consistency was observed in the appraisals of physical symptom subscale score, total MSAS score, and global distress index by patients with COPD and their caregivers. However, the patients’ score was higher than their caregivers’ score as it came to the appraisals of psychological symptoms (patients’ score: median, 0.33 [IQR, 0.00– 0.50]; caregivers’ score: median, 0.17 [IQR, 0.00– 0.44]; P< 0.001). Regression analysis indicated that the factors impacting the differences in psychological symptom appraisal were the patients’ gender, the degree of self-concealment, the caregivers’ social support, and their mutuality.
Conclusion: To decrease differences in the appraisal of psychological symptoms between the two parties and to advance the practice and development of the COPD care model, healthcare professionals should focus on the way patients and caregivers share about psychological states and fortify the structure of the caregiver support system.
Keywords: chronic obstructive pulmonary disease, disease symptom, dyadic appraisals
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a major global health crisis, with rising incidence and mortality. Its global prevalence among adults aged 40 and above is 10%-15%, reaching 13.7% in China.1 COPD causes substantial health and economic burdens.2,3 As there is no cure, clinical management focuses on comprehensive strategies to improve prognosis by reducing acute exacerbations and enhancing quality of life.4
With the gradual formation of the rehabilitation service model in China, where “patients receive treatment in hospitals during the acute stage and return to the community for recovery”, chronic disease patients usually return to the community and their families to receive long-term management after their conditions stabilize.5 Among them, the spouse, as the main caregiver and emotional supporter of the patient, spends more time with the patient and can help the patient better manage the disease by monitoring, identifying changes in the condition and symptom severity. However, as the disease progresses, patients’ declining self-care capacity makes symptom identification increasingly challenging, leading to greater dependence on their spouses. Given the progressive and unpredictable nature of COPD, home care requirements demonstrate long-term dynamic changes. Consequently, spousal caregivers must maintain constant vigilance regarding symptom fluctuations and continuously adapt care strategies to address the disease’s evolving manifestations. This cumulative burden generates significant physical and psychological stress for spousal caregivers, which in turn impacts the physical and mental states of the patients they care for.6 Lyons et al termed these interdependent patient-caregiver relationships during illness as “dyads”.7 Given that similar interdependence exists between patients with COPD and their spousal caregivers, it is imperative to conceptualize them as an integrated dyadic unit and focus on their collaborative disease assessment and management.
Within the Dyadic Illness Management theory, dyadic appraisal serves as a fundamental foundation and prerequisite for effectively improving dyadic management and enhancing dyadic health outcomes. This is because patients-caregivers dyads must first conduct dyadic appraisals of disease-related issues such as symptoms, then collaborate on disease management based on both parties’ needs, ultimately achieving dyadic health. This implies that the smaller the appraisal discrepancy, the more it facilitates collaborative disease coping and promotes dyadic health.7 However, current research demonstrates that differences in dyadic appraisals represent a prevalent phenomenon in chronic disease management, influenced by individual, dyadic, and sociocultural factors. For example, in chronic heart failure dyads, Ren et al found that older, less educated female caregivers tended to overestimate the severity of patients’ psychological symptoms and heart failure-specific symptoms.8 On the contrary, Zhang et al found that factors such as patient self-concealment and caregiver fatigue can lead caregivers to underestimate the severity of patients’ psychological symptoms.9 Such appraisal differences have been shown to adversely affect disease management by creating conflicts in care goals and problem-solving approaches between patients and caregivers. These conflicts ultimately reduce treatment adherence, increase caregiver burden, and compromise dyadic health outcomes.10
Despite the well-documented significance of dyadic appraisals, current COPD research remains predominantly focused on unilateral perspectives, including patients’ symptom experiences, patient-reported outcomes, etc.11,12 These studies consistently overlook the critical dimension of shared symptom appraisal between patients and caregivers. Lü et al shifted their focus to the dyadic system comprising patients with COPD and their spousal caregivers. Their investigation revealed that the dyadic coping abilities within these pairs were at a moderate yet overall negative level, which was influenced by the patients’ self-efficacy, anxiety, depression, comorbidities, marital length, and dyspnea severity. However, their study assessed dyadic coping levels solely through the Dyadic Coping Inventory completed by patients alone. Furthermore, the influencing factors examined—such as patient self-efficacy and anxiety—were confined to the patient level, failing to incorporate any caregiver-related variables.13 In contrast to the study by Lü et al, which primarily focused on dyadic coping levels, we will further explore dyadic appraisal differences between patients and caregivers. In terms of measurement, both patients and caregivers will independently complete the Memorial Symptom Assessment Scale, Mutuality Scale, Social Support Rating Scale, and Self-Concealment Scale to obtain perspectives from both parties. Furthermore, regarding the influencing factors, our investigation will explore variables across patient, caregiver, and dyadic levels to provide a basis for multidimensional improvement of COPD-related dyadic appraisal differences.
Methods
Design
This cross-sectional study was conducted in the Department of Pulmonary Diseases at a tertiary Grade A hospital of traditional Chinese medicine in Jiangsu Province from February to March 2025. Dyads were consecutively recruited during their routine clinic visits or hospitalization. A dyad was defined as a married couple in which one spouse was diagnosed with COPD and the other served as the primary unpaid caregiver. After obtaining written informed consent, both patients and caregivers were invited to separate rooms to independently complete the Memorial Symptom Assessment Scale, Mutuality Scale, Social Support Rating Scale, Self-Concealment Scale, and a general information questionnaire. The data collection process was carried out by trained researchers, who distributed the questionnaires, provided instructions, and collected them upon completion.
