Back to Journals » Lung Cancer: Targets and Therapy » Volume 13
Spotlight on Tepotinib and Capmatinib for Non-Small Cell Lung Cancer with MET Exon 14 Skipping Mutation
Authors Brazel D, Zhang S ![]() , Nagasaka M
, Nagasaka M ![]()
Received 30 January 2022
Accepted for publication 22 April 2022
Published 13 May 2022 Volume 2022:13 Pages 33—45
DOI https://doi.org/10.2147/LCTT.S360574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sai-Hong Ou
Danielle Brazel,1 Shannon Zhang,1 Misako Nagasaka1– 3
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA; 3Department of Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
Correspondence: Misako Nagasaka, Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA, Email [email protected]
Abstract: Mesenchymal-epithelial transition (MET) receptor tyrosine kinase is overexpressed, amplified, or mutated in 1– 20% of NSCLC. MET dysregulation is associated with a poor prognosis. Recently, development of targeted therapies against MET exon 14 mutations has demonstrated efficacy and tolerability in early trials. Here we focus on tepotinib and capmatinib in regards to molecular characteristics, early preclinical and clinical data, and the emerging role in future studies and clinical practice.
Keywords: tepotinib, capmatinib, mesenchymal-epithelial transition inhibitors, MET, RET, non-small cell lung cancer
Introduction
Lung cancer is the leading cause of cancer death, accounting for almost 25% of cancer-related deaths. Development of targeted therapies has significantly improved overall survival (OS) and quality of life for non-small cell lung cancer (NSCLC) patients demonstrating oncogenic driver mutations.1,2 The mesenchymal-epithelial transition (MET) receptor tyrosine kinase is overexpressed in 20% of NSCLC3–5 and amplified in 1–5% of NSCLC.6 The MET exon 14 (METex14) skipping mutation occurs predominantly in NSCLC7 with a prevalence of 3–4% of NSCLC cases.7,8 MET dysregulation is associated with a poor prognosis in NSCLC9–11 and there was an unmet need for therapeutic blockade of this oncogenic driver. A retrospective analysis showed that use of MET-TKIs improves overall survival in NSCLC patients with METex14 skipping mutations with a hazard ratio of 0.11.12
The MET proto-oncogene is located on 7q31 of chromosome 7 and encodes a receptor tyrosine kinase. The MET receptor is expressed by epithelial cells of many solid organs such as liver, pancreas, prostate, kidney, muscle, and bone marrow.13,14 MET binds to its ligand, hepatocyte growth factor (HGF), causing autophosphorylation of tyrosine residues Y1234 and Y1235 which serve as docking sites for proto-oncogenes such as SRC and intracellular molecules such as PI3K, STAT3, and SHP2.7 This in turn activates signaling pathways involved in embryogenesis, cell proliferation, tissue regeneration, wound healing, and formation of nerve and muscle.15 MET dysregulation in certain types of cancer can occur as gene amplification, point mutations, fusions, exon 14 skipping mutations, or protein overexpression. MET exon 14 skipping mutations (METex14) in NSCLC is the first subtype of MET alterations to have Food and Drug Administration (FDA) approved targeted therapy. Clinically, METex14 mutations are found in patients with a median age at diagnosis of 72.5 years, smoking history, female, and pleomorphic carcinoma or adenosquamous cell carcinoma.7,16,17
Historically, METex14 aberrations have been challenging to detect due to their heterogeneity. Immunohistochemical studies detect MET overexpression, which may occur due to increased gene copy number and gene amplification as well as METex14 mutations.18 Additionally, immunohistochemical staining may be due to a high degree of observer variability in interpretation.4 DNA-based assays include either Sanger single gene or next-generation sequencing (NGS panels). Sanger sequencing has high specificity but low sensitivity compared to NGS panels,19 making NGS more widely implemented in clinical practice. Hybrid capture-based NGS panels have produced fewer false-negative results compared to whole-exome panels.17,20,21 RNA-based PCR assays detect a fusion transcript between MET exon 13 and 15. The interpretation of the PCR-based assays are more straightforward but are limited by a primer to specific sequences, thus making them unable to detect novel mutations. One study found that RNA-based assays detected a higher proportion of METex14 skipping mutations than DNA-based assays.22 Liquid biopsies detecting mutations in cell-free DNA and circulating tumor cells have been used in clinical trials8,23 with high sensitivity.
Small molecule MET inhibitors can be divided into three types; type I, II and III. Type I inhibitors include crizotinib (type Ia), tepotinib and capmatinib (type Ib). They block ATP binding, preventing the phosphorylation and activation of the receptor (Figure 1). Type II inhibitors include cabozantinib and competitively bind to a hydrophobic pocket adjacent to the ATP binding site. Type III inhibitors bind to allosteric sites rather than the ATP binding site.24 Tivantinib is an example of a type III inhibitor but its trial was terminated early due to futility.25
Recently, development of targeted therapies against METex14 mutations have demonstrated efficacy and tolerability in trials. Here we discuss tepotinib and capmatinib in regard to molecular characteristics, early preclinical and clinical data, and their emerging role in future studies and clinical practice.
