Back to Journals » International Journal of Women's Health » Volume 18
Emergency Surgical Management of Ectopic Pregnancy Using Transvaginal NOTES (vNOTES) versus Laparoscopy: A Comparative Single-Surgeon Cohort Study
Authors Şahin T ![]()
Received 19 February 2026
Accepted for publication 26 March 2026
Published 1 April 2026 Volume 2026:18 599624
DOI https://doi.org/10.2147/IJWH.S599624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Turan Şahin
Department of Obstetrics and Gynecology, Sancaktepe Şehit Prof. Dr. Ilhan Varank Training and Research Hospital, Istanbul, Türkiye
Correspondence: Turan Şahin, Department of Obstetrics and Gynecology, Sancaktepe Şehit Prof. Dr. Ilhan Varank Training and Research Hospital, Istanbul, Türkiye, Tel +90-553-478-03-76, Email [email protected]
Background: Ectopic pregnancy remains a significant cause of maternal morbidity, and timely surgical intervention is critical, particularly in emergency settings.
Objective: To compare perioperative and early postoperative outcomes of transvaginal natural orifice transluminal endoscopic surgery (vNOTES) and laparoscopy in the emergency surgical management of ectopic pregnancy.
Materials and Methods: This retrospective cohort study included 63 patients who underwent emergency surgery for ectopic pregnancy, of whom 28 were treated with vNOTES and 35 with laparoscopy. Demographic characteristics, operative time, total intraoperative blood loss, procedure-related blood loss, hemoglobin change, β-hCG levels, and length of hospital stay were analyzed. ANCOVA was performed to adjust for the effect of total intraoperative blood loss. A subgroup analysis was conducted in 13 patients who underwent salpingostomy.
Results: Baseline characteristics, including age and BMI, were comparable between groups. Operative time was significantly shorter in the vNOTES group (47.57 ± 14.48 vs. 88.43 ± 26.00 minutes, p = 0.001). Although total intraoperative blood loss was higher in the vNOTES group, procedure-related blood loss was significantly lower (48.57 ± 16.04 vs. 85.71 ± 34.41 mL, p = 0.001). Hemoglobin decrease, postoperative β-hCG levels, and length of hospital stay were similar between groups. After adjustment, vNOTES remained independently associated with shorter operative time, lower procedure-related blood loss, and reduced hemoglobin decrease. In the salpingostomy subgroup, all cases involved tubal ectopic pregnancies.
Conclusion: In selected patients, vNOTES appears to be a feasible and safe minimally invasive approach in selected patients; however, these findings should be interpreted with caution due to the retrospective design and limited sample size.
Keywords: vNOTES, laparoscopy, ectopic pregnancy, emergency surgery, minimally invasive gynecology
Introduction
Ectopic pregnancy represents a significant challenge in obstetric care, accounting for approximately 1–2% of all pregnancies and remaining a leading cause of maternal morbidity and mortality during the first trimester.1 More than 90% of ectopic pregnancies occur within the fallopian tube, and delayed diagnosis or intervention may result in severe complications, including hemoperitoneum, acute anemia, and hemodynamic compromise.2
Laparoscopic surgery is currently considered the standard surgical approach for the management of ectopic pregnancy, offering favorable outcomes in terms of safety, recovery, and postoperative morbidity. Nevertheless, ongoing advances in minimally invasive surgery have led to the development of Natural Orifice Transluminal Endoscopic Surgery (NOTES) as an alternative access strategy. Among NOTES approaches, transvaginal NOTES (vNOTES) provides direct entry to the peritoneal cavity via the vaginal route, eliminating abdominal incisions and potentially reducing access-related surgical trauma.3
Previous studies evaluating vNOTES in benign and elective gynecologic procedures—such as hysterectomy and adnexal surgery—have suggested that this approach may be associated with shorter operative times, reduced postoperative pain, faster recovery, and comparable perioperative safety when compared with conventional laparoscopy.4 However, these findings predominantly originate from elective settings, limiting their generalizability to urgent or emergency clinical scenarios.
Evidence regarding the role of vNOTES in emergency gynecologic surgery, particularly in the management of ectopic pregnancy, remains limited. Emergency cases are characterized by variable degrees of intraperitoneal bleeding and time-sensitive decision-making, raising concerns regarding visualization, surgical control, and procedural safety when alternative access routes are employed.
Therefore, the present study aims to compare perioperative and early postoperative outcomes of vNOTES and conventional laparoscopy in patients undergoing emergency surgical management for ectopic pregnancy. By focusing on operative efficiency, intraoperative blood loss, postoperative recovery, and length of hospital stay, we sought to evaluate whether vNOTES may represent a feasible and safe minimally invasive option in selected emergency cases.
Materials and Methods
This retrospective cohort study was conducted at the Department of Obstetrics and Gynecology of a tertiary referral center. Between September 2021 and March 2025, a total of 63 consecutive patients who underwent emergency surgical management for ectopic pregnancy were included in the analysis. Patients were grouped according to the surgical approach employed: transvaginal natural orifice transluminal endoscopic surgery (vNOTES; n = 28) or conventional laparoscopy (n = 35). The choice of surgical approach was based on surgeon expertise, anatomical suitability (including vaginal accessibility and absence of severe pelvic adhesions), hemodynamic stability, and patient preference after detailed counseling regarding the risks and benefits of each technique. All procedures were performed by a single surgeon experienced in advanced minimally invasive gynecologic surgery. This retrospective study was approved by the Scientific Research Ethics Committee of Sancaktepe Şehit Prof. Dr. İlhan Varank Training and Research Hospital (Approval No: 137, Date: 30 April 2025). Written informed consent for surgical procedures was obtained from all patients prior to surgery. The study was conducted in accordance with the Declaration of Helsinki.
