Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Solo Mothers After Assisted Conception and Their Experiences with Postnatal Care
Authors Jacobsen KS, Vik ES ![]() , Dahl B
, Dahl B ![]()
Received 4 September 2019
Accepted for publication 23 December 2019
Published 16 January 2020 Volume 2020:13 Pages 53—61
DOI https://doi.org/10.2147/JMDH.S229807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kristine Selvik Jacobsen, 1 Eline Skirnisdottir Vik, 2 Bente Dahl 1
1Centre for Women’s, Family and Child Health, Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg N-3603, Norway; 2Faculty of Health and Social Sciences, Western Norway University of Applied Sciences, Bergen, Norway
Correspondence: Bente Dahl
Faculty of Health and Social Sciences, University of South-Eastern Norway, P.O. Box 235, Kongsberg N-3603, Norway
Tel +47 906 26 991
Email [email protected]
Purpose: To explore solo mothers’ postnatal caring experiences.
Patients and Methods: A qualitative interview study including nine solo mothers living in six different counties in Norway. The mothers had a total of twelve children conceived through assisted fertilization and donor sperm. Systematic text condensation was used to analyze the data.
Results: The first theme described how the decision to be a solo mother entailed responsibility and rendered solo mothers vulnerable. Secondly, it was valuable, but sometimes surprising, to be met with care and interest, but, and finally, bending standard rules and regulation of the postnatal ward proved necessary to fit the needs of solo mothers.
Conclusion: Solo mothers see themselves as different from other mothers, and the results of this study underline that solo mothers’ individual needs are not always met in postnatal care.
Keywords: assisted fertilization, donor sperm, postnatal, single mothers by choice, systematic text condensation, solo mothers
Introduction
The term “solo mothers” refers to single women who have become mothers by donor insemination. In a number of countries, such as France, Ireland, Norway and Japan, women have to be married or cohabiting to receive assisted reproductive technology treatment.1 Although assisted reproductive technology treatment is prohibited for single women in Norway, these women are entitled to full medical help and treatment during pregnancy, birth and postpartum.2
In recent decades, an increase of single women who choose to parent alone and have children through donor insemination has been demonstrated.3 There are no official registers of solo mothers who have children through this practice in Norway,4 but an increase in single women aiming to become pregnant has been reported.5 Single women opting for motherhood often travel abroad to evade restrictive legislation in their home country, resulting in maternal care being shared between two different countries and medical systems.6,7 This practice is often referred to as “cross border reproductive care”, and it is an increasing challenge to healthcare services across Europe.7
In a report from 2014 to 2015, the Norwegian Biotechnology Advisory Board evaluated Norwegian legislation on the right of single women to assisted fertilization5 and underlined the lack of knowledge about solo mothers and their ability to provide a secure and positive upbringing for a child. However, international studies demonstrate that solo mothers are well prepared before becoming mothers and that they generally have sound finances, are well educated and have a strong social network.8–10 Their children have been described as having fewer emotional and behavioral difficulties than children of married mothers.11 However, the process of becoming a solo mother has been described as both painful and lonely.12 One study13 describes these women’s struggle for legitimacy, and according to a Swedish pilot study,14 being a solo mother is associated with a high degree of vulnerability to social hostility. The author notes that more knowledge about this group’s vulnerabilities and strengths is required, and argues that the lack of research in the field plays a crucial part in concealing the needs of these women and their children. According to social norms in some societies, single women are not considered suited to be mothers; thus, they risk feeling stigmatized and sometimes feel that they have to defend their choice.15 Solo mothers may have a high threshold for asking for help, and a previous study demonstrated that maternity care does not necessarily improve their situation.16 Consequently, solo mothers can be identified as a vulnerable group in the encounter with maternity care worldwide. The postnatal period is an important part of maternity care.17 Postnatal care is under constant criticism18 and is the least satisfactory aspect of maternity care for women in Norway.19 We, therefore, set up a study to explore solo mothers’ postnatal caring experiences, drawing on theory on woman-centered care to elucidate the findings.
Woman-centered care is an internationally recognized concept, fundamental to midwifery and used as a framework for a range of international policy documents.17 The concept recognizes the woman’s own expertise in decision-making by addressing her different physical and emotional needs, and underscores the woman’s need for choice, continuity and control from her caregiver(s).17 Moreover, the concept includes the woman’s family and others that the woman herself defines as important to her.
