Back to Journals » Journal of Pain Research » Volume 16
Somatosensory Outcomes Following Re-Surgery in Persistent Severe Pain After Groin Hernia Repair: A Prospective Observational Study
Authors Jensen EK ![]() , Ringsted TK, Bischoff JM, Petersen MA, Møller K, Kehlet H
, Ringsted TK, Bischoff JM, Petersen MA, Møller K, Kehlet H ![]() , Werner MU
, Werner MU ![]()
Received 11 August 2022
Accepted for publication 25 February 2023
Published 17 March 2023 Volume 2023:16 Pages 943—959
DOI https://doi.org/10.2147/JPR.S384973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erika Petersen
Elisabeth Kjær Jensen,1,* Thomas K Ringsted,1,* Joakim M Bischoff,1 Morten A Petersen,2 Kirsten Møller,3,4 Henrik Kehlet,5 Mads U Werner1,6
1Department of Anaesthesia, Pain and Respiratory Support, Copenhagen University Hospital-Rigshospitalet, Copenhagen, Denmark; 2Statistical Research Unit, Department of Palliative Care, Bispebjerg Hospital, Copenhagen, Denmark; 3Department of Neuroanaesthesiology, Copenhagen University Hospital-Rigshospitalet, Copenhagen, Denmark; 4Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 5Section for Surgical Pathophysiology, Copenhagen University Hospital-Rigshospitalet, Copenhagen, Denmark; 6Department of Clinical Sciences, Lund University, Lund, Sweden
*These authors contributed equally to this work
Correspondence: Elisabeth Kjær Jensen, Multidisciplinary Pain Center 7612, Department of Anesthesia, Pain and Respiratory Support, Neuroscience Center, Rigshospitalet, Ole Maaløes Vej 26, Copenhagen N, 2200, Denmark, Tel +45 3545 7612, Email [email protected]
Purpose: After groin hernia repair (globally more than 20 million/year) 2– 4% will develop persistent severe pain (PSPG). Pain management is challenging and may require multimodal interventions, including re-surgery. Quantitative somatosensory testing (QST) is an investigational psychophysiological tool with the potential to uncover the pathophysiological mechanisms behind the pain, ie, revealing neuropathic or inflammatory components. The primary objective was to examine and describe the underlying pathophysiological changes in the groin areas by QST before and after re-surgery with mesh removal and selective neurectomy.
Patients and Methods: Sixty patients with PSPG scheduled for re-surgery and with an inflammatory “component” indicated by blunt pressure algometry were examined in median (95% CI) 7.9 (5.8– 11.5) months before and 4.0 (3.5– 4.6) months after re-surgery. The QST-analyses included standardized assessments of cutaneous mechanical/thermal detection and pain thresholds. Suprathreshold heat stimuli were applied. Deep tissue sensitivity was tested by pressure algometry. Testing sites were the groin areas and the lower arm. Before/after QST data were z-transformed.
Results: Re-surgery resulted in median changes in rest, average, and maximal pain intensity scores of − 2.0, − 2.5, and − 2.0 NRS (0/10) units, respectively (P = 0.0001), and proportional increases in various standardized functional scores (P = 0.0001). Compared with the control sites, the cutaneous somatosensory detection thresholds of the painful groin were increased before re-surgery and increased further after re-surgery (median difference: 1.28 z-values; P = 0.001), indicating a successive post-surgical loss of nerve fiber function (“deafferentation”). Pressure algometry thresholds increased after re-surgery (median difference: 0.30 z-values; P = 0.001).
Conclusion: In this subset of patients with PSPG who underwent re-surgery, the procedure was associated with improved pain and functional outcomes. While the increase in somatosensory detection thresholds mirrors the surgery-induced cutaneous deafferentation, the increase in pressure algometry thresholds mirrors the removal of the deep “pain generator”. The QST-analyses are useful adjuncts in mechanism-based somatosensory research.
Keywords: groin, hernia repair, chronic post-surgical pain, reoperation, sensory thresholds
Introduction
Persistent severe pain occurring in the aftermath of a surgical procedure is frequently associated with significant impairment of physical and psycho-social functions.1–4 After groin hernia repair (GHR), 2–4% of patients develop persistent severe pain. The GHR procedure, previously considered belonging to “minor” surgeries, qualifies as a rather complex procedure performed in a territory with a high density of nerve fibers, accommodating essential functions for locomotion and reproduction. More than 20 million repairs are performed annually worldwide,5 and consequently, it is estimated that 400.000–800.000 patients each year will develop persistent severe pain after the groin hernia repair (PSPG). Management of PSPG is medically challenging and may require re-surgery with mesh removal and selective neurectomy.6–9 After re-surgery for pain after open primary GHR, a potential pain-relieving effect, as well as an improvement of the deteriorated physical functions, has been demonstrated.10–12
Quantitative somatosensory testing (QST) is an investigational psychophysiological tool with the potential to uncover the putative pathophysiological substrate in PSPG, ie, neuropathic and inflammatory constituents.13,14 The cutaneous thermal and mechanical stimulation modalities may preferentially indicate a neuropathic origin of pain, while the deep mechanical stimulation by pressure algometry may preferentially uncover an inflammatory origin of pain. The QST method may also facilitate the quantitation of changes induced by the re-surgery.12 Since re-surgery is a potential neuroablative procedure, essentially performed in previously damaged tissue, it is of interest to examine the extent of neurological perturbations, ie, “loss” and “gain” of sensory functions and the relation to clinical outcome measures.
The authors are only aware of one previous PSPG-study (n = 21) finding that re-surgery, including meshectomy and selective neurectomy, was associated with increased pressure pain thresholds, decreased pain ratings, and improved pain-related functional measures.12 The objectives of the current study, comparing pre with post-re-surgery data of patients with PSPG and an inflammatory “component” indicated by blunt pressure algometry, were to perform a more detailed analysis of the quantitative somatosensory data regarding “loss” and “gain” of sensory functions and their relation to clinical outcome measures using a threefold larger cohort.12
Materials and Methods
Research Ethics
Approvals
The study was approved by the Regional Committee on Health Research Ethics: (H-2-2011-023 and KF 11320499) and The Danish Data Protection Agency (2012-41-0008). The study was registered on ClinicalTrials.gov (NCT05238571) and complied with the Declaration of Helsinki most recently amended 2013. All patients signed informed consent prior to their inclusion in the study. The authors have previously conducted a long-term follow-up study (n = 204 available: 172 included) to assess the clinical outcomes of patients with PSPG.8 The current study includes baseline data from 52 patients participating in the previous study. The short-term somatosensory and clinical outcome data relating to the re-surgery have not previously been published.
Study Design
The study was a prospective observational study (Supplementary Table 1).
Study Subjects
Recruitment
The study was conducted at a dedicated center specialized in the management of patients with persistent severe pain after groin hernia repair.8 Patients were referred to the center on a nationwide basis via the Danish Hernia Database’s homepage (http://www.herniedatabasen.dk) by surgeons or general practitioners (Supplementary Figure 1). All patients referred to the center were consecutively offered to participate in the study at the first ambulatory visit. Patients were enrolled in the study between 24-APR-2009 and 19-MAR-2015.
Inclusion Criteria
Patients (>18 yrs) with persistent severe pain (activity-related or maximal pain intensity >7 NRS scores [numeric rating scale 0–10]) and PSPG-related serious impairment of working and social life following unilateral, uncomplicated, open GHR and referred to our center, were candidates to participate.8 However, only patients with criteria for an inflammatory “component” indicated by pressure algometry pain threshold (PPT; cf. “Pressure Pain Thresholds“) difference, compared to the contralateral side >50 kPa (PPT <150kPa) or >100 kPa (PPT >150 kPa), and scheduled for re-surgery with mesh removal and selective neurectomy, were included in the study. The deep tissue tenderness was anticipated to relate to a “meshoma”, an entrapped or dilated spermatic cord, a neuroma, or a combination of these.
Somatosensory Testing
All assessments of somatosensory function were performed in an undisturbed and well-lit room at the Multidisciplinary Pain Center, Copenhagen University Hospital-Rigshospitalet. The assessments were performed before and three to six months after the re-surgery by the same investigator (TKR, MUW, JMB). The methodology has previously been described in detail.8,15
Calibration
Calibration of the thermal equipment was performed by the manufacturer (Somedic AB, Sweden) prior to the study start. Calibrations of the monofilaments were done using a horizontally aligned precision scale (Fx-300i, A&D Weighing, CA). The pressure algometer was calibrated regularly according to the manufacturer’s instructions with a reference weight of 1.000 kg.
