Back to Journals » Risk Management and Healthcare Policy » Volume 16
Stakeholders’ Perspective on the Integration of Pharmacovigilance Activities into the Eritrean Healthcare System: A Qualitative Study
Authors Abraham NA, Tesfagaber M ![]() , Tesfamariam S
, Tesfamariam S ![]()
Received 9 December 2022
Accepted for publication 9 April 2023
Published 21 April 2023 Volume 2023:16 Pages 747—757
DOI https://doi.org/10.2147/RMHP.S398811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Natnael Araya Abraham,1 Meron Tesfagaber,2 Sirak Tesfamariam2
1University of Oxford, Nuffield Department of Medicine, Center of Tropical Medicine and Global Health, Oxford, UK; 2Product Evaluation and Registration Unit, National Medicines and Food Administration, Asmara, Eritrea
Correspondence: Meron Tesfagaber, Tel +291-7501923, Fax +291-1-122899, Email [email protected]
Purpose: Understanding the integration of pharmacovigilance activities in the healthcare system and identifying existing hindering factors systematically through the eyes of stakeholders has paramount importance to realize a successful integration. Thus, this study aimed to assess the perspectives of the stakeholders of the Eritrean Pharmacovigilance Center (EPC) on the integration of pharmacovigilance activities into the Eritrean healthcare system.
Methods: An exploratory qualitative assessment of the integration of pharmacovigilance activities into the healthcare system was conducted. Key informant interviews were conducted among the major stakeholders of the EPC via face-to-face and telephone interviews. Data were collected between October 2020 and February 2021, and analyzed through thematic framework analysis.
Results: A total of 11 interviews were completed. The integration of the EPC in the healthcare system was rated as good and encouraging except in the National Blood Bank, and Health Promotion. The relationship between the EPC and Public health programs was described as mutual with an eminent impact. Several facilitating factors for integration were identified namely: the unique work culture of the EPC; provision of basic and advanced training; motivating and recognizing healthcare professionals in vigilance activities; and the financial and technical support provided to the EPC from national and international stakeholders. On the other hand, the absence of concrete communication systems, inconsistencies in training and communication, the absence of data-sharing mechanisms and policies, and the absence of designated pharmacovigilance focal persons were identified as barriers to successful integration.
Conclusion: Integration of the EPC in the healthcare system was found to be commendable except in some areas of the healthcare system. Therefore, the EPC should work towards identifying further areas of integration, mitigate the identified limitations and at the same time sustain the integration already initiated.
Keywords: key informant interview, thematic framework analysis, facilitating factors, limiting factors
Introduction
Pharmacovigilance is a dynamic scientific and clinical discipline that aims to improve patient care concerning the use of medicines and promotes overall public health.1 A pharmacovigilance system liaises with different sectors of the healthcare system, through its fitting complementary functions, in the attainment of a common public health goal - ensuring patient safety and improving public health.2 Taking the broad scope of pharmacovigilance into account, which expands with the increasing range and potency of pharmaceutical and biological medicines, concerted and cooperative work within the healthcare system becomes indispensable.3 Such collaborative work calls for efficient integration of pharmacovigilance into the entire healthcare system.4–7
Successful integration can create a platform for the healthcare system to resolve safety issues related to medicines, reduce treatment and resistance failures, promote rational use of medicines, and warrant public confidence in the system.8 As a result of this, the formation of partnerships among pharmacovigilance centers and major stakeholders, namely Public Health Programs (PHPs), United Nations (UN) agencies and development programs, academia, and health facilities is necessary to gain from the corresponding expertise and financial opportunities to achieve their targeted outcomes.9,10 Moreover, pharmacovigilance centers should also form collaborations with healthcare consumers, patient representatives, and pharmaceutical industries to promote safe use and reduce the risks of medical products.11,12 The integration of pharmacovigilance systems in Low- and Middle- income countries (LMICs), however, has been challenging despite efforts made to harmonize pharmacovigilance rules and regulations across regions.7,13
In Eritrea, the national pharmacovigilance system is operated under the auspices of the Eritrean Pharmacovigilance Center (EPC). The EPC is involved in activities related to spontaneous reporting of adverse events/ reactions to all medicines, vaccines, biological products, herbal medicines and traditional remedies, and medical devices. It is also responsible for maintaining a single national database for adverse reactions and submission of adverse reaction reports to the WHO global Individual Case Safety Reports (ICSR) database, Vigibase.14 The center has shown rapid growth since its revitalization in 2012, with its focus now centered on the evaluation and research of ICSRs rather than the mere collection of ICSRs.15,16 The success of the EPC has been demonstrated in terms of the number of Adverse Drug Reactions (ADRs) reports, completeness of the reports, number of safety signals generated, recall of substandard and falsified medicines, and the vast diffusion of the system in the Eritrean health facilities.15,17,18 The accomplishments attained by the EPC so far can be attributed to the concerted efforts of the major parties involved. These parties include health professionals, zonal pharmacovigilance focal persons, volunteer medical officers, and ultimately the dedicated pharmacovigilance staff.15
The mandate of the EPC to monitor the safety of medical products creates a platform for a synergistic relationship with all stakeholders who share the goal of improving patient safety. Creating a collaborative partnership and full integration in the healthcare system, with clearly defined mutual activities, thus, could bring an imminent growth and sustainability for the EPC.19 The EPC has made tremendous efforts to integrate pharmacovigilance activities into several sectors of the healthcare system.15 Although a nationwide survey conducted in 2017 revealed that the pharmacovigilance system is well-diffused in the Eritrean healthcare system,17 it can be taken forwards without limits. Several challenges may also exist to hinder a successful integration. Understanding the integration of the pharmacovigilance activities into the healthcare system and identifying the existing hindering factors systematically through the eyes of the stakeholders has paramount importance to sustain the success so far achieved and strive for greater realization of effective integration. This study, therefore, was conceived to qualitatively assess the perspective of the stakeholders on the integration of pharmacovigilance activities into the Eritrean healthcare system.