Materials and Methods
We conducted a qualitative study, using a descriptive and exploratory approach, as this is an appropriate design when previous research about the topic is scarce and the aim is to enhance understanding of personal experiences.20
Recruitment
Participants were recruited through social media. We contacted an administrator of a closed Facebook group for solo mothers and asked her to publish information about the study along with an invitation to participate. We included women who had conceived through assisted fertilization and the use of donor sperm in fertility clinics approved by the authorities in the respective counties. The women had to be of fertile age with healthy term births. Non-Norwegian-speaking women were excluded as cultural and language barriers might entail misinterpretations. As time of interview is recognized as an important factor in childbirth research, interviews took place at least six months after the birth.21
Participants
Initially, twelve women contacted us by e-mail. Two women were pregnant and therefore excluded in line with the inclusion criteria. One woman withdrew after having received further information about the study. Finally, nine women were interviewed, and we aimed for rich descriptive data to deepen our understanding of solo mothers’ postnatal caring experiences.22 Some of the women had conceived more than one child with donor sperm, and thus had different experiences to draw from.
The nine women included in the study lived in different parts of Norway, including both urban and rural areas. They had a total of twelve children conceived through assisted fertilization and use of donor sperm, born between 2004 and 2015. The women were between 28 and 40 years of age at first birth (mean 36 years). Seven children were conceived through in vitro fertilization treatment (IVF). Some women conceived at their first attempt, while others needed up to eleven attempts. The solo mothers in this study were generally well educated and had a steady income. Most of them said that their decision to become a solo mother was made because time was running out for them to have children.
Data Collection and Analysis
We carried out semi-structured interviews with nine solo mothers who had experience of postnatal care in Norway. The interviews lasted from 35 to 67 mins (mean 49 mins) and were conducted between May 2015 and February 2016. They started with an open question aimed at encouraging free association and descriptions of their experiences.23
To analyze the data, systematic text condensation (STC) was used. STC is a strategy for thematic cross-case analysis, inspired by Giorgi’s phenomenological analysis and modified by Malterud.24 The method is suited for developing new descriptions and concepts. The analysis was conducted by the first author and discussed and agreed upon by all authors. The procedure consisted of four steps. First, we read the interviews with an open mind in order to gain an overall impression, noting the following preliminary themes: being responsible, managing alone, not wanting to bother others, appreciating attention from