Back to Journals » Advances in Medical Education and Practice » Volume 17
Standardized Patient Simulation as an Effective Tool for Teaching Gastrointestinal Bleeding to Preclinical Medical Students
Authors Patel S, Leisgang AR, Rodgers B ![]() , Williams E, Razjouyan H
, Williams E, Razjouyan H
Received 20 October 2025
Accepted for publication 1 May 2026
Published 16 May 2026 Volume 2026:17 562714
DOI https://doi.org/10.2147/AMEP.S562714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Swapnil Patel,1 Allison R Leisgang,2 Brandon Rodgers,2 Emmanuelle Williams,2 Hadie Razjouyan2,3
1Department of Medicine, Penn State Health Milton S. Hershey Medical Center, Hershey, PA, USA; 2Division of Gastroenterology and Hepatology, Penn State Health Milton S. Hershey Medical Center, Hershey, PA, USA; 3Department of Public Health and Sciences, Penn State College of Medicine, Hershey, PA, USA
Correspondence: Swapnil Patel, Department of Medicine, Penn State Health, 500 University Drive, Hershey, PA, 17033, USA, Email [email protected]
Introduction: Medical simulations are a well-established educational tool, allowing students hands on practice before starting clinical practice. In this study, we created a medical simulation to guide preclinical first-year medical students through a gastrointestinal (GI) bleed patient encounter. Our objective was to evaluate the educational impact of simulation cases, particularly in the context of GI pre-clinical medical education.
Methods: Students participated in a standardized patient (SP) simulation of a patient with abdominal discomfort and rectal bleeding suggestive of cirrhosis. Sixteen sessions with two SPs were facilitated by five GI attendings and fellows. Student teams performed history-taking, physical examination, differential diagnosis, and management of a dynamically evolving, critically ill patient. Following the simulation, facilitators led a debrief linking clinical findings to preclinical pathophysiology. Students completed post-simulation surveys assessing perceived skills and learning.
Results: Seventy-seven students participated; 63 were included in analysis. Sixty-three percent were female. Students demonstrated significant improvement in perceived history and physical exam skills (pre: 3.23± 1.06 vs post: 4.21± 0.58, P< 0.01) and in developing differential diagnoses (pre: 3.02± 0.91 vs post: 4.13± 0.61, P< 0.01). Ninety-seven percent reported improved understanding of GI bleeding. Additionally, 83% preferred more simulation-based learning prior to clerkships, and 83% desired more GI-focused simulations during clerkship.
Discussion: This simulation case proved to be an effective tool to enhance pre-clinical medical students’ abilities to understand and manage GI bleeding. The simulation allowed for the realistic practice of critical clinical skills while demonstrating to students the relevance of their pre-clinical learning. The perceived improvements observed in knowledge and confidence suggest that integrating simulation-based training early into the medical curriculum could improve the transition from theoretical learning to clinical practice. Future studies should evaluate long-term skill retention and impact on clinical performance.
Keywords: medical simulation, gastrointestinal bleeding, preclinical medical education, standardized patient, clinical skills development
Introduction
Medical education increasingly incorporates simulation-based learning to enhance the preparedness and competence of students prior to their clinical rotations. These simulations offer a controlled environment where learners can practice and refine their skills, build confidence, and improve their clinical judgment without the immediate pressures of patient care. A report from the Association of American Medical Colleges revealed that over 90% of surveyed medical schools incorporate simulation-based content in their preclinical education, predominantly utilizing manikins and standardized patients (SP).1 Clinical simulations have been thoroughly researched in various medical specialties.1,2 For medical students who are in the early stages of their medical education, simulation-based training has been shown to significantly impact their retention of knowledge and their confidence levels.2–9 However, despite these promising results, there is a notable gap in the literature regarding the impact of simulations specific to the field of gastroenterology, particularly among pre-clerkship students.9,10
Gastrointestinal (GI) bleeding represents a common clinical challenge that pre-clerkship students may encounter in their subsequent clerkships and potentially later in their medical training. While procedural skills such as endoscopy simulation training and simulated outpatient GI clinic encounters have been studied in preclinical medical students,10,11 targeted simulations addressing GI bleeding, a common condition with varied presentations and management strategies, remain underexplored to our knowledge. Specifically, we aimed to explore how standardized patient simulations influence students’ knowledge and confidence regarding the evaluation and management of GI bleeding and their overall interest in the field of GI. By bridging this gap, we hope to contribute to developing more effective educational strategies that enhance the clinical preparedness of future physicians.