Tepotinib
Tepotinib (TEPMETKO) is a novel agent that targets and selectively binds MET to disrupt oncogenic signaling and promote tumor cell death (Figure 1).26 On September 11, 2019, the FDA granted Breakthrough Therapy Designation to tepotinib in metastatic NSCLC patients with METex14 skipping mutations who progressed on platinum chemotherapy. Tepotinib gained accelerated approval on February 3, 2021 for this indication.27
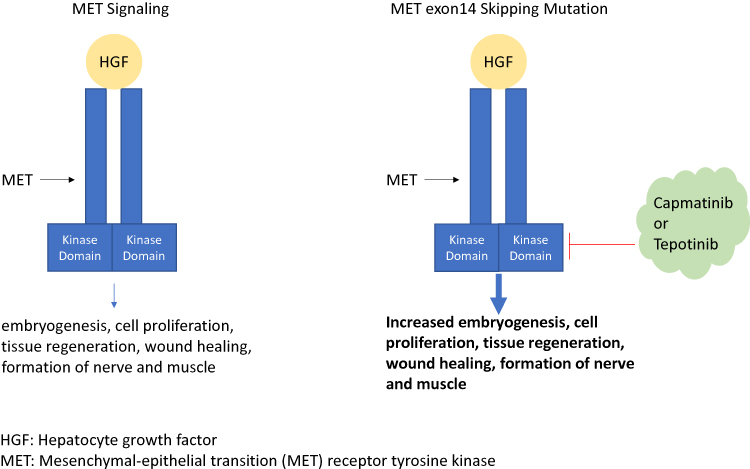 |
Figure 1 Describes the normal MET signaling function (left) and pathogenic effects due to MET exon 14 skipping mutations (right). Capmatinib and tepotinib inhibit the hepatocyte growth factor (HGF). |
Structural Characteristics
Tepotinib (TEPMETKO®, EMD Serono) was synthetically designed to target c-MET thus inhibiting downstream signaling pathways. It binds c-MET in a U-shaped geometry with both hinge and activation loop residue Y1230 to prevent ATP-binding.26
Pharmacodynamic Properties
Tepotinib was shown to inhibit MET kinase with an average IC50 of 1.7 nmol/L. Screening against more than 400 kinases showed the high selectivity of tepotinib for MET.28,29 As shown by the fact that among a panel of 242 protein kinases, only IRAK4, TrkA, Axl, IRAK1 and Mer were inhibited by more than 50% in the presence of tepotinib at 10 mmol/L and with formal IC50 determinations revealing values between 615 and 2272 nmol/L, tepotinib is unlikely to have pharmacologically relevant inhibitory activity against these off-target protein kinases.26 At 1 micrometer, only MET was inhibited in a panel of over 305 kinases.
The recommended dose is 500 mg daily orally once daily after food.29,30
Pharmacokinetics
The median time to maximum dose was 8 to 10 hours after initiation.31 The Cmax and area under the curve (AUC) increased with increasing dose. A dose proportional increase was seen for once-daily doses up to 450 mg. When taken with food, the bioavailability is 71.6%. Food was shown to increase AUC 1.6-fold and Cmax 2-fold.31 The half-life of tepotinib is 32 hours following oral ingestion. Tepotinib is metabolized by CYP3A4 and CYP2C8, which may have implications for drug interactions.
Preclinical Studies
In vivo murine xenograft models of cancer cells, tepotinib was associated with tumor regression regardless of hepatocyte growth factor impact on MET activation.26
In preclinical models, regression of orthotopic brain metastases have been reported with tepotinib administration. Mazieres et al demonstrated that the fraction of unbound tepotinib in rat brain tissue (0.4%) was low compared with plasma (4%), indicating high binding within the brain. In orthotopic brain models, tumors from MET-driven NSCLC brain metastases regressed significantly with a mean tumor volume reduction of 63% for LU5406 and 84% for LU5349.31
Clinical Trials
Phase 1
After a Phase I study of 149 patients with solid tumors (NCT01014936), the recommended dose for Phase II trials was determined to be 500 mg once daily. In this trial, patients received oral tepotinib every 21 days on one of three dose escalation regimens: R1 (n=42) – 30–400 mg daily for 14 days; R2 (n=45) – 30–315 mg daily three times per week; or R3 (n=62) – 300–1400 mg daily.29 Although the maximum tolerated dose was not reached, six patients (R1 n=1, R2 n=3, R3 n=2) reported dose-limiting toxicities. The dose of 500 mg daily was shown to achieve at least 95% MET inhibition in 90% or higher of patients. Treatment related AEs include fatigue, peripheral edema, decreased appetite, nausea, vomiting, and increased lipase.29
Phase 2
In the phase II open-label VISION trial, Paik et al studied tepotinib 500 mg daily in advanced or metastatic NSCLC patients with METex14 skipping mutations (Table 1).8 They compared DNA-based liquid biopsy and RNA-based tissue biopsies. They found similar outcomes in both biopsy groups with ORR 46% (95% CI: 36–57) with median DOR 11.1 months (95% CI: 7.2, could not be estimated). In this trial, 28% of participants experienced grade 3 or higher adverse events, most commonly peripheral edema (7%).
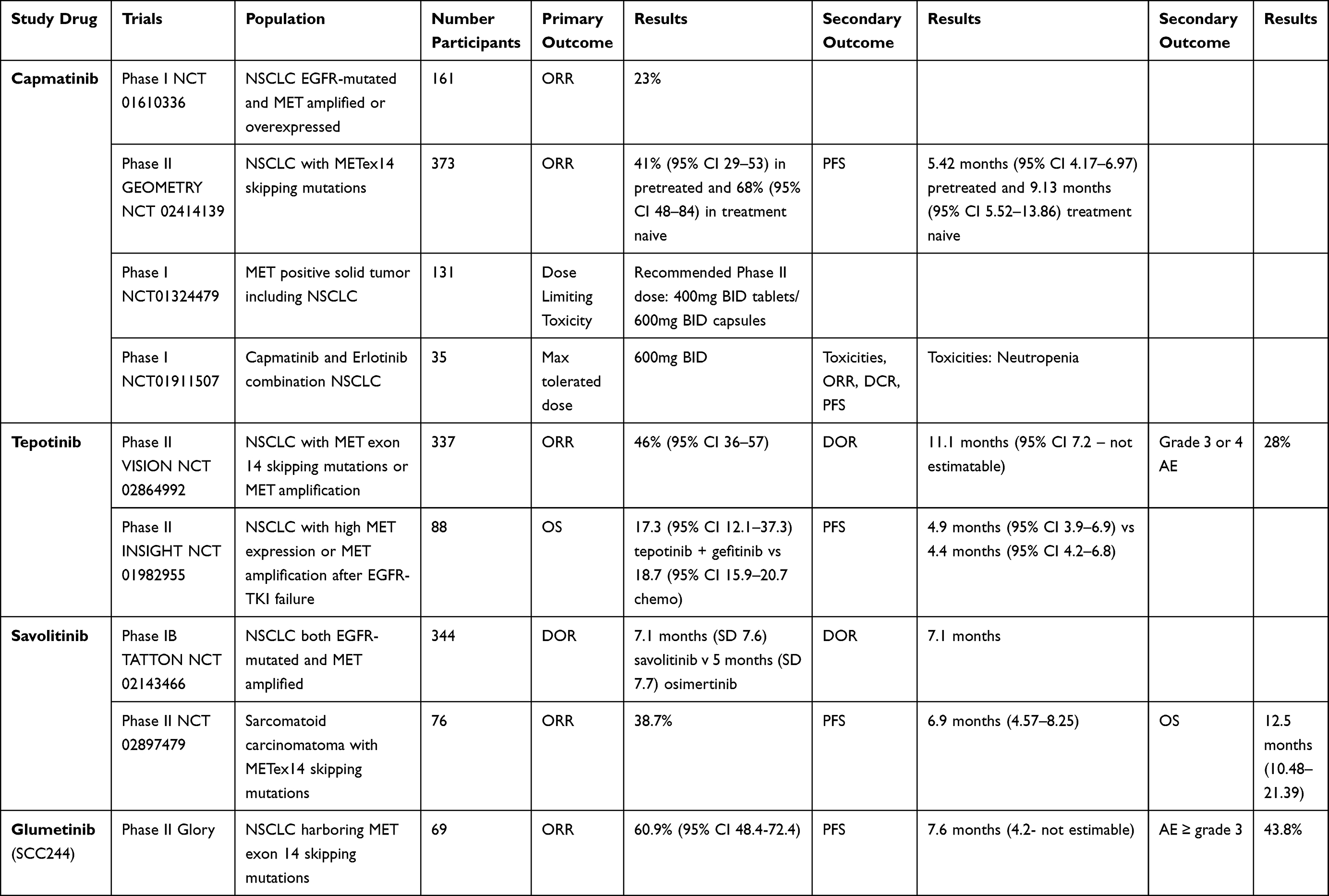 |
Table 1 MET-Targeted Therapy |
Tepotinib has demonstrated intracranial activity. The VISION trial cohort A enrolled 22 patients with neurologically stable baseline brain metastases. Mazieres et al reported efficacy from 21 patients who had at least nine months of follow up.32 The confirmed systemic best overall response was partial response in 52.4% (95% CI 29.8–74.3, 11 patients/21). Median duration of response was 9.5 months (95% CI 5.5-NE) and median PFS was 9.5 months (5.7–11.2).
