Back to Journals » International Journal of Women's Health » Volume 18
Solid Pseudopapillary Neoplasms of the Pancreas with Delayed Ovarian Metastasis During Pregnancy: A Case Report and Literature Review
Authors Jie R, Dai X ![]() , Lei H, Peng F
, Lei H, Peng F
Received 20 October 2025
Accepted for publication 20 January 2026
Published 11 April 2026 Volume 2026:18 575652
DOI https://doi.org/10.2147/IJWH.S575652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Ruixia Jie, Xiaomin Dai, Huan Lei, Fang Peng
Department of Pathology, Zhejiang Hospital, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Fang Peng, Department of Pathology, Zhejiang Hospital, 12 Lingyin Road, Xihu District, Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel +86 13588881606, Email [email protected]
Background: Solid pseudopapillary neoplasm (SPN) of the pancreas is a rare, low-grade malignant epithelial tumor that may originate from embryonic multipotent stem cells. The prevalence of metastatic SPN is approximately 9% to 15%, most commonly in the liver and peritoneum. Delayed ovarian metastasis during pregnancy is exceedingly rare, pregnancy may promote the progression and pose a life-threatening risk.
Case Presentation: A 38-year-old female with an early intrauterine pregnancy was found to have a large mass in the right ovary. Following pregnancy termination and surgical resection, initial pathological assessment indicated a sex cord-stromal tumor, specifically a luteinized Sertoli-Leydig cell tumor. Upon reviewing her medical history, it was noted that a pancreatic tumor resection performed ten years prior. Further immunohistochemical analysis demonstrated diffuse nuclear and cytoplasmic expression of β-catenin, along with positivity for LEF-1, CD10, and TFE-3. Based on these findings, the final diagnosis was revised to pancreatic SPN with delayed ovarian metastasis. The patient showed no evidence of disease recurrence during the 2-year follow-up after treatment.
Conclusion: This is a rare case of ovarian metastatic pancreatic SPN that occurred during pregnancy ten years after the initial diagnosis. Our findings underscore the diagnostic challenge in distinguishing metastatic lesions from primary ovarian tumors and highlight the clinical importance of excluding high-grade transformation during pathological assessment.
Keywords: pregnancy, solid pseudopapillary neoplasm, metastasis, treatment
Background
Solid pseudopapillary neoplasm (SPN) of the pancreas is a rare tumor composed of epithelioid cells with weak intercellular adhesion, forming solid and pseudopapillary structures without definitive pancreatic epithelial differentiation. SPN predominantly affects females, particularly adolescent girls and women of reproductive age.1 While most SPNs demonstrate low-grade malignant behavior and favorable prognosis, up to 20% of cases may develop local recurrence or distant metastasis after complete surgical resection.2 The liver and peritoneum are the most common sites of metastasis, whereas lymph node involvement is rare. Although tumor size and invasive growth pattern have been linked to recurrence and metastatic potential, these features alone are not reliable predictors of postoperative outcome.2 Molecular studies have demonstrated that the majority of SPNs harbor point mutations in exon 3 of the CTNNB1 gene, which encodes β-catenin, leading to nuclear accumulation of β-catenin and subsequent expression of LEF-1.3
The female predominance and age distribution suggest a possible role for hormonal factors in the pathogenesis of SPN, though a clear association with endocrine dysfunction has not been established. Notably, progesterone receptor expression is reported in 80–100% of SPNs, which may promote tumor cell proliferation and could explain the accelerated growth occasionally observed in young women during pregnancy.4 In pregnant patients, lesion size progressively increases over time, posing increased risks for multiorgan resection, tumor rupture with hemorrhage, and malignant transformation. This study reports a case of delayed ovarian metastasis from pancreatic SPN diagnosed during pregnancy and aims to investigate its clinical manifestations, pathological diagnosis, differential diagnosis, and treatment strategies. Furthermore, the systematic review of previously reported cases was conducted to enhance understanding of this entity and reduce misdiagnosis.