healthcare providers without having to ask for it, fearing negative reactions from healthcare providers, the value of positive feedback, being an outsider, rules and regulations in the postnatal ward, being able to have someone with you, and visiting hours at the hospital. In the second step, we read the interview texts line by line, and meaning units, ie, parts of the text representing the participants’ experiences were identified, coded and organized in code groups. We then summarized and condensed the content of each code group in the third step and sorted the different meaning units in each group into subgroups (Table 1). Working with one subgroup at a time, we reduced the meaning units into condensates, ie, artificial quotations using the participants’ words. During this process, we identified quotations to illustrate the subgroups. In the last step, we synthesized the content of the condensates within each code group, extrapolating their significance and meaning and on this basis developed an analytical text.
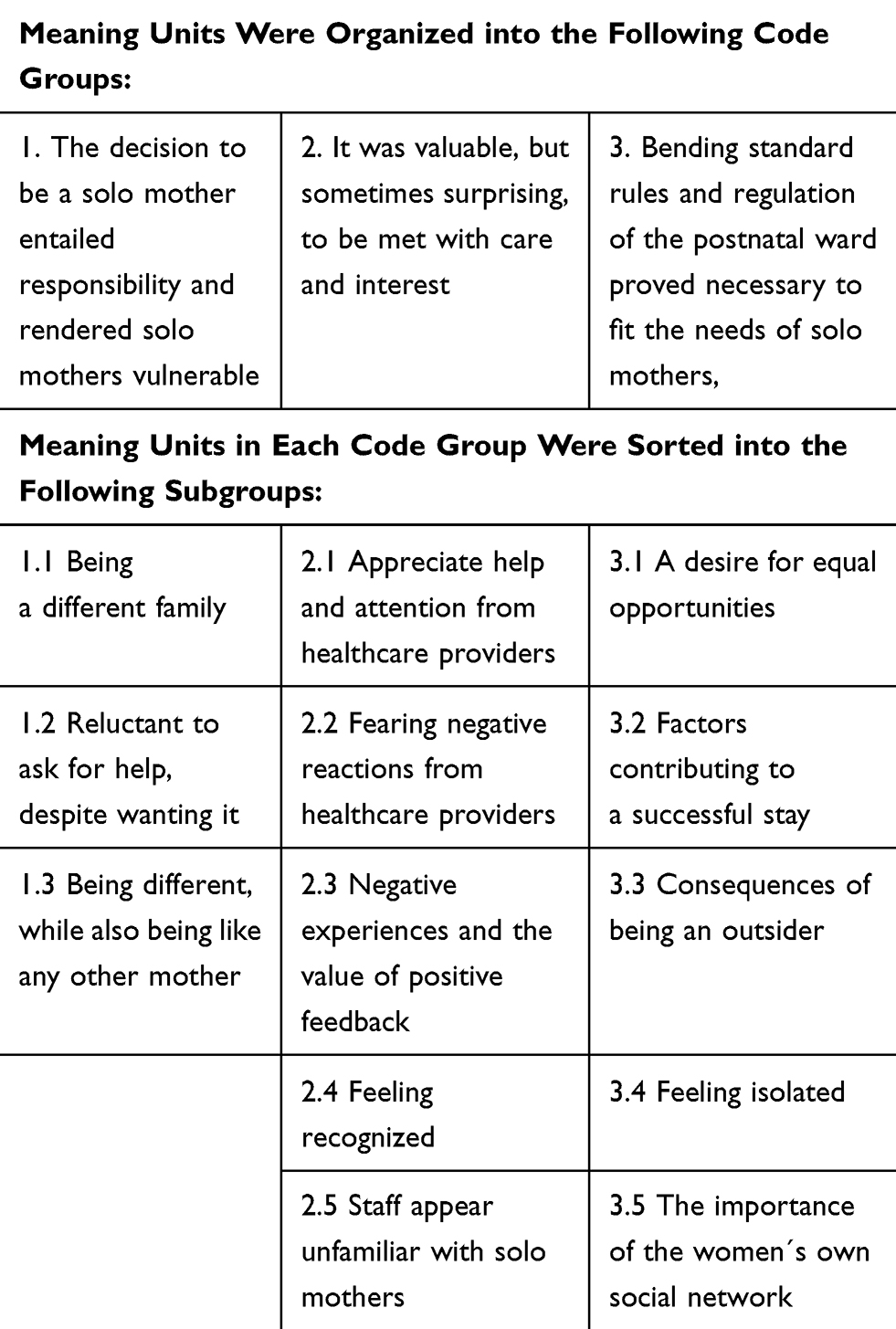 |
Table 1 Code Groups and Subgroups from the Analytic Process |
Ethics
The study was conducted in accordance with the World Medical Association Declaration of Helsinki Principles for Medical Research involving Human Subjects.25 It was approved by the Norwegian Centre for Research Data (42901) and assessed by the Regional Committee for Medical and Health Research Ethics, but considered to be outside the scope of Sections 2 and 4 of the Health Research Act (2015/399). The participants received written and oral information about the study and signed a declaration of consent before the interviews started. They were informed that participation was voluntary and that they could withdraw from the study at any time without giving reasons. Any data they had contributed would then be deleted.
Results
We identified three main themes during the analysis. The first theme described how the decision to be a solo mother entailed responsibility and rendered solo mothers vulnerable. The second theme demonstrated that it was valuable, but sometimes surprising, to be met with care and interest, and the third theme described how bending standard rules and regulation of the postnatal ward proved necessary to fit the needs of solo mothers.
The Decision to Be a Solo Mother Entailed Responsibility and Rendered Solo Mothers Vulnerable
A family constellation consisting of mother and child differs from the traditional family constellation, and the women demonstrated in a number of ways that they were a “different” family. It was important for the women to appear as proper mothers, able to take care of their children and fit for the new task they had assumed. They argued that the decision to start a family was theirs alone, and they were determined to cope with the situation. They described that they were independent and responsible, and considered themselves accountable. They had high demands for themselves, and some even expressed the idea that they ought to handle motherhood particularly well since the decision to start a family was a deliberate choice.
