Back to Journals » Journal of Pain Research » Volume 15
Speaker Gender Representation at the North American Neuromodulation Society Annual Meeting (2017–2021): Have We Made Progress in Closing the Gender Gap?
Authors D'Souza RS ![]() , Pilitsis JG
, Pilitsis JG ![]() , Langford BJ, Orhurhu V, Hussain N, Hoffmann CM
, Langford BJ, Orhurhu V, Hussain N, Hoffmann CM ![]() , Anitescu M, Vanterpool S, Ali R, Patel K, Moeschler SM
, Anitescu M, Vanterpool S, Ali R, Patel K, Moeschler SM ![]()
Received 27 June 2022
Accepted for publication 17 October 2022
Published 26 October 2022 Volume 2022:15 Pages 3423—3432
DOI https://doi.org/10.2147/JPR.S380152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Ryan S D’Souza,1 Julie G Pilitsis,2 Brendan J Langford,1 Vwaire Orhurhu,3 Nasir Hussain,4,5 Chelsey M Hoffmann,1 Magdalena Anitescu,6 Stephanie Vanterpool,7 Rushna Ali,8 Kiran Patel,9 Susan M Moeschler1
1Department of Anesthesiology and Perioperative Medicine, Mayo Clinic Hospital, Rochester, MN, USA; 2Department of Clinical Neurosciences, Florida Atlantic University, Boca Raton, FL, USA; 3Department of Pain Medicine, University of Pittsburgh, Pittsburgh, PA, USA; 4Department of Anesthesiology, Beth Israel Deaconess Medical Center, Boston, MA, USA; 5Department of Anesthesiology, The Ohio State University, Columbus, OH, USA; 6Department of Anesthesia and Critical Care, University of Chicago, Chicago, IL, USA; 7Department of Anesthesiology, University of Tennessee, Knoxville, TN, USA; 8Division of Neurosurgery, Spectrum Health, Grand Rapids, MI, USA; 9Department of Anesthesiology, New York University Langone Medical Center, New York City, NY, USA
Correspondence: Ryan S D’Souza, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA, Email [email protected]
Background: Speaker gender representation at medical conferences is a significant site of gender disparity. Our primary objective was to quantify the proportion of female speakers and compare plenary session opportunities by gender at the North American Neuromodulation Society (NANS) Annual Conference.
Methods: Data from the 2017– 2021 NANS Annual Conference presentations were abstracted. Primary outcomes included gender composition of speaker slots, gender composition of individual speakers, and comparison of plenary speaker slots by gender. Secondary outcomes included comparisons of session size, age, professional degree, and number of presentations per speaker based on gender.
Results: Gender composition of annual speaker slots was (% slots presented by women): 2017:14.6%; 2018:20.5%; 2019:23.5%; 2020:21.0%; 2021:41.4%. Annual gender composition of individual speakers was (% women): 2017:18.7%; 2018:20.6%; 2019:24.6%; 2020:24.9%; 2021:33.8%. Of all speaker slots, the percentage of plenary slots did not differ based on gender, with 11.4% presented by female speakers versus 11.2% presented by male speakers (OR 1.0, 95% CI 0.7– 1.5, P=0.893). Compared to male speaker slots, there was an association of lower age (43.9± 5.6 vs 50.8± 8.9, P< 0.001), lower odds of holding a single doctorate degree (OR 0.3, 95% CI 0.2– 0.5, P< 0.001), and lower odds of holding a dual MD/PhD or DO/PhD degree (OR 0.3, 95% CI 0.1– 0.5, P< 0.001) in female speaker slots. Compared to male speakers, there was an association of higher number of presentations per female speaker at the 2021 NANS Annual Meeting (2.48± 1.60 vs 1.79± 1.30, P=0.008).
Conclusion: Although the volume of female speaker slots and individual speakers trailed behind their male counterparts, female speaker representation steadily increased at each subsequent annual NANS meeting. We identified no difference in plenary session slots based on gender.
Keywords: education, leadership, academic advancement, chronic pain, neuromodulation, gender
Introduction
Representation of women in medicine is increasing in the United States,1 with women now comprising about one-half of medical school applicants and matriculants.2 Yet, gender inequalities persist in academic institutions,3 as highlighted by fewer women achieving professorship rank, holding chairperson appointments, receiving invitations to journal editorial roles, or occupying other leadership roles.4–8 While these disparities are evident across most medical disciplines, they are even more prominent in interventional and surgical subspecialties, such as interventional pain medicine.4,5 A significant issue is the “leaky pipeline” where women fall from the academic ladder, which in turn depletes the potential pool of female candidates for senior academic ranks and leadership positions.9 Prior studies have proposed potential explanations including inadequate time for women to rise through the ranks, significant family responsibilities, domestic responsibilities, lack of role models, inadequate mentoring, discrimination, and implicit biases in hiring and promotion.5,10 These observations suggest that the focus of our responsibilities should shift from merely increasing medical training access to instead equalizing opportunity for the female workforce to facilitate achievement of their full career potential, attain academic advancement, receive appropriate financial remuneration, and importantly feel supported in their career aspirations.3
Speaker gender representation at medical conferences is a notable area of gender disparity.11 There is strong evidence highlighting that women are underrepresented as speakers across medical disciplines including emergency medicine, global health, and surgery.11–14 This occurrence is particularly highlighted by the presence of all-male panels in conference programs, colloquially coined as “manels”.11 Despite many conferences having a 1:1 ratio of women and men among conference attendees, women spoke less than men with an equivalent academic standing;15 further, male attendees asked almost twice as many questions as female attendees, suggesting that factors such as an unwelcoming and “chilly” climate for women in academic medicine may play substantial roles.16 Even in situations where the volume of female speakers is well-represented in conference programs, they may be less likely to receive invitations to deliver highly coveted plenary sessions and keynote presentations.17 Speaker invitations to society conferences are vital to enhancing the speaker’s visibility and recognition in the field, opens doors for new collaborations with other prominent leaders, and helps establish the speaker as an expert in the field.18 Further, invited speakerships are a crucial component for the pathway to academic promotion.19 Specifically, presentation opportunities at plenary sessions or grand rounds sessions are assessed by promotion and tenure committees and are a marker of external recognition. Therefore, gender disparities in speaker opportunities can significantly affect career progression for women in medicine.
