Back to Journals » Risk Management and Healthcare Policy » Volume 19
Stakeholder Perspectives on the Adaptability of Hospital Drug Formularies to Disease Patterns: A Modified Q-Methodology Study in Vietnam
Authors Chuc MH ![]() , Tran TT
, Tran TT ![]() , Ha HA
, Ha HA ![]()
Received 17 March 2026
Accepted for publication 24 May 2026
Published 4 June 2026 Volume 2026:19 607810
DOI https://doi.org/10.2147/RMHP.S607810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Mai-Hien Chuc,1,2 Thi-Thuan Tran,1 Hai-Anh Ha1,3
1Faculty of Pharmacy, College of Medicine and Pharmacy, Duy Tan University, Da Nang, Vietnam; 2Department of Pharmacy, Military Hospital 7B, Dong Nai, Vietnam; 3Faculty of Pharmacy, Da Nang University of Medical Technology and Pharmacy, Da Nang, Vietnam
Correspondence: Hai-Anh Ha, Faculty of Pharmacy, Da Nang University of Medical Technology and Pharmacy, Da Nang, 550000, Vietnam, Email [email protected]
Background: Hospital drug formularies function within Complex Adaptive Systems (CAS), where the alignment between drug supply and disease patterns is critical for patient care and cost-effectiveness. However, measuring this responsiveness is challenging due to conflicting stakeholder priorities and a lack of standardized assessment tools.
Objective: This study aims to analyze the perspectives of three key stakeholder groups — clinical providers, non-clinical service providers, and policymakers — to develop a consensus-based set of indicators for monitoring the adaptability of drug formularies in Vietnam.
Methods: We employed a modified Q-methodology approach involving 69 experts (20 non-clinical, 28 clinical, and 21 policymakers). A Q-set of 92 indicators across 9 criteria was developed. Participants evaluated these indicators using a 5-point Likert scale to determine levels of consensus and discordance, rather than a orced-distribution sort, to assess the absolute importance of adaptability metrics.
Results: Most criteria achieved consensus with a Mean > 4.0, particularly for “Usage” and “Storage” adaptations. However, significant discordance was observed regarding “Drug availability”, “Procurement”, and “Outputs and outcomes”. Notably, the correlation for “Outputs and outcomes” between non-clinical and policy stakeholders was statistically weak (r=0.09, p=0.356), highlighting a profound strategic gap.
Conclusion: The study proposes a management framework that monitors drug list adaptability across four levels: non-adaptive, passive, active, and advanced adaptive. Success requires enhanced collaboration between specialized teams and a shift from efficiency-based to resilience-based performance metrics.
Keywords: complex adaptive systems, drug formulary, supply chain adaptability, stakeholder analysis, modified Q-methodology, Vietnam
Introduction
Hospital drug formularies and supply chain operations are primary agents within the healthcare system-a complex adaptive system (CAS),1 designed to optimize patient care through the safe, appropriate, and cost-effective use of medicines.2 As a CAS, the healthcare environment involves multiple subsystems of interconnected actors,3 including physicians, patients, suppliers, and regulators, whose relationships co-evolve and require careful management.4 Consequently, decision-making in this context is not linear but relies on the storage, retrieval, and processing of knowledge from various stakeholders to support adaptive decisions.5
The management of these systems faces significant challenges. The pharmaceutical supply chain is heavily influenced not only by demand fluctuations but also by rigid health system regulations and the inherent risks of drug supply operations.6 In the public sector, the lack of internal cost pressure often leads to inefficiencies, such as slow demand forecasting and poor coordination between supply and demand.1,7 Furthermore, conventional performance metrics typically focus on efficiency, overlooking critical factors like sustainability, flexibility, and responsiveness, key components of the emerging Industry 5.0 paradigm.8,9
While recent literature has emphasized supply chain resilience (the ability to recover from disruptions),10,11 there is a distinction between resilience and adaptability.12 Adaptability refers to the capacity to evolve continuously without disruption, ensuring the availability of medicines through proactive adjustments.13 Currently, there is a lack of comprehensive tools to monitor and evaluate the specific adaptability of drug formularies to changing disease patterns. Existing frameworks often suffer from limited stakeholder engagement, which undermines the adaptive capacity of health systems.4,14,15
Since stakeholders hold varying and often conflicting perspectives on what constitutes “value” or “efficiency” in drug supply, it is essential to capture these diverse viewpoints.14 A robust evaluation framework must be flexible enough to incorporate these conflicts and guide decision-making toward a balance between maximizing benefits and minimizing adverse impacts.16
To capture the diverse and often conflicting viewpoints inherent in such complex systems, this study adopts a modified Q-methodology. Unlike the traditional approach which relies on a forced-distribution ranking, this improved design utilizes Likert-scale evaluations to assess the absolute importance of metrics while identifying nuanced levels of consensus and discordance among stakeholders. By addressing the conceptual limitations of conventional sorting, this research aims to: (1) analyze stakeholder perspectives on the adaptability of drug formularies to disease patterns; and (2) provide management implications for enhancing pharmaceutical supply chain performance within the Vietnamese healthcare context.
