Back to Journals » International Journal of Women's Health » Volume 18
Spontaneous Heterotopic Pregnancy and Its Clinical Implications
Authors Zhao Y ![]() , Bai Y, Feng C
, Bai Y, Feng C ![]() , Ke R, Lu Y
, Ke R, Lu Y
Received 14 February 2026
Accepted for publication 18 April 2026
Published 23 April 2026 Volume 2026:18 601063
DOI https://doi.org/10.2147/IJWH.S601063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yue Zhao,* Yun Bai,* Chao Feng, Rubin Ke, Yanying Lu
Department of Obstetrics and Gynecology, Hangzhou Linping District Hospital of Integrated Traditional Chinese and Western Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Feng, Department of Obstetrics and Gynecology, Hangzhou Linping District Hospital of Integrated Traditional Chinese and Western Medicine, No. 60, Baojian Road, Linping Street, Hangzhou, Zhejiang, 311100, People’s Republic of China, Tel +8615268130564, Email [email protected]
Background: Heterotopic pregnancy is a rare but potentially life-threatening gynecologic emergency and is particularly uncommon in natural conceptions. Heterotopic pregnancies are prone to misdiagnosis due to the atypical clinical manifestations, especially after an intrauterine pregnancy has been confirmed.
Case Presentation: A case involving a 31-year-old female who presented with persistent abdominal pain and tenesmus after a medical abortion for a naturally conceived pregnancy is discussed. The initial ultrasound confirmed an early intrauterine pregnancy but a repeat ultrasound revealed a right adnexal mass with an accumulation of pelvic fluid accumulation. Laparoscopic exploration confirmed a right tubal heterotopic gestation. The hysteroscopic examination revealed retained products of conception within the uterine cavity.The patient underwent hysteroscopic removal of the retained intrauterine products of conception and a laparoscopic right salpingectomy. The postoperative histopathologic evaluation corroborated the diagnosis. The patient recovered uneventfully.
Conclusion: This case is a reminder that confirmation of an intrauterine pregnancy does not exclude the coexistence of an ectopic pregnancy. Clinicians should maintain a high index of suspicion in patients with ectopic pregnancy risk factors, such as a history of multiple abortions, pelvic inflammatory disease, and/or endometriosis, or in patients who develop persistent or recurrent abdominal pain following an abortion. Early diagnosis and treatment of a heterotopic pregnancy can avert potentially life-threatening complications.
Keywords: spontaneous heterotopic pregnancy, ectopic pregnancy, case report, laparoscopy, medical abortion
Introduction
A heterotopic pregnancy (HP) is a rare pathologic condition of pregnancy that is characterized by the simultaneous occurrence of intra- and extra-uterine gestations. The incidence of HP is estimated to be approximately 1 in 30,000 among natural conceptions.1 HP represents a diagnostic challenge in early pregnancy because of its low incidence and carries a potential risk of life-threatening complications. Because the clinical manifestations of HP often resemble the clinical manifestations of early pregnancy, threatened abortion, or isolated ectopic pregnancy, HP is prone to misdiagnosis or delayed diagnosis, which may lead to adverse outcomes, such as intra-abdominal hemorrhage or uterine rupture2–4. Herein a case of HP following natural conception that was diagnosed after medical abortion is reported. In addition, we have attempted to summarize strategies for early detection and key aspects of HP clinical management, thereby enhancing clinician awareness and vigilance regarding this rare condition through a detailed analysis of the diagnostic and therapeutic process.