To better understand the inequity of female speaker representation in an interventional pain conference, we conducted a five-year analysis (2017–2021) quantifying the proportion of female speakers and factors associated with female speaker representation at the North American Neuromodulation Society (NANS) Annual Conference. Findings from this study would contribute to the scientific literature on gender representation in academic medicine, as well as advance the goals of the NANS organization in maintaining and training a diverse workforce.
Methods
Ethics
The project was deemed as exempt by the Mayo Clinic Institutional Review Board and conformed to principles per the Declaration of Helsinki.
Data Source and Extraction
The annual NANS conference is a well-known and well-attended interventional pain conference with a focus on neuromodulation interventions. The NANS organization and annual conference attracts membership from diverse specialties in pain medicine, including professionals in anesthesiology, physical medicine and rehabilitation, neurology, neurosurgery, emergency medicine, internal medicine, psychiatry, engineering, and other disciplines. Most NANS conference attendees are from the United States, although international delegates frequently attend NANS annual conferences as well as serve on various NANS committee boards. Further, NANS attendees and committee board members are well-represented by both faculty from academic institutions and clinical professionals working in private practice.
Data from the 2017–2021 NANS Annual Conference presentations were abstracted from a database maintained by the NANS society on 10/24/21. Although program data are publicly available for recent NANS conferences (past 1–2 years), data describing prior conferences are not publicly available and were obtained from a database maintained by the NANS organization. Data variables extracted included: speaker first and last name, session title, type of session (plenary, thematic abstract, concurrent session), session size (number of speaker slots in that session), and professional degree(s). A plenary session, also known as general session or main session, is defined as a session where all conference attendees are gathered together to attend. When two or more breakout sessions are held at the same time, they are known as concurrent sessions. Conference attendees can choose which concurrent session to attend. For all sessions included in our analysis (plenary, thematic abstract, or concurrent session), speakers are offered these opportunities by invitation only. Furthermore, due to the Coronavirus Disease 2019 (COVID-19) pandemic, the 2021 annual meeting was held virtually and thus this manuscript can provide unique insights on gender representation in an online conference format.
Session and Speaker Identification
Two co-investigators (BL and RSD) performed manual chart review of all sessions. Inclusion criteria comprised of any speaker, regardless of professional degree (physician or non-physician), who presented in the main meeting. We excluded pre-conference sessions, poster abstract presentations, and problem-based learning discussions. Our justification for these exclusions was that these sessions are unlikely to be invited, and frequently include faculty who have designed the proposals for these sessions.20 Further, poster abstract presentations were commonly presented by resident or fellow trainees, and there was no specific presentation time slot devoted to one poster presentation at a time. Poster abstract presentations were all presented concomitantly, while attendees rotated to view posters.
In terms of definitions, a speaker slot is only filled by one individual speaker. Since an individual speaker can deliver multiple presentations (eg fill multiple presentation slots), we provide data below on both individual speaker gender and the gender of the individual speaker filling a speaker slot. On the contrary, a session is comprised of multiple individual speakers.
Determination of Speaker Gender
While gender is a multidimensional and fluid concept that is determined by the individual, our study assumed binary gender identity to facilitate analysis. We utilized publicly available sources including online healthcare directories (www.healthgrades.com), state licensure boards, online curriculum vitae, and program websites to identify the gender of all speakers. Other methods have been described, such as a commercially available name-based gender identification software (Gender API, http://gender-api.com/Munich). This software utilizes multiple sources of data from governmental databases and social networks to determine gender identity of a name and assigns a probability score.20 This modality was reserved as a last option to identify gender identity in our study.
Outcomes of Interest
Primary outcomes of interest included gender composition of speaker slots, gender composition of individual speakers, and comparison of plenary speaker slots by gender at the annual NANS meetings. Secondary outcomes of interest included comparisons of: session size by gender, age by gender, professional degree by gender, and number of presentations per speaker by gender. Session size was analyzed because larger session sizes may diffuse the prominence and visibility of individual speakers compared to smaller session sizes. Given the greater impact of childbearing and parenthood on women in academia, age was considered an important variable because it may take longer for female professionals to gain visibility in the field and obtain speaker invitations. Similarly, the type of professional degree may also play a role in speaker invitations, possibly favoring those with more advanced degrees and dual advanced degrees.