Testing Areas
All QST assessments were performed bilaterally in the groin and in the left lower arm, as previously described.8 For the initial assessment, the point of maximum tenderness upon digital palpation in the groin, in most cases corresponding to the superficial inguinal ring, was marked on the skin with a semi-permanent marker. A template was then used for delineating a rectangular testing area of 2.5×5.0 cm2 (corresponding to the area of the active surface of the thermode: Thermotest, Somedic AB, Sweden) containing the point of maximal tenderness situated at the center of the rectangle. These markings were transferred to a clear acetate sheet, ensuring that the post-re-surgical assessments were performed in the exact same area as the initial assessment. A homologous test area (control area) was mirrored on the corresponding site in the contralateral groin. An extra control area (2.5×5.0 cm2) was delineated longitudinally on the volar aspect of the non-dominant lower arm, with the distal margin 10 cm from the proximal wrist crease. Prior to assessments, excess hair growth in the testing areas was removed (Surgical Clipper 9681, 3M Healthcare, MN).
Mechanical Detection Thresholds
The mechanical detection thresholds (MDT) were assessed by a modified Dixon’s up-and-down method16 using a standard set of calibrated polyamide monofilaments (Stoelting Europe, Ireland; nominal buckling forces ranging from 0.04 to 4400 mN [logarithmic ordinal values from 1.65 to 6.65]).17 The filaments were applied perpendicularly to the skin, and patients indicated the presence of tactile sensation (MDT). Assessments of MDT were done six times, and the median values were used in the analyses. If the subject did not experience any tactile sensation during stimulation with the 6.65 monofilament, the MDT was assigned the ordinal value 6.85.
Thermal Detection Thresholds
Assessments of warmth detection threshold (WDT) and cool detection threshold (CDT) were done by use of a computerized thermode system. The baseline temperature was 32.0°C, and the ramp rate was ± 1.0°C/s. Cut-off temperatures were 50.0°C (WDT, HPT) and 5.0°C (CDT). The patient was instructed to use a handheld button device when a change in temperature sensation was recognized. The assessments were made in triplicates. The mean values were used in the analyses.
Pressure Pain Thresholds
An electronic handheld pressure algometer (Somedic AB, Sweden) with a felt-tipped probe of 1.0 cm2 was used to assess pain thresholds from deep tissues. The pressure algometer was applied perpendicularly to the skin over the point of maximum pain and corresponding control sites. The blunt pressure probe was applied with an increasing rate of 20–30 kPa/s until the patient indicated the PPT by a handheld button device. The cut-off limit was 350 kPa, and values exceeding this level were assigned the ordinal value of 351 kPa. The test was made in triplicate, and the median value was used in the calculations.
Heat Pain Thresholds
Assessments of heat pain threshold (HPT) were done by the computerized thermode. The assessments were made in triplicates, and the median values were used in the analyses.
Suprathreshold Heat Stimulus
A suprathreshold heat stimulus (STHS) was delivered with a computerized thermode. The thermode was set with a ramp rate of ± 1.0°C/s to reach a plateau of 47.0°C maintained for 5s. The patient was instructed to rate the pain intensity on an NRS scale. If the stimulus was perceived as too uncomfortable, the patient could discontinue the stimulus at any time with a handheld button. The score was calculated as the NRS divided by the duration of the stimulus (a detailed description is presented in Supplementary Text 1).
Temporal Summation
The presence of temporal summation phenomena (TSP), an indicator of central sensitization,18 was tested by repetitive dynamic stimulation with a brush (stroke rate 2–3 cm/s; stroke distance 4–5 cm; stimulation rate 0.3 Hz [SENSELab Brush-05, Somedic AB, Sweden]) and static stimulation by polyamide filaments (one ordinal value below the MPT; stimulation rate 0.5 Hz). Perceived pain intensity was rated by NRS every 15s. The stimulation continued for 60s unless discontinued by the patient due to evoked severe pain. The summation phenomena were evaluated on an ordinal scale, and each patient was assigned to a category (Supplementary Table 2) according to their response to each stimulation modality. Aftersensations were reported, and the pain/discomfort was rated (NRS) for the following 60s.
Questionnaires
Patients filled out a modified groin-hernia repair-specific questionnaire, the Activity Assessment Scale (AAS), evaluating the pain-related impact on Activities of Daily Living (ADL). The original AAS includes 13 statements regarding functional status. However, in the present study, a modified AAS was used, including 8/13 functional status levels. The modified AAS has previously been described in detail.8 The AAS scores were summed for specific activities (AASA-D) (minimum/maximum: 4/20 points) and overall activities (AASE-H) (minimum/maximum: 4/20 points). A higher AAS score indicates a higher negative impact of pain on ADL. The questionnaires were completed before the somatosensory testing sessions. In addition, questionnaires regarding pain intensity scores (NRS) at rest, on average and maximally, during the previous week were completed.
Surgical Procedures
All re-surgical procedures were performed as open surgery by the same surgeon (HK). The details of the surgical procedure have previously been described.8,10 Briefly, complete resection of the mesh and suture material was performed through the prior groin incision, and a conventional GHR (a.m. Bassini) without a mesh implant was performed. In the case of visually confirmed nerve entrapments or signs of lesioned nerves, a selective neurectomy was performed, transecting the nerve(s) 3–5 cm rostrally to the lesion.
Statistics
General note: Discussions concerning the indiscriminate use of P-values as an absolute means of null hypothesis testing have recently been reintroduced.19–21 In this manuscript, the term “statistical significance” is avoided. The advice “correct and careful interpretation of statistical tests demands examining the sizes of effect estimates and confidence limits, as well as precise P-values (not just whether P-values are above or below 0.05 or some other threshold)” is generally followed.22
Analyses of Data Distribution
Data distribution was checked for normality with the Shapiro–Wilk test and visual inspection of residual plots. Data are given as mean (95% CI) or median (95% CI) as appropriate. The MDT data were log-transformed without back-transformation. An a priori sample size estimation was not performed since a sample size of the comparator study of 21 subjects was adequate to confirm the primary objective.12 In the present study, 60 subjects were considered an adequate number to explore the quantitative somatosensory data in more detail.
Analyses of z-Scores
All QST modalities, before and after re-surgery, were standardized by calculating z-scores using the equation:

where xi denotes the modality-specific QST values from the ith patient compiled from the surgical groin or the lower arm. The reference values μCL and SDCL denote the mean and SD-values of the respective sensory modality, respectively, assessed from the contralateral groin. Positive z-scores exceed the mean value of the contralateral groin, whereas negative scores lie below. The modulus of the z-score is a measure of the deviation from the reference values from the contralateral groin.
The z-scores for MDT (zMDT), CDT (zCDT), and WDT (zWDT) were summed and divided by 3, constituting the z-scores of the detection thresholds of the non-nociceptive modalities (zDTH). The z-scores of PPT (zPPT), HPT (zHPT), and STHS (zSTHS) were used directly in the analyses of the nociceptive modalities. Simple comparisons of z-scores before and after surgery, as well as changes in pain scores, were done by the Wilcoxon matched-pairs signed-rank test.
Analyses of Independent Variables
Multiple linear regression models were fitted with the independent (predictor) variables; zDTH, zPPT, zHPT, and zSTHS (all before re-surgery). The dependent (outcome) variables were either ΔAAS scores (overall activities or specific activities) or ΔNRS scores (the sum of the at rest, average, and maximal pain intensity scores).
The within/between-subject reliability of the QST assessments was examined by two-way-random-effects, consistency, single rater/measurement, intra-class correlation coefficients (ICC)23 for the control areas in the lower arm and the contralateral groin. While there is no agreed-upon classification level of reliability for ICCs, for interpretation purposes ICCs were interpreted as indicating slight/poor (<0.2), fair (0.2 to 0.4), moderate (0.4 to 0.6), substantial (0.6 to 0.8) and almost perfect agreement (>0.8).24
In a comparison of the TSP categorical data before and after re-surgery, Fisher’s exact test was applied, and the effect size was presented as the phi (ϕ) coefficient. Statistical effect sizes for the multiple linear regression model and the Wilcoxon matched-pairs signed-rank test were presented as R2 (the coefficient of determination) and r ( ),25 respectively.
),25 respectively.
Analyses of Fractional Changes
The fractional change in functional scores (AAS) and pain intensity (NRS) after the re-surgery was calculated as:

where bRS denotes before re-surgery and aRS denotes after re-surgery. The relationships between summed AAS scores and summed NRS scores were examined by fitting a linear regression model on the fractional changes, with a reduction in pain (NRS) as the independent variable and the improvement in ADL outcomes as the dependent variable.