Case Presentation
Clinical Summary
A 38-year-old female (G3 P1001) was admitted to our hospital with a three-month history of perceived lower abdominal distension and two months of amenorrhea. The patient had a normal menstrual cycle and no significant family history. Ultrasonography examination confirmed an intrauterine pregnancy and revealed an enlarged right ovary with cystic lesion, along with the presence of pelvic and abdominal effusion, raising suspicion for an ovarian tumor. Given the patient’s request for pregnancy termination, further radiological evaluation was performed. Abdominal computed tomography (CT) scan revealed a well-defined, complex cystic-solid mass in the right mid-to-lower abdomen. The lesion was multilocular, with enhancement of the cyst wall and solid components following contrast administration (Figure 1). A feeding artery originating from the anterior wall of the right abdominal aorta was also identified. These imaging features were highly suggestive of an ovary malignant tumor. Laboratory testing revealed an elevated carbohydrate antigen 125 (CA125) level of 413.80U/mL (normal range: <35.00U/mL). Subsequently, the patient underwent surgical resection of the ovarian mass. Intraoperatively, the right ovary was markedly enlarged, measuring approximately 15.0*15.0*12.0 cm. Multiple nodules were observed on the mucosal surface of the lower rectum and within the rectouterine pouch. No abnormal nodules were identified in the left adnexa, omentum, pelvic peritoneum, or hepatic capsule. Furthermore, no enlarged lymph nodes were identified on either side of the abdominal aorta. The procedure lasted approximately three hours, with stable anesthesia maintained throughout, and an estimated intraoperative blood loss of 300 mL.
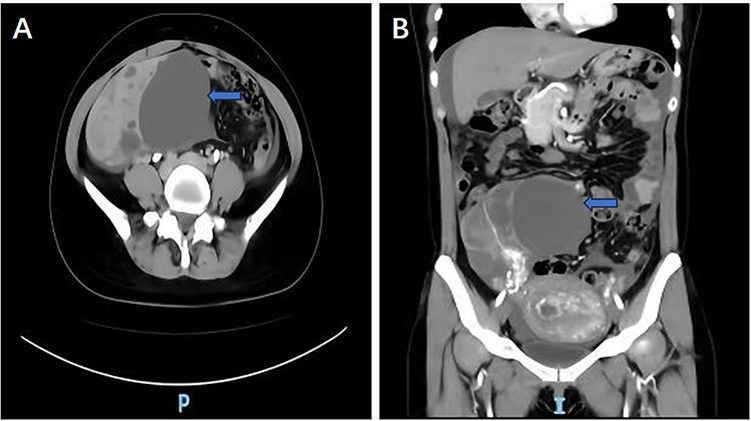 |
Figure 1 The abdominal computed tomography scan revealed a well-defined mass in the right adnexal region with a cystic component. The arterial blood supply to the mass originated from the right anterior aspect of the abdominal aorta ((A and B); blue arrows indicate the mass). |
Pathologic Findings
The resected tumor was well-circumscribed with a smooth external surface and exhibited a mixed cystic and solid components. Old coagulated blood-like material was present within the cystic cavity (Figure 2A). Histologically, the tumor was composed of complex architectural patterns separated by fibrous septa and branching vasculature. These patterns included cystic regions, solid components, pseudopapillary structures, and foci of hemorrhagic necrotic (Figure 2B and C). The pseudopapillary regions were lined by tumor cells with mucinous, clear cytoplasm (Figure 2D). The tumor cells displayed round nuclei, moderately eosinophilic cytoplasm, inconspicuous nucleoli, and rare mitotic figures. Extracellular eosinophilic hyaline globules were observed (Figure 2E). Abundant cholesterol crystals were also present (Figure 2F). The histopathological features of the nodules from the lower rectum mucosa and the rectouterine pouch were identical to those of the ovarian tumor. The immunohistochemical analysis revealed the tumors were negative for CKpan (Figure 3A), EMA, Inhibin-α (Figure 3B), CD99, WT1, ER, and Pax8. Positive staining was observed for CD56 (Figure 3C), PR, and Calretinin. The Ki-67 proliferation index was approximately 15%. The initial diagnosis was an ovarian sex cord-stromal tumor, specifically the Sertoli-Leydig cell tumor with luteinized features.
