")
Back to Journals » International Medical Case Reports Journal » Volume 12
St Elevation Myocardial Infarction in a Patient with an Anomalous Right Coronary Artery Originating from the Distal Left Circumflex
Authors Phan NT, Nguyen HT, Nguyen TT , Ly ND, Le NT
Received 25 September 2019
Accepted for publication 3 November 2019
Published 2 December 2019 Volume 2019:12 Pages 379—382
DOI https://doi.org/10.2147/IMCRJ.S232401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Video S1: Aortic root angiographic revealing left main coronary artery arising from left sinus of Valsalva and absent right coronary ostium (LAO 36o – Caudal 7o view)
Views: 251
Nguyen Thao Phan,1 Huy The Nguyen,1 Tran-Thuy Nguyen,1,2 Ngoc Duc Ly,1 Ngoc-Thanh Le1,2
1Department of Cardiovascular and Thoracic Surgery, Cardiovascular Center, E Hospital, Hanoi, Vietnam; 2School of Medicine and Pharmacy, Vietnam National University (VNU), Hanoi, Vietnam
Correspondence: Tran-Thuy Nguyen
Department of Cardiovascular and Thoracic Surgery, Cardiovascular Center, E Hospital, 87–89 Tran Cung, Cau Giay, Hanoi, Vietnam
Email [email protected]
Abstract: A single coronary artery (SCA) is a rare congenital anomaly that occurs in isolation without associated structural heart disease. Reports of a SCA with acute myocardial infarction are very rare in medical literature. This case study examines a patient with a right coronary artery that originated as a branch of the distal left circumflex artery, which had a total occlusion.
Keywords: single coronary artery, coronary congenital anomaly, coronary intervention, myocardial infarction
Case Report
A 56 year-old man (height: 155 cm, weight: 40 kg, BMI: 20) was admitted to our hospital with a history of chest pain lasting for 5 hrs. He was a heavy smoker (20 cigarettes/day for 20 years). He had hypertension but was not diabetic. His family did not have a history of cardiovascular diseases. His cardiac auscultation and peripheral pulses were normal. The baseline electrocardiograms showed ST elevation in leads DII, DIII, and aVF with BAV I, and ST depression in the anterior precordial lead, which was suggestive of an acute transmural posterior wall injury [Figure 1]. The echocardiogram showed hypokinesia of the infero-septum and inferior wall with an ejection fraction of 50%. The serial cardiac enzymes were found to have an elevated level of Troponin T. He was given aspirin 300 mg, clopidogrel 300 mg and enoxaparin 40 mg.
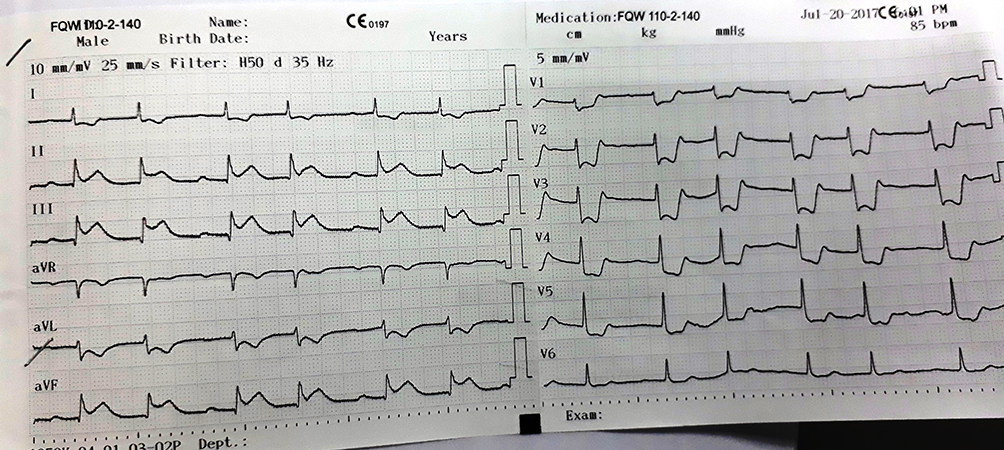 |
Figure 1 An electrocardiogram showing the ST segment elevation in DII, DIII, and aVF, as well as the ST segment depression in V1–V5. |
A coronary angiography was performed using a 5F radial TIG catheter (Terumo Inc., Tokyo, Japan). The left coronary artery angiography revealed a normal left descending artery. However, his left circumflex artery (LCx) was occluded at the midportion [Figure 2]. We were not able to cannulate the right coronary ostium. A right Valsalva sinus angiography and an aortic root angiography were performed to exclude an abnormal take-off of the right coronary artery (RCA) [Video 1, Video 2]. Only a single left coronary ostium arose from the aorta [Figure 3]. The patient’s hemodynamic instability necessitated clinical intervention. The left main coronary artery was engaged with a Launcher EBU 3.5 6F guide catheter (Medtronic Inc., Minneapolis, USA). The lesion was crossed with a light support guidewire 0.014” (Asahi Sion, Asahi Intecc Co., Ltd., Achi, Japan) and then implanted with a 3.0 * 24 mm drug-eluting stent (Yukon Choice stent, Translumina GmbH, Hechingen, Germany) with subsequent TIMI 3 flow distal. The angiographies showed that an additional artery arose from the distal LCx. This artery supplied blood to the right heart chamber and was very similar to the RCA. A review of the angiographic images confirmed an isolated single RCA originating from the distal LCx [Figure 4] [Video 3, Video 4]. The patient recovered successfully after the intervention and was discharged in stable condition after three days.
