")
Back to Journals » Clinical Ophthalmology » Volume 8
Spontaneous resolution of foveal detachment in dome-shaped macula observed by spectral domain optical coherence tomography
Authors Tamura N, Sakai T, Tsuneoka H
Received 24 September 2013
Accepted for publication 5 November 2013
Published 19 December 2013 Volume 2014:8 Pages 83—86
DOI https://doi.org/10.2147/OPTH.S54903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Nazuki Tamura, Tsutomu Sakai, Hiroshi Tsuneoka
Department of Ophthalmology, Jikei University School of Medicine, Tokyo, Japan
Abstract: Dome-shaped macula (DSM) was described by Gaucher et al as a convex protrusion of macula within a staphyloma in highly myopic eyes that causes visual impairment associated with serous foveal detachment (SFD). We describe a patient with spontaneous resolution of SFD in DSM documented by serial spectral domain optical coherence tomography (SD-OCT). A 28-year-old female Japanese patient presented with blurred vision in both eyes. Upon examination, her best-corrected visual acuity was 1.2 with -8.0 sphere and 0.5 with -8.0 sphere in the right and left eyes, respectively. SD-OCT in both eyes showed an anterior bulge of the macula with SFD. The diagnosis of DSM with SFD was made on the basis of characteristic findings. Three months later, the patient achieved spontaneous resolution of SFD without treatment. One month later, there was an occurrence of SFD in the right eye, but the SFD had disappeared in 1 month. In our case, her visual impairment was proven to be a consequence of SFD in relation to DSM. SD-OCT was useful for the detection and follow-up of SFD in DSM.
Keywords: dome-shaped macula, serial spectral domain optical coherence tomography, resolution
Introduction
Dome-shaped macula (DSM) was first described in 2008 using optical coherence tomography (OCT) by Gaucher et al.1 This condition involves a protrusion of the macula within a staphyloma in highly myopic eyes, which causes visual impairment associated with serous foveal detachment (SFD).2 Although the pathogenesis of DSM remains unclear, Imamura et al3 showed that DSM was associated with a relative localized thickness variation of the sclera under the macula. Recently, Caillaux et al4 demonstrated that chronic SFD was associated with decreased vision and was more common when the macular bulge was highly elevated. Therefore, DSM with SFD may be involved in more severe DSM forms. Here, we describe a patient with spontaneous resolution of SFD in DSM documented by serial spectral domain OCT (SD-OCT).
Case report
A 28-year-old female Japanese patient with no previous history of ocular disease was referred to our hospital 14 days after complaining of blurred vision in both eyes. She reported that she had flu-like symptoms 7 days before the initial visit. Upon initial examination, her best corrected visual acuity (BCVA) was 1.2 with −8.0 sphere and 0.5 with −8.0 sphere in the right and left eyes, respectively. No significant findings were observed in the anterior segment or vitreous of either eye. Funduscopy showed a mild staphyloma with some pigmentary changes in the fovea in both eyes (Figure 1A and 1B). Fluorescein angiography (HRA2; Heidelberg Engineering GmbH, Heidelberg, Germany) showed hyperfluorescence in the fovea in both eyes resulting from a retinal pigment epithelium defect, but there was no leakage point (Figure 1C and 1D). Indocyanine green angiography (HRA2; Heidelberg Engineering) in both eyes revealed punctuate hyperfluorescence in the fovea with no vascular hyperpermeability (Figure 1E and 1F). SD-OCT (CIRRUS HD-OCT; Carl Zeiss Meditec AG, Jena, Germany) in both eyes showed an anterior bulge of the macula with SFD in the horizontal scan (Figure 2A and 2B). The diagnosis of DSM with SFD was made on the basis of characteristic findings from previous studies.1–3 No treatment was initiated.