Statistical Analyses
We reported continuous outcomes as mean with standard deviation and dichotomous categorical outcomes as overall counts with percent. Univariable regression analysis was utilized to evaluate whether certain variables have a greater propensity for association with male or female gender. Specifically, variables assessed included: type of session, session size, age, professional degree, and number of presentations per speaker between female and male gender. The selected regression model was dependent on the outcome variable: binary logistic regression was conducted if the outcome variable consisted of two possible categorical outcomes (plenary vs non-plenary session); multinomial logistic regression was conducted if the outcome variable consisted of three or more possible categorical outcomes (professional degree); and, linear regression was conducted if the dependent variable was continuous (session size, age, number of presentations per speaker). Effect sizes for logistic regression were presented as odds ratio (OR) with 95% confidence interval (CI), and effect sizes for linear regression were presented as β-coefficient with 95% CI. A P-value <0.05 was considered statistically significant.
Results
Baseline Characteristics and Gender Composition
Over the five NANS annual meetings studied, there were a total of 1583 speaker slots for individual presentations meeting our criteria (Table 1), which comprised of 376 slots presented by female speakers (23.8%) and 1207 slots presented by male speakers (76.2%). In total, there were 556 unique speakers, comprised of 143 (25.7%) female speakers and 413 (74.3%) male speakers.
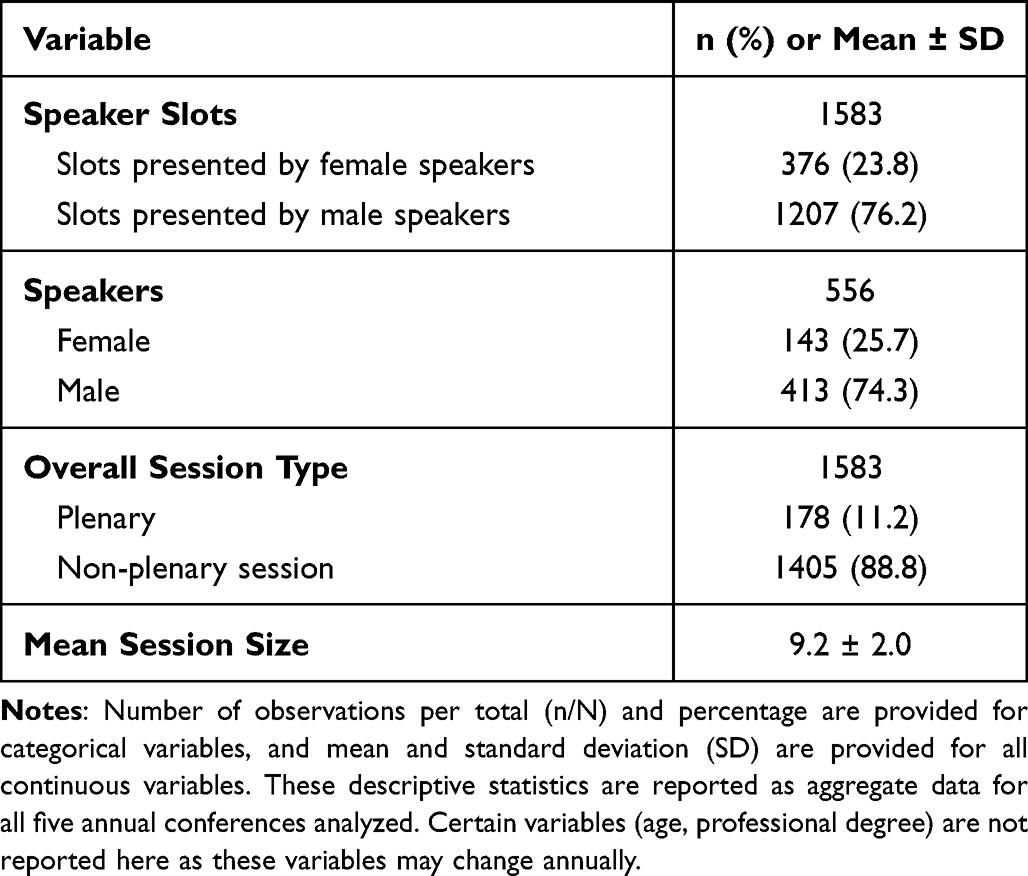 |
Table 1 Baseline Variables of Overall Sample |
The gender composition of annual speaker slots was as follows (% slots presented by women, Figure 1): 2017: 14.6%; 2018: 20.5%; 2019: 23.5%; 2020: 21.0%; 2021: 41.4%. Annual gender composition of unique individual speakers was as follows (% women, Figure 2): 2017: 18.7%; 2018: 20.6%; 2019: 24.6%; 2020: 24.9%; 2021: 33.8%.
