Back to Journals » Vascular Health and Risk Management » Volume 18
Spontaneous Simultaneous Bilateral Basal Ganglia Hemorrhage (SSBBGH): Systematic Review and Data Analysis on Epidemiology, Clinical Feature, Location of Bleeding, Etiology, Therapeutic Intervention and Outcome
Authors Alhashim A, Hadhiah K ![]() , Al-Dandan H, Aljaman M, Alabdali M, Alshurem M
, Al-Dandan H, Aljaman M, Alabdali M, Alshurem M ![]() , Aljaafari D, AlQarni M
, Aljaafari D, AlQarni M
Received 17 November 2021
Accepted for publication 6 April 2022
Published 14 April 2022 Volume 2022:18 Pages 267—276
DOI https://doi.org/10.2147/VHRM.S349912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Ali Alhashim, Kawther Hadhiah, Hassan Al-Dandan, Mugbil Aljaman, Majed Alabdali, Mohammed Alshurem, Danah Aljaafari, Mustafa AlQarni
Neurology Department, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, 34212, Saudi Arabia
Correspondence: Ali Alhashim, Neurology Department, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, 34212, Saudi Arabia, Tel +966509444833, Email [email protected]
Background: Spontaneous simultaneous bilateral basal ganglia hemorrhage (SSBBGH) is an extremely rare condition with only a few published case reports and series. However, there is no systematic review that has been published yet.
Objective: The study aims to conduct a systematic review on spontaneous simultaneous bilateral basal ganglion bleeding and a descriptive statistical analysis of collected data on epidemiology, clinical features, etiology, therapeutic approach and prognosis. This review aims to be a clinical reference for busy clinicians when they are faced with such a rare condition.
Methodology: This review has been carried out in accordance with recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
Results: Review of 60 cases showed that SSBBGH affected predominantly male patients (70%) with an average age of 50.8 ± 15.33 years and the male-to-female ratio was 2.5:1. The female patients tend to be older with an average age of 54.22 ± 16.67 years. Location of SSBBGHwas more common in the putamen (90% vs 10% non-putaminal). SSBBGH posed a significant mortality rate (33.33%). Among patients who survived, only 40.6% (13/32 report) have had favorable outcomes (mRS ≤ 2) and the remaining 59.4% (19/32) ended up with poor functional status (mRS ≥ 3-5). The most common implicated etiologies were hypertension followed by alcohol intoxication.
Conclusion: SSBBGH is a rare clinical entity with significant morbidity and mortality. Systemic approach can lead to early recognition of etiology and prompt treatment. Hypertension and the putamen are the most common etiology and location of SSBBGH, respectively. History of hypertension and age can help narrow differential diagnosis and limit unnecessary testing or intervention.
Keywords: bilateral basal ganglia bleeding, bilateral basal ganglia hemorrhage, non-traumatic, simultaneous
Introduction
Intracerebral hemorrhage (ICH) is defined by the American Stroke Association (ASA) as
Rapidly developing clinical signs of neurological dysfunction attributable to a focal collection of blood within the brain parenchyma or ventricular system that is not caused by trauma1
It is the second most common cause of stroke, accounting for 10–20% of all strokes. It is associated with significant and higher mortality and morbidity compared to ischemic stroke.2 The most widely used classification of ICH is based on anatomical location into deep subcortical ICH or lobar bleeding. Two etiological classifications have been developed lately but are not widely used. The first one is H-ATOMIC (Hypertension, Amyloid angiopathy, Tumor, Oral anticoagulants, Malformation, Infrequent, Cryptogenic and Combination) and the second one is SMASH-U classification (Structure vascular lesion, Medication, Amyloid angiopathy, Systemic disease, Hypertension, Undetermined).3–5 In most ICH cases, bleeding is solitary and unilateral and few are multiple and bilateral.6 Although SSBBGH is extremely rare, sporadic cases have been reported across the world. A precious knowledge of SSBBGH can be obtained by extracting the data from these cases and conducting a pooled data analysis. Presently, there is merely a review article by Yang et al;7 however, that has not provided a comprehensive insight on SSBBGH, since it has not been conducted systematically in accordance with the PRISMA guidelines.8 Additionally, traumatic etiologies were not excluded, which do not count for ICH as per definition from the ASA.1 This study aims to conduct an extensive systematic review of non-traumatic SBBGH to explore more accurate data on epidemiology, demographics, clinical characteristics, etiology and outcome. The main limitations of this study were the rarity of conditions, quality of the studies as all being case reports or case series, wide range of years of publication and insufficient data.
