Back to Journals » Vascular Health and Risk Management » Volume 15
Splanchnic Vein Thrombosis: Current Perspectives
Authors Valeriani E ![]() , Riva N
, Riva N ![]() , Di Nisio M, Ageno W
, Di Nisio M, Ageno W
Received 27 June 2019
Accepted for publication 2 October 2019
Published 22 October 2019 Volume 2019:15 Pages 449—461
DOI https://doi.org/10.2147/VHRM.S197732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Takashi Kajiya
Emanuele Valeriani,1 Nicoletta Riva,2 Marcello Di Nisio,1 Walter Ageno3
1Department of Medicine and Ageing Sciences, University G. D’Annunzio, Chieti-Pescara, Italy; 2Department of Pathology, Faculty of Medicine and Surgery, University of Malta, Msida, Malta; 3Department of Medicine and Surgery, University of Insubria, Varese, Italy
Correspondence: Nicoletta Riva
Department of Pathology, Faculty of Medicine and Surgery, University of Malta, Msida, MSD 2080, Malta
Tel +356 2545 2518
Fax +356 2545 0000
Email [email protected]
Abstract: Splanchnic vein thrombosis (SVT) including portal, mesenteric, splenic vein thrombosis and the Budd-Chiari syndrome, is a manifestation of unusual site venous thromboembolism. SVT presents with a lower incidence than deep vein thrombosis of the lower limbs and pulmonary embolism, with portal vein thrombosis and Budd-Chiari syndrome being respectively the most and the least common presentations of SVT. SVT is classified as provoked if secondary to a local or systemic risk factor, or unprovoked if the causative trigger cannot be identified. Diagnostic evaluation is often affected by the lack of specificity of clinical manifestations: the presence of one or more risk factors in a patient with a high clinical suspicion may suggest the execution of diagnostic tests. Doppler ultrasonography represents the first line diagnostic tool because of its accuracy and wide availability. Further investigations, such as computed tomography and magnetic resonance angiography, should be executed in case of suspected thrombosis of the mesenteric veins, suspicion of SVT-related complications, or to complete information after Doppler ultrasonography. Once SVT diagnosis is established, a careful patient evaluation should be performed in order to assess the risks and benefits of the anticoagulant therapy and to drive the optimal treatment intensity. Due to the low quality and large heterogeneity of published data, guidance documents and expert opinion could direct therapeutic decision, suggesting which patients to treat, which anticoagulant to use and the duration of treatment.
Keywords: Budd-Chiari syndrome, mesenteric vein thrombosis, portal vein thrombosis, splanchnic vein thrombosis, splenic vein thrombosis
Introduction
Splanchnic vein thrombosis (SVT) refers to thrombosis occurring in the splanchnic venous circulation, which drains the digestive system from the lower oesophagus to the upper two-thirds of the rectum.1 SVT encompasses portal vein thrombosis (PVT), mesenteric veins thrombosis (MVT), splenic vein thrombosis and the Budd-Chiari syndrome (BCS). The BCS includes any obstruction of the hepatic venous outflow located between the small hepatic venules and the confluence of the inferior vena cava into the right atrium.2 Thrombosis of the extrahepatic portal axis with possible extension to other splanchnic veins is sometimes referred under the term extrahepatic portal vein obstruction (EHPVO), although EHPVO can also include other mechanisms of portal vein obstruction (e.g. neoplastic infiltration).2,3
Epidemiology
SVT is an unusual manifestation of venous thromboembolism (VTE). While usual site VTE, i.e. deep vein thrombosis of the lower limbs and pulmonary embolism, occur in about 70–270 cases per 100,000 person-years,4 the incidence of SVT is at least 25 times lower. Furthermore, a high variability in the incidence of SVT has been reported which may depend on the type of data source, differences in diagnostic tests, site or type of SVT -incidental or symptomatic- considered.5
PVT is the most frequent type of SVT. A prevalence of 1.0% was reported in a large population study evaluating more than 23,000 consecutive autopsies,6 while an incidence of 3.7 cases per 100,000 person-years was reported in a large multicentre Swedish study.7
BCS is the least common manifestation of SVT, with reported incidence rates of around 1–2 cases per million inhabitants per year.8,9 The estimated prevalence of BCS varies across different countries, ranging from around 1–4 cases per million inhabitants in the West10,11 up to 5–7 cases per million inhabitants in the East.12,13
Age and sex distribution of SVT is heterogeneous, with some differences based on the site of thrombosis. Patients with BCS tend to be the youngest especially in Asian countries, where incidence peaks between 20 and 40 years.14,15 Although this difference is less pronounced in Western countries, BCS patients are still approximately one decade younger than PVT patients (for instance 50 vs 61 years, or 45 vs 54 years, respectively, in the Italian and US cohorts).9,16 Conversely, the incidence of MVT is higher around 70–79 years.17,18
Approximately two thirds of SVT patients are men.9,16,19 Recent data from hospital admissions in North-western Italy documented an annual incidence of PVT of 3.78 and 1.73 cases per 100,000 inhabitants in men and women, respectively.9 BCS showed a predominance of women (52-69%) in Western studies,11,20 whereas a slight predominance of men was reported in Asian studies.12,13 This finding can reflect the different pathogenesis of BCS, being hormonal factors more frequent in the West and membranous web obstruction in the East.2
Risk Factors
Identification of the causative trigger allows the classification of SVT as provoked or unprovoked, based on the presence or absence of a local or systemic risk factor (Table 1).21 The variable prevalence of risk factors among patients with SVT may be explained by differences in study populations. In unselected cohorts of SVT patients, the major risk factors are liver cirrhosis and solid cancer, each responsible for about 25% of cases, while unprovoked SVT represents 15% to 27% of all SVTs.16,19
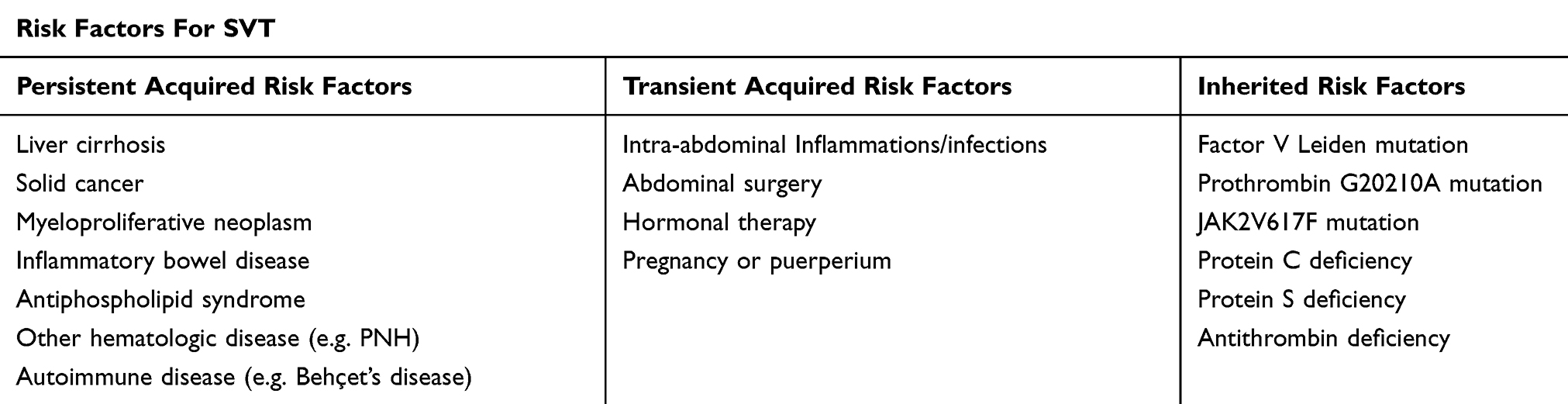 |
Table 1 Risk Factors For Splanchnic Vein Thrombosis |
Cirrhotic patients present both a pro-coagulant status and portal axis hemodynamic alterations which may favour the occurrence of SVT. Recent data showed that patients with liver cirrhosis are not naturally “anticoagulated” as previously believed, and may be at increased risk of thrombosis due to an acquired pro-thrombotic status related to high factor VIII/protein C ratio, increased thrombin generation, and alteration in fibrin clot structure.22–24 Additionally, reduced portal flow can contribute to PVT development.25 Results of clinical studies confirmed these experimental data showing an increased VTE risk and a prevalence of PVT of about 10% in cirrhotic patients.26–28
The association between solid cancer and VTE can be explained by cancer-related haemostatic system alterations and other risk factors frequently associated with cancer, such as immobilization, surgery, chemotherapy, and central venous catheter.29–32 The prevalence of cancer-related SVT is low in outpatients (about 1%),33 with liver (26%) and pancreatic (11%) cancers being the most common neoplasms.34 Furthermore, 15% of patients with SVT receive a diagnosis of solid cancer after a median follow-up of 1.6 years,34 suggesting that, as usual sites VTE,35 SVT may be an early marker of cancer.