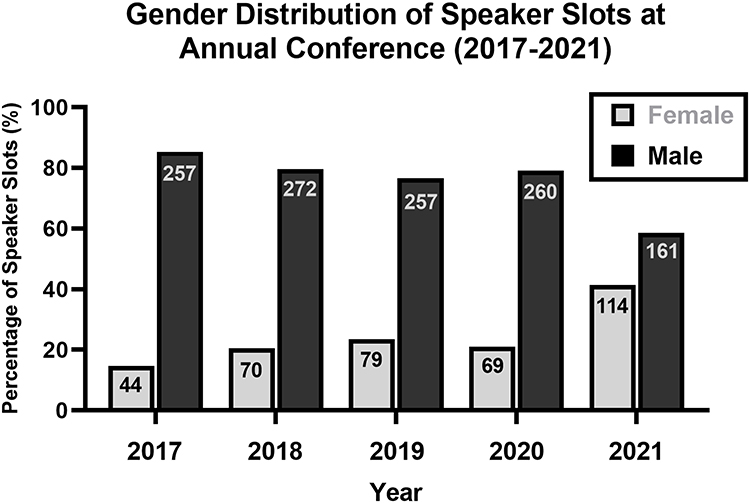 |
Figure 1 Gender Distribution of Speaker Slots at Annual Conference. The percentage of all speaker slots is stratified by gender and is presented for each separate annual NANS conference from year 2017 to year 2021. The absolute value is provided within each bar to reflect the absolute number of speaker slots filled by female and male speakers for that specific conference year. |
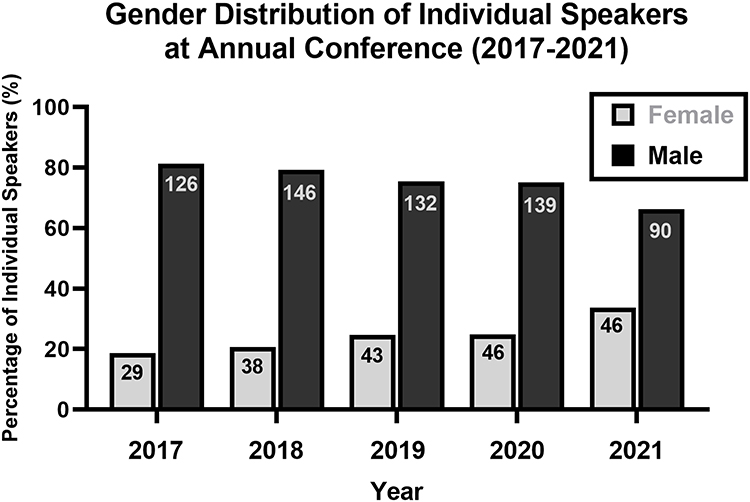 |
Figure 2 Gender Distribution of Speakers at Annual Conference. The percentage of all individual speakers is stratified by gender and is presented for each separate annual NANS conference from year 2017 to year 2021. The absolute value is provided within each bar to reflect the absolute number of female and male speakers for that specific conference year. |
Primary Outcomes of Interest
Of all speaker slots, the percentage of plenary speaker slots did not differ based on gender (Table 2), with 11.4% presented by female speakers versus 11.2% presented by male speakers (11.2%; OR 1.0, 95% CI 0.7–1.5, P=0.893).
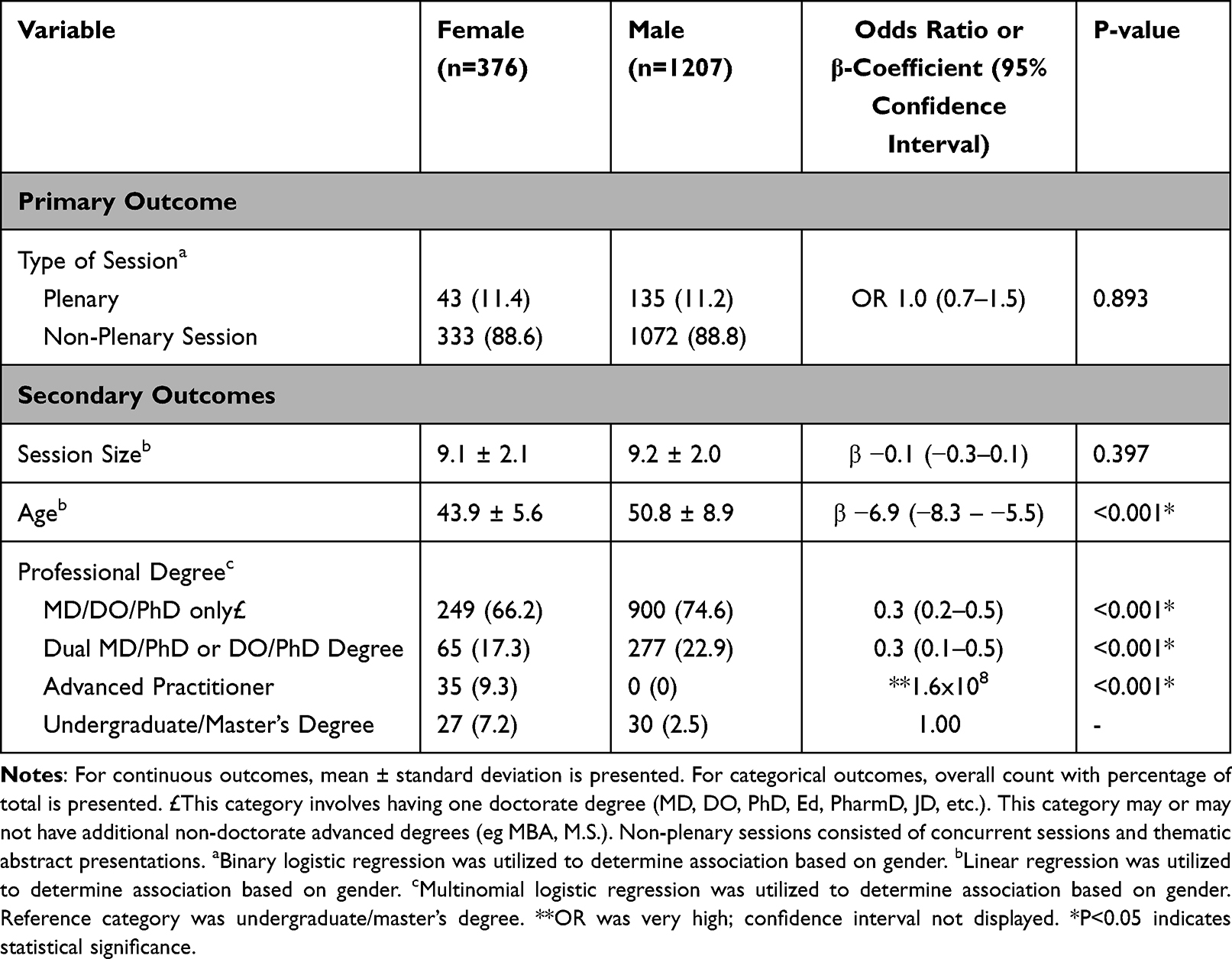 |
Table 2 Characteristics of Speaker Slots Stratified by Gender (Years 2017–2021) |
Secondary Outcomes of Interest
There was no difference in session size between female speakers slots (9.1 ± 2.1) and male speaker slots (9.2 ± 2.0; β −0.1, 95% CI −0.3–0.1, P=0.397; Table 2). Although session size ranged from 5 to 20 speakers, approximately 88.3% of female speakers and 89.6% of male speakers presented in a session featuring 7–10 speakers. There was a significantly higher age in male speaker slots (50.8 ± 8.9 years) compared to female speaker slots (43.9 ± 5.6 years; β −6.9, 95% CI −8.3 – −5.5, P<0.001). Multinomial logistic regression revealed a lower representation of female gender in speaker slots filled by those holding a single doctorate degree (OR 0.3, 95% CI 0.2–0.5, P<0.001), and those holding a dual MD/PhD or DO/PhD degree (OR 0.3, 95% CI 0.1–0.5, P<0.001). There were 35 speaker slots filled by female advanced practice providers ([APPs], 9.3%), but no speaker slots filled by male APPs (P<0.001).
Compared to male speakers, there was an association of higher number of presentations per female speaker at the 2021 NANS Annual Meeting (2.48 ± 1.60 versus 1.79 ± 1.30, P = 0.008; Table 3). No differences in number of presentations per speaker based on gender were identified in other NANS annual meetings or in the overall sample.
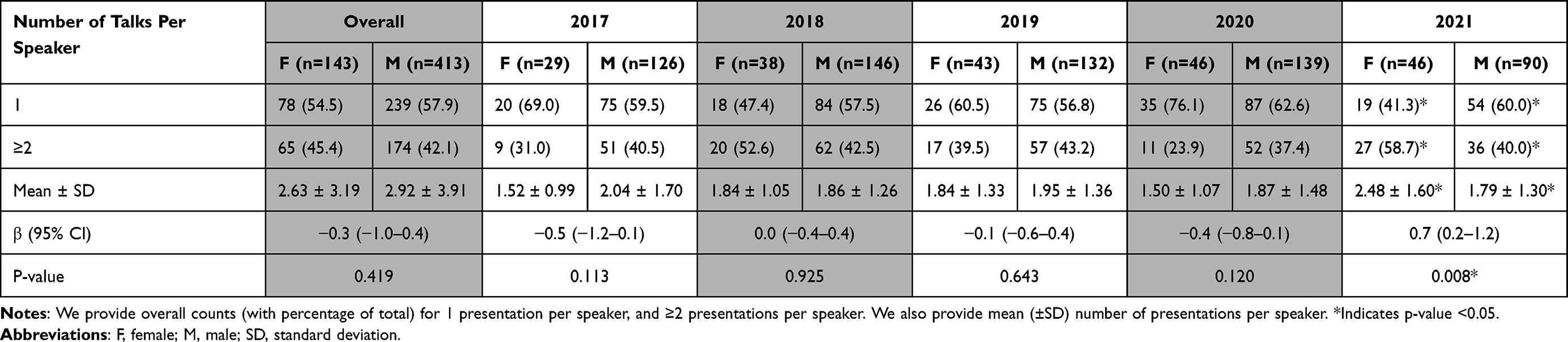 |
Table 3 Number of Presentations per Speaker by Gender |
Discussion
In this five-year cross-sectional analysis, we observed that the number of female speaker slots and individual female speakers were lower than male speaker slots and individual male speakers, respectively. Female representation has been steadily increasing at each subsequent annual meeting and achieved its highest volume in the 2021 annual meeting. This change is particularly highlighted by 41.4% of speaker slots held by women in the 2021 Annual NANS meeting versus only 14.6% of speaker slots held by women in the 2017 Annual NANS meeting. Importantly, we identified no