Back to Journals » Journal of Pain Research » Volume 19
Sphenopalatine Ganglion Block for Postdural Puncture Headache in the Obstetric Population: A Narrative Review
Received 6 March 2026
Accepted for publication 28 May 2026
Published 6 June 2026 Volume 2026:19 607406
DOI https://doi.org/10.2147/JPR.S607406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Karina Gritsenko
Ke Hao, Weilong Jiang
Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
Correspondence: Ke Hao, Department of Anesthesiology, The First Affiliated Hospital, Zhejiang University School of Medicine, 79 Qingchun Road, Hangzhou, Zhejiang, People’s Republic of China, Tel +8618767108776, Email [email protected]
Abstract: Postdural puncture headache (PDPH) frequently complicates neuraxial anesthesia, delaying patient recovery and reducing quality of life after surgery. Epidural blood patch (EBP), the conventional standard of care, is effective but not without risks. Therefore, safer, less invasive alternatives are of increasing interest. The sphenopalatine ganglion block (SPGB) is a minimally invasive regional analgesic technique that has drawn attention in recent years for managing PDPH, largely because it is non‑opioid and generally well tolerated. In this narrative review, we summarize current knowledge on the anatomical basis, proposed mechanisms, procedural techniques, and clinical evidence (mostly from case reports and case series) for SPGB in the obstetric population, and we discuss key controversies that remain unresolved.
Keywords: sphenopalatine ganglion, headache, post-dural puncture, anesthesia, obstetrical, postpartum period, nerve block
Introduction
Neuraxial anesthesia has become the first-line and most widely used option for labor analgesia and cesarean section anesthesia, owing to its reliable analgesic efficacy and acceptable safety profile for both mother and fetus.1 However, this procedure carries inherent risks, with accidental dural puncture being a common complication, occurring in approximately 1.5% of cases,2 and of those, 50% to 80% will subsequently develop PDPH.3 As one of the most prevalent complications following obstetric neuraxial anesthesia, PDPH can significantly delay postpartum recovery and impair the quality of life of parturients.4
Current clinical management of PDPH is primarily based on conservative measures, including bed rest, aggressive fluid hydration, and caffeine administration. However, these approaches have limitations such as delayed onset, prolonged treatment courses, and limited efficacy in moderate-to-severe cases. The EBP is considered the “gold standard” for PDPH treatment, as it seals the dural puncture site with autologous blood to halt cerebrospinal fluid (CSF) leakage, providing rapid relief. Nevertheless, as an invasive procedure, EBP carries potential risks including infection, nerve injury, and exacerbated back pain. Some patients may require multiple punctures, which increases medical trauma and patient discomfort.5,6
Several professional societies have published clinical practice guidelines for managing PDPH. The American Society of Anesthesiologists (ASA) guidelines on obstetric anesthesia recommend starting with conservative measures and reserving EBP for moderate‑to‑severe cases that do not improve with initial treatment. More recently, the multi‑society consensus guidelines from the American Society for Regional Anesthesia and Pain Medicine (ASRA) noted that SPGB is not routinely recommended because the supporting evidence is of low certainty.7,8 This observation only strengthens the case for better‑designed studies on SPGB in the obstetric population. Compared to EBP, SPGB is associated with faster headache relief and is well tolerated in parturients with PDPH.9
The sphenopalatine ganglion (SPG) is the largest parasympathetic ganglion in the craniofacial region and plays a key role in regulating intracranial vascular tone and pain transmission. SPGB was first reported for PDPH by Cohen et al in 2001.10 It has since been used for migraine and cluster headache,11 and its application has expanded to secondary headaches. Preliminary evidence suggests SPGB may relieve PDPH by modulating vascular tone, improving CSF circulation, and inhibiting pain pathways. However, existing studies are limited, and controversies remain regarding efficacy, optimal technique, and drug regimens.
In this narrative review, we summarize the current evidence on SPGB for PDPH in the obstetric population, discuss its advantages and limitations, and identify directions for future research. Unlike existing systematic reviews that focus primarily on efficacy, our review emphasizes anatomical feasibility, technical considerations, pharmacokinetic changes in pregnancy, and unresolved controversies that require further investigation.
Methods
A comprehensive literature search was performed across PubMed/MEDLINE, Embase, and the Cochrane Library, with no restrictions on language or publication date. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords relevant to sphenopalatine ganglion block, postdural puncture headache, and the obstetric population, including “sphenopalatine ganglion”, “pterygopalatine ganglion”, “SPG block”, “postdural puncture headache”, “PDPH”, “spinal headache”, “dural puncture headache”, “obstetric”, “parturient”, “postpartum”, “pregnancy”, “labor” and “cesarean section”. Eligible study types encompassed randomized controlled trials, case reports, and retrospective observational studies.