Women aged 18–45 years with a diagnosis of ectopic pregnancy requiring urgent surgical intervention were eligible for inclusion, provided they were hemodynamically stable or had been stabilized prior to induction of anesthesia. Emergency surgical intervention was defined as cases with suspected or confirmed ectopic pregnancy presenting with clinical signs such as acute abdominal pain, evidence of hemoperitoneum on imaging, decreasing hemoglobin levels, or risk of tubal rupture requiring urgent surgical management. Written informed consent was obtained from all patients. Exclusion criteria included a history of severe pelvic adhesions (such as obliteration of the pouch of Douglas or advanced-stage endometriosis), adnexal masses suspicious for malignancy, contraindications to general anesthesia, or refusal to undergo the proposed surgical approach.
Demographic and clinical data—including age, body mass index (BMI), parity, and obstetric history—were recorded. Perioperative variables included operative time, type of surgical procedure (salpingectomy or salpingostomy), estimated total intraoperative blood loss, presence and volume of hemoperitoneum, and intraoperative complications. Laboratory parameters comprised preoperative and postoperative hemoglobin and β-hCG levels. Postoperative outcomes included pain scores assessed using a visual analogue scale (VAS) at the 24th postoperative hour, length of hospital stay, and postoperative complications. The volume of hemoperitoneum was estimated intraoperatively based on the total amount of aspirated intraperitoneal blood and clots, combined with surgical field assessment by the operating surgeon. Procedure-related blood loss was calculated by subtracting the estimated hemoperitoneum volume from the total aspirated volume.
All surgeries were performed under general anesthesia with the patient in the lithotomy position. In the laparoscopy group, pneumoperitoneum was established at 12–14 mmHg using an umbilical 10-mm trocar (Endopath Xcel™, Ethicon, Cincinnati, OH, USA), followed by placement of two additional 5-mm trocars in the suprapubic and left lower quadrant regions. A 30° laparoscope (Karl Storz, Tuttlingen, Germany) was used for pelvic inspection. Hemoperitoneum was aspirated and the pelvis irrigated using a suction–irrigation system (Endopath Suction/Irrigation, Ethicon, USA). Salpingectomy or salpingostomy was performed using a LigaSure™ vessel sealing device (Medtronic, Minneapolis, MN, USA), with adjunctive monopolar electrosurgery when necessary. Hemostasis was achieved with bipolar forceps (Erbe Elektromedizin GmbH, Tübingen, Germany). Surgical specimens were retrieved using an endobag (EndoCatch™, Covidien, Mansfield, MA, USA). After irrigation with normal saline, hemostasis was reassessed under low-pressure pneumoperitoneum, and trocar sites were closed with absorbable sutures (Vicryl™ 2–0, Ethicon, USA).
In the vNOTES group, following bladder catheterization, a posterior colpotomy measuring approximately 2–2.5 cm was created at the level of the posterior fornix (Video S1). A multi-channel transvaginal access platform (GelPOINT V-Path™, Applied Medical, Rancho Santa Margarita, CA, USA) was inserted, and pneumoperitoneum was established at 10–12 mmHg. A 30° endoscope (Olympus, Tokyo, Japan) was used for pelvic exploration. Hemoperitoneum was aspirated and irrigated until adequate visualization was achieved. The affected fallopian tube was coagulated and divided segmentally using a LigaSure™ vessel sealing system. Bipolar coagulation was applied for hemostasis as required. In cases undergoing salpingostomy, a longitudinal incision was made on the antimesenteric border of the tube, and the ectopic gestation was carefully removed. Hemostasis of the tubal bed was achieved with selective bipolar coagulation to minimize thermal damage and preserve tubal integrity (Video S2). Specimens were retrieved transvaginally, either directly or within an endobag. The pelvis was irrigated with saline, hemostasis was confirmed under low-pressure pneumoperitoneum, and the colpotomy was closed with absorbable sutures (Vicryl™ 0, Ethicon, USA) (Figure 1).
 |
Figure 1 Surgical steps of the vNOTES procedure: colpotomy, peritoneal access, vNOTES port placement, intra-abdominal ectopic focus, ectopic mass after salpingostomy, and colpotomy repair. |
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). Normality of continuous variables was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were expressed as frequencies and percentages and compared using Fisher’s Exact test or the Fisher–Freeman–Halton Exact test. To adjust for potential confounding factors, particularly total intraoperative blood loss, analysis of covariance (ANCOVA) was performed, and adjusted means with corresponding p-values were reported. A two-sided p-value < 0.05 was considered statistically significant.