Materials and Methods
Study Design
A modified Q-methodology was implemented through a cross-sectional survey design to systematically evaluate hospital drug formulary adaptability. While traditional Q-methodology requires a forced-distribution sort to identify relative viewpoints, scholars have noted that such rigid structures may lead to respondent fatigue or the loss of “absolute importance” values when multiple items are perceived as equally significant.17 Consequently, this hybrid approach integrates the rigorous indicator development process inherent in Q-methodology with the quantitative precision of Likert-scale analysis. By transitioning to an independent consensus rating, the design enables a more granular assessment of absolute importance and statistical agreement levels across the identified stakeholder groups, a technique increasingly recognized for its flexibility in complex evaluations.18,19
Development of the Q-Set (Research Instrument)
The “Q-set” (the collection of statements) was constructed based on a comprehensive literature review and expert consultations regarding hospital drug formularies and supply chain adaptability. The development process involved two phases of expert consultation to ensure content validity. Initially, a preliminary set of indicators (Appendix S1) along with the research questionnaire (Appendix Figure S1) were distributed to experts for evaluation and open-ended feedback. Based on the feedback and quantitative scoring from this first round, indicators with low agreement (mean score < 3.5) were removed, and new indicators proposed by experts were added. The refined instrument was then finalized for the official consensus rating (Appendix S2).
The final Q-set comprised 92 indicators categorized into nine key criteria, covering critical aspects including: (1) Adaptive workforce (staffing); (2) Ensuring drug availability requirements; (3); Methods for drug needs assessment; (4) Ensuring legal compliance, (5) Appropriate procurement (ordering); (6) Usage adaptation; (7) Storage adaptation; (8) Risk management; (9) Appropriate outputs and outcomes.
Participant Selection (P-Set)
A purposive sampling strategy was used to select the “P-set” (participants) to ensure diverse representation of the healthcare supply chain ecosystem. In Q-methodology, the primary objective is to capture the full breadth of existing perspectives rather than to achieve statistical generalization to a larger population. Consequently, formal power analysis is not typically required as the methodology focuses on the richness and diversity of viewpoints. The study involved 69 experts (N=69), a size that is considered substantial and robust within the context of Q-methodological research, where a sample of 40 to 60 participants is generally deemed sufficient to identify stable patterns of subjectivity. The participants were divided into three distinct stakeholder groups:
- Non-clinical service providers (NC): N = 20 (pharmaceutical companies, distributors).
- Clinical service providers (CP): N = 28 (hospital pharmacists, doctors, clinical managers).
- Policymakers (PM): N = 21 (health authorities, regulatory bodies).
Data Collection Procedure
This study engaged experts solely in their professional capacity to provide opinions on management indicators. All participants were adults aged between 27 and 60 years; no minors were involved. This study is part of an institutional research project conducted at Military Hospital 7B, which also serves as the doctoral dissertation research of the first author at Duy Tan University. The study involved no clinical intervention, patient data, or biological samples, engaging experts solely in their professional capacity to provide opinions on management indicators. Consequently, formal ethical approval was waived by the Institutional Review Board in Biomedical Research of Military Hospital 7B, Dong Nai, Vietnam (document: Form 13.HĐĐĐ, reference number: .01…/CN-HĐĐĐ, Date of approval: August 16, 2024), as the study does not fall within the scope requiring ethical approval for biomedical research. The study adhered strictly to the ethical principles of the Declaration of Helsinki.
The data collection was conducted from September 1st 2024 to October 1st 2024 (round 1) and from November 15th 2024 to December 31st 2024 (round 2). Prior to study commencement and any data collection, informed consent was obtained from all study participants. The survey cover letter clearly explained the study’s purpose and the right to refuse or withdraw participation at any time without penalty. Informed consent was implied and documented by the participants’ voluntary completion and return of the written questionnaire.
The data collection followed a rigorous three-step process (Figure 1):
- Q-set construction: Establishing the 92 statements (as described above).
- P-set recruitment: Selecting the 69 experts.
- Modified Q-sort (rating): Instead of sorting cards into a forced distribution curve, participants were asked to rate their agreement with each of the 92 statements on a 5-point Likert scale (1 = Strongly disagree to 5 = Strongly agree). This modification allowed experts to express the absolute importance of multiple high-priority indicators simultaneously, which is often restricted in traditional Q-sorting. Data were entered and independently cross-checked three times to ensure accuracy before statistical processing.
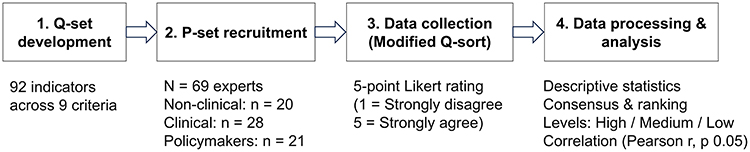 |
Figure 1 Workflow for developing and evaluating adaptability indicators using a modified Q-methodology approach. |
Statistical Analysis
Data were processed using Microsoft Excel, with a primary focus on identifying consensus and discordance through descriptive statistics and correlation analysis. To ensure the robustness of the findings and mitigate potential software limitations, a multi-stage validation protocol was strictly followed. As described in the data collection procedure, all raw data entries were independently cross-checked three times by separate researchers to ensure absolute accuracy.