Anatomy
The SPG is a fusiform structure about 5 mm in diameter, situated within the pterygopalatine fossa—a key anatomical space at the skull base bounded by the maxilla, sphenoid bone, and palatine bone.12–14 It receives three main types of fibers: parasympathetic preganglionic fibers from the greater petrosal nerve, sympathetic postganglionic fibers from the deep petrosal nerve, and sensory fibers from the maxillary division of the trigeminal nerve. Its efferent parasympathetic postganglionic fibers innervate the lacrimal gland, nasal mucosa, and intracranial blood vessels, regulating glandular secretion and cerebrovascular tone. Sympathetic fibers mainly modulate vascular activity to maintain cerebral circulatory homeostasis.
The anatomical location of the SPG gives rise to several potential access routes. In clinical practice, however, the two most commonly used are the transnasal and percutaneous approaches. The transnasal approach utilizes the nasal cavity as a natural operative corridor, with the ganglion precisely located approximately 1 cm medial to the maxillary sinus ostium and 2 cm posterior to the inferior turbinate. This technique avoids skin puncture and minimizes trauma. The percutaneous approach, however, requires needle insertion through the pterygomaxillary fissure to access the pterygopalatine fossa, demanding precise anatomical localization to avoid damaging nearby structures such as the maxillary artery and trigeminal nerve branches.14
For the obstetric population, the transnasal route is common, but whether it truly blocks the SPG remains debatable. Some experts have raised doubts:15,16 the local anesthetic has to cross the nasal mucosa and several fascial layers before reaching the SPG deep inside the pterygopalatine fossa. It is unclear whether enough drug reaches the ganglion to produce effective neural blockade. In fact, some researchers have suggested that any clinical benefit from transnasal SPGB may come from systemic absorption or local mucosal anesthesia rather than from a direct effect on the SPG itself. This uncertainty should be kept in mind when interpreting study results.
More than four anatomical access routes to the pterygopalatine fossa have been described, including transnasal, transoral, percutaneous (via the pterygomaxillary fissure or infrazygomatic approach), and transorbital approaches.17 For the obstetric population, the transnasal route is the most practical and most commonly reported, thanks to its minimally invasive nature and bedside feasibility. The ultrasound-guided percutaneous approach has also been described in case reports involving postpartum women,18,19 though it requires proper patient positioning (supine with head rotated) and operator training. The transoral and transorbital routes are not recommended in obstetric patients due to higher complication risks (eg., infection, orbital injury) and limited supporting evidence.
Mechanism of Action of SPGB in the Treatment of PDPH
The core pathophysiological mechanism of PDPH is CSF leakage following dural puncture, which causes intracranial pressure (ICP) to drop.20 According to the Monro-Kellie principle, the total volume of intracranial components—brain parenchyma, CSF, and blood—remains relatively constant. When CSF volume decreases, cerebral blood vessels widen to maintain intracranial homeostasis — a process driven mainly by parasympathetic signals mediated by the SPG.12,21 Parasympathetic activation triggers the release of vasodilatory transmitters (eg., acetylcholine) from postganglionic SPG fibers. This leads to excessive dilation of meningeal and cerebral blood vessels. This vasodilation further increases vascular permeability and promotes the leakage of inflammatory mediators, which in turn activates trigeminal‑nerve endings in the meninges. Pain signals are then transmitted to the central nervous system, leading to central sensitization. The result is the typical orthostatic headache of PDPH, often with nausea, vomiting, neck stiffness, or trouble with hearing or vision. In severe cases, patients may also develop emotional disorders such as anxiety and depression, which not only interfere with breastfeeding and parent-infant interaction but also add to the medical and economic burden on families and society.
As a minimally invasive nerve block technique, SPGB has emerged as a promising treatment for PDPH. Its core mechanism of action involves blocking nerve signals through the SPG with local anesthetics, thereby interrupting parasympathetic vasodilatory signaling pathways and reversing excessive cerebrovascular dilation. Concurrently, SPGB reduces the release of inflammatory mediators and dampens the activation of meningeal pain receptors, which lessens pain signaling and central sensitization, ultimately leading to the relief of PDPH symptoms. Figure 1 summarizes pathophysiological mechanism of PDPH and the mechanism of action of SPGB to treat it.
