")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 14
Special Considerations in the Management of HIV and Viral Hepatitis Coinfections in Liver Transplantation
Authors McCain JD, Chascsa DM
Received 11 November 2021
Accepted for publication 7 April 2022
Published 29 April 2022 Volume 2022:14 Pages 27—36
DOI https://doi.org/10.2147/HMER.S282662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Gerry Lake-Bakaar
Josiah D McCain,1 David M Chascsa2
1Department of Gastroenterology & Hepatology, Mayo Clinic, Phoenix, AZ, USA; 2Transplant Center, Mayo Clinic, Phoenix, AZ, USA
Correspondence: David M Chascsa, Transplant Center, Mayo Clinic, 5777 E. Mayo Blvd, Phoenix, AZ, 85054, USA, Tel +1 800 344 6296, Email [email protected]
Abstract: Modern therapies for hepatitis B virus, hepatitis C virus, and human immunodeficiency virus have become so effective that patients treated for these conditions can have normal life-expectancies. Suitable livers for transplantation remain a scarce and valuable resource. As such, significant efforts have been made to expand donation criteria at many centers. This constant pressure, coupled with the increasing effectiveness of antiviral therapies, has meant that more and more patients infected with hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) may be considered appropriate donors in the right circumstances. Patients with these infections are also more likely to be considered appropriate transplantation recipients than in the past. The treatment of HBV, HCV, and HIV after liver transplantation (LT) can be challenging and complicated by viral coinfections. The various pharmaceutical agents used to treat these infections, as well as the immunosuppressants used post-LT must be carefully balanced for maximum efficacy, and to avoid resistance and drug–drug interactions.
Keywords: liver transplantation, HIV, hepatitis, antiviral, immunosuppressant
Introduction
In the age of modern antiretroviral therapy (ART) for HIV and direct-acting antiviral (DAA) medications against HCV, the mortality rates of these diseases are consistently decreasing, and patients are enjoying longer lives.1,2 Consequently, the attention of epidemiologists and physicians has turned toward the long-term effects of living with these viruses.
The long-term effects of viral hepatitis – including cirrhosis and hepatocellular carcinoma (HCC) – are well-described. HIV infection, too, is associated with liver disease. In a population study of 49,731 patients from 1999 to 2011 who were infected with HIV in the USA, Australia, and Europe, liver disease (13.2%) was the third leading cause of death.3 An earlier study of 23,441 HIV-infected patients found that liver disease was the most common non-AIDS-related cause of death (14.5%).4
The proposed causes of liver injury in patients with HIV are many and include5 oxidative stress and mitochondrial toxicity from ART therapies (particularly nucleoside reverse transcriptase inhibitors (NRTIs) and protease inhibitors (PIs)),6,7 high prevalence of non-alcoholic fatty liver disease (NAFLD),8 direct viral injury of Kupffer cells,9–11 gut translocation of bacterial degradation products,12 systemic inflammatory processes,13 and development of nodular regenerative hyperplasia.14,15 Perhaps, the most existential hepatic threat in HIV-infected patients is the high incidence of viral hepatitides. Their modes of transmission and risk factors for infection mean that the viruses are commonly found together.16 In the United States, the prevalence of HIV and HBV coinfection has been cited at 9%, and HIV/HCV coinfection as high as 33%.16,17 Furthermore, of those HIV-infected patients who die of liver disease, viral hepatitis has been implicated as the most important offender.4,17–20
Viral hepatitis is an increasingly curable disease21; so much so that transplantation of HCV-positive livers into HCV-negative recipients has become commonplace at many centers. Modern treatment of HCV is safe, affordable for most patients, and usually curative. The scarcity of liver grafts for transplantation has also driven some centers to engage in the transplantation of HBV-viremic livers for select patients. Expansion of the donor pool may create a need for medical providers to gain familiarity with management of viral coinfections in the post-transplant population. LT in these patients produces a unique and growing population with specific medical challenges that can be met with proper guidance, surveillance, and therapies. Herein we review the most recent literature on these medical therapies, as well as a discussion of the current management of viral hepatitis post-transplantation.
Antivirals, Immunosuppression, and Drug–Drug Interaction
Immunosuppressant medications are the foundation of post-liver transplant care for most patients. Drug–drug interactions are very common and there is a great need to be aware of these interactions, which can affect the concentration of both the immunosuppressant and the other medication with which it interacts. Antimicrobial medicines represent an important group of such drugs, especially given the increased risk of infections in immunosuppressed patients. Understanding the risk associated with concomitant use of DAAs and ART with immunosuppressants, and the effect of immunosuppression on the underlying infections is important for practitioners caring for this population of patients. The primary concern in administration of both DAAs and ART post transplantation is variability in trough levels of immunosuppressant medications due to alterations in rates of metabolism. Therefore, regardless of immunosuppressant regimen used, careful drug-level monitoring should be employed.