Methods
Study Design
This was a prospective, cross-sectional study conducted in accordance with ethical standards and approved by the Institutional Review Board (IRB) of the Penn State College of Medicine on May 21, 2024 (IRB Protocol Number: 00024979). The study participants were first-year medical students enrolled in the GI pathophysiology course during the 11th month of their training. The simulation sessions were held simultaneously in two rooms, each lasting one hour, on two separate days, with just one day between them. A total of 16 sessions, each consisting of 5–8 medical students, were conducted. The clinical case that was used during the simulation was inspired by a similar clinical scenario observed during a GI simulation at Harvard Medical School in 2011.
Equipment and Environment
The study was conducted in the simulation center at Penn State University College of Medicine. Two simulation laboratory rooms were equipped for the study. Each room contained a stretcher, monitors to display vital signs, a blood pressure cuff, thermometer, oximeter, a container containing coffee ground material, which was covered until needed, and the SP was lying on a chuck/pad with bright red food coloring to simulate hematochezia. Additionally, each room was equipped with a two-way microphone and speaker, allowing communication between the outside facilitator, the simulation technician and the room.
Each room had a male SP who was well-versed in the scenario and had participated in this practice annually. The SPs wore hospital attire, having changed into their dressing and seated on the stretcher. In each room, an in-room facilitator was present to help guide the simulation as well as concurrently play the role of the SP’s accompanying significant other during the case. The setup also included an artificial packed red blood cell (RBC) bag, a liter of normal saline, an IV set with connectors, and tools to create physical exam findings on the SP, such as a facial spider angioma, palmar erythema, and peri-umbilical color changes suggestive of caput medusa. Two papers, each containing colored images of characteristic physical exam findings in patients with cirrhosis, were available to share with students upon request during their physical examination.
Simulation Case and Encounter Course
The study was designed around a SP simulation focused on a clinical case of GI bleeding in the context of liver cirrhosis. A 65-year-old man presented to the emergency room with abdominal cramping and rectal bleeding. The students, working as a team, were tasked with expanding on the chief complaint to generate the history of present illness, gather the patient’s past medical and surgical history, medication list, allergies, family and social histories. When students obtained the social history, the SP shared information about smoking, alcohol consumption and recent move from Central America.
The group was guided by the in-room facilitator to expand on the information gathered and prompted to proceed to the next steps, such as the review of systems and physical examination. The SP also provided hints to assist in moving the case forward to help the students as necessary.
After the simulation session, a 20-minute recorded presentation was made available to all medical students via their portal. This presentation outlined the learning objectives and key elements of the case, from presentation to diagnosis and management, with the goal of standardizing the teaching experience for all participants. Students were called on to reflect on aspects of the case they found challenging, team work dynamics, and linking of pathophysiological concepts to the live case.
Data Collection and Statistical Analysis
Upon conclusion of the simulation session, participants were voluntarily asked to complete a post-simulation survey via a QR code linked to an online platform, participant consent was implied. The survey remained open for 48 hours following the second day of the simulation sessions. It collected both quantitative and qualitative data on both pre and post simulation perceptions in diagnostic skill improvement, confidence in skills, and the perceived educational value of the simulation (see Figure 1).