Patients with myeloproliferative neoplasms (MPN) show an increased risk for both arterial and venous thrombosis.36,37 The incidence of SVT is higher in MPN (from 1% to about 20%)38 than in the general population,21 and about 10% of all SVT are MPN-related.16,19 The pathogenesis of thrombosis in MPN is a complex and multifactorial process involving quantitative and qualitative alterations of platelet, erythrocytes, leukocytes, and endothelial cells.36 The V617F substitution of the Janus Kinase 2 (JAK2) gene showed a strong association with MPN and SVT.39,40 The prevalence of JAK2V617F mutation is higher in SVT (32.7%) compared with usual sites VTE (0.88%), cerebral vein thrombosis (2.57%) or retinal vein occlusion (0.99%).19,41 Furthermore, this mutation was found in 94.7% of patients with unusual site thrombosis (cerebral and SVT) and overt MPN.40 From a pathophysiologic point of view, the JAK2V617F mutation seems to promote thrombosis through P-selectin overexpression leading to platelet aggregation and fibrin deposition.42,43
Hormonal therapy, abdominal surgery (e.g. splenectomy, liver transplantation and bariatric surgery), inflammatory bowel diseases (Crohn’s disease and ulcerative colitis), pregnancy or puerperium are responsible for the majority of the remaining cases of SVT.16,19 Furthermore, intra-abdominal infections (e.g. diverticulitis, appendicitis, pancreatitis) due to anaerobes, aerobic bacteria or fungi may cause pylephlebitis.44 Other rare causes of SVT are paroxysmal nocturnal hemoglobinuria and Behçet’s disease.21
Thrombophilia may be an additional risk factor, although low levels of anticoagulant proteins are generally related to an impaired liver production.45 The prevalence of significant thrombophilia (mainly factor V Leiden, prothrombin G20210A, and JAK2V617F mutations) is higher in SVT (12.3%) than usual site VTE (8.5%).46 In particular, BCS, MVT and multiple veins thrombosis show the highest rate of pro-thrombotic alterations.19,46 Finally, one third of patients with SVT present with more than one risk factor, reflecting the multifactorial aetiology of SVT.47
Specific venous involvement in SVT shows some peculiarities based on the associated risk factors. While about 90% of cirrhosis-related SVT involve the portal vein,48 cancer-related SVT involves the portal, splenic, and superior mesenteric veins in 48%, 42%, and 21% of cases, respectively.49 In patients with MPN, PVT is the most common type of SVT (about 60%);50 however, the prevalence of BCS is higher in MPN patients (approximately 17% of MPN-related SVT are BCS,50 while <10% of BCS were reported among all SVT).16,19 Nearly half of patients with pancreatitis show splenic vein involvement.16 Multiple vessels thrombosis is reported in approximately a fifth of patients with cancer (24%), cirrhosis (22%), and MPN (17%).16
Clinical Presentation
Clinical manifestations of SVT are nonspecific. The most common symptom is abdominal pain, reported in approximately half of SVT patients, followed by gastrointestinal bleeding and ascites.16,19 Other nonspecific symptoms are nausea, vomiting, anorexia, diarrhoea or constipation, and fever. In up to one third of patients, SVT can be asymptomatic or incidentally detected during abdominal imaging performed for other reasons, such as follow-up of cancer or cirrhosis.51,52 However, each site of thrombosis can manifest with a specific clinical scenario.21
Portal Vein Thrombosis
PVT can be acute or chronic.53 Acute PVT is characterised by the sudden onset of abdominal pain, whereas signs of portal hypertension (such as hypersplenism, ascites, oesophageal varices, and the presence of portal cavernoma or other porto-systemic collateral veins on imaging) are typical manifestations of chronic PVT.
Mesenteric Vein Thrombosis
MVT can present an acute, subacute or chronic course.54 Acute MVT is characterised by the sudden onset of abdominal pain and is complicated by intestinal infarction in one third of patients.17 Abdominal pain lasting for several days without intestinal infarction is more typical of subacute MVT, while signs of portal hypertension identify chronic MVT.54 MVT has a 30-day mortality rate of 20%, mainly due to bowel infarction.17
Splenic Vein Thrombosis
Data on isolated splenic vein thrombosis are scarce. The most common symptom is abdominal pain, reported in 57% of patients, followed by gastrointestinal bleeding (29%) and nausea (23%).16 Up to 17% of patients can be asymptomatic.16
Budd-Chiari Syndrome
BCS can be fulminant, acute, subacute or chronic.53 Patients with BCS typically present with a triad of abdominal pain, ascites, and hepatomegaly. In fulminant BCS, the rapid onset of hepatocellular necrosis may lead to acute liver failure within few days, while chronic BCS generally presents with signs of portal hypertension.55
Diagnosis
The diagnosis of SVT relies on imaging. D-dimer, a well-known biomarker for deep vein thrombosis and pulmonary embolism, has limited utility in this setting. Although some studies showed that mean D-dimer values are increased in SVT patients,56,57 D-dimer can also be elevated in other conditions, such as liver cirrhosis or hepatocellular carcinoma, which reduces its diagnostic predictive value.58 Recent data suggested that D-dimer levels may predict the development of multi-organ dysfunction and short-bowel syndrome after acute MVT.59
Angiography was the gold standard for SVT diagnosis, but it is an invasive examination and rarely performed nowadays. Doppler ultrasonography (DUS) has become the first line diagnostic test with a sensitivity of 89-93% and a specificity of 92-99% for PVT.60 DUS is also very accurate for BCS since it can directly visualise the intra- and supra-hepatic veins and the inferior vena cava, the typical intrahepatic collaterals, and the texture of the liver parenchyma.61 The sensitivity of DUS is lower for the mesenteric veins, due to the bowel gas which can interfere with their visualisation,62 and for the splenic vein, due to the presence of several collaterals near the splenic hilum.63
Computed tomography (CT) angiography and magnetic resonance (MR) angiography are nowadays the standard imaging for MVT, since they can better visualise the mesenteric veins and show signs of intestinal infarction.64 They can also be used in patients with suspected PVT or BCS, when the DUS is not diagnostic or to complete information from DUS.65 CT angiography is faster and widely available, but involves ionizing radiations and the iodinated contrast agent can cause allergic reactions or renal toxicity. MR angiography is used for patients with contraindications to CT angiography, since the scanning time is longer (30–60 mins) and has lower spatial resolution.60 Liver biopsy is usually not needed, except to confirm rare forms of BCS involving only the small intrahepatic veins or to exclude other hepatic disorders, such as the veno-occlusive disease.65,66
Distinguishing acute or recent PVT from chronic PVT represents a difficult but relevant challenge with therapeutic implications. Acute PVT is visualised as hyperechoic material into an enlarged vein with partial or total absence of vascular flow on DUS or as hyperattenuating material without luminal contrast enhancement on CT. Portal cavernoma, easily detected by both DUS and CT, is the main sign of chronic thrombosis and is defined as the presence of multiple small collaterals around the PVT.67,68 In doubtful cases, the clinical presentation, the absence of collateral circulation, and the absence of SVT in previous exams could help establishing the diagnosis of acute/recent SVT.68
Treatment
During the last few years, a large number of observational studies tried to evaluate the safety and efficacy of anticoagulant treatment in patients with SVT. The paucity and variability of available data in terms of type, dose, and duration of anticoagulant therapy can be explained by the relative rarity, extreme clinical variability, and challenging diagnostic evaluation of SVT. All these aspects may have contributed to the heterogenous level of evidence and grade of recommendations in published guidelines.2,3,69–71 Furthermore, “real world” patients are often more complex compared to the typical cases considered by the guidelines and require a careful evaluation of the risk-to-benefit balance of the anticoagulant treatment.