DAAs
The treatment of HCV infection has undergone a paradigm shift in the past decade with the advent and validation of DAA therapies, which have produced high rates of sustained virologic response (SVR) even after LT.22 This generates important questions regarding the safety and efficacy of these medications when used in combination with the standard immunosuppressants prescribed after solid-organ transplantation. While most major treatment regimens for HCV infection are safe in the post-transplant population, there are some important drug–drug interactions that should be highlighted (Table 1). The current first-line DAA regimens are listed in Table 2.74
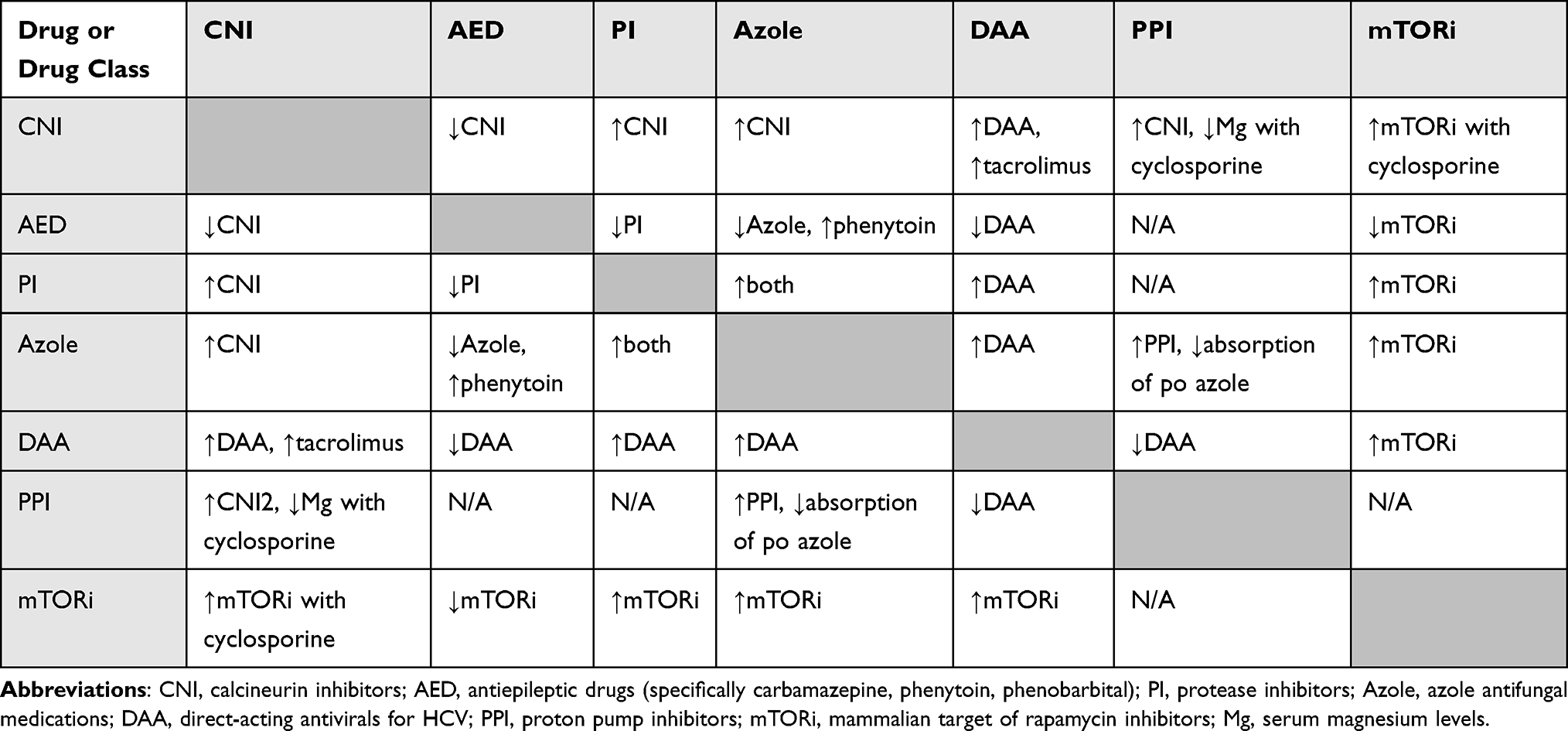 |
Table 1 Potential Drug–Drug Interactions Between Antivirals and Common Medications |
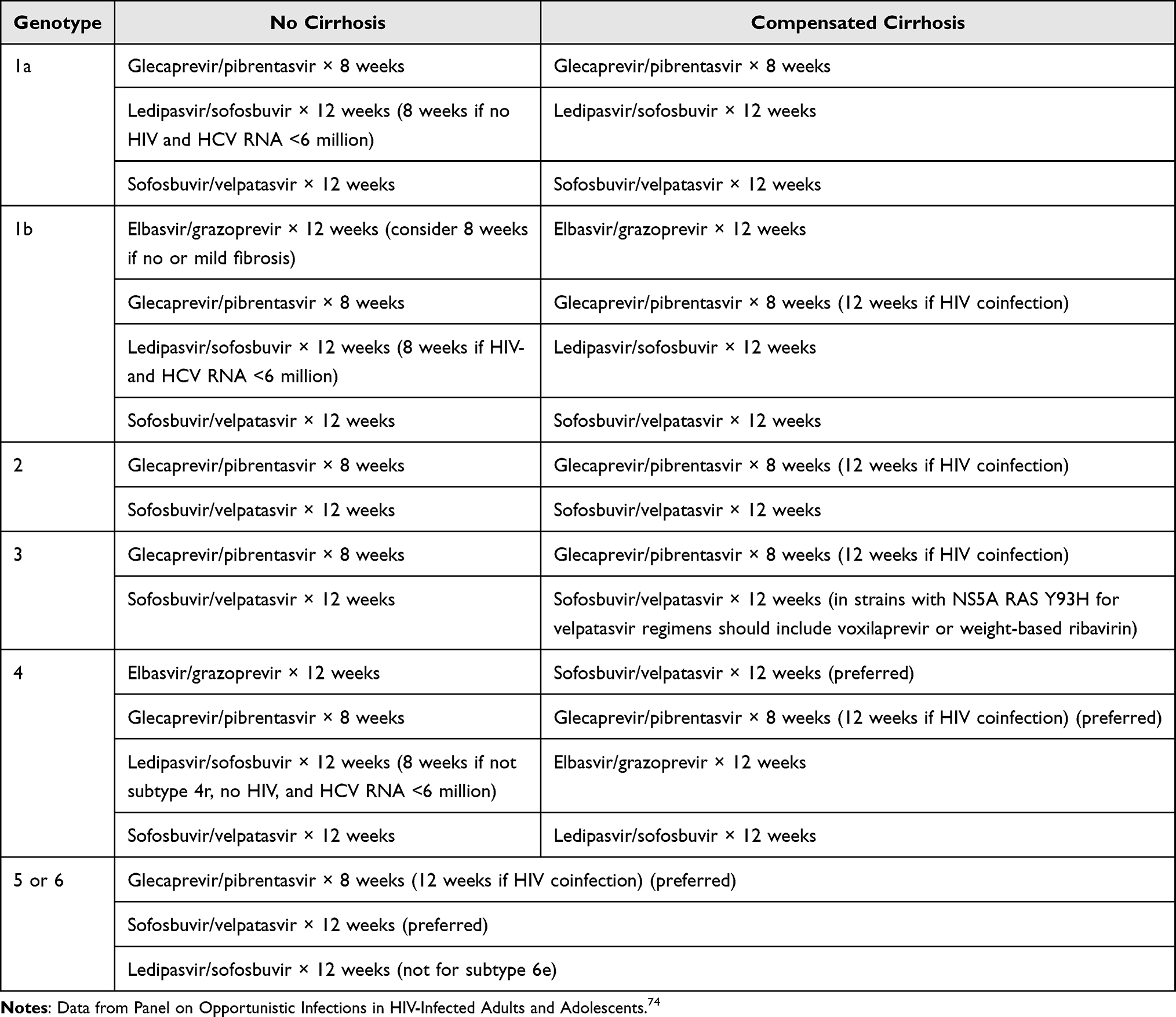 |
Table 2 Preferred HCV DAA Regimens in Treatment-Naïve Patients |
Tacrolimus, cyclosporine, everolimus, and sirolimus are all metabolized by cytochrome P450 3A (CYP3A) and are substrates of the P-glycoprotein transporter (P-gp).23,24 Certain DAAs have inhibitory effects on these metabolic pathways, potentially resulting in increased concentrations of their targets. This was demonstrated in a study of the now-discontinued DAA, telaprevir, when steady state dosing of the drug created a 4.6-fold increase in the AUC of cyclosporine and a 70-fold increase in the AUC of tacrolimus.25 Despite limitations of the study, this did raise caution about dosing considerations in HCV-infected transplant recipients.26
Fortunately, the safety of current regimens is becoming well-established.27–31 The most important interactions to be aware of in current therapies are those which involve cyclosporine, a strong inhibitor of the organic anion-transporting polypeptide (OATP).32 The concomitant use of cyclosporine elbasvir-grazoprevir is contraindicated due to its potential to cause toxic elevations of grazoprevir.33 Similar interactions cause elevations in serum levels of the protease inhibitor voxilaprevir; the regimen sofosbuvir/velpatasvir/voxilaprevir is contraindicated with cyclosporine.34 Administration of DAA regimens containing ritonavir, an inhibitor of CYP3A4 and P-gp, (such as ombitasvir, paritaprevir, ritonavir and dasabuvir) in combination with drugs that are highly dependent on CYP3A metabolism is contraindicated including cyclosporine, everolimus, sirolimus, and tacrolimus.35,36 Azole antifungals, common treatment and prophylactic agents in the post-LT population, also carry the potential for interaction with the DAAs simeprevir and possibly daclatasvir.37 Other common potential drug–drug interactions to consider in the administration of DAAs are those with proton pump inhibitors, metamizole, statins, and carvedilol.38
ART
