Back to Journals » Journal of Pain Research » Volume 13
Spinal Epidural Hematoma After Percutaneous Kyphoplasty: Case Report and Literature Review
Authors Zou P, Gong HL, Wei JM, Wei DM, Qian LX, Liu P ![]() , Hao DJ, Yang JS, Zhao YT
, Hao DJ, Yang JS, Zhao YT
Received 10 September 2020
Accepted for publication 5 October 2020
Published 3 November 2020 Volume 2020:13 Pages 2799—2804
DOI https://doi.org/10.2147/JPR.S280650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Robert B. Raffa
Peng Zou,1,* Han-Lin Gong,2,* Jian-Min Wei,3,* Dong-Mei Wei,4 Li-Xiong Qian,1 Peng Liu,1 Ding-Jun Hao,1 Jun-Song Yang,1 Yuan-Ting Zhao1
1Department of Spine Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Department of Integrated Traditional Chinese and Western Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan Province 610041, People’s Republic of China; 3Department of Spine Surgery, Baoji City Hospital of Traditional Chinese Medicine, Shaanxi, People’s Republic of China; 4Department of Gynecology and Obstetrics, West China Second University Hospital, Sichuan University, Chengdu 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan-Ting Zhao Tel +86 15229376812
Email [email protected]
Jun-Song Yang Tel +86 18792883498
Email [email protected]
Objective: To present the case of a patient on long-term anticoagulants who developed acute spinal epidural hematoma (SEH) after percutaneous kyphoplasty (PKP) without signs of major cement extravasation to the spinal canal.
Methods: A 64-year-old woman with long-term oral antiplatelet drugs underwent the L1 PKP. Immediately after the operation, the back pain improved significantly without neurological deficit. However, 12 hours later, she developed progressive weakness of the bilateral lower limbs. No intraspinal cement leakage was obvious on the postoperative lumbar radiograph and computed tomography.
Results: An emergency MRI examination revealed a high signal aggregation in front of the spinal cord from T12 to L1, indicating spinal cord compression. The SEH was verified and removed during the laminectomy from T12–L1. Following the decompression surgery, the neurological deficit of the lower limbs improved. On follow-up after 6 months, the muscle strength of the bilateral lower limbs had returned to normal.
Conclusion: For the patient with long-term oral antiplatelet drugs or coagulation malfunction, the transpedicle approach or that via the costovertebral joint with a smaller abduction angle is recommended to reduce the risk of injury to the inner wall of the pedicle. For progressive aggravation of neurological dysfunction after surgery, SEH formation should be suspected despite the absence of intraspinal bone cement leakage. Secondary emergency decompression should be considered to avoid permanent damage to spinal cord nerve function caused by continuous compression.
Keywords: spinal epidural hematoma, percutaneous vertebroplasty, percutaneous kyphoplasty, spinal cord compression, coagulation malfunction
Introduction
Percutaneous kyphoplasty (PKP), a minimally invasive procedure, is widely used for treatment of pain owing to osteoporotic vertebral compression fractures (OVCF). However, it has many serious clinical complications, including cement intraspinal canal leakage, that causes spinal cord compression,1–4 pulmonary or renal vascular embolism,5–8 infection,9 and adjacent vertebral body fractures.10 As an emergency complication, spinal epidural hematoma (SEH) is clinically rare after PKP or percutaneous vertebroplasty (PVP), and has been reported in seven studies.11–17 In this report, we present the case of a patient on long-term anticoagulants who developed acute SEH after PKP without signs of major cement extravasation to the spinal canal. Further, we comprehensively review the relevant literature on the possible pathogenesis of SEH.
