Back to Journals » Clinical Ophthalmology » Volume 13
Spectacle Independence And Patient Satisfaction With Pseudophakic Mini-Monovision Using Aberration-Free Intraocular Lens
Authors Abdelrazek Hafez T ![]() , Helaly HA
, Helaly HA ![]()
Received 10 May 2019
Accepted for publication 30 September 2019
Published 31 October 2019 Volume 2019:13 Pages 2111—2117
DOI https://doi.org/10.2147/OPTH.S215229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tarek Abdelrazek Hafez, Hany Ahmed Helaly
Ophthalmology Department, Faculty of Medicine, Alexandria University, Alexandria, Egypt
Correspondence: Hany Ahmed Helaly
Ophthalmology Department, Faculty of Medicine, Alexandria University, 30 Roshdy Street, Roshdy, Alexandria, Egypt
Tel +201225466733
Email [email protected]
Purpose: To assess spectacle independence and patient satisfaction with pseudophakic mini-monovision in patients undergoing routine bilateral cataract surgery with implantation of an aspherical aberration-free intraocular lens (Akreos AO, Bausch and Lomb, USA).
Methods: This study was a retrospective analysis that included 60 eyes of 30 consecutive patients between 2016 and 2018. The included patients had undergone sequential bilateral routine phacoemulsification after choosing the mini-monovision option. Test for ocular dominance was done using a sighting test. Emmetropia was aimed at in the dominant eye, while in the non-dominant eye the aim was myopia between −1 D and −1.5 D. The main outcome parameters were uncorrected distance visual acuity (UDVA), uncorrected near visual acuity (UNVA), and data reported from a questionnaire given to the patients at 3 months postoperative visit.
Results: The study included 60 eyes of 30 consecutive patients. The mean binocular UDVA was 0.09 ± 0.07 logMAR. Twenty-eight patients (93%) had binocular UDVA of 0.2 logMAR or better. The mean binocular uncorrected intermediate distance visual acuity (at 65 cm) was 0.16 ± 0.12 logMAR. Twenty-six patients (87%) had binocular uncorrected intermediate distance visual acuity of 0.2 logMAR or better. The mean binocular UNVA (at 35 cm) was 0.30 ± 0.21 logMAR. Fourteen patients (47%) had binocular UNVA of 0.2 logMAR or better. The patients score in the questionnaire was significantly higher in far and intermediate vision than near vision (p = 0.022). The patients score was significantly higher in day vision than night vision (p = 0.031). The mean overall patient satisfaction was good (9.1 ± 1.54). Twenty-eight patients (93%) reported high spectacle independence for far vision (score 8, 9, or 10).
Conclusion: Pseudophakic mini-monovision shows good results for spectacle independence and high patient satisfaction. It is a safe and inexpensive option after bilateral cataract surgery for correcting distance and intermediate vision. However, it might show lower results with near and night vision which is generally acceptable. Using aberration-free monofocal IOL allows for the residual normal positive corneal aberration that may augment the effect of monovision.
Keywords: mini-monovision, spectacle independence, patient satisfaction, pseudophakia, presbyopia, Akreos AO
Introduction
Patients undergoing routine cataract surgery usually are spectacle dependent after the procedure. Recently, the aim of cataract surgery is now extended to include correction of the refractive state of the eye, in addition to setting the patient free from spectacle dependence.1–3 Many methods have been adopted for this purpose such as monovision or mini-monovision using monofocal intraocular lenses (IOLs),4,5 trifocal or multifocal IOLs,6,7 extended depth of focus (EDOF) IOLs,8 and accommodating IOLs.9 However, many surgeons still prefer pseudophakic monovision as an inexpensive easy method to achieve spectacle independence after bilateral cataract surgery.