Safety, Tolerability, and Adverse Events
In the VISION trial, common adverse events included peripheral edema (63%), nausea (26%), diarrhea (22%), increased blood creatinine (18%) and hypoalbuminemia (16%).8
Analysis of pooled adverse effect data from five phase I and phase II studies of tepotinib 500 mg daily (NCT01014936, NCT01832506, NCT01988493, NCT02115373 and NCT02864992) showed 75.4% of participants experienced any adverse event and 22.8% experienced a grade 3 or higher adverse event. The most common adverse events included peripheral edema (33.8%), diarrhea (19.7%), fatigue (14.9%), nausea (12.7%), decreased appetite (11.8%), increased serum creatinine levels (7.9%), hypoalbuminemia (7.0%) and increased amylase levels (5.7%). Dose reductions occurred in 14.5% of patients due to adverse events and treatment was discontinued in 21.5% of patients. There were two fatal adverse events: an upper gastrointestinal hemorrhage and a hypoglycemic coma.33
Capmatinib
Capmatinib also targets and selectively binds the MET tyrosine kinase, including mutations produced by exon 14 skipping, and inhibits cancer cell growth driven by MET aberrations (Figure 1).34 Capmatinib inhibits phosphorylation of MET and its downstream effects, thus inhibiting tumor proliferation and inducing apoptosis in MET-dependent tumor cell lines.35 On May 6 2020, capmatinib was approved by the FDA for use in adults with metastatic NSCLC with a METex14 skipping mutation.36
Structural Characteristics
Capmatinib (Tabrecta™, Novartis) is a selective and potent small molecule MET inhibitor. It functions as an ATP-competitive type 1b MET inhibitor. The central aromatic ring of capmatinib binds to Y1230 of MET tyrosine kinase in a pi stacking interaction.37 Additionally, the Y1230-capmatinib interaction is further stabilized by a salt bridge between D1228 and K1110 of the MET activation loop. The mechanism behind this interaction is similar to that of crizotinib and other selective MET inhibitors.
Pharmacodynamic Properties
The recommended dose of capmatinib is 400 mg administered twice per day to be taken orally with or without food.39 The exposure-response and time course dynamics are largely unknown.
Pharmacokinetics
Capmatinib was measured with multispot ELISA in tumor lysates from the Cancer Cell Line Encyclopedia project.38 MET inhibition was detectable two hours after the last dose with residual phospho-MET recovery in two of three models 12 hours after the last dose.36
In human studies, capmatinib demonstrates linear pharmacokinetics with exposure increasing in both peak plasma concentration (Cmax) and area under the concentration-time curve dose-proportionally within the range of 200–400 mg daily.39 It is rapidly absorbed with Cmax one-to-two hours after administration. The bioavailability of over 70% was similar both with and without food. With twice per day dosing, steady state was reached by day three. The elimination half-life of capmatinib is 6.5 hours. Capmatinib is metabolized by cytochrome P450 A34 (CYP3A4) and aldehyde oxidase.
