Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Spotlight on Topical Long-Term Management of Plaque Psoriasis
Authors Carrascosa JM ![]() , Theng C, Thaçi D
, Theng C, Thaçi D
Received 17 April 2020
Accepted for publication 7 July 2020
Published 29 July 2020 Volume 2020:13 Pages 495—498
DOI https://doi.org/10.2147/CCID.S254114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jose Manuel Carrascosa,1 Colin Theng,2 Diamant Thaçi3
1Dermatology Department, Hospital Germans Trías i Pujol, Barcelona, Spain; 2The Skin Specialists & Laser Clinic, Singapore; 3Institute and Comprehensive Center for Inflammation Medicine, University of Lübeck, Lübeck, Germany
Correspondence: Jose Manuel Carrascosa
Dermatology Department, Hospital Germans Trías i Pujol, Universitat Autònoma of Barcelona, IGTP Badalona, Barcelona, Espagne
Email [email protected]
Abstract: During the 28th Congress of the European Academy of Dermatology and Venereology (EADV) held in Madrid in October 2019, an industry hub was dedicated to the long-term management of psoriasis. Psoriasis is a systemic inflammatory disease primarily involving the skin that affects up to 4% of the European population, the majority of whom present with chronic plaque psoriasis. Topical therapies are well established in the first-line treatment of psoriatic plaque flares. Nevertheless, as psoriasis is a chronic disease, long-term control should be considered. The aim of the session was to provide expert opinion on the benefit of long-term maintenance therapy in chronic plaque psoriasis and introduce the concept of pro-active management to decrease the number of relapses and improve patient quality of life. The current guidelines and recommendations were reviewed, as well as the available data on published clinical trials. There is still an important role for topical therapy in psoriasis and current recommendations suggest a maintenance regimen for psoriasis. Adherence optimization and proactive management of relapse can be key factors for obtaining clinical outcomes in topical long-term therapy. Calcipotriol/betamethasone dipropionate foam is the only topical formulation with long-term data as a twice-weekly proactive treatment approach for up to 52 weeks for chronic plaque psoriasis.
Keywords: Cal/BD combination, corticosteroids, adherence, maintenance, relapse
Background
The 28th Congress of the European Academy of Dermatology and Venereology (EADV) took place in Madrid in October 2019 and one of the industry hubs was dedicated to the long-term management of psoriasis, a chronic disease with frequent relapses.1
Topical therapies are well established in the first-line treatment of psoriatic plaque flares as they offer rapid clearance of skin symptoms in patients, and symptoms are then manageable with topical treatment only (approx. 80%) or in conjunction with systemic treatment. Nevertheless, as psoriasis is a chronic disease, long-term control of the signs and symptoms should be considered. The aim of this interactive session was to provide expert opinion on the long-term management in chronic plaque psoriasis.
A review of the current guidelines and recommendations was presented, as well as the available data on published clinical trials.
Discussion
Although there is a consensus on flare treatment with topical products, a harmonized recommendation is lacking in the guidelines on the type of products (steroid or vitamin D analogs, alone or in combination), and the frequency of administration that would support long-term management for an effective long-term disease control.2 In addition, most topicals are not approved for longer than the acute phase; only calcipotriol/betamethasone dipropionate (Cal/BD) fixed-dose combinations as gel and ointment and vitamin D analogs have been investigated and approved as treatment for 52 weeks on an as-needed basis.3
A recent consensus in Asia on the management of mild to moderate plaque psoriasis with topical therapy agreed that the maintenance phase and prevention of relapses could be achieved with twice a week or weekend application of a topical steroid or vitamin D analog or a fixed-dose combination of both.4 In France, a twice-weekly application of a combination of a vitamin D analog and topical steroid was recommended by a panel of experts.5 The German consensus also supports topical long-term management with 2 compound-products, once or twice a week after initial therapy, based on the favorable risk–benefit ratio in maintenance trials and better cost-effectiveness.6 In the UK, guidelines recommend maintenance therapy with topical products, but the frequency of application is not specified,7 and this treatment option is not reflected in any current label.
Only few published studies have investigated long-term use of topical treatment in psoriasis and there is a lack of long term (>6 months) maintenance studies. Indeed, a Cochrane systematic review on topical treatments for psoriasis concluded that most findings were limited to short-term treatments (<6 months) and that long-term assessments (6–12 months) are needed.8
The concept and proposals regarding the use of topical therapy in the long-term management of psoriasis have evolved over time.