Pseudophakic monovision was first described by Boerner and Thrasher10 who described the standard pseudophakic monovision which was to correct the dominant eye for distance (i.e. aiming for emmetropia) and the non-dominant eye for near to intermediate (i.e. aiming for myopia) using the commonly used monofocal IOLs. The success of this procedure depends on the process of cortical adaptation in which the brain uses the dominant eye to obtain the image for distance and the other non-dominant eye to obtain the image for near to intermediate.11
The original monovision aimed for −2.50 diopters (D) of anisometropia or more. However, this large error may become intolerable. Many patients cannot tolerate this difference during the preoperative contact lens monovision trial period.12,13 Mini-monovision is a modification that uses lower amount of anisometropia usually between −1 and −1.5 D. Patients with mini-monovision have fewer optical undesirable effects due to lower degrees of anisometropia. The have good distance and intermediate visual acuity with spectacle independence. However, near visual tasks may still require some degree of spectacle dependence.14–16 Implanting the commonly used monofocal IOLs with mini-monovision avoids the problems of glare, waxy vision, and haloes that occur with the multifocal IOLs which might be irritating to the patients to a degree requiring IOL exchange.7,17
The aim of the current study was to assess spectacle independence and patient satisfaction with pseudophakic mini-monovision in patients undergoing routine bilateral cataract surgery with implantation of a hydrophilic acrylic aspherical aberration-free intraocular lens (Akreos AO, Bausch and Lomb, USA).
Methods
This study was a retrospective analysis that included previously collected data of 60 eyes of 30 patients. The included patients had bilateral clinically significant cataract and had undergone sequential bilateral routine phacoemulsification with implantation of a hydrophilic acrylic aspherical aberration-free intraocular lens (Akreos AO, Bausch and Lomb, USA) after choosing the mini-monovision option between 2016 and 2018. Cases of significant corneal or macular pathology were excluded. Cases with significant intraoperative complications affecting IOL proper placement were also excluded. We excluded cases of corneal astigmatism more than 1 D as we did not plan to use toric IOLs or limbal relaxing incisions.
This study was reviewed and approved by the local ethics committee of the faculty medicine, Alexandria University, Egypt on March 2019. The tenets of the Declaration of Helsinki were followed. All the included patients of the current study signed an informed consent after explaining the cataract extraction and mini-monovision procedure and the possible complications.
The records of the included patients were reviewed and the following data about the preoperative, operative, and postoperative periods were collected and recorded. Preoperative complete ophthalmic examinations were conducted including visual acuity (converted in logMAR units), manifest refraction, anterior segment examination, fundus examination for posterior segment abnormalities, measuring intraocular pressure, and macular optical coherence tomography (OCT). IOL power calculation was performed in all cases using optical biometry (IOL-master 700, Carl Zeiss, Germany) with SRK/T formula. The A constant used was 118.5.
Test for ocular dominance was done using a sighting test. The patient was asked to extend his/her arm while holding the thumb in an upright position and keeping both eyes open. Asking the patient to focus on a distant object and superimpose the thumb on this object. Then, close one eye each at a time. The dominant eye is the one which keeps the thumb superimposed on the distant object while the non-dominant eye is the closed one.
Surgical Technique
All included cases had undergone a routine phacoemulsification with implantation of a hydrophilic acrylic aspherical aberration-free intraocular lens (Akreos AO, Bausch and Lomb, USA). Emmetropia was aimed at in the dominant eye, while in the non-dominant eye the aim was myopia between −1 D and −1.5 D. All patients were operated upon by the same surgeon (T.A.H.) with a reproducible technique. Postoperative antibiotic and steroid eye drops were prescribed for 1 month.
Postoperative Evaluation
Patients were followed up on day 1, week 1, and months 1 and 3. The main outcome parameters were uncorrected distance visual acuity (UDVA), uncorrected near visual acuity (UNVA), and data reported from a questionnaire given to the patients at 3 months postoperative visit. This questionnaire was composed of six questions: asking the patients about spectacle independence for far (distant objects and television), intermediate distance (computers and laptops), and near (reading a book). It also asked about spectacle independence during night vision (driving at night) and daily vision. A last (sixth) question about overall patient satisfaction was given to the patients at the end of the questionnaire. Patients were required to give a grade on a scale from 1 to 10 for each question (1 represented poor result and 10 was the optimal grade). Ocular aberrometry (iDesign aberrometer; Abbott Medical Optics, AMO) was performed to measure the total primary spherical aberration (Z4°) at 6-mm pupil diameter. Stereopsis was tested using the Titmus test. Contrast sensitivity under mesopic (6 cd/m2) and photopic (85 cd/m2) conditions with and without glare was also performed.
