Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Spontaneous Changes in Attentional Capabilities and Reasoning After an Alcohol Rehabilitation Treatment: Evidence About the Role of Age and Alcohol Use
Authors Fiabane E ![]() , Scarpina F, Ottonello M
, Scarpina F, Ottonello M ![]() , Pistarini C
, Pistarini C
Received 31 December 2022
Accepted for publication 30 March 2023
Published 31 May 2023 Volume 2023:19 Pages 1321—1329
DOI https://doi.org/10.2147/NDT.S403217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
Elena Fiabane,1 Federica Scarpina,2,3 Marcella Ottonello,4 Caterina Pistarini5
1Istituti Clinici Scientifici Maugeri IRCCS, Psychology Unit of Pavia Institute, Pavia, Italy; 2Rita Levi Montalcini” Department of Neurosciences, University of Turin, Turin, Italy; 3Istituto Auxologico Italiano, IRCCS, U.O. di Neurologia e Neuroriabilitazione, Ospedale S. Giuseppe, Piancavallo, VCO, Italy; 4Istituti Clinici Scientifici Maugeri IRCCS, Department of Physical and Rehabilitation Medicine of Pavia Institute, Pavia, Italy; 5Istituti Clinici Scientifici Maugeri IRCCS, Department of Neurorehabilitation of Pavia Institute, Pavia, Italy
Correspondence: Marcella Ottonello, ICS Maugeri Spa SB, via Missolungi 14, Genova, 16167, Italy, Tel +0039 01030791251, Email [email protected]
Purpose: In this study, we evaluated changes in attentional capabilities and reasoning among early abstinent alcohol-dependent individuals after a 28-day residential rehabilitation program (not including cognitive treatment). Furthermore, we explored the role of individual characteristics and disease-related factors (i.e., length of alcohol use, history of polysubstance dependence, severity of alcohol use) on spontaneous cognitive recovery.
Patients and Methods: Fifty-five patients with a diagnosis of Alcohol Use Disorder (AUD) were consecutively recruited from a residential rehabilitation hospital in Northern Italy. The majority were male (67.3%) with a mean age of 47.83 years (SD = 8.21). The computerized Psychology Experiment Building Language Test Battery was used to assess the performance at the Posner Cueing Test, Go/no-go Task, Trail Making Test (TMT), Tower of London (TOL), and Balloon Analog Risk Scale. The evaluation was performed twice: at the beginning (T0) and at its end (T1, before the hospital discharge).
Results: We observed statistically improvements over time in the performance at the: 1) TOL in the time amount required to solve the task (p < 0.001); and 2) TMT in the indexes relative to the number of errors (p = 0.003) and the total time required to solve the task (p < 0.001). Age played a significant role on the changes observed in the score relative to the time amount used by participants to solve the task in TMT (test (p = 0.03) and in TOL (p = 0.02). Moreover, the length of alcohol dependence had an effect on the change observed for the time amount to solve the TMT (time) (p = 0.01).
Conclusion: We found spontaneous recovery after alcohol detoxification on some, but not all, cognitive functions assessed in our study. The neuropsychological assessment and the identification of patients with cognitive impairment and specific risk factors (e.g., older age and longer history of alcohol use) is important to orient cognitive rehabilitation and increase the efficacy of AUD treatments.
Keywords: neuropsychological functioning, Alcohol Use Disorder, alcohol detoxification, rehabilitation, risk factors, AUD
Introduction
Alcohol Use Disorder (AUD) is a substance use disorder characterized by excessive and uncontrollable drinking that affects a person physically, emotionally, and socially.1 Crucially, AUD negatively impacts not only mental and physical health,2–4 but also multiple domains of cognitive functioning: from memory and learning capabilities, to multiple components of executive domain (i.e., working memory, problem solving and decision making, cognitive flexibility), and attentional resources (i.e., ideative speed processing and cognitive inhibition).5–7 Indeed, some cerebral areas such as frontal lobes, limbic system, and cerebellum are particularly vulnerable to damage and dysfunction associated to alcohol abuse.8–11
In this clinical condition, cognitive impairments can be moderate to severe, but their prevalence is not completely clear: mostly cognitive deficits are undiagnosed, since they are not systematically investigated in the clinical settings through appropriate neuropsychological assessment12 resulting in a possible underestimation of their prevalence. Furthermore, there are divergent findings regarding the extent to which cognitive dysfunctions may recover upon cessation of alcohol intake.13
Some studies reported short-term improvement of cognitive performance, especially in executive functions,12,14 after alcohol detoxification, in absence of specific neuropsychological treatment.15–18 Instead, other studies reported persisting cognitive difficulties, especially in visuospatial ability19 and complex executive functions,17 after 3–4 weeks of abstinence. For examples, Pitel et al (2017) observed alterations in the working memory may reduce after 18 days of detoxification; however, difficulties in cognitive inhibition persisted.20 A recent study (2020)5 found that 31.7% of early-detoxified patients with AUD undergoing alcohol detoxification showed cognitive impairments, especially in executive functions, visuospatial abilities, and memory. Furthermore, a meta-analysis7 showed that a global impairment was still present several months after alcohol detoxification and, in some cases, certain residual cognitive impairment may persist, suggesting fatal long-term negative outcomes of AUD on cerebral functioning.
