Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
SR-HCC Score: A Novel Nomogram for Predicting Spontaneous Rupture in Hepatocellular Carcinoma Patients
Authors Gao S, Zhang X, Jia T, Jin Q, Yang X, Zhao R, Gao J
Received 14 February 2026
Accepted for publication 12 May 2026
Published 25 May 2026 Volume 2026:13 600415
DOI https://doi.org/10.2147/JHC.S600415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Siyuan Gao,1,* Xiuling Zhang,1,* Ting Jia,1 Qiu Jin,1 Xiaodong Yang,1 Ruisi Zhao,2 Jianpeng Gao3,4
1Liver Center, The Third People’s Hospital of Kunming, Kunming, Yunnan, 650041, People’s Republic of China; 2Department of Biomedical Sciences and Biotechnology, Hong Kong Metropolitan University, Hongkong, 999077, People’s Republic of China; 3Cell and Gene Therapy Research Center, Shenzhen Ruipuxun Academy for Stem Cell & Regenerative Medicine, Shenzhen, Guangdong, 518000, People’s Republic of China; 4Department of Gastroenterology, Yan’an Hospital Affiliated to Kunming Medical University, Kunming, Yunnan, 650051, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianpeng Gao, Email [email protected]
Purpose: Hepatocellular carcinoma (HCC) Spontaneous rupture (srHCC) is a life-threatening complication with a high mortality rate; however, no integrated predictive tool exists. This study aimed to develop and validate a novel nomogram (SR-HCC score) for srHCC risk prediction using a combination of clinical, radiological, and laboratory parameters.
Methods: This retrospective cohort study included 186 HCC patients from The Third People’s Hospital of Kunming (2010– 2025), randomly split into training (80%) and validation (20%) sets. Covariates included demographic, tumor-related, and laboratory indices. Univariate and multivariate logistic regression analyses were used to identify independent predictors that were integrated into the nomogram. Model performance was evaluated using Receiver Operating Characteristic (ROC) curves (discrimination) and calibration curves.
Results: Key independent predictors of srHCC included tumor diameter (3– 5 cm and 5– 10 cm), number of tumors (2– 3), capsular protrusion, Alpha-Fetoprotein (AFP) ≥ 100 ng/mL, moderate ΔALT (0– 200 U/L, inverse association), and ΔAST > 200 U/L. The nomogram achieved excellent discrimination (Area Under the Curve, AUC = 0.9617 in the training set; 0.9630 in the validation set) and good calibration, with predicted probabilities that closely matched the observed outcomes.
Conclusion: SR-HCC score is a reliable and user-friendly tool for individualized srHCC risk stratification. This enables clinicians to prioritize preventive interventions and optimize surveillance, especially in resource-limited settings, ultimately improving patient outcomes by preventing catastrophic ruptures.
Keywords: hepatocellular carcinoma, spontaneous rupture, nomogram, SR-HCC score, risk prediction
Introduction
Hepatocellular carcinoma (HCC) is one of the most common and deadly cancers worldwide. In China, it is the fourth leading causes of new cancer cases, and the second leading cause of cancer death.1
In addition to the underlying liver disease, HCC-related death is the most common cause of progressive Hepatocellular Carcinoma, (HCC) patients.2 Spontaneous rupture of HCC (srHCC) is one such complication. It represents a rapid, life-threatening complication with a mortality rate from 25% to 75% according to different research papers.3–5 In recent years, the incidence of srHCC has increased, reaching as high as 10–15% in some parts of Asia.6 Once rupture occurs, most patients with early-stage HCC lose the opportunity for radical treatment such as surgery or transplantation. Rupture is a contraindication for liver transplant exception points, and downstaging to meet the transplant criteria is rarely feasible.7 Identifying patients at high risk of rupture allows clinicians to prioritize treatment, implement preventive strategies, and closely monitor these individuals, especially in settings with limited healthcare resources.8 Early prediction enables timely intervention to prevent catastrophic outcomes.7
While previous studies have identified isolated predictors such as tumor size or arterial enhancement patterns, they lack integration into actionable models. The absence of validated early predictive tools that integrate readily available clinical and radiological parameters creates a critical gap in personalized risk assessment.
These models do not include commonly used clinical or laboratory variables that can further refine the risk prediction.7 Notably, no study has synergized (1) biochemistry markers (eg. alanine aminotransferase, aspartate aminotransferase, albumin, α-fetoprotein), (2) coagulopathy indices (eg. prothrombin time), and (3) demographic characteristics into a unified scoring system—a gap our study addresses.
Recent advances in predictive modeling have highlighted the value of integrated ensemble algorithms and multi-dimensional feature combinations in improving model stability and accuracy. Fitriyani et al9 proposed a novel predictive framework using bagging, histogram gradient boosting, and systematic feature selection, which effectively enhanced model performance and generalizability in complex disease risk assessment. Meanwhile, in the field of HCC research, a recent molecular prognostic study demonstrated that integrated multi-feature modeling can effectively improve risk stratification by capturing heterogeneous biological characteristics. These cutting-edge approaches confirm that hybrid ensemble learning and comprehensive variable integration help build more robust and clinically applicable predictive models.10 Such innovative modeling frameworks offer valuable insights for HCC rupture prediction, highlighting the potential to move beyond traditional single-algorithm approaches to capture the multifaceted biological and clinical drivers of srHCC.