In a similar fashion to the DAAs, many medicines used in ART interact with immunosuppressants via interaction with their metabolic pathways. Protease inhibitors (PI) like ritonavir, as addressed in discussion of DAAs, inhibit CYP3A4 and P-gp. This can result in supra-therapeutic serum levels of cyclosporine, everolimus, sirolimus, and tacrolimus.35,39 Additionally, the integrase strand transfer inhibitor (INSTI) elvitegravir is administered with cobicistat which is a potent CYP3A inhibitor, thereby conveying similar risk for patients taking immunosuppressants metabolized by that enzyme. Nucleoside reverse transcriptase inhibitors (NRTIs) are metabolized by CYP3A4. In contrast to PIs, NRTIs – and especially efavirenz and nevirapine – can induce CYP3A4.40 This can result in subtherapeutic levels of immunosuppression and risk of organ rejection. The current first-line ART therapies are listed in Table 3,85 and the most common drug–drug interactions between PIs, DAAs, and other common medications are listed in Table 1.
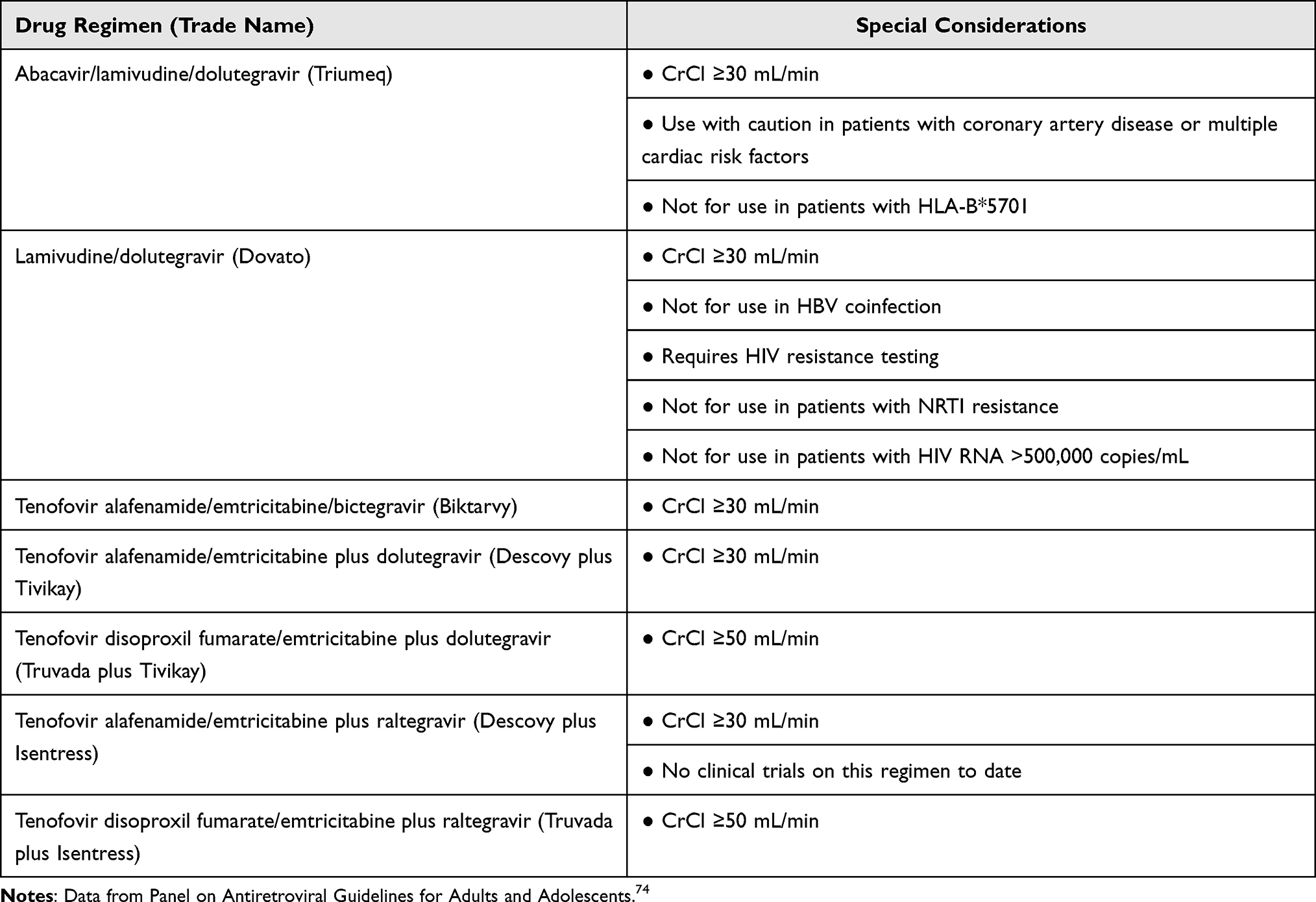 |
Table 3 Current First-Line ART in Non-Pregnant Adults |
HIV Post LT
A decade ago, HIV infection was considered a relative contraindication to solid organ transplantation. It was thought that transplantation, and specifically immunosuppression, might cause acceleration of the patient’s underlying HIV.41 However, more recent studies performed in the era of modern ART therapies have disproven this notion,42–45 and transplantation in the setting of HIV is now commonplace in many centers. Both the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) include routine testing for HIV as part of the transplant evaluation. Per AASLD guidelines, patients with HIV may undergo LT if CD4 counts are >100 cells/µL with a completely suppressed viral load anticipated at time of transplant, and per the EASL a CD4 count of >100–150 cells/µL is needed in the absence of AIDS-related events.46,47 It is important that these patients have a history of well-controlled HIV and medication compliance, and consultation with an infectious diseases specialist is recommended prior to transplantation.46,47
The choice of immunosuppressant remains controversial without uniform agreement among experts. The initial pilot study by Stock et al avoided induction immunosuppression altogether due to concerns about rejection raised by previous research.42,48 Some centers prefer the use of IL-2 receptor blockers for induction based on studies that identified high rates of rejection in kidney recipients with HIV.49,50 There are data in the renal transplant literature suggesting that induction in HIV-infected patients, either with an IL-2 receptor blocker or with anti-thymocyte globulin, had lower rates of delayed graft function, less graft loss, and the same rate of infection as those who received no induction.51 Maintenance therapies have generally attempted to include cyclosporine or mycophenolate mofetil when possible due to data showing activity of those agents against HIV.52,53 The selection of immunosuppression should be carefully reviewed for potential drug–drug interactions with ART as discussed in the previous section on this topic, trough-level monitoring of immunosuppressants should be routine.