Methodology
This review has been carried out in accordance with recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.8
Eligibility Criteria
Published case reports, case series, case summaries or letters of SSBBGH in patients ≥12 years old. Only articles published in English partly (abstract) or fully (full-text) were reviewed. Articles must have provided sufficient data on epidemiology, demographics, clinical features, etiology, therapeutic intervention and prognosis. Traumatic bilateral basal ganglia bleeding was excluded.
Search Strategies and Sources
A comprehensive literature search on PubMed and Scopus was conducted for relevant published studies in English only. The search strategy included the keywords “bilateral basal ganglia hemorrhage” OR “bilateral basal ganglia bleedings”. Each selected full article was further assessed for cross references to find additional reports. Fifteen cases were originally written in Japanese and Chinese, however, we found them summarized and translated in English in other articles.7,9,10 These were included in the analysis.
Study Selection
Articles were selected initially based on the relevance to the topic thoroughly reviewing the titles and abstracts by two independent groups of three authors, and then the full texts of eligible articles were retrieved for further assessment and inclusion in this study. Disagreements were resolved by team consensus.
Data Collection and Management
Two reviewers independently extracted required data using a predesigned data extraction form (Table 1). The form included country and year of publication, patient demographics, clinical features, location and cause of bleeding as well as therapeutic interventions (conservative vs surgical) and prognosis. If modified Rankin Scale (mRS) was not reported, other available scales or descriptive information on outcomes were transformed into mRS by two authors independently and consensus was reached for any discrepancies. Favorable outcomes were considered as mRS ≤2 and unfavorable outcomes were mRS ≥3-5.
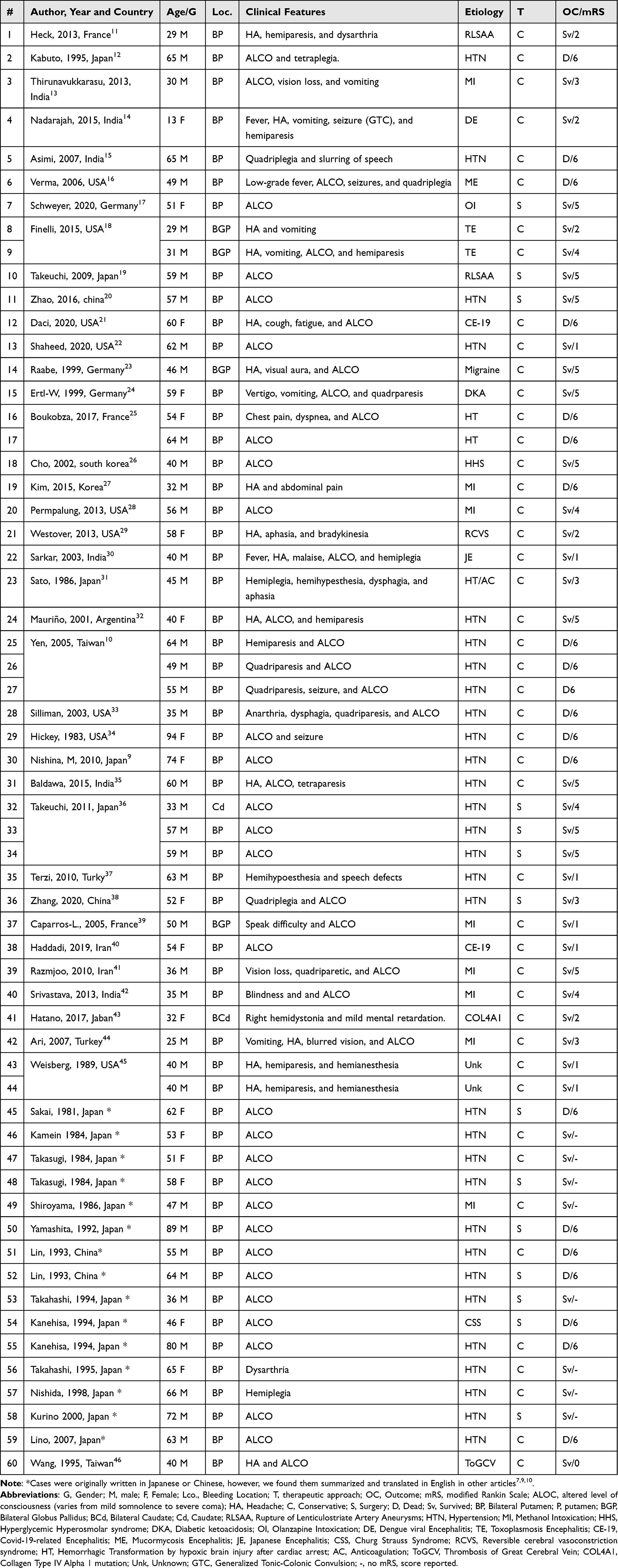 |
Table 1 Demography, Clinical Features, Etiologies, Therapeutic Approaches and Outcome of SSBBG |
Statistical Analysis
A descriptive analysis of the data collected was performed using EXCEL. Continuous variables are presented as mean + standard deviation (SD), and categorical variables are reported as frequencies and percentages.