Participants, Sampling Method, and Sample Size
Using the convenience sampling method, patients who received treatment in the Pulmonary Disease Department of a tertiary grade A hospital in Jiangsu Province from February 2025 to March 2025 and whose conditions were stable, as well as their spousal caregivers, were selected as the research subjects. Inclusion criteria for patients: (1) ≥ 65 years old; (2) married and living with their spouses; (3) diagnosed with COPD, with pulmonary function at levels II to IV; (4) clear consciousness, no cognitive impairment, no communication disorders; (5) free from other terminal diseases (such as malignant tumors, etc); (6) informed consent. Inclusion criteria for caregivers: (1) ≥ 18 years old; (2) marital relationship with the patient; (3) living together with the patient; (4) undertaking most of the patient’s care tasks without compensation; (5) informed consent. According to the rough sample size calculation formula,14 taking the number of independent variables multiplied by 5 to 10, this study expected to include 25 variables, considering a 10% inefficiency rate, the required sample size is at least 139 pairs.
Measurement
General Information Questionnaire
Structured questionnaire, including age, gender, educational level, etc. The general information form for caregivers includes age, gender, caregiving duration, etc.
Memorial Symptom Assessment Scale
Using the revised Chinese version by Cheng et al.15 The symptoms that occurred in the patients within the past week were evaluated. The Chinese version has demonstrated good psychometric properties, including good construct validity (as confirmed by confirmatory factor analysis), content validity (CVI=0.94), and high internal consistency (Cronbach’s α= 0.79–0.87).15 This 32-item scale assesses symptom burden and yields four summary scores. For each symptom, patients report its presence and, if present, rate its frequency, severity, and distress over the past week. The total MSAS score (TMSAS) is the average of all 32 symptom scores. Additionally, subscale scores are calculated from specific subsets of these items: the physical symptom subscale score (PHYS) is the average of 12 designated physical symptoms, and the psychological symptom subscale score (PSYCH) is the average of 6 designated psychological symptoms. The global distress index (GDI) is derived from the average of 4 psychological symptoms and the distress frequency of 6 physical symptoms. Across all scores, higher values represent a greater symptom burden. If a symptom is absent, the score for that symptom and its dimensions is 0. In this study, the MSAS was completed by patients (self-report) and their caregivers (proxy-report). The use of the MSAS for caregiver proxy-rating is an established approach. The psychometric properties (eg reliability and validity) of the caregiver-rated version have been previously documented, and its scoring protocol follows that of the original patient scale.16,17 For this study, the Cronbach’s α coefficients of this scale when applied to patients and caregivers were 0.712 and 0.745, respectively, as shown in Supplementary Table 1.
Mutuality Scale
Using the revised Chinese version by Liu.18 This scale is employed to assess the mutuality between patients and caregivers. The Chinese version has demonstrated excellent reliability and validity, with a high internal consistency (Cronbach’s α=0.951) and a content validity index of 0.91, as established in a validation study.18,19 The scale consists of 4 dimensions: love and affection, pleasurable activities, shared values, and reciprocity, with a total of 15 items. Each item is scored on a 5-point Likert scale, with a total score ranging from 0 to 60. A higher score indicates a better interdependence. In this study, the Cronbach’s α coefficients of this scale when applied to patients and caregivers were 0.907 and 0.859, respectively, as shown in Supplementary Table 1.
Social Support Rating Scale
Using the version compiled by Xiao.20 This scale is used to assess the social support that individuals have obtained. The scale demonstrated sound psychometric properties, including high internal consistency (α=0.896) and construct validity evidenced by its factor correlations.20,21 This scale consists of three dimensions: objective support, subjective support, and support utilization, with a total of 10 items. The scoring method is the sum of the 10 items, with a total score ranging from 12 to 66. A higher score indicates more support received. In this study, the Cronbach’s α coefficients of this scale when applied to patients and caregivers were 0.873 and 0.814, respectively, as shown in Supplementary Table 1.
Self-Concealment Scale
Using the revised Chinese version by Wang.22 This scale is used to assess the psychological tendency of individuals to actively conceal information. The scale demonstrated good psychometric properties, with confirmed construct validity and high internal consistency (Cronbach’s α =0.80).22,23 This scale is a single dimension, consisting of 10 items. Each item uses the Likert 5-point rating method, with a total score ranging from 10 to 50. The higher the score, the greater the degree of self-concealment of the individual. In this study, the Cronbach’s α coefficients of this scale when applied to patients and caregivers were 0.864 and 0.857, respectively, as shown in Supplementary Table 1.
Ethical Considerations
This study does not involve any clinical trials or animal experiments. It has been approved by the Ethical Committee of the Second Affiliated Hospital of Nanjing University of Chinese Medicine (2025SEZKY-012-01), and all operations strictly comply with the Declaration of Helsinki. All participants provided anonymous written informed consent, and they could choose to withdraw from the study at any time during the investigation without any consequences. The data in this study were securely stored.
Data Collection
Before the research began, permission was obtained from the hospital administrators. Two researchers who had received unified training were responsible for conducting the survey. After the patients gave their informed consent, they were arranged to fill out the questionnaire in separate rooms, without interfering with each other. For those who were unable to complete it independently, standard instructions were used to assist them in completing the questionnaire. The content was objectively recorded, and the questionnaire was filled out and collected on the spot.
Data Processing
During the data collection process, we ensured that all questionnaires were fully returned. For the Memorial Symptom Assessment Scale, we found that some patients and caregivers did not make choices for certain symptom items. Specifically, this occurred in 7 out of 142 patient self-reports and 9 out of 142 caregiver proxy-reports. After review, these unanswered items were concentrated among patients with stable conditions, and there was no regularity. Therefore, we assumed them to be completely random missing (Missing Completely at Random, MCAR). Based on clinical reasoning and questionnaire design, we inferred that when participants did not report a certain symptom, it indicated that they believed this symptom did not occur or cause any trouble during the assessment period. Thus, during the data coding stage, we assigned these unanswered MSAS items a value of “0”. After the above processing, all key analysis variables in this study had no missing data, and the complete data were used for statistical analysis.