Case Presentation
A 64-year-old woman with severe back pain was admitted to the primary hospital. Six months ago, she underwent cardiac stent implantation for myocardial infarction and was prescribed oral aspirin (100 mg/daily) and clopidogrel (75 mg/daily). The prothrombin time (PT) and activated partial thromboplastin time (APTT) were within the normal range on preoperative laboratory examination. The lumbar magnetic resonance imaging (MRI) showed a L1 and L2 compression fracture; the high signal of the short time inversion recovery (STIR) sequence was seen in the L1 vertebral body (Figure 1A and B). She had no neurological symptoms, and she underwent the L1 PKP. The puncture, balloon dilatation, and cement injection were performed using intraoperative fluoroscopy (Figure 2A–F). Immediately after the operation, the back pain improved significantly without neurological deficit. However, 12 hours later, she developed progressive weakness of bilateral lower limbs. No intraspinal cement leakage was obvious on the postoperative lumbar radiograph (Figure 3) and computed tomography (CT) (Figure 4). The patient was transferred to our hospital and underwent an emergency MRI examination, which revealed a high signal aggregation in front of the spinal cord from T12 to L1, indicating spinal cord compression (Figure 1C and D). Physical examination revealed grade III strength in the bilateral iliopsoas, quadriceps femoris, and tibialis anterior muscles. We suspected postoperative SEH and performed laminectomy and decompression from T12–L1. Following excision of SEH and decompression of the spinal cord, the neurological deficit of the lower limbs improved. On follow-up after 6 months, the muscle strength of the bilateral lower limbs had returned to normal.
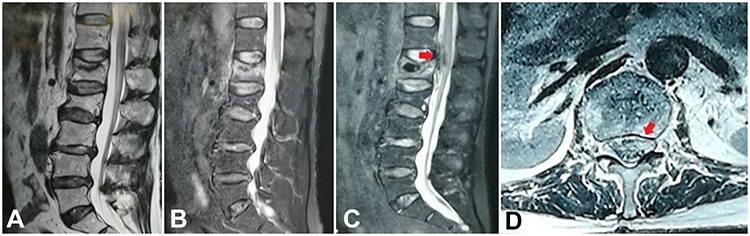 |
Figure 1 Although the L1 and L2 vertebra are wedge shaped at the T2 weighted imaging of magnetic resonance imaging (MRI) (A), the high signal of the short time inversion recovery (STIR) sequence was only seen in the L1 vertebral body (B). Twelve hours after the PKP, a high signal aggregation in front of the spinal cord from T12 to L1 was detected at the sagittal ((C), red arrow) plane of MRI examination, which gathered in the left part of the spinal canal at the axial plane of MRI ((D), red arrow). |