Both ART for HIV infection, and immunosuppressive agents used post-LT can have metabolic effects over time. ART has been known to cause central adiposity and other lipodystrophic effects.54 Common immunosuppressant medications such as calcineurin inhibitors and inhibitors of mammalian target of rapamycin have been implicated in dyslipidemia, diabetes mellitus, and obesity after solid organ transplantation.55 Whether the combination of post-transplant immunosuppression and ART increases the risk of these effects even further has not been thoroughly studied, but the potential for metabolic syndrome in such patients should prompt vigilance and aggressive preventative management.
HIV and HCV Coinfection
Patients coinfected with HIV and HCV who have undergone LT have consistently displayed poorer patient and graft survival.48,56,57 In a study comparing HIV/HCV-coinfected LT recipients with controls, the coinfected patients were more likely than HCV mono-infected patients to suffer acute rejection, lose the graft organ, or die.58 This is in the setting of better outcomes for the post-LT patient with HIV. Since 2012, the rate of graft loss and mortality in those patients has decreased by 42%, surpassing the rate of improvement in the non-HIV infected LT population.59 This reflects data from the non-transplant population where coinfection of HIV and HCV has been recognized for decades as a risk factor for worsening liver disease.60–63
Careful patient and donor selection, too, plays an important role in the presence of HIV/HCV coinfection. The same study that well-characterized the increased risk of death and graft loss also identified lower body mass index (BMI) [hazard ratio (HR): 3.2; 95% confidence interval (CI): 1.3–7.7], simultaneous liver-kidney transplantation (HR: 3.8; 95% CI: 1.6–9.1), and an anti-HCV antibody-positive donor (HR: 2.5; 95% CI: 1.1–5.6) as independent risk factors for graft loss in HIV/HCV-coinfected patients compared to those mono-infected with HCV.58 Given the changes that have taken place in HCV management even in the last decade, the specific conclusions to be drawn from this data are not apparent. However, the associations with low BMI and need for renal transplantation may imply that factors such as time on the waitlist and nutrition in these patients must garner special attention. In a time when expansion of the donor pool is such an important topic, the HIV/HCV-coinfected patient is one in which more conservative donor selection may be appropriate. The previously mentioned AASLD guidelines are paramount in these patients: CD4 counts should be above 100 cells/µL at the time of transplant and the HIV viral load should be suppressed.47 Furthermore, ensuring stability of HIV RNA levels on effective ART therapy for a period of 6 months, and the absence of any AIDS-defining illness are reasonable precautions adopted by some centers.