The number of patients needed to operate for one patient to achieve a positive outcome; a reduction in pain intensity (NRS) or an improvement of ADL outcomes (AAS) of ≥25%/50% were termed  and
and  . The number of patients needed to operate for one patient to be inflicted with a negative pain-related outcome, an increase in pain (NRS), or a deterioration in ADL outcomes (AAS) of ≥25%, were termed
. The number of patients needed to operate for one patient to be inflicted with a negative pain-related outcome, an increase in pain (NRS), or a deterioration in ADL outcomes (AAS) of ≥25%, were termed  and
and  , respectively:10
, respectively:10

where x equals the number of patients with a pain reduction (NRS) or improvement in ADL outcomes ≥25%/50%, y equals the number of patients with an increase in pain intensity (NRS) or deterioration of ADL outcomes ≥25%, and n equals the total number of patients.
Data Handling
Data were analyzed with Graphpad Prism (9.0.1 GraphPad Software, San Diego, CA, USA).
Results
Demographics
Sixty patients with persistent severe pain following unilateral, uncomplicated, open GHR were consecutively included in the study and underwent re-surgery (Supplementary Figure 1). Anthropometrics and demographics are reported in Table 1.
 |
Table 1 Anthropometrics and Demographics |
Somatosensory Testing Outcomes
Detection Thresholds
Following re-surgery, the median difference in zDTH of the painful groin was 1.28 (0.64 to 3.45; Wilcoxon matched-pairs signed-rank test; P = 0.001; r = 0.49), indicating a loss of non-nociceptive sensory function, ie, mechanical and thermal hypoesthesia (Figure 1; Table 2).
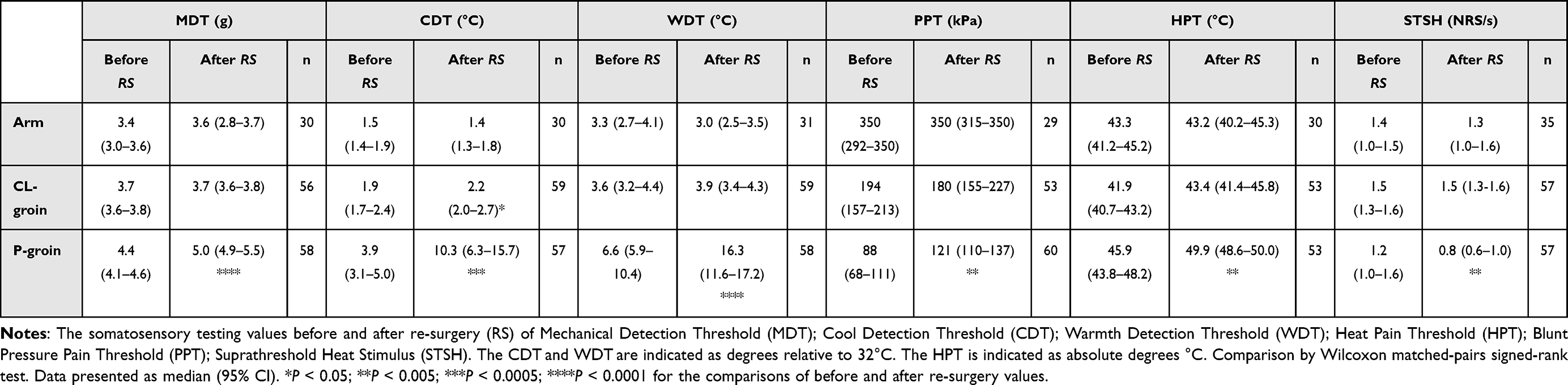 |
Table 2 The Somatosensory Testing Values Before and After Re-Surgery |
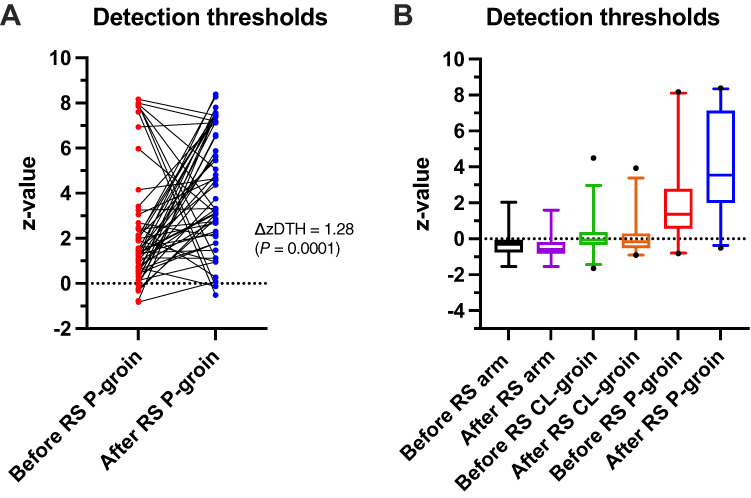 |
Figure 1 Detection Thresholds. The z-scores (zDTH; y-axes) of the mean of the detection thresholds ((MDT + CDT + WDT)/3) before and after re-surgery (RS; x-axes). Reference z-scores are calculated from the contralateral (CL) groin before and after RS. The dot-line diagram (A) illustrates individual zDTH-scores in the painful groin (P-groin) before and after re-surgery (ΔzDTH = 1.28; P = 0.0001; effect size = 0.49). The box-whisker plot (B) illustrates zDTH-scores in the lower arm, in the CL-groin, and in the P-groin before and after re-surgery. Whiskers indicate the 2.5 and 97.5 percentiles. Outliers are indicated. The comparisons of before/after re-surgery data were by Wilcoxon matched-pairs signed-rank tests. |
Pressure Pain Thresholds
Following re-surgery, the median difference in zPPT of the painful groin was 0.30 (0.06 to 0.69; Wilcoxon matched-pairs signed-rank test; P = 0.001; r = 0.40), indicating an increase in blunt PPT after the re-surgery (Figure 2; Table 2).
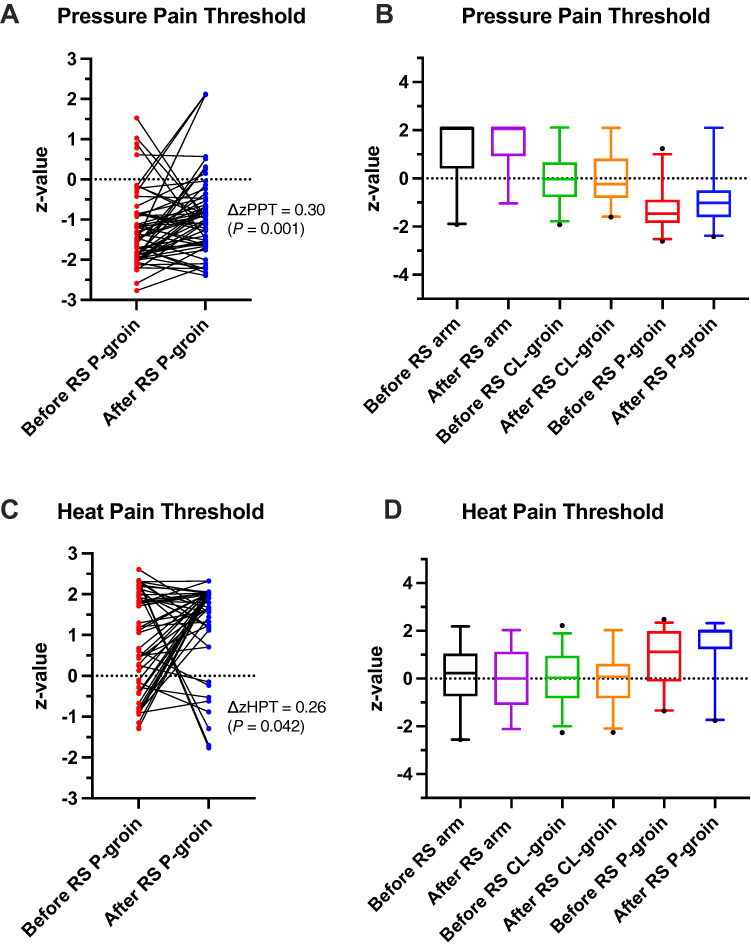 |
Figure 2 Mechanical and Thermal Pain Thresholds. The z-scores before and after re-surgery (RS) pertaining to blunt Pressure Pain Threshold (PPT; zPPT). Reference z-scores are calculated from the contralateral (CL) groin before and after re-surgery. The dot-line diagram (A) illustrates individual zPPT-scores in the painful groin (P-groin) before and after re-surgery (ΔzPPT = 0.30 P = 0.001; effect size = 0.40). The box-whisker plots (B) illustrate zPPT-scores in the lower arm, in the contralateral groin, and in the painful groin, respectively, before and after re-surgery. Please, note in (B), the distribution of PPT scores from the lower arm is skewed since the cut-off limit was reached in most subjects. The dot-line diagram (C) illustrates individual zHPT-scores in the painful groin before and after re-surgery (ΔHPT = 0.26 P = 0.042; effect size = 0.28). The box-whisker plots (D) zHPT-values in the lower arm, in the contralateral groin and in the painful groin, respectively, before and after re-surgery. Whiskers indicate the 2.5 and 97.5 percentiles. Outliers are indicated by dots. The comparisons of before/after re-surgery data were by Wilcoxon matched-pairs signed-rank tests. |
Thermal Pain Thresholds
Following re-surgery, the median difference in zHPT of the painful groin was 0.26 (−0.13 to 0.85; Wilcoxon matched-pairs signed-rank test; P = 0.042; r = 0.28) indicating an increase in HPT after the re-surgery (Figure 2; Table 2).
