Back to Journals » Drug Design, Development and Therapy » Volume 10
Spotlight on botulinum toxin and its potential in the treatment of stroke-related spasticity
Received 3 November 2015
Accepted for publication 12 January 2016
Published 8 March 2016 Volume 2016:10 Pages 1085—1099
DOI https://doi.org/10.2147/DDDT.S80804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Wei Duan
Michelle Kaku, David M Simpson
Department of Neurology, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Abstract: Poststroke spasticity affects up to one-half of stroke patients and has debilitating effects, contributing to diminished activities of daily living, quality of life, pain, and functional impairments. Botulinum toxin (BoNT) is proven to be safe and effective in the treatment of focal poststroke spasticity. The aim of this review is to highlight BoNT and its potential in the treatment of upper and lower limb poststroke spasticity. We review evidence for the efficacy of BoNT type A and B formulations and address considerations of optimal injection technique, patient and caregiver satisfaction, and potential adverse effects of BoNT.
Keywords: poststroke spasticity, botulinum toxin, onabotulinumtoxinA, incobotulinumtoxinA, rimabotulinumtoxinB
Introduction
Spasticity is a velocity-dependent increase in muscle tone as a part of the upper motor neuron syndrome and is seen in a wide variety of neurologic diseases including stroke.1 Poststroke spasticity can develop as early as 1 week after stroke,2 and it is estimated to occur in up to one-half of stroke survivors.3 The most frequent predictors of spasticity include weakness and reduced motor control.2 Long-term spasticity may lead to tendon contractures and limb deformities that can cause significant pain and functional impairment. Depending on the location of the spasticity, this can impact mobility, activities of daily living such as toileting, dressing, and transferring, and quality of life (QoL) and increase the dependence on caregivers.4
The aim of the treatment in poststroke spasticity is focused on muscle limb overactivity reduction. Treatment modalities are used to alleviate spasticity including physical therapy, systemic and intrathecal medications, and surgery. Systemic medications can be helpful if spasticity is generalized. Agents such as baclofen (gamma-aminobutyric acid [GABA]-B receptor agonist) diazepam (GABA-A receptor agonist), dantrolene (decreases calcium release from skeletal muscle sarcoplasmic reticulum), or tizanidine (TZD; alpha-2 adrenergic receptor agonist) often have systemic side effects such as dry mouth, dizziness, sedation, or generalized weakness.5 After several months of treatment, tolerance may develop to systemic medications.
Chemodenervation and neurolytic procedures with alcohol or phenol may be utilized as second-line management. These techniques are more localized and are injected perineurally to destroy the nerve causing spasticity. The effect may be limited by partial nerve regeneration and adverse effects such as bladder, bowel, and sexual dysfunction.6 Intrathecal baclofen acts on GABA receptors in the lumbar spinal cord and may improve walking speed and functional mobility in poststroke spasticity. However, this therapy is invasive and limited by side effects including nausea, vomiting, and urinary retention. Overdosing may lead to death.7,8
The aim of this review is to highlight botulinum toxin (BoNT) and its potential in the treatment of upper and lower limb poststroke spasticity. Optimal treatment may include BoNT injections into focal muscles in conjunction with an integrated multidisciplinary team approach and intensive rehabilitation programs or to help utilize affected muscles.9 Higher-intensity rehabilitation programs (≥3 1-hour weekly session for ~10 weeks) may help patients achieve more upper limb goals following BoNT injections for spasticity when compared with usual care programs (≤2 1-hour weekly sessions).10 A recent consensus panel of 44 neurologists and physiatrists with experience in BoNT therapy recommended starting a rehabilitation program during the first week after BoNT injection therapy.11
Pharmacology
There have been major advances in synthesizing BoNT for therapeutic use since the German physician Justinus Kerner first proposed using it clinically in the early 19th century and coined the term “sausage poison.”12 BoNT is synthesized by the anaerobic bacteria Clostridium botulinum, Clostridium baratii, and Clostridium butyricum.13 Serotypes A through G are produced by C. botulinum, serotypes F and C are produced by C. baratii, and serotype E is produced by C. butyricum. Each serotype has a different neurotoxin complex protein structure and is synthesized as polypeptides. All serotypes exert their mechanism of action by inhibiting the release of acetylcholine from nerve endings at the neuromuscular junction.14,15 However, each exerts its effects via different protein structures and intracellular targets and, therefore, has different potencies and length of effect.16 There are currently two serotypes of BoNT, serotypes A and B, that are widely available on the market. The US Food and Drug Administration (FDA) has approved four preparations in the USA. The serotype A (BoNT-A): abobotulinumtoxinA (Dysport; Ipsen, Paris, France), onabotulinumtoxinA (Botox; Allergan, Inc., Irvine, CA, USA), and incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals GmbH, Frankfurt, Germany) and serotype B (BoNT-B): rimabotulinumtoxinB (Myobloc/Neurobloc; Solstice Neurosciences, Inc., San Francisco, CA, USA). OnabotulinumtoxinA and more recently abobotulinumtoxinA are currently the only approved treatments for upper limb spasticity in adults approved by the FDA.
Each toxin serotype consists of a light chain (50 kDa) and a heavy chain (100 kDa) that is linked by a disulfide bond. This forms a protein with a total molecular weight of 150 kDa. Of the BoNT-A formulations, abobotulinumtoxinA and onabotulinumtoxinA contain the 150 kDa neurotoxin as part of a larger complexing protein, whereas incobotulinumtoxinA contains only the 150 kDa neurotoxin.17 In order to become active, the neurotoxin must be nicked by proteases into two fragments.18 Under normal circumstances, a nerve action potential causes acetylcholine to be released by vesicles from the presynaptic membrane. This requires a complex set of proteins called soluble N-ethylmaleimide-sensitive factor attachment protein receptor (SNARE) proteins to help to mediate fusion of synaptic vesicles. The light chains of BoNT cleave SNARE proteins, thereby preventing vesicle fusion of acetylcholine and inhibiting its release into the neuromuscular junction. BoNT-A and BoNT-E work by removing amino acids from a SNARE protein called synaptosomal-associated protein 25. BoNT B, D, F, and G work by cleaving vesicle-associated membrane protein/synaptobrevin, and BoNT-C cleaves syntaxin and synaptosomal-associated protein 25.19,20 Proposed mechanisms of axonal sprouting play a role in nerve regeneration and eventual repair of paralyzed endplates21 and may play a role in the wearing-off effect after ~3 months.
The potency of each preparation of BoNT is measured by mouse units, which is the dose that is lethal in 50% of mice tested.17 Although studies comparing dosage equivalencies between different toxin types have been published, the conversion ratios are not clear, and the FDA specifies that dose conversions should not be performed.
BoNT for upper limb spasticity
The goals of the current review are to highlight the use of BoNT in the treatment of upper and lower limb spasticity. The current review combines class I and II studies addressing the efficacy and safety of BoNT for the treatment of poststroke spasticity (Tables 1 and 2) by assigning levels of evidence according to the American Academy of Neurology guidelines. A broader search was used for the rest of the article. Studies were reviewed from the 2008 Report of Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology,22 and additional literature search was conducted using the PubMed, OvidSP, and Medline databases from January 2008 to October 2015 with the search items “post stroke spasticity,” “upper-limb post stroke spasticity,” “lower limb post stroke spasticity,” “botulinum toxin,” “botulinum neurotoxin,” “abobotulinumtoxinA,” “onabotulinumtoxinA,” “incobotulinumtoxinA,” and “rimabotulinumtoxinB.” Most studies utilized the Modified Ashworth Scale (MAS) as the primary outcome measure for spasticity reduction.