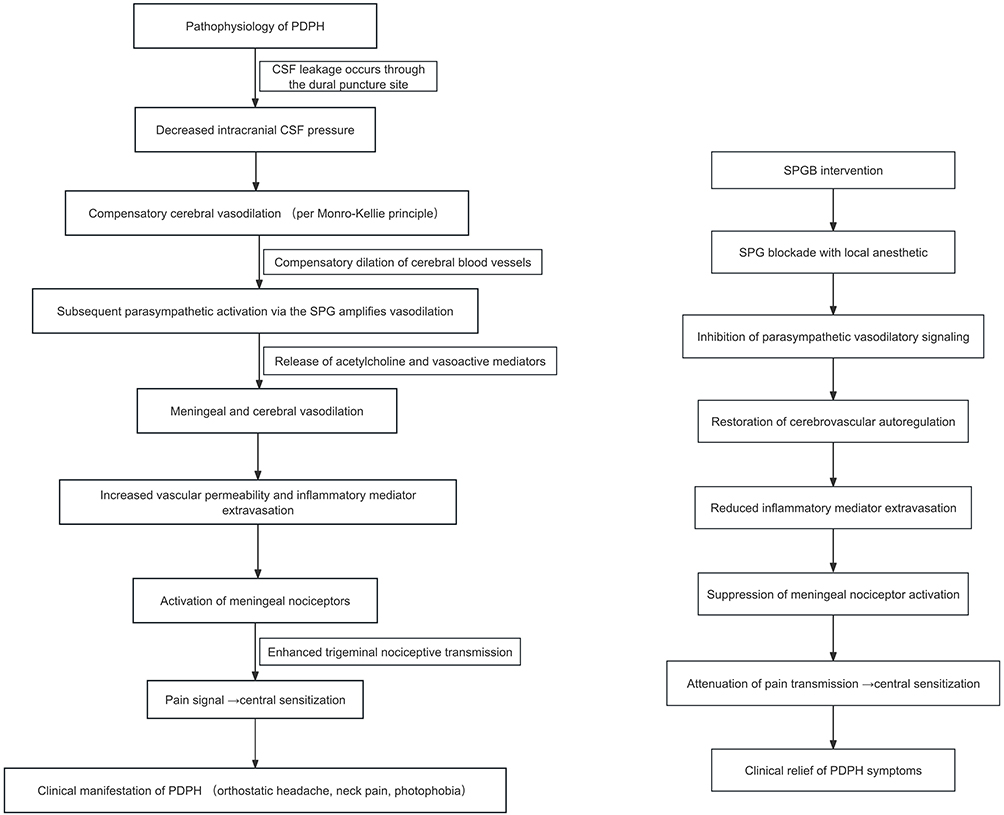 |
Figure 1 Schematic diagram illustrating the pathophysiological mechanism of PDPH and the therapeutic mechanism of SPGB. Pathophysiology of PDPH (left panel), Mechanism of SPGB (right panel). The arrows trace the cause‑and‑effect chain from the initial dural puncture all the way to the final clinical symptoms. Each step triggers the next, building the full pathological mechanism of PDPH. Rightward arrow (→) indicates a direct causal. Abbreviations: CSF, cerebrospinal fluid; PDPH, postdural puncture headache; SPG, sphenopalatine ganglion; SPGB, sphenopalatine ganglion block. |
Pregnancy and the postpartum period bring several physiological changes that can affect both the development of PDPH and the response to SPGB. For example, blood volume increases by roughly 40–50% during pregnancy, estrogen and progesterone levels rise substantially, and cerebrospinal fluid dynamics are altered. These changes may alter the usual relationship between CSF leakage and symptom severity. After delivery, fluid shifts and adjustments in autonomic nervous system activity might also influence SPGB effectiveness. Clinicians should keep these factors in mind when using SPGB in obstetric patients, even though the current evidence does not yet support specific recommendations for any subgroup.
Development and Optimization of SPG Block Techniques
The evolution of SPGB techniques has centered on enhancing targeting accuracy and reducing procedure-related discomfort. Currently, the primary technical approaches for the obstetric population with PDPH include the transnasal blind technique and the ultrasound-guided percutaneous technique. Optimal drug selection and standardized procedural protocols remain to be established.
The transnasal blind technique is the most widely applied method. The patient is positioned in the supine “sniffing position” — neck extended, head tilted back, nostrils facing upward. A long cotton-tipped applicator soaked with local anesthetic (one per nostril) is inserted along the superior border of the middle turbinate into the nasal cavity until it reaches the posterior nasopharynx. Upon encountering resistance, the applicator is left in place for 10 to 15 minutes to complete the block.22 This transnasal blind technique is simple to perform, requires no specialized equipment, and is suitable for bedside emergency intervention. However, the block efficacy is highly dependent on the operator’s experience, and mislocalization may lead to suboptimal therapeutic outcomes. Additionally, clinical studies have reported that PDPH was successfully treated in obstetric patients using intranasal lidocaine via a mucosal atomization device or a 20G intravenous cannula.23,24
In recent years, ultrasound guidance has improved the precision of SPGB. Real-time ultrasound visualization of the SPG within the pterygopalatine fossa via the percutaneous route allows targeted and accurate drug delivery. This can enhance the success rate of the block while reducing the dose of local anesthetic and associated adverse effects. Currently, clinical evidence for ultrasound-guided SPGB in obstetric PDPH remains limited to case reports18 and case series.19
Table 1 summarizes the methods, local anesthetic concentrations and doses, and outcomes of SPGB for obstetric PDPH. Most case reports and case series used the transnasal approach. Lidocaine at 2% was the most common local anesthetic. Several studies reported successful headache relief.