Methods
Study Design and Setting
An exploratory qualitative study using semi-structured face-to-face and telephone interviews was conducted between October 2020 and February 2021. The face-to-face interviews took place at the participants’ workplaces. During the data collection process, no one else was present besides the participants and the researchers.
Study Population
All stakeholders identified by the EPC such as the PHPs, medical services department, academia, UN agencies, non-governmental organizations, zonal medical offices, health facilities, market authorization holders, healthcare professional associations, the general public, and media were the source population of the study. To understand the level of integration of the pharmacovigilance activities, key informants from the stakeholders who have already established networks with the EPC namely the Expanded Program on Immunization (EPI), National Malaria Control Program, Human Immunodeficiency Virus (HIV) and Sexually Transmitted Infections (STI) Control program, and National Tuberculosis and Leprosy Control Program and Neglected Tropical Diseases (NTD) control programs, zonal medical offices, health promotion, and the World Health Organization (WHO) were included in the study.
Sampling Design and Sample Size
The study participants were selected using a purposive sampling technique. The sampling framework was designed to ensure the representation of the major stakeholders identified by the EPC. The sample size of the study was determined by the principle of data saturation, where the emergence of new themes and codes plateaus despite interviewing more participants. In this study, data saturation was met after conducting 11 in-depth interviews.
Interview Procedure
The authors developed an interview guide designed to address key elements of the substantive research topic as provided in Supplementary Data 1. The interview guide was developed based on discussions within the research team. There was flexibility in the use of the guide as the order of the questions and wording could be changed while taking account of individuals’ responses, and prompts were used where the responses were limited.
The participants were contacted to schedule an interview at their convenience. Prior to the involvement of the study participants, formal written invitation letters were sent to the participants. The participants voluntarily responded to the invitation; gave recorded verbal informed consent for the participation and audio recording of the interviews.
The authors (NAA, ST, and MT), who are experienced in qualitative research, conducted the face-to-face and telephone interviews all together. At the beginning of the interview, the aim and objective of the study were explained to each participant.
Eight face-to-face interviews were conducted and lasted for an average of 24 minutes ranging from 16 to 33 minutes. In addition, 2 telephone interviews were conducted with the zonal medical officers due to the inaccessibility of their working areas. The telephone interviews lasted an average of 32 minutes.
The participants were interviewed in a language of their preference; either in Tigrigna (local language) or in English. The interviews were audio-recorded and field notes were taken. No repeat interviews were carried out.
Data Analysis
Thematic framework analysis was used to analyze the data. A seven-step procedure for applying thematic framework analysis was followed.20 The procedure for analysis included the following steps in consecutive order: transcription; familiarization with the interview; coding; developing a working analytical framework; applying the analytical framework; charting data into the framework matrix and interpreting the data.
Initially, all the interviews were transcribed verbatim by all the authors. Interviews undertaken in the local language (Tigrigna) were translated individually by all the authors for comparison. The authors crosschecked each other’s transcripts for any inconsistencies by re-listening to the audio records until an agreement was reached.
During the process of familiarization, all transcripts were read independently by all authors. After a thorough reading of the transcripts, all the researchers (NAA, MT, and ST) applied codes that described their initial impression of the interview transcripts using inductive coding. Coding was done manually and no qualitative data analysis software was used to manage the data. The initially identified codes were matched up with the data extracts that demonstrated the particular code. After all the data have been initially coded and collated, all the researchers met and discussed the emergent codes and refined the initial codes to develop the analytical framework using Excel. In cases where there were inconsistencies in the codes, they were resolved upon the consensus of the authors. Data identified by the same code were compiled together and labeled to create subthemes; and finally, the subthemes were aggregated to form themes. The potential subthemes and themes were then reviewed, refined, and reorganized. Finally, all subthemes and themes were defined and named. Quotations from the participants were used to illustrate the themes and subthemes generated in the study.