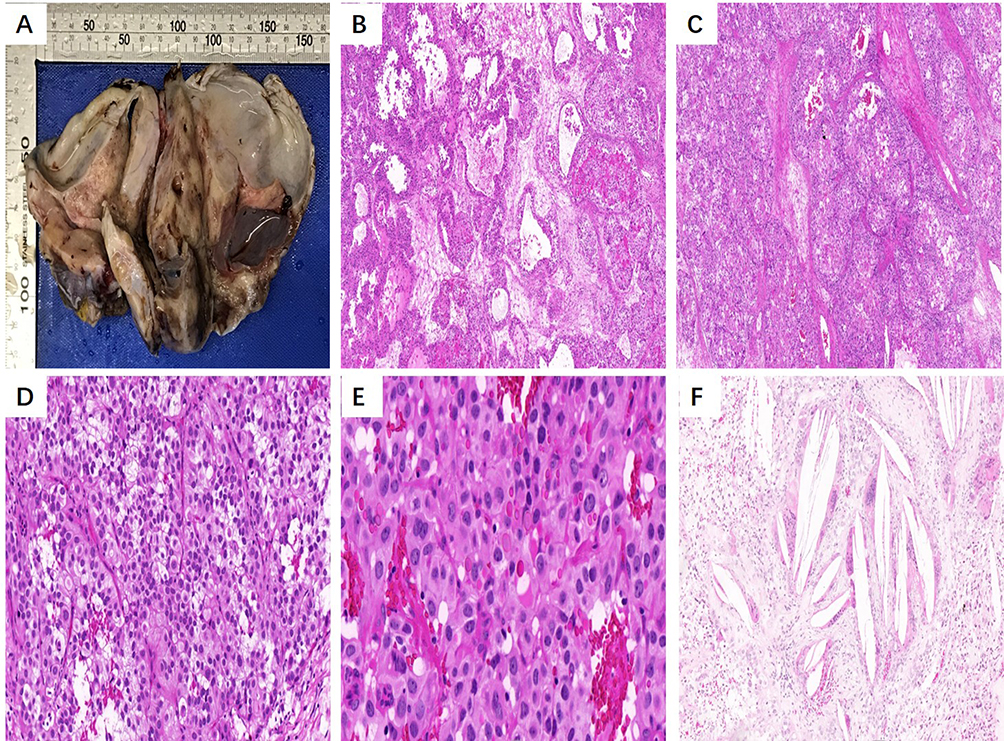 |
Figure 2 The histologic findings of the resected ovarian tumor. Macroscopically, the tumor exhibited a cystic-solid architecture, with evidence of prior hemorrhage observed within the cystic cavity (A). Hematoxylin and eosin (HE) staining showed microcystic structures, and the tumor cell nests were surrounded by distinct fibrous septa ((B and C), 40x). The tumor cells were polygonal, with uniform round nuclei and moderate amount of lightly eosinophilic cytoplasm ((D), 100x). Eosinophilic hyaline globules were prominently visible ((E), 100x). Additionally, cholesterol crystals were identified ((F), 100x). |
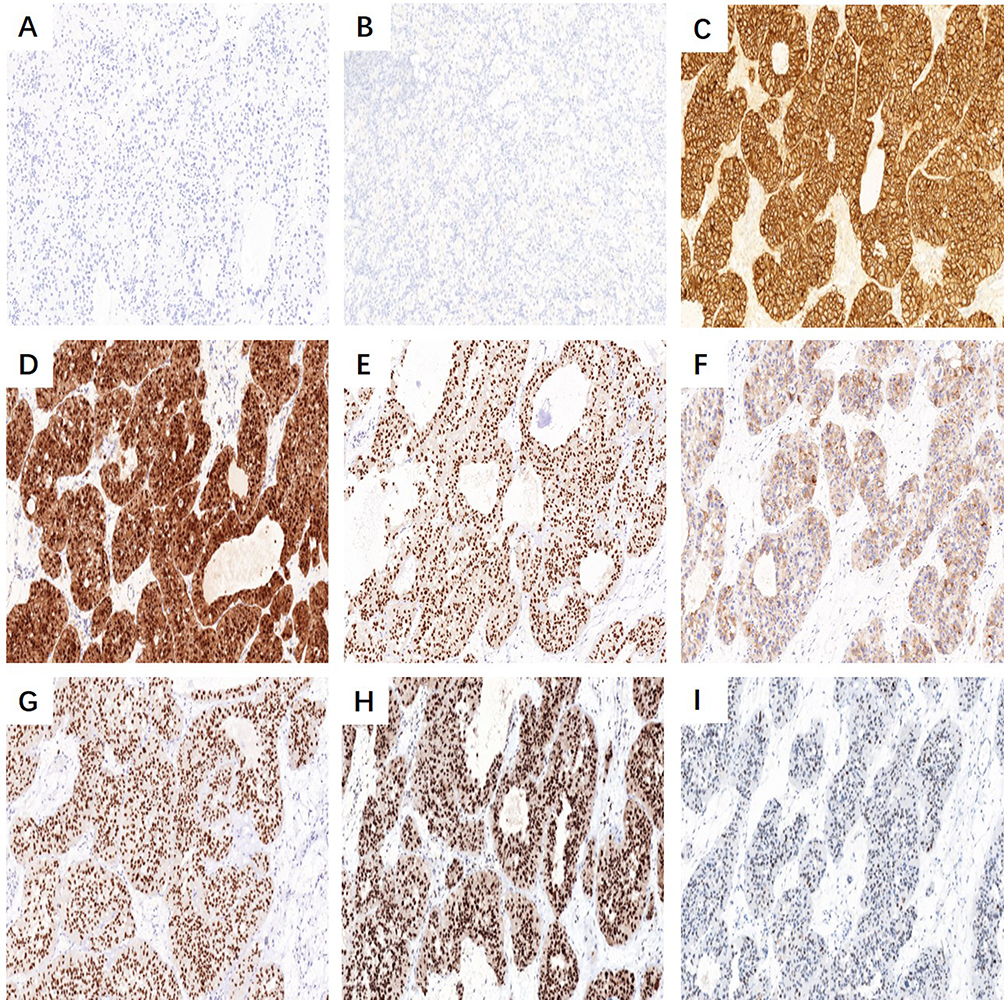 |
Figure 3 Representative immunohistochemical findings in the ovarian tumor (original magnification, 200x). The tumor cells completely lack expression of CKpan (A) and Inhibin-α (B). CD56 is expressed on the cell membrane of tumor cells (C). β-catenin staining demonstrates positive immunoreactivity in both the nucleus and cytoplasm (D). LEF-1 shows nuclear positivity (E). Tumor cells exhibit positive immunoreactivity for CD10 (F), TFE-3 (G), and Rb-1 (H), while p53 staining displays variable intensity (I). |
Upon reviewing the patient’s clinical history, it was noted that she had undergone pancreatic tumor resection ten years prior, although the postoperative pathological diagnosis was not available. To evaluate the possibility of ovarian metastasis from a pancreatic neoplasm, additional immunohistochemical analysis was performed. The tumor cells showed positive nuclear and cytoplasmic β-catenin expression (Figure 3D). Positivity was also observed for LEF-1, CD10, TFE-3, and Rb-1 (Figure 3E–H). In contrast, E-cadherin and p16 were negative, and p53 staining was heterogeneous (Figure 3I).