Results
A total of 63 patients were included in the analysis, of whom 28 underwent vNOTES and 35 underwent conventional laparoscopy. Baseline demographic characteristics were comparable between groups, with no significant differences observed in age (30.18 ± 6.06 vs. 32.14 ± 4.52 years) or body mass index (24.73 ± 3.20 vs. 26.10 ± 2.51 kg/m2; p > 0.05). Differences were noted in obstetric history: a higher proportion of patients in the vNOTES group had a history of vaginal delivery (60.7%), whereas prior cesarean delivery was more common in the laparoscopy group (68.6%) (p = 0.001). The anatomical location of ectopic pregnancy was similar between groups, with tubal ectopic pregnancy accounting for 96.4% of cases in the vNOTES group and 100% in the laparoscopy group. The distribution of surgical procedures (salpingectomy versus salpingostomy) did not differ significantly between groups (p > 0.05) (Table 1).
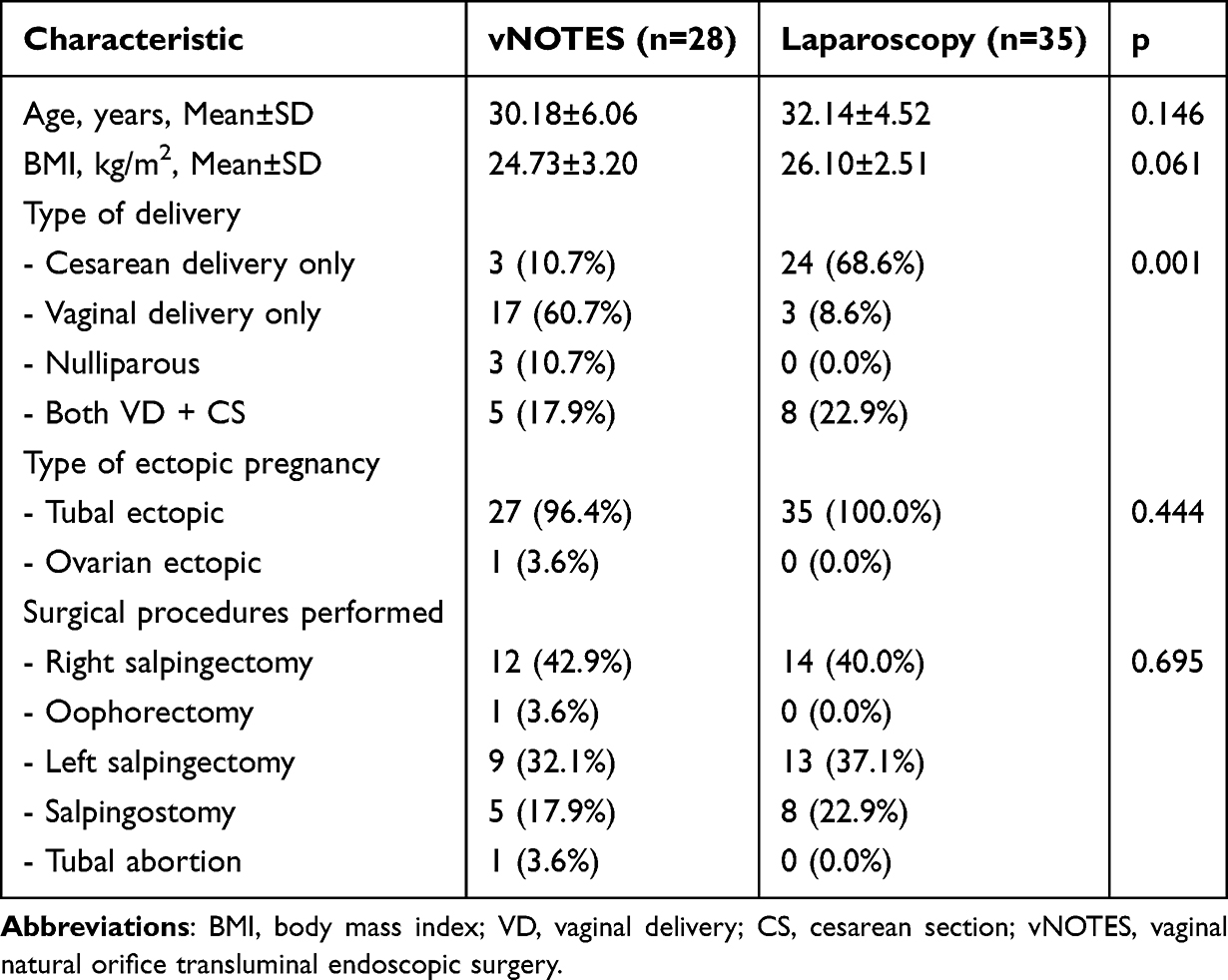 |
Table 1 Demographic and Clinical Characteristics of Patients Undergoing vNOTES and Laparoscopy for Ectopic Pregnancy |
Perioperative outcomes are summarized in Table 2. Operative time was significantly shorter in the vNOTES group compared with the laparoscopy group (47.57 ± 14.48 vs. 88.43 ± 26.00 minutes, p = 0.001). Although total intraoperative blood loss was higher in the vNOTES group (822.32 ± 579.40 mL vs. 485.14 ± 573.01 mL, p = 0.002), procedure-related blood loss was significantly lower in patients undergoing vNOTES (48.57 ± 16.04 mL vs. 85.71 ± 34.41 mL, p = 0.001), indicating reduced surgical bleeding despite greater preexisting hemoperitoneum. Hemoglobin decrease did not differ significantly between groups (p = 0.062). Preoperative and postoperative β-hCG levels were comparable, with no statistically significant differences observed (p > 0.05). The mean length of hospital stay was similar between groups (1.04 ± 0.20 days in the vNOTES group vs. 1.40 ± 0.30 days in the laparoscopy group; p = 0.742). No major intraoperative complications were recorded in either group.