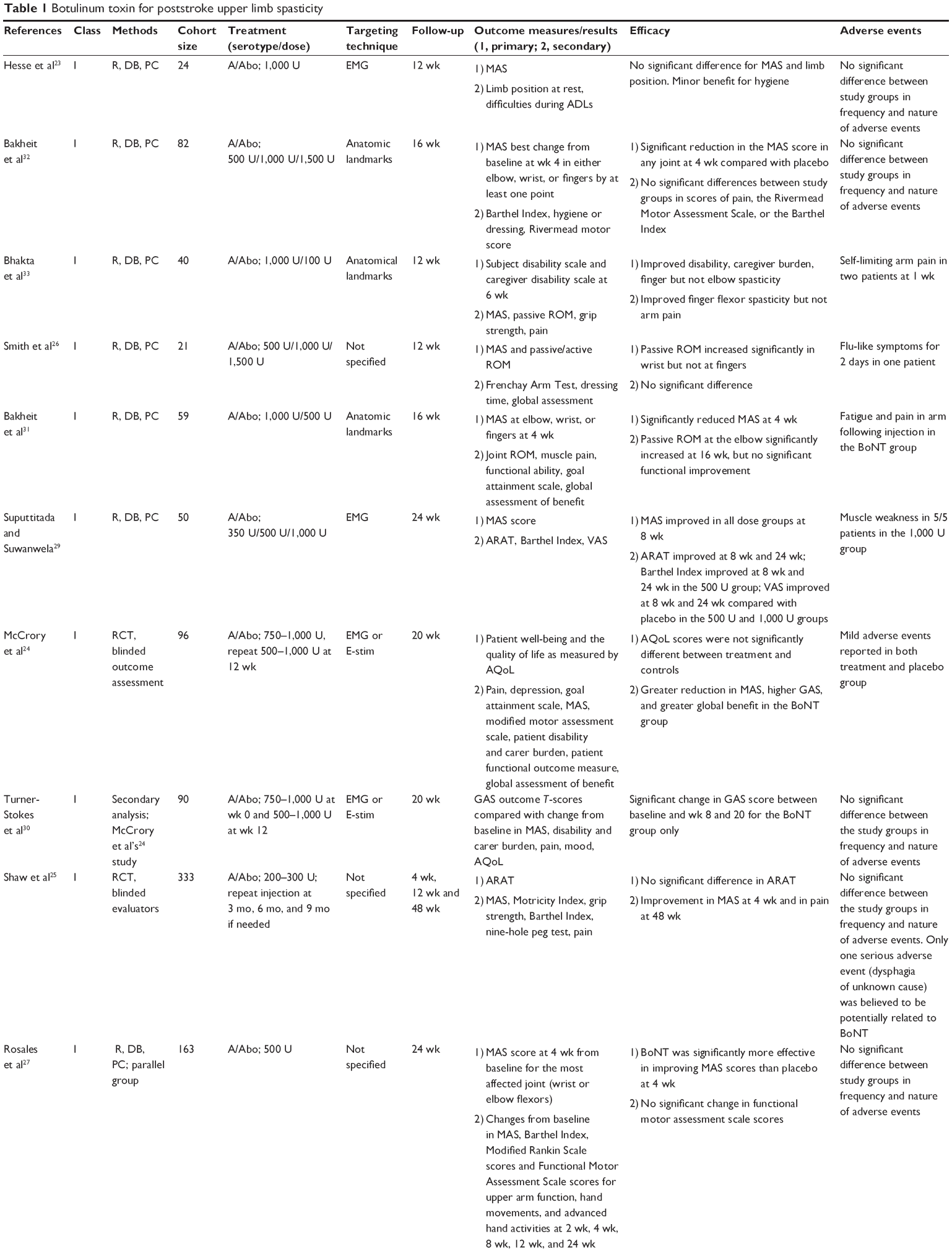  | Table 1 Botulinum toxin for poststroke upper limb spasticity |
 | Table 2 Botulinum toxin for poststroke lower limb spasticity |
AbobotulinumtoxinA
AbobotulinumtoxinA was approved by the FDA in 2015 for the treatment of upper limb poststroke spasticity. Eleven class I trials have found that abobotulinumtoxinA is effective and safe for the reduction in upper limb poststroke spasticity.23–33 Studies assessing both active and passive functional outcomes have demonstrated a significant improvement in passive function (improved range of motion, etc), while failing to show substantial improvement in active muscle function.24,25,27
A trial conducted at 34 neurology and rehabilitation clinics in the USA and in Europe randomized 243 patients to placebo, abobotulinumtoxinA (500 U), or abobotulinumtoxinA (1,000 U). The primary endpoint of mean change in muscle tone of hypertonic muscle groups of the upper limb was significant in both abobotulinumtoxinA groups vs placebo. The secondary endpoint of mean change in the Physician Global Assessment, clinician-rated clinical benefit independent of the MAS, was significantly different after 4 weeks, although the perceived function Disability Assessment Scale (DAS) was not significantly different.34
A study in Australia which assessed 96 patients comparing abobotulinumtoxinA (500–1,000 U) with placebo reported no significant difference in their primary outcome of QoL. However, there was a significant improvement in secondary outcomes including greater reduction in spasticity (P<0.001) and Goal Attainment Scale, pain, mood, global benefit, disability, and carer burden.24 Further analysis of these data suggested significantly higher levels of goal attainment in the treatment group and a cumulative effect over two cycles of treatment.30
Another study randomized 333 patients from 12 stroke services in the UK and found no significant difference in the primary outcome of improved arm function at 1 month, 3 months, or 12 months. Muscle tone and spasticity at the elbow were decreased at 1 month as a secondary outcome measure.25 A final study enrolled 163 patients and randomized them to abobotulinumtoxinA (500 U) vs placebo and found improved scores in the treatment group but failed to find a clinically significant difference in the Functional Motor Assessment Scale.27
Further studies that found improvement in spasticity and passive range of movement in spastic upper limbs have noted improvement in disability with caregiver assistance such as helping dressing and cleaning of the affected limb and decreased caregiver burden.26,31,33,35
OnabotulinumtoxinA
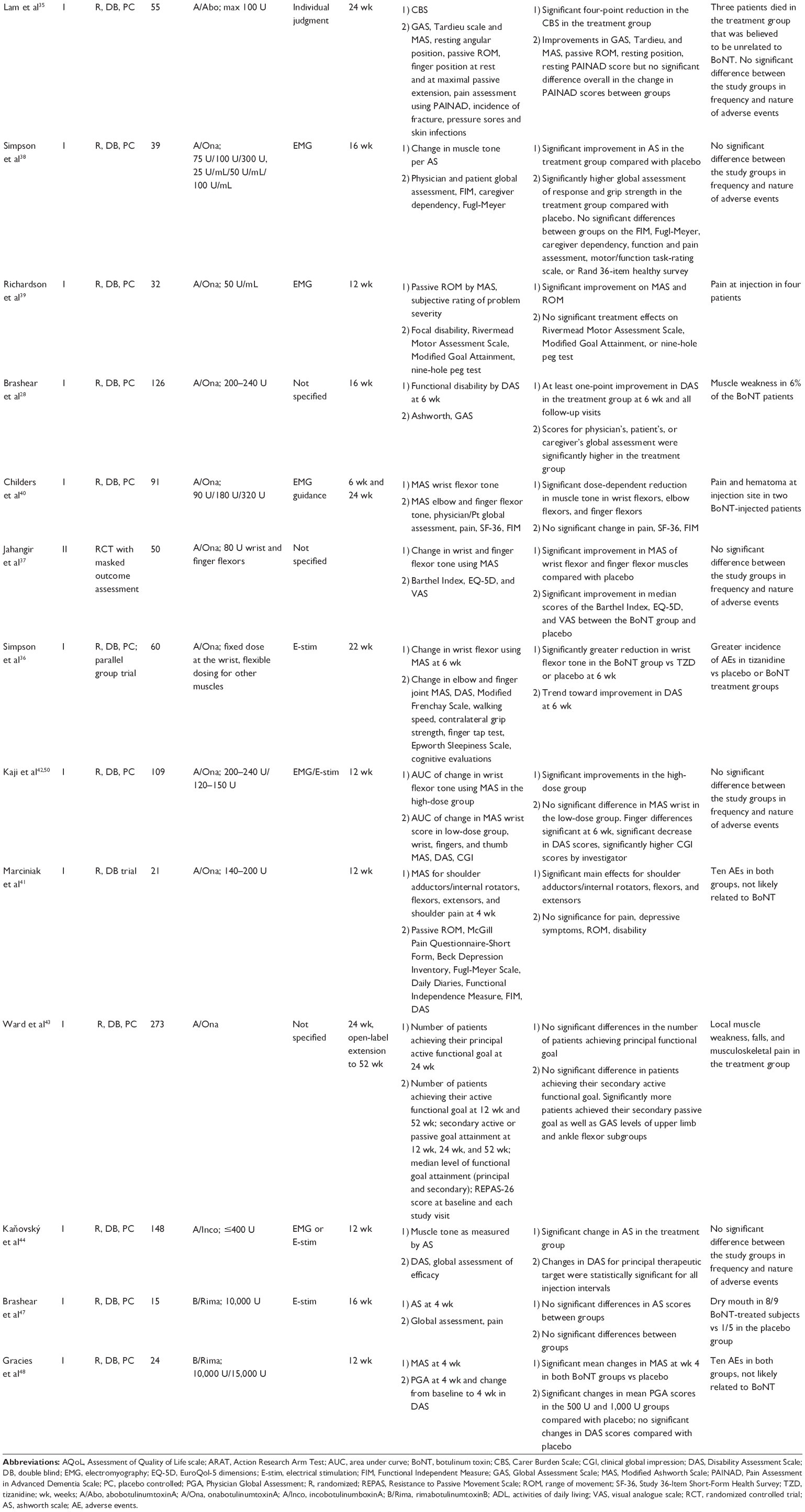
OnabotulinumtoxinA has been studied extensively and found to be safe, and to significantly reduce upper limb spasticity after stroke.28,36–40 Studies also used the MAS and found dose-dependent improvements with sustained benefits at 3 months; however, the reduction in pain measurements was not demonstrated.28,37,39–42 Although some studies have found improvements in functional disability on the DAS28 and the Global Assessment of Response to Treatment,38 others failed to demonstrate gains in functional activity.37,40,43 For example, a class II trial in Malaysia found improvement in flexor tone of the wrist and finger muscles at 1 month and 3 months. Although there were improvements in measures of global function and QoL in the onabotulinumtoxinA group, there were no significant differences between the onabotulinumtoxinA group and placebo.37 The Botox Economic Spasticity Trial randomized onabotulinumtoxinA plus standard of care to placebo plus standard of care and was assessed for passive and active functional goals (as defined by both the patient and the investigator) at 12 weeks followed by an open-label period of 52 weeks. Although more patients in the treatment group achieved their secondary passive goal, there was no difference between groups in the principal and secondary active functional goals.43