You feel it’s difficult to say “This is too hard for me” or “I don’t know what to do”. It follows you all the way – it gets difficult to ask for help because the decision to have a child was your own. (Interview # 2)
One participant stated that she had decided before becoming a mother that she would never allow herself to complain about life as a single mother as she was aware that not everybody understood or approved of her decision. In spite of friends and network offering help and support, most solo mothers were hesitant to ask for help even when feeling exhausted. During their stay in the postnatal ward, the women had similar feelings:
I was a bit reluctant to push the call button to ask for help … Particularly after the first 24 hrs when I felt that I ought to be more on top of the situation. (Interview # 6)
The participants said that they were prepared to defend their choice to start a family, and several women had felt the need to do this in the encounter with maternity care. At the same time, all the women were open about being a solo mother in hope of receiving the best possible care. Women who were acknowledged for their choice felt relieved, and they appreciated healthcare providers taking an interest in their particular situation. They stated that they basically had no desire to receive special treatment just for being solo mothers. However, they also said that in some situations they felt vulnerable being solo mothers and that healthcare providers should be aware of this. One woman described the situation as follows:
I wanted to be seen as any other mother. I wanted them to notice if something was missing or if I was in need of extra help … just to avoid going home feeling worn out and unable to produce any milk. The fact that we’re all alone makes us single women a bit more vulnerable. (Interview # 8)
It Was Valuable, but Sometimes Surprising, to Be Met with Care and Interest
The women reported wanting to be cared for by healthcare providers. They appreciated staff taking an interest and offering their assistance during their stay on the postnatal ward. It was important for them that midwives or nurses acknowledged the fact that most new mothers feel vulnerable, tired and uncertain. Similarly, it felt good when staff entered their room unsolicited:
They came into my room very often, asking me how I felt. I really appreciated that, I didn’t have to use the call button. (Interview # 1)
Most women stated that they did not want to cause any inconvenience, and therefore adapted to the regulations and procedures in the postnatal ward. If they had to ask for help, they paid close attention to how their request was received by staff. Some feared being refused when asking for assistance, and one woman was afraid that her request for help would make the staff think that she had had enough of being a mother after only two days. She decided to ask for help anyway, only to find that her fear was justified. She felt uncertain as to whether the refusal was caused by her status as a solo mother:
I asked the midwives for help although it was really hard for me to do so. When I got a refusal, I didn’t feel like asking again. (…). I didn’t want to seem to be whining, and I thought I’d handle this on my own. Still, the days I spent in the postnatal ward are not something I’d like to experience again. (Interview # 5)
The women described various experiences of being cared for during their stay in the postnatal ward. However, sometimes they felt uncertain about the personal opinions of the staff. Some found that staff made negative comments about their choice to become solo mothers or they suspected that negative interaction may have been due to their decision. In such situations, midwives and nurses appeared disinterested or unengaged. Sometimes, they were even reluctant to offer necessary assistance and care. As a result, these women withdrew from the encounters, feeling uncertain and uncared for. Most solo mothers describing negative experiences with staff had given birth in large hospitals, while those who had given birth in smaller hospitals found that staff took an interest in their situation and demonstrated understanding and kindness. Being met with kindness sometimes felt surprising, but it was appreciated by the women and described by one of them as follows:
Luckily, they were professional and supportive when they understood my situation. But I hadn’t anticipated the warmth, support and care that I met during pregnancy and after birth. It felt so good. (Interview # 9)
Some of the mothers felt that the feedback they got from staff was particularly valuable given their single status, resulting in feelings of being recognized. They described having to process all information on their own, since they lacked a partner. It therefore felt good when staff asked questions about their situation, allowing them to share their story. None of the participants had experienced these questions as wrong or inappropriate. According to one mother:
I remember there was one person who came in and asked me if I’d decided to have a baby on my own. She thought it was so cool. Being given such feedback feels really good. (…). The midwife said that all parents feel inadequate from time to time. At least that reassures you that they’re not thinking “Oh my, what have you been up to now”. (Interview # 2)
The women had found that midwives and nurses sometimes seemed to mind their language in the conversations, appearing uncertain. They suspected that this was because the staff was afraid of using the wrong words, making mistakes or hurting their feelings. In other situations, the women felt uncertain if the feedback they received from staff was well intended or whether it contained some kind of negative message. However, sometimes they simply chose to interpret the staff’s words positively, eg, when one mother was encouraged to contact the child welfare authorities for help and support. In this situation, the woman decided to interpret the statement as a clumsy way to inform her about possible ways of getting help:
I couldn’t be bothered … I choose to think that it was well intended. Badly worded, but well intended. (Interview # 4)
Bending Standard Rules and Regulation of the Postnatal Ward Proved Necessary to Fit the Needs of Solo Mothers