Of note, caution should be used with other CYP3A4 inhibitors which are shown to increase capmatinib exposure, potentially increasing the incidence and severity of adverse events while CYP3A4 inducers are shown to decrease capmatinib exposure, potentially decreasing antitumor activity.39
Preclinical Studies
Preclinical studies screened capmatinib against 57 different human kinases and found potent selectivity for MET within this panel.35 Investigators found capmatinib activity against MET amplification, MET overexpression, METex14 skipping mutations, and MET activation via expression of HGF ligand. Cancer cell lines without MET aberrations showed poor response to capmatinib, which suggests that strict selection criteria should be used and/or used in combination with other kinase inhibitors to combat MET resistance.37 Another study of capmatinib activity in over 600 cancer cell lines in the Cancer Cell Line Encyclopedia project38 showed that cell lines with MET amplification and MET overexpression were associated with dramatic sensitivity to capmatinib both in vitro and in vivo.37 Overall in vivo xenografts showed a more robust response than in vitro cell lines.37
Clinical Trials
Phase 1
A multicenter dose-escalation and expansion of capmatinib in advanced MET positive solid tumors (NCT01324479) found 400 mg BID or 600 mg BID to be tolerable doses. The maximum tolerated dose was not reached. In heavily pretreated patients with NSCLC, the overall response rate (ORR) was 24% with median progression-free survival (PFS) 7.3 months.40
Phase 2
The GEOMETRY trial (NCT 02414139) was a non-randomized phase II investigation of stage IIIB/IV NSCLC patients with METex14 skipping mutations (Table 1). This included 69 pretreated patients and 28 treatment naïve patients. Participants received capmatinib 400 mg BID. The ORR was 41% (95% CI 29–53) in pretreated patients and 68% (95% CI 48–84) in treatment naïve patients. A 4% complete response (CR) rate was seen in the treatment naïve cohort. The median duration of response (DOR) was 9.7 months (95% CI 5.5–13) in the pretreated population versus 12.6 months (95% CI 5.5–25.3) in treatment naïve patients. The median PFS was 5.42 and 9.69 months, respectively. Of note, capmatinib was shown to cross the blood brain barrier with a 54% intracranial response in the phase II GEOMETRY study.41
Another clinical trial in China (NCT 02276027) of 66 patients who failed prior therapy or were unable to receive chemotherapy received targeted therapy based on mutational status (capmatinib – MET, ceritinib – ALK/ROS, binimetinib – KRAS/NRAS/BRAF, and alpelisib – PIK3CA). There was an 18.8% confirmed partial response with capmatinib.42
Safety, Tolerability, and Adverse Events
In the phase II GEOMETRY trial the most common adverse events included peripheral edema (52%), nausea (44%), fatigue (32%), vomiting (28%), dyspnea (24%), and decreased appetite (21%). The most common grade 3 or 4 adverse events were peripheral edema (9%), fatigue (8%), and dyspnea (7%).39,41 Dose interruptions due to adverse events occurred in 54% of patients due to peripheral edema, increased serum creatinine, nausea, or vomiting. Dose reductions occurred in 23% of patients due to peripheral edema, increased alanine aminotransferase (ALT), increased serum creatinine, and nausea.
Future Directions
MET TKIs for EGFR TKI Resistance
MET is implicated as the cause of acquired/adapted resistance to targeted therapies43–50 which further emphasizes the importance of developing potent MET inhibitors.
Based on studies of resistance to EGFR-TKIs, acquired resistance may occur through MET amplification or codriver gene alterations.7 In EGFR-mutated NSCLC, coexisting MET amplification is reported in 4–40% of cases. Codriver gene alterations occur through EGFR amplification (6.4–28.5%), FGFR1 alteration (4.8–16.6%), KRAS activation (8%) or BRAF activation (21.4%) or PIK3CA mutation/amplification (14.2%).51,52
Preclinical data suggested that tepotinib can overcome acquired resistance to EGFR TKIs due to MET signaling pathway.53 Indeed, in the phase II portion of the INSIGHT study (NCT01982955), patients with EGFR-mutant T790M negative NSCLC with either high MET expression by immunohistochemical staining or MET amplification after EGFR-TKI treatment failure were randomly assigned to tepotinib plus gefitinib or to standard platinum-based chemotherapy. At interim data analysis, the combination of tepotinib and gefitinib significantly improved OS and PFS in the MET amplification cohort and high expression cohort. For the MET amplification cohort, the HR was 0.13 for PFS and 0.08 for OS (n=19; median PFS 16.6 months (8.3-not estimable) vs 4.2 months (1.4–7.0); HR 0.13, 0.04–0.43; median OS 37.3 months (90% CI not estimable) vs 13.1 months (3.25-not estimable); HR 0.08, 0.01–0.51)). For the MET high expression cohort, the HR was 0.35 for PFS and 0.33 for OS (n=34; median PFS 8.3 months (4.1–16.6) vs 4.4 months (4.1–6.8); HR 0.35, 0.17–0.74; median OS 37.3 months (90% CI 24.2–37.3) vs 17.9 months (12.0–20.7); HR 0.33, 0.14–0.76)).30
Data also suggests promising results with capmatinib. In EGFR-mutant NSCLC cell lines with developed resistance to EGFR inhibitors and MET dysregulation, capmatinib restores sensitivity to EGFR inhibitors.37,54 Indeed, in a phase 1b trial combining capmatinib and gefitinib in EGFR-mutated, MET amplified or overexpressing NSCLC (NCT01610336), the ORR was found to be 23%.55 Better ORR (47%) and median PFS (5.5 months) were demonstrated in patients with a MET gene copy number of at least 6.
MET inhibitors may allow us to overcome other resistance pathways outside of EGFR. Baltschukat et al found that EML4-ALK translocated PDX cells expressed very high MET mRNA levels without MET amplification and high phospho-MET protein levels. This model did not respond to the second-generation ALK inhibitor ceritinib but when ceritinib was combined with capmatinib, tumor cells regressed.37
Mechanisms of Resistance to MET TKIs
MET-TKI resistance can be acquired through secondary MET mutations or activation of alternate signaling pathways. In a prior study of crizotinib, 35% of patients developed MET mutations and 45% developed mutations in bypass pathways.56 In vitro analysis using Ba/F3 models found MET secondary mutations of D1228 and Y1230 in the activation loop.57 These findings are confirmed by case reports of patients with D1228 and Y1230 mutations who show resistance to MET inhibitors.58,59 Potential alternate pathway mutations for acquired resistance include KRAS amplification/mutation and PIK3CA mutation.7 Changes in MET gene copy number could be another potential mechanism of resistance although the activity of tepotinib and capmatinib in MET-amplified tumors will still need to be better established first.
Ongoing Clinical Trials
Ongoing clinical trials are listed in Table 2. MET inhibitors are being combined with various immune checkpoint inhibitors (NCT04323436, NCT04139317, NCT02323126, NCT03647488). Combination strategies with EGFR TKIs are also being evaluated in the post EGFR TKI progression setting (NCT04816214, NCT03940703).