- Descriptive statistics: Frequencies and mean scores were calculated for each indicator. Normality of the data distribution was assessed using Z-scores for skewness and kurtosis. The results indicated that the data approximated a normal distribution, with Z-values falling within the acceptable range of ±1.96 (at 5% significance level) or ±2.58 (at 10% significance level).
- Consensus and ranking: Indicators were ranked based on mean scores. Consensus was determined by comparing the rankings across the three groups. Items were classified into three adaptability levels based on their scores: High, Medium, and Low.
- Correlation analysis: Pearson correlation coefficients (r) were calculated to examine the relationship between stakeholder perspectives. The correlation was considered statistically significant if the p-value was ≤ 0.05. A strong positive correlation (r close to 1 with p ≤ 0.05) indicated high agreement between groups, whereas a weak correlation or p > 0.05 indicated divergence in perspectives.
Results
Overall Adaptability Ratings and Consensus Levels
The assessment of adaptability across the nine criteria revealed generally positive perceptions among stakeholders, with seven out of nine criteria achieving a mean score above the “Agree” threshold (Mean > 4.0). The criteria “Methods for Determining Drug Needs” (3.96) and “Adaptability Outputs/Results” (3.91) scored slightly lower but remained well above the acceptable threshold of 3.5. Table 1 presents the mean scores and the classification of consensus versus discordance among the three stakeholder groups.
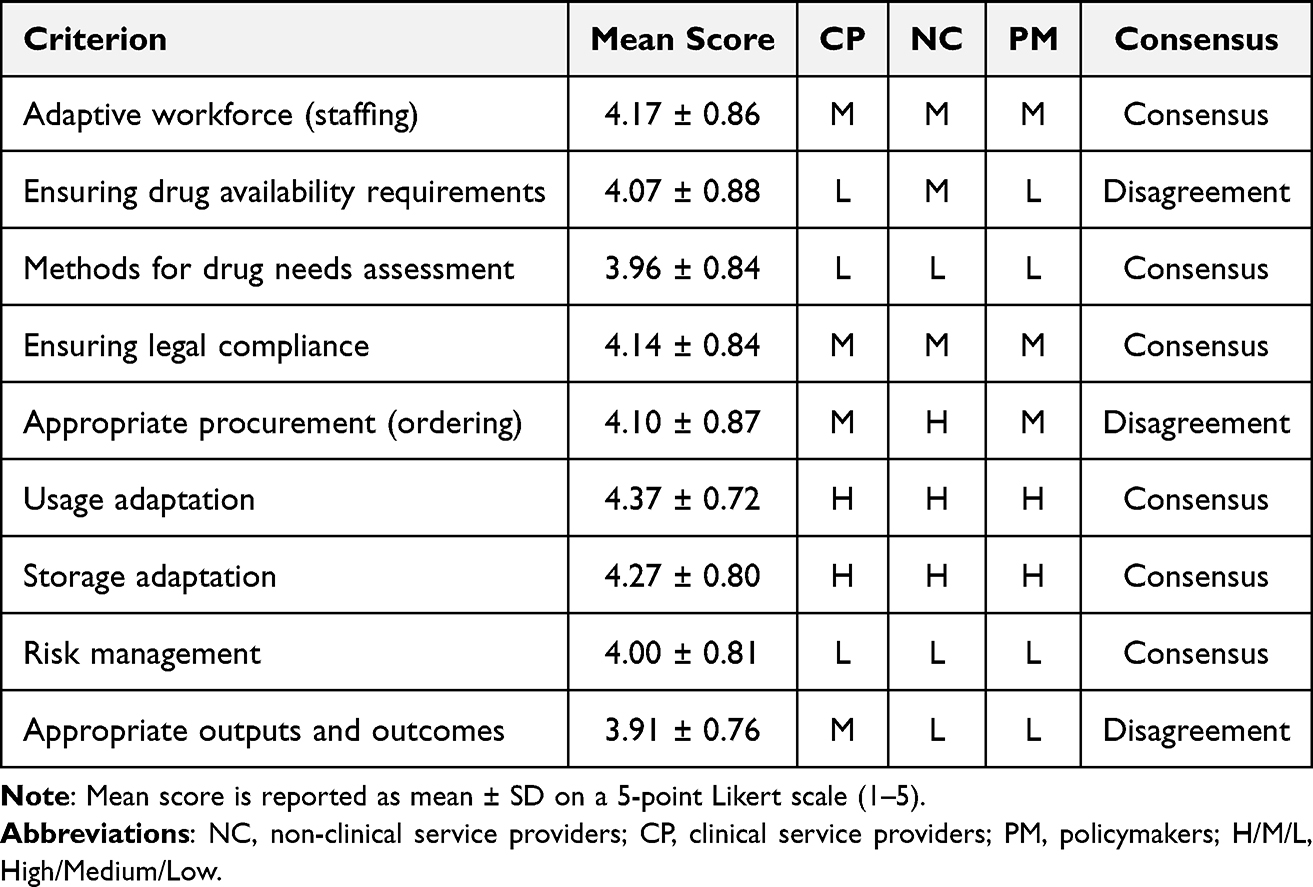 |
Table 1 Perspectives on the Measurability of Adaptability |
The analysis identified distinct levels of consensus. The highest agreement was observed in “Usage Adaptation” and “Storage Adaptation”. This reflects that adaptability is most evident and measurable during the operational stages of drug usage and storage, where reserve calculations and capacity planning are concrete. “Adaptive workforce” and “Ensuring legal compliance” showed medium consensus. Stakeholders recognized these as foundational elements for any adaptive activity. Disagreement was noted in three criteria: “Ensuring drug availability requirements”, “Appropriate procurement” and “Appropriate outputs and outcomes”. While the divergence was not extreme, it highlights varying strategic priorities between providers and policymakers.