Three class I studies assessing the effects of onabotulinumtoxinA vs placebo have found improvements in spasticity but not in pain. The first study randomized 109 patients to receive a lower- (120–150 U) or higher-dose (200–240 U) onabotulinumtoxinA or placebo in spastic upper limbs after stroke and found significant improvements in spasticity with the higher-dose onabotulinumtoxinA. No significant differences were found with the lower-dose onabotulinumtoxinA and placebo. Secondary outcome measures of functional disability showed a significant decrease in the DAS score for limb position and dressing in the higher-dose onabotulinumtoxinA group, but not for hygiene and pain.42 The second study randomized 91 stroke patients to two treatments of placebo and 90 U, 180 U, or 360 U of onabotulinumtoxinA for upper limb spasticity. A dose-dependent response was observed in tone reduction but not in functional disability, pain, or QoL.40 The third study (only 21 patients) assessed the efficacy of onabotulinumtoxinA in reducing pain, impairment, and disability in patients with shoulder pain and spasticity. They found no significant differences in pain scores on the McGill Pain Questionnaire between those injected with BoNT and those injected with placebo (P>0.05), although they did find improvements in hygiene on the DAS (P<0.05) with a similar trend toward significance for improvement on the DAS dressing scale (P=0.061).41
There are few trials comparing BoNT serotypes. Our group reported differences between onabotulinumtoxinA and TZD. This class I study compared injections of onabotulinumtoxinA with TZD vs placebo in 60 patients with upper limb spasticity from either stroke or traumatic brain injury. Patients were randomized to intramuscular onabotulinumtoxinA plus oral placebo, oral TZD plus intramuscular placebo, and intramuscular placebo plus oral placebo. OnabotulinumtoxinA elicited greater reduction in tone than TZD or placebo in finger and wrist flexors at 3 weeks (P<0.001 vs TZD; P<0.02 vs placebo) and 6 weeks (P=0.001 vs TZD; P=0.08 vs placebo). Dressing, hygiene, cosmesis, and pain demonstrated a nonsignificant trend to a greater reduction in the primary therapeutic target 6 weeks after injection in the onabotulinumtoxinA group.36
IncobotulinumtoxinA
Two class I trials have demonstrated reduction in tone with incobotulinumtoxinA. The first study assessed incobotulinumtoxinA by randomizing 148 upper limb poststroke spasticity patients to 400 U of incobotulinumtoxinA vs placebo who were then followed for 20 weeks. At 4 weeks, there was a >1-point improvement in the Ashworth scale score in the finger flexor muscles compared with patients who received placebo (odds ratio 3.91, 95% confidence interval: 1.9–9.3).44 Subsequent open-label extension of the study continued to show benefit, with most investigators, patients, and caregivers rating positive benefit and efficacy throughout the open-label period of 69 weeks.45 The second study randomized 349 patients to incobotulinumtoxinA (400 U) or placebo at 46 international sites. There was a reduction in the Ashworth scale score in the primary target clinical pattern (-0.9 incobotulinumtoxinA vs -0.5 placebo; P<0.001) with >1-point improvement (69.6% incobotulinumtoxinA vs 37.5% placebo) when compared with placebo.46 Both studies demonstrated significant improvements in DAS scores from baseline across domains of dressing, limb position, hygiene, and pain.45,46