Statistical Analysis
Data analysis was performed using the software SPSS for Windows version 20.0 (SPSS Inc., Chicago, USA). Quantitative data were described using range, mean and standard deviation. Kolmogorov–Smirnov test was used for checking the normality of distribution. Paired t-test was used to compare preoperative to postoperative means. Chi square test was used to compare between different percentages. Pearson correlation was used to correlate between different variables. Differences were considered statistically significant when the associated p-value was less than 0.05.
Results
The study included 60 eyes of 30 consecutive patients. The mean age was 56.3 ± 5.5 years (ranged from 45 to 66 years). Twenty patients (66.7%) were males and 10 patients (33.3%) were females. Table 1 shows the preoperative characteristics of the included eyes. Twenty-one patients (70%) had right ocular dominance while 9 patients (30%) had left ocular dominance. There were no major intraoperative complications as all the cataract surgeries were uneventful. None of the included patients suffered from a significant glare or haloes during the postoperative period.
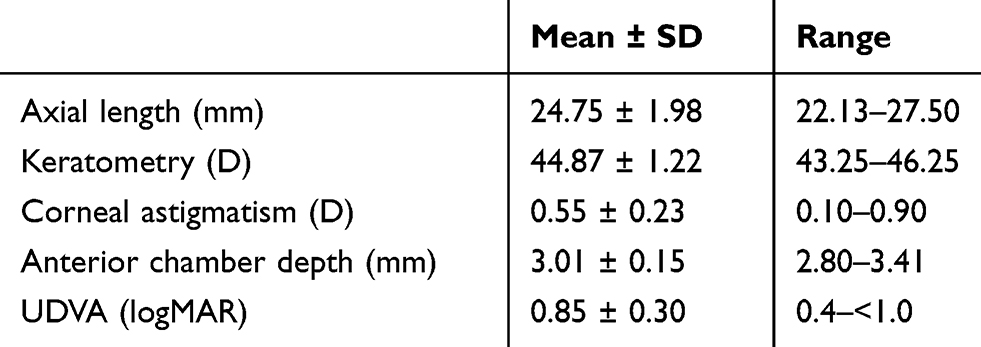 |
Table 1 Preoperative Characteristics Of The Included Eyes (n = 60) |
The target refraction for the dominant eye was emmetropia. Twenty-seven eyes (90%) and 30 eyes (100%) were within ± 0.50 D and ± 1.0 D from the target refraction, respectively. The mean manifest refraction spherical equivalent (MRSE) was −0.08 ± 0.35 D. The mean UDVA was 0.09 ± 0.08 logMAR (ranged from 0.0 to 0.3 logMAR). Postoperative UDVA was statistically significant from preoperative levels (p = 0.001).
The target refraction for the non-dominant eye was myopia between −1 D and −1.5 D. Twenty-eight eyes (93%) and 30 eyes (100%) were within ± 0.50 D and ± 1.0 D from the target refraction, respectively. The mean manifest refraction spherical equivalent (MRSE) was −1.38 ± 0.48 D. The mean uncorrected intermediate distance visual acuity (at 65 cm) was 0.17 ± 0.14 logMAR (ranged from 0.0 to 0.4 logMAR). The mean UNVA (at 35 cm) was 0.31 ± 0.19 logMAR (ranged from 0.1 to 0.6 logMAR).
The mean binocular UDVA was 0.09 ± 0.07 logMAR (ranged from 0.0 to 0.3 logMAR). Twenty-eight patients (93%) had binocular UDVA of 0.2 logMAR or better. The mean binocular uncorrected intermediate distance visual acuity (at 65 cm) was 0.16 ± 0.12 logMAR (ranged from 0.0 to 0.4 logMAR). Twenty-six patients (87%) had binocular uncorrected intermediate distance visual acuity of 0.2 logMAR or better. The mean binocular UNVA (at 35 cm) was 0.30 ± 0.21 logMAR (ranged from 0.1 to 0.5 logMAR). Fourteen patients (47%) had binocular UNVA of 0.2 logMAR or better. Figure 1 shows the cumulative binocular uncorrected visual acuities of the included patients at distance, intermediate, and near. Using t test, there was a statistically significant difference between binocular intermediate and near uncorrected visual acuity (p = 0.001). There was no statistically significant difference between distance and intermediate uncorrected visual acuities (p = 0.071).