The women commented that the first days after birth were challenging, and in most hospitals, the stay was not adapted to the solo mothers’ situations. All hospitals had single and standard shared rooms in the postnatal ward, but in some hospitals, solo mothers were excluded from the possibility of having a single room because they did not fulfill the hospital criteria:
On the postnatal ward, I found it annoying that couples were offered a single room with a double bed and so on, but since I was alone I had no possibility to have a single room. (Interview # 2)
Single rooms allow women to have their partner with them during the stay in the postnatal ward. In the case mentioned, the solo mother was excluded from the opportunity to have a single room and therefore to have someone with her. Regulations for single rooms varied between hospitals, and other women in this study were grateful for the opportunity to have a single room as it contributed to a successful stay in the postnatal ward. Another factor contributing to a successful stay was the duration of the stay:
My mother and I had a single room, and I was told that I could keep it as long as I wanted. I wasn’t discharged until I felt sure that I was ready to go home. They made me feel welcome on the postnatal ward, so my story’s a “golden” story. (Interview # 1)
Women who stayed in a single room were allowed to bring relatives and arrange the visiting hours themselves. However, for most solo mothers visiting hours were described as problematic, particularly for women staying in the postnatal wards of large hospitals. In these wards, only one visitor was allowed to stay for a long period, and in some hospitals, this person had to be your partner, resulting in grandparents or friends not being allowed to visit mother and baby. Because of the strict rules, some women did not receive any visitors at all during their postnatal stay. One woman had a cesarean section and her baby needed treatment for jaundice. This made it impossible for her to leave the ward to meet family and friends. Another woman described how she was allowed to have one visitor, but it had to be the same person who was present at the birth. These rules and regulations were sometimes impossible to follow, and the consequences were unpleasant:
My stay at the postnatal ward was not a pleasant experience. My mother had to work, so I asked the staff if my sister could come stay with me a few hours during the day so I could have a shower and a quick meal. I was told that only fathers and siblings of the baby were allowed, and that this rule had to be followed. I ended up alone in my room, full of hormones and tears and a huge frustration because I couldn’t breastfeed my baby. (Interview # 5)
Many women described feeling isolated. Further, some women mentioned the fear of getting postpartum depression, potentially adding an extra burden to the new family. Some described how their stay on the postnatal ward had ruined their feelings of joy at having given birth to a baby.
My best friend was told to leave. I was alone and in pain. I’ve never felt so lonely before, never experienced such pain. My postnatal period was ruined because of this (…). It took away the pleasure of having had a baby (…) So I think hospitals need to change their rules to include us, although I have argued that we should be treated the same as everybody else. (Interview # 7)
The participants in this study had been open about their decision to have a baby before trying to conceive and said they felt supported by their family and friends. At the same time, they sometimes felt vulnerable being alone, although they were familiar with research demonstrating that children born to solo mothers manage well in life. The women realized that their children had fewer relatives than if they had had a partner and it was therefore important to have a good social network that played a role in their children’s lives. Several women had become members of a network for solo mothers.
I’ve got to know many women who’ve used a donor, and I think they’re amazing women. They seem to be doing just fine. If somebody has a problem, it’s usually an ordinary problem, such as breastfeeding or sleeping. It has nothing to do with being single. I believe that when you choose to become a mother like this, you make an effort to build a network before the baby’s born. (Interview # 6)
Discussion
The women in our study pointed out that their family was different from other families and they recognized that the postnatal period was different for them than for other mothers. These findings are supported by previous research describing how solo mothers stand out from other groups of single mothers, having gone to great lengths in the process of starting a family.26 Yet the women also underlined that it was important to be seen as ordinary mothers as many of their needs mirror the needs one would expect from women in general, including other single mothers, during the postnatal period. However, similar experiences are described by lesbian women,27 demonstrating that some groups of women are particularly vulnerable in the encounter with maternity care services. As long as becoming a solo mother is prohibited in some societies, these women risk challenging cultural understandings of the family constellation.28
The women carefully considered if and when to ask for help, and some expressed a fear of being judged or rejected by staff. In the provision of individualized care, it is important to understand how solo mothers often prefer to adapt to the situation rather than asking for help in order to avoid being a burden. The women in our study accepted considerable responsibility as new mothers, and they identified themselves as independent and responsible women. One woman described the unpleasant feeling of being rebuffed when she finally asked for help, and she decided to manage on her own although she felt exhausted. Solo mothers’ reluctance to ask for help may make them vulnerable during their stay on the postnatal ward. According to the International Confederation of Midwives’ Code of Ethics,29 midwives should provide culturally sensitive care to all women and their families and actively encourage women to participate in caring decisions. This was demonstrated in our study when midwives responded to solo mothers’ individual caring needs, acknowledging their decision to start a family. In such situations, the women felt respected.