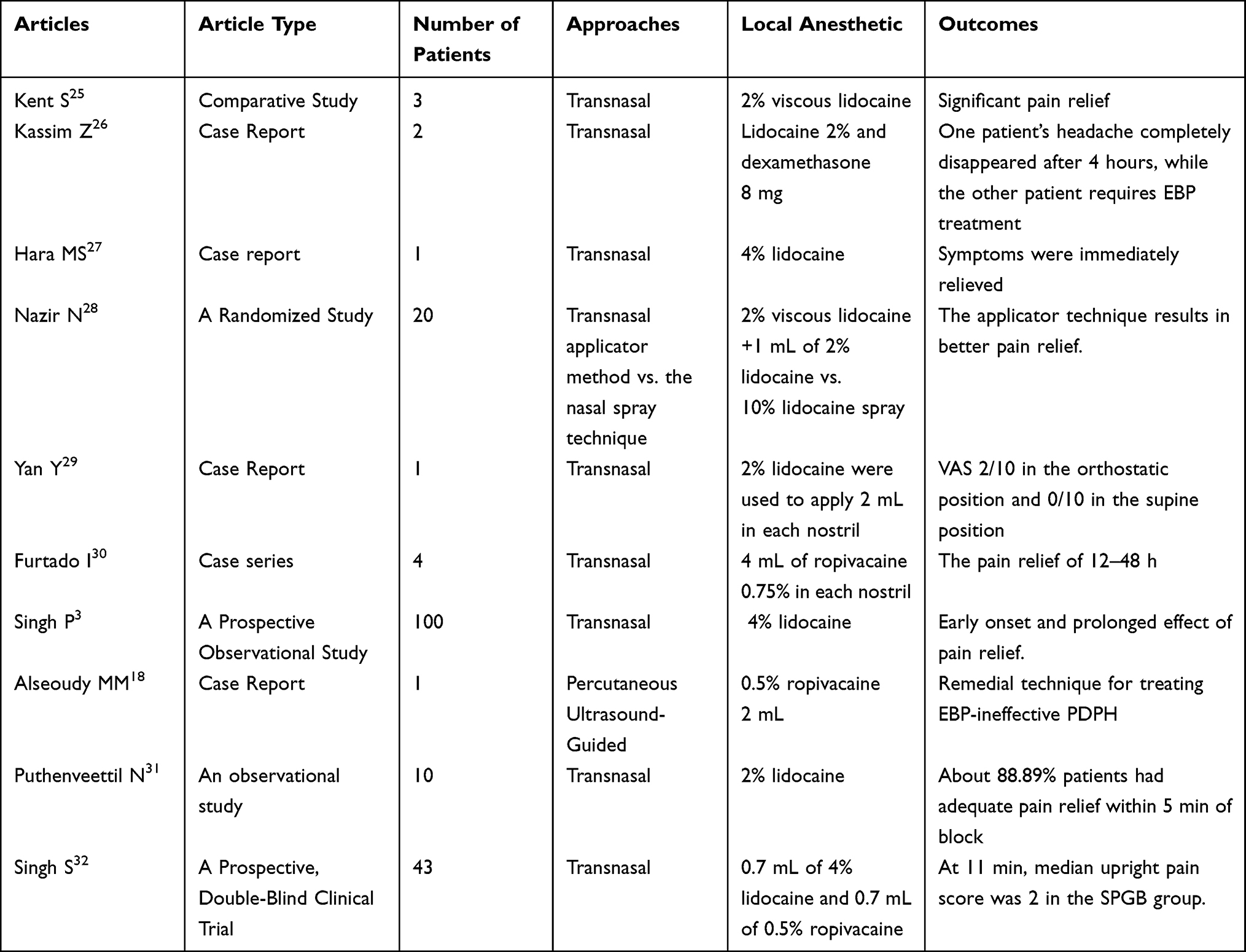 |
Table 1 Selected Clinical Studies on SPGB for PDPH in Obstetric Patients |
No studies have directly compared different SPGB techniques in obstetric patients. Based on the case reports and small series available, the transnasal blind technique appears to help patients. When side effects occur, they tend to be mild and short‑lived — for instance, nasal discomfort or minor epistaxis. The ultrasound‑guided percutaneous approach might deliver the local anesthetic more accurately and possibly lead to better results, but so far only case reports support this.
Pregnancy and the postpartum period bring several physiological changes that can affect how local anesthetics behave in the body. Blood volume goes up by 40‑50%, and protein binding drops due to falling albumin levels — both of which alter drug distribution. Hormone levels also rise during pregnancy, which may influence drug metabolism.33 In addition, the nasal mucosa becomes more vascular,34 so intranasally administered drugs may be absorbed into the bloodstream more easily. Clinicians should keep these factors in mind when using SPGB in obstetric patients, although no specific dose adjustments have yet been established for this population.