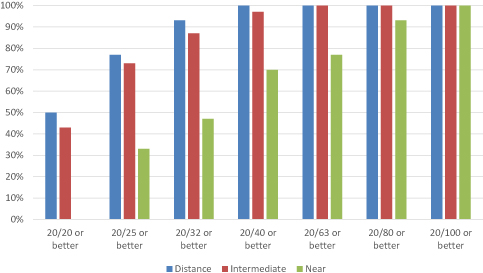 |
Figure 1 Cumulative binocular uncorrected visual acuities at 3 months postoperative. |
Contrast sensitivity was measured at 5 spatial frequencies, namely (1.5, 3, 6, 12, and 18) cycles per degree under mesopic (6 cd/m2) and photopic (85 cd/m2) conditions with and without glare. Figures 2 and 3 show the mean contrast sensitivity plotted against spatial frequency under the four different lighting conditions. There was a statistically significant decline in contrast sensitivity at almost all tested spatial frequencies between photopic and mesopic lighting conditions (p < 0.05). There was a statistically significant decline after using glare at the 6 cycles per degree spatial frequency for both photopic and mesopic conditions (p = 0.022 and 0.017, respectively).
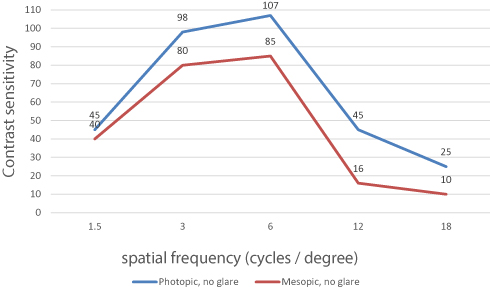 |
Figure 2 Contrast sensitivity testing under photopic and mesopic conditions with no glare. |
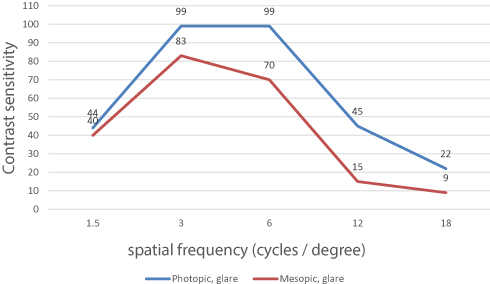 |
Figure 3 Contrast sensitivity testing under photopic and mesopic conditions with glare. |
Table 2 shows the scores of the questionnaire given to the patients to evaluate spectacle independence and overall patient satisfaction. Each question has a scale from 1 to 10 with 1 representing the poor result and 10 representing the optimal result. The patients' score was significantly higher in far and intermediate vision than near vision (p = 0.022). The patients' score was significantly higher in day vision than night vision (p = 0.031). The mean overall patient satisfaction was good (9.1 ± 1.54). Twenty-eight patients (93%) reported high spectacle independence for far vision (score 8, 9, or 10). Twenty-six patients (87%) reported high spectacle independence for intermediate vision (score 8, 9, or 10). The lowest spectacle independence scores were for near vision and night vision where only 13 patients (43%) and 14 patients (47%) reported a score of 8 or 9, respectively. None reported a score of 10 with complete spectacle independence for near vision and night vision.
 |
Table 2 Scores Of A Questionnaire Given To The Patients To Evaluate Spectacle Independence And Patient Satisfaction |
Regarding the 3 months postoperative primary spherical aberrations (Z4°) as measured by the high-resolution optical aberrometer (iDesign aberrometer; Abbott Medical Optics, AMO), the mean was 0.33 ± 0.15 μm for the included eyes. The mean spherical aberrations for the dominant eye were 0.34 ± 0.16 μm and for the non-dominant eye were 0.32 ± 0.15 μm. There was no statistical difference between dominant and non-dominant eyes (p = 0.21).
Testing for stereopsis was done using the Titmus test. The mean stereoacuity was 79 ± 37 s of arc. Twenty-six patients (87%) had a good stereoacuity (100 s of arc or better). There was a positive correlation between the degree of anisometropia and the level of stereoacuity (r = 0.85, p = 0.011).
No significant correlation was found between patients’ age and uncorrected visual acuity, MRSE, spherical aberration, stereopsis, or patient satisfaction. However, a significant good correlation between patient satisfaction and uncorrected postoperative visual acuity was found (r = −0.75, p = 0.032). There was a strong correlation between binocular uncorrected visual acuity and the score of the corresponding question in the patient questionnaire at distance, intermediate, and near (r = 0.97, 0.96, 0.98, respectively, p < 0.05).
