")
Back to Journals » Local and Regional Anesthesia » Volume 14
Spinal Anesthesia Using Ultra-Low-Dose Isobaric Bupivacaine with Intrathecal Morphine-Fentanyl for Bilateral Low Extremity Procedures in a Geriatric Patient with Recent Myocardial Infarction and Percutaneous Coronary Intervention
Authors Rukewe A , Nanyalo-Nashima L, Olivier N
Received 21 October 2020
Accepted for publication 30 December 2020
Published 22 January 2021 Volume 2021:14 Pages 7—11
DOI https://doi.org/10.2147/LRA.S287975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Stefan Wirz
Ambrose Rukewe,1,2 Linea Nanyalo-Nashima,2 Nicola Olivier2
1University of Namibia, School of Medicine, Surgery & Anesthesiology Department, Hage Geingob Campus, Windhoek, Namibia; 2Department of Anaesthesia, Windhoek Central & Katutura State Hospitals, Windhoek, Namibia
Correspondence: Ambrose Rukewe
University of Namibia, School of Medicine, Surgery & Anesthesiology Department, Hage Geingob Campus, Windhoek, Namibia
Tel +264-81-484-0892
Email [email protected]
Abstract: A recent inferior ST-elevation myocardial infarction and percutaneous coronary intervention in an elderly female patient scheduled for bilateral lower extremity operations simultaneously represent significant risks for re-infarction and mortality. Our index patient required an above-knee amputation of the left leg to prevent infection/progressing gangrene as well as application of a back-slab for the conservative management of a fractured right femur. We employed spinal injection of ultra-low-dose 0.5% isobaric bupivacaine 4 mg with morphine 75 mcg plus fentanyl 10 mcg which provided adequate anesthesia for radical amputation, effective postoperative analgesia and good hemodynamic stability.
Keywords: recent myocardial infarction, percutaneous coronary intervention, geriatric, bilateral lower extremity operations, ultra-low-dose, isobaric bupivacaine
Introduction
A recent inferior ST-elevation myocardial infarction (STEMI) and percutaneous coronary intervention (PCI) in an elderly female patient pose significant risks for morbidity and mortality, if exposed to surgery early.1 The American Heart Association/American College of Cardiology (AHA/ACC) recommended that elective surgeries be delayed and when an urgent/emergency surgery becomes necessary, surgical intervention must proceed with appropriate monitoring and therapies tampered by clinical assessment using a multidisciplinary approach.2 In our index patient, we identified the following risk factors: age 74 years, history of hypertension and smoking, STEMI and drug-eluting (Biomatrix) stent insertion 14 days prior, co-existing right humeral and femur fractures, widespread atherosclerosis and thrombi with potential for arterial embolization, low-molecular weight heparin anticoagulant therapy and the need for bilateral lower limb operations simultaneously. There are few reports of peripheral nerve blocks (PNBs) and low-dose unilateral spinal anesthesia (SA) for above-knee amputation (AKA) in high-risk patients but an ultra-low-dose isobaric bupivacaine with intrathecal injections of morphine-fentanyl has not been reported.3–5 We hereby describe our anesthetic management of this case.
Case Report
A 74-year-old female patient, 45 kg and 155 cm tall, American Society of Anesthesiologists’ (ASA) physical status IV, was referred to Katutura Intermediate Hospital, Windhoek, Namibia to the Vascular surgery and Orthopedic units. She reportedly fell off a ladder on 13 August 2020 due to syncope while tending her garden and sustained fractures to her right proximal humerus and right distal femur. Her left leg was found to be discolored, just below the knee. The patient, who admitted to smoking cigarettes (over 40 pack-years), was a known hypertensive on treatment. The report of her electrocardiography (ECG) was: ventricular rate 78 beats/min, normal sinus rhythm, normal QRS axis, ST segment elevation in inferolateral leads (II, III, aVF, V5-V6), reciprocal changes in leads V1-V3 consistent with Infero-lateral STEMI (Figure 1). Figures 2 and 3 are images of computed tomography (CT) angiogram showing the right coronary artery lesion before and after PCI. She had a drug-eluting (Biomatrix) stent implanted following which the cardiologist placed her on subcutaneous low-molecular-weight heparin (Enoxaparin 40 mg 12 hourly) and aspirin75 mg. The plan was for her to receive orthopedic care of the fractures and amputation for the gangrenous left leg before starting long-term clopidogrel. She was scheduled for AKA of the left leg and right distal femur locking plate. Following a discussion between the anesthesiologists, vascular and orthopedic surgeons, the decision was taken to proceed with the left AKA and manage the fractured femur with a back-slab conservatively. In preparing her for surgery, she was instructed in the numerical rating scale [NRS] for pain assessment, where 0 represented no pain and 10, indicated worst pain imaginable. She was transfused with 3 units of packed red cell to correct anemia (hemoglobin concentration was raised from 6.9 g/dL to 12.7 g/dL) and 1 mega unit of platelet which raised the platelet count from 38 x 109/L to 182 x 109/L. Written informed consent was obtained from the patient and relation for the publication of this case report including the associated images. Institutional review is not required for case reports; we have ensured anonymity in our report of this case.