Nevertheless, the role of interindividual differences, and specifically in terms of disease-related components (i.e., length of alcohol use, severity of alcohol use, length of abstinence and polysubstance comorbidity) on the neurocognitive effects of alcohol and the spontaneous cognitive recovery process were underlined, but results are mixed.15,16,21
Why the assessment of the cognitive functioning and its restoration represent an important issue in the field? Cognitive impartments may impair rehabilitation, quality of life, in terms of return-to-work, driving capacity, accidents, activities of daily living, and increased risk of relapse.22
An individual neuropsychological assessment could allow clinicians to better understand the abilities and deficits their patients may have during and after a detoxification period and to implement adapted neurocognitive treatments aimed at reducing the risk of relapse.20
The aim of this study was to evaluate changes in attentional capabilities and reasoning among early abstinent alcohol-dependent individuals, after 28-day residential treatment. Crucially, we did not deliver any cognitive treatment: thus, in this paper we verified the spontaneous recovery from cognitive difficulties. Furthermore, we explored the role of individual characteristics, such as age (since what reported by Rourke & Grant 2009; Pitel et al 2009),23,24 and relevant disease-related factors (length of alcohol dependence, previous polysubstance dependence, severity of alcohol use, according to Le Berre et al 2019; Lookatch et al 2017; Woods et al 2016)15,25,26 on spontaneous cognitive recovery.
Materials and Methods
Participants
This research was conducted in accordance with the Declaration of Helsinki and the study was approved by the Regional Ethics Committee of IRCCS AOU San Martino-IST (P.R.430REG2015). Subjects participated voluntarily; they gave informed written consent, were free to withdraw at will, and were naive to the rationale of the experiment. Moreover, they received no compensation for participating in the experiment; in fact, the Italian National Sanitary System in Italy covers all hospital charges. Because of that, a clinical trial of a rehabilitation group versus “sham rehabilitation” control group was not considered feasible and ethical. Thus, the study was conducted with a quasi-experimental pre–post design without a separate control group.
This study evaluated 65 inpatients consecutively recruited from a 28-day residential rehabilitation institute for alcohol addiction in Northern Italy across a time period of 24 months. Of the initially 65 screened patients, 10 (14%) were excluded because of exclusion criteria (n = 3), refusal to participate in the study (n = 5), or dropping out of treatment (n = 2).
Inclusion criteria to participate in the study were: 1) diagnosis of AUD according to the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5);1 2) Italian mother tongue; 3) right-handed; and 4) no actual substance use. Exclusion criteria were: 1) previous traumatic brain injury or stroke; 2) presence of dementia, evaluated with Mini Mental Examination <23.8;27 3) diagnosis of Korsakoff syndrome; and 4) severe psychiatric conditions (e.g., psychosis or suicidal ideations in the last month).
Procedure and Instruments
At hospital admission, all patients underwent a clinical assessment performed by a physician to collect relevant socio-demographic (e.g., age, educational level) and disease-related information (e.g., duration of addiction, previous polysubstance dependence). Alcohol Use Disorders Identification Test (AUDIT);28 was used to assess the severity of alcohol use in terms of alcohol consumption, drinking behaviors, and alcohol-related problems; it consists of 10 items and the total score range from 0 (absence of problem drinking behavior) to 40 (relevant problem/alcohol dependence).
Neuropsychological assessment was performed by a neuropsychologist after 7 days of detoxification using the computerized Psychology Experiment Building Language (PEBL) Test Battery.29,30 Since its first release in 2006, this computerized battery has been used to study the cognitive functioning in healthy individuals31–36 as well as in clinical samples, such as individuals with neurodegenerative disorders37 and with psychiatric diagnosis.38,39 However, to the best of our knowledge, no previous study has investigated the applicability of PEBL Test Battery in populations with AUD. We decided to adopt a computerized assessment instead of the traditional paper-and-pencil versions, since the computerized software has the advantage to increase the correctness of the data processing, limiting human errors, as well as to reduce the time spent on this process; moreover, individual’s performance is automatically scored in terms of timing and velocity,36 which is very useful in a rehabilitation context requiring multiple cognitive assessments.