Divergence in Stakeholder Perspectives
A deeper analysis of the discordant criteria reveals specific structural conflicts in perspectives (Table 2). Regrading ordering adaptation, the non-clinical service providers (NC) rated “Appropriate procurement” significantly higher (rank 1) compared to the clinical (CP) and policymaker (PM) groups, who ranked it at a medium level (rank 5). This discrepancy suggests that suppliers view proactive ordering as a critical active measure for supply security, whereas hospitals and policymakers tend to view successful ordering as an expected standard duty of the supplier rather than an adaptive achievement.
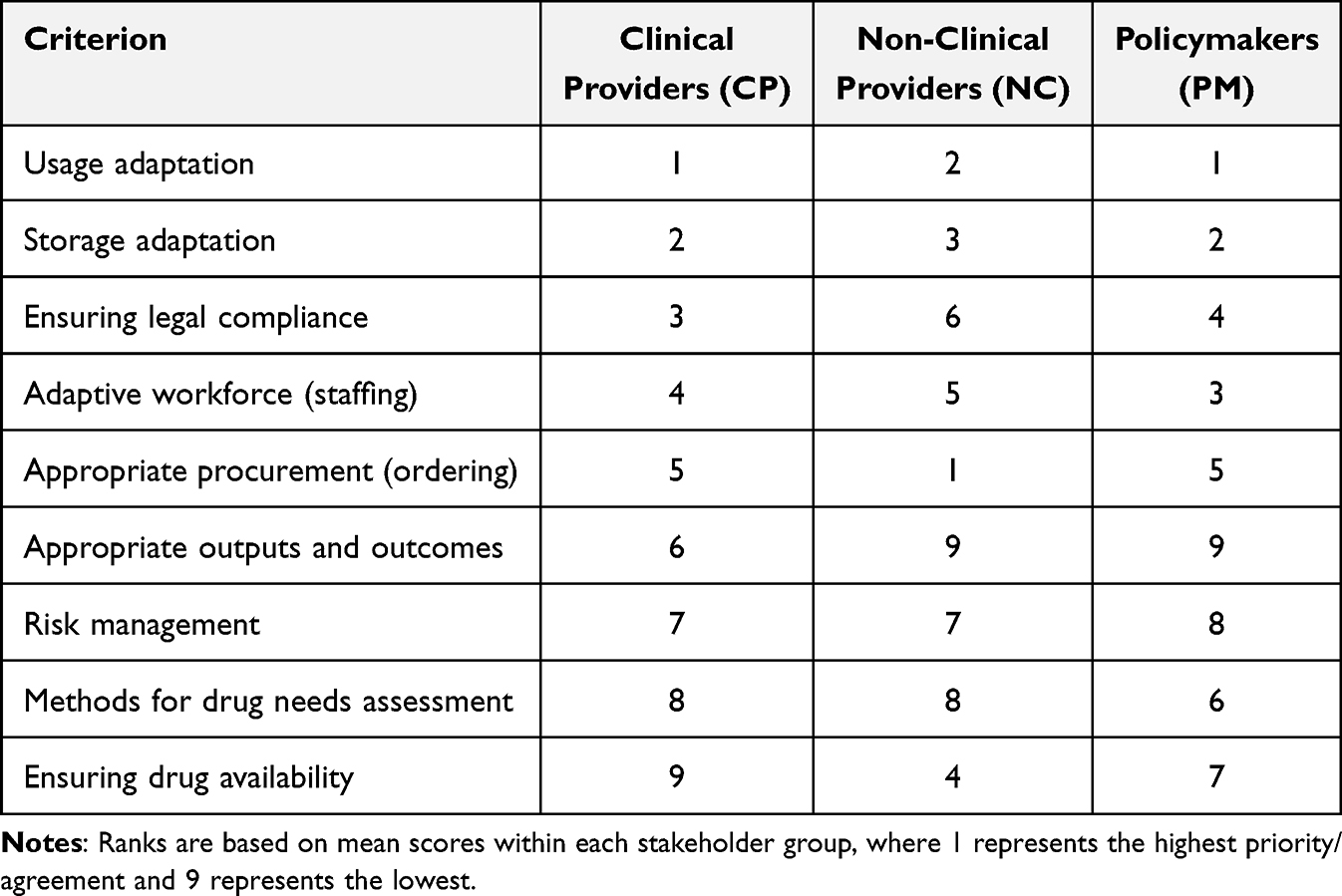 |
Table 2 Rank Matrix of Formulary Adaptability Criteria Across Stakeholder Groups |
In the term of outputs and results: The clinical group placed a higher value on “Appropriate outputs and outcomes” compared to the other two groups. This aligns with the hospital’s direct accountability for treatment outcomes, whereas suppliers and policymakers may focus more on process compliance.