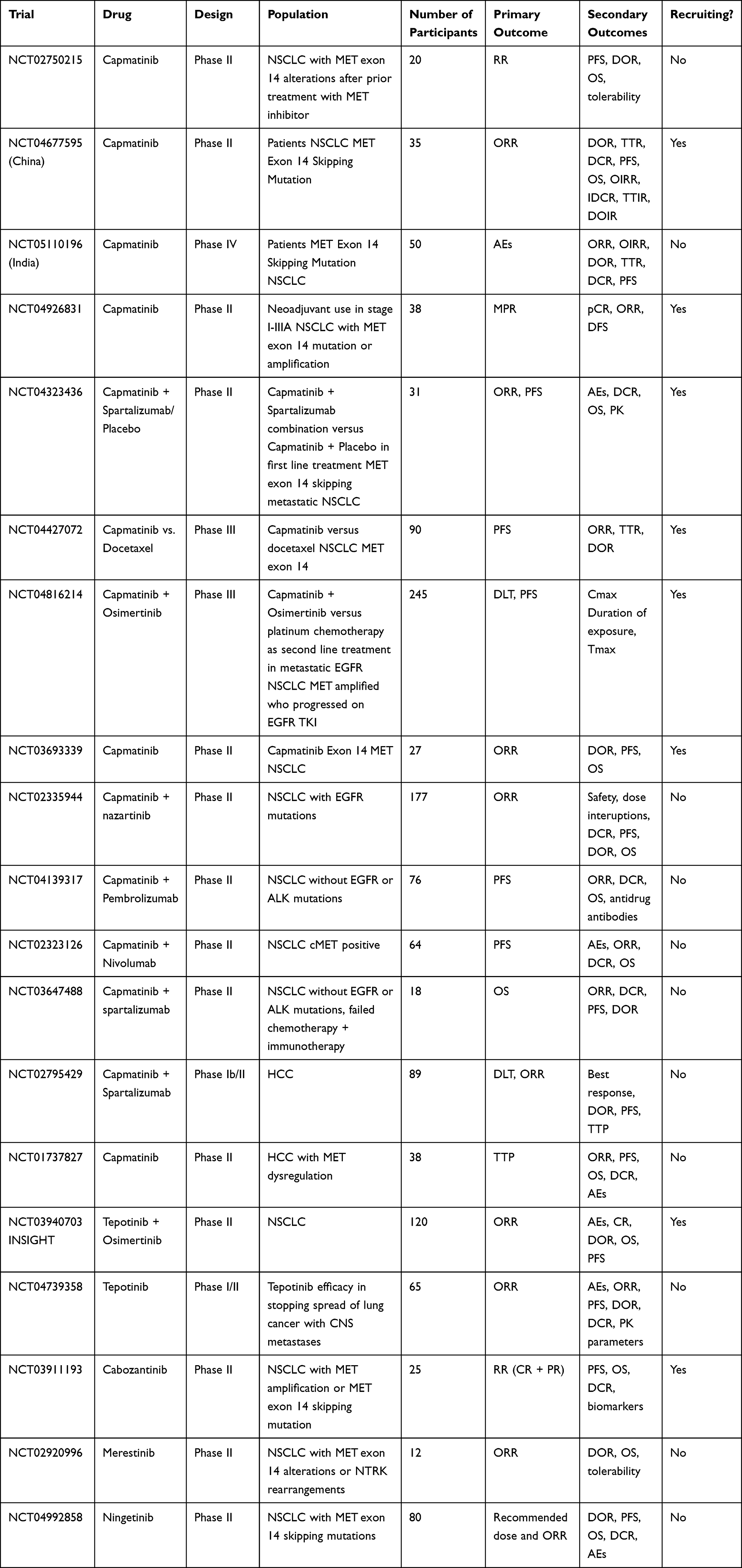 |
Table 2 Ongoing Clinical Trials |
Other Agents Under Investigation
Savolitinib
Savolitinib (Orpathys, HUTCHMED, AstraZeneca) is being investigated in combination with other therapies in the treatment of NSCLC. Interim analysis of the TATTON phase Ib trial of third generation EGFR-TKI osimertinib plus MET inhibitor savolitinib in NSCLC patients with both EGFR mutations and MET amplifications showed ORR 52% with median DOR 7.1 months (Table 1).60 The most common adverse effects were nausea (37%), diarrhea (30%), fatigue (28%), decreased appetite (28%), pyrexia (26%), and vomiting (22%). Serious adverse effects occurred in 37% of patients.
Another phase II trial is examining savolitinib in lung sarcomatoid carcinoma and other NSCLC with METex14 skipping mutations (NCT02897479). At interim analysis, 38.7% of patients had a partial response to therapy. The most common adverse effects were nausea (41%), peripheral edema (38%), increased ALT (32%), increased AST (29%), and vomiting (21%).23 The final analysis was presented at the European Lung Cancer Congress 2022 and reported investigator assessed median PFS of 6.9 months and median OS of 12.5 months.65
Glumetinib
Glumetinib (SCC244) is another highly selective MET inhibitor. Results from the pivotal phase II study66 is summarized in Table 1.
MET Antibodies
Antibodies against MET bind to the sema domain for HGF binding. MET antibodies are proposed to increase receptor internalization and degradation, thus inhibiting the MET signaling pathway. Currently an IgG1 monoclonal antibody Sym015 (Symphogen, Copenhagen, Denmark) is being developed for METex14 NSCLC.
Amivantamab
Amivantamab (JNJ-61186372, Rybrevant, Janssen Biotech) is a bispecific antibody that simultaneously blocks EGFR and cMET receptors. Promising results from the phase I CHRYSALIS trial provided the basis for FDA accelerated approval of amivantamab. This study assessed 81 patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations after treatment with platinum-based chemotherapy. The authors found overall response rate of 40% with median duration of response of 11.1 months.61
Immunotherapy
Retrospective studies show that PD-L1 expression is high in METex14 NSCLC.7 Some studies have shown promise for monotherapy with immune checkpoint inhibitors in METex14 mutated cancers, however this data is retrospective and from small cohort sizes. MET activity in immune cells is associated with immune suppression62 and capmatinib activity has been shown to enhance the activity of immune therapies.63 Indeed, in a post hoc analysis of the GEOMETRY phase II trial, patients previously treated with immune checkpoint inhibitors were significantly more sensitive to capmatinib than those treated with chemotherapy (64 vs 32%).64 There may be a role of combinatory approaches with MET inhibitors and immunotherapy although (immune related) adverse events must be carefully monitored. Ongoing clinical trials are listed in Table 2.
Further clinical trials are needed in MET overexpression and amplified NSCLC. Compared to MET-mutated tumors, MET overexpressed and amplified tumors are anticipated to have lower response rates and shorter survival with MET inhibitors. The most appropriate definition (or cut-off) of MET overexpression or amplification as a potential biomarker needs to be further clarified.