In line with earlier research,3,9,11,26,30 the women in our study explained how they chose to become solo mothers because their biological clock was ticking. They were aware that their child would have few relatives and therefore made an extra effort to establish a social network before giving birth. The value of consciously building a support network to help them on their parenting journey has also been described in other literature.9,31 The women wanted to include significant others during their stay in the postnatal ward, but staff or hospital regulations did not always acknowledge this. As a result, there were restrictions on the visitors they could receive. Consequently, strict hospital rules and regulations amplified their feeling of being different and not being cared for in the same way as two-parent families. Some solo mothers even described how their stay in the postnatal ward deprived them of the joy of becoming a mother. Studies demonstrate that women in postnatal wards are more satisfied with care if they are accompanied by their partners.32 This underlines that the needs of solo mothers are similar to the needs of other women. The postnatal period is considered a profound and precious time in a woman’s life, and woman-centered care acknowledges how the well-being of the mother affects not only her family but society as a whole.17 Lack of acknowledgment of individual women’s needs runs contrary to the idea of woman-centered care, which encourages women to involve people who are important to them and to let the women themselves make decisions, rather than basing the care on the needs of the staff or institution.17
The women realized that being a single parent rendered them vulnerable and some feared postpartum depression. However, studies describe that solo mothers often have better health than unmarried single or divorced women, and do not experience higher levels of depression, anxiety or stress associated with parenting than women who have a partner.26 Nevertheless, several women explained how they felt they had to be extra good mothers. The fact that they had made an active decision to parent alone made them feel they had something to prove and they therefore strived to appear successful. However, such mothers’ deliberate decision to become a solo mother often provides a positive foundation for the new family.26 Research comparing solo mother families with two-parent families, all with children by donor insemination, shows no differences in parenting quality or child adjustment, apart from lower mother-child conflict in solo mother families.26 The findings in this study suggest that staff should be aware of how the postnatal stay can be experienced by solo mothers and strive to provide sensitive and individualized care. Recognizing the woman’s specific needs based on her own expertise is a central tenet in woman-centered care.17 However, it can be challenging for the midwife if solo mothers avoid taking the initiative to ask for help. By accepting the fact that motherhood may result in feelings of insecurity for all women, midwives have the possibility to alleviate solo mothers’ feelings of stress related to being good enough mothers.
A lack of knowledge about solo mothers can create a situation of distrust, in line with research describing how a patient’s trust in nurses depends on the nurses’ level of knowledge and their commitment to forming a relationship with the patient.33 Consequently, not asking for help could result in lack of adequate care for mother and baby, and could in the worst case be a threat to patient safety. It is therefore important to have a holistic approach involving the recognition of the solo mother’s social, emotional, physical, spiritual and cultural needs.17
The solo mothers appreciated midwives’ unsolicited offers of help. Furthermore, women who gave birth in small hospitals expressed a higher level of satisfaction with postnatal care than those in larger hospitals. Similar findings have been described elsewhere,34 showing significantly greater patient satisfaction with receiving help in small hospitals than in medium-sized or large hospitals. Our findings might question the structure of maternity care in larger institutions, where the needs of the organization may have priority over those of the individual woman. If that is the case, it is contrary to the theory of woman-centered care and midwives should aim to create situations where all women can feel empowered.17
Strengths and Limitations
The authors are registered nurse midwives with vast experiences of antenatal, intrapartum and postnatal care, including caring for solo mothers. The first author works as a clinical midwife and conducted the interviews as part of her master’s degree in midwifery. One co-author is a PhD student in midwifery, the other holds a PhD in midwifery. Both teach midwifery in Norwegian universities.
Knowledge about solo mothers’ postnatal caring experiences is scarce, and this study adds important knowledge about a group of women that will probably increase in number in line with a higher average age at childbirth and a changing family structure.35
Our sample consisted of nine women from a hard-to-reach population and can be characterized as a small-scale convenience sample. The sample included women living in urban and rural areas in various parts of Norway and we found that it demonstrated sufficient information power to elucidate the study aim. Information power is a concept that can be regarded as an aspect of a study’s internal validity. Sufficient information power depends upon study aim, sample specificity, use of theory, quality of dialogue and analysis strategy. Thus, when a sample contributes with rich data relevant to elucidate the study aim, a low number of participants are needed.22 However, we recruited the informants from a network for solo mothers, and this may have positively influenced their willingness to share their stories. Furthermore, all women had comparable ethnicity and educational level, thus a sample including women from non-Western cultures would have strengthened the study.