Hierarchy of Views by Stakeholder Group
The ranking of criteria (Q-sort results) varied distinctly across the three groups, reflecting their professional mandates (Table 2). In the views of clinical group, hospital stakeholders focused on operational execution and compliance. Their highest-ranked criteria were Usage (1st), Storage (2nd), and Legal Assurance (3rd). Interestingly, they ranked “Ensuring drug availability” last (9th), possibly indicating that they view availability as a baseline expectation rather than an adaptive variable.
Non-clinical group prioritized logistics and proactive supply management. Their top three criteria were Ordering (1st), Usage (2nd), and Storage (3rd). Conversely, they ranked Risk management and Outputs lowest.
Similar to the clinical group, policymakers prioritized Usage (1st) and Storage (2nd), but placed Human Resources (3rd) higher than other groups. This group ranked Outputs and Results lowest (9th), suggesting a focus on system inputs and processes (HR, Storage) over specific adaptive outcomes in their evaluation model.
Correlation Analysis Between Groups
The Pearson correlation analysis (Table 3) quantifies the degree of alignment between the stakeholder groups. There was a strong and statistically significant correlation regarding “Ensuring legal compliance” (NC-CP: r=0.89; NC-PM: r=0.79) and “Storage adaptation” (NC-CP: r=0.73; CP-PM: r=0.88). This confirms that legal compliance and storage standards are universally understood and agreed-upon pillars of the supply chain.
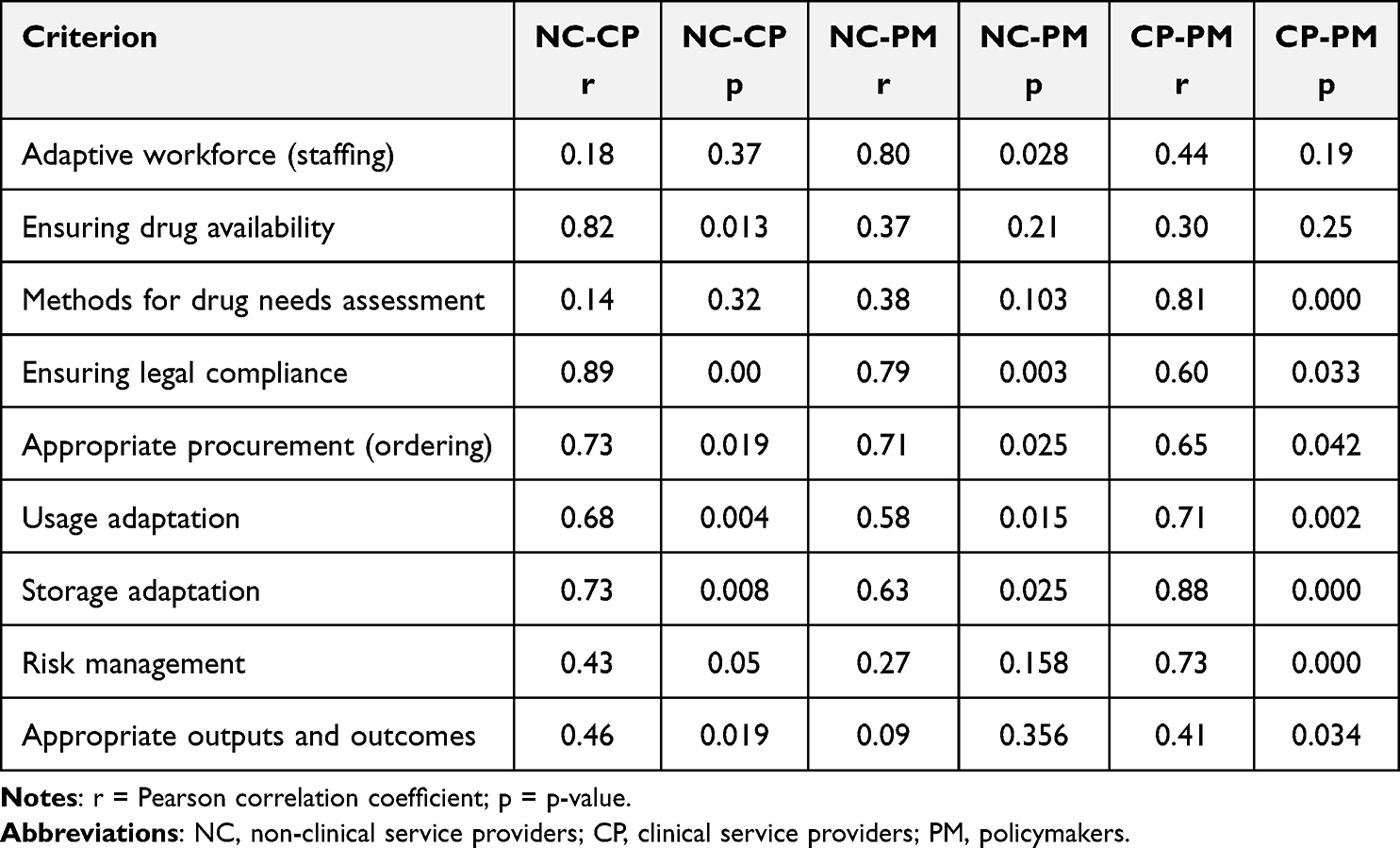 |
Table 3 Correlation Values Between Stakeholder Groups |
In contrast, the correlation for “Appropriate outputs and outcomes” was notably weak, particularly between the NC and PM (r=0.09, p=0.356). This lack of statistical significance reinforces the finding that different stakeholders have fundamentally different definitions of what constitutes a successful “result” in drug adaptability.