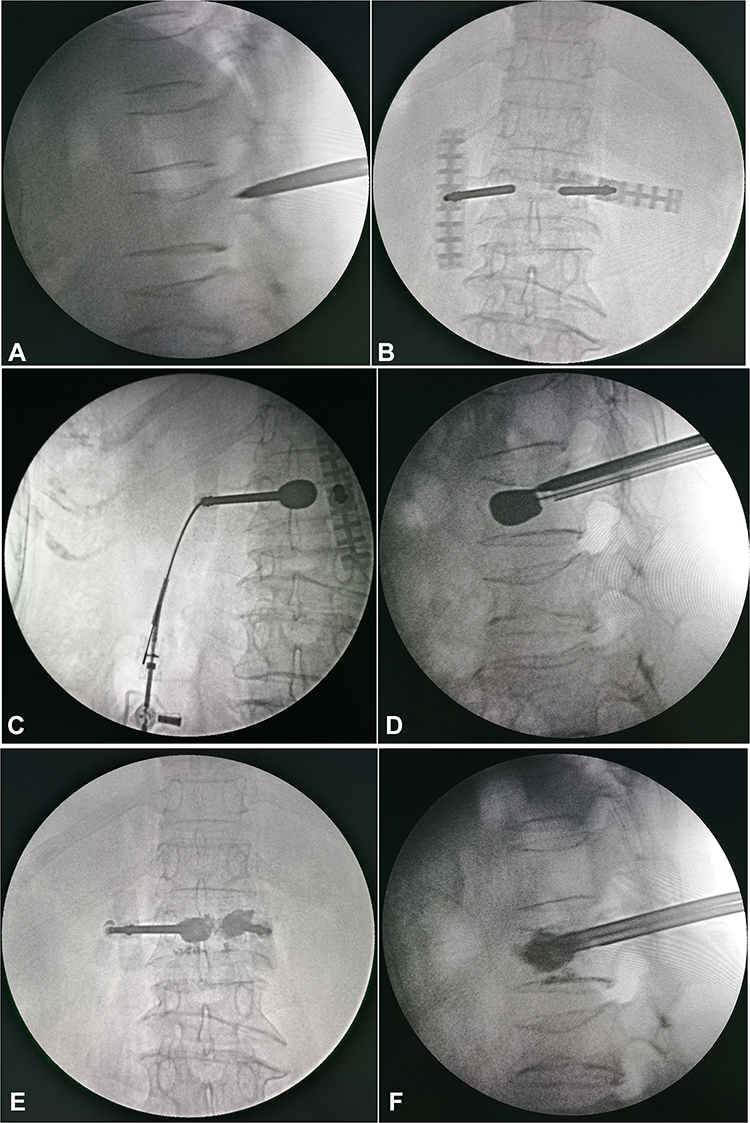 |
Figure 2 At the biplane monitoring, the puncture (A, B), balloon dilatation (C, D), and cement injection (E, F) were performed stepwise. Notably, when the needle arrived at the posterior wall of the vertebral body in the sagittal plane of fluoroscopic view, the intraoperative puncture revealed extension of the puncture needle beyond the inner edge of the projection of the pedicle in the coronal plane, suggesting a large abduction angle of the needle (A, B). |
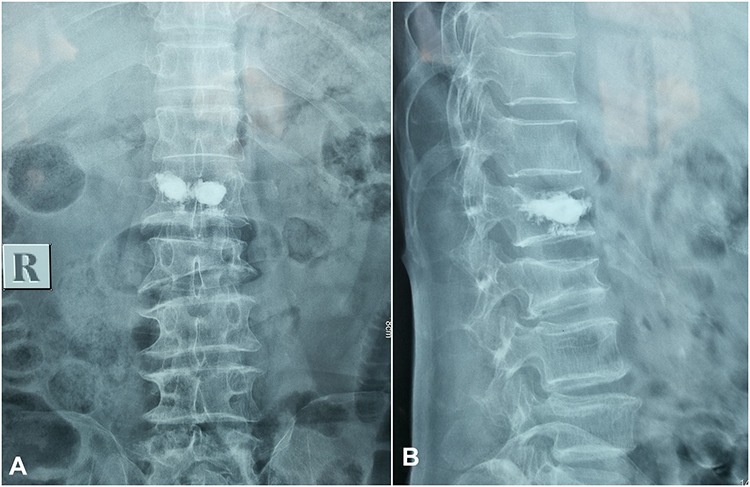 |
Figure 3 No intraspinal cement leakage was obvious on the anteroposterior (A) and lateral (B) view of the postoperative lumbar radiograph. |
 |
Figure 4 While there was no obvious intraspinal cement leakage on the postoperative lumbar computed tomography, there is visible dispersion of the bone cement on the left side of the vertebral body along the puncture trajectory, whose extension line is medial to the inner wall of the pedicle. |
Discussion
PVP and PKP are often used to treat OVCF. They have been applied successfully even in burst fractures without neurological deficit.18 We describe the case of a patient on long-term anticoagulants, who developed acute SEH after PKP, despite the absence of major cement extravasation into the spinal canal, and review the possible pathogenesis.
SEH is associated with idiopathic, iatrogenic, traumatic, and coagulation diseases, and is relatively rare in clinical practice. SEH may cause severe acute spinal cord injury (SCI). Domenicucci et al19 reviewed 1,010 SEH cases in 16 years and concluded that 18% of the significant cases were iatrogenic (spinal puncture), while 29% were non-iatrogenic and caused by factors such as clotting, trauma, and pregnancy. However, iatrogenic SEH after PKP or PVP has been reported in seven previous studies11–17 (Table 1). Wang et al11 suspected that SEH after PKP was caused by direct injury from intraoperative puncture. This finding was supported by three other studies.12–14 Mattei et al15 suggested that venous congestion plays a pivotal role in the etiology of SEH. von der Brelie et al16 attributed the development of SEH after PVP in a patient with long-term oral aspirin to coagulation malfunction owing to aspirin.