Pre-Treatment Evaluation
Before starting anticoagulant treatment, physicians need to carefully evaluate the bleeding risk which is mainly related to portal hypertension complications, such as ascites, varices, or gastro-intestinal bleeding at clinical presentation.68,72,73 The presence of oesophageal varices is an independent risk factor for major bleeding,72,73 thus an upper endoscopy to grade and eventually treat oesophageal varices should be considered before starting the anticoagulant therapy, especially in patients with liver cirrhosis and chronic SVT.21,68 The presence of oesophageal varices should not necessarily contraindicate or defer anticoagulant therapy which can improve the portal hypertension, as long as appropriate prophylactic measures are taken (beta-blockers or endoscopic treatment).69 However, since endoscopic band ligation can require multiple sessions, in patients without active bleeding, an initial treatment with reduced or prophylactic doses of low molecular weight heparin (LMWH) could be considered.74
Who Should Be Treated?
Treatment of acute SVT aims to achieve vessel recanalization and avoid complications, such as bowel ischemia or chronic portal hypertension.67 Therefore, starting anticoagulant therapy in acute symptomatic SVT without absolute contraindications is strongly recommended.2,3,69 Prevention of thrombosis progression or recurrence is the main goal of anticoagulant therapy in patients with chronic SVT, especially those with persistent risk factors. However, several areas of uncertainty still exist in the treatment of chronic SVT.67,75
The 9th edition of the American College of Chest Physician (ACCP) guidelines strongly recommend anticoagulant therapy in symptomatic patients. Conversely, no treatment is suggested for incidentally detected SVT, possible exceptions being acute and extensive SVT, progression of previous known thrombosis, and ongoing chemotherapy in cancer patients.69 Additional information on incidental SVT derived from the results of two recent large cohort studies. In the International Registry on SVT (IRSVT), the prognosis of incidentally detected SVT was comparable to symptomatic SVT,19,51 similarly to previous data on VTE at usual sites.76 Although the use of anticoagulant treatment was significantly lower in patients with incidentally detected SVT (64%) compared with symptomatic patients (84%), the incidence of thrombotic events was not negligible. An overall incidence rate of thrombotic events 8.0 (95% CI, 5.2–12.1) and 7.0 (95% CI, 5.2–9.3) per 100 person-year was reported in incidentally detected and symptomatic SVT, respectively. In particular, untreated incidental SVT had an incidence rate of 11.5 events (95% CI, 6.2 to 21.3).51 Similar results came from the “Registro Informatizado Enfermedad Trombo Embólica” (RIETE) registry where patients with incidentally detected SVT presented a non-significantly higher rate of symptomatic recurrent VTE than those with symptomatic SVT.52
Anticoagulant Choice
Several studies showed that early start of anticoagulation therapy (within one-two weeks from diagnosis) promotes better vessel recanalization compared to commencing later.77–79 Only one recent study found no correlation between early anticoagulant therapy and thrombosis recanalization possibly due to the use of vitamin K antagonists (VKA) without concomitant LMWH administration while reaching the target international normalised ratio (INR).80