The care of such patients after LT merits some special consideration as well. Firstly, recurrence of HCV after LT has been shown to be more frequent and more severe in the coinfected patient and represents an important cause of graft loss and mortality in this population,57,58,64 emphasizing the importance of regular surveillance in these patients even after DAA therapies. Secondly, rates of acute rejection in coinfected patients are higher, and the outcomes of treatment of rejection are poorer.65 Thirdly, the best choice of ART in these patients is not clear. Traditionally, patients have been continued on their previous therapies under the principal of previous good response and avoidance of resistant viral strains. One consideration though might be avoidance of PIs given the protentional drug–drug interactions with immunosuppression and data suggesting that this strategy may associate with lower rates of rejection.66,67
In summary, the difference in outcomes between the HIV and HCV mono-infected patient and the coinfected patient represents one of the most important factors in the post LT population with either virus. Aggressive treatment of HCV ought to be a priority in any patient infected with both viruses. In patients with well-compensated liver disease, pre-transplantation treatment of HCV may be a viable option, while patients with more severe disease may need to delay DAA therapy until after transplant. Surveillance for post-transplant recurrence of HCV should be a routine component of clinical practice, and care must be given to appropriate patient and donor selection.
HIV and HBV Coinfection
Like HIV/HCV, HIV/HBV coinfection is associated with poorer outcomes and higher rates of HCC compared to HBV infection alone.68,69 It is duly imperative then, that the hepatitis B infectious and immune status of all HIV positive patients be tested. Importantly, a patient with an isolated hepatitis B core antibody (HBcAb) usually represents a patient with previous HBV exposure who has cleared their hepatitis B surface antigen (HBsAg). The HBV covalently closed circular DNA (cccDNA) can exist dormant in these patients’ hepatocytes. In such patients, HBV reactivation after immunosuppression – either from drugs or from disease – can occur. Patients with HIV/HBV coinfection also more frequently have detectable hepatitis B e antigen (HBeAg) which associates with more liver dysfunction and worse outcomes.70–72
AASLD guideline recommendations for care of patients with HIV/HBV coinfection include regular monitoring of liver function, serologic surveillance of immune markers and HBV DNA, and liver fibrosis assessment every 6–12 months.73 Patients who are positive for HBsAg, with or without HIV infection, should undergo screening for HCC every 6 months with either ultrasound or AFP.73 Both diseases are caused by retroviruses, and as such can be targeted by some of the same agents. Specifically, both tenofovir and emtricitabine have activity and current guidelines recommend ART therapy for HIV/HBV-coinfected patients include tenofovir.74
The prevention of HBV recurrence after liver transplantation includes the use of prophylactic anti-viral medical therapies. Hepatitis B immunoglobulin (HBIG) has been a cornerstone of post-transplantation management against HBV for decades. Over time, the administration of continued intravenous infusions of HBIG can be financially and logistically burdensome, and has given way to recent studies demonstrating the efficacy of intramuscular and even subcutaneous dosing.75,76 While current practice guidelines from the EASL and AASLD include the use of both HBIG and a nucleos(t)ide analogue to prevent HBV recurrence after LT,46,77 more recent data have questioned the role of HBIG, given the high efficacy and high barrier to resistance of tenofovir preparations, specifically in undetectable HBV DNA levels immediately prior to transplant.78 The use of combination HBIG with a nucleos(t)ide analogue should be reserved for those patients who are high risk for HBV reactivation after LT, such as those patients with detectable HBV DNA, resistance to antiviral regimens, or HCC.78 Shorter courses of HBIG therapy may be reasonable in patients with low level of HBV DNA (<2000 U/mL).
Triple Infections
Triple infections with HIV/HBV/HDV, HIV/HBV/HCV, or HBV/HDV/HCV are less common than coinfections but do occur with some significance in areas where HBV is endemic. As expected, disease course is often severe, and outcomes poorer than in mono-infection. Treatment of triple infections is challenging and should be considered a relative contraindication to LT.79,80
Expansion of the Donor Pool
The primary limitation in LT continues to be the shortage of transplantable organs. Given successful control of HIV and viral hepatitis B and the potential for rapid cure of HCV in the post-transplant setting, there is interest in expansion of the donor pool. The inclusion of donors who are positive for HIV or who have HCV viremia has been a slow and deliberate process that has, so far, been met with favorable outcomes.59,81 The current state of the art is to transplant infected allografts into patients with the same viral comorbidities such as an HIV-positive donor allograft to HIV-positive donor, or HBV-infected allograft to HBV-infected recipient. Carefully selected non-viremic patients who are adequately apprised of the risk–benefit ratio of receiving a thoroughly evaluated viremic organ (excluding HIV at the current time) is becoming commonplace. Hepatitis C viremic organs are commonly used in the US, and HBsAg-positive donors are being used in select centers, particularly in Asia.82–84
Conclusion
Viral hepatitis and HIV infections can lead to end-stage liver disease requiring evaluation for liver transplantation. In the post-transplant setting, treatment of these infections requires a nuanced approach based on the type of viral coinfection, and with special attention to potential drug–drug interactions. The coinfected patient in particular is at risk for more severe liver disease and must be aggressively monitored and treated by an interdisciplinary team including the transplant hepatologist, infectious disease specialist, and a transplant pharmacist.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weber R, Ruppik M, Rickenbach M, et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013;14(4):195–207. doi:10.1111/j.1468-1293.2012.01051.x
2. Kwong A, Kim WR, Mannalithara A, Heo NY, Udompap P, Kim D. Decreasing mortality and disease severity in hepatitis C patients awaiting liver transplantation in the United States. Liver Transpl. 2018;24(6):735–743. doi:10.1002/lt.24973
3. Smith CJ, Ryom L, Weber R, et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384(9939):241–248. doi:10.1016/S0140-6736(14)60604-8
4. Data Collection on Adverse Events of Anti-HIV Drugs Study Group. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Intern Med. 2006;166(15):1632–1641. doi:10.1001/archinte.166.15.1632
5. Kaspar MB, Sterling RK. Mechanisms of liver disease in patients infected with HIV. BMJ Open Gastroenterol. 2017;4(1):e000166. doi:10.1136/bmjgast-2017-000166
6. Boyer TD, Lindor KD. Zakim and Boyer’s Hepatology: A Textbook of Liver Disease e-Book. Elsevier Health Sciences; 2016.