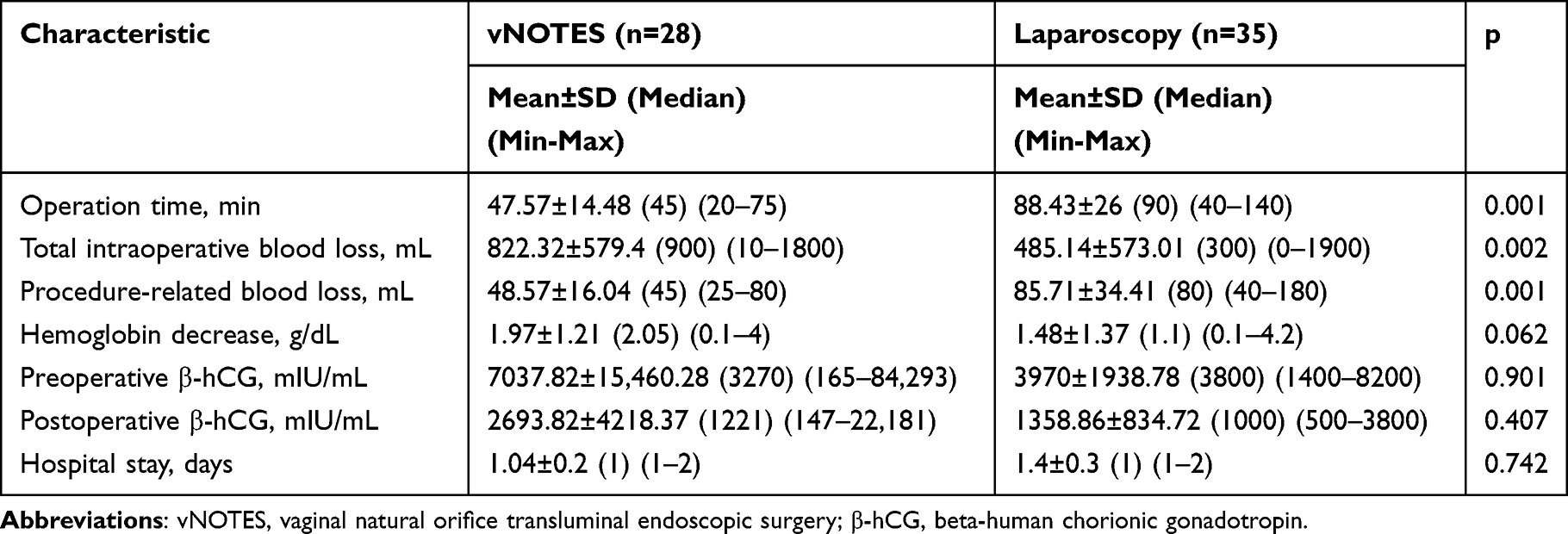 |
Table 2 Perioperative and Postoperative Findings of Patients Undergoing vNOTES and Laparoscopy for Ectopic Pregnancy |
To account for the potential confounding effect of total intraoperative blood loss, an analysis of covariance was performed (Table 3). After adjustment, the vNOTES approach remained independently associated with a shorter operative time (44.84 ± 18.52 vs. 90.61 ± 21.08 minutes, p = 0.001) and lower procedure-related blood loss (50.64 ± 16.12 vs. 84.06 ± 33.31 mL, p = 0.001). In addition, hemoglobin decrease was significantly lower in the vNOTES group after adjustment for total blood loss (p = 0.020). No significant differences were observed in preoperative or postoperative β-hCG levels following adjustment (p > 0.05), suggesting that the observed surgical advantages of vNOTES were independent of the volume of hemoperitoneum.