Data Analysis
The primary objective of this study is to quantify the extent and direction of differences in symptom appraisals within patient-caregiver dyads. The difference score (patient score minus caregiver score) was selected as it most directly and intuitively captures this construct. A positive score indicates a higher patient appraisal, a negative score indicates a higher caregiver appraisal, and zero indicates agreement. This approach is consistent with prior research, ensuring comparability.8,9 Regarding dyadic interdependence, we conceptually treat the difference score as a dyad-level variable. By combining the two interdependent ratings (from the patient and the caregiver) into a single score representing each pair, our unit of analysis has shifted to the dyad. Thus, by shifting the unit of analysis to the dyad, the issue of dyadic interdependence is addressed. The data were analyzed using SPSS 26.0. Descriptive statistics were used to summarize the participants’ demographic characteristics and the Memorial Symptom Assessment Scale scores. Specifically, categorical data were presented as frequencies (percentages). Continuous data were tested for normality; those conforming to a normal distribution were described using the mean and standard deviation, while those not conforming were described using the median and interquartile range. Since the difference scores for the Physical Symptom subscale, Psychological Symptom subscale, Total MSAS score, and Global Distress Index were not normally distributed, the Wilcoxon signed-rank test was employed to explore whether the differences in assessments between patients and caregivers in these four areas were statistically significant. To address the potential inflation of Type I error due to these multiple comparisons, the significance level for the four symptom domain comparisons will be adjusted using the Bonferroni method, with a corrected threshold of P<0.0125 (0.05/4). Non-parametric tests (the Mann–Whitney U-test for dichotomous variables and the Kruskal–Wallis H-test for multi-categorical variables) were used to explore whether the differences in symptom assessments among patients and caregivers with different demographic characteristics were statistically significant. When a Kruskal–Wallis H-test yielded a significant result, post-hoc pairwise comparisons were conducted using the Dunn-Bonferroni test to identify which specific groups differed. Correlation analysis was performed using Pearson correlation analysis, and multivariate analysis was conducted using multiple linear stepwise regression. The variable entry criterion was set at P ≤ 0.05 for the F-statistic, and the removal criterion was set at P ≥ 0.10. Multicollinearity was assessed (with Variance Inflation Factor, VIF <5 considered acceptable), and linearity and residual assumptions were verified. Effect sizes and 95% confidence intervals are reported.
Results
Participant Characteristics
During the data collection period, a total of 170 patient-caregiver dyads were initially approached and assessed for eligibility. Among them, 22 dyads did not meet the inclusion criteria. This left 148 dyads who were confirmed eligible to participate. The research purpose and procedure were explained to all eligible dyads. However, 6 dyads declined to participate. The primary reasons given for non-participation included being too tired after the clinic visit (n=4), lack of interest in the research (n=1), and privacy concerns (n=1). Thus, 142 dyads agreed to participate and completed the questionnaires. All 142 completed sets of questionnaires were included in the final analysis, resulting in a participation rate of 95.9% (142 out of 148 eligible dyads). The age of patients with COPD ranged from 62 to 82 years, with a mean of 75.63 (SD = 4.40), including 42 females and 100 males. The age of spousal caregivers ranged from 58 to 80 years, with a mean of 72.68 (SD = 4.75), and included 100 females and 42 males. More detailed information is provided in Table 1.