difference in plenary session slots based on gender in the entire five-year sample. These findings highlight gradual improvements in speaker gender disparity at a major conference that attracts national and international professionals from diverse disciplines. Our observations contradict the existing literature on gender composition in other notable conferences from other medical fields, which generally highlight persistent underrepresentation in female composition and higher number of plenary invitations to male speakers.11–13,17
Potential explanations for our findings include an increase in female leadership among the NANS organization committees, particularly within the scientific planning committee. This potential explanation is concordant with prior literature highlighting that inclusion of more women as conveners, who invite speakers and moderate conference sessions, may increase the proportion of women who are invited to speak at scientific meetings.9 Several studies have also highlighted that female leadership may be associated with higher proportion of female faculty and trainees in pain medicine21 and other medical specialties.22 Furthermore, the Women in Neuromodulation (WIN) section was recently created within the NANS organization with an overarching purpose to
educate, inspire, and encourage women working in the field of neuromodulation, regardless of medical specialty, to realize their professional and personal goals and to serve the discipline in addressing the issues inherent to training and maintaining a diverse and balanced workforce23.
These initiatives are crucial to motivate more prospective female professionals to consider pursuing interventional medical fields such as pain medicine, reduce the barriers toward academic advancement, and maintain and cherish diversity in a field that is already represented by diverse medical disciplines. Another potential explanation for the increase in female speakers is an increase in the female workforce. However, public specialty data from the Association of American Medical Colleges highlight that 19.0% of pain management physicians were female in 2019, which did not increase substantially from year 2015 when 18.3% of pain management physicians were female.24 It is concerning that these percentages are unlikely to rise significantly in the near future since women represent about 22% of pain medicine fellows.25
Although volume of female professionals in annual NANS meetings is gradually improving, some notable discrepancies in our data may raise concern. For instance, while speaker slots held by women increased to 41.4% at the annual 2021 meeting, individual female speakers actually comprised only 33.8% of total speakers. This discrepancy is explained by a higher number of presentations delivered per female speaker (2.48 ± 1.60) versus presentations per male speaker (1.79 ± 1.30, P=0.008) at the 2021 NANS annual meeting. This occurrence may be advantageous by providing additional speaker opportunities, which in turn may increase visibility and recognition in the field. However, the burden of delivering multiple talks at each conference necessitates