Back to Journals » Vascular Health and Risk Management » Volume 18
Spontaneous Bilateral Basal Ganglia Hemorrhage Due to Severe Hypertension
Authors Sheikh Hassan M ![]() , Mohamed Ali A, Farah Osman M
, Mohamed Ali A, Farah Osman M ![]() , Ahmed A
, Ahmed A
Received 16 February 2022
Accepted for publication 4 July 2022
Published 6 July 2022 Volume 2022:18 Pages 473—477
DOI https://doi.org/10.2147/VHRM.S362059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Mohamed Sheikh Hassan, Abdiladhif Mohamed Ali, Mohamed Farah Osman, Abdulkadir Ahmed
Department of Neurology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Sheikh Hassan, Email [email protected]
Introduction: The basal ganglia, which comprise many subcortical nuclei, constitute an integrated functional unit of the brain. Spontaneous hemorrhage of the basal ganglia is mostly unilateral and secondary to uncontrolled hypertension. Simultaneous bilateral basal ganglia hemorrhage (SBBGH) is very rare. So far, only 40 cases have been documented so far.
Case Presentation: Here, we report a 37-year-old man with a past medical history of uncontrolled hypertension who was brought to the emergency department due to severe headache, worsening confusion, and right-sided weakness for 2 days. An urgent non-contrast brain CT performed immediately revealed bilateral intracerebral hemorrhage (ICH) of the same age in the basal ganglia. On admission, blood pressure was 220/120. Other vital signs were normal. The patient was admitted to the ICU, IV antihypertensive and antiedema medications were given. After clinical improvement, he was transferred to the neurology ward on the fifth day. After another 5 days in the neurology inpatient ward, the patient clinically improved and was referred to the rehabilitation department.
Conclusion: Due to the rarity of SBBGH, it is particularly interesting to report this remarkable case of a man with simultaneous spontaneous bilateral ganglia hemorrhage secondary to uncontrolled hypertension.
Keywords: uncontrolled hypertension, bilateral basal ganglia, hemorrhagic stroke
Background
Simultaneous non-traumatic bilateral basal ganglia hemorrhage (SBBGH) is a very rare entity. The majority of the cases of basal ganglia hemorrhage are unilateral and mostly secondary to poorly controlled hypertension.1 The predisposing factors and pathophysiological processes leading to the development of simultaneous bilateral basal ganglia are not well known. However, several pathophysiologic processes have been proposed, such as direct current thermal effects, induced current electrolytic effects, mechanical harm from lightning, and acute severe hypertension caused by abrupt peripheral vascular contraction.2 Hypertension-induced SBBGH is frequently the result of a long history of poorly treated hypertension. Hypertension damages the vascular wall, causing microaneurysms to form. SBBGH is caused by the rupture of these microaneurysms on the lenticulostriate and thalamo-perforating arteries at the same time.3 Due to the rarity of SBBGH, it is particularly interesting to report this remarkable case of a man with simultaneous spontaneous bilateral ganglia hemorrhage secondary to uncontrolled hypertension.
Case Presentation
A 37-year-old man with a past medical history of poorly controlled hypertension was brought to the emergency department due to severe headache, worsening confusion, and right-side weakness for 2 days. On examination, the patient was in a stuporous condition with a Glasgow coma scale of 8/15 (eye-opening 2, verbal response 2, motor response 4). He had right-side weakness and mixed aphasia (global aphasia with preserved repetition), muscle strength was 0/5 in the right. Pupils were symmetrically equal to normal size and reactive to light. He had no other significant past medical or surgical history. He had no family history of diabetes, hypertension, coagulopathy or any neurological disease. The patient had no history of drug abuse, anticoagulation or trauma.
A non-contrast brain CT was obtained, which demonstrated bilateral basal ganglia hemorrhage (BBGH). Hematoma measured 5x3cm in the left basal ganglia and 3x1cm in the right basal ganglia (see Figures 1 and 2). A subsequent brain MRI later revealed a bilateral basal ganglia hematoma with minimal edema (3.5 cm in the left and 2 cm in the right basal ganglia) (Figures 3 and 4). MR angiography (MRA) was negative for aneurysmal rupture. On admission, blood pressure was 220/120. Other vital signs were normal. The patient’s complete blood count, comprehensive biochemistry profile, and coagulation markers were all within normal limits. An ECG showed a normal sinus rhythm. A chest x-ray and CT scan did not reveal any acute cardiopulmonary disease. The patient was admitted to the ICU and conservatively managed with blood pressure-lowering drugs, mannitol (5 days) and other supportive medications. After 2 days, Glasgow coma scale of the patient improved from 8 to 11 (eye-opening 4, verbal response 3, motor response 4), blood pressure was controlled with multiple antihypertensive medications; and he was transferred to the neurology ward on the fifth day.