Result
A total of 447 articles have been identified. We found 432 articles through PubMed and Scopus and the remaining 15 articles by reviewing article references. There were 19 duplicate articles that were removed. Three hundred articles were excluded due to non-relevance. Twenty-one articles were too old and not retrievable. We ended up with 107 articles that were assessed for eligibility. Of those, 65 articles were excluded for variable reasons: 5 articles because of age below 12 years old, 10 articles due to language barrier (not in English and not translated), 26 articles because of unilateral bleeding, 4 cases of non-simultaneous BBGB, 17 cases of traumatic simultaneous BBGH, and 3 cases with insufficient data. The remaining articles were 42 and included a total of 60 cases. The majority of reports were single case reports (Figure 1).
 |
Figure 1 PRISMA flow chart of this study. |
Epidemiology
SSBBGH is more commonly reported in Asia (68.3%) compared to other continents (31.6%). The majority of SSBBGH cases from Asia were from Japan (21/41; 51.2%) and India (6/41; 14.6%). There were only 11 cases (18.3%) reported in North America, 7 cases in Europe (11.6%) and 1 case (1%) in South America. To our knowledge, there were no case reports from Australia or Africa. This is most likely due to under-reporting rather than non-existence of the disease, since ICH is common in black as well as in low socio-economic populations.47 Table 2 summarizes the geographical distribution of reported SSBBGH cases.
 |
Table 2 Number of Cases and Percentage of SSBBGH in Different Continents and Countries |
Demographic
The overall mean age of patients with SSBBGH was 51.86 ±15.69 years. SSBBGH predominantly affects male patients (70%) with M:F ratio of 2.3:1. Male patients tend to be younger (50.8 ± 15.33 years) compared to their female counterparts (54.22 ± 16.67 years).
Clinical Manifestation
Altered level of consciousness, focal neurological deficit and headache were the most common clinical manifestations. They were present in 78.33%, 46.66% and 25% of SSBBGH reported cases, respectively. Seizure was an infrequent manifestation that was present only in 6.66% of reported cases. Systemic symptoms including vomiting, abdominal pain and fever were not uncommon (16%) and they were likely due to underlying disease rather than brain bleeding per se.
Etiology
Out of 60 reported cases, hypertension was the most common underlying etiology (50%) followed by intoxication and metabolic causes (18.33%). Within the intoxication category, alcohol was the most common offending agent (72.7%). Underlying vascular causes were found only in 16.66% of cases. Infection-related SSBBGH was the least common cause which accounted for only 10% of reported cases. In only 2 patients, there was no defining cause. Co-existence of multiple etiologies is possible. Table 3 summarizes all SSBBGH etiologies in descending order.