Diagnostic Assessment
Based on comprehensive clinicopathological evaluation, including the characteristic immunohistochemical profile of lost E-cad expression and nuclear/cytoplasmic β-catenin positivity, the final diagnosis was revised to SPN of the pancreas with delayed ovarian metastasis. Cytological examination of the peritoneal lavage fluid revealed no evidence of tumor cells.
Postoperative Course and Follow-Up
The patient recovered well postoperatively and did not undergo adjuvant therapy. During the 2-year follow-up period, she remained in good health with no evidence of tumor recurrence or metastasis.
Discussion
Based on a comprehensive assessment of clinical history, histopathological features, and immunohistochemical findings, the present case was definitively diagnosed as an ovarian metastasis from a pancreatic SPN. The clinical significance lies in the rarity of documented instances of delayed ovarian metastasis occurring 10 years after the initial diagnosis of pancreatic SPN. To the best of our knowledge, such cases identified during pregnancy are even rarer. A key diagnostic challenge is the accurate differentiation between metastatic lesions and primary ovarian tumors.
SPN of the pancreas is a rare, low-grade malignant tumor, accounting for 1% to 3% of all pancreatic exocrine neoplasms.5 It can occur at any age but is predominantly observed in adolescent and young adult females, with a male-to-female ratio of approximately 1:10.6 Although SPN can arise in any region of the pancreas, it most frequently arises in the pancreatic tail.7 Clinical manifestations range from asymptomatic presentation to mild upper abdominal discomfort, such as nausea and vomiting, which may result from gastrointestinal compression by the tumor. Imaging plays an indispensable role in the early detection and diagnosis of SPN.8 In addition, cases of SPN arising in extra-pancreatic sites, including the ovary, testis, and retroperitoneum have also been reported,9 with ectopic pancreatic tissue occasionally documented in such instances. It has been hypothesized that these tumors may originate from primordial germinal ridge cells or ectopic ovarian precursor cells in the pancreas during early embryonic development.10
Histologically, SPN exhibits diverse architectural patterns, including cystic, solid, and pseudopapillary components in varying proportions. Tumor cells adjacent to cystic areas exhibited a trabecular or acinar arrangement, while those within solid areas display patchy to diffuse growth. The cells are relatively uniform in size, with round to oval nuclei, abundant eosinophilic cytoplasm, and inconspicuous nucleoli. Mitotic figures are rare. Delicate fibrovascular septa surround and separate tumor clusters, supporting the formation of characteristic pseudopapillary structures, which represent a key diagnostic morphological feature.11 Immunohistochemically, tumors cells typically expression vimentin, CD10, and CD56. Aberrant nuclear and cytoplasmic β-catenin staining is frequently observed, along with nuclear positivity for LEF-1, which serves as a useful adjunct in diagnosis.12 Recent studies also highlight nuclear TFE-3 expression as a distinct immunophenotypic marker in SPN.13 The combined use of β-catenin, CD10, and TFE-3 thus serve as valuable immunohistochemical panel for diagnosing SPN. Notably, fluorescence in situ hybridization (FISH) analysis revealed no evidence of chromosomal translocation.14
Given the extreme rarity of metastatic pancreatic SPN to the ovary, accurate differentiation from primary ovarian tumors is essential, including Sertoli-Leydig cell tumors, granulosa cell tumors, and steroid cell tumors. Sertoli-Leydig cell tumors typically lack pseudopapillary features and are immunoreactive for Inhibin-α, CD56, and Calretinin. In the present case, although tumor cells expressed CD56 and calretinin, it was completely negative for Inhibin-α. Ovarian neuroendocrine tumor also enter the differential diagnosis; however, the tumor cells in this case lacked characteristic neuroendocrine features such as “salt-and-pepper” chromatin. Combined with nuclear β-catenin expression and the absence of neuroendocrine markers including CgA and Syn, a neuroendocrine tumor was confidently excluded. Furthermore, the uniform morphology, absence of significant atypia or pleomorphism, and negative immunohistochemical staining for epithelial markers effectively ruled out a malignant epithelial neoplasm.