In this study, we developed a novel nomogram (SR-HCC score) that integrates biochemical, radiological, and clinical parameters for predicting spontaneous HCC rupture. This tool aims to guide preemptive transarterial embolization or surgical decisions and optimize surveillance interventions. It empowers clinicians—especially in resource-limited settings—to identify high-risk HCC patients early, prioritize preventive interventions (eg., transarterial embolization), and optimize surveillance strategies. While this integrative approach represents a methodological advance, the findings should be interpreted with appropriate caution given the retrospective, single-center design of the study. Further validation is needed before definitive conclusions can be drawn regarding generalizability and clinical implementation.
Methods
Study Design and Populations
This retrospective cohort study aimed to develop and internally validate a predictive nomogram for the risk of srHCC. We retrospectively identified a consecutive cohort of patients diagnosed with primary hepatocellular carcinoma at the Liver Center, the Third People’s Hospital of Kunming, China, between January 2010 and January 2025.
Inclusion criteria were strictly defined as follows: (1) A definitive diagnosis of primary HCC confirmed either by histopathological examination (surgical resection or percutaneous biopsy specimens) or by clinical-radiological diagnostic criteria in line with the Standard for Diagnosis and Treatment of Primary Liver Cancer (2024 Edition) issued by the National Health Commission of the People’s Republic of China;11 (2) Complete clinical, radiological, laboratory, and follow-up data available for retrospective analysis; (3) Spontaneous HCC rupture (for the ruptured group) diagnosed by a composite of: typical clinical manifestations (acute-onset severe abdominal pain with or without hypovolemic shock), characteristic radiological findings (disruption of the peritumoral liver capsule, perihepatic hemoperitoneum, or enhanced fluid collection adjacent to the HCC lesion on contrast-enhanced computed tomography (CT), magnetic resonance imaging (MRI), or contrast-enhanced ultrasound), and/or positive diagnostic abdominocentesis (bloody ascites) or digital subtraction angiography (DSA) evidence of tumor bleeding. As this was an exploratory retrospective study, a formal sample size calculation or power analysis was not performed prior to data collection. The study population included all consecutive eligible patients with HCC treated at our center between 2010 and 2025, representing the complete available cohort for this rare outcome of spontaneous tumor rupture.
Exclusion criteria included: (1) Incomplete clinical, radiological, or laboratory data (eg., missing baseline/follow-up ALT/AST, AFP, or tumor imaging parameters) that precluded full covariate analysis and risk assessment; (2) Comorbid end-stage organ dysfunction meeting clinical diagnostic criteria: New York Heart Association (NYHA) Class III/IV heart failure, stage 4/5 chronic kidney disease (estimated glomerular filtration rate <30 mL/min/1.73m2) or acute renal failure requiring renal replacement therapy, and acute respiratory failure or end-stage lung disease requiring mechanical ventilation; (3) Concurrent malignant tumors of other organs (synchronous or metachronous); (4) Iatrogenic or traumatic HCC rupture induced by invasive procedures (eg., percutaneous biopsy, transarterial intervention) or abdominal trauma; (5) Severe coagulopathy unrelated to HCC (eg., congenital coagulation factor deficiency, immune thrombocytopenic purpura) that could independently cause abdominal bleeding. A total of 186 patients were included in the analysis, and the entire cohort was randomly divided into training and validation sets in a ratio of 8:2.
Outcome Variable
In this study, the outcome variable was srHCC, which was confirmed through a comprehensive review of clinical records and imaging reports (including computed tomography, CT, or MRI). Patients were categorized into ruptured and non-ruptured groups based on this outcome.
Covariates
In this study, covariates included age (<60 years and ≥60 years) and gender (male and female), tumor diameter (≤3 cm, 3–5 cm, 5–10 cm, and >10 cm), number of tumors (1, 2–3, and >3), involvement of liver segments S7 or S8 (S7/S8) (yes, no), and hepatic capsular protrusion (yes, no), vascular involvement (yes, no), abdominal lymph node metastasis (yes, no), portal vein tumor thrombus (yes, no), prothrombin time activity difference, (ΔPTA;calculated by last PTA minus baseline PTA), alpha-fetoprotein (AFP; <100ng/mL and ≥100ng/mL), albumin (ALB; ≤30 g/L and >30 g/L), alanine aminotransferase difference (ΔALT; <0 IU/mL, 0–200 IU/mL, >200 IU/mL, calculated by last ALT minus baseline ALT), and aspartate aminotransferase difference (ΔAST; <0 IU/mL, 0–200 IU/mL, >200 IU/mL, calculated by last AST minus baseline AST).
The cut-off values for continuous variables including age, AFP, ΔALT, and ΔAST were determined based on previously published literature, rather than arbitrary median splits or post hoc ROC analysis. For AFP, the cut-off of <100 ng/mL vs ≥100 ng/mL is a well-validated threshold in HCC research and clinical practice, identifying patients with higher tumor burden, aggressiveness, and complication risk.12 For ALB, ≤30 g/L vs >30 g/L reflects clinically significant impairment of hepatic synthetic function, a key determinant of HCC progression and rupture risk, as validated in studies including.13 The dynamic changes of ALT and AST have been proven to reflect progressive hepatocyte injury and aggressive tumor biological behavior in HCC patients in recent predictive model studies. These studies demonstrated that AST/ALT >200 IU/mL correlates with severe hepatocyte injury, aggressive tumor biology, and elevated risk of spontaneous HCC rupture, while <0 indicates stable or improving liver enzyme levels.12,13 Anatomically, liver segments S7/S8 are superficial and capsule-adjacent regions with a higher inherent rupture tendency, which has been validated in prior HCC complication risk scoring systems.13
Liver segments S7/S8 were selected because these segments are anatomically superficial, adjacent to the liver capsule, and clinically recognized as high-risk locations for spontaneous HCC rupture.14 Other segments were not included due to their lower observed association with rupture risk in clinical practice and prior studies.