Additionally, more research is needed into the role of both tepotinib and capmatinib in patients with metastatic brain lesions in the front line and refractory setting. Although brain metastases are common in lung cancer, the incidence of brain metastases in METex14 NSCLC is unknown. In the VISION trial, only 11% of patients had brain metastases at study entry.8 In the phase II GEOMETRY study, capmatinib showed encouraging results with a 54% intracranial response.40
Conclusion
The approval of tepotinib and capmatinib has made metastatic METex14 an actionable oncogenic driver in NSCLC, identifying a new subset of patients eligible for targeted treatment options. Tepotinib and capmatinib are potent, highly selective MET inhibitors with robust response in NSCLC. Preclinical and clinical data have shown both tepotinib and capmatinib as effective and tolerable in NSCLC patients with METex14 skipping mutations. When used in combination with EGFR TKIs, MET targeted therapies have the potential to overcome resistance to these treatments driven through the MET signaling pathway. This is of particular importance as with the frontline use of osimertinib, T790M will no longer be the resistance mechanism and we should see an increase in MET pathway related resistance to EGFR TKIs. Additionally, resistance pathways to MET TKIs themselves and strategies to overcome them must be further evaluated.
Abbreviations
ALK, anaplastic lymphoma kinase; ALT, alanine aminotransferase; AUC, area under the curve; BRAF, v-raf murine sarcoma viral oncogene homolog B1; CI, confidence interval; Cmax, peak plasma concentration; CR, complete response; CYP3A4, cytochrome p450 3A4; DOR, duration of response; EGFR, epidermal growth factor receptor; FDA, food and drug administration; HEF, hepatocyte growth factor ligand; KRAS, Kirsten rat sarcoma virus; MET, mesenchymal epithelial transition; METex14, MET exon 14 skipping mutations; NGS, next generation sequencing; NRAS, neuroblastoma rat sarcoma virus; NSCLC, non-small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression free survival; TKI, tyrosine kinase inhibitor.
Ethics Approval and Consent to Participate
This report did not meet criteria for IRB approval.
Funding
No funding was secured for this report.
Disclosure
Dr Misako Nagasaka reports personal fees from AstraZeneca, Caris Life Sciences, Daiichi Sankyo, Takeda, Novartis, EMD Serono, Blueprint, Janssen, Pfizer, Lilly, Genentech, and Mirati; personal fees, non-financial support from AnHeart, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Takano T, Fukui T, Ohe Y, et al. EGFR mutations predict survival benefit from gefitinib in patients with advanced lung adenocarcinoma: a historical comparison of patients treated before and after gefitinib approval in Japan. J Clin Oncol. 2008;26(34):5589–5595. doi:10.1200/JCO.2008.16.7254
2. Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
3. Tsakonas G, Botling J, Micke P, et al. c-MET as a biomarker in patients with surgically resected non-small cell lung cancer. Lung Cancer. 2019;133:69–74. doi:10.1016/j.lungcan.2019.04.028
4. Bubendorf L, Dafni U, Schobel M, et al. Prevalence and clinical association of MET gene overexpression and amplification in patients with NSCLC: results from the European Thoracic Oncology Platform (ETOP) lungscape project. Lung Cancer. 2017;111:143–149. doi:10.1016/j.lungcan.2017.07.021
5. Huang L, An S-J, Chen Z-H, Su J, Yan -H-H, Wu Y-L. MET expression plays differing roles in non-small-cell lung cancer patients with or without EGFR mutation. J Thorac Oncol. 2014;9:725–728. doi:10.1097/JTO.0000000000000105
6. Drilon A, Cappuzzo F, Ou S-HI, Camidge DR. Targeting MET in lung cancer: will expectations finally be MET? J Thorac Oncol. 2017;12:15–26. doi:10.1016/j.jtho.2016.10.014
7. Fujino T, Suda K, Mitsudomi T. Emerging MET tyrosine kinase inhibitors for the treatment of non-small cell lung cancer. Expert Opin Emerg Drugs. 2020;25(3):229–249. doi:10.1080/14728214.2020.1791821
8. Paik PK, Felip E, Veillon R, et al. Tepotinib in non-small-cell lung cancer with MET exon 14 skipping mutations. N Engl J Med. 2020;383:931–943. doi:10.1056/NEJMoa2004407
9. Guo B, Cen H, Tan X, et al. Prognostic value of MET gene copy number and protein expression in patients with surgically resected non-small cell lung cancer: a meta-analysis of published literatures. PLoS One. 2014;9(6):e99399. doi:10.1371/journal.pone.0099399
10. Lee GD, Lee SE, Oh DY, et al. MET exon 14 skipping mutations in lung adenocarcinoma: clinicopathologic implications and prognostic values. J Thorac Oncol. 2017;12(8):1233–1246. doi:10.1016/j.jtho.2017.04.031
11. Yeung SF, Tong JHM, Law PPW, et al. Profiling of oncogenic driver events in lung adenocarcinoma revealed MET mutation as independent prognostic factor. J Thorac Oncol. 2015;10:1292–1300. doi:10.1097/JTO.0000000000000620
12. Awad MM, Leonardi GC, Kravets S, et al. Impact of MET inhibitors on survival among patients with non-small cell lung cancer harboring MET exon 14 mutations: a retrospective analysis. Lung Cancer. 2019;133:96–102. doi:10.1016/j.lungcan.2019.05.011
13. Zhang Y, Xia M, Jin K, et al. Function of the c-Met receptor tyrosine kinase in carcinogenesis and associated therapeutic opportunities. Mol Cancer. 2018;17(1):45. doi:10.1186/s12943-018-0796-y
14. Organ SL, Tsao MS. An overview of the c-MET signaling pathway. Ther Adv Med Oncol. 2011;3(1 Suppl):S7–S19. doi:10.1177/1758834011422556
15. Dhillon S. Capmatinib: first approval. Drugs. 2020;80:1125–1131. doi:10.1007/s40265-020-01347-3
16. Vuong HG, Ho ATN, Altibi AMA, et al. Clinicopathological implications of MET exon 14 mutations in non-small cell lung cancer -A systematic review and meta-analysis. Lung Cancer. 2018;123:76–82. doi:10.1016/j.lungcan.2018.07.006
17. Awad MM, Oxnard GR, Jackman DM, et al. MET exon 14 mutations in non–small-cell lung cancer are associated with advanced age and stage-dependent MET genomic amplification and c-Met overexpression. J Clin Oncol. 2016;34(7):721–730. doi:10.1200/JCO.2015.63.4600
18. O’Brien O, Wright MC, O’Brien C, et al. Cost-efficient and easy to perform PCR-based assay to identify met exon 14 skipping in formalin-fixed paraffin-embedded (FFPE) non-small cell lung cancer (NSCLC) samples. Diagnostics. 2019;9. doi:10.3390/diagnostics9010013
19. Kim EK, Kim KA, Lee CY, et al. Molecular diagnostic assays and clinicopathologic implications of MET exon 14 skipping mutation in non-small-cell lung cancer. Clin Lung Cancer. 2019;20(1):e123–e132. doi:10.1016/j.cllc.2018.10.004
20. Frampton GM, Ali SM, Rosenzweig M, et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 2015;5(8):850–859. doi:10.1158/2159-8290.CD-15-0285
21. Schrock AB, Frampton GM, Suh J, et al. Characterization of 298 patients with lung cancer harboring MET exon 14 skipping alterations. J Thorac Oncol. 2016;11(9):1493–1502. doi:10.1016/j.jtho.2016.06.004
22. Davies KD, Lomboy A, Lawrence CA, et al. DNA-based versus RNA-based detection of MET exon 14 skipping events in lung cancer. J Thorac Oncol. 2019;14(4):737–741. doi:10.1016/j.jtho.2018.12.020
23. Lu S, Fang J, Cao L, et al. Preliminary efficacy and safety results of savolitinib treating patients with pulmonary sarcomatoid carcinoma (PSC) and other types of non-small cell lung cancer (NSCLC) harboring MET exon 14 skipping mutations.