Nonetheless, no study can fully describe and understand people’s experiences, and the results can therefore not be generalized to all solo mothers in various settings.36
Conclusion
Solo mothers see themselves as different from other mothers. They are conscious of their needs but have a high threshold for requesting help after birth. The results of this study underline how their individual needs are not always met in postnatal care. The findings suggest a need for increased knowledge and awareness regarding solo mothers and their life situations. When solo mothers have fewer rights than other women, national guidelines on postnatal care need re-evaluation. As this study focus merely on the experiences of solo mothers, future studies are encouraged to investigate the experiences of other single mothers.
Acknowledgment
We would like to thank the women who participated in this study and Paul Farmer for editing the text in the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ory SJ, Devroey P, Banker M, et al. International federation of fertility societies surveillance 2013: preface and conclusions. Fertil Steril. 2014;101(6):1582–1583. doi:10.1016/j.fertnstert.2014.03.045
2. The Norwegian Directorate of Health. Svangerskapsomsorgen. Nasjonal faglig retningslinje [Pregnancy care. National guidelines]. 2018. Available from: https://www.helsedirektoratet.no/retningslinjer/svangerskapsomsorgen.
3. Graham S. Choosing single motherhood? Single women negotiating the nuclear family ideal. In: Cutas D, Chan S, editors. Families – Beyond the Nuclear Ideal. London: Bloomsbury Academic; 2014:97–109.
4. Statistics Norway. Births, main figures. Available from: https://www.ssb.no/en/befolkning/statistikker/fodte.
5. Norwegian Biotechnology Advisory Board. Evaluering av bioteknologiloven 2014–15 [evaluation of the biotechnology act 2014–15]; 2015. Available from: http://www.bioteknologiradet.no/filarkiv/2015/08/Evaluering-av-bioteknologiloven.pdf.
6. Präg P, Mills MC. Assisted reproductive technology in Europe: usage and regulation in the context of cross-border reproductive care. In: Kreyenfeld M, Konietzka D, editors. Childlessness in Europe: Contexts, Causes, and Consequences. Cham: Springer International Publishing; 2017:289–309.
7. Shenfield F, de Mouzon J, Pennings G, et al. Cross border reproductive care in six European countries. Hum Reprod. 2010;25(6):1361–1368. doi:10.1093/humrep/deq057
8. Golombok S. Families created by reproductive donation: issues and research. Child Dev Perspect. 2013;7(1):61–65. doi:10.1111/cdep.12015
9. Jadva V, Badger S, Morrissette M, Golombok S. ‘Mom by choice, single by life’s circumstance … ’ findings from a large scale survey of the experiences of single mothers by choice. Hum Fertil. 2009;12(4):175–184. doi:10.3109/14647270903373867
10. Graham S. Being a ‘good’ parent: single women reflecting upon ‘selfishness’ and ‘risk’ when pursuing motherhood through sperm donation. Anthropol Med. 2018;25(3):249–264. doi:10.1080/13648470.2017.1326757
11. Murray C, Golombok S. Solo mothers and their donor insemination infants: follow-up at age 2 years. Hum Reprod. 2005;20(6):1655–1660. doi:10.1093/humrep/deh823
12. Ben‐Daniel N, Rokach R, Filtzer L, Feldman R. When two are a family: looking backward and looking forward in a group intervention with single‐by‐choice mothers. J Fam Ther. 2007;29(3):249–266. doi:10.1111/j.1467-6427.2007.00385.x
13. Bock JD. Doing the right thing? Single mothers by choice and the struggle for legitimacy. Gend Soc. 2000;14(1):62–86. doi:10.1177/089124300014001005
14. Svensson C. Anknytningsrepresentationer Och Upplevelser Av Social Acceptans Hos Ensamstående Kvinnor Som Planerar Eller Överväger Att Få Barn, Som Väntar Barn Eller Som Har Fått Barn Genom Assisterad Befruktning (Donatorinsemination) - En Pilotstudie [Representations of Attachment and Experiences of Social Acceptance in Single Women Planning or Considering Having a Child, Expecting a Child or Having Had a Child Through Assisted Reproduction (Donor Insemination): A Pilot Study]. Student Publication for Professional Degree. Sweden: Department of Psychology, Lund University; 2014. Available from: http://lup.lub.lu.se/luur/download?func=downloadFile&recordOId=4587833&fileOId=4587834. 2014.