In Table 1, we reported an overview of the adopted neuropsychological PEBL tests and computed scores, as well as their interpretation. Technical details about the tests, including how the scores for each index are computed, can be found online (http://pebl.sourceforge.net) and in Mueller and Piper (2014).30
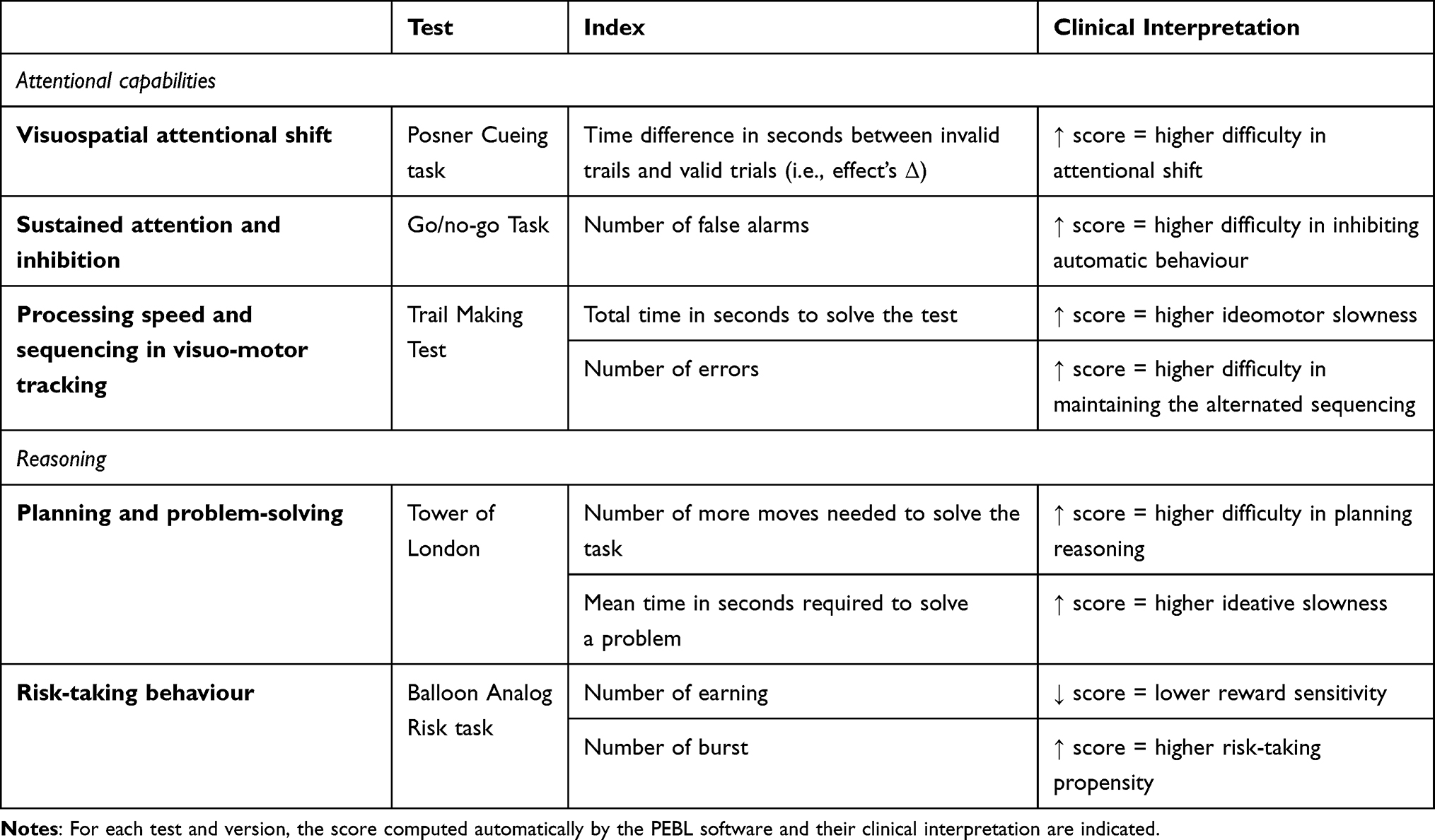 |
Table 1 Overview of the PEBL Tests Adopted |
Specifically, we adopted the Posner Cueing task (1980) to study the visuospatial attentional shift. In the task, participants have to detect a visual target, which can be proceed by a cue, which may be valid (a left or a right cue is provided, indicating where the target is likely to be) or invalid. Traditionally, participants were faster in detecting the target in the case of valid cues, but slower for the valid cue, since the cue enhances the visual processing at the cued/attended location.
We used also the go/no go task, designed according to Bezdjian et al (2009):40 this task assesses inattention and impulsivity. Specifically, it requires participants to respond to the presence of a target stimulus (e.g., a single digit or letter) amidst a stream of similar stimuli (e.g., other digits or letters). Participants have to make a motor response (button press) to one stimulus category (Go stimuli) and refrain from responding to the other (NoGo stimuli).
We included also the Trail Making Test (TMT; designed according to the Halstead–Reitan Neuropsychological Test Battery). It is a very well-known neuropsychological test used widely to assess visuo-motor attention (Trails A) and cognitive flexibility (Trails B) measuring the time amount used by the participants to connect dots that were either numbered (part A) or alternated between numbers and letters (part B).
The Tower of London (TOL) is another well-known neuropsychological test used to assess spatial planning designed originally by Shallice (1982). Specifically, in this version, designed according to Shallice (1982) participants are required to move colored balls on pegs individually from an initial state to match a goal state. Thus, optimal performance involves forming, retaining, and implementing a plan to make as few moves as possible.
Finally, the Balloon Analog Risk task is a laboratory-based behavioral measure of risk taking (i.e., the Impulsive decision making) which involves the evaluation of potential outcomes (risks or rewards) with the tendency to forego a large delayed reward in favour of a smaller immediate reward.41 Designed according to Lejuez et al42 in the task, participants are asked to pump up a series of balloons. On each trial, the larger the balloon is before the participant stops pumping, the greater the reward magnitude. However, each pump increases the likelihood that a balloon will pop, and popping results in no reward on that trial.
The order of the neuropsychological tests was randomized between participants and between conditions within the same subject, to decrease learning effects.
The neuropsychological assessment was performed twice: at the beginning of the rehabilitation after 7 days of detoxification (T0), and 3 days before hospital discharge (T1).
Treatment
The standard residential rehabilitation program in this study lasted 28 consecutive days.
The therapeutic approach is inspired by both American experience of the Minnesota Model, Croatian psychiatry studies, and finally by German and Austrian “psychosomatic clinics”.3,43,44
It consisted of a high intensity of medical and psychological treatments (cognitive behavioural treatment group, physical training, health education sessions, and skills training).3,5 Notably, no specific neuropsychological treatment was administered.