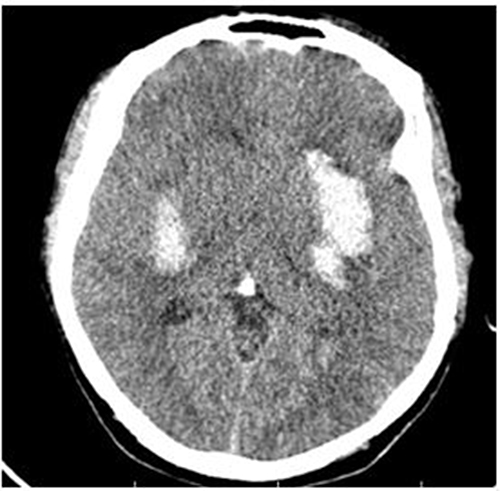 |
Figure 1 Brain CT axial view showing acute bilateral basal ganglia hemorrhage. |
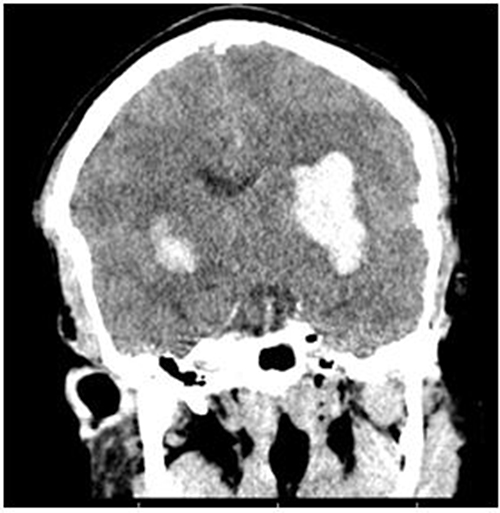 |
Figure 2 Brain CT Coronal view showing acute bilateral basal ganglia hemorrhage. |
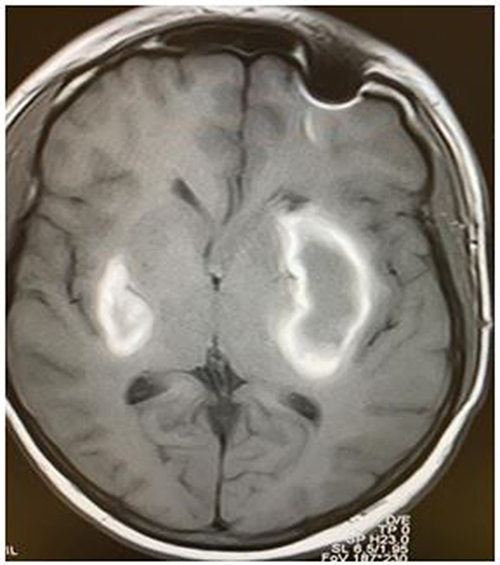 |
Figure 3 Brain MRI T1 axial view showing bilateral basal ganglia hemorrhage after 10 days of admission. |
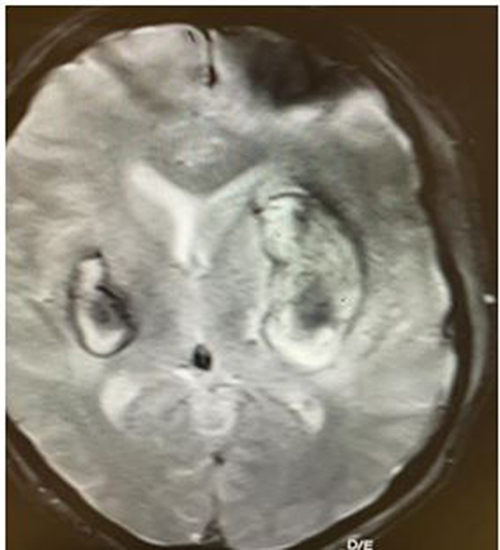 |
Figure 4 Brain MRI gradient echo showing bilateral basal ganglia hemorrhage after 10 days of admission. |
After another 5 days of neurology inpatient unit, the patient clinically improved (GCS 14/15) and was referred to the rehabilitation department.