more resources, time, and commitment which may detract from other potential opportunities at the conference such as collaboration with other field experts and participation in other educational events (eg workshops). This also limits opportunities to a smaller number of women in the field. Due to the COVID-19 pandemic, the 2021 NANS annual meeting was the first fully virtual meeting held by NANS and the authors query whether the virtual format permitted more women to fulfill virtual speaker engagements. Because of the disproportionate burden of household and child care responsibilities that fall on female professionals,26 it is plausible that the virtual format may have facilitated a higher acceptance and willingness to speak among invited female speakers. Future studies should investigate if the rate of speaker invitation to acceptance ratio differs between in-person meetings versus virtual meetings. It is important to note that the disparity in individual female speakers may be representative of the pain medicine field. Physician specialty data from the Association of American Medical Colleges reveal that only 19.0% of pain management physicians are women.24 Further, a study of 3256 pain fellows from 2009 to 2019 revealed that the ratio of men to women pain fellows was between 5:1 and 3.7:1.27 There are currently no data on gender representation in the field of neuromodulation, although it may approach the representation present in the pain medicine field.
While not the focus of this study, our analysis identified that there were no APPs represented as speakers in the 2017 annual meeting. With the advent of the 2018 annual meeting and each subsequent meeting thereafter, APPs gradually experienced greater representation among speakers. Potential explanations include the NANS leadership placing more emphasis on increasing diversity among speakers, attempting to increase conference attendance of APPs, and embracing and reflecting the multidisciplinary and team-based approach in pain medicine. Interestingly, male APP speakers did not deliver any presentations throughout the entire five-year study period. This is likely explained by a higher proportion of females among all APPs,28,29 and is a future area of investigation for the NANS organization. Male APP speakers have been included in the NANS APP pre-conference sessions, although this is not reflected in this analysis because pre-conference sessions were excluded.
Another notable conference devoted to neuromodulation and interventional pain medicine is the International Neuromodulation Society (INS). Given the substantial heterogeneity of combining datasets from two separate societies and cancellation of the two recent in-person INS meetings, we decided not to abstract and combine data from the INS annual meetings. However, this may be an area of future investigation to determine the external validity of our study findings. Other areas that warrant investigation include racial representation among speakers, implementation and assessment of strategies to promote speaker diversity, and dissemination of content devoted toward diversity in neuromodulation.