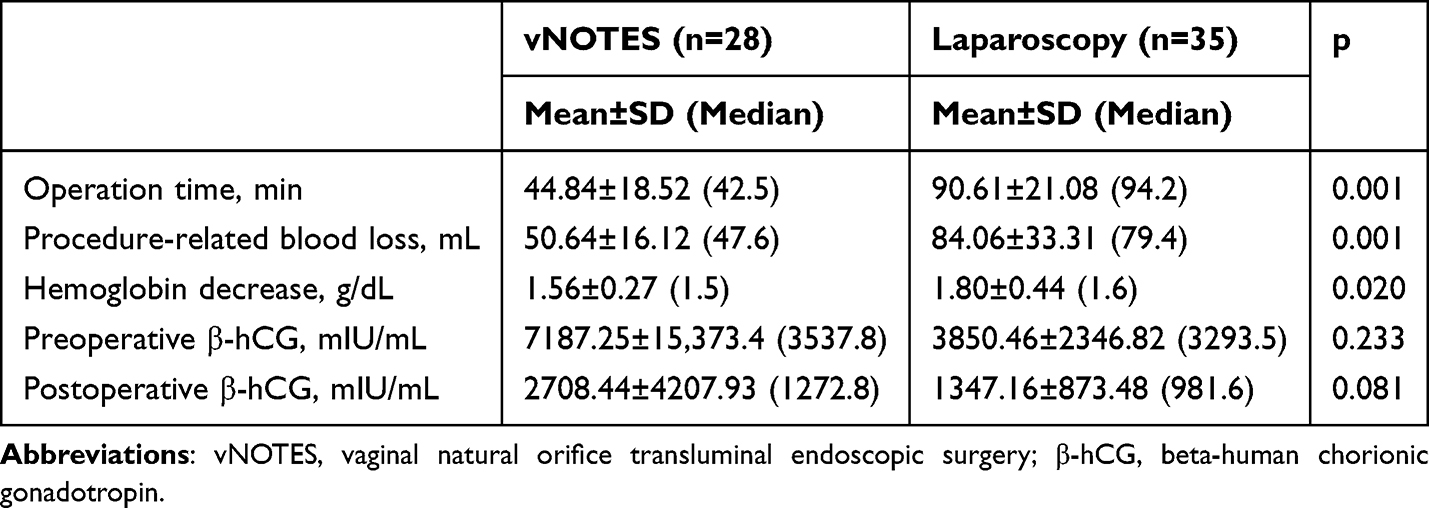 |
Table 3 Outcomes Adjusted for Total Intraoperative Blood Loss |
A subgroup analysis was performed in 13 patients who underwent salpingostomy (Table 4). The mean age of these patients was 30.23 ± 4.88 years, and the mean BMI was 24.78 ± 2.71 kg/m2. The median operative time was 75 minutes (mean 72.31 ± 22.42 minutes). None of the patients in this subgroup had ruptured ectopic pregnancy, and the volume of hemoperitoneum was minimal (18.85 ± 29.45 mL). The mean procedure-related blood loss was 101.15 ± 47.18 mL. All salpingostomy cases involved tubal ectopic pregnancy, with 38.5% managed via vNOTES and 61.5% via laparoscopy. This exploratory subgroup analysis provides descriptive insight into salpingostomy outcomes within the study cohort.
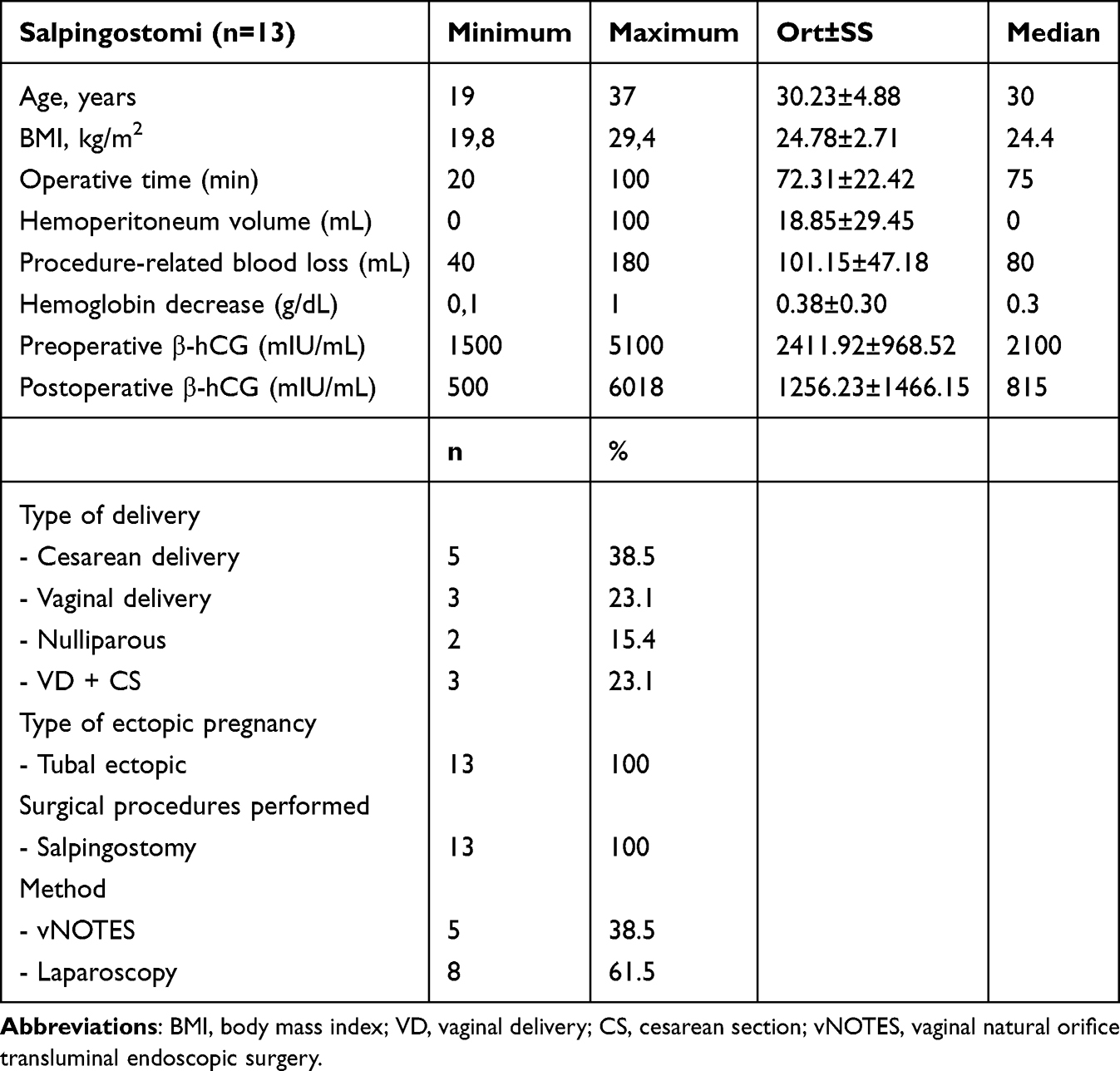 |
Table 4 Clinical and Surgical Characteristics of Patients Who Underwent Salpingostomy (n=13) |
Discussion
In our cohort, the findings that emergency ectopic pregnancy surgery via vNOTES was technically feasible, associated with low procedure-specific blood loss and short hospital stay, are consistent with the high-quality evidence base established in elective gynecology. The HALON randomized controlled trial demonstrated that vNOTES hysterectomy was non-inferior to laparoscopy, achieving higher rates of same-day discharge, shorter operative times, and reduced postoperative pain.5 Similarly, the NOTABLE RCT on adnexal surgery reported significantly shorter operative times and faster recovery with vNOTES compared to laparoscopy.6 A 2020 meta-analysis and subsequent expanded reviews in 2024 confirmed that vNOTES is associated with shorter operative duration, less blood loss, and reduced hospital stay, while complication rates remained comparable to laparoscopy.7–9 Although these data predominantly derive from elective settings, they provide a relevant framework for interpreting our findings, supporting the interpretation that our findings of shorter operative time and lower procedure-specific blood loss—even in an emergency context—may reflect intrinsic technical advantages of a standardized vNOTES technique. Furthermore, the ongoing VaNoLaH pragmatic multicenter RCT, with ≤12-hour discharge as its primary endpoint, is expected to further consolidate these clinical benefits.10
In ruptured ectopic pregnancy, a potential mechanistic time advantage of vNOTES arises from posterior colpotomy, which provides direct access to the most gravity-dependent compartment of the peritoneal cavity, the pouch of Douglas. The rectouterine pouch is the lowest point of the female pelvis, where free blood preferentially accumulates.11 When the posterior colpotomy is opened, a substantial proportion of the hemoperitoneum drains spontaneously via the vaginal route, a principle long recognized from culdocentesis and transvaginal drainage studies.12–14 This facilitates rapid clearance of the operative field, restoring optical visualization at an