Case Presentation
The patient was a 31-year-old G4P0030. Her last menstrual period was on 17 August 2024. The menstrual cycles were of regular length of 25 days and 3–4 days of menses. At 4 weeks gestation she experienced slight vaginal bleeding. The urine human chorionic gonadotropin (hCG) test was positive. The serum β-hCG level at 5 weeks gestation was 26,897 mIU/mL. Transvaginal ultrasonography confirmed an early intrauterine gestational sac with a visible yolk sac (Figure 1) and corpus luteum in the right ovary (Figure 2). The patient chose to undergo a voluntary interruption of pregnancy because the pregnancy was unintended. She was administered oral mifepristone (200 mg in divided doses) 3 d after the ultrasound.The products of conception, which were visually identified and confirmed by a physician (the specimen was not sent for histopathologic evaluation), were expelled 2 d after mifepristone administration. After the expulsion of the gestational sac, the patient had slightly increased vaginal bleeding, and a single dose of misoprostol 600 μg was administered. She was discharged from the outpatient observation room after 4 h with minimal vaginal bleeding and no abdominal pain. The patient noted intermittent lower abdominal pain 4 dafter the expulsion, which she did not consider concerning at the time. However, the pain intensified and was accompanied by a sensation of tenesmus. She returned to the hospital 7 d after the onset of pain for evaluation and was shown to have a serum β-hCG level of 12,123.4 mIU/mL. A transvaginal ultrasound revealed an inhomogeneous echogenic area within the uterine cavity (2.2 × 2.3×1.6 cm) (Figure 3), a mixed echogenic mass (6.6 × 3.1×3.5 cm) in the right adnexa (Figure 4), and free fluid in the pelvic cavity (Figure 5). She was admitted to the hospital with a preliminary diagnosis of “abdominal pain of undetermined cause, suspected right tubal ectopic pregnancy and incomplete abortion.” The medical history included three previous abortions but no history of abdominal surgery or pelvic inflammatory disease. After fully informed consent of the risks and benefits was confirmed, she underwent emergency diagnostic laparoscopy with concurrent hysteroscopy. Hysteroscopy was performed to evaluate the uterine cavity for retained products of conception given the ultrasound finding of an inhomogeneous echogenic area and the history of an incomplete abortion.The diagnostic laparoscopy revealed a hemoperitoneum (approximately 100 mL), slightly enlarged uterus, and right fallopian tube with a thickened ampulla (sausage-like in appearance) measuring approximately 7×4 × 3.5 cm. The right fallopian tube was unruptured with a blood clot adherent to the fimbria. The diagnostic hysteroscopy revealed gray-yellow residual tissue gray-yellow in color that was approximately 2 cm in size on the right uterine wall. A laparoscopic right salpingectomy and hysteroscopic removal of the retained products of conception were performed. The postoperative pathologic diagnosis was as follows: 1. right fallopian tube, chorionic villi, and decidual tissue in the tissue sample, confirming a tubal pregnancy (Figure 6); and 2. intrauterine contents, degenerated decidua, and some villous tissue (Figure 7). The final diagnosis was spontaneous HP (right tubal pregnancy). The patient recovered uneventfully and was discharged from the hospital in good condition.
 |
Figure 1 Intrauterine yolk sac (transvaginal ultrasound). |
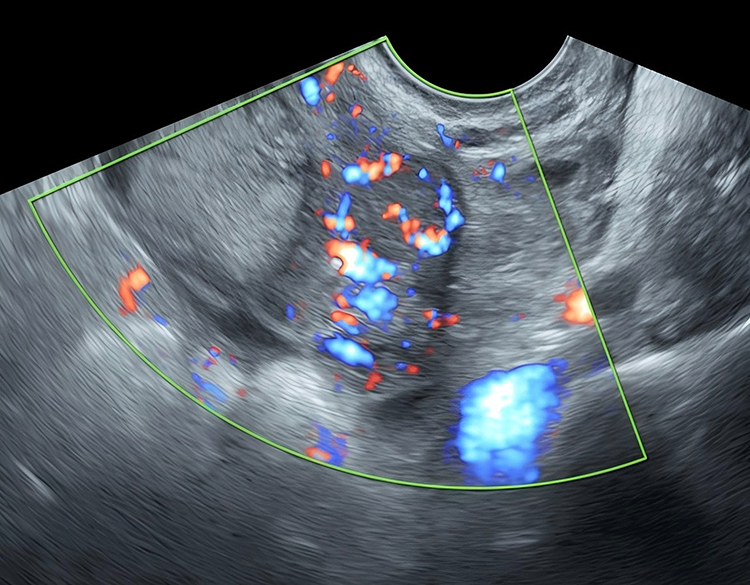 |