In the past a three-phase sequential approach was commonly used for psoriasis treatment:9
- Step 1 was the clearance phase including treatments with corticosteroid and vitamin D analog
- Step 2 was the transition phase and proposes corticosteroid (weekends) and vitamin D analog (weekdays)
- Step 3 was the maintenance phase with vitamin D analog treatment
Current clinical practice in the long-term management is more to treat relapses as needed than regularly or proactively in the maintenance phase: however, the maintenance of twice-weekly application of Cal/BD gel was found to be more effective and was associated with a lower rate of re-occurrence of the signs and symptoms of psoriasis versus on-demand treatment in a 12-week multicenter study evaluating the efficacy and tolerability of Cal/BD gel applied to scalp psoriasis following complete remission.10
The clinical evidence of the benefit of long-term management was shown in the few trials found and analyzed based on a systematic literature review.11 These trials are listed in Table 1. Best evidence regarding topical long-term management is available for the formulation containing calcipotriene and betamethasone. In a comparative trial in plaque-type psoriasis, this combination showed superior tolerability and cost-effectiveness compared to calcipotriene monotherapy. In scalp psoriasis, a gel formulation of the fixed combination was also superior compared to calcipotriene monotherapy. Standardized and simplified treatment application modes resulted in a better clinical outcome compared to on-demand therapies.11
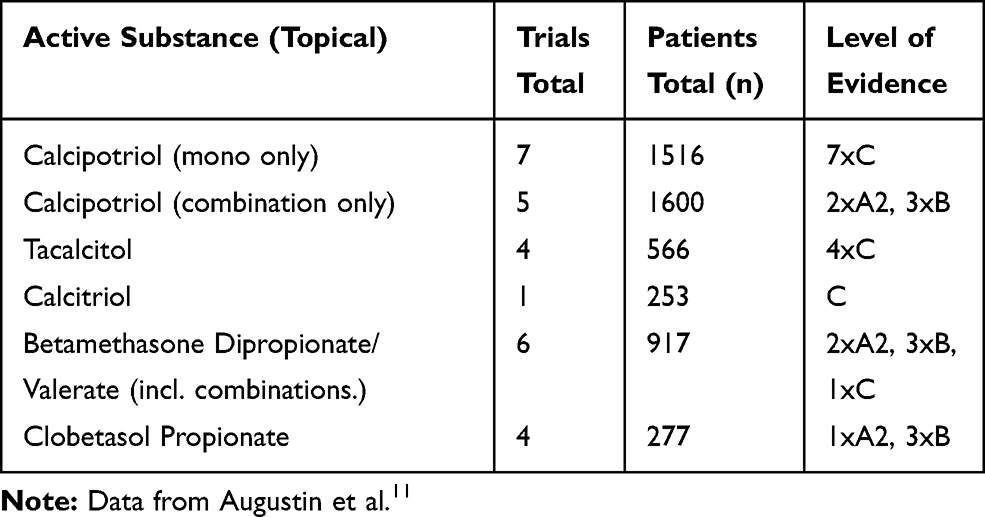 |
Table 1 Evidence on Long-Term Management |
The main challenge of long-term topical management for chronic mild to moderate psoriasis is long-term adherence, which is a barrier to successful topical treatment.12 The following factors have been identified as important drivers of adherence to prescribed therapies: frequency of treatment application, safety, local tolerability and cosmetic acceptance of the formulation, treatment formulation, the need for multiple therapies, fast onset of action, corticosteroid phobia, long-term psychological burden of chronic treatment and topical fatigue. Adherence to prescribed medication is fundamental to improving clinical outcomes. However, it has been shown that the adherence rates to topical treatments are relatively low (50–70%) with psoriasis and even lower (40%) for topical corticosteroids.3
Treatment goals agreed between the patient and the physician are also key to ongoing patient adherence.13 Effective strategies can be put in place by physicians to help patients to achieve therapeutic outcomes: positive patient–physician relationships, patient education, follow up visits or calls, and patient participation in treatment decisions.14
In this context, the Topical Treatment Optimization Programme (TTOP) study, which was a large European investigator-initiated study, was designed to improve adherence to treatment in psoriasis. This included guidance for the conversation between dermatologists/nurses and patients, patient information material, telephone/email helpdesks, and treatment reminders. Patients with mild to moderate psoriasis who had already failed previous topical therapy received Cal/BD gel as standardized study medication and were randomized to either TTOP or non TTOP management for the entire study (64 weeks). Cal/BD gel was applied once daily for 8 weeks followed by “as needed” application for an additional 56 weeks. After 8 weeks of therapy, significantly more patients achieved a PGA of “clear” or almost “clear” in the TTOP arm than those in the non-TTOP arm (36.3% vs 31.3%, p<0.05). This difference is expected to increase over time but the clinical relevance of these data remains to be determined. Patients ranked the one-to-one conversation with dermatologists/nurses as being the most important element of the TTOP.3
One randomized double-blind Phase III clinical trial (PsoLong – NCT02899962)15 has recently been completed investigating the long-term efficacy and safety up to 52 weeks of Cal/BD foam in a twice-weekly pro-active management regimen in the prevention of relapses compared to the current reactive approach of treating flares and relapses. In the pro-active treatment arm, Cal/BD foam is applied once daily for 4 weeks on flares and then twice weekly when in remission. In the reactive arm, Cal/BD foam is applied once daily for 4 weeks on flares, and on relapses, Cal/BD foam vehicle is applied twice weekly in remission for blinding purposes.
Results are awaited at the beginning of 2020 and will bring evidenced-based clinical data for the long-term therapy of this chronic condition.