RimabotulinumtoxinB
Two smaller class I trials on rimabotulinumtoxinB (BoNT-B) have been completed. The first study randomized 15 patients to 10,000 U of rimabotulinumtoxinB or placebo in elbow, wrist, and fingers and found a significant decrease in wrist tone 2 weeks after injection, but it did not find a decrease in tone at the finger flexors or elbow at 10,000 U of rimabotulinumtoxinB over a 16-week period.47 The second trial randomized 24 patients with elbow flexor spasticity after stroke or traumatic brain injury to 10,000 U or 15,000 U of rimabotulinumtoxinB or placebo and followed for 3 months. Patients who had received either dose of rimabotulinumtoxinB had significantly improved active elbow extension compared with placebo.48
BoNT for lower limb spasticity
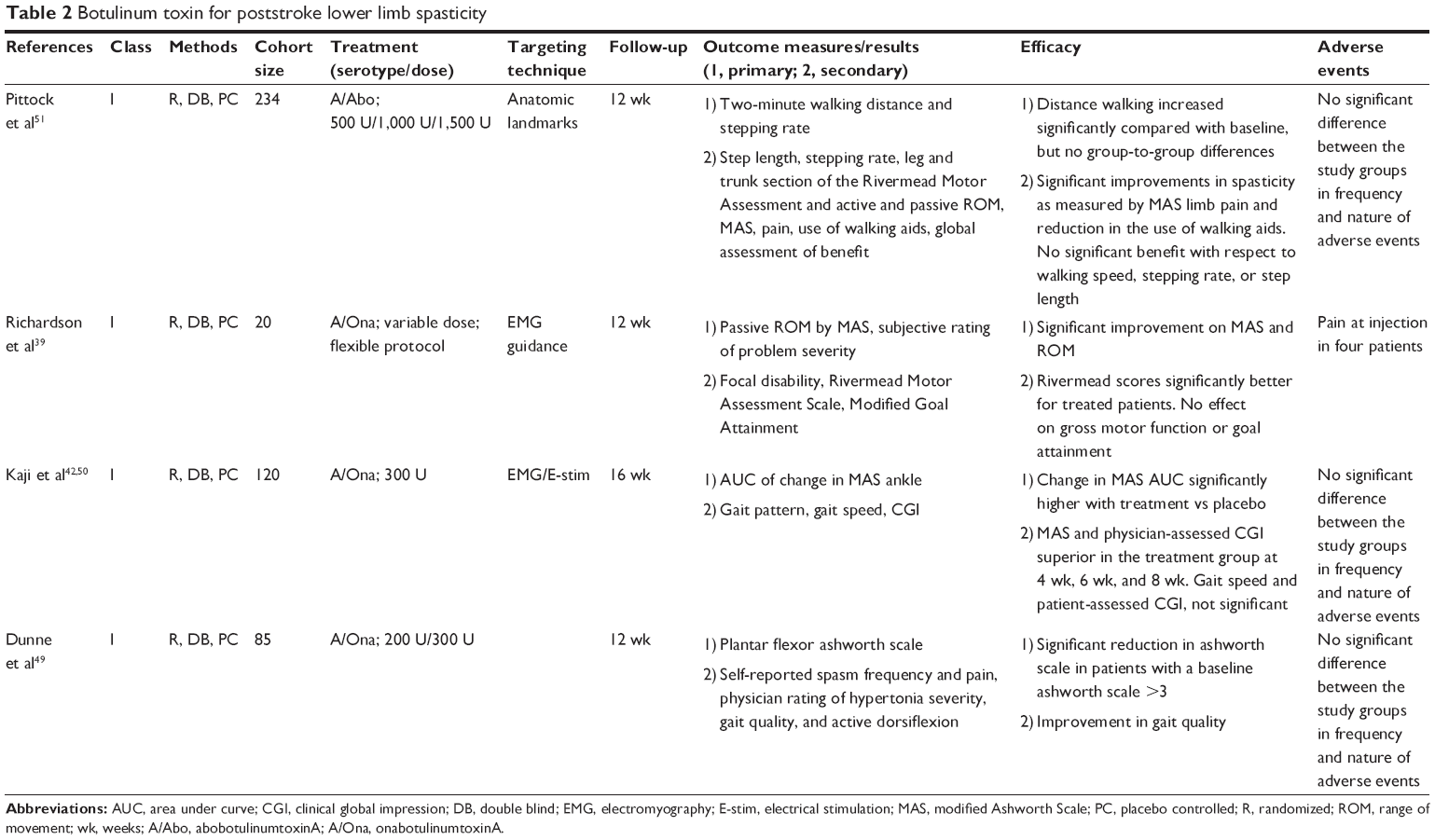
There are fewer studies assessing the effects of BoNT in the treatment of lower limb poststroke spasticity compared with upper limb poststroke spasticity (Table 2). Most class I studies have assessed the efficacy and safety of abobotulinumtoxinA and onabotulinumtoxinA.
There are three class I studies of onabotulinumtoxinA which have established significant reduction in muscle tone in poststroke lower limb spasticity. In the first study, 85 subjects received 200 U or 300 U of onabotulinumtoxinA or saline injections with the primary measure being plantar flexor Ashworth scores at 12 weeks. Subjects noted significantly greater decrease in spasm frequency (P=0.01), pain reduction (P=0.02), active dorsiflexion (P=0.03), and gait quality (P=0.02).49 In the second study, Kaji et al randomized 120 patients with lower limb spasticity to BoNT-A (300 U) or placebo. Although a significant improvement in spasticity was seen, no change in the speed of gait was found between groups.50 In the third study, Richardson et al assessed onabotulinumtoxinA vs placebo with assessments at 3-week intervals after injection until 12 weeks in patients with either upper or lower limb spasticity from a variety of injuries including stroke. Among 52 people, 20 of which had lower limb spasticity; onabotulinumtoxinA had an effect on focal disability and impairment in lower limbs.39
There is one class I study of abobotulinumtoxinA. In this study, the effects of three doses of abobotulinumtoxinA at 500 U, 1,000 U or 1,500 U in 234 stroke patients were assessed. The primary outcome measure of 2-minute walking distance and stepping rate increased significantly in both groups, but no significant difference was found between groups including placebo. Significant improvements in calf spasticity, limb pain, and reduction in the reuse of walking aids were found with abobotulinumtoxinA compared with placebo, with the greatest benefits found in patients receiving 1,500 U.51
Technical considerations
Optimal dosing and time of administration
Minor differences exist between storing and preparing the various BoNT serotypes, and care should be taken to read the package insert to ensure optimal preparation. For example, onabotulinumtoxinA and abobotulinumtoxinA are both available as powders for reconstitution which must be refrigerated at 2°C–8°C, whereas incobotulinumtoxinA does not need to be refrigerated. RimabotulinumtoxinB does not require reconstitution and is stable for 21 months in refrigerator storage.