People used to evaluate long-term survival outcomes after hepatectomy in hepatocellar carcinoma by studying changes in serum transaminases.15,16 In our study, ΔALT and ΔAST were calculated as the difference between the last value before rupture (or end of follow-up) and the baseline value. This model represents a static retrospective risk prediction tool rather than a real-time dynamic or prospective prediction system, which may limit its real-time clinical applicability.
The 2022 version of the BCLC classification also underscores the importance of liver function and AFP level, as well as tumor burden, when considering treatment strategies for HCC patients.17
Statistical Analysis
All statistical analyses were performed using R 4.2.2, with a two-sided P-value < 0.05, considered statistically significant. Categorical variables were presented as frequencies and percentages, and differences between groups were assessed using the chi-square test. Continuous variables were expressed as mean ± standard deviation and compared using t-tests. Variables that were statistically significant or demonstrated potential clinical relevance in the univariate analysis were included in the multivariate logistic regression model.
A nomogram was constructed to predict the risk of spontaneous rupture. Model performance was evaluated using the area under the ROC curve (AUC) for discrimination and calibration curves for agreement between predicted and observed probabilities.
Ethics
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board and Ethics Committee of the Third People’s Hospital of Kunming.
Results
Participant Characteristics
As shown in Table 1, of 186 patients with hepatocellular carcinoma, 94 had non-ruptured tumors and 92 had ruptured tumors. There were no significant differences in age or gender between the two groups (both P> 0.05). In contrast, ruptured cases were characterized by significantly larger tumor diameters, a greater number of tumor nodules, and a higher proportion of lesions located in hepatic segments S7/S8. The presence of capsular protrusion, vascular invasion, portal vein tumor thrombus, and abdominal lymph node metastasis was also markedly more frequent in the ruptured group (all P < 0.001). In terms of laboratory findings, patients with ruptured tumors exhibited greater decreases in PTA, lower ALB levels, higher AFP concentrations, and greater changes in ALT and AST levels than those without rupture (all P ≤ 0.05). This relatively high overall rupture rate of approximately 50% in the current cohort