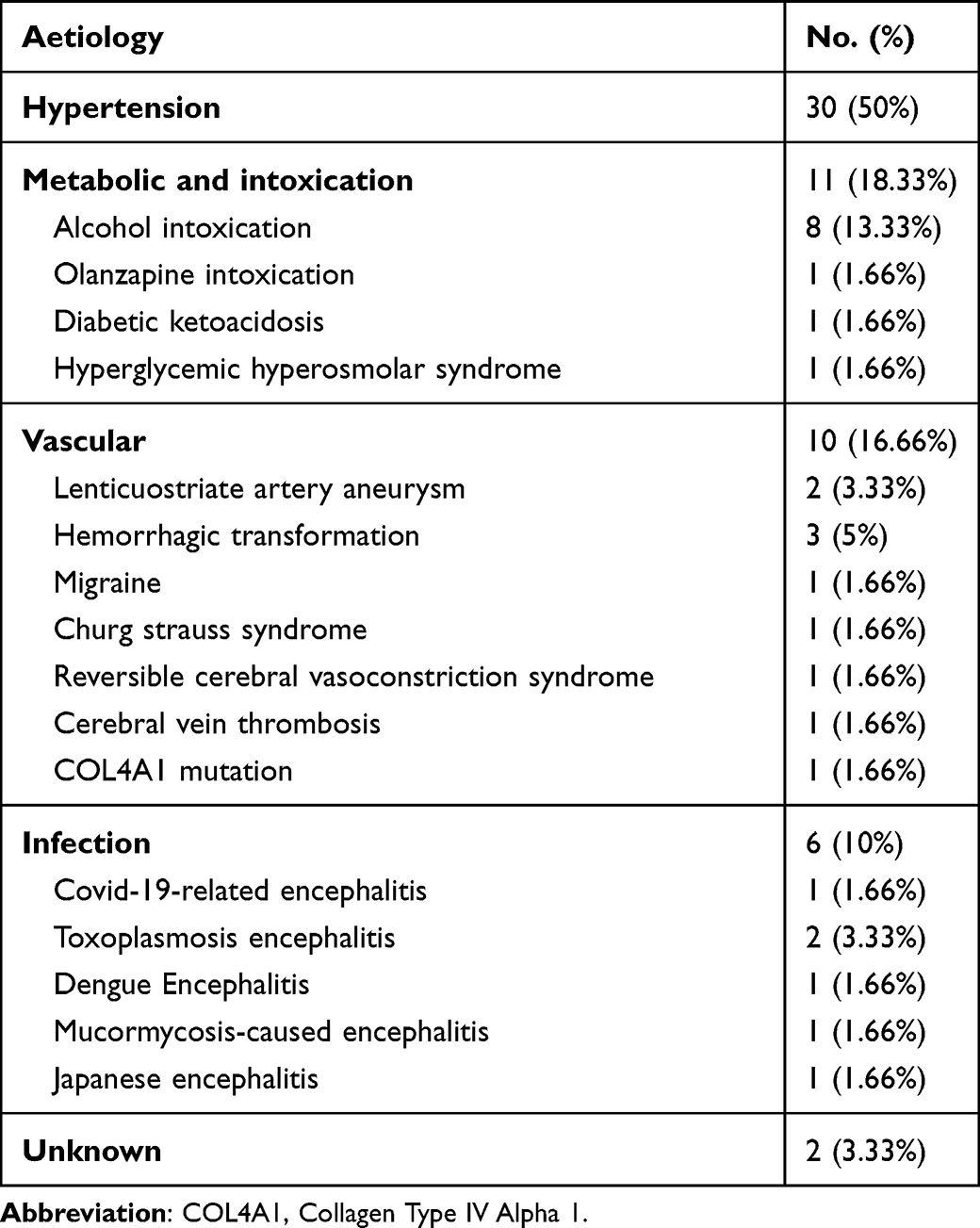 |
Table 3 Prevalence of SSBBGH Etiologies |
Location of Bleeding
Similar to unilateral basal ganglia hemorrhage (UBGH), putaminal SSBBGH was more common (54/60; 90%) than non-putaminal SSBBGH 6/60 (10%).
Therapeutic Approach and Prognosis
Conservative therapy was the main therapeutic approach with only 23.33% of patients undergoing surgical intervention mainly for complication management rather than primary intervention. The overall mortality of SSBBGH is 33.33%.
Discussion
SSBBGH is a rare subtype of ICH that carries similar mortality and morbidity to spontaneous unilateral ICH. Based on our systematic review, SSBBGH is more common in male and Asian ethnicity, similar to unilateral ICH.2
Decreased level of consciousness was the most common clinical manifestation which is expected given the bleeding is bilateral. The presence of systemic and visual impairment suggest metabolic and intoxication induced rather than brain bleeding per se.