early stage of the procedure and allowing targeted hemostatic interventions—such as mesosalpinx coagulation and selective bipolar cauterization—without delay.15 In contrast, laparoscopic management of massive hemoperitoneum often begins with prolonged aspiration of clots and blood before visualization is achieved, which may prolong operative time even in experienced hands.16,17 While laparoscopy remains feasible and safe in hemodynamically stable patients with ruptured ectopic pregnancy, vNOTES may confer a procedural time advantage by providing “natural drainage” and direct entry into the pouch of Douglas, thereby explaining the shorter operative times observed in our series. By reporting both total blood loss and procedure-specific blood loss (excluding pre-existing hemoperitoneum), our study quantitatively highlights this distinction, consistent with step-by-step vNOTES technique descriptions.15
Specifically for ectopic pregnancy, recent comparative and prospective data published between 2024 and 2025 support vNOTES as a safe and effective alternative to laparoscopy in selected cases. A 2024 Heliyon cohort demonstrated that vNOTES salpingectomy reduced pain, shortened hospital stay, and aligned with ERAS principles while offering scarless cosmetic benefits.14 A 2025 multicenter and case-control series further reported that vNOTES salpingectomy was safe, associated with shorter hospital stay, and in some series, shorter operative times compared to laparoscopy.18,19 These findings align with our results of short operative time and hospitalization; however, definitive conclusions regarding superiority in the emergency setting require validation through prospective randomized comparisons. The ongoing vNOTESTEP RCT is designed to compare vNOTES with TU-LESS in tubal ectopic pregnancy, assessing perioperative and long-term outcomes including sexual function.20
In terms of safety and learning curve, large elective series and learning curve analyses consistently show low complication rates and a manageable pathway to proficiency with vNOTES.21–23 Analyses between 2022 and 2024 demonstrated that CUSUM-based competence plateaus can be reached within a limited number of cases, with significant reductions in operative time and blood loss once standardized surgical steps (posterior fornix entry, multichannel vaginal port placement, mesosalpinx coagulation, selective bipolar hemostasis) are applied.22,23 The absence of major complications and low procedure-specific blood loss in our cohort are consistent with this literature and may, in part, reflect the impact of single-surgeon expertise. Prior to the study period, the operating surgeon had performed more than 200 vNOTES procedures and over 400 laparoscopic adnexal surgeries, and was also maintaining an active series of more than 220 vaginal myomectomies. This high-volume surgical experience likely contributed to technical standardization and minimized variability related to learning curve effects.