All audio recordings, transcripts, coding reports, and notes were retained and well-documented. Each participant in the study was sent their transcript and quotes for verification and approval.
The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist21 was used to ensure comprehensive reporting as shown in Supplementary Data 2.
Ethical Approval
The study was approved by the Health Research Ethics and Protocol Review Committee of the Ministry of Health, Eritrea. Audiotaped verbal informed consent was taken from each participant as some of the interviews were conducted via telephone and to lighten respondents’ insecurities that may come with written informed consent. Approval for verbal informed consent was also obtained from the ethics committee. The name and other identifiers of the participants were kept anonymous; the participants’ transcripts were assigned codes for identification and later quoting. All methods in this study were performed in accordance with the requirements of the Declaration of Helsinki.
Results
A total of 11 participants were enrolled in the study until data saturation was reached. After the qualitative framework analysis, 17 distinct sub-themes emerged and were aggregated to form 4 main themes namely, integration of pharmacovigilance into the healthcare system, impact of the integration, facilitating factors, and limiting factors for the integration (Figure 1).
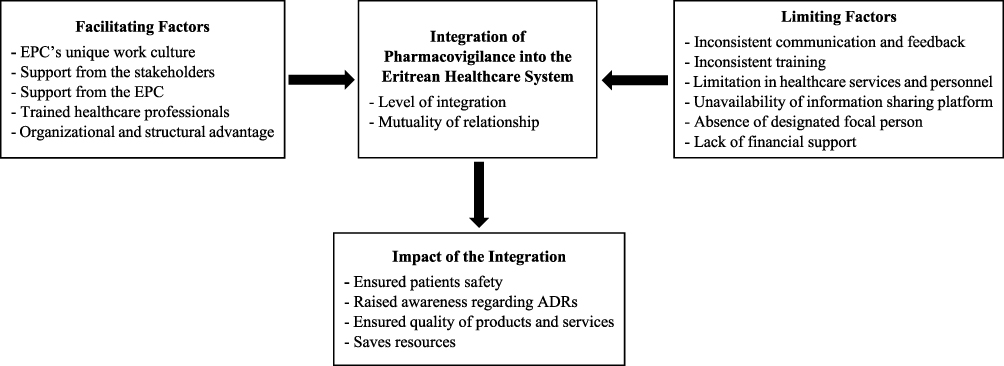 |
Figure 1 Summary of the themes and subthemes developed after framework analysis. |
Integration of Pharmacovigilance into the Healthcare System
Overall, the respondents rated the integration of pharmacovigilance in the Eritrean healthcare system as “good” and “encouraging”. All of the participants claimed that the good relationship, collaborative work, and communication created between the center and different stakeholders, since its establishment, are indicators of effective integration.
Most of the respondents claimed that the integration is satisfactory at the zonal level and has even gone down to the lower-level health facilities. At the higher level, some respondents disclosed that pharmacovigilance is not diffused well in some PHPs such as the health promotion division and the national blood bank. On the contrary, another respondent noted that the integration is very good at the national level, but has not descended downward to the zonal level. The respondent further explained,
The integration is very well. We are even told by foreign partners that the EPC is one of the best. Its relationship and collaborative work with PHPs are indicators of this. From my point of view, even though the integration is good, particularly at the national level, it has to descend downwards. [F]
Several respondents stated that the relationship established between their respective programs and EPC is mutual and that the center is involved during the development of the programs’ strategic plans and introduction of new program medicines. One respondent put it as:
Our relationship is mutual. We do communicate and exchange information and we have benefited a lot in the last 5 years from the center. Had it not been for the EPC, we would have faced problems with drug safety profiles. [F]
Impact of the Integration
The second theme covers the influence of the center’s integration into the healthcare system. Most of the respondents disclosed that the major impact brought by the EPC has been the identification, prevention, and/or minimization of drug-related health risks. The respondents provided practical achievements in this regard including the detection of artesunate-amodiaquine-related extrapyramidal side effects, withdrawal of substandard/falsified medications, Isoniazid Preventive Therapy related hepatic injury, and introduction of allergy notification cards in hospitals. According to the respondents, all these examples were believed to have resulted in reduced risks related to ADRs, associated morbidities and mortalities, and ultimately improvements in the overall quality of patient care. One respondent explained the impact of the EPC integration as:
Pharmacovigilance, as a department, has heightened the public confidence in the healthcare system, ensured a better livelihood for people, and reduced the incidence of adverse effects of drugs through identification and withdrawal of substandard and falsified medical products. It has also played an immense role in the development of national health guidelines. [C]
The respondents believed that the EPC has also enhanced the awareness level of physicians and has energized every physician to be vigilant in his/her practice. They said that the physicians have developed the habit of close patient follow-up and being on the watch for the incidence of any ADRs. One respondent added that the EPC has brought about changes in prescribing practices, especially in the cases of pediatric dose calculations. This particular impact was reported as:
The pharmacovigilance center has increased the awareness of healthcare providers, especially the EPI focal persons. It has sensitized them to work beyond just vaccinating children but also following them up, and educating mothers about adverse events following immunization. The enhanced awareness has increased in the general public as well. [I]
In terms of quality, some respondents highlighted that the establishment of EPC has enhanced the quality of services and products provided in the healthcare system. They claimed that the center has strengthened the overall activities of the national regulatory agency, which had added quality to the services provided. The notable example mentioned was the detection of false negative results with malaria rapid diagnostic tests. Another respondent stated that the presence of EPC in the healthcare system has also financially benefited the country as management of ADRs consumes resources.