7. Williams K, Rao Y-P, Natarajan R, Pandak WM, Hylemon PB. Indinavir alters sterol and fatty acid homeostatic mechanisms in primary rat hepatocytes by increasing levels of activated sterol regulatory element-binding proteins and decreasing cholesterol 7α-hydroxylase mRNA levels. Biochem Pharmacol. 2004;67(2):255–267. doi:10.1016/j.bcp.2003.08.044
8. Lemoine M, Serfaty L, Capeau J. From nonalcoholic fatty liver to nonalcoholic steatohepatitis and cirrhosis in HIV-infected patients: diagnosis and management. Curr Opin Infect Dis. 2012;25(1):10–16. doi:10.1097/QCO.0b013e32834ef599
9. Housset C, Boucher O, Girard P, et al. Immunohistochemical evidence for human immunodeficiency virus-1 infection of liver Kupffer cells. Hum Pathol. 1990;21(4):404–408. doi:10.1016/0046-8177(90)90202-G
10. Hufert FT, Schmitz J, Schreiber M, Schmitz H, Rácz P, von Laer DD. Human Kupffer cells infected with HIV-1 in vivo. J Acquir Immune Defic Syndr. 1993;6(7):772–777.
11. Persidsky Y, Berger S, Gendrault J, et al. Signs of Kupffer cell involvement in productive simian immunodeficiency virus infection in monkey liver. Res Virol. 1994;145:229–237. doi:10.1016/S0923-2516(07)80027-6
12. Sacchi P, Cima S, Corbella M, et al. Liver fibrosis, microbial translocation and immune activation markers in HIV and HCV infections and in HIV/HCV co-infection. Digest Liver Dis. 2015;47(3):218–225. doi:10.1016/j.dld.2014.11.012
13. Mastroianni CM, Lichtner M, Mascia C, Zuccalà P, Vullo V. Molecular mechanisms of liver fibrosis in HIV/HCV coinfection. Int J Mol Sci. 2014;15(6):9184–9208. doi:10.3390/ijms15069184
14. Chang P-E, Miquel R, Blanco J-L, et al. Idiopathic portal hypertension in patients with HIV infection treated with highly active antiretroviral therapy. ACG. 2009;104(7):1707–1714.
15. Wanless IR. Micronodular transformation (nodular regenerative hyperplasia) of the liver: a report of 64 cases among 2500 autopsies and a new classification of benign hepatocellular nodules. Hepatology. 1990;11(5):787–797. doi:10.1002/hep.1840110512
16. Ockenga J, Tillmann HL, Trautwein C, Stoll M, Manns MP, Schmidt RE. Hepatitis B and C in HIV-infected patients. Prevalence and prognostic value. J Hepatol. 1997;27(1):18–24. doi:10.1016/S0168-8278(97)80274-7
17. Staples CT, Rimland D, Dudas D. Hepatitis C in the HIV (human immunodeficiency virus) Atlanta V.A. (Veterans Affairs Medical Center) Cohort Study (HAVACS): the effect of coinfection on survival. Clin Infect Dis. 1999;29(1):150–154. doi:10.1086/520144
18. Salmon-Ceron D, Lewden C, Morlat P, et al. Liver disease as a major cause of death among HIV infected patients: role of hepatitis C and B viruses and alcohol. J Hepatol. 2005;42(6):799–805. doi:10.1016/j.jhep.2005.01.022
19. Rosenthal E, Poirée M, Pradier C, et al. Mortality due to hepatitis C-related liver disease in HIV-infected patients in France (Mortavic 2001 study). Aids. 2003;17(12):1803–1809. doi:10.1097/00002030-200308150-00009
20. Konopnicki D, Mocroft A, De Wit S, et al. Hepatitis B and HIV: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA cohort. Aids. 2005;19(6):593–601. doi:10.1097/01.aids.0000163936.99401.fe
21. Cox AL, El-Sayed MH, Kao J-H, et al. Progress towards elimination goals for viral hepatitis. Nat Rev Gastroenterol Hepatol. 2020;17(9):533–542. doi:10.1038/s41575-020-0332-6
22. Ciesek S, Proske V, Otto B, et al. Efficacy and safety of sofosbuvir/ledipasvir for the treatment of patients with hepatitis C virus re‐infection after liver transplantation. Transpl Infect Dis. 2016;18(3):326–332. doi:10.1111/tid.12524
23. Kelly P, Kahan BD. Review: metabolism of immunosuppressant drugs. Curr Drug Metab. 2002;3(3):275–287. doi:10.2174/1389200023337630
24. Steiner R, Raguž-Lučić N, Erceg D. Direct-acting antivirals (daas): drug-drug interactions (DDIs) in the treatment of hepatitis C virus (HCV). In: Update on Hepatitis C. London, UK: IntechOpen; 2017:70788.
25. Garg V, van Heeswijk R, Eun Lee J, Alves K, Nadkarni P, Luo X. Effect of telaprevir on the pharmacokinetics of cyclosporine and tacrolimus. Hepatology. 2011;54(1):20–27. doi:10.1002/hep.24443
26. Charlton M. Telaprevir, boceprevir, cytochrome P450 and immunosuppressive agents — a potentially lethal cocktail. Hepatology. 2011;54(1):3–5. doi:10.1002/hep.24470
27. Mansour M, Hill L, Kerr J. Safety and effectiveness of direct acting antivirals for treatment of hepatitis C virus in patients with solid organ transplantation. Transpl Infect Dis. 2018;20(6):e12972. doi:10.1111/tid.12972
28. Charlton M, Everson GT, Flamm SL, et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology. 2015;149(3):649–659. doi:10.1053/j.gastro.2015.05.010
29. Pungpapong S, Aqel B, Leise M, et al. Multicenter experience using simeprevir and sofosbuvir with or without ribavirin to treat hepatitis C genotype 1 after liver transplant. Hepatology. 2015;61(6):1880–1886. doi:10.1002/hep.27770
30. Trakroo S, Qureshi K. Successful treatment of chronic hepatitis C infection with direct-acting antivirals in a heart transplant recipient: a case report.