Primary ovarian SPN, which exhibits histological and immunohistochemical features similarly to pancreatic SPN, represents another significant differential diagnosis. This entity is exceedingly rare and can only be diagnosed after excluding metastatic pancreatic SPN. Extra-pancreatic SPN may also occur in sites such as the testis, reproductive tract, retroperitoneum, and mesocolon, with or without associated ectopic pancreatic tissue.15 In the present case, a diagnosis of metastatic SPN was established based on the following findings: (1) a history of pancreatic tumor resection 10 years prior, despite unavailable pathological records; (2) identification of multiple metastatic lesions in the lower rectum and rectouterine pouch during surgery; (3) most importantly, thorough histological sampling revealed no ectopic pancreatic tissue within or adjacent to the ovarian lesion, effectively excluding primary ovarian SPN.
The unique aspect of this case is the presentation of delayed ovarian metastasis during pregnancy, occurring 10 years after radical resection of the primary pancreatic tumor. SPNs are considered hormone-sensitive tumors, frequently expression of PR. Their predilection for young women, together with reports suggesting that elevated serum progesterone may promote tumor progression, supports a potential role for PR-mediated signaling in regulating tumor growth.16 A literature review identified only three reported cases of metastatic SPN occurring during pregnancy, including the present case17,18 (Table 1). One reported pulmonary and hepatic metastases 8 years after pancreatic tumor resection, and another presented with hepatic metastasis at initial diagnosis.
 |
Table 1 Clinical Analysis of 3 Cases of Pancreatic SPN Metastasis During Pregnancy |
Recent studies have described an aggressive SPN characterized by diffuse tumor cell proliferation, extensive apoptosis, and elevated mitotic activity. According to the fifth edition of World Health Organization (WHO) classification of digestive system tumors, this rare subtype is designated as “SPN with foci of high-grade malignant transformation”.19 Honda et al further characterized this variant pathologically and molecularly, noting that high-grade SPNs exhibit more aggressive behavior and distinct genetic alterations compared to conventional SPN.20 Necrosis and high-grade nuclear atypia are recognized as key indicators of aggressive malignancy. In our case, thorough histopathological evaluation revealed only mild nuclear pleomorphism, rare mitotic figures, and no evidence of necrosis. Immunohistochemically, the tumor revealed focal weak positivity for p16, intact Rb-1 expression, and wild-type p53 staining pattern. Collectively, these findings support the absence of high-grade malignant transformation.
Surgical resection remains the mainstay of treatment, with the primary goal of achieve complete tumor removal while preserving functional pancreatic parenchyma.21 In cases with evidence of invasive growth, concurrent peripancreatic lymph node dissection is recommended.22 The management of SPN during pregnancy presents particular challenges due to the absence of clear treatment guidelines, especially regarding the optimal timing of surgery.23 Decisions regarding surgical intervention during pregnancy or deferral until postpartum should therefore be individualized, based on multidisciplinary discussion and tailored to the patient’s specific clinical scenario. Recent studies also suggest that endocrine therapy may offer potential benefit in patients whose tumors express sex hormone receptors.24
Conclusion
Pancreatic SPN is a low-grade malignant tumor that predominantly affects young females and carries a risk of recurrence and metastasis. Its clinical manifestations are nonspecific, frequently resulting in misdiagnosis as benign lesions. To the best of our knowledge, based on a comprehensive review of the current literature, this represents the first reported case of delayed ovarian metastasis occurring during pregnancy many years after surgical resection of the primary tumor. Thorough pathological examination is essential for establishing an accurate diagnosis and guiding subsequent treatment strategies. Surgical resection remains the treatment of choice for SPN, whereas alternative therapeutic approaches require further investigation and clinical validation.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The retrospective analysis of clinical data and publication of this case report were reviewed and approved by the Ethics Committee of Zhejiang Hospital. The study was exempted from full ethical review due to its retrospective nature, with the ethical approval number: 2024-CA-15.