24. Reungwetwattana T, Liang Y, Zhu V, et al. The race to target MET exon 14 skipping alterations in non-small cell lung cancer: the why, the how, the who, the unknown, and the inevitable. Lung Cancer. 2017;103:27–37. doi:10.1016/j.lungcan.2016.11.011
25. Scagliotti G, von Pawel J, Novello S, et al. Phase III multinational, randomized, double-blind, placebo-controlled study of tivantinib (ARQ 197) plus erlotinib versus erlotinib alone in previously treated patients with locally advanced or metastatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2015;33(24):2667–2674. doi:10.1200/JCO.2014.60.7317
26. Bladt F, Faden B, Friese-Hamim M, et al. EMD 1214063 and EMD 1204831 constitute a new class of potent and highly selective c-Met inhibitors. Clin Cancer Res. 2013;19(11):2941–2951. doi:10.1158/1078-0432.CCR-12-3247
27. US Food & Drug Administration. FDA grants accelerated approval to tepotinib for metastatic non-small cell lung cancer [media release]; 2021. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-tepotinib-metastatic-non-small-cell-lung-cancer.
28. Markham A. Tepotinib: fIrst approval. Drugs. 2020;80:829–833. doi:10.1007/s40265-020-01317-9
29. Falchook GS, Kurzrock R, Amin HM, et al. First-in-man phase I trial of the selective MET inhibitor tepotinib in patients with advanced solid tumors. Clin Cancer Res. 2020;26(6):1237–1246. doi:10.1158/1078-0432.CCR-19-2860
30. Wu Y-L, Cheng Y, Zhou J, et al. Tepotinib plus gefitinib in patients with EGFR-mutant non-small-cell lung cancer with MET overexpression or MET amplification and acquired resistance to previous EGFR inhibitor (INSIGHT study): an open-label, phase 1b/2, multicentre, randomized trial. Lancet Respir Med. 2020;8(11):1132–1143. doi:10.1016/S2213-2600(20)30154-5
31. EMD Serono Medical Resources. Tepmetko® (tepotinib) tablets prescribing informtaion. Available from: https://medical.emdserono.com/en_US/home/oncology/tepmetko-tepotinib-tablets/tepmetko-tepotinib-prescribing-information.html.
32. Mazieres J, Veillon R, Felip E, et al. Activity of tepotinib in brain metastases: preclinical models and clinical data from patients with MET exon 14 skipping NSCLC.
33. Yamazaki K, Ryoo BY, Doi T, et al. Pooled safety analysis of tepotinib in Asian patients with advanced solid tumours [abstract no. 67P]. Ann Oncol. 2019;30(Suppl 9):ix26. doi:10.1093/annonc/mdz420.006
34. Tan AC, Loh TJ, Kwang AL, et al. Therapies for metastatic non-small cell lung cancer with MET exon 14 Alterations: a spotlight on capmatinib. Lung Cancer. 2021;12:11–20. doi:10.2147/LCTT.S263610
35. Liu X, Wang Q, Yang G, et al. A novel kinase inhibitor, INCB28060, blocks c-MET-dependent signaling, neoplastic activities, and cross-talk with EGFR and HER-3. Clin Cancer Res. 2011;17:7127–7138. doi:10.1158/1078-0432.CCR-11-1157
36. US Food & Drug Administration. FDA grants accelerated approval to capmatinib for metastatic non-small cell lung cancer [media release]; 2021. Available from: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-grants-accelerated-approval-capmatinib-metastatic-non-small-cell-lung-cancer.
37. Baltschukat S, Engstler BS, Huang A, et al. Capmatinib (INC280) is active against models of non-small cell lung cancer and other cancer types with defined mechanisms of MET activation. Transl Cancer Mech Ther. 2019. doi:10.1158/1078-0432
38. Barretina J, Caponigro G, Stransky N, et al. The cancer cell line encyclopedia enables predictive modelling of anticancer drug sensitivity. Nature. 2012;483:603–607. doi:10.1038/nature11003
39. Novartis. TABRECTA TM (capmatinib): US prescribing information; 2020. Available from: https://www.accessdatafda.gov/drugsatfda_docs/label/2020/213591s000lbl.pdf.