Better outcomes may be obtained if BoNT is injected after a shorter duration of onset to spasticity.52,53 This may be attributed to the fact that contractures begin to develop as early as 2 weeks after stroke.2 There are currently no well-defined guidelines regarding optimal BoNT dosing, although several strategies have been implemented. The European Consensus data on BoNT-A for adult spasticity recommend 600 U of onabotulinumtoxinA and incobotulinumtoxinA and up to 1,500 U of abobotulinumtoxinA per injection session.54 More recent literature suggests using higher doses for poststroke spasticity. Baricich et al recently recommended dosing of up to 600–800 U of onabotulinumtoxinA in upper and lower poststroke spasticity.55 A recent review article of eight selected studies suggests that higher doses of BoNT-A are efficacious in reducing upper and lower limb poststroke spasticity, with mild adverse effects.56
Another study aimed at characterizing the dose–response relationships between muscle tone and onabotulinumtoxinA tone pooled data from seven trials. A total of 544 patients were randomized to receive onabotulinumtoxinA or placebo. Dose–response relationships demonstrated greater improvements in muscle tone with increasing doses of onabotulinumtoxinA. Doses estimated to cause a decreased muscle tone were 22.5 U, 18.4 U, 66.3 U, and 42.5 U in the flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, and flexor digitorum profundus, respectively, and not determinable in the biceps brachii.57
Injection patterns and optimal targeting
The most frequently injected upper and lower limb muscles were reported in a meta-analysis of 70 randomized, nonrandomized, and single-arm studies evaluating onabotulinumtoxinA muscle injection patterns in 2,163 adult spasticity patients. The upper limbs included the flexor carpi radialis (64.0%), flexor carpi ulnaris (59.1%), flexor digitorum superficialis (57.2%), flexor digitorum profundus (52.5%), and biceps brachii (38.8%). The most commonly injected lower limb muscles included the gastrocnemius (66.1%), soleus (54.7%), and tibialis posterior (50.5%).58 A modified Delphi panel of ten clinical experts identified a treatment paradigm for muscle selection, dose for each muscle and for each posture, and use of localization techniques for injecting onabotulinumtoxinA in poststroke upper limb spasticity. The authors identified three common aggregating upper limb postures in poststroke spasticity including 1) adducted shoulder, flexed elbow, pronated forearm, flexed wrist, and clenched fist; 2) flexed elbow, pronated forearm, flexed wrist, and clenched fist; and 3) flexed wrist and clenched fist. They recommended a dilution of onabotulinumtoxinA of 50 U/mL (2:1 dilution ratio) and starting doses for each aggregate were 300 U, 300 U, and 200 U with total maximum doses of 400 U, 400 U, and 300 U, respectively. They also concluded that localization techniques were needed to identify muscles.59
Practitioners commonly used landmark localization, electrical stimulation, electromyography guidance, and ultrasound to identify targeted muscles for injection. The knowledge of high-density endplate areas can maximize yield when using anatomic landmarks for injection. Although some muscles have well-defined motor endplates, other muscles may require a more even spread of injection across the muscle54 or higher dilutions.60 Optimal targeting based on anatomic knowledge of highest endplate density may yield the highest results. Amirali et al histologically mapped endplate bands in relation to external landmarks in human biceps brachii muscles. The study found that the area of highest endplate density is an inverted V-shaped band 1 cm in width between the lower third and upper two-thirds of the muscle belly.61 In an attempt to determine the effects of onabotulinumtoxinA dilution and endplate targeting in elbow flexors, Gracies et al randomized 21 patients in four groups, 4 months after a 160 U injection of BoNT-A into spastic biceps brachii muscles. These four groups included 1) 100 U/mL dilution, 0.4 cc/site, four-quadrant injection; 2) 100 U/mL dilution, 0.4 cc/site, four sites along endplate band; and 3) 20 U/mL dilution, 2 cc/site, four-quadrant injection. They found that a high-volume dilution (20 U/mL) and an endplate-targeted injection are superior to a low-volume, endplate nontargeted injection, when injecting biceps brachii.60
Although anatomic knowledge of surface landmarks and endplate densities may be important while injecting, electrical stimulation and ultrasound have been shown to be important tools for ensuring accurate injection into the targeted muscles. One study found that only 37% of needle placement attempts reached target muscle fascicles, suggesting that further guidance tools may be needed for correct localization, particularly for small or deep muscles.62 Picelli et al randomized 60 poststroke spasticity patients to manual needle placement, electrical stimulation, and ultrasound techniques using abobotulinumtoxinA. They found that patients injected using electrical stimulation and ultrasound guidance had improved MAS scores, Tardieu angle, and passive range of motion when compared with the manual needle placement group. They found no differences between the ultrasound and electrical stimulation groups.63
Two additional studies have found the benefit of ultrasound over surface landmark techniques and manual needle placement. One study compared surface landmark technique with ultrasound guidance when injecting spastic muscles of the upper extremity with abobotulinumtoxinA and found significant differences between methods, concluding that ultrasound guidance can help avoid injection into nerve and vascular structures and ensure the injection remains within the fascicle borders.64 Another randomized study compared ultrasound guidance with surface landmark techniques by measuring MAS and finger position in poststroke patients with upper limb spasticity treated with incobotulinumtoxinA. After 1 month of follow-up, MAS and finger position at rest were significantly improved in both groups, although they were significantly better in patients treated with ultrasound guidance than those with manual needle placement.65
Adverse events associated with BoNT
Adverse short-term issues related to BoNT include local pain at the site of injection and spread, or the diffusion of toxin from the injected muscle into neighboring muscles causing undesirable weakness. Depending on the location, spread can be dangerous and adverse events that have been reported include dysphagia, dysarthria, dysphonia, respiratory compromise, and rarely death.66 A solid knowledge of the muscle anatomy can help decrease this risk. The long-term effects include anatomic denervation and muscle atrophy, as well as immunoresistance. However, more recent studies demonstrate that a relatively small group of patients actually develop immunoresistance. One study measured 207 patients’ posttreatment serum samples for neutralizing antibodies who received onabotulinumtoxinA with poststroke spasticity and found that one patient who had received four treatments tested positive to neutralizing antibodies after the first injection and did not respond to treatment.67 A meta-analysis assessing rates of neutralizing antibody conversion with onabotulinumtoxinA found that only one subject out of 317 (0.32%) of poststroke spasticity subjects converted from a baseline status of antibody negative to antibody positive after treatment.68 Given the relatively low rate of antibody formation, authors suggest considering other factors when faced with a patient with nonresponsiveness such as technical issues. Several ways of minimizing these effects include increasing doses of BoNT69 and switching serotypes of BoNT.70 IncobotulinumtoxinA theoretically may have less immunoresistance given that it is free of complexing proteins, although no study has confirmed this.