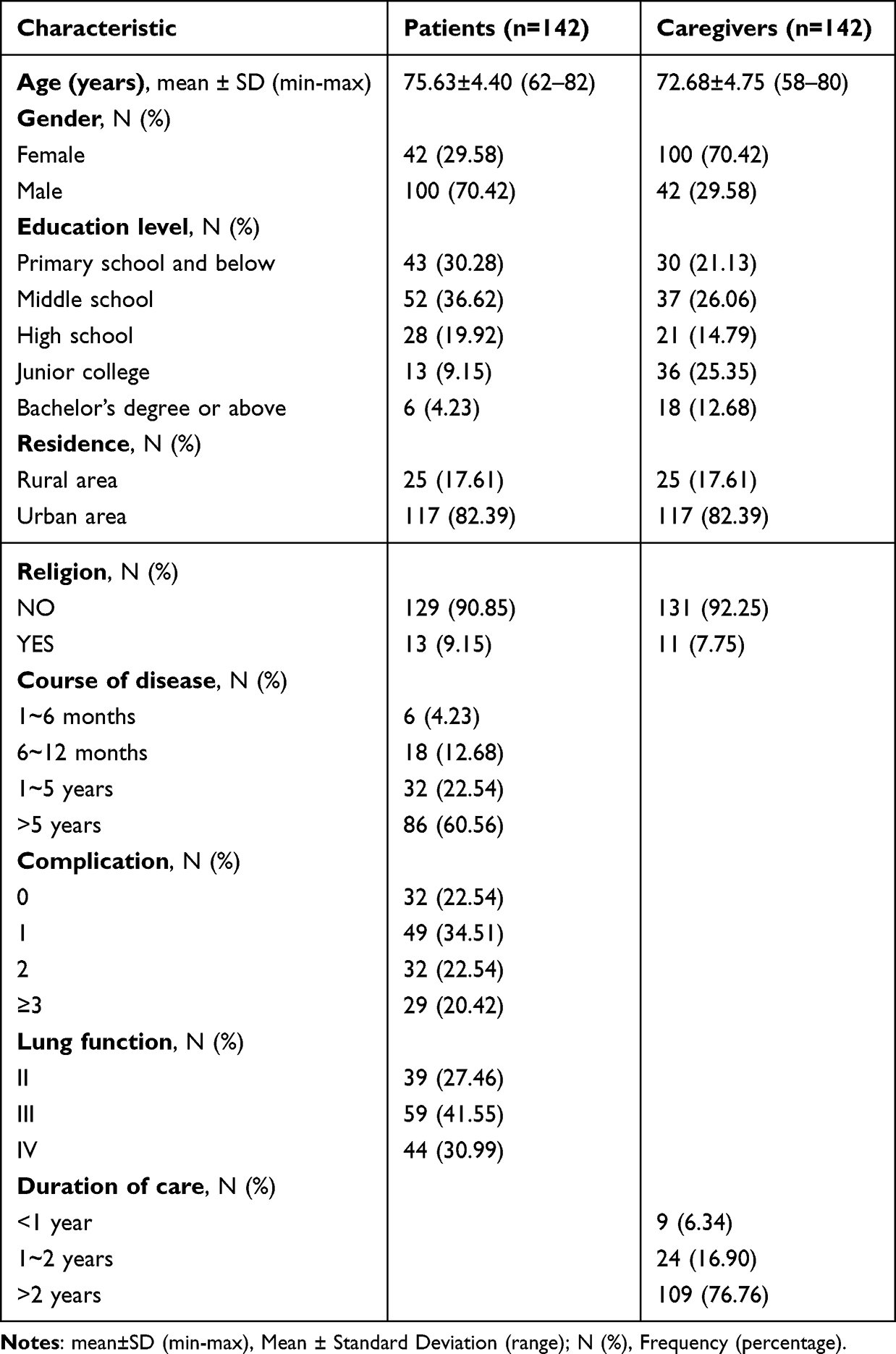 |
Table 1 Characteristics of Patients with COPD and Their Spousal Caregivers (n=142) |
The Differences in the Dyadic Appraisals of Disease Symptoms by Patients with COPD and Their Caregivers
In line with our statistical plan to adjust for multiple comparisons, the significance level was set at P<0.0125. At this corrected threshold, the dyadic appraisals congruence between the patients and their caregivers was relatively high in terms of physical symptom subscale score (PHYS), total MSAS score (TMSAS), and global distress index (GDI). However, there was a significant difference in terms of psychological symptom subscale score (PSYCH) (P<0.001), and the caregivers’ scores were significantly lower than those of the patients, as shown in Table 2.
 |
Table 2 Results of the Dyadic Appraisals Differences of Disease Symptoms Between Patients with COPD and Their Caregivers (n=142) |
Univariate Analysis of Differences in Psychological Symptom Appraisals
The gender of the patients and caregivers, as well as the educational level of the caregivers, can affect the differences in the dyadic appraisals of psychological symptoms, and these differences are statistically significant (all P<0.05), as shown in Supplementary Table 2.
Correlation Analysis of Differences and Interrelationships in Psychological Symptom Evaluations, Self-Concealment, and Social Support
The differences in the appraisals of psychological symptoms among patients with COPD and their caregivers were negatively correlated with the scores of mutuality and the scores of caregivers’ social support (r=−0.633, r=−0.632), and positively correlated with the score of patients’ self-concealment (r=0.582), all with P<0.001.
Multivariate Analysis of Differences in Psychological Symptom Appraisals
We conducted a multiple stepwise linear regression analysis to investigate the factors influencing the differences in psychological symptom appraisal between patients with COPD and their caregivers. The dependent variable was the appraisal difference, and the independent variables included statistically significant variables from the univariate analysis, as well as scores from both patients and caregivers on self-concealment, mutuality, and social support. The criteria for variable entry and removal were set at P ≤ 0.05 and P ≥ 0.10, respectively. After controlling for the competing effects of other variables, the final model identified four independent predictors, which entered the model in the following order: mutuality, level of social support for caregivers, patient’s self-concealment, and patient gender. The R2 value of 0.508 indicates that the independent variables explain 50.8% of the variance in the dependent variable. The adjusted R2 of 0.493 demonstrates that the model robustly accounts for 49.3% of the total variance, indicating good explanatory power. Model diagnostics showed that all Variance Inflation Factor (VIF) values ranged between 1.472 and 2.487, all below 2.5, suggesting no severe multicollinearity. The overall regression model was significant (F(4, 137)=35.340, P<0.001), supporting the assumption of a linear relationship among the variables. The standardized residuals ranged from −3.79 to 2.89, largely consistent with the normality assumption. In summary, the model diagnostics were satisfactory. The results indicate that patient gender, self-concealment, mutuality, and level of social support for caregivers are influential factors in the discrepancy of psychological symptom appraisals, as shown in Table 3.