Suprathreshold Heat Stimulus
Following re-surgery, the median difference in zSTHS of the painful groin was −0.19 (−0.28 to 0.14; Wilcoxon matched-pairs signed-rank test; P = 0.001; r = 0.46), indicating that the re-surgery was associated with lowered pain scores during the STHS (Table 2; Supplementary Figure 2).
Temporal Summation with Brush
Before the re-surgery, 50/60 patients experienced TSP (Supplementary Table 3). Twenty-two of these reported painful aftersensations lasting >60s. After the re-surgery, 37/60 patients still experienced TSP (P = 0.013; ϕ = −0.24), and among these 15 patients reported painful aftersensations. Eight of the 37 patients with TSP after re-surgery did not experience TSP prior to re-surgery, indicating a surgery-associated shift in TSP-phenotype. Before the re-surgery, four patients experienced TSP during stimulation with the brush. After the re-surgery, three of these still experienced TSP by brush and additionally during stimulation with the polyamide monofilaments (Supplementary Table 3).
Temporal Summation with Monofilaments
Before the re-surgery, 21/60 patients experienced TSP during stimulation with the polyamide monofilaments. After re-surgery 30/60 (P = 0.139; ϕ = 0.15) patients experienced TSP by the polyamide monofilaments (Supplementary Table 3).
Test-Retest Reliability
The ICCs for assessments in the lower arm ranged from 0.53 to 0.77 (Table 3), except for STSH, where ICC was 0.11 (−0.25 to 0.44). Comparable ICCs for assessments at the contralateral groin ranged between 0.40 and 0.73 for all assessments except PPT and STHS, where the ICCs were 0.34 (0.08 to 0.56) and 0.28 (−0.02 to 0.47), respectively. The ICCs indicated a moderate to almost perfect reliability, except for PPT and STHS, where the reliability was indicated as fair.
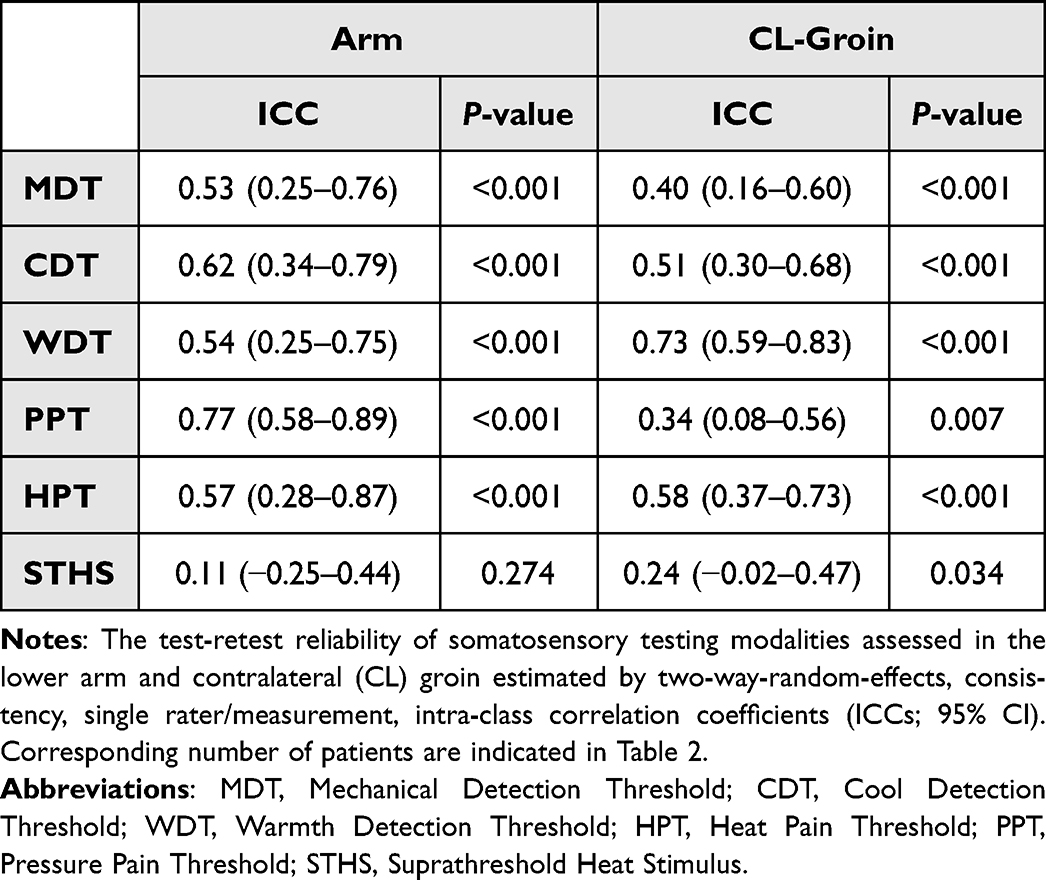 |
Table 3 The Test-Retest Reliability of Somatosensory Testing Modalities |
Clinical Outcomes
Pain Scores (NRS)
Re-surgery resulted in median differences in resting, average, and maximal pain intensity scores of −2.0, −2.5, and −2.0 NRS units, respectively (Wilcoxon matched-pairs signed-rank test, P = 0.0001, all scores [r = 0.63 to 0.71]; Table 4; Supplementary Figure 3). The median fractional changes for the resting, average, and maximal pain intensity scores were 0.5 (0.20 to 0.66), 0.42 (0.33 to 0.50) and 0.25 (0.12 to 0.40), respectively (Figure 3).
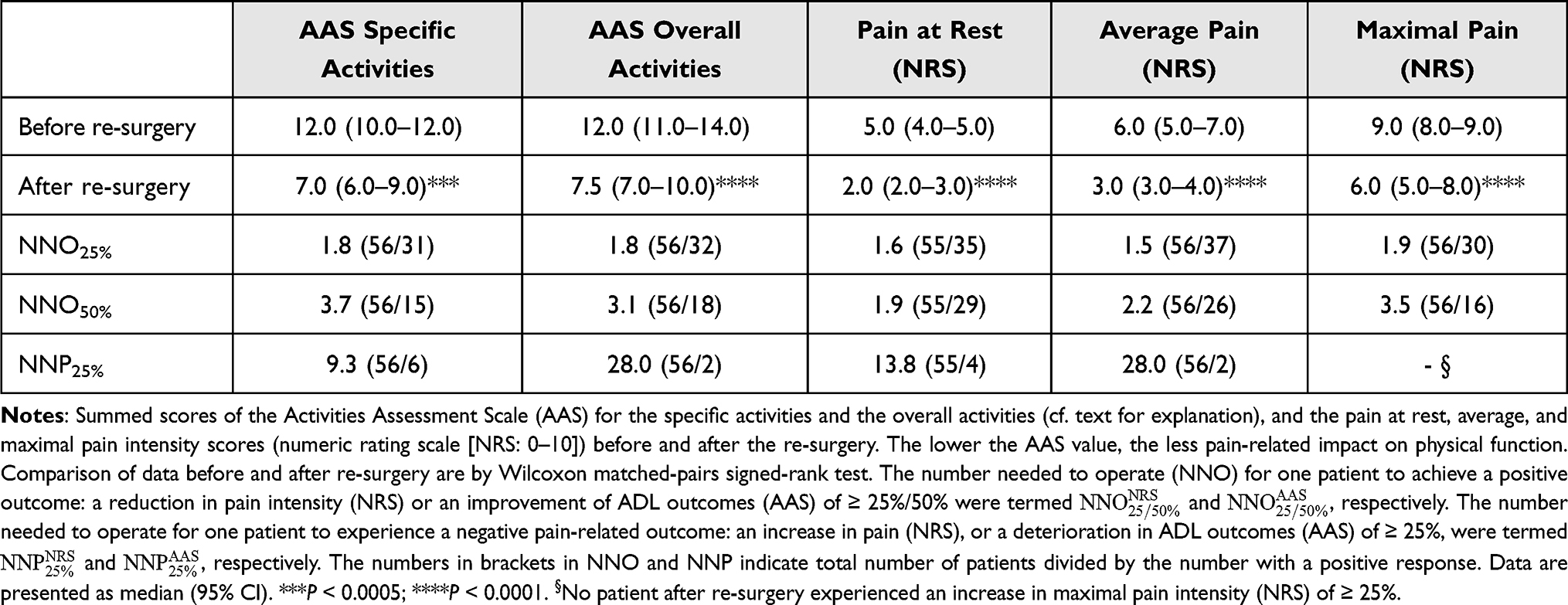 |
Table 4 Summed Scores of the Activities Assessment Scale |
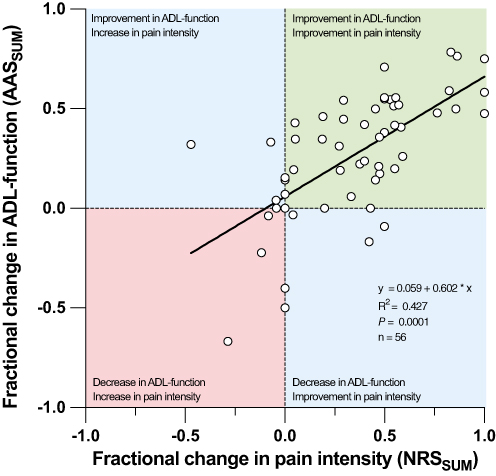 |
Figure 3 Composite Outcome Analysis. Scatter plot depicting the relationship between the fractional changes in physical function scores (summed AAS scores) and pain intensity scores (summed NRS scores; cf. “Analyses of Fractional Changes”” in main text) (n = 56). A fractional change > 0 indicates an improvement in ADL-outcome or a reduction in NRS, whereas a fractional change < 0 indicates a deterioration in ADL-outcome or an increase in NRS. The linear regression model had an R2 of 0.427 (95% CI: 0.24 to 0.61 P = 0.0001) and a slope (α) of 0.602 (95% CI: 0.41 to 0.79; P = 0.0001) indicating an evident relationship. Long-term efficacy has previously been presented and compared to a non-interventional control-group.8 Abbreviations: AAS, Activities Assessment Scale; NRS, Numeric Rating Scale. |
The  for pain intensity scores (NRS) ranged from 1.5 to 1.9, indicating that on average, 10/17 patients experienced a reduction in pain (at rest, average, and maximal pain) of ≥25% after the re-surgery (Table 4).