LMWH and VKA are the mainstay of the anticoagulant treatment for SVT (Table 2).2,3,69–71 Treatment is usually commenced with LMWH switching to VKA after a few days of overlapping treatment, once the INR is in the target range (2.0–3.0).69 However, continuation of LMWH alone may be preferred in cases of low platelet count, active cancer, or hepatic disease.69
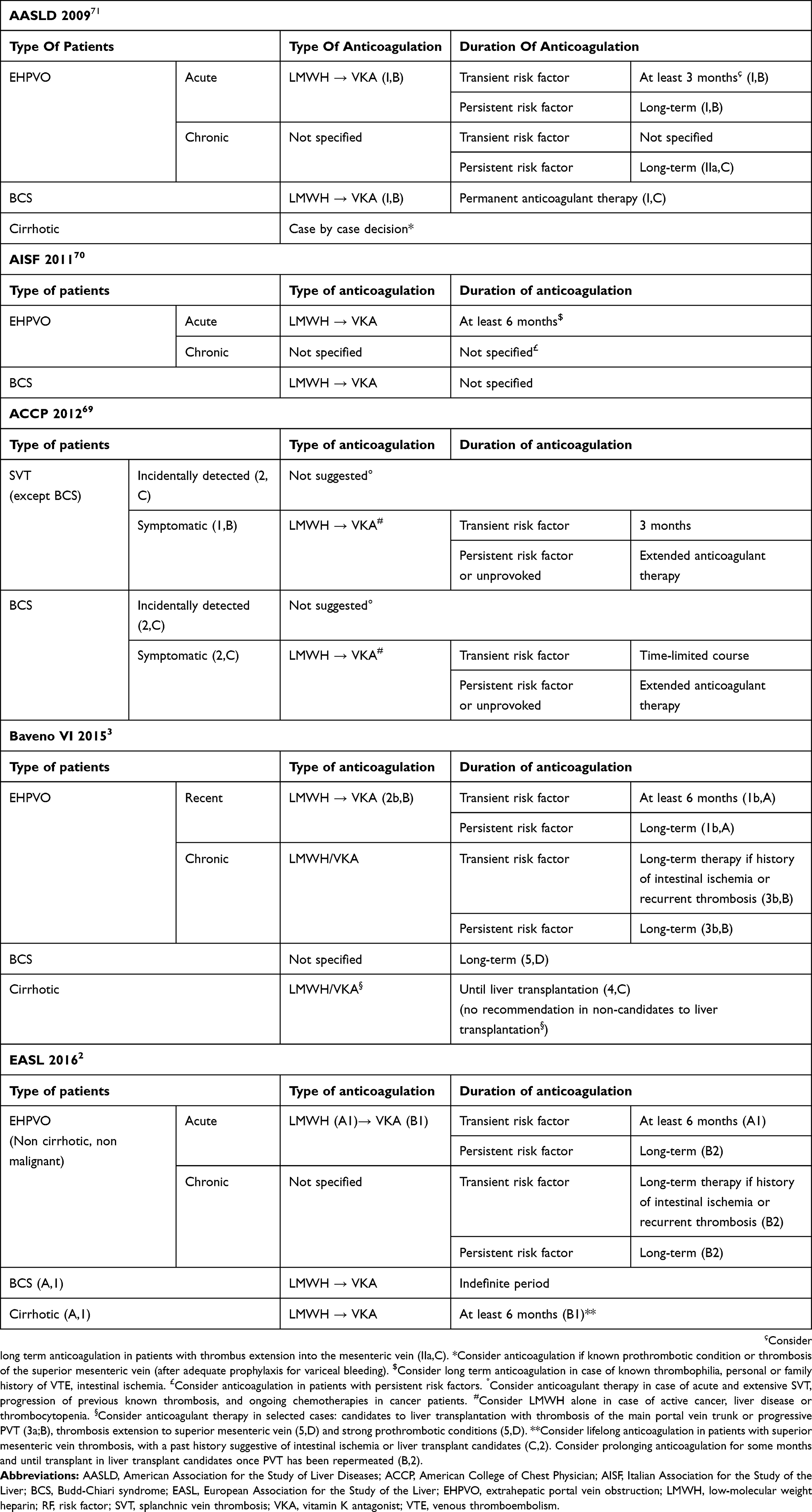 |
Table 2 Guidelines Recommendations For The Anticoagulant Treatment Of Splanchnic Vein Thrombosis |
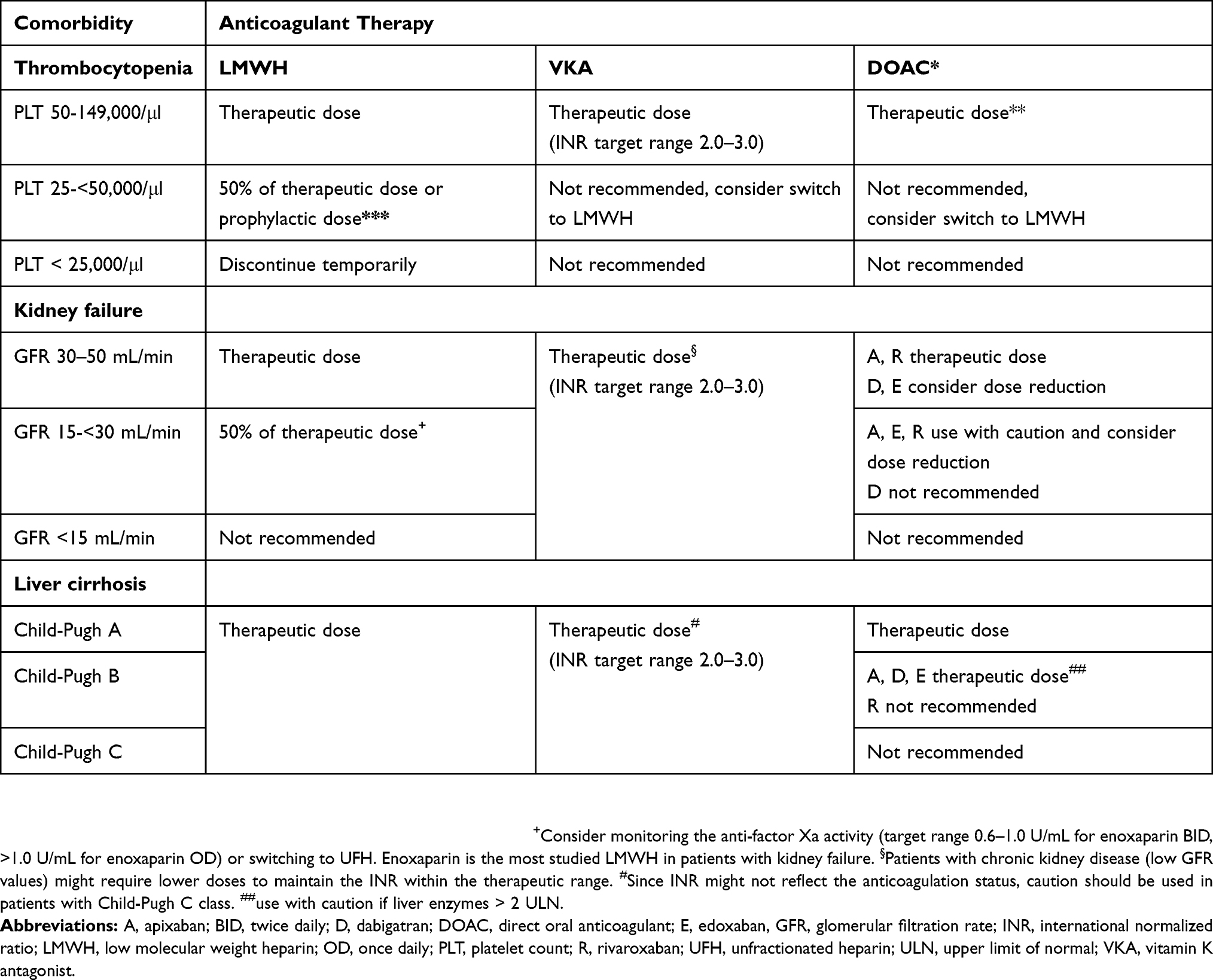 |
Table 3 Therapeutic Strategies For Patients With Splanchnic Vein Thrombosis And Thrombocytopenia, Kidney Failure Or Liver Cirrhosis |
To date, only few but promising data are available on the direct oral anticoagulants (DOAC) for the treatment of SVT. In a recent small randomized controlled trial in 80 cirrhotic patients with PVT, rivaroxaban seemed more effective and safer compared with VKA.81 In a retrospective cohort of 50 cirrhotic patients with PVT treated with edoxaban or warfarin after an initial 2-week period with danaparoid sodium, edoxaban reduced recurrent VTE but increased the rate of major bleeding compared with VKA dose-adjusted to a lower INR target range (1.5–2.0).82 Finally, a small prospective observational cohort of patients with atypical site thrombosis including 26 SVTs, found similar rates of VTE recurrence and bleeding in patients treated with apixaban or rivaroxaban and those on enoxaparin.83 While waiting for future data, clinicians should cautiously consider the use of DOACs for SVT, as they are still considered off-label in this group of patients. The same therapeutic schemes and dose modification as for usual site VTE could be applied with a careful clinical and laboratory follow-up.74 However, all DOACs are contraindicated in patients with Child-Pugh class C, and rivaroxaban is contraindicated also in Child-Pugh class B. A number of ongoing studies is evaluating the use of the DOAC in SVT patients (NCT02627053, NCT02555111, NCT03193502, NCT03778502).
Concomitant medications and patient comorbidities (e.g. low platelet count, chronic liver disease, and moderate to severe renal failure) need to be carefully considered when deciding on the type and dose of anticoagulant treatment.2,69,84–88 Based on current available evidence on the treatment of patients with usual site VTE and expert opinions, our suggested approach to SVT patients with the above mentioned comorbidities is summarised in Table 3.21,84,85,89–93
For How Long Should Patients Be Treated?
The recommended duration of anticoagulant therapy differs across guidelines (Table 2). The ACCP guidelines suggest 3 months of anticoagulant treatment in patients with a transient thrombotic risk factor and longer duration in those with a persistent thrombotic risk factor or unprovoked SVT and low bleeding risk.69
The Baveno VI Consensus Workshop and the European Association for the Study of the Liver recommend at least six months of treatment for acute/recent SVT secondary to transient risk factors and long-term anticoagulation in case of persistent risk factors. Long-term anticoagulation should also be considered in patients with chronic SVT and a persistent pro-thrombotic state and in patients with transient risk factors who have a history of intestinal ischemia or recurrent thrombosis.2,3
Confirming these data, a recent study showed an higher incidence of thrombotic events in patients with unprovoked SVT or SVT related to persistent risk factors such as liver cirrhosis, solid cancer, and MPN.19 Therefore, these categories of patients should be considered for long-term anticoagulation.