Figure 1 continued. Figure 1 Simulation survey assessment.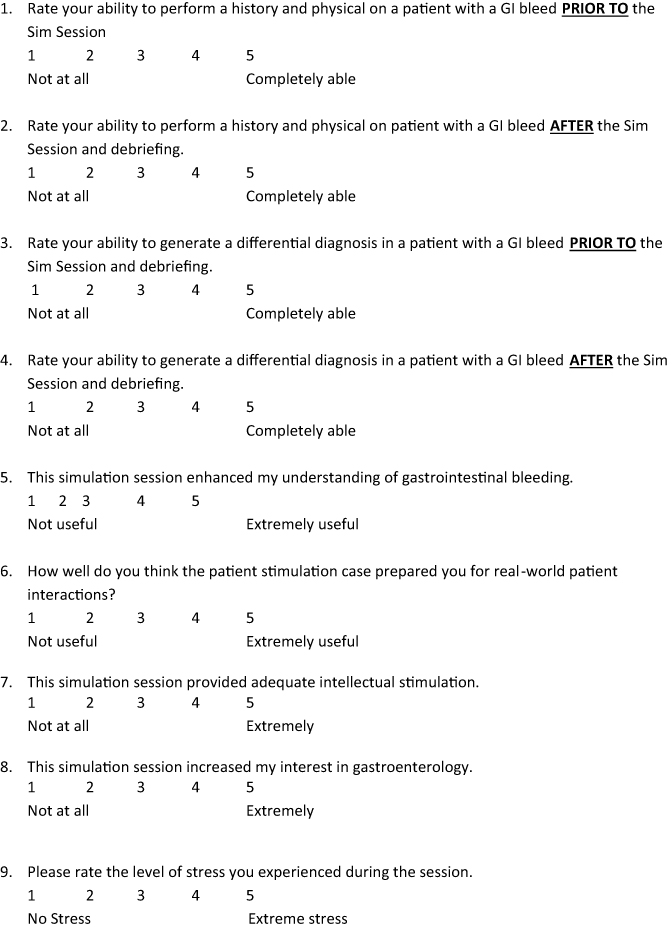
Qualitative data were reviewed to provide insights into students’ perceptions and learning experiences during the simulated patient encounter. Numerical variables are reported as means ± standard deviation. Univariate analysis was performed using the chi-squared test for categorical variables and paired t-test and ANOVA, as appropriate. A two-sided P value of <0.05 was considered statistically significant. Data analysis was conducted using IBM SPSS Statistics (IBM, Armonk, NY), version 27.
Results
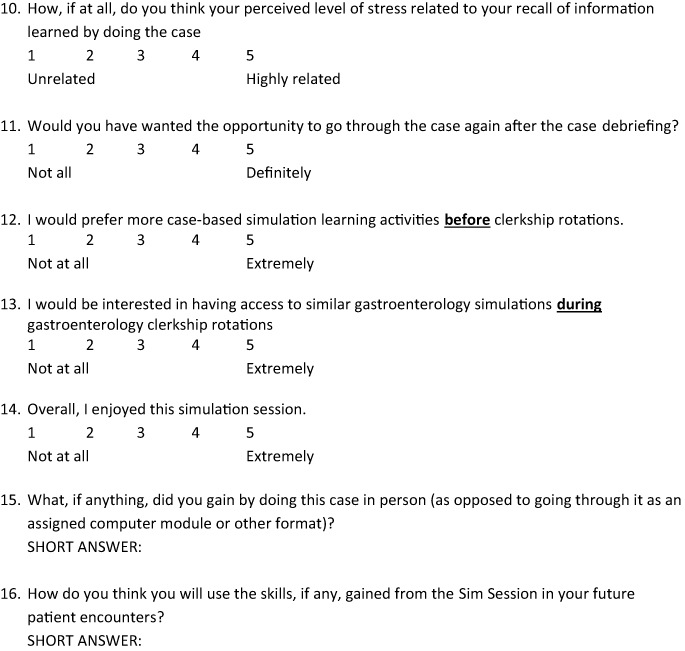
Seventy-seven first year medical students participated in simulation sessions and we included responses from 63 participants who completed at least 33% of the survey as depicted in Figure 2. As illustrated in Table 1, 97% of students reported that the simulation enhanced their understanding of GI bleeding, and 87% rated their enjoyment of the session as high (rating 4–5 on a Likert scale). Additionally, 83% expressed a preference for more case-based simulation learning activities prior to starting clerkship rotations, while 83% also indicated an interest in having additional GI simulations specifically during the GI clerkship. Regarding preparedness for real-world patient interactions, 89% of students felt the simulation was useful (rating 4–5 on Likert scale), and 87% indicated that it provided adequate intellectual stimulation. Post-simulation, 62% reported an increased interest in the GI specialty. As indicated in Figure 3, students perceived stress levels associated with the simulation were generally low, with 52% of students reporting minimal stress (rating 1–2 on Likert scale).