Discussion
Interpreting Consensus
The strong alignment observed in operational-level criteria suggests that stakeholders view physical reserves and tangible usage processes as the primary evidence of adaptability. Our findings suggest that stakeholders view physical reserves and tangible usage processes as the primary evidence of adaptability. This supports the work of Ding et al, who identified inventory redundancy and facility redundancy as critical components of a resilient hospital supply chain.20 Similarly, Hart Nibbrig et al emphasize that redundancy provides necessary “buffers”, such as inventory, while flexibility supports adaptability through planning adjustments.21 In the Vietnamese context, where supply disruptions can occur, the reliance on storage as a buffer mechanism is a logical, albeit reactive, adaptive strategy.
Analyzing Discordance
A significant finding of this study is the divergence in perspectives regarding “Appropriate procurement” and “Outputs and outcomes”, which exposes a structural vulnerability in the healthcare supply chain. As illustrated in the Strategic layer (Layer 2) of our proposed framework (Figure 2), there is a profound “strategic disconnect” between the upstream and downstream stakeholders. Non-clinical providers (suppliers) ranked this as their top priority, whereas clinical providers (hospitals) ranked it significantly lower. This discrepancy likely reflects the suppliers’ shift toward modern supply chain management paradigms, such as Industry 4.0 and 5.0. Alidoost et al note that Industry 4.0 technologies facilitate accurate forecasting, planning, and traceability.22 Suppliers, driven by market efficiency, value the proactive nature of “ordering” as a mechanism to manage demand fluctuations. In contrast, hospitals may perceive ordering as an administrative task rather than a strategic adaptive capability. This view is risky; Abdulkadir et al argue that supply chain performance hinges on understanding customer demand and sharing information on ordering times.23 The lack of consensus here suggests a need for better integration. As Ghag et al suggest, moving toward Industry 5.0 requires collaboration between humans and systems to enhance responsiveness.8
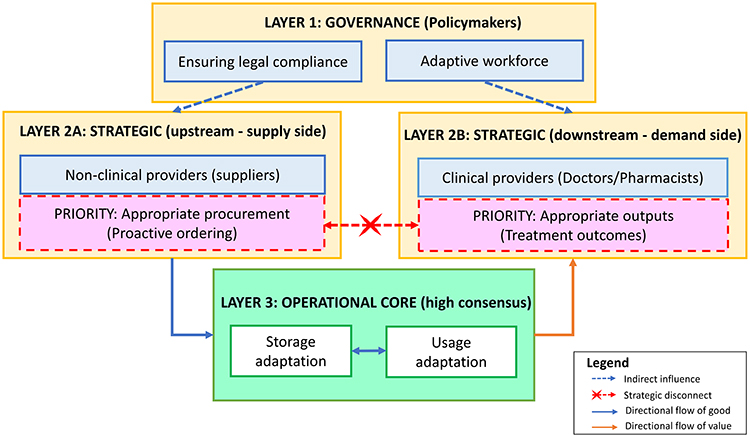 |
Figure 2 A multi-level framework of stakeholder perspectives on formulary adaptability. |
This misalignment validates the CAS theory within the Vietnamese context: different agents (suppliers vs clinicians) operate under distinct internal rules and define “value” differently. The weak correlation observed in “Appropriate outputs and outcomes” (r=0.09, p=0.356) further proves that the “flow of goods” and the “flow of value” are currently decoupled.
While the Operational core (Layer 3) serves as a “shared anchor” with high consensus, our framework suggests that this is a form of passive adaptability. Stakeholders rely on physical buffers (inventory) to bridge the gap because a direct strategic link between supply proactivity and clinical demand is missing. To transition from this reactive state to active adaptability, the Governance layer (Layer 1) must move beyond “indirect regulation”. It requires institutionalizing integrated performance metrics that synchronize supplier proactivity with clinical outcomes, effectively, connecting the red “X” in our model through shared digital ecosystems (Figure 2).
The Human Element in Adaptability
While stakeholders converged on the fundamental role of the workforce, the variation in priority suggests a lack of unified standards for utilizing human resources in adaptive versus routine operations. Khan et al identified “skills and human resource participation” as one of the top three factors impacting pharmaceutical supply chain performance.24 Our study reinforces this, suggesting that specialized teams are essential for building adaptive capacity. However, the variation in ranking implies that while all agree HR is important, there is no unified standard for how HR should be utilized for adaptability versus routine operations.
Managing Complexity and Stakeholder Perspectives
The healthcare system is a complex adaptive system. The discordance found in our study confirms that different agents (doctors, suppliers, policymakers) operate with different internal rules and goals. Petrie argues that communication between these stakeholders is critical for adaptability.25 The divergent definitions of success identified in this study confirm that agents within the healthcare CAS operate under distinct internal rules, hindering synchronized adaptability. Boon et al recommend evaluation frameworks that are detailed enough for specific cases but general enough to allow for cross-case learning.26 The indicators developed in this study provide that necessary common language.