Consent for Publication
Written informed consent was obtained from the patient to publish this paper.
Acknowledgments
We are grateful to the patients who provided message for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Vassos N, Agaimy A, Klein P, Hohenberger W, Croner RS. Solid-pseudopapillary neoplasm (SPN) of the pancreas: case series and literature review on an enigmatic entity. Int J Clin Exp Pathol. 2013;6(6):1051–8.
2. Abudalou M, Vega EA, Dhingra R, et al. Solid pseudopapillary neoplasm-diagnostic approach and postsurgical follow up: three case reports and review of literature. World J Clin Cases. 2021;9(7):14. doi:10.12998/wjcc.v9.i7.1682
3. Patil P, Patel NR, Jackson C, Mathews CA, Singh K. Primary ovarian solid pseudopapillary neoplasm with CTNNB1 c.98C>G (p.S33C). Point Mutation. 2016;37(2):110–116.
4. Shih-Chiang H, Tsung-Han W, Chien-Cheng C, Tse-Ching C. Spontaneous rupture of solid pseudopapillary neoplasm of the pancreas during pregnancy. Obstet Gynecol. 2013;121(2):486–488. doi:10.1097/AOG.0b013e31826d292f
5. Dinarvand P, Lai J. Solid pseudopapillary neoplasm of the pancreas: a rare entity with unique features. Arch Pathol Lab Med. 2017;141(7):990–995. doi:10.5858/arpa.2016-0322-RS
6. Hang L, Zhiquan X, Yaxu W, et al. Case report: a case report and literature review of extrapancreatic solid pseudopapillary neoplasm. Front Surg. 2022;9:1020044. doi:10.3389/fsurg.2022.1020044
7. Theodossios P, Spiros P. Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature. J Am Coll Surg. 2005;200(6):965–972. doi:10.1016/j.jamcollsurg.2005.02.011
8. Agnieszka P, Wiktoria B, Paulina W, Beata J, Sławomir M. Pancreatic solid pseudopapillary neoplasms-clinicopathological characteristics and surgical outcomes: a 10-year single-centre observational study. Biomedicines. 2025;13(9):2050.
9. Akane Y, Yasuji R, Harumi T, Yoshihide A, Mitsuaki S, Shintaro T. An extrapancreatic solid-pseudopapillary neoplasm in the greater omentum. BJR Case Rep. 2017;3(3):20170008. doi:10.1259/bjrcr.20170008
10. Jingci C, Liju Z, Pengyan W, et al. Solid pseudopapillary neoplasms of the pancreas: clinicopathologic analysis and a predictive model. Mod Pathol. 2023;36(6):100141. doi:10.1016/j.modpat.2023.100141
11. Benoît T, Catherine C. Diagnosis and molecular aspects of solid-pseudopapillary neoplasms of the pancreas. Semin Diagn Pathol. 2014;31(6):484–490. doi:10.1053/j.semdp.2014.08.010
12. Saroja Devi G, Atif K, Anam K, et al. Application of LEF-1 immunohistochemical staining in the diagnosis of solid pseudopapillary neoplasm of the pancreas. Pathol Res Pract. 2024;263:155662. doi:10.1016/j.prp.2024.155662
13. Grant H, Amanda H, Cynthia G, et al. Overexpression of SOX11 and TFE3 in solid-pseudopapillary neoplasms of the pancreas. Am J Clin Pathol. 2017;149(1):67–75. doi:10.1093/ajcp/aqx142
14. Yina J, Juan X, Bo W, Yudong M, Peijun L. TFE3 is a diagnostic marker for solid pseudopapillary neoplasms of the pancreas. Hum Pathol. 2018;81:166–175. doi:10.1016/j.humpath.2018.07.005
15. Hejia Z, Dan X, Bo W, Hongzhou M. Extrapancreatic solid pseudopapillary neoplasm: report of a case of primary retroperitoneal origin and review of the literature. Oncol Lett. 2013;5(5):1501–1504. doi:10.3892/ol.2013.1242
16. Ladanyi M, Mulay S, Arseneau J, Bettez P. Estrogen and progesterone receptor determination in the papillary cystic neoplasm of the pancreas. With immunohistochemical and ultrastructural observations. Cancer. 1987;60(7):1604–1611.