 |
Figure 1 ECG showing inferolateral elevation myocardial infarction. |
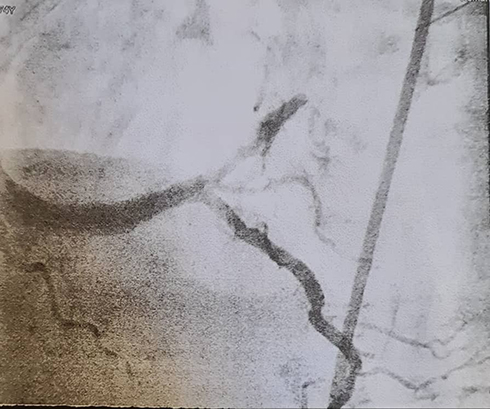 |
Figure 2 CT angiogram showing right coronary artery lesion. |
 |
Figure 3 CT angiogram post percutaneous coronary intervention. |
In the operating room, monitoring consisted of non-invasive blood pressure (NIBP), ECG, heart rate and oxygen saturation (SaO2). The baseline heart rate was 92 b/min, BP 130/70 mmHg and SaO2 92% on room air. We administered intravenous (IV) dexamethasone 4 mg and metoclopramide 10 mg as prophylaxis for nausea and vomiting (our preferred choice, ondansetron was unavailable). In order to make lateral positioning tolerable due to the right humeral and right distal femur fractures, 50 mcg fentanyl was injected intravenously and lumbar puncture performed by the most experienced anesthesiologist available succeeded at the first attempt using 25G pencil-point Spinocan® (B Braun, Melsungen, Germany) needle. A 0.5% isobaric bupivacaine 4 mg with preservative-free morphine 75 mcg plus fentanyl 10 mcg (total volume of the LA mixture was 1.35 mL) was injected intrathecally. The patient was then placed supine and sensory block was confirmed up to L1 dermatome with modified Bromage score of 2 (unable to flex knee but able to flex ankle). She was given a total of 600 mL Ringers’ lactate solution, IV paracetamol 1 g and supplemental oxygen via nasal prongs at 3 L/min was commenced which improved the SaO2 to 99%. The patient remained hemodynamically stable throughout the left AKA and right femur back-slab application that lasted 42 minutes, heart rate ranged between 70 and 85 beats/min, systolic blood pressure 100–130 mmHg, diastolic blood pressure 50–75 mmHg. A cheerful theater environment was ensured with music, and the patient received water (up to a total of 30 mL) at intervals orally to moisten her tongue. Postoperatively, the patient was observed in the recovery room for about 30 minutes before being transferred to a monitored bed on the ward. Monitoring included NRS score for pain, respiratory depression parameters such as respiratory rate >10 breaths/min and SaO2 >90%. Her first analgesic request was 6 hours after surgery and the NRS score ranged between 0/10 and 3/10 which was managed with oral codeine-paracetamol tablets. She was discharged from the orthopedic service on the 11th postoperative day in stable conditions.