is mainly attributed to single-center referral bias and admission selection: our institution is a regional specialized liver disease center, which preferentially admits advanced and high-risk HCC patients with severe complications, including clinically suspected or acute ruptured tumors, thereby leading to an elevated proportion of rupture cases compared with unselected general HCC populations.
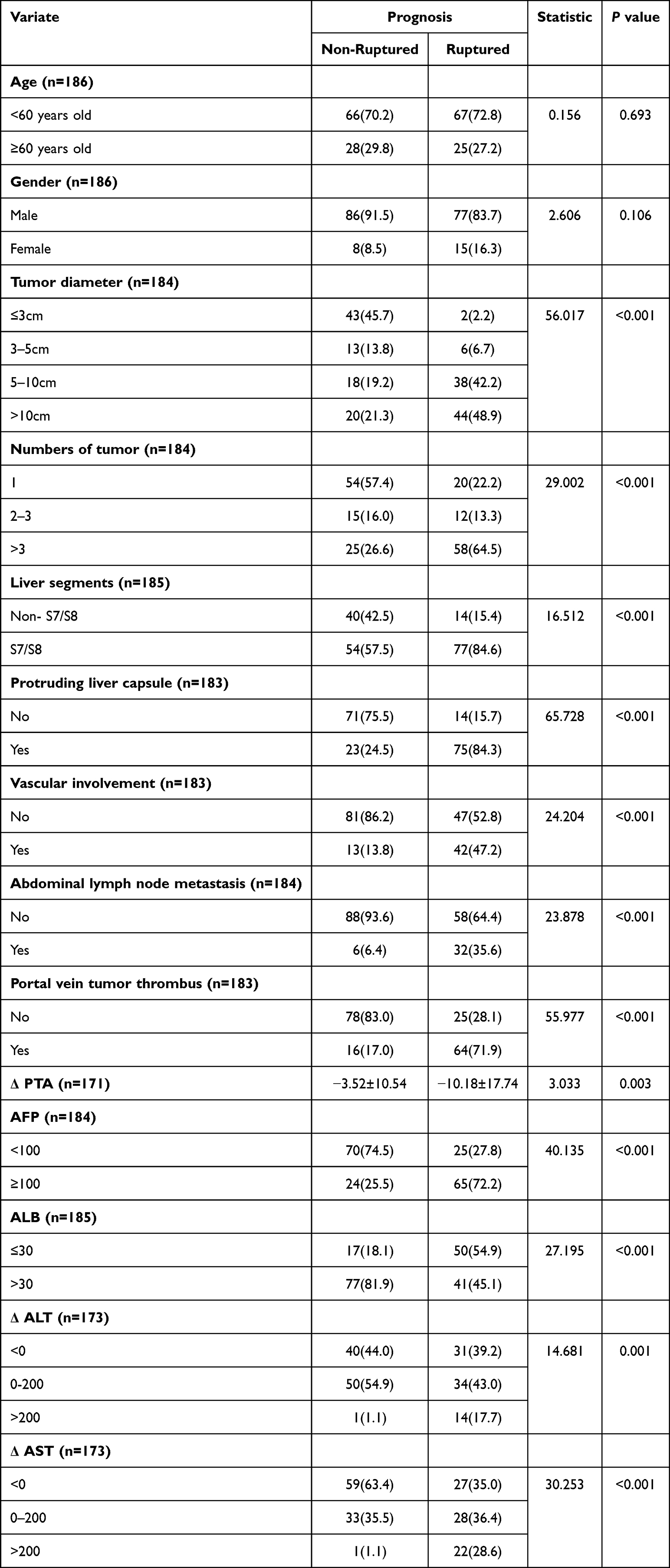 |
Table 1 Univariate Analysis |
Factors Associated with Tumor Rupture
Multivariate logistic regression (Table 2) was performed to identify variables independently associated with tumor rupture. Compared with tumors ≤3 cm, lesions measuring 3–5 cm (OR = 26.848, 95% CI: 1.597–451.291, P = 0.022) and 5–10 cm (OR = 18.063, 95% CI: 1.337–244.107, P = 0.029) were more likely to rupture. Patients with two–three tumors had a higher likelihood of rupture than those with a single lesion (OR = 13.744, 95% CI: 1.479–127.700, P = 0.021), whereas cases with more than three tumors did not show a significant difference (P = 0.828). The presence of capsular protrusion was strongly associated with rupture (OR = 12.545, 95% CI, 2.470–63.701; P = 0.002). Patients with AFP levels ≥100 ng/mL had a higher likelihood of rupture than those with AFP levels <100 ng/mL (OR = 6.228, 95% CI, 1.692–22.928; P = 0.006). Moderate increases in ALT levels (0–200 U/L) were inversely associated with rupture (OR = 0.055, 95% CI: 0.008–0.366, P = 0.003), whereas elevated AST levels (>200 U/L) were closely associated with rupture (OR = 382.878, 95% CI, 3.405–43,048.630; P = 0.014). Other clinical and pathological variables showed no statistically significant associations (P > 0.05).
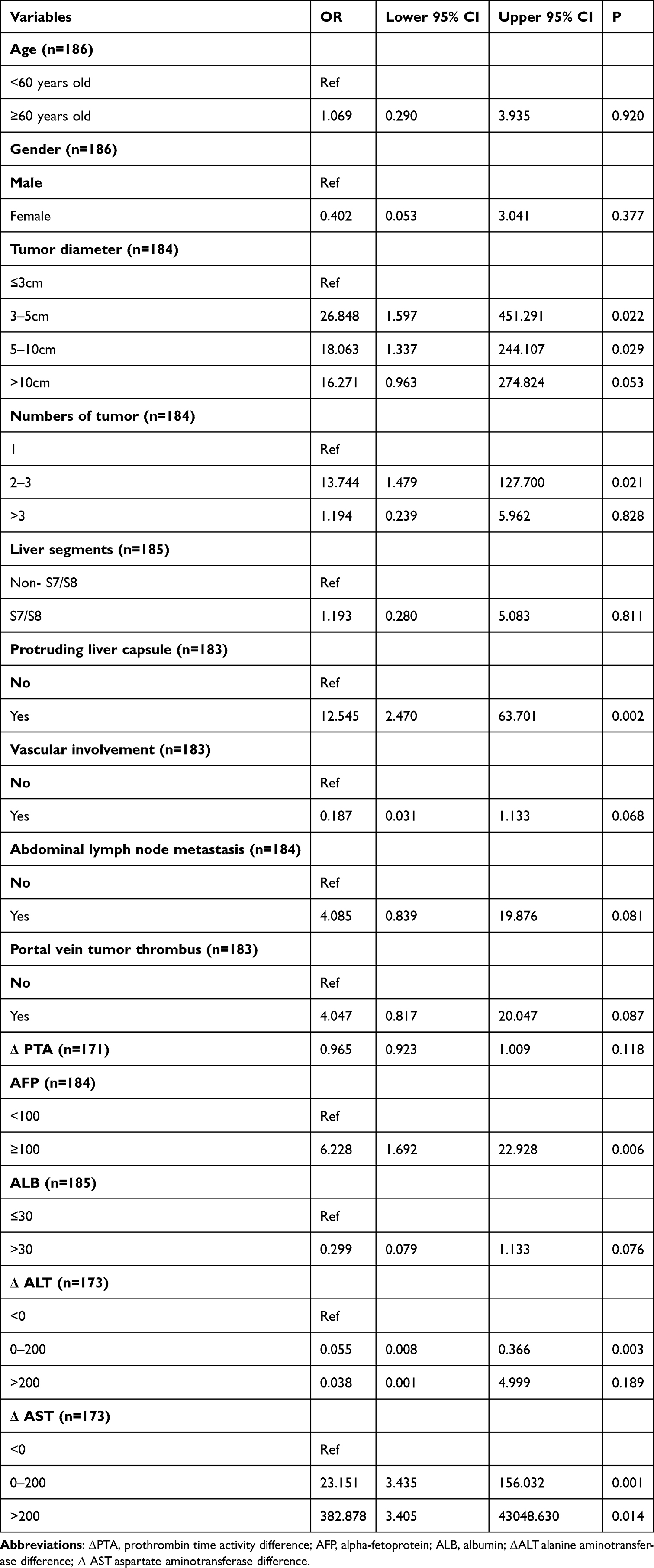 |
Table 2 Multivariate Analysis |
Nomogram Model
A nomogram model (Figure 1) was developed based on the results of the multivariate logistic regression analysis and previous literature. The model included age, gender, tumor diameter, number of tumors, liver segments, capsular protrusion, vascular involvement, abdominal lymph node metastasis, portal vein tumor thrombus, PTA, AFP, ALB, ΔALT, and ΔAST levels. Each variable was assigned a score on the corresponding scale, and the sum of all the scores represented the total score. The total points were then mapped to the probability of tumor rupture, as shown at the bottom of the nomogram. A higher total score indicated an increased likelihood of rupture, allowing for individualized estimation of bleeding risk in patients with hepatocellular carcinoma.