Conclusion
There is still an important role for topical therapy in psoriasis treatment and current recommendations suggest a maintenance regimen for psoriasis despite the lack of labeling for any topicals in that sense. Adherence optimization and proactive management of relapse can be key factors for obtaining clinical outcomes in topical long-term management. Calcipotriol/betamethasone dipropionate foam is the only topical formulation that will present long-term data as a twice-weekly proactive treatment approach up to 52 weeks for chronic plaque psoriasis.
Abbreviations
Cal/BD, calcipotriol/betamethasone dipropionate; TTOP, topical treatment optimization programme.
Acknowledgments
Editorial assistance was provided by Pascale Tronche, PhD, and Peggy Cance, of Alhena Consult SAS (Valbonne, France). This assistance was supported by Leo Pharma.
Disclosure
Dr Jose-Manuela Carrascosa has participated as invited speaker, PI/SI in clinical trials and advisor for LEO Pharma, Novartis, Lilly, Janssen, Abbvie, Celgene, Amgen, Mylan, Biogen, Pfizer, Sandoz. Dr Colin Theng has participated as invited speaker and/or served on the advisory board of LEO Pharma, Novartis, Lilly, Janssen, Abbvie. Prof Diamant Thaçi has been a consultant and advisor and/or received speaking fees and/or grants and/or served as an investigator in clinical trials for the following companies: AbbVie, Almirall, Amgen, Bioskin, Boehringer Ingelheim, BMS, Celgene, Dignity, Eli Lilly, Galderma, Galapagos, GSK, LEO Pharma, Janssen-Cilag, MSD, Morphosis, Novartis, Pfizer, Regeneron, Roche, Samsung, Sandoz, Sanofi, and UCB. The authors report no other conflicts of interest in this work.
References
1. Sarac G, Koca TT, Baglan T. A brief summary of clinical types of psoriasis. North Clin Istanbul. 2016;3: 79–82. doi:10.14744/nci.2016.16023
2. Segaert S, Calzavara-Pinton P, de la Cueva P, et al. Long- term topical management of psoriasis: the road ahead. J Dermatolog Treat. 2020;1–10. doi:10.1080/09546634.2020.1729335
3. Reich K, Zschocke I, Bachelez H, et al. PSO-TOP study group: a topical treatment optimization programme (TTOP) improves clinical outcome for calcipotriol/betamethasone gel in psoriasis: results of a 64-week multinational randomized phase IV study in 1790 patients (PSO-TOP). Br J Dermatol. 2017;177(1):197–205. doi:10.1111/bjd.15466
4. Imafuku S, Zheng M, Tada Y, et al. Asian consensus on assessment and management of mild to moderate plaque psoriasis with topical therapy. J Dermatol. 2018;45(7):805–811. doi:10.1111/1346-8138.14338
5. Paul C, Gallini A, Archier E, et al. Evidence-based recommendations on topical treatment and phototherapy of psoriasis: systematic review and expert opinion of a panel of dermatologists. J Eur Acad Dermatol Venereol. 2012;26(Suppl 3):1–10. doi:10.1111/j.1468-3083.2012.04518.x
6. Körber A, Wilsmann-Theis D, Augustin M, et al. Topical therapy of psoriasis vulgaris – a treatment pathway. J Dtsch Dermatol Ges. 2019;17(Suppl 4):S1–12.
7. National Institute for health and Care Excellence (NICE). Psoriasis: assessment and management. [Updated September, 2017]. Available from: https://www.nice.org.uk/guidance/cg153.
8. Schlager JG, Rosumeck S, Werner RN, et al. Topical treatments for scalp psoriasis: summary of a cochrane systematic review. Br J Dermatol. 2017;176(3):604–614. doi:10.1111/bjd.14811
9. Koo JY. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10(9):1–4.
10. Saraceno R, Camplone G, D’Agostino M, et al. Efficacy and maintenance strategies of two-compound formulation calcipotriol and betamethasone dipropionate gel (Xamiol® gel) in the treatment of scalp psoriasis: results from a study in 885 patients. J Dermatolog Treat. 2014;25(1):30–33. doi:10.3109/09546634.2013.800182
11. Augustin M, Mrowietz U, Bonnekoh B, et al. Topical long-term therapy of psoriasis with vitamin D analogues, corticosteroids and their two compound formulations: position paper on evidence and use in daily practice. J Dtsch Dermatol Ges. 2014;12(8):667–682.
12. Stein Gold LF. Topical therapies for psoriasis: improving management strategies and patient adherence. Semin Cutan Med Surg. 2016;35(2):
13. Strober BE, van der Walt JM, Armstrong AW, et al. Clinical goals and barriers to effective psoriasis care. Dermatol Ther. 2019;9(1):5–18. doi:10.1007/s13555-018-0279-5
14. Feldman SR. Improving adherence to topical treatment. Cutis. 2009;83(4):215–217.
15. NCT02899962. 2019 [cited June 02, 2020]. Available from: https://clinicaltrials.gov/ct2/show/NCT02899962.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.