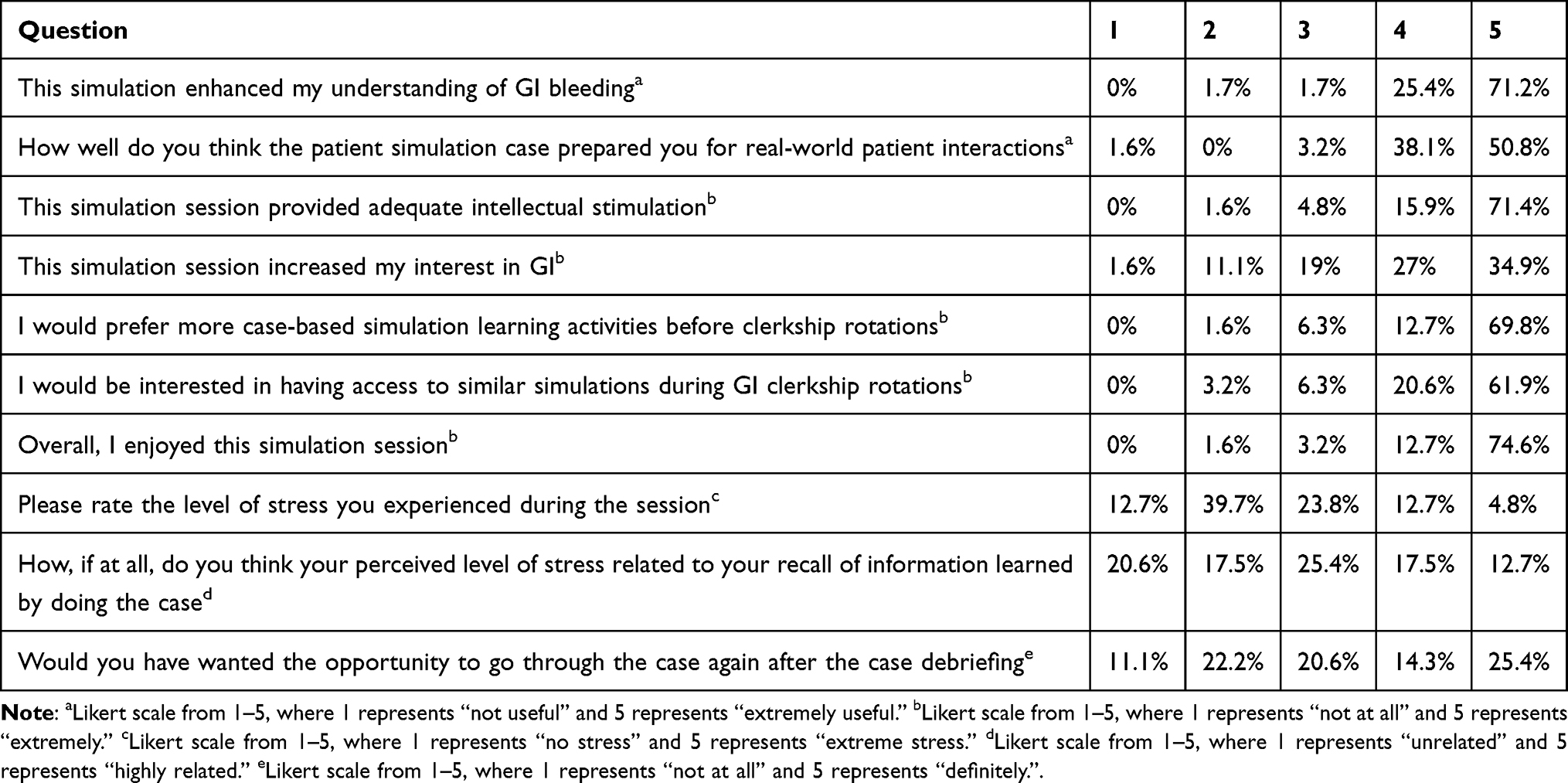 |
Table 1 Student Responses to Survey Questions |
 |
Figure 2 Study population characteristics. |
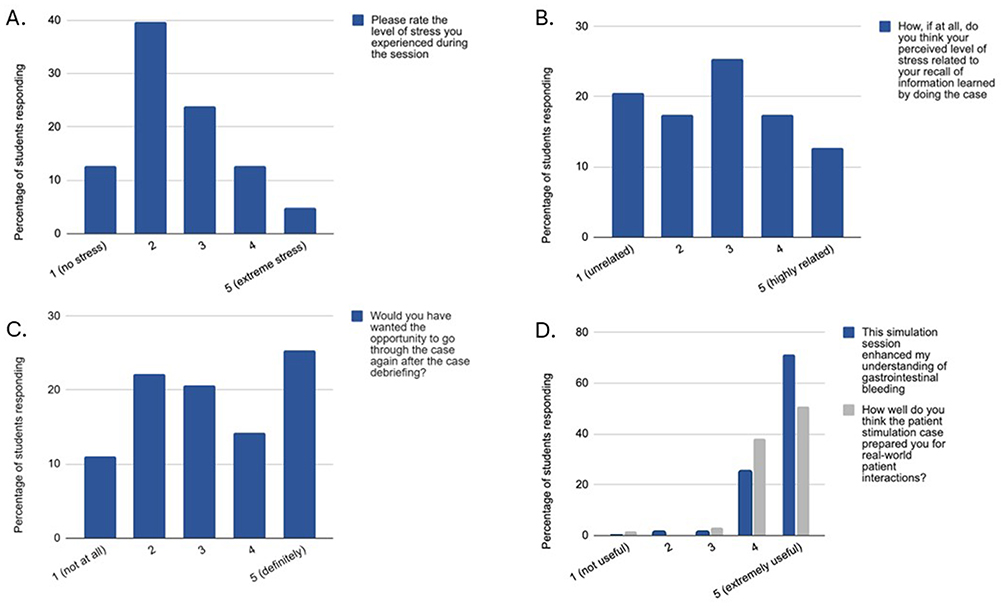 |
Figure 3 Quantitative representation of student evaluation data regarding (A) level of stress during simulation (B) impact of stress on recall of information (C) willingness to go through case after debriefing and (D) understanding of GI bleeding and preparedness for real-world patient interactions. These questions were assessed on a five-choice Likert scale. |
The simulation led to significant improvements in the students’ perceived clinical skills (Figure 4). The mean score for students’ perceived ability to perform a history and physical exam increased from a pre-simulation score of 3.23 ± 1.06 to a post-simulation score of 4.21 ± 0.58 (P < 0.01). Similarly, students’ perceived ability to develop a differential diagnosis for GI bleeding showed a significant increase, with scores improving from 3.02 ± 0.91 pre-simulation to 4.13 ± 0.61 post-simulation (P < 0.01).
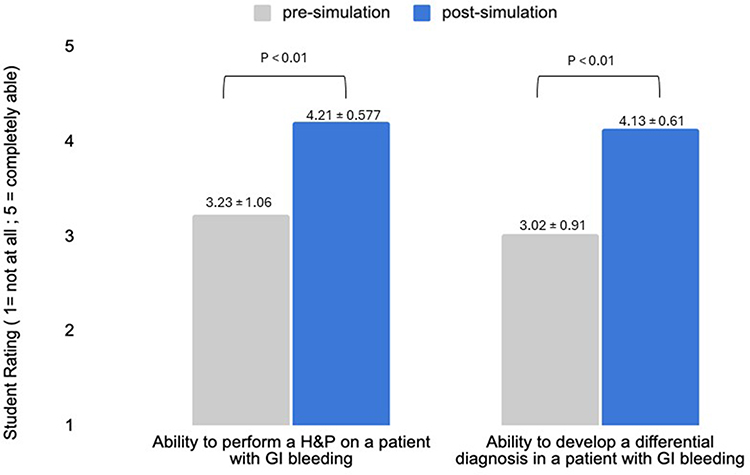 |
Figure 4 Representation of statistically significant improvement in perceived H&P and differential diagnosis skills post-simulation. |
As illustrated in Table 1, 97% of students reported that the simulation enhanced their understanding of the pathophysiology and management of GI bleeding, and 87% rated their enjoyment of the session as high (rating 4–5 on a Likert scale). Additionally, 83% expressed a preference for more case-based simulation learning activities prior to starting clerkship rotations, while 83% also indicated an interest in having additional GI simulations specifically during the GI clerkship.