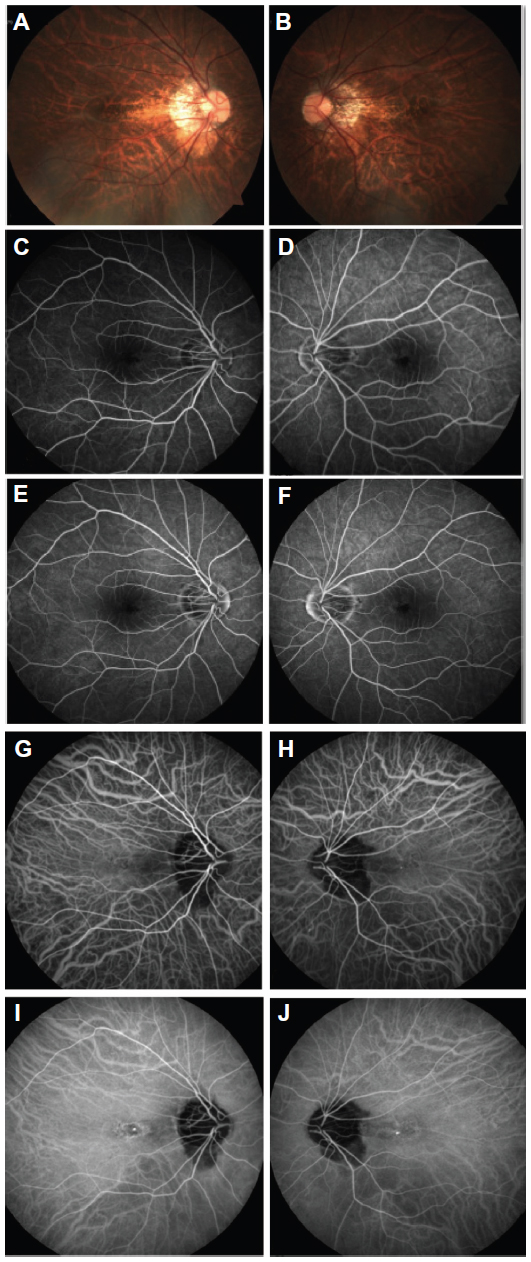 | Figure 1 Fundus photography, fluorescein angiography, and indocyanine green angiography. |
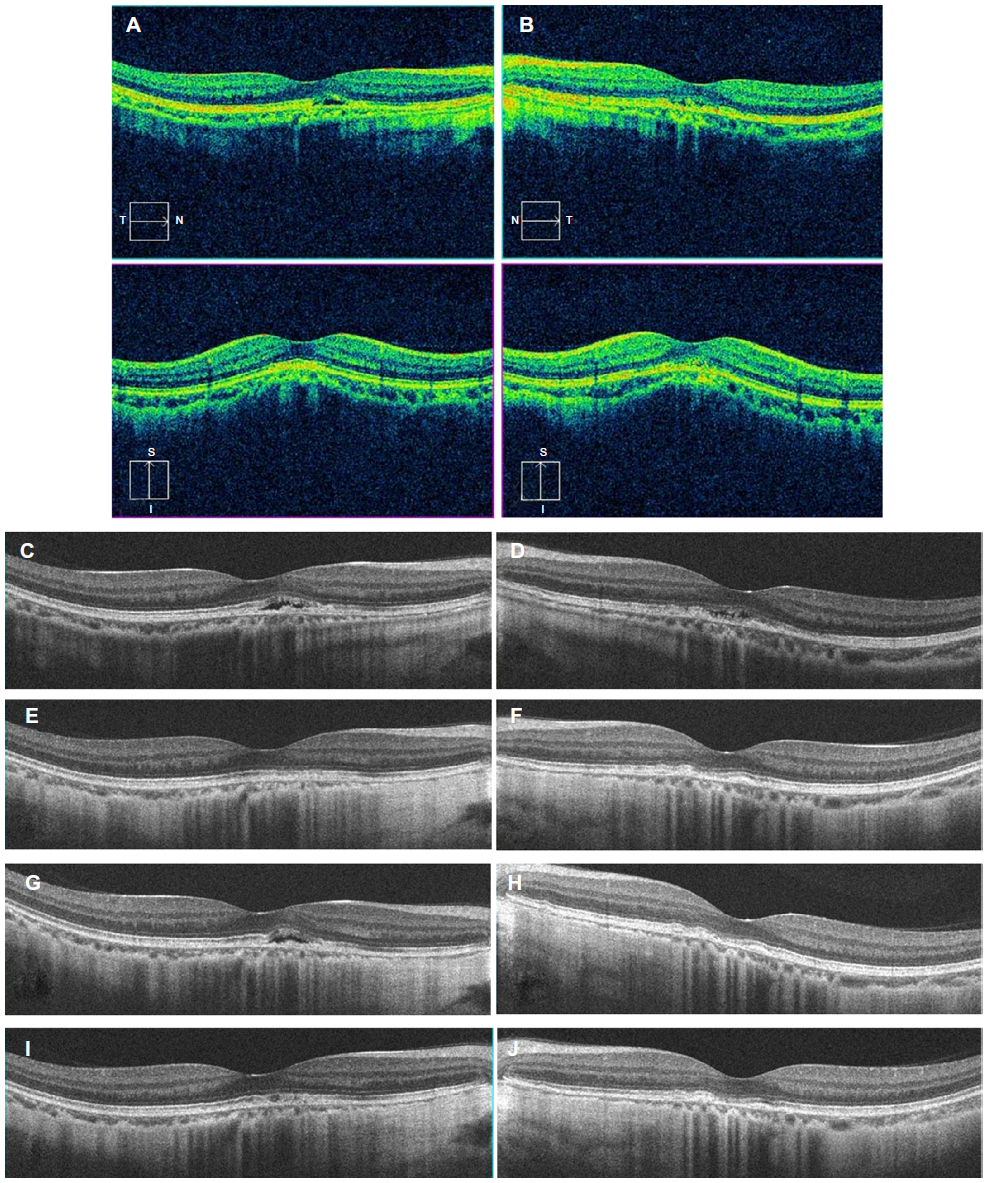 | Figure 2 Spectral domain optical coherence tomography in both eyes at initial and follow-up visits for dome-shaped macula with serous foveal detachment. |
Three months later, SFD seen at the initial visit disappeared on SD-OCT (Figure 2C and 2F), and the patient’s BCVA was 1.2 and 1.0 in the right and left eyes, respectively. Her symptoms had also subjectively improved. One month later, there was an occurrence of SFD in the right eye (Figure 2G and 2H), although subjective visual worsening was not reported. The left eye remained unaffected. One month later, the SFD had disappeared (Figure 2I and 2J), and the patient’s BCVA was 0.9 in the right eye.
Discussion
To our knowledge, this is the first report of the spontaneous resolution of SFD in DSM, based on a MEDLINE® (US National Library of Medicine, Bethesda, MD, USA) search of the English literature available on this subject. In this case, SD-OCT provided a definite diagnosis of DSM with SFD and permitted documentation of the spontaneous resolution of SFD in DSM. Similar spontaneous resolution was noted in cases with idiopathic central serous chorioretinopathy, and angiography and OCT enable differentiation from idiopathic central serous chorioretinopathy. In particular, punctuate hyperfluorescence with no vascular hyperpermeability on indocyanine green angiography, and an abnormal convex profile with no choroidal thickening on SD-OCT, may be important findings in DSM with SFD.1
Regarding the pathophysiology of DSM with SFD, Imamura et al3 suggested that severe obstruction in the outflow of choroidal fluid might be associated with the characteristic findings of DSM, while Byeon and Chu5 proposed that compressive changes of the choroid and choriocapillaris, as well as the resultant secondary retinal pigment epithelium changes, may be involved in the pathophysiology of DSM. Additional imaging analyses may reveal the details of the pathophysiology of DSM with SFD.