Discussion
This case report illustrates that an ultra-low-dose bupivacaine-opioid combination is a viable option in high-risk patients undergoing AKA for providing effective surgical anesthesia and postoperative analgesia with minimal hemodynamic disruption. Peripheral nerve block (PNB) and low-dose unilateral spinal anesthesia has been shown to offer satisfactory anesthesia as well as good hemodynamic stability, going by a few case reports and case series of patients who underwent AKA.3–7 Our test case was scheduled for bilateral lower extremity procedures which precluded the use of hyperbaric bupivacaine for a unilateral spinal block or performing PNB because of the greater risk of local anesthetic systemic toxicity (LAST). Furthermore, complete analgesia/anesthesia are sometimes elusive under PNB despite targeting femoral, lateral femoral cutaneous, obturator (anterior and posterior divisions) and sciatic nerves separately with LA volumes and concentrations approaching the maximum safe threshold – some authors have admitted to exceeding the recommended doses without adverse toxic effects.3,4
Although Moreira et al8 posited that the mode of anesthesia did not have a significant effect on perioperative outcomes after major lower extremity amputation in functionally impaired geriatric patients, we felt it was better to avoid general anesthesia (GA) in view of its propensity to cause hemodynamic instability due to increased stress response, increased myocardial irritability and decreased systemic vascular resistance. Conventional spinal anesthesia has been considered as the gold standard approach for lower limb surgeries but many authors agree that they are best avoided in patients with poor cardiovascular reserve because significant hemodynamic disruption might ensue.4,9 Our ultra-low-dose technique helped us to maintain the MAP and avoid spinal-induced hypotension which is associated with perioperative adverse cardiac events.10 Using ultra-low-dose neuraxial technique limits the blocked spinal segments, the extent of the sympathetic blockade and minimizes the effect on the systemic vascular resistance.11 Being able to maintain MAP coupled with supplemental oxygen administration could have contributed to maintaining the balance between myocardial oxygen demand and supply, in our test case.
The decision to employ this ultra-low dose LA-opioid technique was not taken lightly because neuraxial anesthesia is not without risks in cardiac patients, we proceeded having weighed the benefits. Our test patient having had recent stent inserted for STEMI was placed on antithrombotics – low molecular weight heparin (enoxaparin) and aspirin, required urgent orthopedic management of fractured humerus, femur and AKA. We had to optimize her condition by correcting anemia with packed red cell transfusion, thrombocytopenia with one mega unit of plasma as well as withholding enoxaparin for 24 hours to minimize the risk of spinal hematoma formation. We believe that following the American Society of Regional Anesthesia [ASRA] guidelines on regional anesthesia in patients receiving anticoagulants made neuraxial anesthesia auspicious in this patient.12 We were cautious to assign the more experienced anesthesiologist to site the spinal using a fine pencil-point needle in cognizance of the difficulty with lateral positioning of the patient. Combined spinal epidural anesthesia (CSEA) was our second option for managing this case especially because it affords the use of low-dose LA-opioid combination and the possibility of prolonging the anesthetic, if required. However, both the AKA and back-slab application were straightforward, our single-shot spinal anesthesia proved safe, cost-effective and applicable under the guidelines for the use of antithrombotic agents in the setting of neuraxial procedures.
We added low-dose morphine-fentanyl combination to an ultra-low-dose isobaric bupivacaine. Intrathecal combination of hydrophilic and lipophilic opioids is common practice in some countries.13–17 Studies have reported intraoperative pain following 100–200 mcg spinal morphine alone due to up to 30–60 minutes delayed onset of action. Whereas fentanyl, being highly lipid soluble (580:1) compared to morphine acts faster and its rapid clearance from the cerebrospinal fluid limits its effect to the intraoperative and immediate postoperative periods. The morphine-fentanyl combination actually complements their different pharmacokinetic and pharmacodynamic properties for superior perioperative analgesia. Intrathecal morphine at a dose of 75 mcg has been shown to be the minimum effective analgesic dose and as little as 10 mcg fentanyl has been reported to improve intraoperative analgesia.13,14,16,18 Neuraxial opioids have dose-related side effects, the most concerning is respiratory depression and the others are pruritus, nausea and vomiting. Our low-dose neuraxial opioid combinations were an attempt at striking a balance between optimal perioperative analgesia and reducing dose-related adverse effect.18 We were cautious when we had to administer IV fentanyl 50 mcg to facilitate positioning the patient for spinal as it could increase the risk of respiratory depression, even that dose was titrated to effect. The postoperative parameters monitored to exclude respiratory depression included respiratory rate >10 breaths/min and SaO2 >90%.19 Pruritus, nausea and vomiting, which are recognized complications of intrathecal opioids were not observed in our case patient.
In conclusion, we believe that the technique we employed in this index case might be suitable for other high-risk patients.
Author Contributions
All authors contributed to the work reported in the conception, execution, data acquisition and analysis; participated in drafting, revising the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
We (the authors) report no conflicts of interest in this work.