31. Manns M, Samuel D, Gane EJ, et al. Ledipasvir and sofosbuvir plus ribavirin in patients with genotype 1 or 4 hepatitis C virus infection and advanced liver disease: a multicentre, open-label, randomised, Phase 2 trial. Lancet Infect Dis. 2016;16(6):685–697. doi:10.1016/S1473-3099(16)00052-9
32. Uchida M, Tajima Y, Kakuni M, et al. Organic Anion-Transporting Polypeptide (OATP)-mediated drug-drug interaction study between rosuvastatin and cyclosporine A in chimeric mice with humanized liver. Drug Metab Dispos. 2018;46(1):11–19. doi:10.1124/dmd.117.075994
33. Zepatier (elbasvir-grazoprevir) [package insert]. Whitehouse Station, NJ: Merck & Company Inc; 2019.
34. Vosevi (sofosbuvir/velpatasvir/voxilaprevir) [package insert]. Foster City, CA: Gilead Sciences; 2017.
35. Norvir (ritonavir) [package insert]. Lake Bluff, IL: AbbVie Inc; 2017.
36. Viekira pak (ombitasvir, paritaprevir, and ritonavir tablets; dasabuvir tablets) [package insert]. Lake Bluff, IL: AbbVie Inc; 2019.
37. Dick TB, Lindberg LS, Ramirez DD, Charlton MR. A clinician’s guide to drug-drug interactions with direct-acting antiviral agents for the treatment of hepatitis C viral infection. Hepatology. 2016;63(2):634–643. doi:10.1002/hep.27920
38. Schulte B, Wübbolding M, Marra F, et al. Frequency of potential drug–drug interactions in the changing field of HCV therapy. Open Forum Infect Dis. 2020;7(2). doi:10.1093/ofid/ofaa040
39. Kramer C, Blumberg E. Immunosuppressants and antiretroviral therapy in HIV-positive transplant patients. In: Fundamentals of HIV Medicine 2017(CME Edition). Oxford, UK: Oxford University Press; 2017.
40. Marfo K, Greenstein S. Antiretroviral and immunosuppressive drug-drug interactions in human immunodeficiency virus–infected liver and kidney transplant recipients. Transplant Proc. 2009;41(9):3796–3799. doi:10.1016/j.transproceed.2009.06.186
41. Spital A. Should all human immunodeficiency virus-infected patients with end-stage renal disease be excluded from transplantation? The views of U.S. transplant centers. Transplantation. 1998;65(9):1187–1191. doi:10.1097/00007890-199805150-00008
42. Stock PG, Roland ME, Carlson L. Kidney and liver transplantation in human immunodeficiency virus-infected patients: a pilot safety and efficacy study. Transplantation. 2003;76(2):370–375. doi:10.1097/01.TP.0000075973.73064.A6
43. Roland ME, Barin B, Carlson L. HIV-infected liver and kidney transplant recipients: 1- and 3-year outcomes. Am J Transplant. 2008;8(2):355–365. doi:10.1111/j.1600-6143.2007.02061.x
44. Neff GW, Bonham A, Tzakis AG. Orthotopic liver transplantation in patients with human immunodeficiency virus and end-stage liver disease. Liver Transpl. 2003;9(3):239–247. doi:10.1053/jlts.2003.50054
45. Ragni MV, Belle SH, Im K. Survival of human immunodeficiency virus-infected liver transplant recipients. J Infect Dis. 2003;188(10):1412–1420. doi:10.1086/379254
46. European Association for The Study of the Liver. EASL clinical practice guidelines: liver transplantation. J Hepatol. 2016;64(2):433–485. doi:10.1016/j.jhep.2015.10.006
47. Martin P, DiMartini A, Feng S, Brown Jr R, Fallon M. Evaluation for liver transplantation in adults: 2013 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Hepatology. 2014;59(3):1144–1165. doi:10.1002/hep.26972
48. Fox AN, Vagefi PA, Stock PG. Liver transplantation in HIV patients. Semin Liver Dis. 2012;32(02):177–185. doi:10.1055/s-0032-1316474
49. Stock PG, Barin B, Murphy B, et al. Outcomes of kidney transplantation in HIV-infected recipients. N Engl J Med. 2010;363(21):2004–2014. doi:10.1056/NEJMoa1001197
50. Carter JT, Melcher ML, Carlson LL, Roland ME, Stock PG. Thymoglobulin-associated Cd4+ T-cell depletion and infection risk in HIV-infected renal transplant recipients. Am J Transplant. 2006;6(4):753–760. doi:10.1111/j.1600-6143.2006.01238.x
51. Kucirka LM, Durand CM, Bae S, et al. Induction immunosuppression and clinical outcomes in kidney transplant recipients infected with human immunodeficiency virus. Am J Transplant. 2016;16(8):2368–2376. doi:10.1111/ajt.13840
52. Schwarz A, Offermann G, Keller F. The effect of cyclosporine on the progression of human immunodeficiency virus type 1 infection transmitted by transplantation—data on four cases and review of the literature. Transplantation. 1993;55(1):95–103. doi:10.1097/00007890-199301000-00019
53. Chapuis AG, Paolo Rizzardi G, D’Agostino C. Effects of mycophenolic acid on human immunodeficiency virus infection in vitro and in vivo. Nat Med. 2000;6(7):762–768. doi:10.1038/77489
54. Koethe JR, Lagathu C, Lake JE, et al. HIV and antiretroviral therapy-related fat alterations. Nat Rev Dis Primers. 2020;6(1):1–20. doi:10.1038/s41572-019-0135-7
55. Bhat M, Usmani SE, Azhie A, Woo M. Metabolic consequences of solid organ transplantation. Endocr Rev. 2020;42(2):171–197. doi:10.1210/endrev/bnaa030
56. de Vera ME, Dvorchik I, Tom K. Survival of liver transplant patients coinfected with HIV and HCV is adversely impacted by recurrent hepatitis C. Am J Transplant. 2006;6(12):2983–2993. doi:10.1111/j.1600-6143.2006.01546.x
57. Duclos-Vallée JC, Féray C, Sebagh M. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2008;47(2):407–417. doi:10.1002/hep.21990
58. Terrault NA, Roland ME, Schiano T, et al. Outcomes of liver transplant recipients with hepatitis C and human immunodeficiency virus coinfection. Liver Transplant. 2012;18(6):716–726. doi:10.1002/lt.23411