In addition, the American Association for the Study of Liver Diseases and the Report of the Baveno VI Consensus Workshop guidelines weakly recommend long-term anticoagulation for patients with thrombus extension into the mesenteric veins.3,71 Finally, long-term anticoagulant therapy should be administered to all patients with BCS, especially if unprovoked.3
Thrombus extension (partial versus total occlusion), involvement of multiple vessels, and lack of recanalization during follow-up are all associated with worse prognosis and should be considered when deciding on treatment duration.21 Indeed, the dose and duration of the anticoagulant therapy was directed by the rate of vessel recanalization in several studies.68,94,95
Our recommendations on the anticoagulant treatment in patients with SVT are summarized in Figure 1.
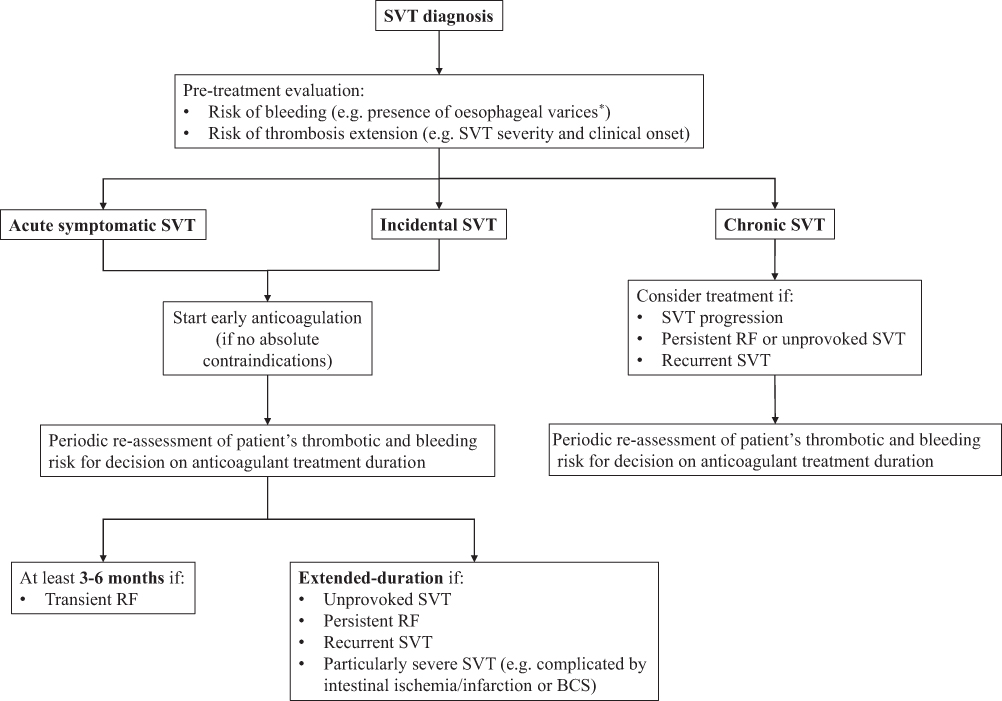 |
Figure 1 Suggested algorithm for the treatment of splanchnic vein thrombosis. *Consider prophylaxis of oesophageal bleeding (if varices). Abbreviations: BCS, Budd-Chiari syndrome, RF, risk factor, SVT, splanchnic vein thrombosis. |
Thrombolysis
Only few studies evaluated the role of thrombolysis in SVT and reported conflicting results. Smalberg and colleagues showed that its effectiveness may be associated with a not negligible risk of bleeding.96 In contrast, promising results were reported in another study involving patients with acute MVT.97,98
The use of thrombolysis may be carefully considered in specialized centres for very selected cases (e.g. failure of anticoagulant therapy or MVT complicated by intestinal ischemia).74
Budd-Chiari Syndrome
Due to the severity of BCS, anticoagulant treatment should be established as soon as possible and continued lifelong. Patients not-responsive to medical treatment should be managed according to a stepwise approach with angioplasty/stenting or thrombolysis, followed by trans-jugular intrahepatic portosystemic shunting (TIPS) and, at last, orthotopic liver transplantation.2,3 It has been reported that approximately half of BCS patients require interventional procedures.99
Prognosis
Data from several observational studies showed that the prognosis of SVT depends on several variables, such as older age, underlying risk factors (e.g. active cancer and MPN), site and extension of SVT.16,21 In an international prospective cohort study evaluating the long-term clinical outcomes of 604 patients with SVT, the mortality rate was 10.3 per 100 patient-years (95% CI, 8.5 to 12.5) during a median follow-up of 2 years.19 The highest and the lowest mortality rates were reported, respectively, in patients with solid cancer (39.5 per 100 patient-years; 95% CI, 31.1 to 50.1) and with unprovoked SVT (2.3 per 100 patient-years; 95% CI, 1.1 to 4.8).19 Data from Danish registries showed that MVT was associated with the highest 30-day mortality rate (63.1%), followed by PVT and BCS (15.6% and 13.2%, respectively).18
Furthermore, SVT carry also an increased risk of bleeding events and arterial cardiovascular events.100 The risk of bleeding was particularly relevant in the first 30 days (4.3% in SVT patients vs 0.5% in patients with DVT or PE), and remained significantly higher than usual site VTE up to 10 years after SVT diagnosis. The risk of cardiovascular events was also particularly relevant in the first 30 days (3.3% in SVT patients vs 0.9% in patients with DVT or PE), but remained high up to 1 year.100
Conclusions
SVT represents a diagnostic and therapeutic challenge. Based on limited available evidence, treatment decisions should be individualized with careful evaluation of the risks of bleeding and SVT recurrence or extension. The presence of oesophageal varices does not represent an absolute contraindication for anticoagulant therapy, but medical and endoscopic prophylaxis are warranted before starting anticoagulation to reduce bleeding risk. LMWH and VKA are the treatment of choice for SVT whereas the use of DOACs remains still off-label in several countries. Recent evidence suggests that incidentally detected SVT has similar prognosis as symptomatic SVT and a similar treatment approach is suggested. Treatment of chronic SVT is still controversial, especially in cirrhotic patients, but it should be considered in patients with persistent risk factors or selected cases at high risk of progression. Similarly to usual site VTE, a short course of anticoagulation (up to 6 months) is suggested for SVT provoked by transient risk factors, whereas longer treatment duration should be considered for unprovoked SVT, SVT provoked by persistent risk factors, and SVT with a high risk of recurrence or progression.
A great scientific effort has been made in the past years trying to clarify some of the challenges associated with SVT. However, future studies will be needed to strengthen some areas of uncertainty including both the diagnostic (e.g. identification of new underlying diagnostic and prognostic risk factors) and therapeutic approaches (e.g. identification of which patients to treat, which anticoagulant to use and the duration of treatment) to SVT.
Disclosure
EV and NR report no conflicts of interest in relation to this paper. MDN reports personal fees from Bayer, Daiichi Sankyo, Pfizer, Leo Pharma, and Aspen, outside the submitted work. WA has received a research grant from Bayer to support a clinical study in patients with splanchnic vein thrombosis, received honoraria for participation at advisory boards from Bayer, Boehringer Inghelheim, Daiichi Sankyo, BMS/Pfizer, Sanofi, and Portola, and reports grants and personal fees from Bayer, and personal fees from BMS/Pfizer, Daiichi Sankyo, Sanofi, Aspen, and Portola, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Myers K, Hannah P. Anatomy of veins and lymphatics. In: Myers K, Hannah P, editors. Manual of Venous and Lymphatic Diseases. London, UK: Taylor & Francis Ltd. 2018:13–38.