Satisfaction
No significant differences were found in caregiver dependency in a small study of 39 patients randomized to onabotulinumtoxinA vs placebo. Two recent cross-sectional surveys conducted in the USA, Canada, France, and Germany of 79 patients found that 40.5% of patients were very satisfied, 48.1% were somewhat satisfied, and 11.4% were not satisfied with at least two treatment sessions of any of the BoNT-A formulations. Interestingly, patient satisfaction was the lowest right before injection and the highest at the time-of-peak effect. Most of the participating physicians were moderately (57.7%) or very (36.5%) satisfied with the BoNT-A treatment.71 AbobotulinumtoxinA decreases caregiver burden in the long-term care patients who are treated for upper limb spasticity. In this study, 55 patients randomized to abobotulinumtoxinA vs placebo noted a four-point reduction in carer burden (P<0.001) when treated with abobotulinumtoxinA.35 Another study randomized 40 patients with poststroke spasticity to receive abobotulinumtoxinA vs placebo and found a reduction in carer burden at week 6 after injection with abobotulinumtoxinA. This benefit was extended for at least 12 weeks.33
Cost analysis
The cost of BoNT may be prohibitive to patients without insurance coverage, and even for those with insurance coverage that cannot get approval for treatments such as booster injections within 3 months. The BoNT for Upper Limb after Stroke trial assessed the cost-effectiveness of BoNT-A plus an upper limb therapy program in the treatment of poststroke upper limb spasticity in England and Wales. They found that the addition of BoNT-A was not estimated to be cost-effective and in fact two-and-a-half times the cost-effectiveness threshold as set by the National Institute for Health and Clinical Excellence.72 Another study evaluated the cost per patient per injection of two types of BoNT-A, onabotulinumtoxinA (100 U) and abobotulinumtoxinA (500 U), using the recommended dosing of 300 U and 1,000 U for upper limb spasticity, respectively. The cost per patient per injection for upper limb spasticity was less for abobotulinumtoxinA than for onabotulinumtoxinA in 18 of the 19 countries assessed, while allowing for different prices per vial in each country. Ultimately, the authors suggested that substantial savings could be made by using abobotulinumtoxinA in the treatment of upper limb spasticity.73
Conclusion
Poststroke spasticity can be a major source of morbidity and has an impact on activities of daily living, hygiene, caregiver burden, and QoL. The mainstays of conventional treatment include a multifaceted approach that may include incorporating a structured rehabilitation program and/or multidisciplinary team approach, although more data are needed in this area. Based on current class I and II studies, we suggest that BoNT is used as part of a dynamic approach to treating poststroke spasticity. The current data on BoNT demonstrate that it effectively decreases muscle tone in poststroke spasticity of the upper and lower limbs. However, studies assessing both improvements in active function as well as pain reduction have not had as robust a response.
The lack of strong active functional outcomes when compared with passive functional outcomes may reflect the need for more sensitive assessment scales that assess more than just muscle tone. Most studies currently utilize the MAS, while more flexible and patient-centered approaches may be considered, including the Goal Attainment Scale that allows for the use of individualized functional treatment goals.74 Investigators from the BoNT for Upper Limb after Stroke trial who demonstrated reduction in spasticity but not in active function of the upper limb suggest that weakness is more important than spasticity in reduced upper limb function.25 The cumulative data on pain reduction are mixed in poststroke spasticity, but interestingly there have been some data suggesting a role for BoNT in the reduction of pain including diabetic neuropathic pain,75,76 occipital neuralgia,77 trigeminal neuralgia,78 and complex region pain syndrome.79
Strategies to reduce adverse effects on BoNT injections include having a solid knowledge of anatomy of muscles to be injected before injection, using additional methods such as electromyography, electrical stimulation, or ultrasound guidance. It is important to identify and exclude populations who may have hypersensitivity to BoNT including neuromuscular junction disorders and anterior horn cell disorders prior to injection. In addition, as botulinum serotypes can differ, reading the packaging label before use and being familiar with proper storage techniques, planning out dosing, and knowing reconstitution techniques may be prudent.66
Thus far, there have been only few comparator trials comparing different BoNT formulations, and one study comparing BoNT with an oral therapy, TZD.36 Future head-to-head trials are needed to determine the efficacy of one BoNT serotype and formulation when compared with another in addition to BoNT in comparison with other treatments. Determining which muscles to inject should be tailored to each patient individually. Further research is needed to identify standard muscles in the upper and lower extremity, and further recommendations are needed to identify the number and location of injection sites. As the usage of the other formulations continues to grow, we expect to acquire more information on safety, dosing, efficacy, and potential uses for particular muscles in upper and lower limb spasticity. Given the differences in formulation, mechanism of action, dosing and potential adverse effect profile, we recommend that future studies address formulations individually.
Disclosure
Dr David M Simpson receives consulting fees and research grant support from Allergan, Inc., Merz, and Ipsen. Dr Michelle Kaku reports no conflicts of interest in this work.
References
Lance JW. The control of muscle tone, reflexes, and movement: Robert Wartenberg lecture. Neurology. 1981;30(12):1303–1313. | ||
Allison R, Shenton L, Bamforth K, Kilbride C, Richards D. Incidence, time course and predictors of impairments relating to caring for the profoundly affected arm after stroke: a systematic review. Physiother Res Int. Epub 2015 May 25. | ||
Urban PP, Wolf T, Uebele M, et al. Occurrence and clinical predictors of spasticity after ischemic stroke. Stroke. 2010;41:2016–2020. | ||
Brainin M, Norrving B, Sunnerhagen KS, et al. Poststroke chronic disease management: towards improved identification and interventions for poststroke spasticity-related complications. Int J Stroke. 2011;6:42–46. | ||
Chou R, Peterson K, Helfand M. Comparative efficacy and safety of skeletal muscle relaxants for spasticity and musculoskeletal conditions: a systematic review. J Pain Symptom Manage. 2004;28:140–175. | ||
Stevenson V. Rehabilitation in practice: spasticity management. Clin Rehabil. 2010;24:293–304. | ||
Francisco GE, Boake C. Improvement in walking speed in poststroke spastic hemiplegia after intrathecal baclofen therapy: a preliminary study. Arch Phys Med Rehabil. 2003;84:1194–1199. | ||