for pain intensity scores (NRS) ranged from 1.5 to 1.9, indicating that on average, 10/17 patients experienced a reduction in pain (at rest, average, and maximal pain) of ≥25% after the re-surgery (Table 4).
The  % for pain intensity scores (NRS) at rest and on average were 13.8 and 28.0, respectively, indicating that, on average, 1/20 patients experienced an increase in pain intensity (NRS) of ≥25% after the re-surgery.
% for pain intensity scores (NRS) at rest and on average were 13.8 and 28.0, respectively, indicating that, on average, 1/20 patients experienced an increase in pain intensity (NRS) of ≥25% after the re-surgery.
Functional Scores (AAS)
Re-surgery resulted in median decrease in the specific and overall functional AAS scores of 3.5 and 4.0, respectively (Wilcoxon matched-pairs signed-rank test, P = 0.0001 [r = 0.69] and P = 0.0001 [r = 0.59], respectively; Table 4; Supplementary Figure 4). The median fractional change was 0.32 (0.16 to 0.41) for the specific AAS score and 0.29 (0.20 −0.44) for the overall AAS score (Figure 3).
The  equaled 1.8 for the specific activities and 1.6 for the overall activities. This indicates that, on average, 10/17 patients experienced an improvement in ADL-outcomes of ≥25% after the re-surgery (Table 4). The corresponding
equaled 1.8 for the specific activities and 1.6 for the overall activities. This indicates that, on average, 10/17 patients experienced an improvement in ADL-outcomes of ≥25% after the re-surgery (Table 4). The corresponding  for specific and overall activities were 9.3. and 28.0, respectively, indicating that, on average, 1/19 patients experienced a deterioration in ADL-outcomes of ≥25% after the re-surgery.
for specific and overall activities were 9.3. and 28.0, respectively, indicating that, on average, 1/19 patients experienced a deterioration in ADL-outcomes of ≥25% after the re-surgery.
Composite Outcome Analyses
The linear regression model of the fractional changes in functional scores (ADL-outcome) as a function of fractional pain reduction had an R2 of 0.43 (0.24 to 0.61; P = 0.0001), and a slope of 0.60 (0.41 to 0.79; P = 0.0001; Figure 3). This indicates that a 10% pain reduction is on average accompanied by a 6% improvement in ADL-outcome.
Multivariate Multiple Linear Regression Models
Multiple linear regression models were fitted with the independent variables; zDTH, zPPT, zHPT, and zSTHS (all before re-surgery), and the dependent variables as either ΔAAS scores (overall/specific activities) or ΔNRS score (the sum of the at rest, average, and maximal pain intensity scores). No meaningful predictive regression models could be inferred from the data (Supplementary Table 4).
Discussion
Synopsis
The current study examined somatosensory and clinical outcomes after re-surgery in patients (n = 60) suffering from persistent severe pain after groin hernia repair. Regarding the somatosensory outcomes, first, a “loss” of non-nociceptive thermal and mechanical sensory function was observed, demonstrating that re-surgery was associated with an enhanced deafferentation compared to the primary surgery. Second, the “gain” in mechanical deep nociceptive function, generated by the primary surgery, was attenuated by the dual mechanisms of the re-surgery; mitigation of the inflammatory drive by the meshectomy, and deafferentation, by the selective neurectomy. The study results corroborated an improvement in clinical outcomes following the re-surgical procedure by decreasing pain severity and increasing ADL-outcome.8
Neurectomy Issue
Neurectomy in GHR procedures has been discussed as a prophylactical measure preventing the development of PSPG or as a selective procedure in the management of PSPG.26 While prophylactic neurectomy has been debated, it is presently not recommended.5 Other pain-relieving procedure includes triple neurectomy by a laparoscopic extraperitoneal approach27–29 or, as in the current study, selective neurectomy of damaged nerves in the surgical field (cf. “Re-Surgery: Clinical Outcomes”).
Somatosensory Physiology
Somatosensory stimulation in the groin area elicits responses from nerve fiber endings embedded in the skin and deeper tissues. While the responses to superficial thermal and punctate (stimulation area <1 mm2 (maximal pressure 10.500 kPa17)) mechanical stimuli are elicited from receptors situated in the epidermis, and upper dermis, the stimulation by pressure algometry activates proprioceptors and nociceptors in the deeper connective tissue layers. The blunt (1 cm2; max 350 kPa [in the current study])) pressure probe indents, deforms, and stretches the skin, subcutaneous tissue, superficial fascia (the aponeurosis of the external oblique, the external spermatic fascia, the transversalis fascia), the spermatic cord (the internal spermatic fascia, ductus deferens, nerves, and vasculature) compressing the tissues against the pubic bone structure.
Only recently, studies of fascial innervation have pinpointed neural networks residing in the superficial and deep fasciae. The networks are of potential importance in nociception and proprioception and have been examined in detail in rodents30,31 and humans.32 In the skin of the hip region in man, estimates of the mean (SD) nerve fiber densities and nerve fiber diameters are 64.0 (5.2) per cm2 and 26.9 (10.2) microns, respectively.32 Corresponding values for the superficial fascia, the second most densely innervated tissue, are 33.0 (2.5) per cm2 and 19.1 (7.2) microns. The neural networks have not yet been examined in the groin tissues but appear essential for locomotion, nociception, proprioception, and reproduction.
Somatosensory Testing Outcomes
“Loss”
Previous studies have demonstrated that the GHR procedure is associated with a loss in intraepidermal nerve fiber density (IENFD) at the surgical side of 51% (40–75%; n = 67; weighted mean data) compared to the contralateral side.15,33 Unpublished data from one of these studies (n = 21)33 indicate that the reduction in IENFD at the surgical site, estimated by similar z-techniques as in the present study, is accompanied by an increase in the mean of thermal detection thresholds (P = 0.009), HPT (P = 0.034) and blunt PPT (P = 0.0001). An inverse linear correlation with IEFND was demonstrated for thermal detection thresholds (R2 = 0.25, P = 0.0007) and for HPT (R2 = 0.14, P = 0.02), while a weak proportional correlation was found for PPT (R2 = 0.06, P = 0.11). The reduction in IENFD neatly explains the increases in thermal detection thresholds and HPT observed after the primary surgery (Figures 1 and 2). The weak correlation between nerve fiber density and PPT indicates that deafferentation does not seem to represent a major cause of the increase in the nociceptive drive after the primary surgery. The findings thus indicate that the major pain generator likely resides in the deeper peripheral networks (cf. “Somatosensory Physiology”).
Following re-surgery, the additional increases in thermal detection thresholds and HPT observed (Table 2) are likely explained by a further loss of intraepidermal nerve fibers due to the selective neurectomy and the mesh explant per se. The loss of nociceptive nerve fibers after the re-surgery also may contribute to the increased pain thresholds, particularly for the PPT (Figure 2).