Conclusions in the present study are constrained by study methodology, ascertainment of speaker details, and assumptions that the NANS database accurately reflected all speakers. Notable study limitations include a retrospective cross-sectional study design that may omit certain key variables such as metrics of peer-reviewed publication productivity (eg Hirsch-index), institutional leadership positions (eg division chair, program director), and NANS society leadership positions. These variables may be important components in determining visibility of the individual, and may be associated with invitations to present at the annual NANS conference. Missing data for certain variables (eg age) may impact study findings. Reporting bias may impact data extracted from public databases. The 2021 annual meeting was held virtually while the other annual meetings were held in-person, introducing some heterogeneity into our analysis. Finally, we categorized gender using a binary construct that did not account for non-binary people. Inclusion of non-binary people would have further highlighted the representation of another under-represented cohort in academic medicine. Further investigation is also warranted on other diverse populations in academic medicine such as sole parents, same-gender couples, those living outside the couple structure, dual career academic couples, those with complex and multiple caring duties, those conducting migrant academics, and those conducting academic medicine in remote locations that are distant from travel hubs. Future research on this topic may highlight implications on the intersection between care, mobility, and academic medicine. Future studies should determine if the recent increase in female speaker representation at the NANS annual meeting will be maintained in future annual meetings and approach male speaker representation. As aforementioned, even when female and male representation in conference attendance is similar, studies have highlighted that women speak far less than men. Future studies of the NANS annual meetings or other similar meetings should determine if length of presentations differ based on gender. Studies on gender representation among other society roles, such as committee leadership positions and other membership roles, may contribute to the literature. Concordant with this study’s objective and the NANS mission of promoting diversity, we also welcome future studies assessing speaker representation based on race and other sociodemographic variables (eg geographical location).
Conclusion
Although the volume of female speaker slots and individual female speakers trailed behind their male counterparts, female speaker representation steadily increased at each subsequent annual NANS meeting. In 2017, only 14.6% of speaker slots were held by women. However, a peak of 41.4% of speaker slots held by women was attained in the 2021 Annual NANS meeting. Importantly, there was no difference in plenary session slots based on gender. There was an association of lower age, lower odds of single doctorate degree, and lower odds of dual MD/PhD or DO/PhD in female speaker slots versus male speaker slots. Future studies are warranted to confirm the external validity of our findings to other notable society meetings.
Author Contributions
RSD was involved in study conception, study design, data collection, statistical analysis, manuscript composition, and final manuscript approval. All authors made significant contribution to the work reported (conception, study design, executing, acquisition of data, analysis or interpretation), drafted or revised or critically reviewed the article, agreed to the journal of submission, reviewed and agreed to all versions of the article before submission, during revision, and final version, and agree to take responsibility and accountability for the contents of the article.
Disclosure
Ryan D’Souza receives research support from Nevro Corp for an investigator-initiated grant. Julie Pilitsis is a consultant for Boston Scientific, Nevro, TerSera, Abbott, and receives grant support from Medtronic, Boston Scientific, Abbott, Nevro, TerSera, NIH 2R01CA166379-06, and NIH U44NS115111. Chelsey Hoffmann is a consultant for Sprint Therapeutics and Nalu Medical. Magdalena Anitescu reports personal fees from Boston Scientific, personal fees from Medtronic, outside the submitted work. Stephanie Vanterpool is a consultant for Abbott, Nevro, and Boston Scientific. Kiran Patel is a consultant and speaker for Abbott. Brendan Langford, Vwaire Orhurhu, Nasir Hussain, Magdalena Anitescu, Rushna Ali, and Susan Moeschler have no COI. The authors report no other conflicts of interest in this work.
References
1. Penny M, Jeffries R, Grant J, Davies SC. Women and academic medicine: a review of the evidence on female representation. J R Soc Med. 2014;107(7):259–263. doi:10.1177/0141076814528893
2. Joseph MM, Ahasic AM, Clark J, Templeton K. State of women in medicine: history, challenges, and the benefits of a diverse workforce. Pediatrics. 2021;148(Suppl 2). doi:10.1542/peds.2021-051440C
3. Bailey EL. Women in medicine: increasing in number but not regard. Br J Gen Pract. 2020;70(695):296. doi:10.3399/bjgp20X710225