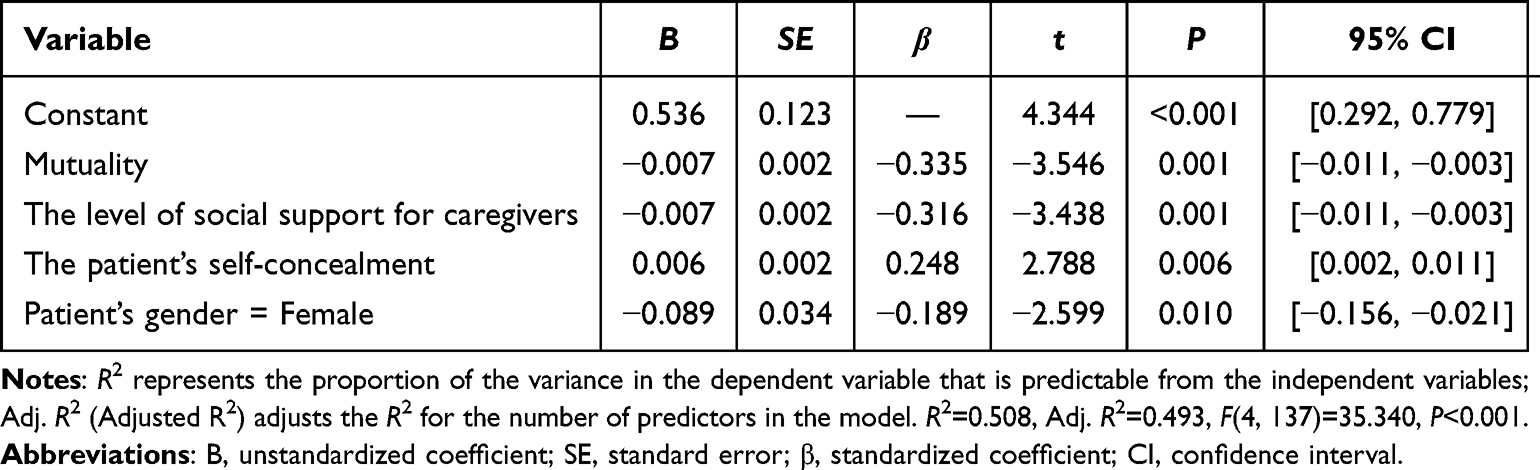 |
Table 3 Multiple Regression Analysis of Differences in Psychological Symptom Appraisals Between Patients with COPD and Their Spousal Caregivers |
Discussion
This study revealed that while symptom appraisal within COPD dyads was highly consistent in terms of the Physical Symptom Subscale (PHYS), the Total MSAS score (TMSAS), and the Global Distress Index (GDI), a notable divergence was observed specifically for the Psychological Symptom Subscale (PSYCH). These differences were influenced by patient gender, mutuality, self-concealment, and the social support level of their spousal caregivers. Therefore, healthcare providers should pay particular attention to female patients with COPD, those with high levels of self-concealment, caregivers with low social support levels, and COPD dyads with poor mutuality.
The Dyadic Appraisal Outcomes of Disease Symptoms Between Patients with COPD and Their Spousal Caregivers
The results demonstrated significant concordance (P > 0.05) in symptom evaluations between patients with COPD and their spousal caregivers regarding physical symptom subscale score, total MSAS score, and global distress index. This finding differs from studies on patients with intractable epilepsy or aphasia, disease-specific factors such as loss of consciousness or communication deficits can mask underlying physiological symptoms and hinder accurate caregiver assessment.24,25 In contrast, the physiological symptoms of COPD, such as coughing, expectoration, and shortness of breath, are more overt, making it easier for caregivers to effectively monitor changes in patients’ symptoms and functional decline through daily care activities. These findings suggest that the outcomes of dyadic appraisals may be related to disease characteristics. Consequently, when cognitive impairment or advanced disease limits the reliability of self-report in patients with COPD, caregiver assessments serve as vital complementary data for clinical decision-making and disease management.
Significant discrepancies (P<0.001) were observed in terms of psychological symptom subscale score between patients with COPD and their spousal caregivers, with caregivers rating symptoms as less severe than patients. This contrasts with the findings of studies on the late-stage cancer dyad, where caregivers are typically more sensitive to the psychological distress of the patients.26 This difference may stem from a plausible explanation that psychological symptoms such as depression and sadness in patients with COPD are often highly subjective and concealed. They can also be prone to overlap with the physiological manifestations of the disease, which may make it more difficult for non-professionals to identify them.27 Furthermore, at present, the management system for COPD in China typically prioritizes physical health over mental health. There is a lack of systematic training for caregivers in identifying psychological symptoms, and such teams usually consist of respiratory doctors, community doctors, and nurses, without including psychological experts. This may further exacerbate the challenge of identifying such psychological symptoms.28
Influencing Factors of Psychological Symptom Appraisal Differences in patients with COPD and Their Spousal Caregivers
First, female gender was significantly associated with larger assessment differences (B=−0.089, 95% CI [−0.156, −0.021], P=0.010). This may be related to traditional gender role differences: Male caregivers may have received less training during socialization to express or respond to emotional needs, which could lead to identity dilemmas when they assume the role of a caregiver, causing resistance and hindering their active participation in emotional interactions and the recognition of emotions.29 This may lead female patients to seek emotional resonance from same-sex partners rather than their spouses,30 potentially widening the assessment gap between them.
Second, poorer mutuality was significantly correlated with larger appraisal differences (B=−0.007, 95% CI [−0.011, −0.003], P=0.001). In the context of family planning policies and population aging in China, spouses have become the main caregivers for patients with chronic disease. In this social context, the quality of marital relationships is of crucial importance.31 As an important bond for maintaining the emotional relationship and happiness between spouses, good mutuality can promote effective communication and trust-building between spouses, thereby enhancing the empathetic ability of caregivers and their enthusiasm for participating in the patient’s health management, and strengthening the patient’s willingness to disclose symptoms and confidence in disease management.32–34 This may help caregivers to better identify the patient’s psychological experiences.