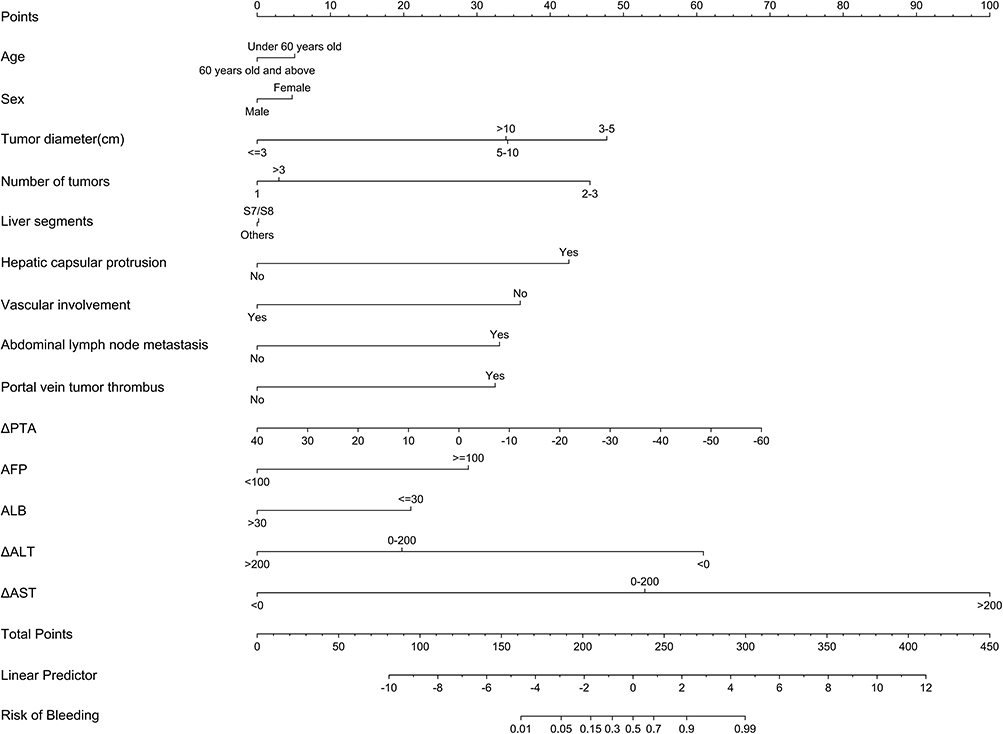 |
Figure 1 Nomogram model. |
Discrimination and Validation of the Nomogram Model
The dataset was randomly divided into training and validation sets in a ratio of 8:2 to evaluate the performance of the nomogram model. The discriminative ability of the model was assessed using receiver operating characteristic (ROC) curve analysis. In the training set, the area under the ROC curve (AUC) was 0.9617, indicating excellent discrimination between ruptured and non-ruptured hepatocellular carcinoma (Figure 2). In the validation set, the AUC was 0.9630, indicating consistent discriminative performance (Figure 3). These findings suggest that the nomogram provides a stable and reliable differentiation of rupture risk across both datasets.
 |
Figure 2 ROC curve of the model in the training set. The area under the ROC curve (AUC) was 0.9617. |
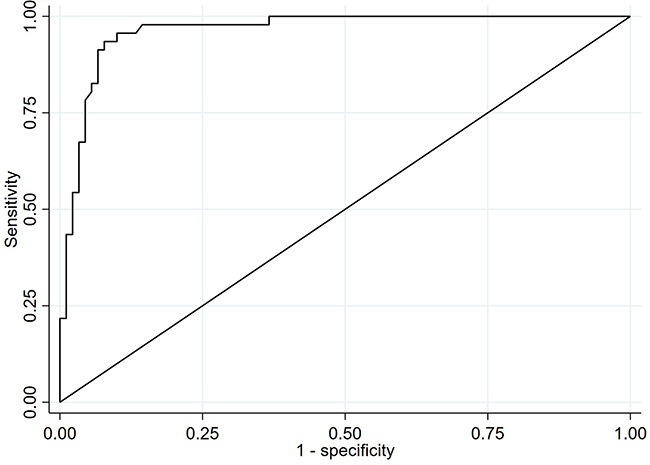 |
Figure 3 ROC curves of the prediction model. Validation set the AUC was 0.9630. |
Calibration of the Nomogram Model
Calibration curves were constructed to evaluate the agreement between the predicted and observed probabilities of tumor rupture. In both the training and validation sets (Figures 4 and 5), the calibration plots show that the predicted probabilities were closely aligned with the actual outcomes. The bias-corrected curves nearly coincided with the ideal reference line, indicating good calibration of the nomogram model and that the model’s predicted risks accurately reflected the observed probabilities.