Limitations of the Study
This study has several limitations. First, the uneven distribution of indicators across the nine criteria may have influenced the ranking results, as criteria with fewer indicators might be skewed by extreme values. Second, the study relies on the perceptions of key opinion leaders rather than direct observation of the supply chain processes. Finally, as the study was conducted exclusively in Vietnam, the findings regarding specific regulatory or operational behaviors may require cautious interpretation when generalized to other healthcare contexts.
Furthermore, while the modified Likert-based Q-methodology addresses the limitations of forced distribution, it introduces specific methodological trade-offs that warrant critical consideration. The transition to independent ratings may subject the data to acquiescence bias, where experts tend to assign high scores to most indicators, potentially leading to a “ceiling effect” that obscures the relative priority of statements. Unlike traditional Q-methodology, which is inherently ipsative and forces participants to make difficult trade-offs (more accurately reflecting real-world budget and resource constraints) the Likert approach allows for the simultaneous high prioritization of multiple items. This may result in less distinct factor profiles, necessitating the rigorous use of correlation and discordance analysis to identify meaningful divergent perspectives that might otherwise be masked by high mean scores.
Global Policy Implications and Translatability
Beyond the Vietnamese context, the findings of this study offer a scalable blueprint for enhancing drug formulary adaptability in other healthcare systems, particularly in Low-and-Middle-Income Countries that face similar structural volatilities in pharmaceutical supply chains. As health systems worldwide transition toward the Industry 5.0 paradigm, policymakers can utilize consensus-based indicators to shift from traditional efficiency-driven models to more responsive, value-based healthcare delivery. The 92 indicators developed provide a standardized “common language” that enables international cross-case learning and benchmarking, allowing health authorities to harmonize stakeholder priorities across diverse regulatory and economic environments.
Conclusion and Implications
Conclusion
This study successfully utilized a modified Q-methodology to identify and analyze the diverse perspectives of stakeholders regarding the adaptability of drug formularies within the Vietnamese healthcare context. The results demonstrate a robust consensus on operational functions, specifically storage and usage adaptation, while revealing significant strategic divergence concerning procurement proactivity and clinical outcomes. This misalignment confirms that while the physical flow of medicines remains well-managed, the strategic synchronization between hospital demand and supplier behavior remains a critical challenge. Consequently, addressing this gap requires the institutionalization of integrated performance metrics and shared digital ecosystems to bridge the disconnect between logistics and treatment results.
Implications of the Study
The primary findings directly indicate that hospital drug formularies must transition from a passive administrative list to a strategic tool for proactive adaptation. Because ordering efficiency dictates the quality of care in subsequent cycles, it is essential for hospitals to elevate procurement to a strategic function that leverages Industry 4.0 data-sharing capabilities. Furthermore, the successful application of the modified Q-methodology provides a validated set of 92 indicators that health authorities can immediately employ to monitor system responsiveness under financial and regulatory constraints.
Through a broader interpretation of these results within the framework of CAS, the identified “strategic disconnect” implies a fundamental decoupling between the flow of goods and the flow of value. This suggests that stakeholders currently define system success through distinct internal rules, which hinders the co-evolution of supply and demand. To mitigate this, policy decisions should prioritize narrowing the discordance between stakeholders by placing patient satisfaction at the center of the adaptive process. Such an approach would transform the formulary from a static inventory plan into a dynamic mechanism capable of responding to individualized care needs and modeled disease patterns.
Finally, this research opens significant avenues for future speculation and identifies critical gaps for subsequent studies. While the current framework provides a scalable blueprint for Vietnam, future research should investigate the translatability of these 92 indicators to other low-and-middle-income countries to facilitate international benchmarking. There is also an urgent need to explore how specialized, cross-functional teams can specifically utilize shared digital ecosystems to move beyond passive resilience. Prospective studies should focus on the long-term impact of integrating these adaptive metrics into national health policies to verify their effectiveness in enhancing pharmaceutical supply chain performance globally.
Disclosure
The authors report no conflicts of interest in this work. This paper is available as a preprint on medrxiv at: https://www.medrxiv.org/content/10.64898/2025.12.18.25342605v1.