Meythaler JM, Guin-Renfroe S, Brunner RC, Hadley MN. Intrathecal baclofen for spastic hypertonia from stroke. Stroke. 2001;32:2099–2109. | ||
Esquenazi A, Novak I, Sheean G, Singer B, Ward A. International consensus statement for the use of botulinum toxin treatment in adults and children with neurological impairments–introduction. Eur J Neurol. 2010;17:1–8. | ||
Demetrios M, Gorelik A, Louie J, Brand C, Baguley IJ, Khan F. Outcomes of ambulatory rehabilitation programmes following botulinum toxin for spasticity in adults with stroke. J Rehabil Med. 2014;46:730–737. | ||
Franceschini M, Iocco M, Molteni F, Santamato A, Smania N. Management of stroke patients submitted to botulinum toxin type A therapy: a Delphi survey of an Italian expert panel of specialist injectors. Eur J Phys Rehabil Med. 2014;50:525–532. | ||
Erbguth FJ, Naumann M. Historical aspects of botulinum toxin Justinus Kerner (1786–1862) and the “sausage poison”. Neurology. 1999;53:1850–1850. | ||
Gimenez DF, Giménez JA. Serological Subtypes of Botulinal Neurotoxins. Botulinum and Tetanus Neurotoxins. New York: Springer; 1993:421–431. | ||
Simpson LL. The origin, structure, and pharmacological activity of botulinum toxin. Pharmacol Rev. 1981;33:155–188. | ||
Simpson LL. Identification of the major steps in botulinum toxin action. Annu Rev Pharmacol Toxicol. 2004;44:167–193. | ||
Aoki K, Guyer B. Botulinum toxin type A and other botulinum toxin serotypes: a comparative review of biochemical and pharmacological actions. Eur J Neurol. 2001;8:21–29. | ||
Frevert J. Content of botulinum neurotoxin in botox®/vistabel®, dysport®/azzalure®, and xeomin®/bocouture®. Drugs R D. 2010;10:67–73. | ||
Gupta BRD, Sugiyama H. Role of a protease in natural activation of Clostridium botulinum neurotoxin. Infect Immun. 1972;6:587–590. | ||
Blasi J, Chapman ER, Link E, et al. Botulinum neurotoxin A selectively cleaves the synaptic protein SNAP-25. Nature. 1993;365:160–163. | ||
Schiavo GG, Benfenati F, Poulain B, et al. Tetanus and botulinum-B neurotoxins block neurotransmitter release by proteolytic cleavage of synaptobrevin. Nature. 1992;359:832–835. | ||
de Paiva A, Meunier FA, Molgó J, Aoki KR, Dolly JO. Functional repair of motor endplates after botulinum neurotoxin type A poisoning: biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc Natl Acad Sci U S A. 1999;96:3200–3205. | ||
Simpson D, Gracies J, Graham H, et al. Assessment: botulinum neurotoxin for the treatment of spasticity (an evidence-based review) Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2008;70:1691–1698. | ||
Hesse S, Reiter F, Konrad M, Jahnke MT. Botulinum toxin type A and short-term electrical stimulation in the treatment of upper limb flexor spasticity after stroke: a randomized, double-blind, placebo-controlled trial. Clin Rehabil. 1998;12:381–388. | ||
McCrory P, Turner-Stokes L, Baguley IJ, et al. Botulinum toxin A for treatment of upper limb spasticity following stroke: a multi-centre randomized placebo-controlled study of the effects on quality of life and other person-centred outcomes. J Rehabil Med. 2009;41:536–544. | ||
Shaw LC, Price CI, van Wijck FM, et al. Botulinum toxin for the upper limb after stroke (BoTULS) trial effect on impairment, activity limitation, and pain. Stroke. 2011;42:1371–1379. | ||
Smith S, Ellis E, White S, Moore A. A double-blind placebo-controlled study of botulinum toxin in upper limb spasticity after stroke or head injury. Clin Rehabil. 2000;14:5–13. | ||
Rosales RL, Kong KH, Goh KJ, et al. Botulinum toxin injection for hypertonicity of the upper extremity within 12 weeks after stroke a randomized controlled trial. Neurorehabil Neural Repair. 2012;26:812–821. | ||
Brashear A, Gordon MF, Elovic E, et al. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N Engl J Med. 2002;347:395–400. | ||
Suputtitada A, Suwanwela N. The lowest effective dose of botulinum A toxin in adult patients with upper limb spasticity. Disabil Rehabil. 2005;27:176–184. | ||
Turner-Stokes L, Baguley IJ, De Graaff S, et al. Goal attainment scaling in the evaluation of treatment of upper limb spasticity with botulinum toxin: a secondary analysis from a double-blind placebo-controlled randomized clinical trial. J Rehabil Med. 2010;42:81–89. | ||
Bakheit A, Pittock S, Moore A, et al. A randomized, double-blind, placebo-controlled study of the efficacy and safety of botulinum toxin type A in upper limb spasticity in patients with stroke. Eur J Neurol. 2001;8:559–565. | ||
Bakheit A, Thilmann A, Ward A, et al. A randomized, double-blind, placebo-controlled, dose-ranging study to compare the efficacy and safety of three doses of botulinum toxin type A (Dysport) with placebo in upper limb spasticity after stroke. Stroke. 2000;31:2402–2406. | ||
Bhakta BB, Cozens JA, Chamberlain MA, Bamford JM. Impact of botulinum toxin type A on disability and carer burden due to arm spasticity after stroke: a randomised double blind placebo controlled trial. J Neurol Neurosurg Psychiatry. 2000;69:217–221. | ||
Gracies J-M, Brashear A, Jech R, et al. Safety and efficacy of abobotulinumtoxinA for hemiparesis in adults with upper limb spasticity after stroke or traumatic brain injury: a double-blind randomised controlled trial. Lancet Neurol. 2015;14:992–1001. | ||
Lam K, Lau KK, So KK, et al. Can botulinum toxin decrease carer burden in long term care residents with upper limb spasticity? A randomized controlled study. J Am Med Dir Assoc. 2012;13:477–484. | ||
Simpson DM, Gracies J-M, Yablon SA, Barbano R, Brashear A. Botulinum neurotoxin versus tizanidine in upper limb spasticity: a placebo-controlled study. J Neurol Neurosurg Psychiatry. 2009;80:380–385. | ||
Jahangir A, Tan H, Norlinah M, et al. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after stroke. Med J Malaysia. 2007;62:319. | ||
Simpson D, Alexander D, O’brien C, et al. Botulinum toxin type A in the treatment of upper extremity spasticity A randomized, double-blind, placebo-controlled trial. Neurology. 1996;46:1306–1306. | ||
Richardson D, Sheean G, Werring D, et al. Evaluating the role of botulinum toxin in the management of focal hypertonia in adults. J Neurol Neurosurg Psychiatry. 2000;69:499–506. | ||
Childers MK, Brashear A, Jozefczyk P, et al. Dose-dependent response to intramuscular botulinum toxin type A for upper-limb spasticity in patients after a stroke. Arch Phys Med Rehabil. 2004;85:1063–1069. | ||
Marciniak CM, Harvey RL, Gagnon CM, et al. Does botulinum toxin type A decrease pain and lessen disability in hemiplegic survivors of stroke with shoulder pain and spasticity?: a randomized, double-blind, placebo-controlled trial. Am J Phys Med Rehabil. 2012;91:1007–1019. | ||
Kaji R, Osako Y, Suyama K, Maeda T, Uechi Y, Iwasaki M. Botulinum toxin type A in post-stroke upper limb spasticity. Curr Med Res Opin. 2010;26:1983–1992. | ||
Ward AB, Wissel J, Borg J, et al. Functional goal achievement in post-stroke spasticity patients: the BOTOX® economic spasticity trial (BEST). J Rehabil Med. 2014;46:504–513. | ||