Statistical Analyses
Data have been analysed through IBM SPSS Statistics-Statistical Package for Social Sciences, version 22.0 for Windows. Descriptive statistics were used to describe the characteristics of the sample. Firstly, paired t-test was used to explore statistical difference in cognitive performance for each neuropsychological test between admission (i.e., T0) and discharge (i.e., T1). Effect size estimates (Cohen’s d) were also calculated in order to explore the magnitude of the statistical difference. Considering the presence of multiple comparisons, we applied the Bonferroni correction; thus, p value was considered significant if less than (0.05/8) = 0.006.
Secondly, for each score independently, to verify the possible role of, we performed, an analysis of covariance to assess the within-group differences over time (T0 vs. T1), while statistically controlling for the effect of the age, length of alcohol dependence, AUDIT, and polysubstance dependence on cognitive performance. Alpha level was set at 0.05.
Results
Sociodemographic and clinical aspects of the sample are shown in Table 2. The majority of the sample were male (67.3%) with a mean age of 47.83 years (SD = 8.21). Most of the participants reported a history of more than 10 years of alcohol dependence (44.4%) and no previous polysubstance abuse (58.2%).
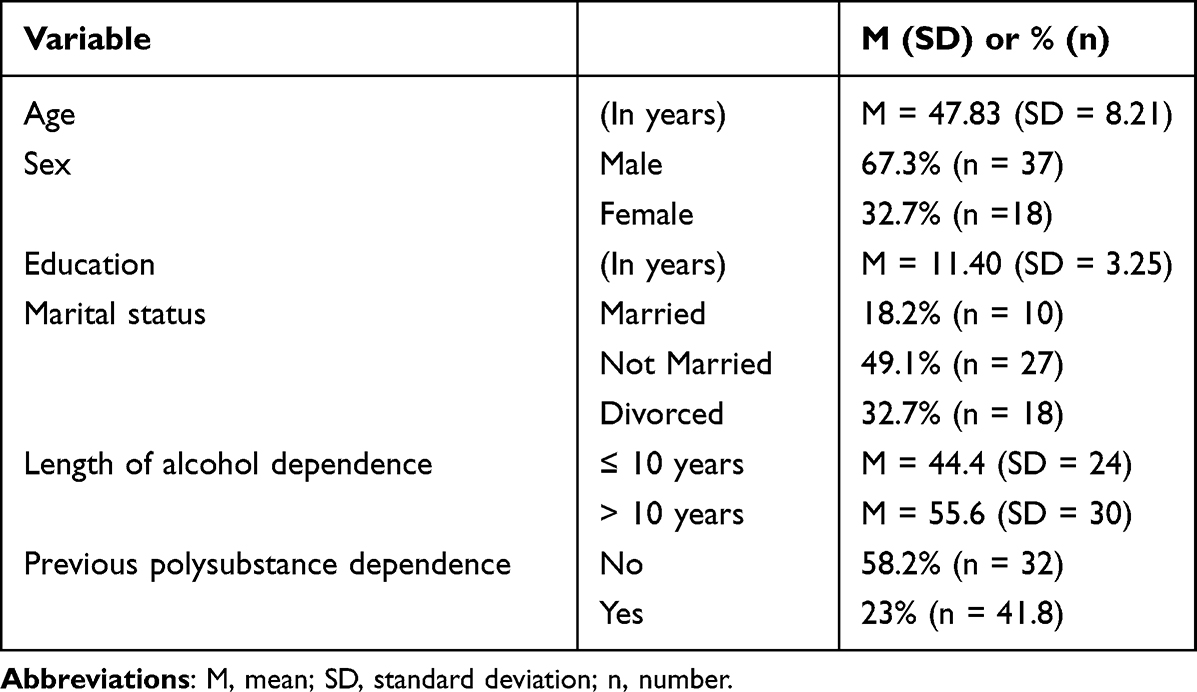 |
Table 2 Key Socio-Demographic and Disease-Related Characteristics of the Sample (N = 55) |
Cognitive Changes from Admission (T0) to Discharge (T1)
For each index of the neuropsychological test, we reported means and standard deviations together with the complete statistical results relative to the comparison between the scores at T0 (i.e., the admission) and the T1 (i.e., discharge) in Table 3.