Patient-reported outcomes and cosmetic benefit are among the strongest advantages of vNOTES. The absence of visible abdominal scars is not merely cosmetic but clinically relevant for body image, self-esteem, and patient satisfaction. Contemporary reviews highlight that the “scarless” advantage, combined with reduced pain and faster mobilization, constitutes a comprehensive benefit package.9 In reproductive-aged women, validated instruments such as SCAR-Q and the Female Genital Self-Image Scale (FGSIS) capture the psychosocial impact of scars, while studies have shown that sexual function outcomes following vNOTES are at least equivalent to laparoscopy.24–26 Although these outcomes were not specifically assessed in the present study, they remain relevant considerations for future research, particularly in emergency settings.
From an economic perspective, a 2025 comparative analysis of benign adnexal surgery reported that vNOTES was associated with shorter operative and recovery times and lower overall costs, largely driven by reduced operating room and inpatient utilization.27 While cost analysis was not performed in our cohort, the shorter hospital stay and operative duration observed in our cohort suggest the potential for similar economic benefits in the emergency setting, a hypothesis that requires direct evaluation in future studies.
This study has several limitations. The retrospective design inherently carries a risk of confounding that cannot be completely excluded. The choice of surgical approach (vNOTES vs. laparoscopy) was not based on hemodynamic stability but rather on clinical judgment, surgeon experience, and institutional logistics. Consequently, selection bias related to unmeasured variables cannot be excluded. The relatively small sample size limits the statistical power, particularly for secondary outcomes, and should be considered when interpreting the results. Although a single-surgeon experience ensures technical standardization, it also restricts generalizability. Furthermore, long-term outcomes including fertility, pelvic floor function, sexual health, and quality of life were not assessed. Validation of these findings will require large-scale, multicenter, and preferably randomized prospective studies.
In summary, posterior colpotomy provides direct access to the dependent pelvic recess, allowing immediate evacuation of hemoperitoneum and early restoration of visualization, an anatomic and technical advantage in ruptured ectopic pregnancy. This may explain the lower procedure-specific blood loss and shorter operative times observed in our series. Together with improved recovery, cosmetic outcomes, and patient satisfaction, vNOTES appears to be a feasible minimally invasive option in selected emergency ectopic pregnancies. However, these findings should be interpreted with caution due to the retrospective design and limited sample size. Further prospective, preferably randomized studies are required to confirm these findings and to better define its comparative effectiveness against laparoscopy. The results of ongoing studies such as VaNoLaH and vNOTESTEP are expected to provide higher-level evidence regarding patient selection and long-term outcomes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author declares no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Zhang S, Liu J, Yang L, Li H, Tang J, Hong L. Global burden and trends of ectopic pregnancy: an observational trend study from 1990 to 2019. PLoS One. 2023;18(10):e0291316. doi:10.1371/journal.pone.0291316
2. Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertil Res Pract. 2015;1:15. doi:10.1186/s40738-015-0008-z
3. Sarah VP, Jan B. Natural orifice transluminal endoscopic surgery (NOTES) salpingectomy for ectopic pregnancy: a first series demonstrating how a new surgical technique can be applied in a low-resource setting. Gynecol Surg. 2015;12(4):299–9. doi:10.1007/s10397-015-0904-6
4. Zhang S, Zhou D, Yan J-B, Zhang B, Meng Q-W, Lv Q-B. Analysis of feasibility, effectiveness and safety of transvaginal natural orifice transluminal endoscopic surgery(vNOTES) of ectopic pregnancy: a retrospective study. BMC Surgery. 2025;25(1):49. doi:10.1186/s12893-024-02740-5
5. Baekelandt JF, De Mulder PA, Le Roy I, et al. Hysterectomy by transvaginal natural orifice transluminal endoscopic surgery versus laparoscopy as a day-care procedure: a randomised controlled trial. Bjog. 2019;126(1):105–113. doi:10.1111/1471-0528.15504
6. Baekelandt J, De Mulder PA, Le Roy I, et al. Adnexectomy by vaginal Natural Orifice Transluminal Endoscopic Surgery versus laparoscopy: results of a first randomised controlled trial (NOTABLE trial). Bjog. 2021;128(11):1782–1791. doi:10.1111/1471-0528.16838
7. Housmans S, Stuart A, Bosteels J, Deprest J, Baekelandt J. Standardized 10-step approach for successfully performing a hysterectomy via vaginal natural orifice transluminal endoscopic surgery. Acta Obstet Gynecol Scand. 2022;101(6):649–656. doi:10.1111/aogs.14367
8. Marchand GJ, Masoud AT, Ulibarri H, et al. Systematic review and meta-analysis of vaginal natural orifice transluminal endoscopic surgery vs laparoscopic hysterectomy. AJOG Glob Rep. 2024;4(1):100320. doi:10.1016/j.xagr.2024.100320
9. Lerner VT, May G, Iglesia CB. Vaginal natural orifice transluminal endoscopic surgery revolution: the next frontier in gynecologic minimally invasive surgery. Jsls. 2023;27(1):
10. Baekelandt J, Stuart A, Wagenius J, et al. VaNoLaH trial: a study protocol—a multinational randomised controlled trial including two identical substudies comparing vaginal versus vNOTES (vaginal natural orifice transluminal surgery) hysterectomy or laparoscopic versus vNOTES hysterectomy. BMJ Open. 2024;14:e081979. doi:10.1136/bmjopen-2023-081979
11. Montanarella M, Boldig K, Virarkar M, et al. Intraperitoneal anatomy with the aid of pathologic fluid and gas: an imaging pictorial review. J Clin Imaging Sci. 2023;13:13. doi:10.25259/jcis_29_2023
12. Ching KC, Sumkin JH. Transvaginal drainage of pelvic abscesses and collections using transabdominal ultrasound guidance. Obstetrics Gynecol Int. 2015;2015(1):283576. doi:10.1155/2015/283576
13. Varghese JC, O’Neill M-J, Gervais DA, Boland GW, Mueller PR. Transvaginal catheter drainage of tuboovarian abscess using the trocar method. Am J Roentgenol. 2001;177(1):139–144. doi:10.2214/ajr.177.1.1770139
14. Lafans K, Culdocentesis KSJ. StatPearls. Treasure Island (FL): StatPearls Publishing, Copyright © 2025, StatPearls Publishing LLC.; 2025.