Discussion
While prior research has largely focused on the benefits of simulation-based learning during the clinical years of medical education, including the final two years of medical school and residency, there has been limited investigation into case-based learning for pre-clinical years (first and second years of medical school). These early years are typically focused on foundational science education, leaving limited opportunities for clinical application or hands-on experiences. Studies have shown that simulation enhances learner engagement and self-reported confidence in clinical skills in prior studies.12–14 Early clinical exposure in a well-controlled setting may enhance learner engagement and perceive value of the educational experience.
Although some publications have explored and described the integration of GI simulations into preclinical medical education,9–11 to our knowledge, no research has specifically evaluated the impact of GI bleeding simulations on preclinical medical students. GI bleeding is a critical topic in medical education due to its prevalence, potentially life-threatening nature, and the complexity of its diagnosis and management. In addition, the initial management of GI bleeding relies on the foundational skills of appropriate resuscitation and thus using it as a clinical scenario may provide a framework for introducing core clinical concepts in a simulated setting.
This simulation emphasized the multidisciplinary nature of patient care by incorporating key clinical competencies. Students were exposed to opportunities to practice taking a thorough history, including social history and social determinants of health, which are critical for understanding a patient’s overall well-being. The case highlighted the importance of reviewing consent for care, particularly in complex scenarios such as determining decision-making authority (eg., friend vs. next of kin) and discussing blood transfusion in cases of loss of consciousness. Students were also introduced to the process of calling in expert care including summarizing key clinical information to consultants. Additionally, students were exposed to effective handovers of care as students navigated transitions between teams, ensuring continuity of care.
The most striking outcome of the study was the improvement in students’ self-reported confidence, as evidenced by statistically significant increases in their mean scores for performing a history and physical exam and developing a differential diagnosis pre- and post-simulation (Figure 4). The improvement in self-reported confidence in history-taking suggests that students perceived exposure to a structured, realistic approach to systematically gathering relevant clinical information in a time sensitive manner. Likewise, the enhancement in self-reported confidence in physical examination reflects participants’ perceptions of increased comfort following the simulation. The improvement in self-reported differential diagnosis scores may indicate increased perceived comfort with clinical reasoning tasks. Students were encouraged to synthesize clinical findings into a coherent diagnostic framework, a skill critical for effective patient management. Developing these skills during the preclinical years establishes a strong foundation for future clinical success.
It was notable that most students indicated a preference for more case-based simulation learning activities prior to starting clerkship rotations (Table 1). These findings are consistent with the growing body of literature supporting the impact of simulation-based learning in medical education, particularly in the early stages of medical training.15–20 The overwhelmingly positive feedback from participants highlights the simulation’s value as an engaging and effective learning modality. Nearly all students reported an enhanced understanding of GI bleeding, and the majority rated their enjoyment of the session as high (Table 1). This engagement is particularly important, as motivation and enjoyment are known to improve the retention of information and foster a positive attitude toward learning.21
The simulation’s impact extended beyond knowledge and skills, influencing students’ confidence and interest in real-world patient care. Most students found the simulation useful for preparing them for future patient interactions and indicated an increased interest in the GI specialty post-simulation (Table 1). It is well-documented that exposure to clinical specialties in early medical training plays a pivotal role in shaping students’ future career choices.22–24 By incorporating GI simulations in preclinical years, medical schools may be able to increase interest in GI, potentially addressing the workforce shortages in the field.25 Additionally, GI simulation cases serve as a versatile educational tool, allowing students to engage with fundamental concepts across multiple disciplines. These simulations can be used to teach key aspects of resuscitation, initial management of critically ill patients, and ethical considerations, such as informed consent and decision-making in life-threatening situations. They also provide opportunities to explore humanities in medicine, including patient-centered communication and the social determinants of health. By leveraging GI simulations as a platform for interdisciplinary learning, medical educators can effectively prepare students for the complexities of real-world clinical practice while reinforcing essential skills relevant to a broad range of medical specialties.