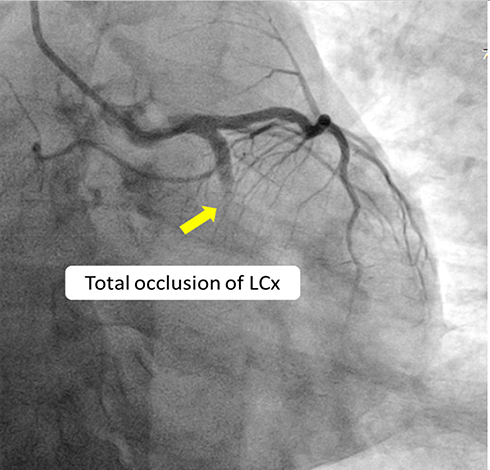 |
Figure 2 A coronary angiographic image showing the total occlusion of the LCx (RAO 12° – Caudal 36°). |
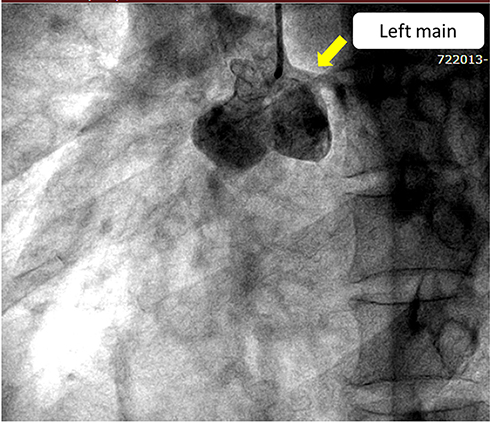 |
Figure 3 An aortic root angiographic image revealing the left main coronary artery arising from the left Valsalva sinus and an absent right coronary ostium (LAO 36° – Caudal 7°) (Video 1). |
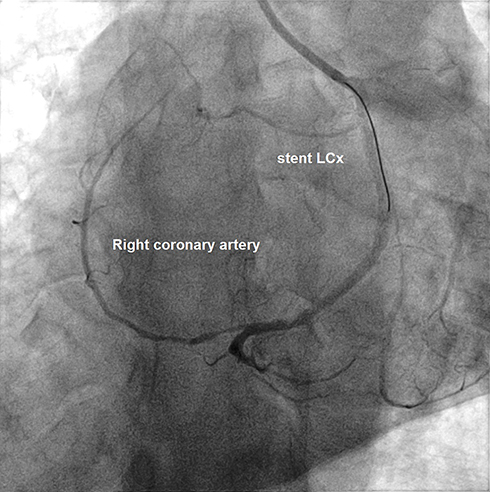 |
Figure 4 A post-stent angiographic image revealing that the RCA originated from the LCx (RAO 10° – Caudal 39°) (Video 3). |
To further evaluate the anatomy of the coronary arteries, a three-dimensional CT angiography was performed. It showed a single coronary artery (SCA) arising from the aorta (Figure 5, Figure 6).
 |
Figure 5 A three-dimensional CT angiographic image showing an SCA. |
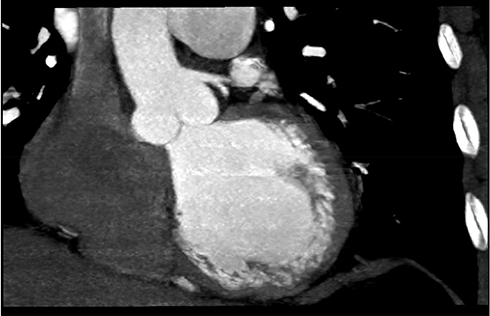 |
Figure 6 A CT angiographic image showing a single coronary artery arising from aorta. |
Discussion
An isolated SCA is extremely rare. Desmet et al reviewed 50,000 different coronary angiographies and only discovered 33 cases of SCA, yielding an incidence rate of 0.066%.6 Most SCAs are associated with coronary heart disease. Butto et al showed that the SCA ratio in persistent truncus arteriosus accounted for 18% of the cases.4
Lipton et al introduced a valuable classification system for SCAs in 1979: it described their origins and courses of these anomalies.9 Lipton based this on ten SCA angiographic analyses according to their sites of origin and the anatomical distribution of their branches. The classification of SCAs is as follows:
- Group I: A solitary vessel arises from the left (LI) or right (RI) coronary cusp, following the course of either a normal right or left coronary artery.
- Group II: The SCA arises from the right or left aortic sinus. This group is divided into three types depending on the relationship between the aberrant vessel and the great vessels.
- Type A: The aberrant vessel courses anterior to the pulmonary trunk.