Facilitating Factors for Integration
The respondents stated that several facilitating factors have played essential roles in the integration process. The characteristic/peculiar work culture of the EPC was mentioned as one facilitating factor for the success of the center in integrating its role in the healthcare system. The dedication, motivation, efficiency, and competency of the staff, the good organization, and the participatory environment created within the center were among the most mentioned organizational characteristics. A respondent commented on this as follows:
The department is exemplary, and I have a good impression on the department. It has good management, work division, and skilled people. I like the positive and participatory environment which opens doors to enhance the skill and experience of every employee. [A]
Support from the stakeholders was also vital for the integration as per the respondents. They mentioned financial support from stakeholders such as the Global fund, Global Alliance for Vaccines and Immunization (GAVI), and the WHO; support from PHPs in conducting training and workshops, and development of reporting tools and guidelines; availability of international linkages such as with the Uppsala Monitoring Center (UMC) as enabling factors for the integration.
On the other direction, some respondents claimed that the support offered by the EPC to the stakeholders was another facilitating factor for integration. They said that continuous training provided to enhance the awareness level of healthcare professionals and the close follow-up and supervision of activities have played an important role in integration. The quality of training offered by the center, and the presence of trained focal persons at sub-national levels were also other ingredients for the successful implementation and integration of the system in health facilities. As a unique character, the respondents explained that the center’s unceasing support, through motivating healthcare professionals to report ADRs and recognizing their contribution by various means, has accelerated and sustained the integration at health facilities. A respondent clarified this as follows:
The pharmacovigilance center recognizes and motivates healthcare workers, even those in remote health facilities, by sending certificates of recognition/acknowledgment letters and others. They also document and share findings. [H]
Some respondents disclosed that the enabling environment in the regulatory authority, under which the EPC operates, was a key factor for its performance. The structure of the regulatory authority, as it directly reports to the Minister, and the organization within the unit are essential facilitators as per the respondents. One respondent explained the role of the director of the Eritrean medicines regulatory authority, the National Medicines and Food Administration (NMFA) as:
The director of the NMFA has created an enabling environment for the pharmacovigilance center including encouraging and giving the staff opportunities for capacity building and training across the country, and as such much progress has been witnessed. [J]
Limiting Factors for Integration
Even though the integration is boosting, the participants stated that there exist some factors that limit the successful integration. The respondents reflected the inconsistency of the communication between the EPC and the PHPs as a major limitation. They stated that there are no regular meetings and continuous supervisions/follow-ups, and currently the meetings only take place with occurring issues/events. One respondent put the limitation as:
The drawback that exists in the way the center is communicating and discussing the reports is a limiting factor. The programs should not be notified at the end but rather be involved in the process of ADR investigations, particularly those related to program medicines. Currently, there is no regular meeting and I recommend there should be one, at least biannually. [A]
Some respondents claimed that the absence of a concrete communication system and known platforms to keep abreast of the progress has resulted in inadequate communication. They added that the EPC has generated a lot of information and knowledge, yet there has been no established platform to inform the PHPs in a timely manner. They also mentioned that there are no monthly updates regarding the safety of medicines with the publication time of the medicine information bulletin - A bulletin prepared by the NMFA in collaboration with the Pharmacy Service Division of the Department of Public Health to disseminate medicine-related information - being too irregular.