2. European Association for the Study of the Liver. EASL clinical practice guidelines: vascular diseases of the liver. j hepatol. 2016;64(1):179–202. doi:10.1016/j.jhep.2015.07.040
3. de Franchis R, Faculty BV. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63(3):743–752. doi:10.1016/j.jhep.2015.05.022
4. Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016;118(9):1340–1347. doi:10.1161/CIRCRESAHA.115.306841
5. Ageno W, Squizzato A, Togna A, et al. Incidental diagnosis of a deep vein thrombosis in consecutive patients undergoing a computed tomography scan of the abdomen: a retrospective cohort study. J Thromb Haemost. 2012;10(1):158–160. doi:10.1111/j.1538-7836.2011.04565.x
6. Ögren M, Bergqvist D, Björck M, Acosta S, Eriksson H, Sternby NH. Portal vein thrombosis: prevalence, patient characteristics and lifetime risk: A population study based on 23 796 consecutive autopsies. World J Gastroenterol. 2006;12(13):2115–2119. doi:10.3748/wjg.v12.i13.2115
7. Rajani R, Björnsson E, Bergquist A, et al. The epidemiology and clinical features of portal vein thrombosis: a multicentre study. Aliment Pharmacol Ther. 2010;32(9):1154–1162. doi:10.1111/j.1365-2036.2010.04454.x
8. Li Y, De Stefano V, Li H, et al. Epidemiology of Budd-Chiari syndrome: a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2018. pii: S2210-7401(18)30230-4. doi: 10.1016/j.clinre.2018.10.014. [Epub ahead of print] PubMed PMID: 30528513.
9. Ageno W, Dentali F, Pomero F, et al. Incidence rates and case fatality rates of portal vein thrombosis and Budd-Chiari Syndrome. Thromb Haemost. 2017;117(4):794–800. doi:10.1160/TH16-10-0781
10. Rajani R, Melin T, Björnsson E, et al. Budd-Chiari syndrome in Sweden: epidemiology, clinical characteristics and survival - an 18-year experience. Liver Int. 2009;29(2):253–259. doi:10.1111/j.1478-3231.2008.01838.x
11. Ollivier-Hourmand I, Allaire M, Goutte N, et al. The epidemiology of Budd-Chiari syndrome in France. Dig Liver Dis. 2018;50(9):931–937. doi:10.1016/j.dld.2018.04.004
12. Ki M, Choi HY, Kim KA, Kim BH, Jang ES, Jeong SH. Incidence, prevalence and complications of Budd-Chiari syndrome in South Korea: a nationwide, population-based study. Liver Int. 2016;36(7):1067–1073. doi:10.1111/liv.13008
13. Zhang W, Qi X, Zhang X, et al. Budd-Chiari Syndrome in China: a systematic analysis of epidemiological features based on the Chinese literature survey. Gastroenterol Res Pract. 2015;2015:738548. doi:10.1155/2015/750932
14. Parkash O, Khan A, Hamid S. Clinical characteristics and outcome of Budd-Chiari Syndrome at a Tertiary Care Hospital in Pakistan. J Coll Physicians Surg Pak. 2017;27(5):301–304. doi:2617
15. Zhang W, Wang QZ, Chen XW, et al. Budd-Chiari syndrome in China: a 30-year retrospective study on survival from a single center. World J Gastroenterol. 2018;24(10):1134–1143. doi:10.3748/wjg.v24.i10.1134
16. Thatipelli MR, McBane RD, Hodge DO, Wysokinski WE. Survival and recurrence in patients with splanchnic vein thromboses. Clin Gastroenterol Hepatol. 2010;8(2):200–205. doi:10.1016/j.cgh.2009.09.019
17. Acosta S, Alhadad A, Svensson P, Ekberg O. Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. Br J Surg. 2008;95(10):1245–1251. doi:10.1002/bjs.6319
18. Søgaard KK, Darvalics B, Horváth-Puhó E, Sørensen HT. Survival after splanchnic vein thrombosis: a 20-year nationwide cohort study. Thromb Res. 2016;141:1–7. doi:10.1016/j.thromres.2016.02.024
19. Ageno W, Riva N, Schulman S, et al. Long-term clinical outcomes of splanchnic vein thrombosis: results of an international registry. JAMA Intern Med. 2015;175(9):1474–1480. doi:10.1001/jamainternmed.2015.3184
20. Derman BA, Kwaan HC. Risk Factors, Diagnosis, Management, and. Outcome of splanchnic vein thrombosis: a retrospective analysis. Semin Thromb Hemost. 2015;41(5):503–513.
21. Ageno W, Dentali F, Squizzato A. How I treat splanchnic vein thrombosis. Blood. 2014;124(25):3685–3691. doi:10.1182/blood-2014-07-551515
22. Tripodi A, Primignani M, Chantarangkul V, et al. An imbalance of pro- vs anti-coagulation factors in plasma from patients with cirrhosis. Gastroenterology. 2009;137(6):2105–2111. doi:10.1053/j.gastro.2009.08.045
23. Gatt A, Riddell A, Calvaruso V, Tuddenham EG, Makris M, Burroughs AK. Enhanced thrombin generation in patients with cirrhosis-induced coagulopathy. J Thromb Haemost. 2010;8(9):1994–2000. doi:10.1111/j.1538-7836.2010.03937.x
24. Hugenholtz GC, Macrae F, Adelmeijer J, et al. Procoagulant changes in fibrin clot structure in patients with cirrhosis are associated with oxidative modifications of fibrinogen. J Thromb Haemost. 2016;14(5):1054–1066. doi:10.1111/jth.13278
25. Stine JG, Wang J, Shah PM, et al. Decreased portal vein velocity is predictive of the development of portal vein thrombosis: a matched case-control study. Liver Int. 2018;38(1):94–101. doi:10.1111/liv.13500
26. Ambrosino P, Tarantino L, Di Minno G, et al. The risk of venous thromboembolism in patients with cirrhosis. A systematic review and meta-analysis. Thromb Haemost. 2017;117(1):139–148. doi:10.1160/TH16-06-0450
27. Nery F, Chevret S, Condat B, et al. Causes and consequences of portal vein thrombosis in 1,243 patients with cirrhosis: results of a longitudinal study. Hepatology. 2015;61(2):660–667. doi:10.1002/hep.27546
28. Violi F, Corazza GR, Caldwell SH, et al. Incidence and recurrence of portal vein thrombosis in cirrhotic patients. Thromb Haemost. 2019;119(3):496–499. doi:10.1055/s-0038-1676981
29. Khorana AA. Cancer and thrombosis: implications of published guidelines for clinical practice. Ann Oncol. 2009;20(10):1619–1630. doi:10.1093/annonc/mdp068
30. Gerotziafas GT, Galea V, Mbemba E, et al. Tissue factor over-expression by human pancreatic cancer cells BXPC3 is related to higher prothrombotic potential as compared to breast cancer cells MCF7. Thromb Res. 2012;129(6):779–786. doi:10.1016/j.thromres.2011.07.049
31. Rak J, Milsom C, Magnus N, Yu J. Tissue factor in tumour progression. Best Pract Res Clin Haematol. 2009;22(1):71–83. doi:10.1016/j.beha.2008.12.008
32. Prandoni P, Falanga A, Piccioli A. Cancer and venous thromboembolism. Lancet Oncol. 2005;6(6):401–410. doi:10.1016/S1470-2045(05)70207-2
33. Santoro RC, Prejano S, Iannaccaro P Splanchnic venous thromboembolism in ambulatory cancer patients receiving chemotherapy.