15. Ben-Ari A, Weinberg-Kurnik G. The dialectics between the personal and the interpersonal in the experiences of adoptive single mothers by choice. Sex Roles. 2007;56(11–12):823–833. doi:10.1007/s11199-007-9241-1
16. Jacobsen KS, Dahl B. More than just a child – solo mothers’ maternity care experiences. Sex Reprod Healthc. 2017;12:58–63. doi:10.1016/j.srhc.2017.03.001
17. Leap N. Woman-centred or women-centred care: does it matter? Br J Midwifery. 2009;17(1):12–16. doi:10.12968/bjom.2009.17.1.37646
18. Rudman A, Waldenström U. Critical views on postpartum care expressed by new mothers. BMC Health Serv Res. 2007;7(1):178. doi:10.1186/1472-6963-7-178
19. Norwegian institute of Public Health. User experiences of pregnancy, birth and postnatal care. National results; 2013. Available from: https://www.fhi.no/en/publ/2013/user-experiences-of-pregnancy-birth-and-postnatal-care.-national-results/.
20. Schneider Z, Whitehead D, Lobiondo-Wood G, Haber J. Nursing and Midwifery Research: Methods and Appraisal for Evidence-Based Practice.
21. Waldenström U. Why do some women change their opinion about childbirth over time? Birth. 2004;31(2):102–107. doi:10.1111/j.0730-7659.2004.00287.x
22. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
23. Kvale S, Brinkmann S. InterView: en introduktion til det kvalitative forskningsinterview [Interviews: An Introduction to Qualitative Research Interviewing]. Copenhagen: Hans Reitzel; 2002.
24. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40:795–805. doi:10.1177/1403494812465030
25. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects; 2018. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
26. Golombok S, Zadeh S, Imrie S, Smith V, Freeman T. Single mothers by choice: mother-child relationships and children’s psychological adjustment. J Fam Psychol. 2016;30(4):409–418. doi:10.1037/fam0000188
27. Spidsberg BD. Vulnerable and strong – lesbian women encountering maternity care. J Adv Nurs. 2007;60(5):478–486. doi:10.1111/jan.2007.60.issue-5
28. Dalton SE, Bielby DD. That’s our kind of constellation: lesbian mothers negotiate institutionalized understandings of gender within the family. Gend Soc. 2000;14(1):36–61. doi:10.1177/089124300014001004
29. ICM International Confederation of Midwives. International code of ethics for Midwives; 2008. Available from: https://www.internationalmidwives.org/assets/files/general-files/2019/01/cd2008_001-eng-code-of-ethics-for-midwives.pdf.
30. Hertz R. Single by Chance, Mothers by Choice: How Women are Choosing Parenthood Without Marriage and Creating the New American Family. New York: Oxford University Press; 2006. Available from: https://ezproxy2.usn.no:2537/lib/ucsn-ebooks/detail.action?docID=430936.
31. Golash D, Turkulainen T. Challenges and Resources of Single Mothers by Choice in Helsinki, Finland. Student Publication for Professional Degree. Helsinki: Diaconia University of Applied Sciences; 2018. Available from: https://www.theseus.fi/handle/10024/145909.
32. Barimani M, Vikström A. Successful early postpartum support linked to management, informational, and relational continuity. Midwifery. 2015;31(8):811–817. doi:10.1016/j.midw.2015.04.009
33. Rørtveit K, Hansen BS, Leiknes I, Joa I, Testad I, Severinsson E. Patients’ experiences of trust in the patient-nurse relationship - a systematic review of qualitative studies. Open J Nurs. 2015;5:195–209. doi:10.4236/ojn.2015.53024
34. Holte TO, Bjertnaes ØA, Stavem K. Er det sammenheng mellom sykehusstørrelse og pasienterfaringer? [Is there a correlation between hospital size and patient experiences?]. Tidsskr nor Laegeforen. 2005;125(12):1685–1688.
35. Letablier MT, Wall K. Changing lone parenthood patterns: new challenges for policy and research. In: Bernardi L, Mortelmans D, editors. Lone Parenthood in the Life Course. Cham: Springer; 2018:29–55.
36. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/S0140-6736(01)05627-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.