Similar to unilateral deep ICH, hypertensive vasculopathy with formation of microaneurysm (Charcot-Bouchard aneurysm) of lateral lenticulostriate arteries was the main etiology for SSBBGH in patients above 50 years with longstanding hypertension. However, other eitopathogensis (eg, metabolic, infectious and vascular) (Table 3) was prevalent in the younger patient (<50 years) who presented with normal blood pressure (Figure 2). Ruíz-Sandoval found that the most common cause of unilateral ICH in young populations was vascular malformation (49%).48 Nevertheless, in our search, we could not find any VAM-related SSBBGH cases. Moreover, no primary brain tumor or metastases related SSBBGH were reported in the literature. These two conditions are possible and should always be included in etiological differential diagnoses of SSBBGH.
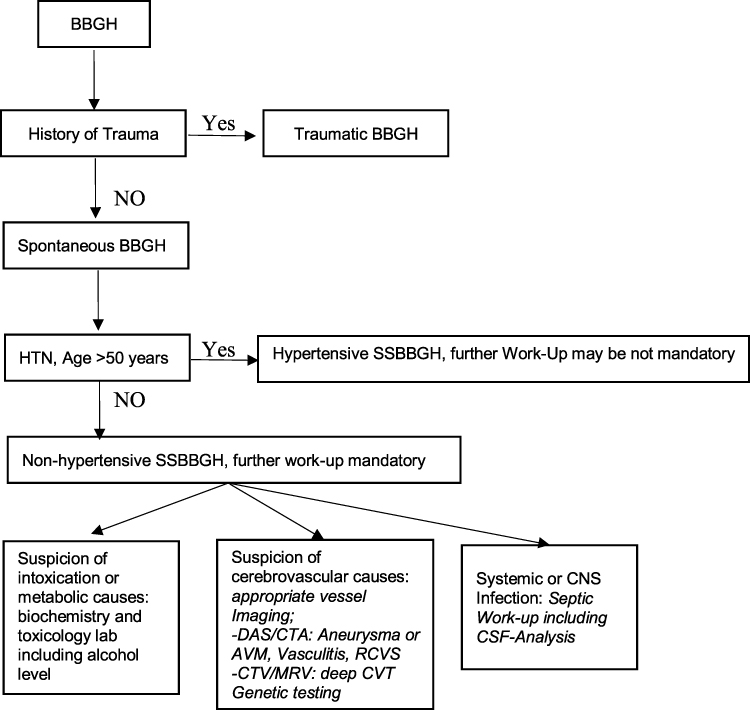 |
Figure 2 Logarithm for etiological approach of SSBBGH. Abbreviations: CNS, central nervous system; DSA, Digital Subtraction Angiography; CTA, Cerebral CT-Angiography; VAM, Arteriovenous Malformation; RCVS, Reversible Cerebral Vasoconstriction Syndrome; CTV, Cerebral CT-Venography; MRV, Magnetic Resonance Venography; CVT, Cerebral Vein Thrombosis; CSF, cerebrospinal fluid. |
Traumatic causes of BBGH are beyond the scope of this review; however, if we include traumatic literature, it is the second most common cause after hypertensive vasculopathy. The most common trauma mechanisms were direct head injury, neurosurgical procedures, and lightning strike.7
Forty percent of unilateral ICH occurs in the basal ganglia, particularly the putamen.49 Comparably, SSBBGH occurs predominantly in the putamen (93.3%) which is the most common location for both hypertensive and metabolic SSBBGH. Bleeding predilection to putamen may be due vulnerability of lateral lenticulostriate arteries to chronic hypertension.50 Moreover, some studies suggest that putaminal neurons are very sensitive to metabolic derangement such as acidosis and hypoxia.51
Looking at the literature, there is a comparable mortality rate among patients with either primary UBGH or SSBBGH that ranges from 37% to 46% and this is congruent with this study’s result (33.33%).52,53
Conclusion
Health-care providers should be aware of SSBBGH and its underlying etiopathogenesis. The most common cause of SSBBGH is hypertension. However, patients under 50 years with no history of hypertension are likely to have metabolic or intoxication induced SSBBGH which should prompt appropriate etiology-based workup and intervention.