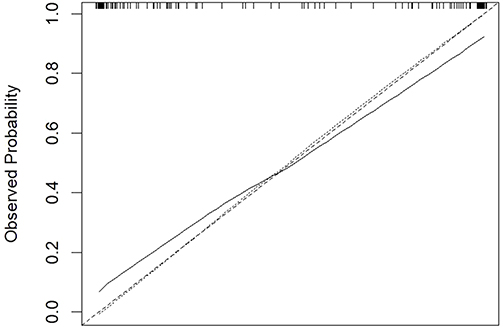 |
Figure 4 Calibration curves of the prediction model in the training sets. |
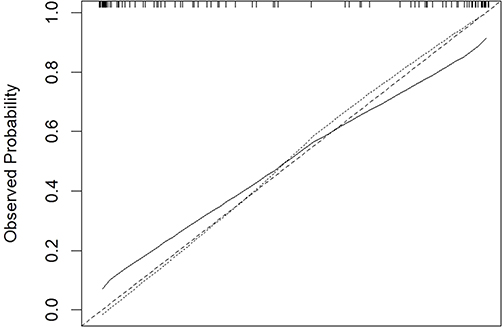 |
Figure 5 Calibration curves of the prediction model in the Validation sets. |
Discussion
Our study developed and validated a novel risk prediction nomogram—the SR-HCC score—for spontaneous rupture in HCC patients, a critical clinical gap with no integrated predictive tools to date. This model integrates readily accessible clinical, radiological, and laboratory parameters (exploiting both traditional tumor factors and novel ΔALT/ΔAST indices) and exhibits excellent predictive performance, with an AUC of 0.9617 in the training cohort and 0.9630 in the validation cohort. Such robust discriminative ability enables accurate stratification of HCC patients into distinct rupture risk categories, laying a solid foundation for personalized clinical management.
Our findings align with previous studies that identified tumor size, liver functional reserve,18 and AFP7 as key determinants of HCC rupture risk. Of note, our multivariate analysis revealed a non-monotonic relationship between tumor diameter and rupture risk, with the highest risk observed in tumors 3–5 cm (OR = 26.8), followed by 5–10 cm (OR = 18.1), whereas tumors >10 cm did not reach statistical significance (P = 0.053). This pattern appears to contradict the conventional clinical assumption that larger tumors carry higher rupture risk.14 However, this non-monotonic trend is most likely attributable to the small subgroup sample size, particularly for tumors >10 cm, which reduced statistical power and led to unstable odds ratio estimates. Biologically, tumors measuring 3–5 cm often exhibit rapid growth, high intratumoral pressure, incomplete capsule formation, and fragile neovascularization, all of which predispose to acute rupture.14,19,20 In contrast, larger tumors (>10 cm) may develop more extensive internal necrosis or fibrosis, which could lower immediate rupture risk. This finding should be interpreted cautiously and requires confirmation in larger cohorts. Notably, we extend previous research by incorporating dynamic ΔALT and ΔAST changes as potential independent prognostic factors for srHCC. To our knowledge, few prior studies have specifically explored and validated the relationship between longitudinal liver enzyme variation and spontaneous HCC rupture. Elevated ALT/AST levels reflect progressive hepatocyte injury, which correlates with more aggressive and advanced HCC phenotypes; this mechanistic link not only explains the observed rupture risk association but also enriches the biological understanding of srHCC pathogenesis.21 Consistent with existing evidence,22,23 we further confirm that high AFP levels augment rupture risk through multiple pathways, including increased tumor vascularity, rapid proliferation, and poor differentiation, reinforcing the clinical relevance of AFP in srHCC risk assessment.
Several variables that were not statistically significant in multivariate analysis—including age, gender, vascular invasion, abdominal lymph node metastasis, portal vein tumor thrombus, and albumin—were still incorporated into the nomogram. These variables were retained based on strong clinical relevance and well-established biological plausibility from previous studies, as they are closely linked to tumor aggressiveness, liver functional reserve, and disease severity24–26 in HCC patients. In clinical prediction model development, including variables with recognized clinical importance improves model robustness, generalizability, and clinical interpretability, even if they do not reach statistical significance in a single-center cohort with a relatively small sample size. Thus, these variables were included to ensure the nomogram reflects comprehensive clinical practice rather than statistical results alone.
Adopting a nomogram for model visualization further amplifies the SR-HCC score’s clinical utility. Nomograms translate complex statistical models into a user-friendly graphical format, enabling frontline clinicians to perform rapid bedside risk estimation without specialized statistical expertise.27 This design is particularly valuable for clinical practice, as it bridges the gap between research findings and actionable decision-making.
Potential Clinical Implications of the SR-HCC Nomogram
The SR-HCC score offers distinct and practical clinical value for HCC management, especially in resource-limited settings where advanced predictive tools are scarce and srHCC-related mortality remains high. First, it enables rapid bedside risk stratification, allowing clinicians to identify high-risk patients and prioritize timely preemptive interventions (eg., transarterial embolization, elective surgical resection) to mitigate life-threatening rupture and preserve curative treatment opportunities—an unmet need in current srHCC care. Second, for moderate and low-risk patients, the model optimizes personalized surveillance strategies (eg., adjusted imaging follow-up intervals), balancing rigorous risk monitoring with rational utilization of limited healthcare resources and reducing unnecessary clinical procedures. Third, constructed with routinely collected clinical parameters (no specialized testing or equipment required), the nomogram has broad applicability in primary hospitals and regional medical centers, addressing the global disparity in HCC care access. Additionally, it serves as an effective communication tool, helping clinicians explain individual rupture risk to patients and families, and facilitating informed shared decision-making to improve treatment and surveillance adherence.