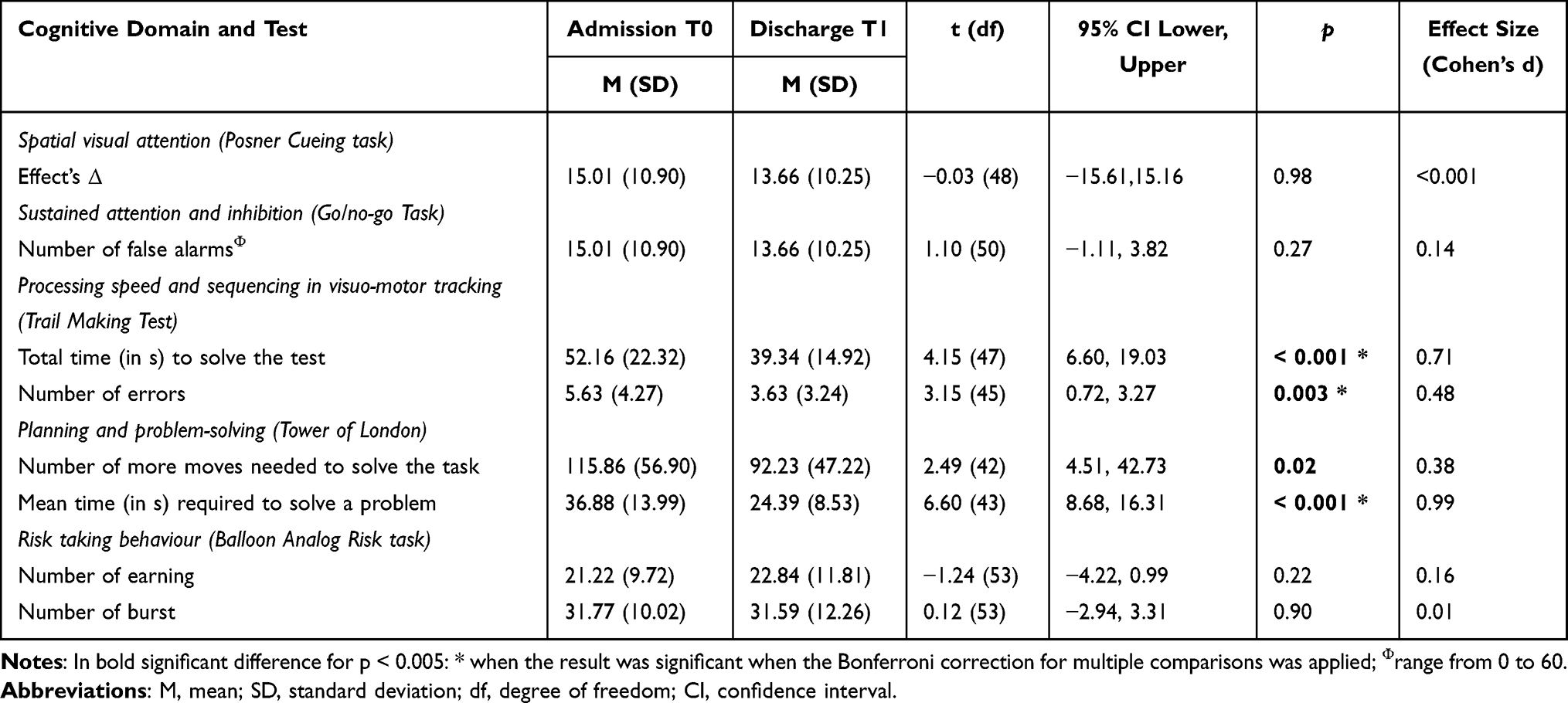 |
Table 3 Spontaneous Cognitive Changes After a 28-Day Residential AUD Treatment |
Statistically improvement over time was found in two neuropsychological tests. Specifically, at the TOL test, participants reported a lower mean time required to solve a problem (p < 0.001) with a very large effect size and a significant lower numbers of more moves needed to solve the task (p = 0.02) with a nearly small effect size; notably, this value is not significant when we considered the Bonferroni correction for multiple comparison. Moreover, we observed a significant lower amount of total time required to solve the Trial Making Test (p < 0.001) with a very large effect size and a lower number of errors (p = 0.003) with a medium effect size. No other significant difference emerged.
Effect of Covariates on Cognitive Domains
No significant effect of previous polysubstance dependence and alcohol severity on cognitive performances were observed, as reported in Table 4.
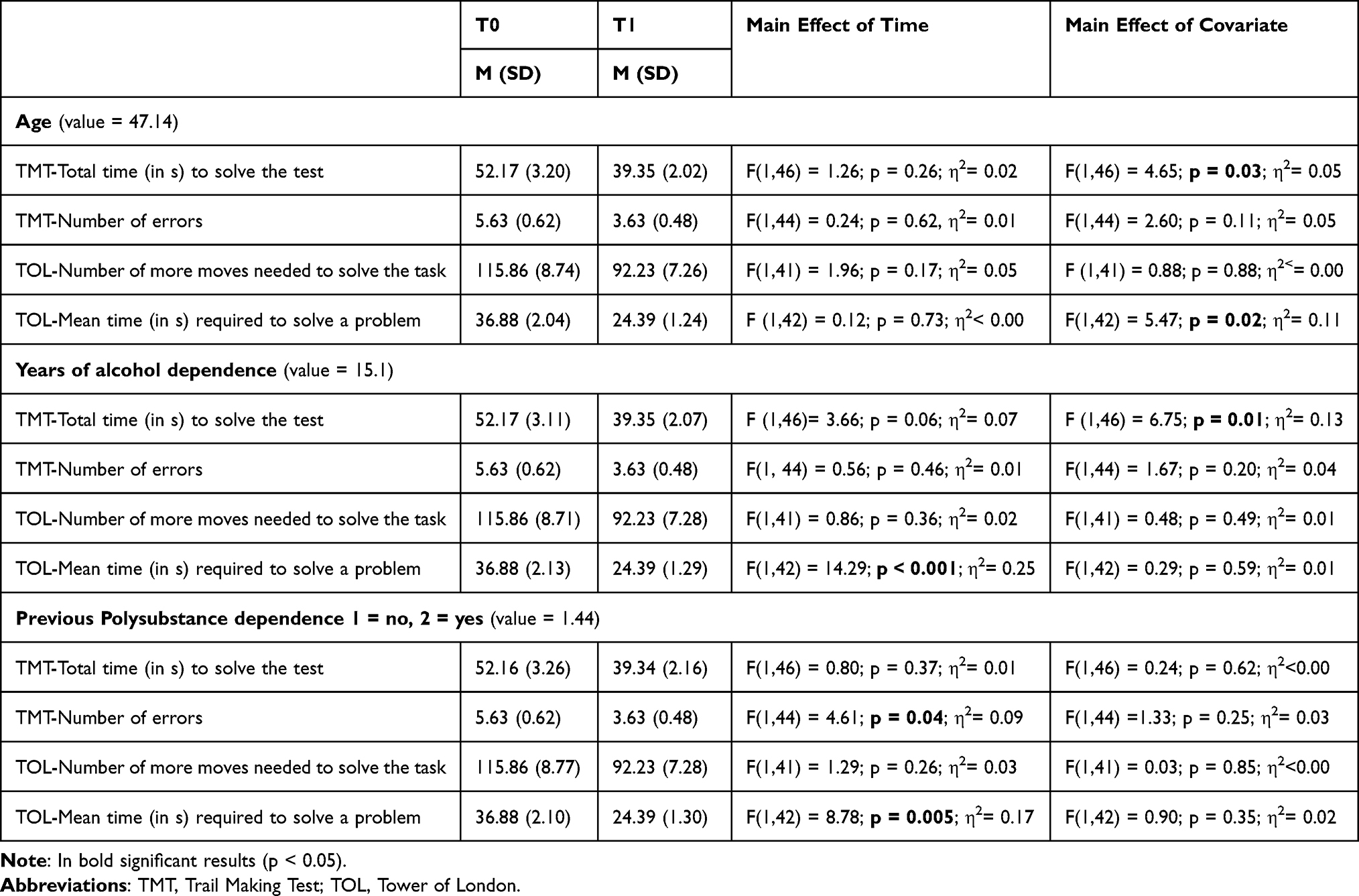 |
Table 4 Effects of Covariates on Neuropsychological Tests |
Discussion
In this study, we described positive changes in some, but not all, assessed cognitive functions, even in absence of a tailored neuropsychological treatment, after a residential rehabilitation for AUD.
Specifically, changes in cognitive performance after the treatment was observed in the neuropsychological test measuring planning and problem-solving (TOL): specifically, participants seems to be faster in their reasoning. We found similar results about the TMT, which measured processing speed and sequencing: after the rehabilitation, we observed a significant lower amount of total time required to solve the test and a lower number of errors in comparison with T0: thus, an increased performance at this test, in terms of ideo-motor velocity and sequencing, emerged. So, overall, we may observe that participants were faster in their cognitive processing after the treatment. Crucially, no other differences emerged.
The Go/No go test and Posner test measure respectively motor inhibition and attentional shift, while Balloon Analog Risk task is a behavioral measure of risk taking, impulsivity, and deficiencies in behavioral constraint. So, overall, we may suggest that higher level cognitive functions (i.e., inhibition/impulsivity) present more persistent impairment over time among patients with AUD, and they would not recover spontaneously. This is in line with previous studies suggesting that dysfunctions among certain cognitive functions (e.g., complex executive abilities) may last form many months or even years following the cessation of alcohol consumption.17,24