Kanovský P, Slawek J, Denes Z, et al. Efficacy and safety of botulinum neurotoxin NT 201 in poststroke upper limb spasticity. Clin Neuropharmacol. 2009;32:259–265. | ||
Kaňovský P, Slawek J, Denes Z, et al. Efficacy and safety of treatment with incobotulinum toxin A (botulinum neurotoxin type A free from complexing proteins; NT 201) in post-stroke upper limb spasticity. J Rehabil Med. 2011;43:486–492. | ||
Elovic EP, Munin MC, Kaňovský P, Hanschmann A, Hiersemenzel R, Marciniak C. Randomized, placebo-controlled trial of incobotulinumtoxinA for upper-limb post-stroke spasticity. Muscle Nerve. Epub 2015 Jul 22. | ||
Brashear A, McAfee AL, Kuhn ER, Fyffe J. Botulinum toxin type B in upper-limb poststroke spasticity: a double-blind, placebo-controlled trial. Arch Phys Med Rehabil. 2004;85:705–709. | ||
Gracies J-M, Bayle N, Goldberg S, Simpson DM. Botulinum toxin type B in the spastic arm: a randomized, double-blind, placebo-controlled, preliminary study. Arch Phys Med Rehabil. 2014;95:1303–1311. | ||
Dunne JW, Gracies J-M, Hayes M, Zeman B, Singer BJ, Group MS. A prospective, multicentre, randomized, double-blind, placebo-controlled trial of onabotulinumtoxinA to treat plantarflexor/invertor overactivity after stroke. Clin Rehabil. 2012;26:787–797. | ||
Kaji R, Osako Y, Suyama K, Maeda T, Uechi Y, Iwasaki M. Botulinum toxin type A in post-stroke lower limb spasticity: a multicenter, double-blind, placebo-controlled trial. J Neurol. 2010;257:1330–1337. | ||
Pittock S, Moore A, Hardiman O, et al. A double-blind randomised placebo-controlled evaluation of three doses of botulinum toxin type A (Dysport®) in the treatment of spastic equinovarus deformity after stroke. Cerebrovasc Dis. 2003;15:289–300. | ||
Mohammadi B, Abdoulrahmani Balouch S, Dengler R, Kollewe K. Long-term treatment of spasticity with botulinum toxin type A: an analysis of 1221 treatments in 137 patients. Neurol Res. 2010;32:309–313. | ||
Burbaud P, Wiart L, Dubos J, et al. A randomised, double blind, placebo controlled trial of botulinum toxin in the treatment of spastic foot in hemiparetic patients. J Neurol Neurosurg Psychiatry. 1996;61:265–269. | ||
Wissel J, Ward AB, Erztgaard P, et al. European consensus table on the use of botulinum toxin type A in adult spasticity. J Rehabil Med. 2009;41:13–25. | ||
Baricich A, Grana E, Carda S, Santamato A, Cisari C, Invernizzi M. High doses of onabotulinumtoxinA in post-stroke spasticity: a retrospective analysis. J Neural Transm (Vienna). 2015;122(9):1283–1287. | ||
Santamato A, Micello MF, Ranieri M, et al. Employment of higher doses of botulinum toxin type A to reduce spasticity after stroke. J Neurol Sci. 2015;350:1–6. | ||
Yablon SA, Brin MF, VanDenburgh AM, et al. Dose response with onabotulinumtoxinA for post-stroke spasticity: a pooled data analysis. Mov Disord. 2011;26:209–215. | ||
Nalysnyk L, Papapetropoulos S, Rotella P, Simeone JC, Alter KE, Esquenazi A. OnabotulinumtoxinA muscle injection patterns in adult spasticity: a systematic literature review. BMC Neurol. 2013;13:118. | ||
Simpson D, Patel A, Alfaro A, et al. Using a Delphi panel to identify a treatment paradigm for injecting botulinum toxin to treat common postures in post-stroke upper limb spasticity (P5. 167). Neurology. 2015;84(P5):167. | ||
Gracies J-M, Lugassy M, Weisz DJ, Vecchio M, Flanagan S, Simpson DM. Botulinum toxin dilution and endplate targeting in spasticity: a double-blind controlled study. Arch Phys Med Rehabil. 2009;90:9.e–16.e. | ||
Amirali A, Mu L, Gracies J-M, Simpson DM. Anatomical localization of motor endplate bands in the human biceps brachii. J Clin Neuromuscul Dis. 2007;9:306–312. | ||
Molloy F, Shill H, Kaelin-Lang A, Karp B. Accuracy of muscle localization without EMG: implications for treatment of limb dystonia. Neurology. 2002;58:805–807. | ||
Picelli A, Lobba D, Midiri A, et al. Botulinum toxin injection into the forearm muscles for wrist and fingers spastic overactivity in adults with chronic stroke: a randomized controlled trial comparing three injection techniques. Clin Rehabil. 2014;28:232–242. | ||
Henzel MK, Munin MC, Niyonkuru C, Skidmore ER, Weber DJ, Zafonte RD. Comparison of surface and ultrasound localization to identify forearm flexor muscles for botulinum toxin injections. PM R. 2010;2:642–646. | ||
Santamato A, Micello MF, Panza F, et al. Can botulinum toxin type A injection technique influence the clinical outcome of patients with post-stroke upper limb spasticity? A randomized controlled trial comparing manual needle placement and ultrasound-guided injection techniques. J Neurol Sci. 2014;347:39–43. | ||
Yiannakopoulou E. Serious and long-term adverse events associated with the therapeutic and cosmetic use of botulinum toxin. Pharmacology. 2015;95:65–69. | ||
Gordon M, Brashear A, Elovic E, et al. Repeated dosing of botulinum toxin type A for upper limb spasticity following stroke. Neurology. 2004;63:1971–1973. | ||
Naumann M, Carruthers A, Carruthers J, et al. Meta-analysis of neutralizing antibody conversion with onabotulinumtoxinA (BOTOX®) across multiple indications. Mov Disord. 2010;25:2211–2218. | ||
Dressler D, Münchau A, Bhatia KP, Quinn NP, Bigalke H. Antibody-induced botulinum toxin therapy failure: can it be overcome by increased botulinum toxin doses? Eur Neurol. 2001;47:118–121. | ||
Barnes M, Best D, Kidd L, et al. The use of botulinum toxin type-B in the treatment of patients who have become unresponsive to botulinum toxin type-A-initial experiences. Eur J Neurol. 2005;12:947–955. | ||
Bensmail D, Hanschmann A, Wissel J. Satisfaction with botulinum toxin treatment in post-stroke spasticity: results from two cross-sectional surveys (patients and physicians). J Med Econ. 2014;17:618–625. | ||
Shaw L, Rodgers H, Price C, et al. BoTULS: a multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A. Health Technol Assess. 2010;14(26):1–113, iii–iv. | ||
Roze S, Kurth H, Hunt B, Valentine W, Marty R. Evaluation of the cost per patient per injection of botulinum toxin A in upper limb spasticity: comparison of two preparations in 19 countries. Med Devices (Auckl). 2012;5:97. | ||
Rosales RL, Kanovsky P, Fernandez HH. What’s the “catch” in upper-limb post-stroke spasticity: expanding the role of botulinum toxin applications. Parkinsonism Relat Disord. 2011;17:S3–S10. | ||
Ghasemi M, Ansari M, Basiri K, Shaigannejad V. The effects of intradermal botulinum toxin type a injections on pain symptoms of patients with diabetic neuropathy. J Res Med Sci. 2014;19:106. | ||
Yuan R, Sheu J, Yu J, et al. Botulinum toxin for diabetic neuropathic pain A randomized double-blind crossover trial. Neurology. 2009;72:1473–1478. | ||
Taylor M, Silva S, Cottrell C. Botulinum toxin type-A (BOTOX®) in the treatment of occipital neuralgia: a pilot study. Headache. 2008;48:1476–1481. | ||
Wu C-J, Lian Y-J, Zheng Y-K, et al. Botulinum toxin type A for the treatment of trigeminal neuralgia: results from a randomized, double-blind, placebo-controlled trial. Cephalalgia. 2012;32:443–450. | ||
Carroll I, Clark JD, Mackey S. Sympathetic block with botulinum toxin to treat complex regional pain syndrome. Ann Neurol. 2009;65:348–351. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.