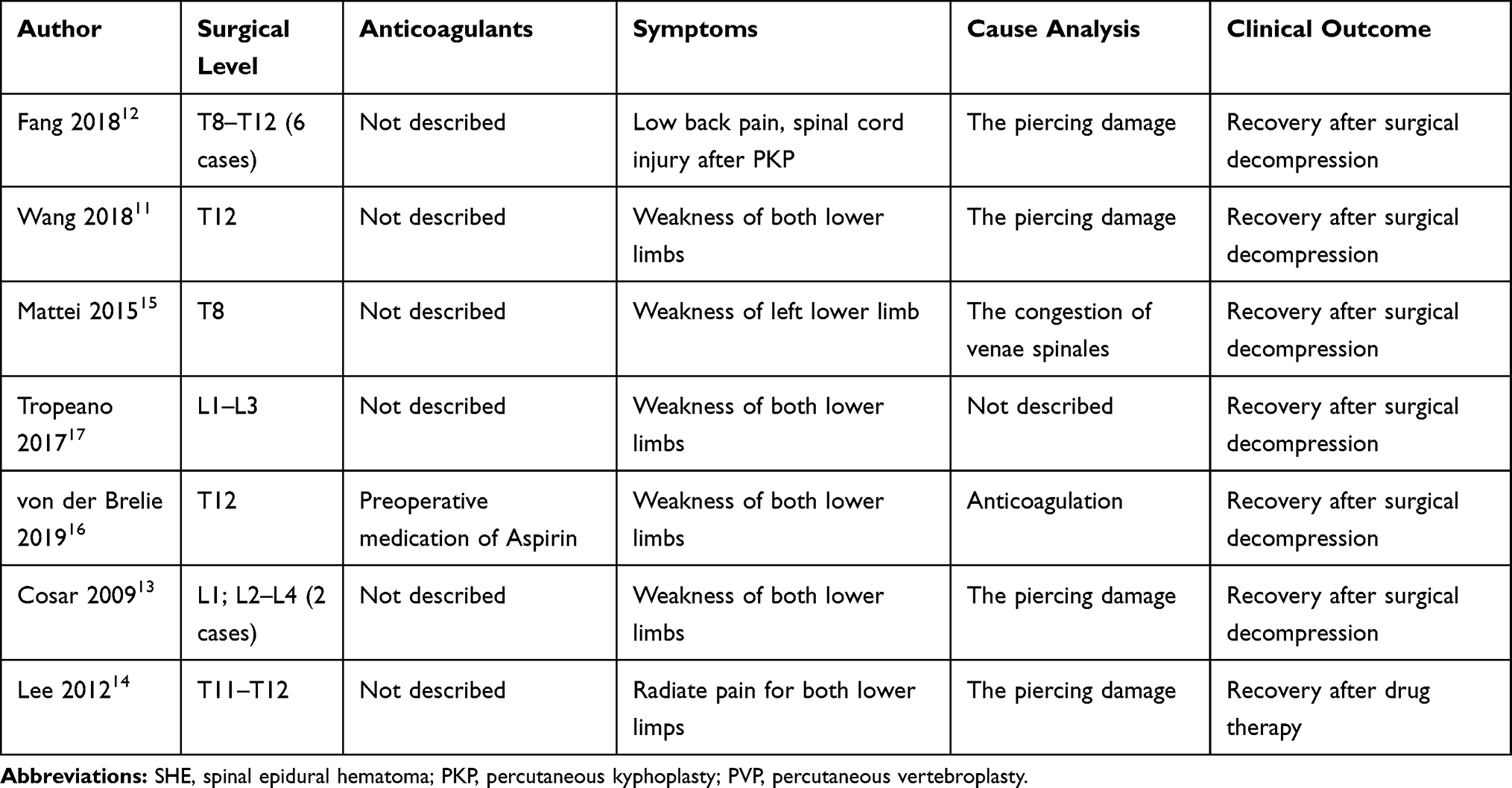 |
Table 1 Surgical Level, Anticoagulants, Symptoms, Cause Analysis, and Clinical Outcome for the Cases with Iatrogenic SEH after PKP or PVP |
When the needle arrived at the posterior wall of the vertebral body in the sagittal plane of fluoroscopic view, the intraoperative puncture revealed an extension of the puncture needle beyond the inner edge of the projection of the pedicle in the coronal plane, suggesting a large abduction angle of the needle (Figure 2) and increased risk of perforation of the inner wall of the pedicle. Postoperative CT also revealed dispersion of the bone cement on the left side of the vertebral body along the puncture trajectory whose extension line is medial to the inner wall of the pedicle (Figure 4). Owing to the significant buffer space surrounding the spinal cord at the level of L1, the puncture needle did not damage it, despite it's large puncture angle or slightly perforated inner wall of the pedicle. Thus, the patient did not experience nerve dysfunction immediately after the operation. Owing to stent implantation, long-term oral aspirin and clopidogrel were administered, which had inhibitory effects on platelet aggregation. Despite normal preoperative PT and APTT, a lack of effective blood clotting resulted in flow of blood from the sinus of the vertebral body through the hole in the inner wall of the pedicle along the pressure gradient, causing SEH and acute compression of the spinal cord. Therefore, the patient showed a gradual decline in neurological function 12 hours after surgery.
Özkan20 reported that if a patient receiving anticoagulant therapy has local or reflected pain and loss of strength and sensation, spontaneous SEH should be considered. There is a lack of consensus on the role of long-term oral antiplatelet drugs and coagulation malfunction on the risk of postoperative SEH in patients with OVCF. In this case, anexcessive puncture angle was considered to have damaged the inner wall of the pedicle, causing SEH. The transpedicle approach or that via the costovertebral joint with a smaller abduction angle is recommended to reduce the risk of injury to the inner wall of the pedicle. Thus, a bilateral procedure is theoretically better than a unilateral procedure. For progressive aggravation of neurological dysfunction after surgery, SEH formation should be suspected despite the absence of intraspinal bone cement leakage. Secondary emergency decompression should be considered to avoid permanent damage to spinal cord nerve function caused by continuous compression.