Figure 2 Right ovarian corpus luteum. |
 |
Figure 3 A transvaginal ultrasound revealed an inhomogeneous echogenic area within the uterine cavity (2.2 × 2.3×1.6 cm). |
 |
Figure 4 A mixed echogenic mass (6.6 × 3.1×3.5 cm) in the right adnexa. |
 |
Figure 5 Transvaginal ultrasound image showing free pelvic fluid. |
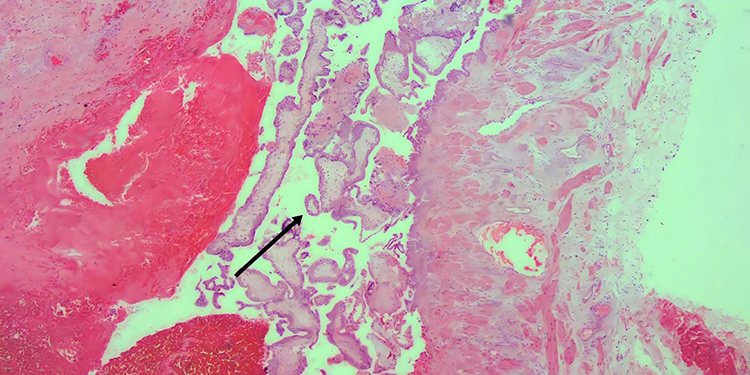 |
Figure 6 (HE staining, ×40) Villous structures (V) observed in the right fallopian tube (arrow). |
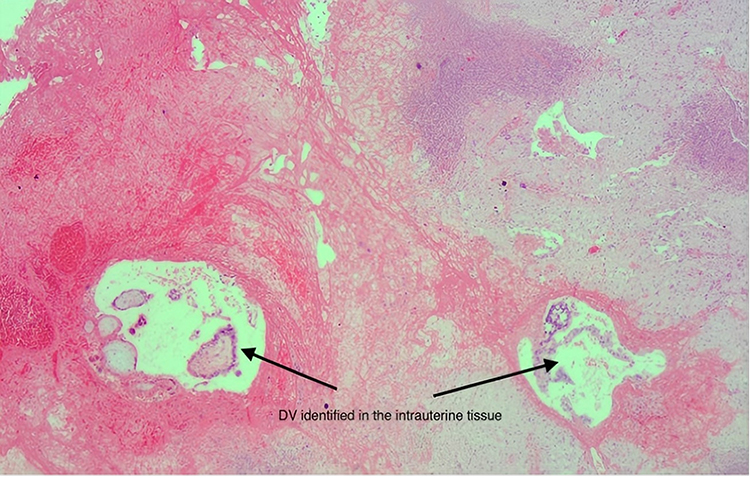 |
Figure 7 Degenerating villi (DV) identified in the intrauterine tissue (arrow). |
Discussion
This case clearly illustrates the typical trap of “confirmation bias” in the diagnosis of HP. When an early ultrasound confirms an intrauterine pregnancy and the patient subsequently undergoes a “successful” medical abortion, clinicians are prone to close the diagnostic loop, thereby overlooking the possibility of a concurrent ectopic pregnancy. In this case, an HP was only diagnosed after the patient presented with symptoms indicative of intra-abdominal hemorrhage, including abdominal pain and tenesmus, highlighting the critical importance of maintaining a high level of clinical suspicion.
The pathogenesis of HP is not completely understood, although HP is generally believed to share risk factors with ectopic pregnancy, including pelvic and fallopian tube abnormalities, cigarette smoking, intrauterine contraceptive device use, assisted reproductive technologies, and a history of multiple abortions.5,6 The patient reported herein had previously undergone three induced abortions, which may have been a risk factor leading to tubal mucosal inflammation or dysfunction and increasing the risk of embryo retention and implantation within the fallopian tube. The patient’s recent history of multiple sexual encounters during the ovulatory phase and ultrasound findings of bilateral ovarian corpus lutea (Figure 2–Figure 8). Support the hypothesis of a concurrent pregnancy, in which two ova were fertilized during the same ovulatory cycle and implanted ectopically. Although traditional studies suggest that follicle recruitment only occurs during the follicular phase, recent research has shown that follicle recruitment can also occur after ovulation in the mid-to-late luteal phase and even in the early follicular phase.7
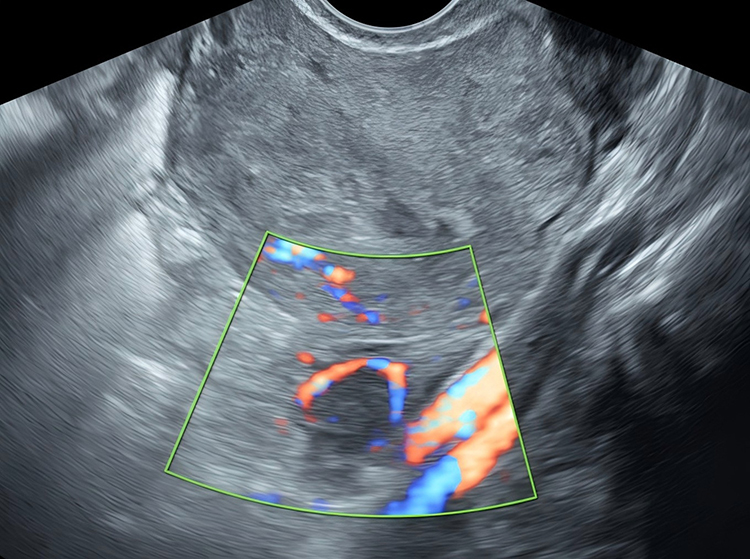 |
Figure 8 Left ovarian corpus luteum. |
Diagnostic Challenges and Implications
The clinical presentation of HP is non-specific and 30%–40% of patients may be asymptomatic with HP only detected through early ultrasound8 Other patients may present with symptoms of an intrauterine or ectopic pregnancy, including post-amenorrhea abdominal pain, vaginal bleeding, pelvic masses, or even intra-abdominal hemorrhage.9 The diagnosis of HP primarily relies on imaging (especially transvaginal ultrasound) with a diagnostic accuracy ranging from 82%–92.4%.10,11 However, the missed diagnosis rate for an initial ultrasound examination is notably high (12%–29%).4,10 In addition to confirmation bias, missed diagnoses may also result from the slower development of the ectopic pregnancy sac compared to an intrauterine sac or from confusion with structures, such as the ovarian corpus luteum.12 Therefore, we emphasize the need for a systematic and thorough evaluation of both adnexal regions for masses and fluid-filled areas despite the presence of an intrauterine gestational sac. In addition, attention should be paid to the size of the intrauterine sac and the examination should be performed by an experienced sonographer.10