References
1. Livhits M, Ko CY, Leonardi MJ, Zingmond DS, Gibbons MM, de Virgilio C. Risk of surgery following recent myocardial infarction. Ann Surg. 2011;253(5):857–864. doi:10.1097/SLA.0b013e3182125196
2. Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;64(22):e77–e137. doi:10.1016/j.jacc.2014.07.944
3. Karm MH, Lee S, Yoon SH, Lee S, Koh W. A case report: the use of ultrasound guided peripheral nerve block during above knee amputation in a severely cardiovascular compromised patient who required continuous anticoagulation. Medicine (Baltimore). 2018;97(9):e9374. doi:10.1097/MD.0000000000009374
4. Chandran R, Beh ZY, Tsai FC, Kuruppu SD, Lim JY. Peripheral nerve blocks for above knee amputation in high-risk patients. J Anaesthesiol Clin Pharmacol. 2018;34(4):458–464. doi:10.4103/joacp.JOACP_346_17
5. Chuah KH, Thong CL, Krshnan H, Chan L. Low dose unilateral spinal anaesthesia for lower limb amputation in critically ill patients. Med J Malaysia. 2007;62(1):81–82.
6. Bech B, Melchiors J, Børglum J, Jensen K. The successful use of peripheral nerve blocks for femoral amputation. Acta Anaesthesiol Scand. 2009;53:
7. Chia N, Low TC, Poon KH. Peripheral nerve blocks for lower limb surgery – A choice anaesthetic technique for patients with a recent myocardial infarction? Singapore Med J. 2002;43:583–586.
8. Moreira CC, Farber A, Kalish JA, et al. The effect of anesthesia type on major lower extremity amputation in functionally impaired elderly patients. J Vasc Surg. 2016;63(3):696–701. doi:10.1016/j.jvs.2015.09.050
9. Guay J, Choi P, Suresh S, et al. Neuraxial blockade for the prevention of postoperative mortality and major morbidity: an overview of Cochrane systematic reviews. Cochrane Database Syst Rev. 2014;6(1):CD010108. doi:10.1002/14651858.CD010108.pub2
10. Walsh M, Devereaux PJ, Garg AX, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery toward an empirical definition of hypotension. Anesthesiology. 2013;119(3):507–515. doi:10.1097/ALN.0b013e3182a10e26
11. Kuusniemi KS, Pihlajamäki KK, Pitkänen MT, Korkeila JE. Low‐dose bupivacaine: a comparison of hypobaric and near isobaric solutions for arthroscopic surgery of the knee. Anaesthesia. 1999;54(6):540–545. doi:10.1046/j.1365-2044.1999.00855.x
12. Horlocker TT, Vandermeuelen E, Kopp SL, Gogarten W, Leffert LR, Benzon HT. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American society of regional anesthesia and pain medicine evidence-based guidelines (fourth edition). Reg Anesth Pain Med. 2018;43(3):263–309.
13. Hein A, Gillis-Haegerstrand C, Jakobsson JG. Neuraxial opioids as analgesia in labour, caesarean section and hysterectomy: a questionnaire survey in Sweden. F1000Research. 2017;6:133.
14. Al-Kazwini H, Sandven I, Dahl V, Rosseland LA. Prolonging the duration of single-shot intrathecal labour analgesia with morphine: a systematic review. Scand J Pain. 2016;13:36–42. doi:10.1016/j.sjpain.2016.06.010
15. Carvalho B, Butwick A. Postoperative analgesia: epidural and spinal techniques. In: Chestnut D, Wong C, Tsen L, Ngan Kee W, Beilin Y, Mhyre J, editors. Chestnut’s Obstetric Anesthesia Principles and Practice.
16. Sawi W, Choy YC. A comparative study of post operative analgesia, side effects profile and patient satisfaction using intrathecal fentanyl with and without morphine 0.1 mg in caesarean section. Middle East J Anaesthesiol. 2013;22:21–26.
17. Weigl W, Bieryło A, Wielgus M, Krzemień-Wiczyńska Ś, Kołacz M, Dąbrowski MJ. Perioperative analgesia after intrathecal fentanyl and morphine or morphine alone for cesarean section: a randomized controlled study. Medicine (Baltimore). 2017;96(48):e8892. doi:10.1097/MD.0000000000008892
18. Sultan P, Guiterrez MC, Carvalho B. Neuraxial morphine and respiratory depression finding the right balance. Drugs. 2011;71(14):1807–1819. doi:10.2165/11596250-000000000-00000
19. Horlocker TT, Burton AW, Connis RT, et al. Practice guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid administration. Anesthesiology. 2009;110:218–230.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.