Third, a higher level of patient self-concealment was associated with larger appraisal differences (B=0.006, 95% CI [0.002, 0.011], P=0.006). Patients may conceal psychological distress due to cultural values emphasizing self-reliance or to avoid burdening caregivers.35,36 Additionally, the inherent characteristics of COPD itself heighten patients’ motivation for self-concealment. On one hand, the chronic nature of COPD often leads patients to perceive themselves as distinct from healthy individuals.37 Consequently, to preserve their self-image, they frequently choose to hide negative emotions; On the other hand, patients with COPD often delay seeking medical care due to psychosocial factors like illness denial and stigma. Caregivers, however, are more inclined to seek timely treatment out of concern for worsening conditions.6 This discrepancy may prompt patients to conceal psychological distress to avoid triggering greater pressure or conflict around medical care. However, while this protective buffering behavior may be motivated in part by good intentions, it can undermine effective communication. Not only can this hinder caregivers from recognizing the true extent of the patient’s suffering, but it may also exacerbate the patient’s own negative emotions, such as anxiety and depression. Ultimately, this risks creating a vicious cycle of “symptom aggravation - coping failure - psychological exhaustion”.38
Finally, a significant negative correlation was found between caregivers’ social support levels and appraisal differences (B=−0.007, 95% CI [−0.011, −0.003], P=0.001). In the context of the rapid social transformation in China, elderly care institutions and community services are facing challenges such as a shortage of beds and insufficient professional strength, which has led to the shift of out-of-hospital care focus for patients with COPD to their families.39,40 Additionally, the long-term care insurance pilot programs in China mainly cover the patients themselves, and the direct support for family caregivers is limited. There are also problems such as a single payment method and insufficient coverage, making it difficult to fully meet the diverse needs of caregivers. In this context, caregivers with insufficient support are more vulnerable to social isolation and multiple burdens. This may lead to feelings of social isolation and burnout, thereby diminishing their enthusiasm and capacity for caregiving and reducing their sensitivity to the emotional state of patients.41–43 At the same time, caregivers lacking sufficient support are prone to simply attribute patients’ emotional changes, such as anxiety and sadness, to “normal reactions to disease stress”, further exacerbating the differences in psychological symptom evaluations between the two parties.
Clinical Implications and Recommendations
Based on these findings, we consolidate the following practical recommendations for clinicians and caregivers. Based on the high congruence in physical symptom appraisals, healthcare providers should collaborate with patients with COPD and their caregivers to engage in advance care planning, ensuring that patient treatment preferences are respected during periods of decisional incapacity. To reduce differences in psychological symptom appraisals, we recommend encouraging patient emotional expression while training caregivers in recognition and intervention techniques. The integration of Artificial Intelligence (AI)-enabled wearable technologies and Internet of Things (IoT)-based platforms can provide objective, continuous monitoring of affective states and physiological parameters, delivering real-time alerts to facilitate timely interventions.44 Furthermore, dyad-centered interventions, such as reminiscence therapy, shared priority alignment using tools like iSCIP, and emotion expression training, can enhance mutuality and improve relationship quality. Cognitive behavioral therapy and COPD support groups can also be used to address patients’ motivations for self-concealment. These approaches can be supplemented with virtual reality (VR)-based scenarios to practice effective communication, encouraging patients to disclose their condition and thereby reducing the extent of self-concealment. Simultaneously, community and institutional efforts should challenge gendered care norms through public education and simulated training, fostering male caregiver engagement. Finally, strengthening professional care institutions and expanding welfare policies are essential to provide comprehensive social support for family caregivers.
Strengths & Contributions
This study makes several important contributions to the dual care of COPD. Previous research, such as that by Lü et al,13 has examined the dyadic coping of COPD from the patient’s perspective. Our study, however, provides a more nuanced understanding by shifting the focus to differences in dyadic symptom appraisal. The primary advantage stems from our overcoming the limitation of relying solely on patient self-reports. By having both patients and caregivers independently complete the same questionnaire, we achieved independent data collection across multiple dimensions from both perspectives, including physical symptom subscale scores, psychological symptom subscale scores, total MSAS scores, and global distress indices. This provides a genuine dyadic perspective, contrasting with studies that depend on reports from a single information provider. Additionally, by integrating the Theory of Dyadic Illness Management, we identified three levels of influencing factors: patients with COPD (gender, self-concealment), spousal caregivers (social support), and dyadic (mutuality) levels. This provides a more comprehensive, multi-level framework for understanding and ultimately reducing differences in psychological symptom appraisal among dyads. This multidimensional approach offers clearer evidence for designing targeted, dyad-centered interventions.
Limitations
We acknowledge that this study has certain limitations. Firstly, due to time and resource constraints, we selected patients from only one comprehensive hospital in China for the investigation. Therefore, the conclusions of this study may not apply to all patients with COPD and their spouses in all regions. In the future, we plan to increase the sample size and include samples from multiple centers, cities, and various medical institutions. Secondly, the interpretation of the results by gender, mutuality, the degree of patient self-concealment, and the level of social support of caregivers accounted for only 49.3%, and the cross-sectional design of this study implies that we can only establish correlations but cannot infer causal relationships, indicating that there may be other influencing factors that have not been discovered. Finally, this study concentrated solely on their spousal caregivers; it failed to look at other caregivers, like parents or siblings. Therefore, in the future, qualitative research should be combined with quantitative research to comprehensively explore the influencing factors of the differences in symptom appraisals of patients with COPD and their caregivers, and to explore targeted measures to reduce the differences in symptom appraisals of COPD dyads, improving the management effect and quality of life of the COPD dyads.
Conclusion
This study revealed a significant difference in symptom appraisals between patients with COPD and their spousal caregivers. While they demonstrated alignment in their assessments of the physical symptom subscale score, total MSAS score, and global distress index, a significant difference was observed in the psychological symptom subscale score, wherein caregivers tended to underestimate the patients’ level of distress. This difference was closely associated with the patient gender, degree of self-concealment, mutuality, and the level of social support of the caregivers. These findings suggest that the management of COPD should not be confined to a patient-centric model but should focus on dyad-centered interventions that address these specific individual, dyadic, and social factors to enhance the congruence of their symptom appraisals.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding authors (Xirong Cheng) upon reasonable request.