Discussion
Nowadays, spectacle independence has become an important goal for both the patient and the surgeon following cataract extraction. Many methods have been described and different intraocular lenses with different designs have been manufactured to achieve this propose.17,18 Many studies addressed spectacle independence for both near and distant vision only. Additionally, the current study aimed at studying the intermediate vision spectacle independence which is also important in many aspects of our daily life, e.g. computer work, reading price tags, etc.
Pseudophakic monovision as a method for spectacle independence is a common practice among many surgeons. Although this is an effective way to set the patient free from glasses after cataract extraction, the resultant unexpected significant anisometropia may limit the advantage of this technique with subsequent effects on the stereopsis, contrast sensitivity and other visual functions. Therefore, targeting the eye to be slightly myopic for intermediate vision (mini-monovision) may avoid those potential complications and provide spectacle independency for patients during performing many of their daily activities.14,19
The use of monofocal IOLs with monovision to achieve spectacle independence avoids the financial burden of using the higher cost IOLs, e.g. multifocal or EDOF IOLs. Additionally, it lacks the problems of significant glare, haloes, and waxy vision.7,17 Similarly, the surgeon should pay attention while choosing the possible candidates for multifocal IOLs or pseudophakic monovision. It is advised to do a contact lens trial to simulate monovision and determine whether the candidate will be able to deal with the anisometropic error between the two eyes. However, using mini-monovision technique, candidate selection is not that critical as the original monovision because of smaller degrees of anisometropia between the two eyes. As with other IOLs, the surgeon should set realistic expectations before the surgery by explaining the principle of the procedure to the patients and letting them know that they might need glasses for near vision and night vision, e.g. night driving.
The important issue was to achieve a predictable manifest refraction matching the original intended target. In the current study, around 90% were within ± 0.50 D of the intended refraction and all the included eyes were within ± 1.0 D. Accurate IOL power calculation was a key point to the success of mini-monovision technique. Paying attention to spherical aberrations was another important issue. Nowadays, aspheric monofocal IOLs are used instead of the old spherical monofocal IOLs. The spherical aberration of the new aspheric IOLs ranges from 0 up to −0.27 µm. The monofocal IOLs with negative asphericity aimed at neutralizing the positive spherical aberration of the cornea to simulate the younger eyes. However, small amount of residual positive spherical aberration helps in increasing the depth of focus to allow for a greater range of near and intermediate vision.20,21 In the current study, we chose to implant a hydrophilic acrylic aspherical aberration-free intraocular lens (Akreos AO, Bausch and Lomb, USA). Having zero spherical aberration, this IOL did not add further aberrations to the eye and it maintained the normal positive corneal spherical aberration which provided some depth of field which enhanced the outcome of the mini-monovision technique. The mean spherical aberration was 0.33 ± 0.15 μm for the included eyes. This was comparable to the results reported by Ye et al22 where they reported postoperative spherical aberration after Akreos adapt implantation of 0.271 ± 0.151 µm for 5.0 mm optical zone.
Wilkins et al23 compared spectacle independence in patients randomized to receive bilateral multifocal IOLs versus monofocal IOLs with mini-monovision. Uniocular distance refractions in the monovision arm showed a mean spherical equivalent of +0.075 D in the distance eye and −0.923 in the near eye. A total of 24 of 93 patients (25.8%) in the monovision arm reported never wearing glasses. Binocular uncorrected acuity was 0.058 logMAR, for intermediate acuity was 0.149 logMAR and for near acuity was 0.013 logMAR. Those results were comparable to our results except for the binocular near visual acuity where our patients performed more poorly.
Goldberg et al24 evaluated patient satisfaction and spectacle dependence with pseudophakic mini-monovision. They used a similar questionnaire to the one used in the current study. They reported 93% of the patients having the surgery met their expectations for decreased dependence on spectacles. They found that most patients reported little or no use of spectacles for computer use (93%), distance viewing (93%) and general use throughout the day (87%). Those results are comparable to our results. They also found a small number of patients reported spectacle use for reading (9%) and night driving (18%). Those results were better than that reported by our patients. Like our study, they found no relationships between demographic variables and visual acuity or patient satisfaction. They used an aspheric monofocal IOL with negative asphericity, but they did not comment on the postoperative spherical aberration result of their included patients.