Moreover, the lack of transparency and sharing of ADR reports with the programs was also mentioned as a barrier to integration. One respondent presented the drawback regarding data accessibility as:
Another expectation we had is regarding the data accessibility. The reports come from health facilities all over Eritrea, and the center acts as an ADR data bank but how do you access the data is the question. There is a need for a clearly stated data access/share policy and strategies to protect sensitive data. [F]
The majority of the respondents disclosed the lack of periodic training, to raise the awareness of healthcare professionals, is a drawback of the EPC. They further explained that the lack of continuous training has resulted in reduced quality of reporting; and as such recommended continuous training to new recruits, owing to the high staff turnover the healthcare system is facing. There is also a need for regular sensitization of the frontline healthcare workers and community health agents to make them understand the importance of regular reporting of ADRs. One participant summarized as follows:
The pharmacovigilance center used to train health professionals before they got deployed, and this gave us continuity in our practice. As there is high staff turnover, it is necessary to maintain continuity. If a new recruit is going to get to the same knowledge level as the experienced ones, he/she needs training right-off college or the time they get assigned to their workplaces. [E]
Limitations in healthcare services and personnel were also mentioned as barriers to effective integration. Some of the respondents said that the PHPs are dormant in terms of being vigilant for ADRs. They also added that physicians are not fully motivated and not sending constant reports to the center. They supported their argument by stating that only a few numbers of healthcare workers are constantly reporting ADRs. Pharmacists, who should oversee the availability of reporting forms and problems in filling the forms, were also blamed for not being committed to taking responsibility for this role. One participant explained the limitation of healthcare personnel as:
The physicians, including the specialists, are equipped with adequate knowledge, and they play the greatest role in providing care for critical patients and follow-up of in-patients for long durations. Despite practicing in hospitals with good laboratory provisions and having in-depth knowledge, they are not motivated to report the ADRs they encounter throughout their practice. [H]
Several respondents commented that the absence of a focal person across different levels of the healthcare system to work closely with the EPC was a limiting factor of the integration. One respondent further highlighted the need for establishing zonal pharmacovigilance centers, having at least one dedicated focal person with the same knowledge and level of exposure as that of the EPC, to facilitate the programs.
The budget constraint was also mentioned as a limiting factor for the integration of the pharmacovigilance system by some respondents. They said that the unavailability of a budget to conduct supervision and consistent training was limiting the center to realize greater success.
Discussion
In this study, the critical standpoints of the EPC stakeholders concerning the integration of pharmacovigilance in the Eritrean healthcare system have been aggregated into 4 main themes and 17 subthemes. These themes produced a vivid picture of the level of integration of EPC along with its impact, and the facilitating and limiting factors of the integration, through the eyes of the EPC stakeholders.
According to the findings of this study, the EPC has shown promising integration with the major PHPs, especially with EPI, the National Malaria Control Program, HIV and STI Control program, and the National TB and Leprosy Control program. Although the importance of pharmacovigilance in improving patient care and public health is undeniable, its integration into public healthcare remains a challenge in many countries.9,11 A study conducted by Ampadu et al reported that most national pharmacovigilance centers in African countries have been successful in integrating with some but not all PHPs.9 In this respect, the EPC has been determined to integrate pharmacovigilance systems into the PHPs over the last few years.15 The integration of pharmacovigilance activities such as reporting of AEFI and effective communication to tackle immunization-related safety issues with EPI, in particular, has been commendable as it was built upon the already standing EPI system which involved the utilization of the existing EPI focal persons at all levels of the healthcare system and sustainable financial support through funds. This signifies that pharmacovigilance activities in PHPs can function optimally if they operate in an existing strong infrastructure of the health programs.7,22 The successful integration of the EPC with EPI should be emulated in other health programs, especially with the National Blood Bank, Health Promotion, Non-Communicable Disease Control, Academia; pharmaceutical industries, healthcare consumers, and patient representatives as integration does not exist at present. These findings were similar to those reported by Ampadu et al9 and Adenuga Bafanso et al.11
Moreover, the relationship between the EPC and major PHPs has been described as mutual, a relationship that has resulted in the attainment of great accomplishments that boosted both the EPC and the involved PHPs. Such an association has resulted in the identification of significant safety signals,23–26 including but not limited to findings of false positive results using Malaria Rapid Diagnostic Test (RDT) due to genetic mutation23 and extrapyramidal adverse effects related to Artesunate/ Amodiaquine therapy.24 Moreover, in collaboration with the EPI, the EPC has been able to document around 1000 AEFIs and 3600 AEFIs during the Measles and Rubella, and Meningococcal-A Vaccine vaccination campaigns respectively.15 Similarly, in collaboration with the Neglected Tropical Diseases (NTD) control program, the EPC has collected 2579 adverse events (as of September 28, 2019) related to mass administration of Praziquantel, which accounted for 65% of all such reports in VigiBase.15 Such achievements, especially those attained through the collaboration with Communicable Disease Control Division (CDCD), may have resulted due to the reciprocal efforts of the EPC and the programs during the development of strategic plans and conduction of training. Similarly, a study conducted by Garashi et al reported that collaboration between national centers and other stakeholders during policy development and that training provided by members of the national centers are facilitating factors for a successful pharmacovigilance system implementation.27