It is noteworthy that the serum β-hCG level at 5 weeks gestation was 26,897 mIU/mL, which is considerably higher than the typical range for a singleton intrauterine pregnancy of that gestational age. Such an elevated β-hCG level should have raised suspicion for a multiple gestation, including the possibility of a heterotopic pregnancy, even before the abortion was initiated. This underscores the importance of considering β-hCG dynamics as an adjunctive clue in early pregnancy evaluation.
In the present case, because the initial ultrasound suggested an early intrauterine pregnancy and the patient requested termination of the pregnancy, the focus appeared to shift toward how to terminate the pregnancy. The subsequent apparently “successful” medical abortion led the clinician to overlook the abnormally elevated hCG level and the possibility of a concurrent heterotopic pregnancy.
Treatment Strategy
HP management should be individualized based on factors, such as the location of the ectopic pregnancy, size of the mass, gestational age, presence of internal bleeding, and the patient’s reproductive plans. Because the patient reported herein had undesired fertility, surgical removal of the ectopic pregnancy combined with hysteroscopic clearance of residual intrauterine tissue represented a thorough and reasonable approach. The primary goal of treatment for patients with desired fertility is thorough removal of the ectopic pregnancy while maximizing the probability of preserving the intrauterine pregnancy. Notably, 78%–91% of HP patients require surgical intervention.8,13 However, whether surgical treatment of HP increases the risk of early intrauterine fetal loss is controversial. Chen et al8 reported an early pregnancy loss rate of 14.4%, live birth rate of 85.6%, and preterm birth rate of 24.2% following surgery for HP. However, others contend that surgical treatment does not increase the risk of early intrauterine fetal loss.14
Conclusion
The current case represents a rare finding of an HP following a medical abortion and strongly underscores that the diagnosis of an intrauterine pregnancy and even what may appear to be a successful abortion cannot definitively rule out the possibility of a concurrent ectopic pregnancy. Maintaining a high level of diagnostic vigilance, performing standardized imaging evaluations, and actively investigating abdominal pain symptoms are essential for preventing missed diagnoses and ensuring patient safety. The diagnostic challenge was compounded in this case by “confirmation bias” after the initial ultrasound and the subsequent medical abortion, leading to a delay in diagnosis until the onset of symptoms (abdominal pain and tenesmus). The ultrasonographic finding of bilateral corpora lutea further supports the unique pathophysiology of superfecundation in this natural cycle.
Data Sharing Statement
The deidentified clinical dataset generated and analysed during this case report has been deposited in the Science Data Bank repository and is publicly available via the following persistent identifier (DOI): 10.57760/sciencedb.36360.
Ethical Statement
Written informed consent was obtained from the patient for this report.And written informed consent was obtained from the patient for the publication of this case report and any accompanying images.The publication of this case report details was approved by the Ethics Committee of Hangzhou Linping District Hospital of Integrated Traditional Chinese and Western Medicine.