15. Lamblin G, Chene G, Mansoor A, Katuta C, Bouvet L, Nohuz E. Ectopic pregnancy management by V-NOTES technique. J Gynecol Obstet Hum Reprod. 2021;50(5):102073. doi:10.1016/j.jogoh.2021.102073
16. Cohen A, Almog B, Satel A, Lessing JB, Tsafrir Z, Levin I. Laparoscopy versus laparotomy in the management of ectopic pregnancy with massive hemoperitoneum. Int J Gynaecol Obstet. 2013;123(2):139–141. doi:10.1016/j.ijgo.2013.05.014
17. Odejinmi F, Sangrithi M, Olowu O. Operative laparoscopy as the mainstay method in management of hemodynamically unstable patients with ectopic pregnancy. J Minim Invasive Gynecol. 2011;18(2):179–183. doi:10.1016/j.jmig.2010.11.005
18. Vertongen AS, Stuart A, Stuhr Olsson K, Källén K, Baekelandt J. Ectopic pregnancies: laparoscopic versus vNOTES approach. Surgical and obstetric outcomes. Arch Gynecol Obstet. 2025;312:1117–1123. doi:10.1007/s00404-025-08098-0
19. Yoong W, Ho J, Mathieu V, Wylie S, Lodhi W, Rouabhi S. A case control study of vNOTES versus conventional laparoscopic salpingectomy for ectopic pregnancy. J Minim Invasive Gynecol. 2025;32(1):15–21. doi:10.1016/j.jmig.2024.08.016
20. Xiao X, Liu T, Li X, He L, Lin Y, Feng D. Transvaginal natural orifice transluminal endoscopic surgery for tubal ectopic pregnancy(vNOTESTEP): a protocol for a randomized controlled trial. BMC Pregnancy Childbirth. 2025;25(1):477. doi:10.1186/s12884-025-07595-z
21. Mereu L, Pecorino B, Ferrara M, et al. Cumulative sum analysis of learning curve process for vaginal natural orifice transluminal endoscopic surgery hysterectomy. J Minim Invasive Gynecol. 2023;30(7):582–586. doi:10.1016/j.jmig.2023.03.013
22. Huang L, He L, Huang L, Gan X, Lin Y, Xiong Z. Learning curve analysis of transvaginal natural orifice transluminal endoscopic hysterectomy combined under the standard operating procedure. Int J Gynaecol Obstet. 2022;159(3):689–695. doi:10.1002/ijgo.14238
23. Feng D, Liu T, Li X, et al. Learning curve analysis of transvaginal natural orifice transluminal endoscopic surgery in treating ovarian cysts: a retrospective cohort study. BMC Womens Health. 2024;24(1):424. doi:10.1186/s12905-024-03261-2
24. Ziolkowski NI, Pusic AL, Fish JS, et al. Psychometric Findings for the SCAR-Q patient-reported outcome measure based on 731 children and adults with surgical, traumatic, and burn scars from four countries. Plast Reconstr Surg. 2020;146(3):331e–8e. doi:10.1097/prs.0000000000007078
25. Herbenick D, Schick V, Reece M, Sanders S, Dodge B, Fortenberry JD. The Female Genital Self-Image Scale (FGSIS): results from a nationally representative probability sample of women in the United States. J Sex Med. 2011;8(1):158–166. doi:10.1111/j.1743-6109.2010.02071.x
26. Xu D, He L, Lin Y, et al. Does transvaginal natural orifice transluminal endoscopic surgery affect female sexual function?: a prospective cohort study. BMC Women’s Health. 2023;23(1):405. doi:10.1186/s12905-023-02566-y
27. Yoong W, Penny Z, Ho J, Ariyo O, Wylie S. Outcomes and cost-effectiveness of vNOTES vs conventional laparoscopic ovarian cystectomy for ovarian teratoma (dermoid cysts): a comparison of two minimal access routes of surgery. Eur J Obstet Gynecol Reprod Biol. 2025;312:114087. doi:10.1016/j.ejogrb.2025.114087
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multiple Spontaneous Ectopic Pregnancies Following Bilateral Salpingectomy
Al-Nuaimy Y, John J, Alhomsi SM, Al-Baghdadi OO
International Medical Case Reports Journal 2023, 16:725-729
Published Date: 7 November 2023
Spontaneous Heterotopic Pregnancy and Its Clinical Implications
Zhao Y, Bai Y, Feng C, Ke R, Lu Y
International Journal of Women's Health 2026, 18:601063
Published Date: 23 April 2026