Discussion
Hemorrhagic stroke is the second main cause of stroke after cerebral infarction. It accounts for about 10–15% of all strokes. Hypertension is considered the most important risk factor for intracerebral hemorrhage, which frequently results in a unilateral hematoma. Around 35–44% of hypertensive ICH cases are caused by bleeding in the basal ganglia or thalamus.4
Multiple simultaneous ICH has been documented in 2% of all hemorrhagic strokes. Hypertension-related multiple ICH, on the other hand, is unusual. Only 40 cases of spontaneous bilateral intracerebral hemorrhage have been recorded in the medical literature. The majority of reported cases were treated conservatively and had a bad outcome.5
Bilateral basal ganglia hemorrhages have been linked to trauma, methanol poisoning, diabetic ketoacidosis, hyperglycemic hyperosmolar syndrome, lighting, uncontrolled hypertension, anticoagulant use, and fungal infection6,7 The patient’s history was significant only for uncontrolled hypertension in which he had poor compliance with the medication. There was no history of trauma, coagulopathy, diabetes, or infections. Hypertension was considered to be the underlying etiology since there was no other identified etiology or risk factor. The location of the hematoma was also typical for hypertension-related intracerebral hemorrhage.
One pathologic process is that rupture of bilateral intracerebral microaneurysms can abruptly occur, and hemodynamic instability may occur as a result of the initial hemorrhage induced by a ruptured microaneurysm. (eg, reflex blood pressure elevation and collateral circulation abnormalities) and structural derangement, causing rupture of other microaneurysms.8 Poisoning, metabolic disorders, vascular diseases, degenerative diseases, inflammatory and cerebral amyloid angiopathy, which put patients at risk for repeated spontaneous intracerebral hemorrhages, are all potential risk factors for bilateral abnormalities of the basal ganglia.9,10 Our patient had no metabolic, inflammatory, vascular, or trauma history. The only risk factor identified was uncontrolled hypertension. The patient was admitted to the ICU and conservatively managed with blood pressure-lowering drugs, mannitol, and other supportive medications. After five days of ICU treatment, he was transferred to the neurology ward, where he spent time until he was good enough to be transferred to rehabilitation.
Conclusion
The occurrence of simultaneous bilateral basal ganglia hemorrhage is unusual. In the medical literature, only 40 cases have been reported. Severe uncontrolled hypertension has been suggested as one of the etiologies. In this case, we present a rare example of bilateral basal ganglia hemorrhage caused by uncontrolled hypertension.
Abbreviations
SBBGH, simultaneous bilateral basal ganglia hemorrhage; ICH, intracerebral hemorrhage; BBGH, bilateral basal ganglia hemorrhage.
Ethics and Consent
Informed Consent: Written informed consent was obtained from the patient for publication of this case report and the accompanying images. In our institution, ethical approval is not required for case reports.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Terzi M, Akkaya O, Onar M. Pure sensory stroke due to bilateral basal ganglion hemorrhage: a case report. Turk Neurosurg. 2010;20(3):406–408. doi:10.5137/1019-5149.JTN.1891-09.1
2. Stanley LD, Suss RA. Intracerebral hematoma secondary to lightning stroke: case report and review of the literature. Neurosurgery. 1985;16(5):686–688. doi:10.1227/00006123-198505000-00020
3. Yen CP, Lin CL, Kwan AL, et al. Simultaneous multiple hypertensive intracerebral haemorrhages. Actaneurochirurgica. 2005;147(4):393–399.
4. Laiwattana D, Sangsawang B, Sangsawang N. Primary multiple simultaneous intracerebral hemorrhages between 1950 and 2013: analysis of data on age, sex and outcome. Cerebrovasc Dis Extra. 2014;4(2):102–114. doi:10.1159/000362111
5. Takeuchi S, Takasato Y, Masaoka H, Hayakawa T, Yatsushige H, Sugawara T. Simultaneous multiple hypertensive intracranial hemorrhages. J Clin Neurosci. 2011;18(9):1215–1218. doi:10.1016/j.jocn.2011.01.020
6. Verma A. Bilateral basal ganglionic hemorrhage. Arch Neurol. 2006;63(3):464. doi:10.1001/archneur.63.3.464
7. Sato M, Tanaka S, Kohama A, Sone T, Fukunaga M, Morita R. Spontaneous bilateral intracerebral hemorrhage occurring simultaneously case report. Neurol Med Chir. 1986;26(7):545–547. doi:10.2176/nmc.26.545
8. Kabuto M, Kubota T, Kobayashi H, Nakagawa T, Arai Y, Kitai R. Simultaneous bilateral hypertensive intracerebral hemorrhages—two case reports. Neurol Med Chir. 1995;35(8):584–586. doi:10.2176/nmc.35.584
9. Seo JS, Nam TK, Kwon JT, Park YS. Multiple spontaneous simultaneous intracerebral hemorrhages. J Cerebrovasc Endovasc Neurosurg. 2014;16(2):104–111. doi:10.7461/jcen.2014.16.2.104
10. Asimi R, Wani M, Ahmad F. Bilateral simultaneous hypertensive intracerebral hemorrhage in both putamen. Ann Indian Acad Neurol. 2007;10(4):272. doi:10.4103/0972-2327.37824
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.