4. D’Souza RS, Langford B, Moeschler S. Gender representation in fellowship program director positions in ACGME-accredited chronic pain and acute pain fellowship programs. Pain Med. 2021;22(6):1360–1366. doi:10.1093/pm/pnab041
5. Bissing MA, Lange EMS, Davila WF, et al. Status of women in academic anesthesiology: a 10-year update. Anesth Analg. 2019;128(1):137–143. doi:10.1213/ANE.0000000000003691
6. D’Souza R, King R, Strand N, Barman R, Olatoye O. Gender Disparity Persists in Pain Medicine: a Cross-Sectional Study of Chairpersons within ACGME-Accredited Chronic Pain Fellowship Programs in the United States. JEPM. 2022;24. E680
7. Orhurhu MS, Orhurhu V, Salisu B, Abimbola A, Cohen SP. Factors associated with academic rank among chronic pain medicine faculty in the USA. Reg Anesth Pain Med. 2020;45(8):589–596. doi:10.1136/rapm-2019-101139
8. D’Souza RS, Langford B, D’Souza S, Rose S, Long T. Characteristics of designated institutional officials and sponsoring institutions of ACGME-accredited training programs. J Grad Med Educ. 2021;13(1):70–75. doi:10.4300/JGME-D-20-00313.1
9. Casadevall A, Handelsman J, Miller JF. The presence of female conveners correlates with a higher proportion of female speakers at scientific symposia. mBio. 2014;5(1):e00846–e00913. doi:10.1128/mBio.00846-13
10. Henderson EF. Sticky care and conference travel: unpacking care as an explanatory factor for gendered academic immobility. Higher Educ. 2021;82(4):715–730. doi:10.1007/s10734-020-00550-1
11. Arora A, Kaur Y, Dossa F, Nisenbaum R, Little D, Baxter NN. Proportion of female speakers at academic medical conferences across multiple specialties and regions. JAMA Netw Open. 2020;3(9):e2018127. doi:10.1001/jamanetworkopen.2020.18127
12. Carley S, Carden R, Riley R, et al. Are there too few women presenting at emergency medicine conferences? Emerg Med J. 2016;33(10):681–683. doi:10.1136/emermed-2015-205581
13. Schroeder E, Rochford C, Voss M, Gabrysch S. Beyond representation: women at global health conferences. Lancet. 2019;393(10177):1200–1201. doi:10.1016/S0140-6736(18)32854-X
14. Walters T. Gender equality in academic tourism, hospitality, leisure and events conferences. J Policy Res Tour Leis Events. 2018;10(1):17–32. doi:10.1080/19407963.2018.1403165
15. Jones TM, Fanson KV, Lanfear R, Symonds MR, Higgie M. Gender differences in conference presentations: a consequence of self-selection? PeerJ. 2014;2:e627. doi:10.7717/peerj.627
16. Hinsley A, Sutherland WJ, Johnston A, Pavlova MA. Men ask more questions than women at a scientific conference. PLoS One. 2017;12(10):e0185534. doi:10.1371/journal.pone.0185534
17. Sleeman KE, Koffman J, Higginson IJ. Leaky pipeline, gender bias, self-selection or all three? A quantitative analysis of gender balance at an international palliative care research conference. BMJ Support Palliat Care. 2019;9(2):146–148. doi:10.1136/bmjspcare-2016-001211
18. Martin JL, Bourne PE. Ten simple rules to achieve conference speaker gender balance. PLoS Comput Biol. 2014;10(11):e1003903. doi:10.1371/journal.pcbi.1003903
19. Kraus MB, Gali B, Cunningham GW, et al. Speaker gender representation for anesthesiology grand rounds at a large academic medical center. J Educ Perioper Med. 2020;22(4):E654. doi:10.46374/volxxii-issue4-sharpe
20. Moeschler SM, Gali B, Goyal S, et al. Speaker Gender representation at the American society of anesthesiology annual meeting: 2011–2016. Anesth Analg. 2019;129(1):301–305. doi:10.1213/ANE.0000000000003944
21. Hagedorn JM, Pittelkow T, Warner N, et al. Gender of pain medicine leadership and trainees: a survey study. Reg Anesth Pain Med. 2019:rapm-2019–100878. DOI:10.1136/rapm-2019-100878
22. Keane AM, Larson EL, Santosa KB, et al. Women in leadership and their influence on the gender diversity of academic plastic surgery programs. Plast Reconstr Surg. 2021;147(3):516–526. doi:10.1097/PRS.0000000000007681
23. North American Neuromodulation Society. Women in Neuromodulation. Available from: https://neuromodulation.org/Default.aspx?TabID=455.
24. Association of American Medical Colleges. Physician specialty data report; 2020.
25. Doshi TL, Bicket MC. Why aren’t there more female pain medicine physicians? Reg Anesth Pain Med. 2018;43(5):516–520. doi:10.1097/AAP.0000000000000774
26. ALobaid AM, Gosling CM, Khasawneh E, McKenna L, Williams B. Challenges faced by female healthcare professionals in the workforce: a scoping review. J Multidiscip Healthc. 2020;13:681–691. doi:10.2147/JMDH.S254922
27. Odonkor CA, Leitner B, Taraben S, et al. Diversity of pain medicine trainees and faculty in the United States: a cross-sectional analysis of fellowship training from 2009–2019. Pain Med. 2021;22(4):819–828. doi:10.1093/pm/pnab004
28. Bumbach MD, Harman JS, Lucero R, Cimiotti JP, Felber Neff D. Gender differences in nurse practitioners: job satisfaction and patterns of care. J Am Assoc Nurse Pract. 2020;32(2):138–144. doi:10.1097/JXX.0000000000000207
29. Lindsay S. The feminization of the physician assistant profession. Women Health. 2005;41(4):37–61. doi:10.1300/J013v41n04_03
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Becoming Leaders – A Qualitative Research Study on the Priorities and Concerns of Early Career Women Faculty in Academic Medicine
Liu O, Grieb SM, Halsey JN, Levine RB, Oliva-Hemker M, Lee JK
Journal of Healthcare Leadership 2024, 16:511-523
Published Date: 2 December 2024