According to our results, two individuals’ characteristics interact with the changes observed in the cognitive functioning after the treatment. The first one was the age: spontaneous changes in processing speed and ideative/ideomotor velocity are explained by age, in line with previous studies.26 This result is not surprising considering that it is well-known that older age decreases the spontaneous brain recovery, specifically in terms of plasticity.45 Another crucial factor was the length of alcohol dependence, which is disease-specific: the shorter the length of alcohol abuse, the better the gains in ideative velocity/reasoning.15 Then, in the rehabilitative contexts, it should be considered that age as well as the length of alcohol dependence may have a significant negative effect on the cognitive outcome, suggesting the importance of early intervention in AUD.
Findings from this study also have important clinical implications for therapeutic strategies. Treatments typically were provided to patients during the first month of abstinence.3 However, normalization of certain cognitive functions may require more time, then even over the end of the rehabilitation treatments; nevertheless, in some cases, tailored cognitive rehabilitation may be necessary, specifically when the cognitive difficulties may significantly impact on individual daily-functioning or compliance to the rehabilitative treatment. Indeed, to effectively learn and apply the strategies provided by therapeutic interventions for relapse prevention, cognitive functions (i.e., attention, memory as well as executive functions) need to be functional. Cognitive domains as decision making, controlling impulsive tendencies, and risk behaviours are also necessary for maintaining abstinence.
Finally, some limitations in this study may be underlined. First, we adopted computerized neuropsychological tests; even though the methodological advantages in using them (as previously stated), on the other as in our knowledge the adopted tests do not have normative data, limiting their applicability in clinical setting. On the other hand, the role of familiarity with technologies, which may impact on the individual performance, was not directly measured; however, we underlined that the neuropsychologist was always presented during the assessment, in order to assist the participants in case of technological issue. Also, the results may be limited by the relatively small study population and their clinical heterogeneity, as well as the absence of a control group, and should be regarded with caution.
Conclusions
In this study we found that patients with AUD who underwent a 28-day rehabilitation program (not including cognitive treatment) have a spontaneous recovery in reasoning and processing speed.
On the contrary, higher level cognitive functions (i.e., inhibition/impulsivity) present more persistent impairment over time and did not recover spontaneously. Furthermore, our findings suggest that age, as well as the length of alcohol dependence, may have a significant negative effect on the cognitive outcome.
Future studies should explore the effectiveness of tailored cognitive treatments on the functions that did not show spontaneous recovery, including inhibition and attentional shift and impulsivity.