Acknowledgment
We thank International Science Editing (http://www.internationalscienceediting.com) for editing this manuscript.
Disclosure
There are no relevant financial or non-financial competing interests to report.
References
1. Stanic Z, Roje D, Matić D, et al. Spontaneous heterotopic pregnancy as an uncommon clinical problem. Z Geburtshilfe Neonatol. 2020;224(4):223–8. doi:10.1055/a-1079-6260
2. OuYang Z, Yin Q, Xu Y, et al. Heterotopic cesarean scar pregnancy: diagnosis, treatment, and prognosis. J Ultrasound Med. 2014;33(9):1533–1537. doi:10.7863/ultra.33.9.1533
3. Gyokova E, Kostadinova Y, Odumosu EA. A rare case of heterotopic twin pregnancy after spontaneous conception. Cureus. 2025;17(2):e78928. doi:10.7759/cureus.78928
4. Talbot K, Simpson R, Price N, et al. Heterotopic pregnancy. J Obstet Gynaecol. 2011;31(1):7–12. doi:10.3109/01443615.2010.522749
5. Oancea M, Ciortea R, Diculescu D, et al. Spontaneous heterotopic pregnancy with unaffected intrauterine pregnancy: systematic review of clinical outcomes. Medicina. 2020;56(12):666. doi:10.3390/medicina56120665
6. Zhu S, Fan Y, Lan L, et al. Heterotopic pregnancy secondary to in vitro fertilization-embryo transfer: risk factors and pregnancy outcomes. Front Med Lausanne. 2022;9:864560. doi:10.3389/fmed.2022.864560
7. Baerwald AR, Adams GP, Pierson RA. A new model for ovarian follicular development during the human menstrual cycle. Fertil Steril. 2003;80(1):116–122. doi:10.1016/s0015-0282(03)00544-2
8. Chen L, Wen H, Xu D, et al. Management and pregnancy outcomes of heterotopic pregnancy [Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2018;53(11):768–775. doi:10.3760/cma.j.issn.0529-567x.2018.11.007
9. Elsayed S, Farah N, Anglim M. Heterotopic pregnancy: case series and review of diagnosis and management. Case Rep Obstet Gynecol. 2023;2023:2124191. doi:10.1155/2023/2124191
10. Xiao J, Zhou X, Wang S, et al. Ultrasound manifestations and clinical analysis of 50 cases of heterotopic pregnancy. J Clin Ultrasound. 2024;52(5):491–498. doi:10.1002/jcu.23660
11. Li XH, Ouyang Y, Lu GX. Value of transvaginal sonography in diagnosing heterotopic pregnancy after in-vitro fertilization with embryo transfer. Ultrasound Obstet Gynecol. 2013;41(5):563–569. doi:10.1002/uog.12341
12. Ahmed AA, Tom BDM, Calabrese P. Ectopic pregnancy diagnosis and the pseudo-sac. Fertil Steril. 2004;81(5):1225–1228. doi:10.1016/j.fertnstert.2003.09.068
13. Barrenetxea G, Barinaga-Rementeria L, Lopez de Larruzea A, et al. Heterotopic pregnancy: two cases and a comparative review. Fertil Steril. 2007;87(2):
14. Jeon JH, Hwang YI, Shin IH, et al. The risk factors and pregnancy outcomes of 48 cases of heterotopic pregnancy from a single center. J Korean Med Sci. 2016;31(7):1094–1099. doi:10.3346/jkms.2016.31.7.1094
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multiple Spontaneous Ectopic Pregnancies Following Bilateral Salpingectomy
Al-Nuaimy Y, John J, Alhomsi SM, Al-Baghdadi OO
International Medical Case Reports Journal 2023, 16:725-729
Published Date: 7 November 2023
Diagnostic Pitfall: Intrauterine Pseudogestational Sac Mimicking an Anembryonic Pregnancy in Tubal Ectopic Pregnancy A Case Report
Bunjamin IA, Gianina K, Nisa AS, Bhanuwati QR, Juslin NP, Aziz MA, Rahmarjanto BP
International Journal of Women's Health 2026, 18:582019
Published Date: 7 March 2026
Emergency Surgical Management of Ectopic Pregnancy Using Transvaginal NOTES (vNOTES) versus Laparoscopy: A Comparative Single-Surgeon Cohort Study
Şahin T
International Journal of Women's Health 2026, 18:599624
Published Date: 1 April 2026