Ethics Statement
The study has been approved by the Ethical Committee of the Second Affiliated Hospital of Nanjing University of Chinese Medicine (2025SEZKY-012-01), and all operations strictly comply with the Declaration of Helsinki.
Funding
This study was supported by the Key Laboratory of Geriatric Long-term Care (Naval Medical University), Ministry of Education (LNYBPY-2023-21), and the Jiangsu Provincial Fourth Phase Priority Academic Program Development Fund (The Open Research Project of Nanjing University of Chinese Medicine Nursing Discipline) (YSHL202510), High-Level Traditional Chinese Medicine Key Discipline of Nursing, State Administration of Traditional Chinese Medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chronic Obstructive Pulmonary Disease Group of Chinese Thoracic Society, Chronic Obstructive Pulmonary Disease Working Committee of Chinese Association of Chest Physicians. Guidelines for the diagnosis and management of chronic obstructive pulmonary disease (2021 update). Chin J Tuberc Respir Dis. 2021;44(3):170–205. doi:10.3760/cma.j.cn112147-20210109-00031
2. Cai L, Wang XM, Liu L, Zhao Y, Golden AR. Socioeconomic differentials of trends in the prevalence and economic burden of chronic obstructive pulmonary disease in rural southwest China. BMC Public Health. 2023;23(1):141. doi:10.1186/s12889-023-15096-x
3. Yin P, Wu J, Wang L, et al. The burden of COPD in China and its provinces: findings from the global burden of disease study 2019. Front Public Health. 2022;10:859499. doi:10.3389/fpubh.2022.859499
4. Expert Consensus Writing Group of Integrated Traditional Chinese and Western Medicine Management for Chronic Obstructive Pulmonary Disease. Expert consensus on integrated traditional Chinese and western medicine management for chronic obstructive pulmonary disease (2023 edition). Chin Gen Pract. 2023;26(35):4359–4371. doi:10.12114/j.issn.1007-9572.2023.0348
5. Chen XF, Li SQ, Hu D, Gao SH, Chen JY, Zhang CY. Competence of community-based rehabilitative service among rural doctors in China. Chin Gen Pract. 2025;28(19):2384–2389, 2397. doi:10.12114/j.issn.1007-9572.2023.0816
6. Suresh M, Young J, Fan V, et al. Caregiver experiences and roles in care seeking during COPD exacerbations: a qualitative study. Ann Behav Med. 2022;56(3):257–269. doi:10.1093/abm/kaab045
7. Lyons KS, Lee CS. The theory of dyadic illness management. J Fam Nurs. 2018;24(1):8–28. doi:10.1177/1074840717745669
8. Ren J, Pan H, Zhang Z, Wang Y. Status quo and factors influencing dyadic disease appraisal in chronic heart failure based on latent profile analysis in Northern Sichuan Province, China. BMC. 2024;23(1):680. doi:10.1186/s12912-024-02340-x
9. Zhang H, Lu LJ, Cheng ZR, Luo X, Zhang ZM, Zhang J. Status and influencing factors of dyadic appraisals congruence between patients with chronic heart failure and their caregivers. Chin Nurs Manag. 2024;24(3):356–361. doi:10.3969/j.issn.1672-1756.2024.03.008
10. Buck HG, Kitko L, Hupcey JE. Dyadic heart failure care types: qualitative evidence for a novel typology. J Cardiovasc Nurs. 2013;28(6):E37–E46. doi:10.1097/JCN.0b013e31827fcc4c
11. Yao JM. Path analysis on the effect of symptom experience on frailty among patients with chronic obstructive pulmonary disease. Hebei Med J. 2023;45(19):3004–3009. doi:10.3969/j.issn.1002-7386.2023.19.030
12. Zhang H, Li XH, Liu GX, Ji S. Influencing factors of self-reported outcomes in patients with chronic obstructive pulmonary disease. Chin J Gerontol. 2023;43(16):4066–4069. doi:10.3969/j.issn.1005-9202.2023.16.059
13. Lü CE, Lai W, Liu LY. Analysis of dyadic coping status and influencing factors in patients with chronic obstructive pulmonary disease. Chin Gen Pract Nurs. 2024;22(11):2146–2149. doi:10.12104/j.issn.1674-4748.2024.11.043
14. Xiao SZ. Clinical. University Medical Press; 2003.
15. Cheng KK, Wong EM, Ling WM, Chan CW, Thompson DR. Measuring the symptom experience of Chinese cancer patients: a validation of the Chinese version of the memorial symptom assessment scale. J Pain Symptom Manage. 2009;37(1):44–57. doi:10.1016/j.jpainsymman.2007.12.019
16. Lobchuk MM. The memorial symptom assessment scale: modified for use in understanding family caregivers’ perceptions of cancer patients’ symptom experiences. J Pain Symptom Manage. 2003;26(1):644–654. doi:10.1016/s0885-3924(03)00205-7
17. McPherson CJ, Wilson KG, Lobchuk MM, Brajtman S. Family caregivers’ assessment of symptoms in patients with advanced cancer: concordance with patients and factors affecting accuracy. J Pain Symptom Manage. 2008;35(1):70–82. doi:10.1016/j.jpainsymman.2007.02.038
18. Liu JY. The correlation between interdependence and role strain in caregiving activities among family caregivers of dementia patients. Taoyuan, Taiwan: Chang Gung University; 2006.
19. Zhang XQ, Wang MJ, Liu LL, Chen MX. Correlations among mutuality, perceived social support and resilience among main caregivers of pancreatic cancer patients after surgery. Chin J Mod Nurs. 2020;26(14):1865–1870. doi:10.3760/cma.j.cn115682-20191205-04456
20. Xiao SY. Theoretical basis and research application of the social support rating scale. J Clin Psychiatry. 1994;4(2):98–100.