Study Limitations
While the SR-HCC score demonstrates strong predictive performance and clinical potential, this study has several limitations that warrant objective consideration—and which our subsequent research aims to address. First, this is a single-center retrospective cohort study with 186 patients, which may introduce selection bias and temporarily limit the model’s generalizability to HCC populations with distinct ethnic backgrounds or underlying liver disease etiologies. Second, model validation currently relies solely on an internal 80:20 random split, which represents weak form of model assessment. The small validation set of only approximately 37 patients is insufficient to produce stable AUC estimates, and the nearly identical AUC values between training and validation sets may reflect random sampling variation rather than genuine generalizability. External validation from independent institutions or different time periods is therefore essential to confirm real-world performance. Third, the total sample size of 186 patients with 92 rupture events is underpowered for 14 covariates included in the multivariate model, failing to meet the conventional criterion of 10–20 events per variable for logistic regression. This issue increases the risk of overfitting and leads to wide confidence intervals and unstable odds ratio estimates, such as the exceptionally high OR for ΔAST >200 U/L. In addition, as an exploratory retrospective investigation of a relatively rare complication, a formal a priori sample size calculation or power analysis was not performed. The modest sample size may reduce statistical power and increase the risk of overfitting; these limitations are recognized and highlight the need for subsequent validation in larger, multi-center populations. Nonetheless, these limitations represent key directions for model refinement, not fundamental flaws in its core predictive value. In future research, we may draw on the methods of machine learning to further validate and optimize the model.28 And as many other centers as possible should be included to facilitate better external validation. Further, we may incorporate penalized regression (eg., LASSO or ridge regression) or bootstrapping which have been proven effective in stabilizing model parameters and reducing overfitting in limited clinical samples29 to address potential overfitting, small sample size, or unstable odds ratio estimates. These methods may improve model stability and will be considered in future larger-scale studies.
Conclusion
The SR-HCC score is a novel, robust, and user-friendly predictive tool that fills a critical clinical gap in srHCC risk assessment. By integrating traditional tumor factors and novel dynamic liver enzyme indices (ΔALT/ΔAST), it achieves excellent discriminative ability for spontaneous HCC rupture and enables accurate individualized risk stratification. Its design with routinely accessible clinical parameters and nomogram visualization ensures broad clinical applicability, especially in resource-limited settings, where it can guide preemptive interventions, optimize surveillance strategies, and improve shared decision-making between clinicians and patients—ultimately mitigating life-threatening srHCC events and preserving curative treatment opportunities for HCC patients.
While the single-center retrospective design and lack of external validation represent current limitations, these are actionable for future research. Rigorous external validation in large, multi-center prospective cohorts will further confirm the SR-HCC score’s stability, refine model parameters, and address potential overfitting, thereby strengthening its clinical impact and translational value. Collectively, this study establishes a promising foundation for srHCC risk management, and the SR-HCC score has the potential to become a standard clinical tool for personalized HCC care following further multi-center validation.
Ethics Approval
This study was reviewed and approved by the Ethics Committee of the Third People’s Hospital of Kunming (approval number 2023-03-08-002). All procedures involving human participants (including the use of human samples and related data) were conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments or comparable standards. Informed consent was obtained from all individual participants prior to their involvement in the study, ensuring that participants were fully informed of the study purpose, procedures, potential risks, and benefits and had the right to withdraw from the study at any time without prejudice to their medical treatment.
Consent for Publication
All participants were involved in the study and provided written consent for publication. Prior to obtaining consent, each participant was fully shown and informed of all the contents of the article to be published, including relevant clinical data, images, videos, and any other recordings related to the study. The participants explicitly confirmed their agreement with the publication of these details, with a full understanding that the publication of such information is for academic research and exchange purposes, and that all efforts have been made to protect their privacy and anonymize personal identifying information in accordance with ethical guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Kunming Municipal Health Commission, Health Research Project Funding (Grant No. 2023-03-08-002) awarded to Siyuan Gao, and Shenzhen Science and Technology Research Funding (Grant No. JCYJ20220530163602006) were awarded to Jianpeng Gao.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Han B, Zheng R, Zeng H. et al. Cancer incidence and mortality in China, 2022. J Nat Cancer Center. 2024;4(1):47–13. doi:10.1016/j.jncc.2024.01.006
2. Yen YH, Kee KM, Li WF, et al. Causes of death among patients with hepatocellular carcinoma according to chronic liver disease etiology. Cancers. 2023;15(6):1687. doi:10.3390/cancers15061687
3. Aziz H, Kwon YIC, Park A, Kwon Y, Aswani Y, Pawlik TM. Comprehensive review of clinical presentation, diagnosis, management, and prognosis of ruptured hepatocellular carcinoma. J Gastrointestinal Surg. 2024;28(8):1357–1369. doi:10.1016/j.gassur.2024.05.018
4. Huang X, Jia C, Xu L, et al. Survival of patients subjected to hepatectomy after spontaneous rupture of hepatocellular carcinoma: a meta-analysis of high-quality propensity score matching studies. Front Oncol. 2022;12:877091. doi:10.3389/fonc.2022.877091
5. Tan NP, Majeed A, Roberts SK, et al. Survival of patients with ruptured and non-ruptured hepatocellular carcinoma. Med J Aust. 2020;212(6):277–278. doi:10.5694/mja2.50483
6. Xia F, Ndhlovu E, Zhang M, Chen X, Zhang B, Zhu P. Ruptured hepatocellular carcinoma: current status of research. Front Oncol. 2022;12(848903). doi:10.3389/fonc.2022.848903
7. Ye F, Ma D, Gong X-Y, Yang Y-C, Chen Y-J. Development and validation of risk score for predicting spontaneous rupture of hepatocellular carcinoma. Annals Surg Treatment Res. 2020;99(5):268–274. doi:10.4174/astr.2020.99.5.268
8. Sandomenico F, Arpaia V, De Rosa F, et al. Spontaneously ruptured hepatocellular carcinoma: computed tomography-based assessment. Diagnostics. 2023;13(6):1021. doi:10.3390/diagnostics13061021
9. Fitriyani NL, Syafrudin M, Chamidah N, et al. A novel approach utilizing bagging, histogram gradient boosting, and advanced feature selection for predicting the onset of cardiovascular diseases. Mathematics. 2025;13(13):2194. doi:10.3390/math13132194
10. Zaidi SAJ, Ghafoor A, Kim J, Abbas Z, Lee SW. HeartEnsembleNet: an innovative hybrid ensemble learning approach for cardiovascular risk prediction. Healthcare. 2025;13(5):507. doi:10.3390/healthcare13050507
11. Zhou J, Sun H, Wang Z, et al. China liver cancer guidelines for the diagnosis and treatment of hepatocellular carcinoma (2024 Edition). Liver Cancer. 2025:1–57. doi:10.1159/000546574.