Controversies and Limitations
Before we dive into specific controversies, it is worth being clear about the quality of the evidence we have. Most studies on SPGB for obstetric PDPH are case reports or case series; only a handful of randomized controlled trials exist. Sample sizes tend to be small, and many studies lack control groups or blinding. So any conclusions about efficacy or safety need to be treated with caution. The discussion that follows takes these limitations into account and points out where stronger evidence is most needed.
As a minimally invasive alternative for treating obstetric PDPH, SPGB has demonstrated acceptable safety and preliminary efficacy. However, numerous unresolved controversies persist in both clinical application and research, primarily focusing on the following three core aspects:
Local Anesthetic and Adjuvants
Currently, evidence regarding the optimal dosage, concentration, and adjuvants of local anesthetics for SPGB in PDPH treatment remains limited. Most studies employ 2%–4% lidocaine or 0.375%–0.5% ropivacaine, yet the volume of administration varies considerably, ranging from 1 mL to 4 mL per nostril. A systematic review of PDPH in obstetric patients indicated that 4% lidocaine was less effective than 2% lidocaine,35 although the underlying mechanism (eg., whether mucosal irritation from high-concentration local anesthetics affects block efficacy) remains unclear. The optimal drug regimen requires further investigation.
Several studies have attempted to combine dexamethasone as an adjuvant with local anesthetics, achieving acceptable outcomes in PDPH treatment.36 However, such evidence is derived solely from small-sample, randomized, single-blind controlled trials. Large-scale randomized controlled trials are lacking to validate the actual benefits of adjuvants. Furthermore, the optimal dosage, timing of administration, and safety profile (eg., potential hormonal effects on the postpartum mother) remain undetermined.
Heterogeneity Across Studies and Lack of Standardized Outcomes
A close look at the published literature shows considerable heterogeneity across studies, which makes it hard to draw firm conclusions. The main sources of this variability are as follows: some studies use the transnasal cotton‑tipped applicator, others use mucosal atomization devices, and still others use ultrasound‑guided percutaneous approaches. These methods differ markedly in how the local anesthetic is delivered, how deep it penetrates, and whether true SPG blockade is likely to be achieved. No study has directly compared one technique against another.
Lidocaine concentrations range from 2% to 4%, and ropivacaine from 0.375% to 0.5%. Volumes per nostril vary between 1 mL and 4 mL. One systematic review found that 4% lidocaine might work less well than 2% lidocaine,35 but why this happens remains unexplained. Without standardized regimens, pooling data for meta‑analysis is not possible.
Studies use different endpoints—for example, headache relief within 30 minutes, pain scores at 1 hour, or the need for a rescue EBP. This variety makes it difficult to compare results across studies. Standardized outcome measures would be helpful for future research.
Most studies are uncontrolled case reports or case series. This makes it hard to know whether the improvement seen is truly due to SPGB or simply reflects natural recovery or a placebo effect.
Timing and Frequency of Block Administration
Evidence on the optimal timing and repeat dosing of SPGB for obstetric PDPH is limited. Existing studies confirm that SPGB effectively alleviates symptoms whether given within 24 hours of PDPH diagnosis or later. However, early intervention (within 24 hours) may offer advantages such as shorter hospital stays, lower symptom recurrence, earlier return to daily activities, and reduced medical costs.37 These findings come from small observational studies and need confirmation in larger, prospective trials. No data are available to guide timing based on symptom severity (eg., mild orthostatic headache versus severe headache with nausea, vomiting, or visual disturbances).
Some patients have symptom recurrence after a single SPGB, but no studies have defined the ideal interval between repeat blocks or the maximum number of treatments. Safety data on potential harms of repeated blocks (eg., nasal mucosal injury or local anesthetic toxicity) are also lacking.
Long-Term Efficacy and Recurrence Rate
Most existing studies focus on short‑term outcomes (hours to days). Evidence on long-term prognosis and recurrence rates is insufficient. Although SPGB is a safe option, it does not eliminate the need for epidural blood patch (EBP) in all cases. When SPGB was given more than 24 hours after PDPH diagnosis, one study observed a higher symptom recurrence rate.37 Factors influencing recurrence remain poorly understood. Prospective research is needed to identify predictors of treatment failure.38
EBP remains the “gold standard” for PDPH treatment. Current evidence indicates that SPGB cannot fully replace EBP, and some patients with refractory PDPH still require EBP rescue. No systematic studies have examined predictors of SPGB failure (eg., block technique, drug regimen, patient characteristics). Moreover, where SPGB fits in the PDPH treatment pathway — for instance, as a first‑line minimally invasive option after failed conservative therapy or as a rescue after EBP — requires clarification through higher‑level evidence.
Comparison with EBP as the Standard of Care
EBP remains the standard treatment for PDPH.39 After a single procedure, reported success rates range from 70% to 98%. Only one retrospective study has directly compared SPGB with EBP in postpartum women. That study found faster headache relief with SPGB (15.6 minutes on average versus 87.5 minutes for EBP) and no new complications in the SPGB group.9 However, the study was non‑randomized and had selection bias. A side-by-side comparison of SPGB and EBP is presented in Table 2.