Regarding stereopsis, the mean stereoacuity of our included patients was 79 ± 37 s of arc with 26 of 30 patients having a good stereoacuity (100 s of arc or better). Ye et al22 reported a better mean stereoacuity of 92.3±37.8 s of arc with patients having bilateral implantation of Akreos adapt but without monovision. This agreed with our finding of having a positive correlation between the degree of anisometropia and the level of stereoacuity.
The results of this study showed that most patients achieved a satisfactory binocular UDVA for far and intermediate tasks. These results are like that of Labiris et al25 where they concluded that pseudophakic monovision could provide a very useful near vision with a good near stereopsis and visual acuity outcomes with time. Similarly, spectacle independence and patients’ satisfaction were increasing during the follow up period. Many authors showed that uncorrected near vision in monovision patients was not statistically different from multifocal or accommodating intraocular lens patients.18,25 On the other hand, some studies revealed that multifocal group has better near visual function when compared to monovision group.23 The current study has similar results to that reported by crossed monovision technique.26
Our work has some limitations among them was the lack of comparative nature with another group such as bilateral multifocal IOLs implantation. However, the literature shows enough data about multifocal IOLs that can be compared to. Also, the retrospective nature of the study was chosen. Longer follow up periods may provide additional strength to further studies as well as using more tests for quality of vision using objective methods.
In conclusion, pseudophakic mini-monovision shows good results for spectacle independence and high patient satisfaction. It is a safe and inexpensive option after bilateral cataract surgery for correcting distance and intermediate vision. However, it might show lower results with near and night vision which is generally acceptable. Using aberration-free monofocal IOL allows for the residual normal positive corneal aberration that may augment the effect of monovision.
Abbreviations
IOL, intraocular lens; EDOF, extended depth of focus; D, diopter; UDVA, uncorrected distance visual acuity; UNVA, uncorrected near visual acuity; OCT, optical coherence tomography; MRSE, manifest refraction spherical equivalent.
Ethics And Consent To Participate
The study was approved by the local ethics committee at the Faculty of Medicine, Alexandria University, Egypt. Tenets of the Declaration of Helsinki were followed. All included patients were recalled for a final follow up visit and signing of an informed consent. Informed consent was obtained from all individual participants included in the study.
Availability Of Data
Data are available upon reasonable request to the authors.
Author Contributions
Both authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leaming DV. Practice styles and preferences of ASCRS members – 2003 survey. J Cataract Refract Surg. 2004;30:892–900. doi:10.1016/j.jcrs.2004.02.064
2. Pick ZS, Leaming DV, Elder MJ. The fourth New Zealand cataract and refractive surgery survey: 2007. Clin Exp Ophthalmol. 2008;36:604–619. doi:10.1111/j.1442-9071.2008.01869.x
3. Farhoudi DB, Behndig A, Montan P, Lundström M, Zetterström C, Kugelberg M. Spectacle use after routine cataract surgery: a study from the Swedish National Cataract Register. Acta Ophthalmol (Copenh). 2018;96(3):283–287. doi:10.1111/aos.13554
4. Mahrous A, Ciralsky JB, Lai EC. Revisiting monovision for presbyopia. Curr Opin Ophthalmol. 2018;29(4):313–317. doi:10.1097/ICU.0000000000000487
5. Rosa AM. Presbyopia monovision correction and cortical adaptation. J Physiol. 2018;596(2):135. doi:10.1113/JP276586
6. Steinwender G, Schwarz L, Böhm M, et al. Visual results after implantation of a trifocal intraocular lens in high myopes. J Cataract Refract Surg. 2018;44(6):680–685. doi:10.1016/j.jcrs.2018.04.037
7. Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2019;10:1–3.