17. Diogo S, Ana C, Filipe B, Joaquim V. Solid pseudopapillary neoplasm of pancreas with distant metastasis during pregnancy: a diagnostic and treatment challenge. BMJ Case Rep. 2020;13(12):e237309.
18. Ammad Javaid C, Taher J, Yara D, Abdulmalik S, Reena S. Late presentation of recurrent solid pseudopapillary pancreatic neoplasm with liver metastases during pregnancy. ACG Case Rep J. 2024;11(8):e01418. doi:10.14309/crj.0000000000001418
19. Francesca S, Magda Z, Andrea P, et al. The classification of neuroendocrine neoplasms of the lung and digestive system according to WHO, 5th edition: similarities, differences, challenges, and unmet needs. Panminerva Med. 2022;64(2):259–264. doi:10.23736/S0031-0808.22.04602-X
20. Shogo H, Hiroshi Y, Eriko A, et al. High-grade solid pseudopapillary neoplasms of the pancreas: distinct clinicopathological malignant features with intriguing gene alterations through a comparison with the conventional type. Am J Surg Pathol. 2024;48(3):353–363. doi:10.1097/PAS.0000000000002177
21. Lubezky N, Papoulas M, Lessing Y, et al. Solid pseudopapillary neoplasm of the pancreas: management and long-term outcome. Eur J Surg Oncol. 2017;43(6):1056–1060. doi:10.1016/j.ejso.2017.02.001
22. Gen S, Kang F, Xiaowei F, et al. Solid pseudopapillary neoplasm of the pancreas: a multi-institution study of 118 cases. Pancreas. 2023;52(2):121–126. doi:10.1097/MPA.0000000000002219
23. Huang TT, Zhu J, Zhou H, Zhao AM. Solid pseudopapillary neoplasm of pancreas in pregnancy treated with tumor enucleation: case report and review of the literature. Niger J Clin Pract. 2018;21(9):1234–1237. doi:10.4103/njcp.njcp_39_18
24. Anna K, Sevindzh E, Andrei K, et al. Endocrine therapy for metastatic solid pseudopapillary neoplasm of the pancreas: a case report. Front Oncol. 2022;12:970142. doi:10.3389/fonc.2022.970142
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Too Late to Treat: Missed Antenatal Syphilis Screening and a Fatal Neonatal Outcome – A Case Report
Nisa AS, Bayuaji H, Winarno GNA
International Medical Case Reports Journal 2025, 18:1111-1116
Published Date: 29 August 2025
High-Risk Pregnancy with Solid Pseudopapillary Tumor of the Pancreas Complicated by Obstetric Antiphospholipid Syndrome: A Case Report
Li S, Yu S, Yu X, Meng X, Zhu Y
International Journal of Women's Health 2025, 17:3693-3698
Published Date: 15 October 2025
A Case of Cutaneous Dirt-Adherent-Like Sweet Syndrome in Pregnancy
Ruan Z, Yang L, Tu P, Yu D
International Journal of Women's Health 2025, 17:5355-5360
Published Date: 10 December 2025