- Type B: The aberrant vessel travels between the aorta and the pulmonary artery.
- Type P: The aberrant vessel travels posterior to the aorta.
- Group III: An absent left coronary artery. The LAD and LCx arise separately from the common trunk with a normal RCA
This case belongs to the L1 group of single coronary artery anomalies. The L1 group has an incidence rate of 0–0.035% and constitutes 1.2% of all coronary anomalies. There was only one case of this particular group out of 11 SCA cases in Chou et al report.5
Most patients are asymptomatic at the time of diagnosis. A literature review of Elbadawi et al found that many patients may have atypical chest pain or non-specific symptoms, with the absence of obstructive coronary artery disease and negative workup for ischemia.1 Most SCA cases were found incidentally during coronary angiography.12
Moreover, the combination of an SCA with acute myocardial infarction is really rare. Several reports were published, but all of them were single clinical cases. Gur et al and Giorgi et al reported cases with the R subgroup.2,7 Kafkas et al reported the first case of acute coronary syndrome with an L1-type coronary artery.8 Nasir et al and Mishra et al also reported primary PCI in patients with an L1 subtype.10,11 However, all of these reported cases featured anterior wall STEMI with left anterior descending occlusions. To our knowledge, this is the first case of PCI with an L1 subtype with a total occlusion of the LCx artery.
When performing PCI in patients with SCA, it is important to remember that it is similar to performing PCI on patients with unprotected left main coronary artery disease. Due to the risk of single ostium dissection, guided-wire manipulation and other devices must be kept with extra care. Unsuitable guided-wire catheters and inaccurate movements in PCI can lead to either serious dissection or thrombus formation, which will put the myocardium at serious risk or even cause death. If the presence of SCA is unclear, an aortic root angiogram is needed. Coronary CT angiography can also be used to carry out this task. SCAs have important prognostic implications and could put the patient at increased risk of sudden cardiac death or arrhythmia. Therefore, long-term follow-up is essential.1,3
Conclusion
SCA is regarded as a benign condition. However, the recognition of this coronary artery anomaly is of paramount importance for interventional cardiologists whenever the identification of both coronary ostia during a coronary angiogram is challenging. This case is a very rare instance of a patient with SCA (L1 group) with STEMI undergoing PCI to the LCx. PCI in SCA has its unique risks but, with improving technology and expertise, it is likely to be performed more frequently and successfully in the future.
Acknowledgements
The authors would like to thank Dr. Chau Nguyen for his help with the three-dimensional CT angiography images. Nguyen Thao Phan, Huy The Nguyen and Tran-Thuy Nguyen are considered first authors.
Consent for Publication
Written informed consent has been obtained from the patient’s wife for the case details and accompanying images to be published. This report and research have been approved by the E Hospital’s Cardiovascular Center Ethics Committee.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elbadawi A, Baig B, Elgendy IY, et al. Single coronary artery anomaly: a case report and review of literature. Cardiol Ther. 2018;7:1–5. doi:10.1007/s40119-018-0103-4
2. Gür M, Demirbağ YA, Yılmaz R. Isolated single coronary artery originating from a single right coronary ostium in a patient with acute myocardial infarction. Arch Turk Soc Cardiol. 2006;34:173–176.
3. Akcay A, Tuncer C, Batyraliev T, et al. Isolated single coronary artery: a series of 10 cases. Circ J. 2008;72(8):1254–1258. doi:10.1253/circj.72.1254
4. Butto F, Lucas RV
5. Chou LP, Kao C, Lee M-C, et al. Right coronary artery originating from distal left circumflex artery in a patient with an unusual type of isolated single coronary artery. Jpn Heart J. 2004;45(2):337–342. doi:10.1536/jhj.45.337
6. Desmet W, VANHAECKE J, VROLIX M, et al. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992;13(12):1637–1640. doi:10.1093/oxfordjournals.eurheartj.a060117
7. Giorgi B, Dymarkowski S, Rademakers FE, et al. Single coronary artery as cause of acute myocardial infarction in a 12-year-old girl: a comprehensive approach with MR imaging. AJR Am J Roentgenol. 2002;179(6):1535–1537. doi:10.2214/ajr.179.6.1791535
8. Kafkas N, Triantafyllou K, Babalis D. An isolated single L-I type coronary artery with severe LAD lesions treated by transradial PCI. J Invasive Cardiol. 2011;23(9):E216–8.
9. Lipton MJ, Barry WH, Obrez I, et al. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130(1):39–47. doi:10.1148/130.1.39
10. Mishra TK, Mishra CK, Das B. Percutaneous coronary intervention in a patient with single coronary artery. Indian Heart J. 2014;66(3):382–385. doi:10.1016/j.ihj.2014.03.011
11. Nasir JM, Hawkins K, Patino G, et al. Anterior ST-segment elevation myocardial infarction in a patient with an L-I type single coronary artery. JACC Cardiovasc Interv. 2012;5(4):e9–10. doi:10.1016/j.jcin.2011.09.030
12. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21(1):28–40. doi:10.1002/(ISSN)1097-0304
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.