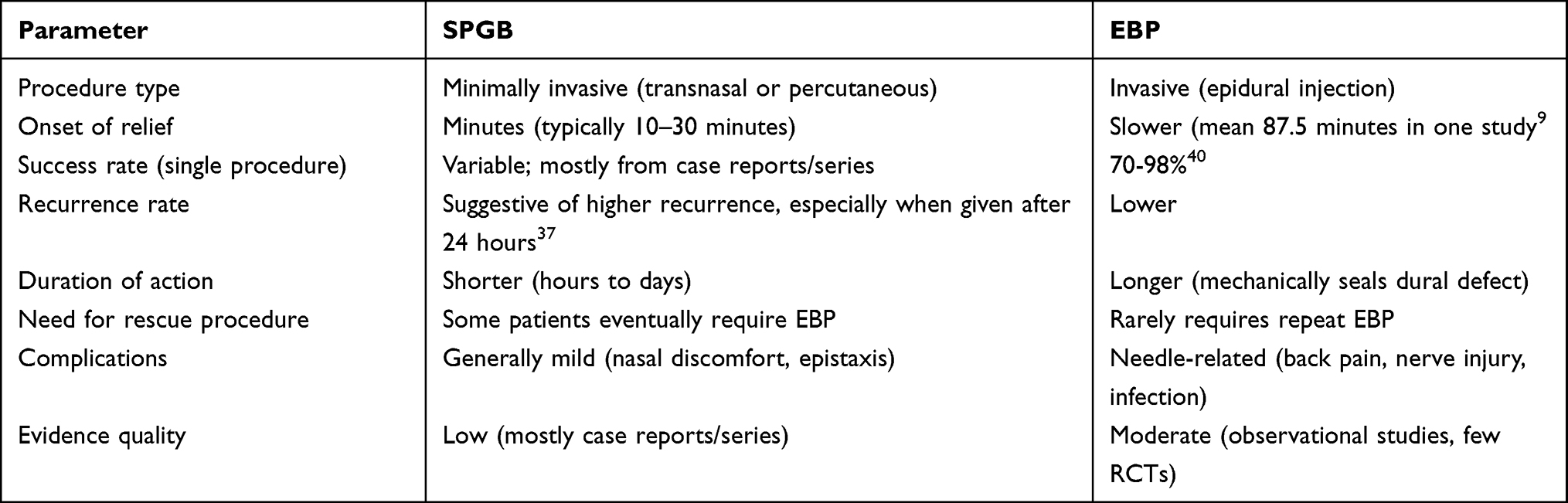 |
Table 2 Comparison Between SPGB and EBP for Obstetric PDPH |
Based on current evidence, SPGB cannot replace EBP as the standard of care. Nevertheless, it could be a reasonable minimally invasive option, especially for women who want to avoid the risks of an epidural procedure or in settings where EBP is not immediately available.
Conclusions
SPGB is a minimally invasive, non‑opioid technique for pain relief. It seems safe and may be effective for PDPH. By adjusting intracranial vascular tone, reducing neurogenic inflammation, and blocking pain signals, it offers a new treatment option. Several studies — including a few small randomized trials28,36 and a retrospective comparison9— suggest that SPGB may provide short-term relief and is generally well tolerated in obstetric patients with PDPH. That said, the overall evidence has clear limits: most studies are small and of low quality. Clinicians can choose between the transnasal and ultrasound‑guided percutaneous routes based on the patient’s situation and their own experience.
Still, several questions remain unanswered. We do not yet know the best local anesthetic or dose, the ideal timing for the block, how long any benefit lasts, or exactly where SPGB fits in the PDPH treatment pathway. Larger, well‑designed, multicenter prospective studies are needed to address these gaps.
Based on the available evidence, SPGB may be considered as a minimally invasive option for PDPH in obstetric patients, particularly when conservative measures have failed or when epidural blood patch is contraindicated or not immediately available. The transnasal route is the most practical and best-studied approach. A reasonable starting protocol is 2% lidocaine, 1–2 mL per nostril, using a cotton-tipped applicator left in place for 10–15 minutes. Patients should be monitored for symptom relief within 30 minutes, and the block can be repeated if needed.