References
1. Yaroson EV, Breen L, Hou J, Sowter J. Advancing the understanding of pharmaceutical supply chain resilience using complex adaptive system (CAS) theory. Supply Chain Manag Int J. 2021;26(3):323–10. doi:10.1108/SCM-05-2019-0184
2. Goldberg RB. Managing the pharmacy benefit: the formulary system. JMCP. 2020;26(4):341–349. doi:10.18553/jmcp.2020.26.4.341a
3. Gurupur VP. A review on advances in design and development of complex adaptive systems for healthcare using concept maps. Health Technol. 2021;5. doi:10.21037/ht-21-12
4. Franco-Trigo L, Fernandez-Llimos F, Martínez-Martínez F, Benrimoj SI, Sabater-Hernández D. Stakeholder analysis in health innovation planning processes: a systematic scoping review. Health Policy. 2020;124(10):1083–1099. doi:10.1016/j.healthpol.2020.06.012
5. Olazabal M, Galarraga I, Ford J, Sainz De Murieta E, Lesnikowski A. Are local climate adaptation policies credible? A conceptual and operational assessment framework. Int J Urban Sustain Dev. 2019;11(3):277–296. doi:10.1080/19463138.2019.1583234
6. Marrone PV, Mathias FR, Bernardo WM, et al. Decision criteria for partial nationalization of pharmaceutical supply chain: a scoping review. Economies. 2023;11(1):25. doi:10.3390/economies11010025
7. Marube N, Longaray AA, Ensslin L, Ensslin SR, Dutra A. Evaluating supply chain management performance in public health care: an MCDA approach. Pesqui Oper. 2024;44:e275847. doi:10.1590/0101-7438.2023.043.00275847
8. Ghag N, Sonar H, Sawant R, Bankapalli K. Examining industry 5.0 and supply chain performance: an empirical study for managing supply chain complexity. Prod Manuf Res. 2025;13(1):2501181. doi:10.1080/21693277.2025.2501181
9. Kazakov R, Howick S, Morton A. Managing complex adaptive systems: a resource/agent qualitative modelling perspective. Eur J Oper Res. 2021;290(1):386–400. doi:10.1016/j.ejor.2020.08.007
10. Bastani P, Dehghan Z, Kashfi SM, et al. Strategies to improve pharmaceutical supply chain resilience under politico-economic sanctions: the case of Iran. J Pharm Policy Pract. 2021;14(1):56. doi:10.1186/s40545-021-00341-8
11. Apeh CE, Odionu CS, Bristol-Alagbariya B, Okon R, Austin-Gabriel B. Reviewing healthcare supply chain management: strategies for enhancing efficiency and resilience. IJMRGE. 2024;5(1):1209–1216. doi:10.54660/.IJMRGE.2024.5.1.1209-1216
12. Yule EL, Donovan K, Graham J. The challenges of implementing adaptation actions in Scotland’s public sector. Clim Serv. 2023;32:100412. doi:10.1016/j.cliser.2023.100412
13. Ansah EW, Amoadu M, Obeng P, Sarfo JO. Health systems response to climate change adaptation: a scoping review of global evidence. BMC Public Health. 2024;24(1):2015. doi:10.1186/s12889-024-19459-w
14. Dinh TS, Brueckle MS, González-González AI, et al. Stakeholder perspectives on the development and implementation of a polypharmacy management program in Germany: results of a qualitative study. J Pers Med. 2022;12(7):1115. doi:10.3390/jpm12071115
15. Fritz MMC, Rauter R, Baumgartner RJ, Dentchev N. A supply chain perspective of stakeholder identification as a tool for responsible policy and decision-making. Environ Sci Policy. 2018;81:63–76. doi:10.1016/j.envsci.2017.12.011
16. Saesen R, Lejeune S, Quaglio G, Lacombe D, Huys I. Views of European drug development stakeholders on treatment optimization and its potential for use in decision-making. Front Pharmacol. 2020;11:43. doi:10.3389/fphar.2020.00043
17. McKeown B, Thomas D. Q Methodology. SAGE Publications, Inc.; 2013. doi:10.4135/9781483384412
18. Buchholtz N, Vollstedt M. Q methodology as an integrative approach: bridging quantitative and qualitative insights in a mixed methods study on mathematics teachers’ beliefs. Front Psychol. 2024;15:1418040. doi:10.3389/fpsyg.2024.1418040
19. Jiren TS, Kernecker ML, Moroder A. Q methodology. Participatory research methods for sustainability - toolkit #14. GAIA Ecol Perspect Sci Soc. 2025;34(3):171–173. doi:10.14512/gaia.34.3.10
20. Ding B, Yang X, Gao T, Liu Z, Sun Q. Confirmation of a measurement model for hospital supply chain resilience. Front Public Health. 2024;12:1369391. doi:10.3389/fpubh.2024.1369391
21. Hart Nibbrig M, Sharif Azadeh S, Maknoon MY. Adaptive resilience strategies for supply chain networks against disruptions. Transp Res Part E. 2025;200:104172. doi:10.1016/j.tre.2025.104172
22. Alidoost F, Mustafee N, Monks T, Harper A. Simulation in healthcare supply chains with perishable products: a scoping review. J Oper Res Soc. 2025;1–36. doi:10.1080/01605682.2025.2509698
23. Abdulkadir R, Matellini DB, Jenkinson ID, Pyne R, Nguyen TT. Assessing performance using maturity model: a multiple case study of public health supply chains in Nigeria. J Humanit Logist Supply Chain Manag. 2023;14(1):17–70. doi:10.1108/JHLSCM-05-2022-0053
24. Khan SA, Gupta H, Gunasekaran A, Mubarik MS, Lawal J. A hybrid multi-criteria decision-making approach to evaluate interrelationships and impacts of supply chain performance factors on pharmaceutical industry. J Multi-Criteria Decis Anal. 2023;30(1–2):62–90. doi:10.1002/mcda.1800
25. Petrie DA. Integration as innovation in healthcare systems. Healthc Manage Forum. 2025;38(2):76–83. doi:10.1177/08404704241292629
26. Boon E, Body NS, Biesbroek R. Developing and testing an evaluation framework for climate services for adaptation. Clim Serv. 2025;38:100549. doi:10.1016/j.cliser.2025.100549
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.