Acknowledgments
We thank the National Natural Science Foundation of China (No. 81830077), the Project of China post-doctoral research fund (project no.: 2016M602943XB); Basic scientific research operating expenses (natural science); scientific research project of central university (project no.: XZY012019124); and Shaanxi province post-doctoral research fund enterprise project (project no.: 2017BSHQYXMZZ19) for providing the grant.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lee BJ, Lee SR, Yoo TY. Paraplegia as a complication of percutaneous vertebroplasty with polymethylmethacrylate: a case report. Spine (Phila Pa 1976). 2002;27(19):E419–E422. doi:10.1097/00007632-200210010-00022
2. Sidhu GS, Kepler CK, Savage KE, et al. Neurological deficit due to cement extravasation following a vertebral augmentation procedure. J Neurosurg Spine. 2013;19(1):61–70. doi:10.3171/2013.4.SPINE12978
3. Chen YJ, Tan TS, Chen WH, et al. Intradural cement leakage: a devastatingly rare complication of vertebroplasty. Spine (Phila Pa 1976). 2006;31(12):E379–E382. doi:10.1097/01.brs.0000219495.57470.67
4. Chen JK, Lee HM, Shih JT, et al. Combined extraforaminal and intradiscal cement leakage following percutaneous vertebroplasty. Spine (Phila PA 1976). 2007;32(12):E358–E362. doi:10.1097/BRS.0b013e31805c0b25
5. Zhao Y, Liu T, Zheng Y, et al. Successful percutaneous retrieval of a large pulmonary cement embolus caused by cement leakage during percutaneous vertebroplasty: case report and literature review. Spine (Phila PA 1976). 2014;39(26):E1616–E1621. doi:10.1097/BRS.0000000000000613
6. Chung SE, Lee SH, Kim TH, et al. Renal cement embolism during percutaneous vertebroplasty. Eur Spine J. 2006;15(Suppl S5):590–594. doi:10.1007/s00586-005-0037-0
7. Choe DH, Marom EM, Ahrar K, et al. Pulmonary embolism of polymethyl methacrylate during percutaneous vertebroplasty and kyphoplasty. AJR Am J Roentgenol. 2004;183(4):1097–1102. doi:10.2214/ajr.183.4.1831097
8. Iliopoulos P, Korovessis P, Vitsas V. PMMA embolization to the left dorsal foot artery during percutaneous vertebroplasty for spinal metastases. Eur Spine J. 2014;23(Suppl S2):187–191. doi:10.1007/s00586-013-2919-x