Acknowledgments
The authors would like to thank all the researchers and healthcare professionals whose work contributed to the foundational knowledge in this field. We are also grateful to our colleagues in the Department of Anesthesiology for their insightful discussions and support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegler BH, Oehler B, Kranke P, et al. Postdural puncture headache in obstetrics: pathogenesis, diagnostics and treatment. Die Anaesthesiologie. 2022;71(8):646–9. doi:10.1007/s00101-022-01171-2
2. Alatni RI, Alsamani R, Alqefari A. Treatment and Prevention of Post-dural Puncture Headaches: a Systematic Review. Cureus. 2024;16(1):e52330. doi:10.7759/cureus.52330
3. Singh P, Ghatak T, Mani UA, et al. The effect of bilateral nasal sphenopalatine ganglion block in managing headaches after dural puncture following lower segment cesarean section: a prospective observational study. Cureus. 2025;17(3):e80289. doi:10.7759/cureus.80289
4. Kwak K-H. Postdural puncture headache. Korean J Anesthesiol. 2017;70(2):136–143. doi:10.4097/kjae.2017.70.2.136
5. Patel R, Urits I, Orhurhu V, et al. A comprehensive update on the treatment and management of postdural puncture headache. Curr Pain Headache Rep. 2020;24(6):24. doi:10.1007/s11916-020-00860-0
6. Li H, Wang Y, Oprea AD, et al. Postdural puncture headache—risks and current treatment. Curr Pain Headache Rep. 2022;26(6):441–452. doi:10.1007/s11916-022-01041-x
7. American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Practice guidelines for obstetric anesthesia: an updated report by the American society of anesthesiologists task force on obstetric anesthesia and the society for obstetric anesthesia and perinatology. Anesthesiology. 2016;124(2):271–300.
8. Uppal V, Russell R, Sondekoppam RV, et al. Evidence-based clinical practice guidelines on postdural puncture headache: a consensus report from a multisociety international working group. Reg Anesth Pain Med. 2024;49(7):471–501. doi:10.1136/rapm-2023-104817
9. Cohen S, Levin D, Mellender S, et al. Topical sphenopalatine ganglion block compared with epidural blood patch for postdural puncture headache management in postpartum patients: a retrospective review. Reg Anesth Pain Med. 2018;43(8):880–884. doi:10.1097/AAP.0000000000000840
10. Cohen S, Trnovski S, Zada Y. A new interest in an old remedy for headache and backache for our obstetric patients: a sphenopalatine ganglion block. Anaesthesia. 2001;56(6):606–607. doi:10.1111/j.1365-2044.2001.2094-34.x
11. Binfalah M, Alghawi E, Shosha E, et al. Sphenopalatine Ganglion block for the treatment of acute migraine headache. Pain Res Treat. 2018;2018:2516953. doi:10.1155/2018/2516953
12. Robbins MS, Robertson CE, Kaplan E, et al. The sphenopalatine ganglion: anatomy, pathophysiology, and therapeutic targeting in headache. Headache. 2016;56(2):240–258. doi:10.1111/head.12729
13. Nair AS, Rayani BK. Sphenopalatine ganglion block for relieving postdural puncture headache: technique and mechanism of action of block with a narrative review of efficacy. Korean J Pain. 2017;30(2):93–97. doi:10.3344/kjp.2017.30.2.93
14. Iwanaga J, Wilson C, Simonds E, et al. Clinical anatomy of blockade of the pterygopalatine ganglion: literature review and pictorial tour using cadaveric images. Kurume Med J. 2018;65(1):1–5. doi:10.2739/kurumemedj.MS651001
15. Narouze S. Topical intranasal lidocaine is not a sphenopalatine ganglion block. Reg Anesth Pain Med. 2021;46(3):276–279. doi:10.1136/rapm-2020-102173
16. Jespersen MS, Jaeger P, Ægidius KL, et al. Sphenopalatine ganglion block for the treatment of postdural puncture headache: a randomised, blinded, clinical trial. Br J Anaesth. 2020;124(6):739–747. doi:10.1016/j.bja.2020.02.025
17. Mahanty PR, Sen B, Anand R, et al. Sphenopalatine ganglion block for postdural puncture headache: a review of current evidence. World J Clin Cases. 2026;14(3). doi:10.12998/wjcc.v14.i3.114521
18. Alseoudy MM, Abd-Elmoaty WA, Ramzy EA, et al. Ultrasound-guided suprazygomatic sphenopalatine ganglion block for postdural puncture headache resistant to epidural blood patch: a case report. A&A Practice. 2024;18(4):e01778. doi:10.1213/XAA.0000000000001778
19. Boezaart AP, Smith CR, Zasimovich Y, et al. Refractory primary and secondary headache disorders that dramatically responded to combined treatment of ultrasound-guided percutaneous suprazygomatic pterygopalatine ganglion blocks and non-invasive vagus nerve stimulation: a case series. Reg Anesth Pain Med. 2024;49(2):144–150. doi:10.1136/rapm-2023-104967