8. Akella SS, Juthani VV. Extended depth of focus intraocular lenses for presbyopia. Curr Opin Ophthalmol. 2018;29(4):318–322. doi:10.1097/ICU.0000000000000490
9. Brady D, Silvestrini T, Rao R, inventors; Lensgen Inc, assignee. Two-part accommodating intraocular lens device.
10. Boerner CF, Thrasher BH. Results of monovision correction in bilateral pseudophakes. Am Intra-Ocular Implant Soc J. 1984;10:49–50. doi:10.1016/S0146-2776(84)80077-4
11. Greenstein S, Pineda R. The quest for spectacle independence: a comparison of multifocal intraocular lens implants and pseudophakic monovision for patients with presbyopia. Semin Ophthalmol. 2017;32(1):111–115.
12. Hayashi K, Yoshida M, Manabe S, Hayashi H. Optimal amount of anisometropia for pseudophakic monovision. J Refract Surg. 2011;27(5):332–338. doi:10.3928/1081597X-20100817-01
13. Jain S, Ou R, Azar DT. Monovision outcomes in presbyopic individuals after refractive surgery. Ophthalmology. 2001;108(8):1430–1433. doi:10.1016/s0161-6420(01)00647-9
14. Hayashi K, Ogawa S, Manabe SI, Yoshimura K. Binocular visual function of modified pseudophakic monovision. Am J Ophthalmol. 2015;159(2):232–240. doi:10.1016/j.ajo.2014.10.023
15. Evans BJ. Monovision: a review. Ophthalmic Physiol Opt. 2007;27(5):417–439. doi:10.1111/j.1475-1313.2007.00488.x
16. Xiao J, Jiang C, Zhang M. Pseudophakic monovision is an important surgical approach to being spectacle-free. Indian J Ophthalmol. 2011;59(6):481. doi:10.4103/0301-4738.77010
17. Buckhurst PJ, Naroo SA, Davies LN, Shah S, Drew T, Wolffsohn JS. Assessment of dysphotopsia in pseudophakic subjects with multifocal intraocular lenses. BMJ Open Ophthalmol. 2017;1(1):e000064. doi:10.1136/bmjophth-2016-000064
18. Mu J, Chen H, Li Y. Comparison study of visual function and patient satisfaction in patients with monovision and patients with bilateral multifocal intraocular lenses. Zhonghua Yan Ke Za Zhi. 2014;50(2):95–99.
19. Osher RH, Golnik KC, Barrett G, Shimizu K. Intentional extreme anisometropic pseudophakic monovision: new approach to the cataract patient with longstanding diplopia. J Cataract Refract Surg. 2012;38(8):1346–1351. doi:10.1016/j.jcrs.2012.04.029
20. Rocha KM, Soriano ES, Chamon W, Chalita MR, Nosé W. Spherical aberration and depth of focus in eyes implanted with aspheric and spherical intraocular lenses: a prospective randomized study. Ophthalmology. 2007;114(11):2050–2054. doi:10.1016/j.ophtha.2007.01.024
21. Yi F, Iskander DR, Collins M. Depth of focus and visual acuity with primary and secondary spherical aberration. Vision Res. 2011;51(14):1648–1658. doi:10.1016/j.visres.2011.05.006
22. Ye PP, Li X, Yao K. Visual outcome and optical quality after bilateral implantation of aspheric diffractive multifocal, aspheric monofocal and spherical monofocal intraocular lenses: a prospective comparison. Int J Ophthalmol. 2013;6(3):300.
23. Wilkins MR, Allan BD, Rubin GS, et al; Moorfields IOL Study Group. Randomized trial of multifocal intraocular lenses versus monovision after bilateral cataract surgery. Ophthalmology. 2013;120(12):2449–2455. doi:10.1016/j.ophtha.2013.07.048
24. Goldberg DG, Goldberg MH, Shah R, Meagher JN, Ailani H. Pseudophakic mini-monovision: high patient satisfaction, reduced spectacle dependence, and low cost. BMC Ophthalmol. 2018;18(1):293. doi:10.1186/s12886-018-0963-3
25. Labiris G, Giarmoukakis A, Patsiamanidi M, Papadopoulos Z, Kozobolis VP. Mini-monovision versus multifocal intraocular lens implantation. J Cataract Refract Surg. 2015;41(1):53–57. doi:10.1016/j.jcrs.2014.06.015
26. Kim J, Shin HJ, Kim HC, Shin KC. Comparison of conventional versus crossed monovision in pseudophakia. Br J Ophthalmol. 2015;99(3):391–393. doi:10.1136/bjophthalmol-2014-305449
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.