Consent for Publication
Approval from the IRB committee at Imam Abdulrahman Bin Faisal University was not required to publish this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sacco RL, Kasner SE, Broderick JP, et al. American Heart Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Peripheral Vascular Disease; Council on Nutrition, Physical Activity and Metabolism. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. PMID: 23652265. doi:10.1161/STR.0b013e318296aeca
2. An SJ, Kim Tj, Yoon BW. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: an update. J Stroke. 2017;19(1):3–10. PMID: 28178408; PMCID: PMC5307940. doi:10.5853/jos.2016.00864
3. Meretoja A, Strbian D, Putaala J, et al. SMASH-U: a proposal for etiologic classification of intracerebral hemorrhage. Stroke. 2012;43(10):2592–2597. PMID: 22858729. doi:10.1161/STROKEAHA.112.661603
4. Martí-Fàbregas J, Prats-Sánchez L, Guisado-Alonso D, Martínez-Domeño A, Delgado-Mederos R, Camps-Renom P. SMASH-U versus H-ATOMIC: a head-to-head comparison for the etiologic classification of intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2018;27(9):2375–2380. PMID: 29779884. doi:10.1016/j.jstrokecerebrovasdis.2018.04.026
5. Mosconi MG, Paciaroni M, Agnelli G, et al. SMASH-U classification: a tool for aetiology-oriented management of patients with acute haemorrhagic stroke. Intern Emerg Med. 2021;16(1):109–114. PMID: 32266689. doi:10.1007/s11739-020-02330-2
6. Wu TY, Yassi N, Shah DG, et al. Simultaneous Multiple Intracerebral Hemorrhages (SMICH). Stroke. 2017;48(3):581–586. doi:10.1161/STROKEAHA.116.015186
7. Yang Z, Chen J, Mu J. Simultaneous bilateral basal ganglia hemorrhage. Curr Drug Deliv. 2017;14(6):807–815. doi:10.2174/1567201813666160607202811
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
9. Nishina M, Suga H, Deguchi Y, et al. A case of simultaneous bilateral putaminal hemorrhage. J Jpn Coll Surg. 2010;35(5):724–728.
10. Yen CP, Lin CL, Kwan AL, et al. Simultaneous multiple hypertensive intracerebral haemorrhages. Acta Neurochir. 2005;147(4):
11. Heck O, Anxionnat R, Lacour JC, et al. Rupture of lenticulostriate artery aneurysms. J Neurosurg. 2014;120(2):426–433. PMID: 24053505. doi:10.3171/2013.8.JNS13608
12. Kabuto M, Kubota T, Kobayashi H, Nakagawa T, Arai Y, Kitai R. Simultaneous bilateral hypertensive intracerebral hemorrhages–two case reports. Neurol Med Chir. 1995;35(8):584–586. PMID: 7566389. doi:10.2176/nmc.35.584
13. Thirunavukkarasu S, Nair PP, Wadwekar V. Acute bilateral putaminal haemorrhagic necrosis in methanol poisoning. BMJ Case Rep. 2013;2013:bcr2013201026. PMID: 24214154; PMCID: PMC3830263. doi:10.1136/bcr-2013-201026
14. Nadarajah J, Madhusudhan KS, Yadav AK, Gupta AK, Vikram NK. Acute hemorrhagic encephalitis: an unusual presentation of dengue viral infection. Indian J Radiol Imaging. 2015;25(1):52–55. PMID: 25709166; PMCID: PMC4329688. doi:10.4103/0971-3026.150145
15. Asimi RP, Wani MA, Ahmad F. Bilateral simultaneous hypertensive intracerebral hemorrhage in both putamen. Ann Indian Acad NeuroI. 2007;10:272. doi:10.4103/0972-2327.37824