40. Bang YJ, Su WC, Schuler M, et al. Phase 1 study of capmatinib in MET-positive solid tumor patients: dose escalation and expansion of selected cohorts. Cancer Sci. 2020;111(2):536–547. doi:10.1111/cas.14254
41. Wolf J, Seto T, Han J-Y, et al. Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell lung cancer. N Engl J Med. 2020;383:944–957. doi:10.1056/NEJMoa2002787
42. Zhou Q, Zhang X-C, Tu H-Y, et al. Biomarker-integrated study of a single agent targeting molecular alterations of PI3KCA, MET, ALK, ROS1, KRAS, NRAS, or BRAF in advanced NSCLC: Phase 2 umbrella trial in China (CTONG1505). Ann Oncol. 2018;29(9):IX113. doi:10.1093/annonc/mdy441.002
43. Engelman JA, Zejnullahu K, Mitsudomi T, et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science. 2007;316(5827):1039–1043. doi:10.1126/science.1141478
44. Bean J, Brennan C, Shih JY, et al. MET amplification occurs with or without T790M mutations in EGFR mutant lung tumors with acquired resistance to gefitinib or erlotinib. Proc Natl Acad Sci USA. 2007;104(52):20932–20937. doi:10.1073/pnas.0710370104
45. Chen HJ, Mok TS, Chen ZH, et al. Clinicopathologic and molecular features of epidermal growth factor receptor T790M mutation and c-MET amplification in tyrosine kinase inhibitor-resistant Chinese non-small cell lung cancer. Pathol Oncol Res. 2009;15(4):651–658. doi:10.1007/s12253-009-9167-8
46. Sequist LV, Waltman BA, Dias-Santagata D, et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med. 2011;3:75ra26–75ra26. doi:10.1126/scitranslmed.3002003
47. Yu HA, Arcila ME, Rekhtman N, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. 2013;19(8):2240–2247. doi:10.1158/1078-0432.CCR-12-2246
48. Papadimitrakopoulou VA, Wu YL, Han JY, et al. Analysis of resistance mechanisms to osimertinib in patients with EGFR T790M advanced NSCLC from the AURA3 study. Ann Oncol. 2018;29:viii741. doi:10.1093/annonc/mdy424.064
49. Ramalingam SS, Cheng Y, Zhou C, et al. Mechanisms of acquired resistance to first-line osimertinib: preliminary data from the phase III FLAURA study. Ann Oncol. 2018;29:viii740. doi:10.1093/annonc/mdy424.063
50. Dagogo-Jack I, Yoda S, Lennerz JK, et al. MET alterations are a recurring and actionable resistance mechanism in ALK-positive lung cancer. Clin Cancer Res. 2020;26(11):2535–2545. doi:10.1158/1078-0432.CCR-19-3906
51. Rotow JK, Gui P, Wu W, et al. Co-occurring alterations in the RAS-MAPK pathway limit response to MET inhibitor treatment in MET exon 14 skipping mutation-positive lung cancer. Clin Cancer Res. 2019;26(2):439–449. doi:10.1158/1078-0432.CCR-19-1667
52. Jamme P, Fernandes M, Copin M-C, et al. Alterations in the PI3K pathway drive resistance to MET inhibitors in NSCLC harboring MET exon 14 skipping mutations. J Thoracic Oncol. 2020;15(5):741–751. doi:10.1016/j.jtho.2020.01.027
53. Manja Friese-Hamim FBGL. The selective c-Met inhibitor tepotinib can overcome epidermal growth factor receptor inhibitor resistance mediated by aberrant c-Met activation in NSCLC models. Am J Cancer Res. 2017;7(4):962–972.
54. Lara MS, Holland WS, Chinn D, et al. Preclinical evaluation of MET inhibitor INC-280 with or without the epidermal growth factor receptor inhibitor erlotinib in non-small-cell lung cancer. Clin Lung Cancer. 2017;18(3):281–285.
55. Wu YL, Zhang L, Kim DW, et al. Phase Ib/II study of capmatinib (INC280) plus gefitinib after failure of epidermal growth factor receptor (EGFR) inhibitor therapy in patients with EGFR-mutated, MET factor-dysregulated non-small-cell lung cancer. J Clin Oncol. 2018;36(31):3101–3109. doi:10.1200/JCO.2018.77.7326
56. Recondo G, Bahcall M, Spurr LF, et al. Molecular mechanisms of acquired resistance to MET tyrosine kinase inhibitors in patients with MET Exon 14–Mutant NSCLC. Clin Cancer Res. 2020;26(11):2615. doi:10.1158/1078-0432.CCR-19-3608
57. Fujino T, Kobayashi Y, Suda K, et al. Sensitivity and resistance of MET Exon 14 mutations in lung cancer to eight MET tyrosine kinase inhibitors in vitro. J Thoracic Oncol. 2019;14(10):1753–1765. doi:10.1016/j.jtho.2019.06.023
58. Heist RS, Sequist LV, Borger D, et al. Acquired resistance to crizotinib in NSCLC with MET exon 14 skipping. J Thorac Oncol. 2016;11:1242–1245. doi:10.1016/j.jtho.2016.06.013
59. Ou SI, Young L, Schrock AB, et al. Emergence of preexisting MET Y1230C mutation as a resistance mechanism to crizotinib in NSCLC with MET exon 14 skipping. J Thorac Oncol. 2017;12:137–140. doi:10.1016/j.jtho.2016.09.119
60. Yu H, Ahn MJ, Kim SW, et al. TATTON phase Ib expansion cohort: osimertinib plus savolitinib for patients (pts) with EGFR-mutant, MET-amplified NSCLC after progression on prior first/second-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI).
61. Sabari JK, Shu CA, Park K, et al. Amivantamab in post-platinum EGFR exon 20 insertion mutant non–small cell lung cancer. WorldConf Lung Cancer. 2021;16:s108–s109.
62. Molnarfi N, Benkhoucha M, Funakoshi H, Nakamura T, Lalive PH. Hepatocyte growth factor: a regulator of inflammation and autoimmunity. Autoimmun Rev. 2015;14:293–303. doi:10.1016/j.autrev.2014.11.013
63. Glodde N, Bald T, van den Boorn-konijnenberg D, et al. Reactive neutrophil responses dependent on the receptor tyrosine kinase cMET limit cancer immunotherapy. Immunity. 2017;47:789–802.e9. doi:10.1016/j.immuni.2017.09.012
64. Vansteenkiste JF, Smit EF, Groen HJM, et al. 1285P Capmatinib in patients with METex14-mutated advanced non-small cell lung cancer who received prior immunotherapy: the phase II GEOMETRY mono-1 study. Ann Oncol. 2020;2:31.
65. Lu S, Fang J, Li X, et al. Final OS results and subgroup analysis of savolitinib in patients with MET exon 14 skipping mutations(METex14+) NSCLC. Presented at: European Lung Cancer Congress 2022; Mar 30-April 2, 2022; Prague, Czech Republic.
66. Lu s. Phase II Study of SCC244 in NSCLC Patients Harboring MET exon 14(METex14) Skipping Mutations (GLORY Study). Presented at American Association for Cancer Research; April 8-13, 2022; New Orleans, USA.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.