Although the results are encouraging, several limitations warrant caution. The study relies on self-reported survey data, which may introduce response bias, and pre-simulation scores were obtained retrospectively, potentially leading to response shift bias. Reported gains in confidence and perceived skills may partly reflect the novelty of the simulation rather than true skill acquisition. Additionally, a gastrointestinal bleeding scenario may be advanced for first-year students, and improvements likely reflect early exposure to clinical reasoning rather than mastery of clinical skills.
While many students rated the simulation positively, further objective measures, such as performance on subsequent clinical assessments, would be beneficial to substantiate these findings. Improvements in history taking and physical examination were based on self-reported perceptions and were not independently assessed and thus may be inherently biased. The study’s single-center design and a sample size of 63 participants, predominantly female, limit generalizability. Future studies incorporating objective assessments and longitudinal follow-up would help determine whether perceived gains translate into measurable outcomes.
Although this simulation study was well received, it is important to acknowledge that replicating such outcomes across all academic centers may present challenges. Variability in resources, including access to high-fidelity simulation equipment, trained facilitators, and space constraints, can limit the feasibility of conducting similar simulations at every institution. However, educational objectives can still be met through alternative approaches.
Future research should focus on evaluating case-based learning modules, virtual simulations, and alternative delivery methods in GI education.
Conclusion
To the best of our knowledge, this study represents the first to investigate the role of a GI bleeding simulation among pre-clinical medical students, offering them an opportunity to apply the knowledge they have gained throughout their coursework and make interdisciplinary connections. This study demonstrates that a SP simulation focused on GI bleeding was associated with increased self-reported confidence among preclinical medical students in areas such as history-taking, physical examination, and clinical reasoning. These findings suggest that simulation-based learning may enhance learners’ perceived comfort with approaching complex clinical scenarios early in medical training.
However, these results are based on subjective assessments and do not reflect objective measures of clinical competence or performance. As such, the findings should be interpreted cautiously. Further research incorporating objective evaluation methods and longitudinal follow-up is needed to determine whether these perceived gains translate into measurable improvements in clinical skills or knowledge retention.
Acknowledgment
The abstract of this paper was presented as a poster at the American College of Gastroenterology (ACG) Annual Scientific Meeting (Philadelphia, Pennsylvania, October 2024). The abstract was published in The American Journal of Gastroenterology (“Poster Abstracts”): The American Journal of Gastroenterology 119(10S):p S700–S701, October 2024. DOI: 10.14309/01.ajg.0001033364.19047.90. https://journals.lww.com/ajg/fulltext/2024/10001/s999_gastrointestinal_bleed__a_simulation_case_for.1000.aspx
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Passiment M, Sacks H, Huang G. Medical simulation in medical education: results of an AAMC survey. AAMC. 2011.
2. Okuda Y, Bryson EO, DeMaria S, et al. The utility of simulation in medical education: what is the evidence? Mt Sinai J Med. 2009;76(4):330–9. doi:10.1002/msj.20127
3. Battaglia F, Ivankovic V, Merlano M, et al. A pre-clerkship simulation-based procedural skills curriculum: decreasing anxiety and improving confidence of procedural skill performance. Can Med Educ J. 2021;12(5):34–39. doi:10.36834/cmej.71483
4. Al-Elq AH. Simulation-based medical teaching and learning. J Family Commun Med. 2010;17(1):35–40. doi:10.4103/1319-1683.68787
5. Austin JP, Baskerville M, Bumsted T, et al. Development and evaluation of a simulation-based transition to clerkship course. Perspect Med Educ. 2020;9(6):379–384. doi:10.1007/s40037-020-00590-4