12. Kim J, Kim J-H, Ko E, et al. Model predicting survival in intermediate-stage HCC patients reclassified for TACE based on the 2022 BCLC criteria. Cancers. 2025;17(5):849. doi:10.3390/cancers17050894
13. Beumer B, Buettner S, Galjart B, et al. Systematic review and meta-analysis of validated prognostic models for resected hepatocellular carcinoma patients. Eur J Surg Oncol. 2022;48(3):492–499. doi:10.1016/j.ejso.2021.09.012
14. Xia F, Liu Y, Huang H, et al. Risk factors for hepatocellular carcinoma rupture: multicentre retrospective study. BJS Open. 2025;9(6). doi:10.1093/bjsopen/zraf105
15. Lu J, Wang F, Zhang W, et al. Perioperative changes in serum transaminases levels predicts long-term survival following liver resection of hepatocellular carcinoma. Ann Surg Oncol. 2024;32(4):2446–2455. doi:10.1245/s10434-024-16705-8
16. Kostakis ID, Kotelis N, Safavi D, Iype S. Preoperative blood tests provide diagnostic and prognostic information about patients with hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2025;37(2):219–229. doi:10.1097/meg.0000000000002896
17. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
18. Chen Y, Guo D, Li X, Xu C, Zhu Q. Predictors of spontaneous rupture of hepatocellular carcinoma and clinical outcomes following hepatectomy. Front Oncol. 2022;12:820867. doi:10.3389/fonc.2022.820867
19. Gnanendran D, Olaru A, Shah M, Jackson J, Venkatachalapathy SV, Aravinthan AD. The size-growth rate relationship in hepatocellular carcinoma. JGH Open. 2025;9(7):e70224. doi:10.1002/jgh3.70224
20. Xia F, Chen Q, Liu Z, et al. Machine learning models for predicting postoperative peritoneal metastasis after hepatocellular carcinoma rupture: a multicenter cohort study in China. Oncologist. 2025;30(1). doi:10.1093/oncolo/oyae341
21. Li ZC, Li Z, Li C, et al. Letter: elevated aspartate aminotransferase and aspartate aminotransferase to alanine aminotransferase ratio predicts poor survival in hepatocellular carcinoma after resection. Aliment Pharmacol Ther. 2020;52(11–12):1762–1763. doi:10.1111/apt.16124
22. She WH, Chan MY, Ma KW, et al. Alpha-Fetoprotein in predicting survival of patients with ruptured hepatocellular carcinoma after resection. J Invest Surg. 2021;35(5):1091–1097. doi:10.1080/08941939.2021.2012615
23. Xia F, Ndhlovu E, Liu Z, et al. Alpha-Fetoprotein+Alkaline phosphatase (A-A) score can predict the prognosis of patients with ruptured hepatocellular carcinoma underwent hepatectomy. Dis Markers. 2022;2022(1875–8630):1–16. doi:10.1155/2022/9934189
24. Wang B, Xiong Y, Li R, Zhang S. Age-related nomogram revealed optimal therapeutic option for older patients with primary liver cancer: less is more. Aging. 2024;16(11):9824–9845. doi:10.18632/aging.205901
25. Radu IP, Scheiner B, Schropp J, et al. The influence of sex and age on survival in patients with hepatocellular carcinoma. Cancers. 2024;16(23). doi:10.3390/cancers16234023
26. Chang Y, Yu SJ, Kim HC, et al. Reappraisal of portal vein tumor thrombosis as a prognostic factor for patients with hepatocellular carcinoma. Gut Liver. 2024;18(1):156–164. doi:10.5009/gnl230057
27. Wang J, Kong C, Pan F, Lu S. Construction and validation of a nomogram clinical prediction model for predicting osteoporosis in an asymptomatic elderly population in Beijing. J Clin Med. 2023;12(4):1293. doi:10.3390/jcm12041292
28. Valencia MN, Kim J, Abbas Z, Lee SW. Early detection of chronic kidney disease in men using lifestyle and demographic indicators: a machine learning approach for primary healthcare settings. Healthcare. 2026;14(3). doi:10.3390/healthcare14030405
29. Kim MS, Yon DK, Lee SW, et al. Quantifying the impact of immortal time bias: empirical evidence from meta-analyses. J R Soc Med. 2025;118(9):293–303. doi:10.1177/01410768251366880
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Risk Prediction Model for Female Stress Urinary Incontinence in Rural Fujian, China
Wang Q, Jiang XX, Que YZ, Wan XY, Lin CQ
Risk Management and Healthcare Policy 2024, 17:1101-1112
Published Date: 30 April 2024