Acknowledgments
The authors thank Anna Sedda for her helpful comments on this research.
This work was partially supported by the Ricerca Corrente Funding scheme of the Italian Ministry of Health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Washington, DC: American Psychiatric Publishing; 2013.
2. Beaufort IN, De Weert-Van Oene GH, Buwalda VA, et al. The depression, anxiety and stress scale (DASS-21) as a screener for depression in substance use disorder inpatients: a pilot study. Eur Addict Res. 2017;23(5):260–268. doi:10.1159/000485182
3. Fiabane E, Ottonello M, Zavan V, Pistarini C, Giorgi I. Motivation to change and posttreatment temptation to drink: a multicenter study among alcohol-dependent patients. Neuropsychiatr Dis Treat. 2017;13:2497–2504. doi:10.2147/NDT.S137766
4. Ronksley PE, Brien SE, Turner BJ, Mukamal KJ, Ghali WA. Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. BMJ. 2011;342:d671. doi:10.1136/bmj.d671
5. Caneva S, Ottonello M, Torselli E, Pistarini C, Spigno P, Fiabane E. Cognitive impairments in early-detoxified alcohol-dependent inpatients and their associations with socio-demographic, clinical and psychological factors: an exploratory study. Neuropsychiatric Dis and Treat. 2020;16:1705–1716. doi:10.2147/NDT.S254369
6. Martelli C, Petillion A, Brunet-Lecomte M, et al. Neuropsychological impairment in Detoxified alcohol-Dependent subjects with Preserved Psychosocial Functioning. Front Psychiatry. 2017;8:193. doi:10.3389/fpsyt.2017.00193
7. Stavro K, Pelletier J, Potvin S. Widespread and sustained cognitive deficits in alcoholism: a meta‐analysis. Addict Biol. 2013;18(2):203–213. doi:10.1111/j.1369-1600.2011.00418.x
8. Oscar-Berman M, Alcohol: MK. Effects on Neurobehavioral Functions and the Brain. Neuropsychol Rev. 2007;17:239–257. doi:10.1007/s11065-007-9038-6
9. Galandra C, Basso G, Manera M, et al. Salience network structural integrity predicts executive impairment in alcohol use disorders. Sci Rep. 2018;8:14481. doi:10.1038/s41598-018-32828-x
10. Nixon K. Alcohol and adult neurogenesis: roles in neurodegeneration and recovery in chronic alcoholism. Hippocampus. 2006;16(3):287–295. doi:10.1002/hipo.20162
11. Xiao PR, Dai ZY, Zhong JG, Zhu YL, Shi HC, Pan PL. Regional gray matter deficits in alcohol dependence: a meta-analysis of voxel-based morphometry studies. Drug Alcohol Depend. 2015;153(1):22–28. doi:10.1016/j.drugalcdep.2015.05.030
12. Bernardin F, Maheut-Bosser A, Paille F. Cognitive impairments in alcohol-dependent subjects. Front Psychiatry. 2014;5:78. doi:10.3389/fpsyt.2014.00078
13. Petit G, Luminet O, Cordovil de Sousa Uva M, Zorbas A, Maurage P. Differential spontaneous recovery across cognitive abilities during detoxification period in alcohol-dependence. PLoS One. 2017;12(8):e0176638. doi:10.1371/journal.pone.0176638
14. Bartsch AJ, Homola G, Biller A, et al. Manifestations of early brain recovery associated with abstinence from alcoholism. Brain. 2007;130(1):36–47. doi:10.1093/brain/awl303
15. Lookatch SJ, Elledge LC, Anderson S, Shorey RC, Stuart GL, Tood MM. Cognitive and psychological changes during 28-day residential substance use treatment. Addict Res Theory. 2017;25(4):334–341. doi:10.1080/16066359.2017.1281408
16. Mulhauser K, Weinstock J, Ruppert P, Benware J. Changes in neuropsychological status during the initial phase of abstinence in alcohol use disorder: neurocognitive impairment and implications for clinical care. Subst Use Misuse. 2018;53(6):881–890. doi:10.1080/10826084.2017.1408328
17. Manning V, Wanigaratne S, Best D, et al. Changes in neuropsychological functioning during alcohol detoxification. Eur Addict Res. 2008;14(4):226–233. doi:10.1159/000156479
18. Angerville B, Ritz L, Pitel AL, et al. Early Improvement of Neuropsychological Impairments During Detoxification in Patients with Alcohol Use Disorder. Alcohol Alcohol. 2023;58(1):46–53. doi:10.1093/alcalc/agac048
19. Beatty WW, Hames KA, Blanco CR, Nixon SJ, Tivis LJ. Visuospatial perception, construction and memory in alcoholism. J Stud Alcohol. 1996;57(2):136–143.
20. Brion M, D’Hondt F, Pitel AL, et al. Executive functions in alcohol-dependence: a theoretically grounded and integrative exploration. Drug Alcohol Depend. 2017;177:39–47. doi:10.1016/j.drugalcdep.2017.03.018
21. Bartels C, Kunert HJ, Stawicki S, Kroener-Herwig B, Ehrenreich H, Krampe H. Recovery of hippocampus-related functions in chronic alcoholics during monitored long-term abstinence. Alcohol Alcohol. 2006;42(2):92–102. doi:10.1093/alcalc/agl104
22. Pelletier S, Nalpas B, Alarcon R, Rigole H, Perney P. Investigation of cognitive improvement in alcohol-dependent inpatients using the Montreal cognitive assessment (MoCA) score. J Addict. 2016. doi:10.1155/2016/1539096
23. Rourke SB, Grant I. The neurobehavioral correlates aof alcoholism. In: Grant I, Adams K, editors. Neuropsychological Assessment of Neuropsychiatric and Neuromedical Disorders.