9. Abdelrahman H, Siam AE, Shawky A, et al. Infection after vertebroplasty or kyphoplasty. A series of nine cases and review of literature. Spine J. 2013;13(12):1809–1817. doi:10.1016/j.spinee.2013.05.053
10. Kamano H, Hiwatashi A, Kobayashi N, et al. New vertebral compression fractures after prophylactic vertebroplasty in osteoporotic patients. AJR Am J Roentgenol. 2011;197(2):451–456. doi:10.2214/AJR.10.5937
11. Wang X, Peng Y, Qiu J, et al. Spinal subdural and epidural hematomas after vertebroplasty for compression fracture: a case report. Spinal Cord Ser Cases. 2018;4(1):1–4. doi:10.1038/s41394-018-0120-5
12. Fang M, Zhou J, Yang D, et al. Management and outcomes of spinal epidural hematoma during vertebroplasty: case series. Medicine (Baltimore). 2018;97(21):
13. Cosar M, Sasani M, Oktenoglu T, et al. The major complications of transpedicular vertebroplasty. J Neurosurg Spine. 2009;11(5):607–613. doi:10.3171/2009.4.SPINE08466
14. Lee KD, Sim HB, Lyo IU, et al. Delayed onset of spinal subdural hematoma after vertebroplasty for compression fracture: a case report. Korean J Spine. 2012;9(3):285–288. doi:10.14245/kjs.2012.9.3.285
15. Mattei TA, Rehman AA, Dinh DH. Acute spinal subdural hematoma after vertebroplasty: a case report emphasizing the possible etiologic role of venous congestion. Global Spine J. 2015;5(5):e52–e58. doi:10.1055/s-0035-1544155
16. von der Brelie C, Fiss I, Rohde V. Multilevel spinal combined subdural/subarachnoid hemorrhage resulting in paraplegia: an unusual complication of kyphoplasty. J Neurol Surg a Cent Eur Neurosurg. 2019;80(3):220–222. doi:10.1055/s-0038-1676594
17. Tropeano MP, La Pira B, Pescatori L, et al. Vertebroplasty and delayed subdural cauda equina hematoma: review of literature and case report. World J Clin Cases. 2017;5(8):333–339. doi:10.12998/wjcc.v5.i8.333
18. Yin P, Li Z, Zhu S, et al. The treatment of osteoporotic thoraco-lumbar burst fractures by unilateral percutaneous kyphoplasty: a prospective observation study. Eur J Pain. 2020;24(3):659–664. doi:10.1002/ejp.1516
19. Domenicucci M, Mancarella C, Santoro G, et al. Spinal epidural hematomas: personal experience and literature review of more than 1000 cases. J Neurosurg Spine. 2017;27(2):1–11. doi:10.3171/2016.12.SPINE15475
20. Özger Ö, Kaplan N. Spontaneous spinal epidural hematoma following warfarin treatment: case report. J Turk Spinal Surg. 2020;31(2):108–110. doi:10.4274/jtss.galenos.2020.93
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.