“Gain”
Persistent severe pain after GHR is characterized by critical movement-related evoked pain and spontaneous pain, which may lead to debilitating functional impairment. The increased “gain” in the nociceptive system has been hypothesized to be caused by a synergy of peripheral and central mechanisms (Figure 4), mainly deafferentation and inflammation-induced sensitization.18,34
 |
Figure 4 Pathophysiological Mechanisms. A schematic presentation of putative pathophysiological mechanisms in persistent severe pain after groin hernia repair. (A) Depicts the normal conditions of the nociceptive (red) and non-nociceptive system (blue) circuitry from the primary afferents to the dorsal horn neurons with ensuing central projections. The “mirrored” arrows indicate the crosstalk between the circuitries in the peripheral and central nervous systems. Following the primary surgery (B), an inflammatory reaction surrounding the polypropylene mesh implant, may develop into a peripheral “pain generator”, ie, a “meshoma”. The “pain-generator”, including neo-innervation and reinnervation of nerve fibers, induces increased nociceptive-signaling from the fascial layers, eg, a lowered blunt pressure pain threshold (PPT). In contrast, the surgery causes a long-term “deafferentation”: a reduction in intraepidermal nerve fiber density (IENFD), leading to increased cutaneous thermal and mechanical detection and pain thresholds. Following re-surgery (C), the mesh explant leads to removal of the functional “pain generator”: the spontaneous and evoked pain diminishes (increase in PPT). However, the re-surgery also increases the cutaneous deafferentation (reduction of IENFD) leading to an additional increase of cutaneous thermal and mechanical thresholds. |
Although the exact pathophysiological mechanism in PSPG is unknown, ie, nociceptive, neuropathic vs nociplastic origin, noteworthy, all patients, prior to re-surgery, did experience intense deep tissue tenderness residing at the superficial inguinal ring. An interesting histopathological study in explanted inguinal polypropylene meshes has demonstrated re-innervation and neoinnervation of nerve fibers.35 Furthermore, a significantly higher nerve fiber density was observed in specimens obtained due to pain than after re-surgery for a non-pain hernia recurrence. The degree of innervation by the nerve fibers infiltrating the inflammatory tissues inside the mesh showed a significant correlation with the manifestation of clinical pain. In addition, focal inflammatory reactions with foreign body giant cells and lymphocytic infiltrates were observed. Recently, autoimmune or autoinflammatory reactions, including systemic manifestations, have been associated with the implantation of polypropylene meshes.36
The putative “pain generator” may relate to the development of a “meshoma”, neuroma, mesh invasion into an entrapped or dilated spermatic cord, or a combination of these factors (Figure 4). Two controlled, randomized studies have examined the effect of attenuating the pain generator by a tender point block targeted at the superficial inguinal ring in patients with PSGP.37,38 The first study was a double-blind, placebo-controlled, crossover study (n = 14 + 6), using ultrasound-guided blockade of the tender point in the superficial inguinal ring just above the spermatic cord. The median (95% CI) reduction in pain was 63% (44.1% to 73.6%) after local anesthesia compared with 36% (11.6% to 49.7%; P = 0.003) after placebo. The study demonstrated that the peripheral afferent input from the tender point area is important for the maintenance of evoked and spontaneous pain in PSPG. The second study used unspecified tender point blocks (n = 57) in an enrichment design, where patients demonstrating successful blocks were randomized to repeat blocks or had tailored neurectomy performed.37 The repeat block was successful in 6/27 of the patients, while neurectomy was successful in 17/27 of the patients (P < 0.001), demonstrating a better long-term efficacy of the neurectomy procedure than the repeat block procedure.
Reliability
Several normative studies have been carried out, in different anatomical sites, during normal and disease-specific conditions, testing the reliability of various modalities of quantitative somatosensory testing.39–44 Most of the studies have used a simple test-retest design. However, in the current study, these premises were violated by the surgical intervention. Nevertheless, since the re-surgery only affected somatosensory testing conditions in the surgical area, the random error could be estimated by analyzing test-retest data from the two control sites: the contralateral groin and the lower arm. The ICCs generally indicated a good to almost perfect reliability, which is consistent with findings from other anatomical regions45,46 (Table 3). Interestingly, however, a deviation was noted regarding PPT in the contralateral groin, putatively a sign of mirror image sensory dysfunction (MISD)47 from the deeper tissues.
Re-Surgery: Clinical Outcomes
Pain Outcomes
Previous studies of pain intensities after mesh removal and/or neurectomy have used different methodologies with regard to the type of primary surgery, duration and method of follow-up, and type of re-surgical approach.48 Most of these studies used unspecific pain and patient satisfaction questionnaires, making outcome comparisons difficult. The overall success rate has ranged from 33–100% in retrospective studies8,49–52 and 63–100% in corresponding prospective cohort studies.53–58 In the current study, the initial GHR and the re-surgery were performed by an open surgical approach. In comparable studies,10,12,59 significant improvements in pain intensities (NRS) on average,10,12,59 at rest, activity-related and maximal,10,12 have been observed, with follow-up intervals ranging from 6 to 36 months.
Functional Outcomes
Four studies of mesh removal and/or neurectomy in patients with PSPG have included an assessment of ADL-outcomes. Three of these included a modified AAS questionnaire and showed significant group-level improvement in ADL-outcomes after three months,54 six months,12 and five-year follow-up (median follow-up time 2.2 (1.9 to 2.8) months).8 One of these studies compared outcomes of patients allocated to either re-surgery or pharmacotherapy.8 Interestingly, the study showed that the re-surgery group had enhanced improvement in ADL-outcomes compared to the pharmacotherapy group.
Limitations
The lack of a control group is a limitation in the study design since the spontaneous regression trajectory is unknown. However, the authors have previously presented data from a large control cohort (n = 118) compared to a re-surgery cohort (n = 54).8 Furthermore, the short follow-up time (median 4.0 months) is a study limitation, although previous studies have shown similar improvements in pain intensities and ADL-outcomes in two and three years assessments after the re-surgery.8,10
Strengths
The patients were included on a nationwide basis, and all had persistent severe pain after unilateral, uncomplicated, open groin hernia, resulting in a homogeneous patient cohort. In order to reduce data variability, a single surgeon (HK) performed the re-surgeries, and a limited number of investigators collected data. Finally, only standardized and validated methods and questionnaires were used in assessing the somatosensory function and pain outcomes.
Conclusions
The pathophysiologic data indicate that the beneficial effects of re-surgery on pain and functional outcomes in persistent pain after groin hernia repair are attributed to “meshectomy” and selective “neurectomy”, leading to the removal of the peripheral pain generator and a loss of nerve fiber function, respectively. See Table 5 for a qualitative conclusion of the study findings.