The findings of the study have also demonstrated that there are several limiting factors that could hinder an effective integration; one of which is the inconsistent communication between the EPC and the major PHPs. In this study, it was found that the communication system of the EPC has a weak point in terms of being fragile with no regular mechanism of information exchange. Similarly, the absence of effective communication as a limiting factor for integration has been reported in other Sub-Saharan African countries.6,28 Effective operation of a pharmacovigilance center necessitates the exchange of information with stakeholders4 and coordination of such exchange through the identification of mechanisms to communicate the information to link medicines safety with healthcare practices and health policies.29 In this respect, a regular platform involving annual conferences, regular biannual or quarterly meetings, and consistent publication of the medicines bulletin should be established by the EPC to correct the existing inconsistent and ad hoc communications. Such regular flow and exchange of information would place the center in a position to identify gaps and prepare health programs for better drug monitoring and management of drug-related issues.10
In line with the inconsistent communications, the participants have highlighted the absence of data-sharing mechanisms and policies to allow PHPs to gain access to gathered ADR reports for research and other purposes. All ADR and AEFI reports, gathered from healthcare professionals all over the country through spontaneous reporting are, however, held confidential and entered into an international database, the VigiBase by the EPC only.14 According to the UMC data privacy policy, UMC only grants access to those services with a valid user agreement, and transfer of entered data to third parties is generally prohibited.30,31 The EPC is the only center that has a valid user agreement to enter data into the VigiBase; hence it solely takes the responsibility of entering ADR and AEFI reports to VigiBase.14 However, through the establishment of regional pharmacovigilance centers, having their own data entry units, the partners could access the data by signing a user contract agreement with the UMC.30 Hence, to promote transparency and allow PHPs and health facilities first-hand access to pharmacovigilance data, the EPC should work towards creating regional pharmacovigilance centers. Moreover, the PHPs and zonal medical offices can gain access to aggregated and analyzed reports from the EPC in an event where safety signals have been identified (Eritrean Pharmacovigilance Center Archives, unpublished data, 2012–2020) or utilize VigiAccess.32 Therefore, the EPC should work to systematically counteract the negative perception of the PHPs regarding data use as this perception might hinder a successful integration.
With respect to training and pharmacovigilance sensitization, the findings of the study have indicated that the training provided by the EPC is inconsistent and not targeted to the lower healthcare professionals. The EPC has developed standardized basic and advanced training courses and manuals to train health professionals and equip them with pharmacovigilance knowledge before they get deployed to their practice areas.15 This being said, continuous and refresher courses, however, are not given to those healthcare professionals who have taken the basic courses as well; this can have a negative impact on ADR vigilance, the number of ADR reports from healthcare professionals, and ultimately on patient safety. Therefore, to address the training issues, the EPC should regularize the formal training and supportive supervision, and incorporate pharmacovigilance courses into the curriculum of medical and health science colleges.12,28,33
The participants have also highlighted a decreased motivation of physicians in major hospitals to report ADRs as a barrier to integration. This opinion, however, contradicts the findings of the study conducted by Araya et al, in 2017. In that study, physicians were found to be the major reporters among other healthcare professionals, and almost 70.8% of the physicians claimed to have reported ADRs to the EPC. The study further reported that 91% of the healthcare professionals involved in the study believed that reporting ADRs does not negatively affect their professional practice.17 To sustain healthcare professionals’ motivation in reporting ADRs, the EPC sends quick feedback to each reporter and recognizes the best reporters with awards.15 Hence, to sustain the overall healthcare professionals’ motivation to remain vigilant for ADRs and increase the number of ADR reports coming to the EPC, there should be regular follow-up and supervision. This approach has also been shared as a successful strategy by the Democratic Republic of Congo’s experience in implementing pharmacovigilance systems.5
The respondents have further highlighted the need for continual input from the EPC, through the designation of pharmacovigilance focal persons and zonal pharmacovigilance centers, to fuel healthcare professionals and health programs to remain active in performing vigilance activities. In support of this, a study conducted by Stegmann et al highlighted that having clinicians and pharmacists as pharmacovigilance focal points could be advantageous as they could have a motivating influence on the healthcare system.28 Currently, the EPC relies on zonal pharmaceutical services to carry out pharmacovigilance activities in terms of collecting and sending ADR reports, organization of training activities, communication of findings, and other liaisons. Such reliance, however, cannot be sustained as there is high staff turnover and poor follow-up of their performance. As such, there is a need to establish a decentralized system that entails the presence of officially assigned focal persons with defined responsibilities, both in the national health programs and the zonal health facilities.34 Hence, the EPC should work towards creating a pool of trained focal persons in respective zones at all levels of the healthcare system. A system should also be established whereby the EPC could follow up and supervise the focal representatives in a timely manner.
Overall, insights into the stakeholders’ perspectives have identified key gaps for targeted intervention to ensure effective integration of the EPC in the healthcare system. Thus, the EPC in conjunction with the Ministry of Health has to make concerted efforts to promote pharmacovigilance activities and advocate the incorporation of pharmacovigilance training into the curricula of health science students.28,33 In addition, there is a need for a policy framework, incorporating communication and decentralization strategies to ensure sustainable integration of the pharmacovigilance system at the PHPs and health facilities.35
Finally, the main limitation of the study was that, even though an inductive analysis approach was followed, the interview questions used might have shaped the generated themes.