34. Søgaard KK, Farkas DK, Pedersen L, Sørensen HT. Splanchnic venous thrombosis is a marker of cancer and a prognostic factor for cancer survival. Blood. 2015;126(8):957–963. doi:10.1182/blood-2015-03-631119
35. Hettiarachchi RJ, Lok J, Prins MH, Büller HR, Prandoni P. Undiagnosed malignancy in patients with deep vein thrombosis: incidence, risk indicators, and diagnosis. Cancer. 1998;83(1):180–185. doi:10.1002/(sici)1097-0142(19980701)83:1<180::aid-cncr24>3.0.co;2-s
36. Barbui T, Finazzi G, Falanga A. Myeloproliferative neoplasms and thrombosis. Blood. 2013;122(13):2176–2184. doi:10.1182/blood-2013-03-460154
37. Falanga A, Marchetti M. Thrombotic disease in the myeloproliferative neoplasms. Hematology Am Soc Hematol Educ Program. 2012;2012:571–581. doi:10.1182/asheducation-2012.1.571
38. Sekhar M, McVinnie K, Burroughs AK. Splanchnic vein thrombosis in myeloproliferative neoplasms. Br J Haematol. 2013;162(6):730–747. doi:10.1111/bjh.12461
39. Baxter EJ, Scott LM, Campbell PJ, et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet. 2005;365(9464):1054–1061. doi:10.1016/S0140-6736(05)71142-9
40. De Stefano V, Fiorini A, Rossi E, et al. Incidence of the JAK2 V617F mutation among patients with splanchnic or cerebral venous thrombosis and without overt chronic myeloproliferative disorders. J Thromb Haemost. 2007;5(4):708–714.
41. Dentali F, Squizzato A, Brivio L, et al. JAK2V617F mutation for the early diagnosis of Ph- myeloproliferative neoplasms in patients with venous thromboembolism: a meta-analysis. Blood. 2009;113(22):5617–5623. doi:10.1182/blood-2008-12-196014
42. Arellano-Rodrigo E, Alvarez-Larrán A, Reverter JC, Villamor N, Colomer D, Cervantes F. Increased platelet and leukocyte activation as contributing mechanisms for thrombosis in essential thrombocythemia and correlation with the JAK2 mutational status. Haematologica. 2006;91(2):169–175.
43. Robertson B, Urquhart C, Ford I, et al. Platelet and coagulation activation markers in myeloproliferative diseases: relationships with JAK2 V6I7 F status, clonality, and antiphospholipid antibodies. J Thromb Haemost. 2007;5(8):1679–1685. doi:10.1111/j.1538-7836.2007.02626.x
44. Kanellopoulou T, Alexopoulou A, Theodossiades G, Koskinas J, Archimandritis AJ. Pylephlebitis: an overview of non-cirrhotic cases and factors related to outcome. Scand J Infect Dis. 2010;42(11–12):804–811. doi:10.3109/00365548.2010.508464
45. Primignani M, Mannucci PM. The role of thrombophilia in splanchnic vein thrombosis. Semin Liver Dis. 2008;28(3):293–301. doi:10.1055/s-0028-1085097
46. Sutkowska E, McBane RD, Tafur AJ, et al. Thrombophilia differences in splanchnic vein thrombosis and lower extremity deep venous thrombosis in North America. J Gastroenterol. 2013;48(10):1111–1118. doi:10.1007/s00535-012-0728-3
47. Janssen HL, Meinardi JR, Vleggaar FP, et al. Factor V Leiden mutation, prothrombin gene mutation, and deficiencies in coagulation inhibitors associated with Budd-Chiari syndrome and portal vein thrombosis: results of a case-control study. Blood. 2000;96(7):2364–2368.
48. Senzolo M, Riva N, Dentali F, et al. Long-term outcome of splanchnic vein thrombosis in cirrhosis. Clin Transl Gastroenterol. 2018;9(8):176. doi:10.1038/s41424-018-0043-2
49. García-Villa A, Yarza R, Pagès M, Díaz-Pedroche C, Font C Cancer-associated splanchnic venous thrombosis: clinical findings at presentation.
50. De Stefano V, Vannucchi AM, Ruggeri M, et al. Splanchnic vein thrombosis in myeloproliferative neoplasms: risk factors for recurrences in a cohort of 181 patients. Blood Cancer J. 2016;6(11):e493. doi:10.1038/bcj.2016.103
51. Riva N, Ageno W, Schulman S, et al. Clinical history and antithrombotic treatment of incidentally detected splanchnic vein thrombosis: a multicentre, international prospective registry. Lancet Haematol. 2016;3(6):e267–e275. doi:10.1016/S2352-3026(16)30020-5
52. Tufano A, Ageno W, Di Micco P, et al. Outcomes during anticoagulation in patients with symptomatic vs. incidental splanchnic vein thrombosis. Thromb Res. 2018;164:69–74. doi:10.1016/j.thromres.2018.02.143
53. De Stefano V, Martinelli I. Splanchnic vein thrombosis: clinical presentation, risk factors and treatment. Internal Emergency Med. 2010;5(6):487–494. doi:10.1007/s11739-010-0413-6
54. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001;345(23):1683–1688. doi:10.1056/NEJMra010076
55. Akamatsu N, Sugawara Y, Kokudo N. Budd-Chiari syndrome and liver transplantation. Intractable Rare Dis Res. 2015;4(1):24–32. doi:10.5582/irdr.2014.01031
56. Zhang DL, Hao JY, Yang N. Value of D-dimer and protein S for diagnosis of portal vein thrombosis in patients with liver cirrhosis. J Int Med Res. 2013;41(3):664–672. doi:10.1177/0300060513483413
57. Malaguarnera M, Latteri S, Bertino G, et al. D-dimer plasmatic levels as a marker for diagnosis and prognosis of hepatocellular carcinoma patients with portal vein thrombosis. Clin Exp Gastroenterol. 2018;11:373–380. doi:10.2147/CEG.S172663
58. Spadaro A, Tortorella V, Morace C, et al. High circulating D-dimers are associated with ascites and hepatocellular carcinoma in liver cirrhosis. World J Gastroenterol. 2008;14(10):1549–1552. doi:10.3748/wjg.14.1549
59. Yang S, Fan X, Ding W, et al. D-dimer as an early marker of severity in patients with acute superior mesenteric venous thrombosis. Medicine (Baltimore). 2014;93(29):e270. doi:10.1097/MD.0000000000000270
60. Riva N, Ageno W. Clinical manifestations and imaging tools in the diagnosis of splanchnic and cerebral vein thromboses. Thromb Res. 2018;163:252–259. doi:10.1016/j.thromres.2017.06.030
61. Millener P, Grant EG, Rose S, et al. Color Doppler imaging findings in patients with Budd-Chiari syndrome: correlation with venographic findings. AJR Am J Roentgenol. 1993;161(2):307–312. doi:10.2214/ajr.161.2.8333368
62. Bradbury MS, Kavanagh PV, Chen MY, Weber TM, Bechtold RE. Noninvasive assessment of portomesenteric venous thrombosis: current concepts and imaging strategies. J Comput Assist Tomogr. 2002;26(3):392–404. doi:10.1097/00004728-200205000-00014
63. Weber SM, Rikkers LF. Splenic vein thrombosis and gastrointestinal bleeding in chronic pancreatitis. World J Surg. 2003;27(11):1271–1274. doi:10.1007/s00268-003-7247-6
64. Chou CK, Mak CW, Tzeng WS, Chang JM. CT of small bowel ischemia. Abdom Imaging. 2004;29(1):18–22. doi:10.1007/s00261-003-0073-3
65. DeLeve LD, Valla DC, Garcia-Tsao G. American Association for the study liver diseases. Vascular disorders of the liver. Hepatology. 2009;49(5):1729–1764. doi:10.1002/hep.22772
66. Janssen HL, Garcia-Pagan JC, Elias E, et al. Budd-Chiari syndrome: a review by an expert panel. J Hepatol. 2003;38(3):364–371. doi:10.1016/s0168-8278(02)00434-8
67. Condat B, Valla D. Nonmalignant portal vein thrombosis in adults. Nat Clin Pract Gastroenterol Hepatol. 2006;3(9):505–515. doi:10.1038/ncpgasthep0577