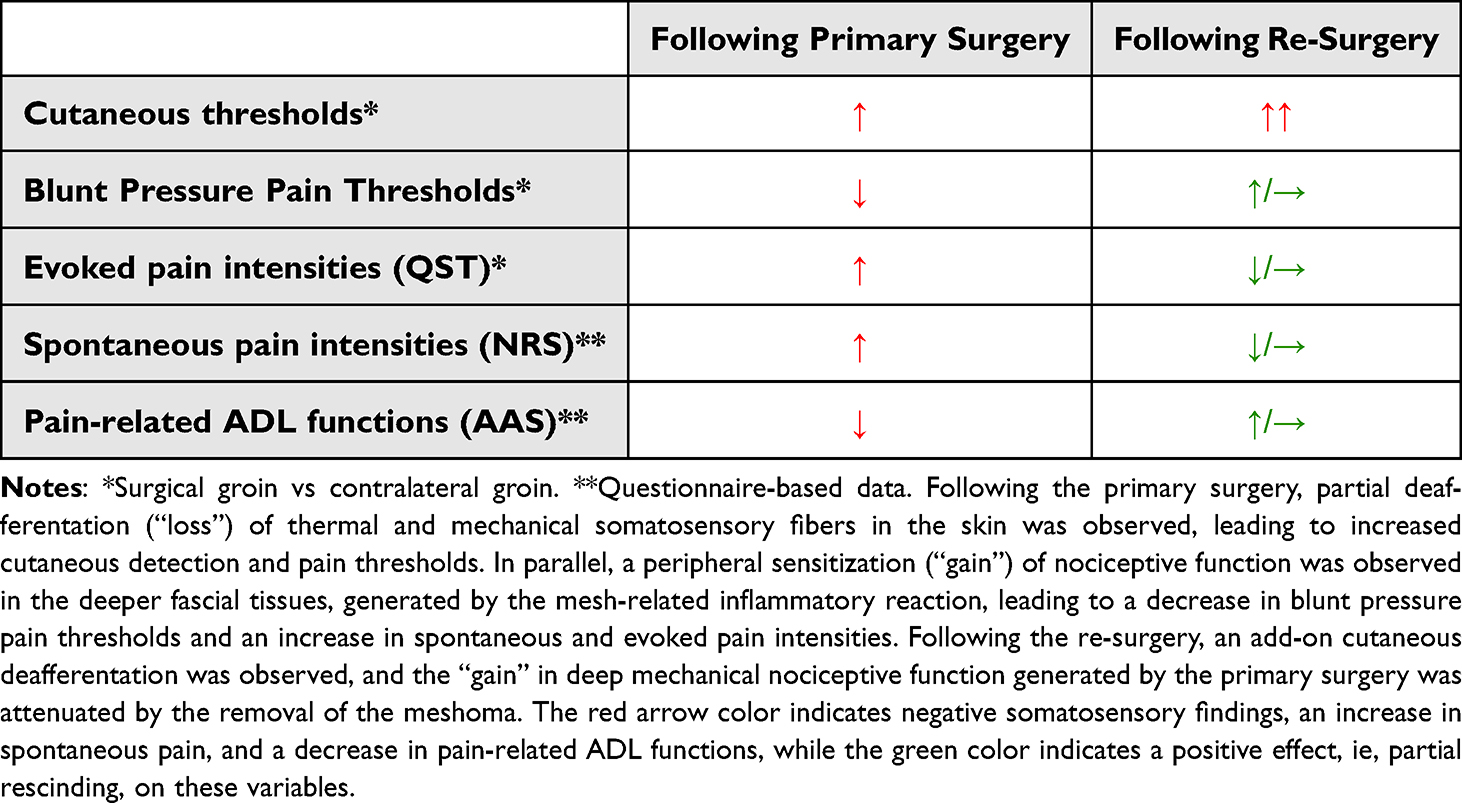 |
Table 5 Overview of Findings |
Abbreviations
AAS, Activities Assessment Scale; ADL, Activities of Daily Living; aRS, After Re-surgery; bRS, Before Re-surgery; CDT, Cool Detection Threshold; CL-, Contralateral (pre-fix, ie, CL-groin); GHR, Groin Hernia Repair; HPT, Heat Pain Threshold; ICC, Intra-class Correlation Coefficient; IENFD, Intraepidermal Nerve Fiber Density; MDT, Mechanical Detection Threshold; MISD, Mirror Image Sensory Dysfunction; NNO, Number Needed to Operate (to achieve an improved outcome); NNP, Number Needed to inflict a Pain-related outcome; NRS, Numeric Rating Scale; P-, Pain (pre-fix, ie, P-groin); PPT, Pressure Pain Threshold; PSPG, Persistent Severe Pain after Groin hernia repair; QST, Quantitative Somatosensory Testing; RS, Re-Surgery; STHS, Suprathreshold Heat Stimulus; TSP, Temporal Summation Phenomena; WDT, Warmth Detection Threshold; zCDT, z-scores of Cool Detection Threshold; zDTH, Mean of z-scores of the Detection Thresholds (CDT, WDT, MDT); zHPT, z-scores of Heat Pain Threshold; zMDT, z-scores of Mechanical Detection Threshold; zPPT, z-scores of Pressure Pain Threshold; zSTHS, z-scores of Suprathreshold Heat Stimulus; zWDT, z-scores of Warmth Detection Threshold.
Data Sharing Statement
Full dataset available in Supplementary Table 5.
Ethical Approval
The study was approved by the Regional Committee on Health Research Ethics: (H-2-2011-023 and KF 11 320499) and The Danish Data Protection Agency (2012-41-0008). The study was registered on ClinicalTrials.gov (NCT05238571) and complied with the Declaration of Helsinki most recently amended 2013.
Consent for Publication
Authors state full consent to publish. The final manuscript including figures, tables and Supplementary Information has been seen and approved by all authors.
Acknowledgments
The authors wish to extend special thanks to all participating patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Authors state that only departmental funding was involved. Salary expenses for PhD-student EKJ were covered by a two-year institutional grant from “Rigshospitalets Forskningsfond” (E-22491-04).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bande D, Molto L, Pereira JA, Montes A. Chronic pain after groin hernia repair: pain characteristics and impact on quality of life. BMC Surg. 2020;20(1):147. doi:10.1186/s12893-020-00805-9
2. Chapman CR, Vierck CJ. The transition of acute postoperative pain to chronic pain: an integrative overview of research on mechanisms. J Pain. 2016;18(4):359.e351–359.e338.
3. Campanelli G, Bruni PG, Morlacchi A, Cavalli M. Chronic pain after inguinal hernia repair. In: Campanelli G, editor. Inguinal Hernia Surgery. Milano: Springer Milan; 2017:157–168.
4. Nikkolo C, Kirsimagi U, Vaasna T, et al. Prospective study evaluating the impact of severity of chronic pain on quality of life after inguinal hernioplasty. Hernia. 2017;21(2):199–205. doi:10.1007/s10029-016-1569-4
5. HerniaSurge G. International guidelines for groin hernia management. Hernia. 2018;22(1):1–165.
6. Jorgensen SG, Oberg S, Rosenberg J. Treatment of longstanding groin pain: a systematic review. Hernia. 2019;23(6):1035–1044. doi:10.1007/s10029-019-01919-7
7. Andresen K, Rosenberg J. Management of chronic pain after hernia repair. J Pain Res. 2018;11:675–681. doi:10.2147/JPR.S127820
8. Jensen EK, Ringsted TK, Bischoff JM, et al. A national center for persistent severe pain after groin hernia repair: five-year prospective data. Medicine. 2019;98(33):e16600. doi:10.1097/MD.0000000000016600
9. Werner MU. Management of persistent postsurgical inguinal pain. Langenbecks Arch Surg. 2014;399(5):559–569. doi:10.1007/s00423-014-1211-9
10. Bischoff JM, Enghuus C, Werner MU, Kehlet H. Long-term follow-up after mesh removal and selective neurectomy for persistent inguinal postherniorrhaphy pain. Hernia. 2013;17(3):339–345. doi:10.1007/s10029-013-1073-z
11. Aasvang E, Kehlet H. Surgical management of chronic pain after inguinal hernia repair. Br J Surg. 2005;92(7):795–801. doi:10.1002/bjs.5103
12. Aasvang EK, Kehlet H. The effect of mesh removal and selective neurectomy on persistent postherniotomy pain. Ann Surg. 2009;249(2):327–334. doi:10.1097/SLA.0b013e31818eec49
13. Linderoth G, Kehlet H, Aasvang EK, Werner MU. Neurophysiological characterization of persistent pain after laparoscopic inguinal hernia repair. Hernia. 2011;15(5):521–529. doi:10.1007/s10029-011-0815-z
14. Aasvang EK, Gmaehle E, Hansen JB, et al. Predictive risk factors for persistent postherniotomy pain. Anesthesiology. 2010;112(4):957–969. doi:10.1097/ALN.0b013e3181d31ff8
15. Bischoff JM, Ringsted TK, Petersen M, Sommer C, Uceyler N, Werner MU. A capsaicin (8%) patch in the treatment of severe persistent inguinal postherniorrhaphy pain: a randomized, double-blind, placebo-controlled trial. PLoS One. 2014;9(10):e109144. doi:10.1371/journal.pone.0109144
16. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991;15(1):47–50. doi:10.1016/S0149-7634(05)80090-9
17. Ringsted TK, Enghuus C, Petersen MA, Werner MU. Demarcation of secondary hyperalgesia zones: punctate stimulation pressure matters. J Neurosci Methods. 2015;256:74–81. doi:10.1016/j.jneumeth.2015.08.018
18. Finnerup NB, Kuner R, Jensen TS. Neuropathic pain: from mechanisms to treatment. Physiol Rev. 2021;101(1):259–301. doi:10.1152/physrev.00045.2019
19. Wasserstein RLLN. The ASA statement on p-values: context, process, and purpose. Am Stat. 2016;70(2):129–133. doi:10.1080/00031305.2016.1154108
20. Amrhein V, Greenland S, McShane B. Scientists rise up against statistical significance. Nature. 2019;567(7748):305–307. doi:10.1038/d41586-019-00857-9