Conclusions
This research has demonstrated that the integration of EPC in the healthcare system is satisfactory. The center needs to work towards integrating with some stakeholders of the healthcare system, particularly the National Blood Bank, Health Promotion Center, Non-communicable Disease Control Division, Academia, pharmaceutical companies, healthcare consumers, and patient representatives. To ensure effective integration of pharmacovigilance in the entire healthcare system, the EPC should expand its systems to unreached PHPs for a more descended integration; regularize training and communications and correct any existing misperceptions with regards to sharing pharmacovigilance data with PHPs.
Abbreviations
ADR, Adverse Drug Reactions; CDCD, Communicable Disease Control Division; COREQ, Consolidated Criteria for Reporting Qualitative Research; EPC, Eritrean Pharmacovigilance Center; EPI, Expanded Program on Immunization; GAVI, Global Alliance for Vaccines and Immunization; HIV, Human Immunodeficiency Virus; ICSRs, Individual Case Safety Reports; NMFA, National Medicines and Food Administration; NTD, Neglected Tropical Diseases; PHPs, Public Health Programs; RDT, Rapid Diagnostic Test; STI, Sexually Transmitted Infection; UMC, Uppsala Monitoring Center; UN, United Nations; WHO, World Health Organization.
Acknowledgments
The authors would like to thank all the participants who agreed to be interviewed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jeetu G, Anusha G. Pharmacovigilance: a worldwide master key for drug safety monitoring. J Young Pharmacist. 2010;2(3):315–320. doi:10.4103/0975-1483.66802
2. Dal Pan GJ. Ongoing Challenges in Pharmacovigilance. Drug Saf. 2014;37:1–8. doi:10.1007/s40264-013-0123-x
3. Suke SG, Kosta P, Negi H. Role of Pharmacovigilance in India: an overview. OJPHI. 2015;7(2):e223. doi:10.5210/ojphi.v7i2.5595
4. Swain S, Patra CN. Impact of pharmacovigilance in healthcare system: regulatory perspective. Pharmaceut Reg Affairs. 2014;3:5. doi:10.4172/2167-7689.1000e143
5. Nzolo D, Kuemmerle A, Lula Y, et al. Development of a pharmacovigilance system in a resource limited country: the experience of the Democratic Republic of Congo. Ther Adv Drug Saf. 2019;10:1–10. doi:10.1177/2042098619864853
6. Akarowhe K. A case study of pharmacovigilance in Nigeria: challenges and solutions. AJBSR. 2020;10(1). doi:10.34297/AJBSR.2020.10.001470
7. Kiguba R, Olsson WC, Waitt C. Pharmacovigilance in low-and middle-income countries; A review with particular focus on Africa. Br J Clin Pharmacol. 2023;89:491–509. doi:10.1111/bcp.15193
8. Isah AO, Pal SN, Olsson S, Dodoo A, Bencheikh RS. Specific features of medicines safety and pharmacovigilance in Africa. Ther Adv Drug Saf. 2012;3(1):25–34. doi:10.1177/2042098611425695
9. Ampadu H, Hoekman J, Arhinful D, et al. Organizational capacities of national pharmacovigilance centres in Africa: assessment of resource elements associated with successful and unsuccessful pharmacovigilance experiences. Global Health. 2018;14:109. doi:10.1186/s12992-018-0431-0
10. Elshafe S, Roberti AM, Zaghloul I. Pharmacovigilance in developing countries (part II): a path forward. Int J Clin Pharm. 2018. doi:10.1007/s11096-017-0588-2
11. Adenuga AB, Kibuule D, Bamitale SDK, Rennie WT. Effective integration of pharmacovigilance systems at public health facilities in resource-limited settings: a qualitative study. RSAP. 2020;16(8):1111–1116. doi:10.1016/j.sapharm.2019.11.010
12. Adenuga AB. Embracing the changing needs for pharmacovigilance in Africa. Pharmacovigilance. 2023;2. doi:10.5772/intechopen.106356
13. Alshmmari TM, Mendi N, Alenzi KA, et al. Pharmacovigilance systems in Arab Countries: overview of 22 Arab Countries. Drug Safety. 2019;42:849–868. doi:10.1007/s40264-019-00807-4
14. The State of Eritrea- Ministry of Health. Eritrean National Pharmacovigilance Policy. Asmara, Eritrea: Ministry of Health; 2014.
15. Russom M, Bahta I, Debesai M. Eritrean Pharmacovigilance system: key strategies, success stories, challenges and lessons learned. Drug Saf. 2021;44:1021–1032. doi:10.1007/s40264-021-01102-x
16. Uppsala Monitoring Centre. The Master key to Eritrea’s signal detection success. Uppsala, Sweden: Uppsala Reports; 2020. Available from: https://www.uppsalareports.org/articles/the-master-keyto-eritrea-s-signal-detection-success/.