16. Verma A. Bilateral basal ganglionic hemorrhage. Arch Neurol. 2006;63(3):464. PMID: 16533979. doi:10.1001/archneur.63.3.464
17. Schweyer K, Fatke B, Kreiser K, Rabe C, Seifert C, Ikenberg B. Bilateral basal ganglion hemorrhage after severe olanzapine intoxication. Case Rep Psychiatry. 2020;2020:2398721. PMID: 32953191; PMCID: PMC7481995. doi:10.1155/2020/2398721
18. Finelli PF, Wrubel GL. Bilateral pallidal hemorrhage in toxoplasmosis update of acute symmetric lesions of deep nuclei. Neuroradiol J. 2015;28(4):413–417. PMID: 26427898; PMCID: PMC4757304. doi:10.1177/1971400915609345
19. Takeuchi S, Takasato Y, Masaoka H, et al. Bilateral lenticulostriate artery aneurysms. Br J Neurosurg. 2009;23(5):543–544. PMID: 19718551. doi:10.1080/02688690902789166
20. Zhao J, Chen Z, Wang Z, Yu Q, Yang W. Simultaneous bilateral hypertensive basal ganglia hemorrhage. Neurol Neurochir Pol. 2016;50(4):275–279. PMID: 27375143. doi:10.1016/j.pjnns.2016.03.003
21. Daci R, Kennelly M, Ferris A, et al. Bilateral basal ganglia hemorrhage in a patient with confirmed COVID-19. AJNR Am J Neuroradiol. 2020;41(10):1797–1799. PMID: 32819902; PMCID: PMC7661071. doi:10.3174/ajnr.A6712
22. Shaheed TA, Glover N, Alboiny S. Nontraumatic spontaneous bilateral basal ganglia hemorrhage: a rare case report. Cureus. 2020;12(11):e11299. PMID: 33282576; PMCID: PMC7710344. doi:10.7759/cureus.11299
23. Raabe A, Krug U. Migraine associated bilateral intracerebral haemorrhages. Clin Neurol Neurosurg. 1999;101(3):193–195. PMID: 10536906. doi:10.1016/s0303-8467(99)00024-4
24. Ertl-Wagner B, Jansen O, Schwab S, Sartor K. Bilateral basal ganglion haemorrhage in diabetic ketoacidotic coma: case report. Neuroradiology. 1999;41(9):670–673. PMID: 10525769. doi:10.1007/s002340050822
25. Boukobza M, Baud FJ. Hemorrhagic infarct of basal ganglia in cardiac arrest. CT and MRI findings. 2 cases. Neurol Neurochir Pol. 2018;52(1):94–97. PMID: 28965668. doi:10.1016/j.pjnns.2017.09.004
26. Cho SJ, Won TK, Hwang SJ, Kwon JH. Bilateral putaminal hemorrhage with cerebral edema in hyperglycemic hyperosmolar syndrome. Yonsei Med J. 2002;43(4):533–535. PMID: 12205743. doi:10.3349/ymj.2002.43.4.533
27. Kim HJ, Na JY, Lee YJ, Park JT, Kim HS. An autopsy case of methanol induced intracranial hemorrhage. Int J Clin Exp Pathol. 2015;8(10):13643–13646. PMID: 26722590; PMCID: PMC4680535.
28. Permpalung N, Cheungpasitporn W, Chongnarungsin D, Hodgdon TM. Bilateral putaminal hemorrhages: serious complication of methanol intoxication. N Am J Med Sci. 2013;5(10):623–624. PMID: 24350079; PMCID: PMC3842708. doi:10.4103/1947-2714.120804
29. Westover MB, Cohen AB. Reversible vasoconstriction syndrome with bilateral basal ganglia hemorrhages. J Neuroimaging. 2013;23(1):122–125. PMID: 21899647; PMCID: PMC6788746. doi:10.1111/j.1552-6569.2011.00645.x
30. Sarkar N, Roy BK, Das SK, Roy T, Dhibar T, Ghorai S. Bilateral intracerebral haemorrhages: an atypical presentation of Japanese encephalitis. J Assoc Physicians India. 2005;53:144–146. PMID: 15847037.