21. Wasserstein RLSA, Lazar NA. Moving to a world beyond “p < 0.05”. Am Stat. 2019;73(sup1):1–19.
22. Greenland S, Senn SJ, Rothman KJ, et al. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. 2016;31(4):337–350. doi:10.1007/s10654-016-0149-3
23. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
24. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
25. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. 2012;141(1):2–18. doi:10.1037/a0024338
26. Cirocchi R, Sutera M, Fedeli P, et al. Ilioinguinal nerve neurectomy is better than preservation in Lichtenstein hernia repair: a systematic literature review and meta-analysis. World J Surg. 2021;45(6):1750–1760. doi:10.1007/s00268-021-05968-x
27. Bjurstrom MF, Nicol AL, Amid PK, Lee CH, Ferrante FM, Chen DC. Neurophysiological and clinical effects of laparoscopic retroperitoneal triple neurectomy in patients with refractory postherniorrhaphy neuropathic inguinodynia. Pain Pract. 2017;17(4):447–459. doi:10.1111/papr.12468
28. Bjurstrom MF, Alvarez R, Nicol AL, Olmstead R, Amid PK, Chen DC. Quantitative validation of sensory mapping in persistent postherniorrhaphy inguinal pain patients undergoing triple neurectomy. Hernia. 2017;21(2):207–214. doi:10.1007/s10029-017-1580-4
29. Moore AM, Bjurstrom MF, Hiatt JR, Amid PK, Chen DC. Efficacy of retroperitoneal triple neurectomy for refractory neuropathic inguinodynia. Am J Surg. 2016;212(6):1126–1132. doi:10.1016/j.amjsurg.2016.09.012
30. Mense S, Hoheisel U. Evidence for the existence of nociceptors in rat thoracolumbar fascia. J Bodyw Mov Ther. 2016;20(3):623–628. doi:10.1016/j.jbmt.2016.01.006
31. Fede C, Petrelli L, Guidolin D, et al. Evidence of a new hidden neural network into deep fasciae. Sci Rep. 2021;11(1):12623. doi:10.1038/s41598-021-92194-z
32. Fede C, Porzionato A, Petrelli L, et al. Fascia and soft tissues innervation in the human hip and their possible role in post-surgical pain. J Orthop Res. 2020;38(7):1646–1654. doi:10.1002/jor.24665
33. Bischoff JM, Petersen M, Uceyler N, Sommer C, Kehlet H, Werner MU. Lidocaine patch (5%) in treatment of persistent inguinal postherniorrhaphy pain: a randomized, double-blind, placebo-controlled, crossover trial. Anesthesiology. 2013;119(6):1444–1452. doi:10.1097/ALN.0b013e3182a2a243
34. Woolf CJ. Pain amplification—a perspective on the how, why, when, and where of central sensitization. J Appl Behav Res. 2018;2(23(e12124)):1–9.
35. Bendavid R, Lou W, Grischkan D, et al. A mechanism of mesh-related post-herniorrhaphy neuralgia. Hernia. 2016;20(3):357–365. doi:10.1007/s10029-015-1436-8
36. Cohen Tervaert JW. Autoinflammatory/autoimmunity syndrome induced by adjuvants (Shoenfeld’s syndrome) in patients after a polypropylene mesh implantation. Best Pract Res Clin Rheumatol. 2018;32(4):511–520. doi:10.1016/j.berh.2019.01.003
37. Verhagen T, Loos MJA, Scheltinga MRM, Roumen RMH. The GroinPain trial: a randomized controlled trial of injection therapy versus neurectomy for postherniorraphy inguinal neuralgia. Ann Surg. 2018;267(5):841–845. doi:10.1097/SLA.0000000000002274
38. Wijayasinghe N, Ringsted TK, Bischoff JM, Kehlet H, Werner MU. The role of peripheral afferents in persistent inguinal postherniorrhaphy pain: a randomized, double-blind, placebo-controlled, crossover trial of ultrasound-guided tender point blockade. Br J Anaesth. 2016;116(6):829–837. doi:10.1093/bja/aew071
39. Maier C, Baron R, Tolle TR, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain. 2010;150(3):439–450. doi:10.1016/j.pain.2010.05.002
40. Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): standardized protocol and reference values. Pain. 2006;123(3):231–243. doi:10.1016/j.pain.2006.01.041
41. Neziri AY, Scaramozzino P, Andersen OK, Dickenson AH, Arendt-Nielsen L, Curatolo M. Reference values of mechanical and thermal pain tests in a pain-free population. Eur J Pain. 2011;15(4):376–383. doi:10.1016/j.ejpain.2010.08.011
42. Biurrun Manresa JA, Neziri AY, Curatolo M, Arendt-Nielsen L, Andersen OK. Test-retest reliability of the nociceptive withdrawal reflex and electrical pain thresholds after single and repeated stimulation in patients with chronic low back pain. Eur J Appl Physiol. 2011;111(1):83–92. doi:10.1007/s00421-010-1634-0
43. Blankenburg M, Junker J, Hirschfeld G, et al. Quantitative sensory testing profiles in children, adolescents and young adults (6–20 years) with cerebral palsy: hints for a neuropathic genesis of pain syndromes. Eur J Paediatr Neurol. 2018;22(3):470–481. doi:10.1016/j.ejpn.2017.12.015
44. Blankenburg M, Boekens H, Hechler T, et al. Reference values for quantitative sensory testing in children and adolescents: developmental and gender differences of somatosensory perception. Pain. 2010;149(1):76–88. doi:10.1016/j.pain.2010.01.011
45. Marcuzzi A, Wrigley PJ, Dean CM, Adams R, Hush JM. The long-term reliability of static and dynamic quantitative sensory testing in healthy individuals. Pain. 2017;158(7):1217–1223. doi:10.1097/j.pain.0000000000000901
46. Wildgaard K, Ringsted TK, Kehlet H, Werner MU. Quantitative sensory testing in patients with postthoracotomy pain syndrome: part 2: variability in thermal threshold assessments. Clin J Pain. 2013;29(9):784–790. doi:10.1097/AJP.0b013e318277b6ea
47. Werner MU, Ringsted TK, Kehlet H, Wildgaard K. Sensory testing in patients with postthoracotomy pain syndrome: part 1: mirror-image sensory dysfunction. Clin J Pain. 2013;29(9):775–783. doi:10.1097/AJP.0b013e318277b646
48. Beel E, Berrevoet F. Surgical treatment for chronic pain after inguinal hernia repair: a systematic literature review. Langenbecks Arch Surg. 2022;407(2):541–548. doi:10.1007/s00423-021-02311-9
49. Delikoukos S, Fafoulakis F, Christodoulidis G, Theodoropoulos T, Hatzitheofilou C. Re-operation due to severe late-onset persisting groin pain following anterior inguinal hernia repair with mesh. Hernia. 2008;12(6):593–595. doi:10.1007/s10029-008-0392-y
50. Koopmann MC, Yamane BH, Starling JR. Long-term follow-up after meshectomy with acellular human dermis repair for postherniorrhaphy inguinodynia. Arch Surg. 2011;146(4):427–431. doi:10.1001/archsurg.2011.49
51. Loos MJ, Scheltinga MR, Roumen RM. Tailored neurectomy for treatment of postherniorrhaphy inguinal neuralgia. Surgery. 2010;147(2):275–281. doi:10.1016/j.surg.2009.08.008
52. Valvekens E, Nijs Y, Miserez M. Long-term outcome of surgical treatment of chronic postoperative groin pain: a word of caution. Hernia. 2015;19(4):587–594. doi:10.1007/s10029-013-1125-4
53. Campanelli G, Bertocchi V, Cavalli M, et al. Surgical treatment of chronic pain after inguinal hernia repair. Hernia. 2013;17(3):347–353. doi:10.1007/s10029-013-1059-x
54. Pedersen KF, Chen DC, Kehlet H, Stadeager MW, Bisgaard T. A simplified clinical algorithm for standardized surgical treatment of chronic pain after inguinal hernia repair: a quality assessment study. Scand J Surg. 2020;110(3):359–367.
55. Fafaj A, Tastaldi L, Alkhatib H, et al. Surgical treatment for chronic postoperative inguinal pain-short term outcomes of a specialized center. Am J Surg. 2020;219(3):425–428. doi:10.1016/j.amjsurg.2019.10.020
56. Keller JE, Stefanidis D, Dolce CJ, Iannitti DA, Kercher KW, Heniford BT. Combined open and laparoscopic approach to chronic pain after inguinal hernia repair. Am Surg. 2008;74(8):695. doi:10.1177/000313480807400805
57. Rosen MJ, Novitsky YW, Cobb WS, Kercher KW, Heniford BT. Combined open and laparoscopic approach to chronic pain following open inguinal hernia repair. Hernia. 2006;10(1):20–24. doi:10.1007/s10029-005-0032-8
58. Vuilleumier H, Hubner M, Demartines N. Neuropathy after herniorrhaphy: indication for surgical treatment and outcome. World J Surg. 2009;33(4):841–845. doi:10.1007/s00268-008-9869-1
59. Zwaans WA, Perquin CW, Loos MJ, Roumen RM, Scheltinga MR. Mesh removal and selective neurectomy for persistent groin pain following Lichtenstein repair. World J Surg. 2017;41(3):701–712. doi:10.1007/s00268-016-3780-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.