17. Araya N, Yemane D, Andegiorgish AK, Bahta I, Russom M. Diffusion of pharmacovigilance in the Eritrean healthcare system: a cross-sectional study. J Pharmacovigil. 2019;7(2):277. doi:10.35248/2329-6887
18. Pharmacovigilance and Medicines Information Control Unit, Pharmaceutical Information Unit. Medicines Information Bulletin Volume 30. Asmara, Eritrea: National Medicines and Food Administration; 2019.
19. Adenugaa AB, Aluvilua A, Olafusib OO, Kibuule D. Effective stakeholder analysis and engagement: a vital strategy for enhanced pharmacovigilance systems in sub-Saharan Africa. Iberoamericanjm. 2020;03:134–136. doi:10.5281/zenodo.3744977
20. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi:10.1186/1471-2288-13-117
21. Tong A, Sainsbury P, Craig J. Consolidated Criteria for Reporting Qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Intqhc. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. World Health Organization. The safety of medicines in public health programs: pharmacovigilance an essential tool. Geneva, Switzerland: World Health Organization; 2006. Available from: https://www.who.int/medicines/areas/quality_safety/safety_efficacy/Pharmacovigilance_B.pdf.
23. Berhane A, Russom M, Bahta I, Hagos F, Ghirmai M, Uqubay S. Rapid diagnostic tests failing to detect Plasmodium falciparum infections in Eritrea: an investigation of reported false negative RDT results. Malar J. 2017;16:105. doi:10.1186/s12936-017-1752-9
24. Russom M, Tesfai D, Gebregiorgis S, et al. Artesunate/amodiaquine-induced acute extrapyramidal reactions in children and younger adults: case series assessment. Drug Saf. 2016;39:763–768. doi:10.1007/s40264-016-0429-6
25. Russom M, Debesai M, Zeregabr M, Berhane A, Tekeste T, Teklesenbet T. Serious hepatotoxicity following use of isoniazid preventive therapy in HIV patients in Eritrea. Pharmacol Res Perspect. 2018;6:e00423. doi:10.1002/prp2.423
26. Russom M, Berhane A, Debesai M, et al. Challenges of hepatotoxicity associated with Isoniazid preventive therapy among people living with HIV in Eritrea. Adv Pharmacoepidemiol Drug Saf. 2019;8:2. doi:10.35248/2167-1052.19.8.228
27. Garashi HY, Steinke DT, Schafheutle EI. Qualitative exploration of pharmacovigilance policy implementation in Jordan, Oman, and Kuwait using Matland’s ambiguity-conflict model. Global Health. 2021;17:97. doi:10.1186/s12992-021-00751-y
28. Stegmann JU, Jusot V, Menang O, et al. Challenges and lessons learned from four years of planning and implementing pharmacovigilance enhancement in sub‑Saharan Africa. BMC Public Health. 2022;22:1568. doi:10.1186/s12889-022-13867-6
29. Davies N. Successful Pharmacovigilance: harnessing Relationships between Stakeholders. Reuters Events; 2015. Available from: https://www.reutersevents.com/pharma/clinical/successful-pharmacovigilance-harnessing-relationships-between-stakeholders.
30. Uppsala Monitoring Centre. Privacy Policy. Uppsala Monitoring Center website. Available from: https://www.who-umc.org/media/165706/privacy-policy-12-external_2020.pdf.
31. Uppsala Monitoring Center. Accompanying statement to data released from VigiBase, the WHO international database of suspected adverse drug reactions. Available from: https://bmjpaedsopen.bmj.com/content/bmjpo/1/1/e000039/DC1/embed/inline-supplementary-material-1.pdf?download=true.
32. Shankar PR. VigiAccess: promoting public access to VigiBase. Indian J Pharmacol. 2016;48(5):606–607. doi:10.4103/0253-7613.190766
33. Reumerman M, Tichelaar J, Piersma B, Richir MC, Agtmael MA. Urgent need to modernize pharmacovigilance education in healthcare curricula: review of the literature. Eur J Clin Pharmacol. 2018;74:1235–1248. doi:10.1007/s00228-018-2500-y
34. Uppsala Monitoring Centre, WHO Collaborating Centre for International Drug Monitoring. Safety monitoring of medicinal products: guidelines for setting up and running a pharmacovigilance centre. Uppsala, Sweden: Uppsala Monitoring Center; 2000. Available from: https://www.who-umc.org/media/1703/24747.pdf.
35. Khan MAA, Hamid S, Khan SA, Sarfraz M, Babar ZUD. A qualitative study of stakeholders’ views on pharmacovigilance system, policy, and coordination in Pakistan. Front Pharmacol. 2022;13:891954. doi:10.3389/fphar.2022.891954
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.