59. Campos-Varela I, Dodge JL, Berenguer M, et al. Temporal trends and outcomes in liver transplantation for recipients with HIV infection in Europe and United States. Transplantation. 2020;104(10):2078–2086. doi:10.1097/TP.0000000000003107
60. Telfer P, Sabin C, Devereux H, Scott F, Dusheiko G, Lee C. The progression of HCV-associated liver disease in a cohort of haemophilic patients. Br J Haematol. 1994;87(3):555–561. doi:10.1111/j.1365-2141.1994.tb08312.x
61. Soto B, Sánchez-Quijano A, Rodrigo L, et al. Human immunodeficiency virus infection modifies the natural history of chronic parenterally-acquired hepatitis C with an unusually rapid progression to cirrhosis. J Hepatol. 1997;26(1):1–5. doi:10.1016/S0168-8278(97)80001-3
62. Benhamou Y, Bochet M, Di Martino V, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology. 1999;30(4):1054–1058. doi:10.1002/hep.510300409
63. Graham CS, Baden LR, Yu E, et al. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta-analysis. Clin Infect Dis. 2001;33(4):562–569. doi:10.1086/321909
64. Miro J, Montejo M, Castells L, et al. Outcome of HCV/HIV‐coinfected liver transplant recipients: a prospective and multicenter cohort study. Am J Transplant. 2012;12(7):1866–1876. doi:10.1111/j.1600-6143.2012.04028.x
65. Miro JM, Stock P, Teicher E, Duclos-Vallée J-C, Terrault N, Rimola A. Outcome and management of HCV/HIV coinfection pre- and post-liver transplantation. A 2015 update. J Hepatol. 2015;62(3):701–711. doi:10.1016/j.jhep.2014.10.032
66. Tricot L, Teicher E, Peytavin G, et al. Safety and efficacy of raltegravir in HIV‐infected transplant patients cotreated with immunosuppressive drugs. Am J Transplant. 2009;9(8):1946–1952. doi:10.1111/j.1600-6143.2009.02684.x
67. Moreno A, Pérez‐Elías MJ, Casado JL, et al. Raltegravir‐based highly active antiretroviral therapy has beneficial effects on the renal function of human immunodeficiency virus–infected patients after solid organ transplantation. Liver Transplant. 2010;16(4):530–532. doi:10.1002/lt.22005
68. Thio CL, Seaberg EC, Skolasky R, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet. 2002;360(9349):1921–1926. doi:10.1016/S0140-6736(02)11913-1
69. Bräu N, Fox RK, Xiao P, et al. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: a U.S.-Canadian multicenter study. J Hepatol. 2007;47(4):527–537. doi:10.1016/j.jhep.2007.06.010
70. Colin JF, Cazals-Hatem D, Loriot MA, et al. Influence of human immunodeficiency virus infection on chronic hepatitis B in homosexual men. Hepatology. 1999;29(4):1306–1310. doi:10.1002/hep.510290447
71. Gilson RJ, Hawkins AE, Beecham MR, et al. Interactions between HIV and hepatitis B virus in homosexual men: effects on the natural history of infection. Aids. 1997;11(5):597–606. doi:10.1097/00002030-199705000-00007
72. Hou F, Qi X, Zhang Y, et al. Association of hepatitis B e antigen and DNA viral load with severity of liver dysfunction and in-hospital outcomes in hepatitis B-related liver cirrhosis. AME Med J. 2017;2(9):145. doi:10.21037/amj.2017.09.10
73. Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, Murad MH. AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 2016;63(1):261–283. doi:10.1002/hep.28156
74. Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America; 2016. Available from: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf.
75. Yahyazadeh A, Beckebaum S, Cicinnati V, et al. Efficacy and safety of subcutaneous human HBV-immunoglobulin (Zutectra®) in liver transplantation: an open, prospective, single-arm phase III study. Transpl Int. 2011;24(5):441–450. doi:10.1111/j.1432-2277.2011.01222.x
76. Filipponi F, Franchello A, Carrai P, et al. Efficacy, safety, and pharmacokinetics of intramuscular hepatitis B immune globulin, igantibe®, for the prophylaxis of viral B hepatitis after liver transplantation. Digest Liver Dis. 2010;42(7):509–514. doi:10.1016/j.dld.2009.09.005
77. Lucey MR, Terrault N, Ojo L, et al. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transpl. 2013;19(1):3–26. doi:10.1002/lt.23566
78. Lok AS. Liver transplantation for chronic hepatitis B virus infection. In: Brown Jr RS, editor. UpToDate. Waltham, MA: UpToDate; 2011.
79. Riaz M, Idrees M, Kanwal H, Kabir F. An overview of triple infection with hepatitis B, C and D viruses. Virol J. 2011;8:368. doi:10.1186/1743-422X-8-368
80. Coffin CS, Terrault NA. Treatment of HCV, HDV, or HIV coinfection. In: Kao J-H, Chen D-S, editors. Hepatitis B Virus and Liver Disease. Singapore: Springer Singapore; 2018:239–262.
81. Cotter TG, Aronsohn A, Reddy KG, Charlton M. Liver transplantation of HCV-viremic donors into HCV-negative recipients in the United States: increasing frequency with profound geographic variation. Transplantation. 2021;105(6):1285–1290. doi:10.1097/TP.0000000000003382
82. Yu S, Yu J, Zhang W, et al. Safe use of liver grafts from hepatitis B surface antigen positive donors in liver transplantation. J Hepatol. 2014;61(4):809–815. doi:10.1016/j.jhep.2014.05.003
83. Lee WC, Chou HS, Lee CS, et al. Viral activity and outcome of hepatitis B surface antigen‐positive grafts in deceased liver transplantation. J Viral Hepat. 2018;25(7):874–877. doi:10.1111/jvh.12880
84. Loggi E, Micco L, Ercolani G, et al. Liver transplantation from hepatitis B surface antigen positive donors: a safe way to expand the donor pool. J Hepatol. 2012;56(3):579–585. doi:10.1016/j.jhep.2011.09.016
85. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services. Available from: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/archive/AdultandAdolescentGL_2021_08_16.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.