20. Candido KD, Stevens RA. Post-dural puncture headache: pathophysiology, prevention and treatment. Best Pract Res Clin Anaesthesiol. 2003;17(3):451–469. doi:10.1016/S1521-6896(03)00033-8
21. Mokri B. The Monro–Kellie hypothesis. Neurology. 2001;56(12):1746–1748. doi:10.1212/WNL.56.12.1746
22. Babaiyan S, Shakhs Emampour F. Avoiding invasive measures: sphenopalatine ganglion block as a substitute for epidural blood patch in post-dural puncture headache: a case report. Anesthesiol Pain Med. 2024;14(4):e148291. doi:10.5812/aapm-148291
23. Siegler BH, Dos Santos Pereira RP, Keßler J, et al. Intranasal lidocaine administration via mucosal atomization device: a simple and successful treatment for postdural puncture headache in obstetric patients. Biomedicines. 2023;11(12):3296. doi:10.3390/biomedicines11123296
24. Singh P, Verma S. Case series on the efficacy of sphenopalatine ganglion block using a 20G intravenous cannula for postdural puncture headache after cesarean section: a novel approach and feasibility for home use in migraine patients. Indian J Pain. 2025;39(2):81. doi:10.4103/ijpn.ijpn_17_25
25. Kent S, Mehaffey G. Transnasal sphenopalatine ganglion block for the treatment of postdural puncture headache in obstetric patients. J Clin Anesth. 2016;34:194–196. doi:10.1016/j.jclinane.2016.04.009
26. Kassim Z, Kamar RM, Zakariah MF, et al. Transnasal sphenopalatine ganglion block for postdural puncture headache in obstetric patients: a Malaysian experience report. J Taibah Univ Med Sci. 2022;17(5):805–809. doi:10.1016/j.jtumed.2022.02.008
27. Hara MS, Furuya K, Kishida K, et al. Efficacy and potency of sphenopalatine ganglion block for the management of postdural puncture headaches in post-cesarean section: a case report and literature review. J Obstet Gynaecol Res. 2024;50(12):2357–2361. doi:10.1111/jog.16121
28. Nazir N, Saxena A, Asthana U. Efficacy and safety of trans-nasal sphenoid ganglion block in obstetric patients with post-dural puncture headache: a randomized study. Cureus. 2021;13(12):e20387. doi:10.7759/cureus.20387
29. Yan Y, Chang W, Chen S. Transnasal sphenopalatine ganglion block for treating postdural puncture headache: a case report and literature review. Asian J Surg. 2024;S1015-9584(24):1531–1538.
30. Furtado I, de Lima IFD, Pedro S. Uso de ropivacaína em bloqueio do gânglio esfenopalatino via transnasal para cefaleia pós-punção dural em pacientes obstétricas – série de casos. Braz J Anesthesiol. 2018;68(4):421–424. doi:10.1016/j.bjan.2017.11.007
31. Puthenveettil N, Rajan S, Mohan A, et al. Sphenopalatine ganglion block for treatment of post-dural puncture headache in obstetric patients: an observational study. Indian J Anaesth. 2018;62(12):972–977. doi:10.4103/ija.IJA_443_18
32. Singh S, Mishra R, Deigheidy EM. Trans-nasal sphenopalatine ganglion block for post-dural puncture headache after caesarean delivery: a prospective, double-blind clinical trial. Int J Pain. 2025;16(2):66–75. doi:10.56718/ijp.25-012
33. Feghali M, Venkataramanan R, Caritis S. Pharmacokinetics of drugs in pregnancy. Semin Perinatol. 2015;39(7):512–519. doi:10.1053/j.semperi.2015.08.003
34. Bhatia P, Chhabra S. Physiological and anatomical changes of pregnancy: implications for anaesthesia. Indian J Anaesth. 2018;62(9):651. doi:10.4103/ija.IJA_458_18
35. Albaqami MS, Alwarhi FI, Alqarni AA. The efficacy of sphenopalatine ganglion block for the treatment of postdural puncture headache among obstetric population. Saudi J Anaesth. 2022;16(1):45–51. doi:10.4103/sja.sja_651_21
36. Youssef HA, Abdel-Ghaffar HS, Mostafa MF, et al. Sphenopalatine Ganglion versus greater occipital nerve blocks in treating post-dural puncture headache after spinal anesthesia for cesarean section: a randomized clinical trial. Pain Physician. 2021;24(4):E443–E451.
37. Santos NS, Nunes JM, Font ML, et al. Early versus late sphenopalatine ganglion block with ropivacaine in postdural puncture headache: an observational study. Braz J Anesthesiol. 2023;73(1):42–45. doi:10.1016/j.bjane.2021.01.007
38. Xavier J, Pinho S, Silva J, et al. Postdural puncture headache in the obstetric population: a new approach? Reg Anesth Pain Med. 2020;45(5):373–376. doi:10.1136/rapm-2019-101053
39. Singh S, Mishra R, Deigheidy EM. Comparison of efficacy and efficiency of trans-nasal spheno-palatine ganglion block for the management of post-dural puncture headache. J Port Soc Anesthesiol. 2025;34(3):92–98.
40. Elhamrawy A, Syed A, Smith T, et al. Management of post-dural puncture headaches in pediatric patients with epidural blood or saline patch: an educational focused review. J Pain Res. 2024;17:1197–1207. doi:10.2147/JPR.S444381
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.