The SD-OCT images in our patient clearly showed shallow SFD in the parafovea and foveal center in the right and left eyes, respectively. In this case, a conservative observation was used, although left visual acuity was poor. Use of antivascular endothelial growth factor therapy, photodynamic therapy, and focal laser treatment have been described in other cases, but none of these approaches were effective.4 This suggests that choroidal neovascularization and choroidal vascular hyperpermeability are not associated with the pathophysiology of DSM with SFD.
In conclusion, the patient in this case had DSM with SFD, which showed spontaneous recovery without treatment. This case illustrates the utility of SD-OCT for the detection and follow-up of DSM with SFD.
Disclosure
The authors did not receive financial support for this study. The authors report no conflicts of interest in this work.
References
Gaucher D, Erginay A, Leleire-Collet A, et al. Dome-shaped macula in eyes with myopic posterior staphyloma. Am J Ophthalmol. 2008; 145(5):909–914. | |
Pardo-López D, Gallego-Pinazo R, Mateo C, et al. Serous macular detachment associated with dome-shaped macula and tilted disc. Case Rep Ophthalmol. 2011;2(1):111–115. | |
Imamura Y, Iida T, Maruko I, Zweifel SA, Spaide RF. Enhanced depth imaging optical coherence tomography of the sclera in dome-shaped macula. Am J Ophthalmol. 2011;151(2):297–302. | |
Caillaux V, Gaucher D, Gualino V, Massin P, Tadayoni R, Gaudric A. Morphologic characterization of dome-shaped macula in myopic eyes with serous macular detachment. Am J Ophthalmol. 2013;156(5):987–967. e1. | |
Byeon SH, Chu YK. Dome-shaped macula. Am J Ophthalmol. 2011; 151(6):1101; author reply 1101–1102. |
 © 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2013 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.