24. Pitel AL, Rivier J, Beaunieux H, Vabret F, Desgranges B, Eustache F. Changes in the Episodic Memory and Executive Functions of Abstinent and Relapsed Alcoholics Over a 6-Month Period. Alcohol Clin Exp Res. 2009;33(3):490–498.
25. Le Berre AP, Laniepce A, Segobin S, Pitel AL, Sullivan EV. Alcohol use disorder: permanent and transient effects on the brain and neuropsychological functions. In: Stern RA, Alosco ML, editors. The Oxford Handbook of Adult Cognitive Disorders. Oxford, UK: Oxford University Press; 2019:302–332.
26. Woods AJ, Porges EC, Bryant VE, et al. Current heavy alcohol consumption is associated with greater cognitive impairment in older adults. Alcohol Clin Exp Res. 2016;40(11):2435–2444. doi:10.1111/acer.13211
27. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psych Res. 1985;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
28. Babor TF, De la Fuente RJ, Saunders J, et al. AUDIT: The Alcohol Use Disorders Test: Guidelines for Use in Primary Care. Geneva: World Health Organisation (WHO); 1992.
29. Mueller ST. The PEBL Manual, Version 0.13. Hillsborough: Lulu Press; 2012.
30. Mueller ST, Piper BJ. The psychology experiment building language (PEBL) and PEBL Test Battery. J Neurosci Methods. 2014;222:250–259. doi:10.1016/j.jneumeth.2013.10.024
31. Piper BJ, Li V, Eiwaz MA, et al. Executive function on the Psychology Experiment Building Language tests. Behav Res Methods. 2012;44(1):110–123. doi:10.3758/s13428-011-0096-6
32. Piper BJ, Mueller ST, Geerken AR, et al. Reliability and validity of neurobehavioral function on the Psychology Experimental building language Test Battery in young adults. PeerJ PrePrints. 2015;3:e1460. doi:10.7717/peerj.1460
33. Piper B, Mueller ST, Talebzadeh S, Ki MJ. Evaluation of the validity of the Psychology Experiment Building Language tests of vigilance, auditory memory, and decision making. PeerJ PrePrints. 2016;15(4):e1772. doi:10.7717/peerj.1772
34. Schoene D, Valenzuela T, Toson B, et al. Interactive cognitive-motor step training improves cognitive risk factors of falling in older adults: a randomized controlled trial. PLoS One. 2015;10(12):e0145161. doi:10.1371/journal.pone.0145161
35. Stuhr C, Hughes CML, Stöckel T. Task-specific and variability-driven activation of cognitive control processes during motor performance. Sci Rep. 2018;8(1):10811. doi:10.1038/s41598-018-29007-3
36. Scarpina F, D’Agata F, Priano L, Mauro A. Difference between young and old adults’ performance on the psychology experiment building language (PEBL) test battery: what is the role of familiarity with technology in cognitive performance? Assessment. 2021;28(6):1723–1734. doi:10.1177/1073191120918010
37. Peterson DS, Fling BW, Mancini M, Cohen RG, Nutt JG, Horak FB. Dual-task interference and brain structural connectivity in people with Parkinson’s disease who freeze. J Neurol Neurosurg Psychiatry. 2015;86(7):786–792. doi:10.1136/jnnp-2014-308840
38. Firth J, Stubbs B, Teasdale SB, et al. Diet as a hot topic in psychiatry: a population-scale study of nutritional intake and inflammatory potential in severe mental illness. World Psychiatry. 2018;17(3):365–367. doi:10.1002/wps.20571
39. Baune BT, Air T. Clinical, Functional, and Biological Correlates of Cognitive Dimensions in Major Depressive Disorder – rationale, Design, and Characteristics of the Cognitive Function and Mood Study (CoFaM-Study). Front Psychiatry. 2016;7:150. doi:10.3389/fpsyt.2016.00150
40. Bezdjian S, Baker LA, Lozano DI, Raine A. Assessing inattention and impulsivity in children during the Go/NoGo task. Br J Dev Psychol. 2009;27(2):365–383. doi:10.1348/026151008X314919
41. Madden GJ, Bickel WK, Eds. Impulsivity: The Behavioral and Neurological Science of Discounting. Washington (DC): American Psychological Association (APA); 2010. doi:10.1037/12069-000.
42. Lejuez CW, Read JP, Kahler CW, et al. Evaluation of a behavioral measure of risk-taking: the Balloon Analogue Risk Task (BART). J Exp Psychol Appl. 2002;8(2):75–84. doi:10.1037//1076-898x.8.2.75
43. Anderson DJ, McGovern JP, DuPont RL. The origins of the Minnesota model of addiction treatment – a first person account. J Addict Dis. 1999;18(1):107–114. doi:10.1300/J069v18n01_10
44. Hodolin V, Corlito G. Psichiatria, Alcologia, Riabilitazione. Trento: Centro Studi Erickson; 1996.
45. Johnston MV. Plasticity in the developing brain: implications for rehabilitation. Dev Disabil Res Rev. 2009;15(2):94–101. doi:10.1002/ddrr.64
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.