21. Liu JW, Li FY, Lian YL. Investigation of reliability and validity of the social support scale. Xinjiang Med Univ J. 2008;31(1):1–3.
22. Wang CK. The factor structure of the Chinese adaptation of self-concealment scale in middle school students. Chin J Appl Psychol. 2002;8(2):15–17, 7. doi:10.3969/j.issn.1006-6020.2002.02.003
23. Teng Y. The Relationship Between College Students’ Interpersonal Competence and Internet Addiction: The Role of Belief and Self-Concealment. Harbin, Heilongjiang, China: Harbin Normal University; 2019.
24. Shen F, Wu C, Shen MF, Zhang HR. Qualitative study of true experience of patients with refractory epilepsy and primary caregivers during preoperative assessment. J Nurses Train. 2019;34(20):1887–1890. doi:10.16821/j.cnki.hsjx.2019.20.014
25. Cruice M, Worrall L, Hickson L, Murison R. Measuring quality of life: comparing family members’ and friends’ ratings with those of their aphasic partners. Aphasiology. 2005;19(2):111–129. doi:10.1080/02687030444000651
26. Jiang TT, Gao YS, Ji Z, Zhao BY, Zheng RJ, Chen Q. A study on the consistency of life-sustaining treatment preferences between advanced cancer patients and their families based on the theory of planned behavior. J. Chengdu Med Coll. 2025;20(3):536–540. doi:10.3969/j.issn.1674-2257.2025.03.040
27. Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: a systematic review. Respir Care. 2013;58(5):858–866. doi:10.4187/respcare.01862
28. Han X, Wang BQ, An JH, Zhang CP, Yuan LR. Research progress on hospital-community-family-individual management model for patients with chronic obstructive pulmonary disease. J Nurs Sci. 2021;35(4):682–684. doi:10.12102/j.issn.1009-6493.2021.04.024
29. Robinson CA, Bottorff JL, Pesut B, Oliffe JL, Tomlinson J. The male face of caregiving: a scoping review of men caring for a person with dementia. Am J Mens Health. 2014;8(5):409–426. doi:10.1177/1557988313519671
30. Liang LX, Li WF. Effects of gender on emotional interactions in family elderly care. J Chin Womens Stud. 2024;2024(1):13–27.
31. Luo CL, Zhang WJ. Living arrangements and subjective well-being of rural residents. Stud. 2000;13(3):71–105.
32. Chen C, Zhai QH, Li XJ, Hao JJ, Wang LM. Intimate family relationship changes between stroke patients and family caregivers: a meta-synthesis of qualitative studies. Mil Nurs. 2024;41(2):93–97. doi:10.3969/j.issn.2097-1826.2024.02.022
33. Hernandez NJ, Bislick L, Engelhoven A, Hunting Pompon R. Self-report and caregiver proxy-report agreement of perceived chronic stress and mutuality in poststroke aphasia. Am J Speech Lang Pathol. 2021;30(4):1700–1710. doi:10.1044/2021_AJSLP-20-00248
34. Park EO, Schumacher KL. The state of the science of family caregiver-care receiver mutuality: a systematic review. Nurs Inq. 2014;21(2):140–152. doi:10.1111/nin.12032
35. Zhou MY. A study on the relationship between perceived social support, self-concealment and health among empowerment community-based geriatric patients with chronic diseases. Jinzhou Medical University; 2023. doi:10.27812/d.cnki.glnyx.2023.000052
36. Li X, Fan LD, Wang YY, Wang L. Qualitative study on the reasons for delayed medical treatment in patients with chronic obstructive pulmonary disease under the theory of planned behavior. Chin. 2024;10(6):1081–1085. doi:10.12102/j.issn.2095-8668.2024.06.021
37. Zhang W, Liu LF, Cao J, et al. Study on the correlation between stigma and frailty in elderly patients with chronic obstructive pulmonary disease. Chin J Prev Contr Chron Dis. 2024;32(3):216–220. doi:10.16386/j.cjpccd.issn.1004-6194.2024.03.01
38. Kelly AE. The Psychology of Secrets. Springer Science & Business Media; 2002.
39. Xiang ZF. Building a multi-level care network for disabled elderly. People’s Daily. 2025 Mar 24;Sect. 008. doi:10.28655/n.cnki.nrmrb.2025.003401
40. Chen HL, Wang L, Song BX, et al. Gratification and frustration: the ambivalent experiences of community-based eldercare providers and the role of social work intervention. J East China Univ Sci Technol. 2017;32(3):47–55. doi:10.3969/j.issn.1008-7672.2017.03.006
41. Cabral IE, de Moraes JR. Family caregivers articulating the social network of a child with special health care needs. Rev Bras Enferm. 2015;68(6):1078–1085. doi:10.1590/0034-7167.2015680612i
42. Ding XT, Ding YP, Xu Q, Li HP. Relation among positive feelings, adult attachment, social support of the primary caregivers of cancer patients. Chin Gen Pract. 2019;17(12):2111–2114. doi:10.16766/j.cnki.issn.1674-4152.001140
43. van Roij J, Brom L, Youssef-El Soud M, van de Poll-Franse L, Raijmakers NJH. Social consequences of advanced cancer in patients and their informal caregivers: a qualitative study. Support Care Cancer. 2019;27(4):1187–1195. doi:10.1007/s00520-018-4437-1
44. Wang XF, Qiu QY, Dong WP, Ding WH. Application of continuous care based on internet-of-things cloud platform among patients with chronic obstructive pulmonary disease. Mil Nurs J. 2021;38(9):75–78. doi:10.3969/j.issn.1008-9993.2021.09.019
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.