6. Kwan B, Bui G, Jain P, Shah N, Juang D. Exploring simulation in the internal medicine clerkship. Clin Teach. 2017;14(5):349–354. doi:10.1111/tct.12577
7. Takayesu JK, Farrell SE, Evans AJ, Sullivan JE, Pawlowski JB, Gordon JA. How do clinical clerkship students experience simulator-based teaching? A qualitative analysis. Simulation Healthcare. 2006;1(4):215–219. doi:10.1097/01.SIH.0000245787.40980.89
8. Nalini YC, Manivasakan S, Pai DR. Importance of simulation in undergraduate medical education with specific emphasis on preclinical phase – a narrative review. BLDE Univ J Health Sci. 2023;8(2):205–209. doi:10.4103/bjhs.bjhs_200_22
9. DeSipio J, Gaughan J, Perlis S, Phadtare S. Use of real patients and patient-simulation-based methodologies for teaching gastroenterology to pre-clinical medical students. Healthcare. 2018;6(2):61. doi:10.3390/healthcare6020061
10. Persad AR, Verma LK, Persad R. Endoscopy simulation for pre-clerkship students. Can Med Educ J. 2020;11(1):e141–e143. doi:10.36834/cmej.67898
11. Williams DM, Bruggen JT, Manthey DE, Korczyk SS, Jackson JM. The GI simulated clinic: a clinical reasoning exercise supporting medical students’ basic and clinical science integration. MedEdPORTAL. 2020;16:10926. doi:10.15766/mep_2374-8265.10926
12. Bergmann J, Krewer C, Bauer P, Koenig A, Riener R, Müller F. Virtual reality to augment robot-assisted gait training in non-ambulatory patients with a subacute stroke: a pilot randomized controlled trial. Eur J Phys Rehabil Med. 2018;54(3):397–407. doi:10.23736/S1973-9087.17.04735-9
13. Mackay EC, Patel KR, Davidson C, et al. Simulation as an effective means of preparing trainees for active participation in MDT meetings. Future Healthc J. 2024;11(1):100017. doi:10.1016/j.fhj.2024.100017
14. Lembo D, Abate Daga F, Calì C, et al. Early introduction of simulation in the medical curriculum: the MedInTo perspective. Front Med. 2024;10:1280592. doi:10.3389/fmed.2023.1280592
15. Williams K-L, Dunne C, Parsons MH. Emergency department presentation of a patient with a severe upper gastrointestinal bleed: a simulation case for training emergency medicine residents. Cureus. 2019;11(1):e3908. doi:10.7759/cureus.3908
16. Vera-Diaz FA, Johnson C. Perceived enhanced clinical readiness for second-year optometry interns. Optom Educ. 2017;43:1–13.
17. Wenrich MD, Jackson MB, Wolfhagen I, Ramsey PG, Scherpbier AJ. What are the benefits of early patient contact? - A comparison of three preclinical patient contact settings. BMC Med Educ. 2013;13(1):80. doi:10.1186/1472-6920-13-80
18. Dornan T, Tan N, Boshuizen H, et al. How and what do medical students learn in clerkships? Experience based learning (ExBL). Adv Health Sci Educ. 2014;19(5):721–749. doi:10.1007/s10459-014-9501-0
19. Godefrooij MB, Diemers AD, Scherpbier A. Students’ perceptions about the transition to the clinical phase of a medical curriculum with preclinical patient contacts; a focus group study. BMC Med Educ. 2010;10(1):28. doi:10.1186/1472-6920-10-28
20. Diemers AD, Dolmans DHJM, Verwijnen MGM, Heineman E, Scherpbier AJJA. Students’ opinions about the effects of preclinical patient contacts on their learning. Adv Health Sci Educ. 2008;13(5):633–647. doi:10.1007/s10459-007-9070-6
21. Kpolovie PJ, Joe AI, Okoto T. Academic achievement prediction: role of interest in learning and attitude towards school. Int J Humanit Soc Sci Educ. 2014;1(11):73–100.
22. Branstetter BF, Faix LE, Humphrey AL, Schumann JB. Preclinical medical student training in radiology: the effect of early exposure. AJR Am J Roentgenol. 2007;188(1):W9–W14. doi:10.2214/AJR.05.2139
23. Zeldow PB, Preston RC, Daugherty SR. The decision to enter a medical specialty: timing and stability. Med Educ. 1992;26(4):327–332. doi:10.1111/j.1365-2923.1992.tb00177.x
24. Gawad N, Moussa F, Christakis GT, Rutka JT. Planting the ‘SEAD’: early comprehensive exposure to surgery for medical students. J Surg Educ. 2013;70(4):487–494. doi:10.1016/j.jsurg.2013.03.006
25. Ying X, Yao L, Mathis WS, et al. Geographic disparities in access to gastroenterologists in the United States. Gastroenterology. 2025;168(6):1189–1191.e1. doi:10.1053/j.gastro.2025.01.232
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.