31. Sato M, Tanaka S, Kohama A, Sone T, Fukunaga M, Morita R. Spontaneous bilateral intracerebral hemorrhage occurring simultaneously–case report. Neurol Med Chir. 1986;26(7):545–547. PMID: 2430218. doi:10.2176/nmc.26.545
32. Mauriño J, Saposnik G, Lepera S, Rey RC, Sica RE. Multiple simultaneous intracerebral hemorrhages: clinical features and outcome. Arch Neurol. 2001;58(4):629–632. PMID: 11295994. doi:10.1001/archneur.58.4.629
33. Silliman S, McGill J, Booth R. Simultaneous bilateral hypertensive putaminal hemorrhages. J Stroke Cerebrovasc Dis. 2003;12(1):44–46. doi:10.1053/jscd.2003.3
34. Hickey WF, King RB, Wang AM, Samuels MA. Multiple simultaneous intracerebral hematomas. Clinical, radiologic, and pathologic findings in two patients. Arch Neurol. 1983;40(8):519–522. PMID: 6870614. doi:10.1001/archneur.1983.04210070059016
35. Baldawa S. Owl eye appearance: simultaneous bilateral hypertensive putaminal hematoma. J Neurol Disord. 2015;3:225. doi:10.4172/2329-6895.1000225
36. Takeuchi S, Takasato Y, Masaoka H, Hayakawa T, Yatsushige H, Sugawara T. Simultaneous multiple hypertensive intracranial hemorrhages. J Clin Neurosci. 2011;18(9):1215–1218. PMID: 21752649. doi:10.1016/j.jocn.2011.01.020
37. Terzi M, Akkaya O, Onar M. Pure sensory stroke due to bilateral basal ganglion hemorrhage: a case report. Turk Neurosurg. 2010;20(3):406–408. doi:10.5137/1019-5149.JTN.1891-09.1
38. Zhang D, Yu J, Wang Z, Wang Y. Two different minimally invasive surgery puncture points with thrombolysis in a patient with bilateral basal ganglia hemorrhages. Int J Gen Med. 2020;13:1435–1439. PMID: 33335415; PMCID: PMC7737542. doi:10.2147/IJGM.S289238
39. Caparros-Lefebvre D, Policard J, Sengler C, Benabdallah E, Colombani S, Rigal M. Bipallidal haemorrhage after ethylene glycol intoxication. Neuroradiology. 2005;47(2):105–107. PMID: 15714272. doi:10.1007/s00234-005-1347-y
40. Haddadi K, Ghasemian R, Shafizad M. Basal ganglia involvement and altered mental status: a unique neurological manifestation of coronavirus disease 2019. Cureus. 2020;12(4):e7869. PMID: 32489724; PMCID: PMC7255547. doi:10.7759/cureus.7869
41. Razmjoo K, Naeeni RH, Nafissi S. Bilateral basal ganglia hemorrhagic necrosis due to methanol toxicity. Acta Neurol Belg. 2010;110(4):354–355.
42. Srivastava T, Kadam N. Bilateral putaminal hemorrhagic necrosis with rapid recovery of sensorium in a patient with methanol intoxication. J Postgrad Med. 2013;59(3):243–244. doi:10.4103/0022-3859.118058
43. Hatano T, Daida K, Hoshino Y, et al. Dystonia due to bilateral caudate hemorrhage associated with a COL4A1 mutation. Parkinsonism Relat Disord. 2017;40:80–82. PMID: 28442301. doi:10.1016/j.parkreldis.2017.04.009
44. Ari S, Caça I, Kayabaşi H. Bilateral complete optic atrophy and hemorrhagic infarction of the putamen caused by methanol intoxication. Ann Ophthalmol. 2007;39(3):249–252. doi:10.1007/s12009-007-0038-1
45. Weisberg LA, Stazio A, Elliott D, Shamsnia M. Putaminal hemorrhage: clinical-computed tomographic correlations. Neuroradiology. 1990;32(3):200–206. doi:10.1007/BF00589112
46. Wang PY, Shen WC. MRI in internal cerebral vein thrombosis: case note. Neuroradiology. 1995;37(6):447–448. doi:10.1007/BF00600088
47. O’Donnell MJ, Xavier D, Liu L, et al; INTERSTROKE investigators. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112–123. PMID: 20561675. doi:10.1016/S0140-6736(10)60834-3
48. Ruíz-Sandoval JL, Cantú C, Barinagarrementeria F. Intracerebral hemorrhage in young people: analysis of risk factors, location, causes, and prognosis. Stroke. 1999;30(3):537–541. PMID: 10066848. doi:10.1161/01.str.30.3.537
49. Steiner T, Kaste M, Forsting M, et al. Recommendations for the management of intracranial haemorrhage - part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis. 2006;22(4):294–316. PMID: 16926557. doi:10.1159/000094831
50. Gupta K, Das M. Charcot Bouchard Aneurysm. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. PMID: 31971704.
51. Dang YX, Shi KN, Wang XM. Early changes in glutamate metabolism and perfusion in basal ganglia following hypoxia-ischemia in neonatal piglets: a multi-sequence 3.0T MR study. Front Physiol. 2017;8:237. PMID: 28487658; PMCID: PMC5404207. doi:10.3389/fphys.2017.00237
52. Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the atherosclerosis risk in communities (ARIC) cohort. Stroke. 1999;30:736–743. doi:10.1161/01.STR.30.4.736
53. El-Saed A, Kuller LH, Newman AB, et al. Geographic variations in stroke incidence and mortality among older populations in four US communities. Stroke. 2006;37:1975–1979. doi:10.1161/01.STR.0000231453.98473.67
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.