68. Senzolo M, Sartori T, Rossetto V, et al. Prospective evaluation of anticoagulation and transjugular intrahepatic portosystemic shunt for the management of portal vein thrombosis in cirrhosis. Liver Int. 2012;32(6):919–927. doi:10.1111/j.1478-3231.2012.02785.x
69. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e419S–e496S. doi:10.1378/chest.11-2301
70. Senzolo M, Riggio O, Primignani M. Vascular disorders of the liver: recommendations from the Italian Association for the Study of the Liver (AISF) ad hoc committee. Dig Liver Dis. 2011;43(7):503–514. doi:10.1016/j.dld.2010.11.006
71. DeLeve LD, Valla DC, Garcia-Tsao G, Diseases A. Vascular disorders of the liver. Hepatology. 2009;49(5):1729–1764. doi:10.1002/hep.22772
72. Riva N, Ageno W, Poli D, et al. Safety of vitamin K antagonist treatment for splanchnic vein thrombosis: a multicenter cohort study. J Thromb Haemost. 2015;13(6):1019–1027. doi:10.1111/jth.12930
73. Spaander MC, Hoekstra J, Hansen BE, Van Buuren HR, Leebeek FW, Janssen HL. Anticoagulant therapy in patients with non-cirrhotic portal vein thrombosis: effect on new thrombotic events and gastrointestinal bleeding. J Thromb Haemost. 2013;11(3):452–459. doi:10.1111/jth.12121
74. Ageno W, Beyer-Westendorf J, Garcia DA, Lazo-Langner A, McBane RD, Paciaroni M. Guidance for the management of venous thrombosis in unusual sites. J Thromb Thrombolysis. 2016;41(1):129–143. doi:10.1007/s11239-015-1308-1
75. Riva N, Donadini MP, Dentali F, Squizzato A, Ageno W. Clinical approach to splanchnic vein thrombosis: risk factors and treatment. Thromb Res. 2012;130(Suppl 1):S1–S3. doi:10.1016/j.thromres.2012.08.259
76. Di Nisio M, Lee AY, Carrier M, Liebman HA, Khorana AA. Subcommittee on haemostasis and malignancy. Diagnosis and treatment of incidental venous thromboembolism in cancer patients: guidance from the SSC of the ISTH. J Thromb Haemost. 2015;13(5):880–883. doi:10.1111/jth.12883
77. Turnes J, García-Pagán JC, González M, et al. Portal hypertension-related complications after acute portal vein thrombosis: impact of early anticoagulation. Clin Gastroenterol Hepatol. 2008;6(12):1412–1417. doi:10.1016/j.cgh.2008.07.031
78. Delgado MG, Seijo S, Yepes I, et al. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin Gastroenterol Hepatol. 2012;10(7):776–783. doi:10.1016/j.cgh.2012.01.012
79. Joh JH, Kim DI. Mesenteric and portal vein thrombosis: treated with early initiation of anticoagulation. Eur J Vasc Endovasc Surg. 2005;29(2):204–208. doi:10.1016/j.ejvs.2004.10.005
80. Chen H, Liu L, Qi X, et al. Efficacy and safety of anticoagulation in more advanced portal vein thrombosis in patients with liver cirrhosis. Eur J Gastroenterol Hepatol. 2016;28(1):82–89. doi:10.1097/MEG.0000000000000482
81. Hanafy AS, Abd-Elsalam S, Dawoud MM. Randomized controlled trial of rivaroxaban versus warfarin in the management of acute non-neoplastic portal vein thrombosis. Vascul Pharmacol. 2019;113:86–91. doi:10.1016/j.vph.2018.05.002
82. Nagaoki Y, Aikata H, Daijyo K, et al. Efficacy and safety of edoxaban for treatment of portal vein thrombosis following danaparoid sodium in patients with liver cirrhosis. Hepatol Res. 2018;48(1):51–58. doi:10.1111/hepr.12895
83. Janczak DT, Mimier MK, McBane RD, et al. Rivaroxaban and apixaban for initial treatment of acute venous thromboembolism of atypical location. Mayo Clin Proc. 2018;93(1):40–47. doi:10.1016/j.mayocp.2017.10.007
84. Samuelson Bannow BT, Lee A, Khorana AA, et al. Management of cancer-associated thrombosis in patients with thrombocytopenia: guidance from the SSC of the ISTH. J Thromb Haemost. 2018;16(6):1246–1249. doi:10.1111/jth.14015
85. Grand’Maison A, Charest AF, Geerts WH. Anticoagulant use in patients with chronic renal impairment. Am J Cardiovasc Drugs. 2005;5(5):291–305. doi:10.2165/00129784-200505050-00002
86. Steffel J, Verhamme P, Potpara TS, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018;39(16):1330–1393. doi:10.1093/eurheartj/ehy136
87. Dhar A, Mullish BH, Thursz MR. Anticoagulation in chronic liver disease. J Hepatol. 2017;66(6):1313–1326. doi:10.1016/j.jhep.2017.01.006
88. Hughes S, Szeki I, Nash MJ, Thachil J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin Kidney J. 2014;7(5):442–449. doi:10.1093/ckj/sfu080
89. Garcia DA, Baglin TP, Weitz JI, Samama MM. Parenteral anticoagulants: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e24S–e43S. doi:10.1378/chest.11-2291
90. European Medicines Agency. Eliquis (apixaban): summary of product characteristics. Available from: https://www.ema.europa.eu/documents/product-information/eliquis-epar-product-information_en.pdf (
91. European Medicines Agency. Lixiana (edoxaban): summary of product characteristics. Available from: https://www.ema.europa.eu/documents/product-information/lixiana-epar-product-information_en.pdf (
92. European Medicines Agency. Pradaxa (dabigatran etexilate): summary of product characteristics. Available from: https://www.ema.europa.eu/documents/product-information/pradaxa-epar-product-information_en.pdf (
93. European Medicines Agency. Xarelto (rivaroxaban): summary of product characteristics. Available from: https://www.ema.europa.eu/documents/product-information/xarelto-epar-product-information_en.pdf (
94. Condat B, Pessione F, Helene Denninger M, Hillaire S, Valla D. Recent portal or mesenteric venous thrombosis: increased recognition and frequent recanalization on anticoagulant therapy. Hepatology. 2000;32(3):466–470. doi:10.1053/jhep.2000.16597
95. Amitrano L, Guardascione MA, Scaglione M, et al. Splanchnic vein thrombosis and variceal rebleeding in patients with cirrhosis. Eur J Gastroenterol Hepatol. 2012;24(12):1381–1385. doi:10.1097/MEG.0b013e328357d5d4
96. Smalberg JH, Spaander MV, Jie KS, et al. Risks and benefits of transcatheter thrombolytic therapy in patients with splanchnic venous thrombosis. Thromb Haemost. 2008;100(6):1084–1088.
97. Yang SF, Liu BC, Ding WW, He CS, Wu XJ, Li JS. Initial transcatheter thrombolysis for acute superior mesenteric venous thrombosis. World J Gastroenterol. 2014;20(18):5483–5492. doi:10.3748/wjg.v20.i18.5483
98. Yang S, Zhang L, Liu K, et al. Postoperative catheter-directed thrombolysis versus systemic anticoagulation for acute superior mesenteric venous thrombosis. Ann Vasc Surg. 2016;35:88–97. doi:10.1016/j.avsg.2016.02.019
99. Darwish Murad S, Plessier A, Hernandez-Guerra M, et al.; EN-Vie (European Network for Vascular Disorders of the Liver). Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009;151(3):167–175. doi:10.7326/0003-4819-151-3-200908040-00004
100. Søgaard KK, Adelborg K, Darvalics B, et al. Risk of bleeding and arterial cardiovascular events in patients with splanchnic vein thrombosis in Denmark: a population-based cohort study. Lancet Haematol. 2018;5(10):e441–e449. doi:10.1016/S2352-3026(18)30133-9
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.