Back to Journals » International Journal of Women's Health » Volume 17
High-Risk Pregnancy with Solid Pseudopapillary Tumor of the Pancreas Complicated by Obstetric Antiphospholipid Syndrome: A Case Report
Authors Li S, Yu S, Yu X, Meng X, Zhu Y
Received 28 July 2025
Accepted for publication 2 October 2025
Published 15 October 2025 Volume 2025:17 Pages 3693—3698
DOI https://doi.org/10.2147/IJWH.S554457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Shan Li, Shasha Yu, Xiaomei Yu, Xiangcheng Meng, Yuchun Zhu
Obstetrics Medical Center, WeiFang People’s Hospital, Shandong Second Medical University, WeiFang, People’s Republic of China
Correspondence: Yuchun Zhu, Obstetrics Medical Center, WeiFang People’s Hospital, Shandong Second Medical University, WeiFang, People’s Republic of China, Email [email protected]
Background: Antiphospholipid syndrome(APS) is a common cause of recurrent miscarriage.This case report presents a rare case of a high-risk pregnancy complicated by the concurrent solid pseudopapillary neoplasm (SPN) and obstetric antiphospholipid syndrome (OAPS).
Case: A 35-year-old patient was diagnosed with SPN at the age of 27, accompanied by extensive abdominal metastases, and underwent palliative metastatic tumor resection and chemotherapy, achieving stable disease. After a 24-month treatment-free interval, pregnancy was attempted. She had a history of five adverse pregnancy outcomes (one intrauterine fetal demise at 28 weeks, three instances of embryonic arrest, and one biochemical pregnancy). OAPS was diagnosed based on persistent positivity (≥ 12 weeks apart) for lupus anticoagulant, anti-β 2 glycoprotein I antibody, and anti-cardiolipin antibody. Following a multidisciplinary evaluation, she was treated with a combination of tacrolimus, hydroxychloroquine, and prednisone to control antibody levels before planning for pregnancy. During the pregnancy, low molecular weight heparin combined with aspirin was administered, and ultimately, a healthy live baby was delivered via cesarean section at 36 weeks of gestation, with favorable maternal and neonatal outcomes. Currently, the patient remains disease-free with regular oncology follow-up and has preserved ovarian function.
Conclusion: This case suggests that for patients with tumors and pathological pregnancies, screening for the presence of antiphospholipid syndrome should be emphasized. Although SPN poses risks such as tumor growth and hemorrhage during pregnancy, patients with long-term stable disease may attempt pregnancy under close monitoring. It is important to balance the risks of anticoagulation with those of tumor-related bleeding during pregnancy.
Keywords: solid pseudopapillary neoplasm, obstetric antiphospholipid syndrome, pathological pregnancies
Introduction
SPN of the pancreas is a rare pancreatic tumor, accounting for 10–15% of pancreatic cystic tumors.1 Due to its malignant potential, with metastasis or local invasion occurring in 10–15% of cases, the World Health Organization(WHO) classifies it as a borderline tumor.2,3 SPN predominantly occurs in young women, particularly between the ages of 20 and 30. Immunohistochemical studies have shown that over 80% of SPN exhibit progesterone receptor overexpression.4 This characteristic suggests that the physiologically elevated serum progesterone during pregnancy may drive tumor proliferation/malignancy, making SPN a significant clinical challenge that impacts reproductive decision-making in women of childbearing age. APS is a systemic autoimmune disease characterized by the presence of autoantibodies—antiphospholipid antibodies (aPLs)—that recognize cell surface phospholipids and phospholipid-binding proteins.5 Recently, antiphospholipid antibodies have also been found in patients with malignant tumors. When pathological pregnancy is the primary clinical manifestation, it is referred to as OAPS.6 This disease is an important cause of increased incidence of recurrent miscarriage and late pregnancy complications related to placental dysfunction, such as fetal growth restriction and preeclampsia.7
Case Report
The patient is a 35-year-old female who presented to a local hospital at the age of 27 due to “right abdominal pain”. An enhanced abdominal CT scan showed: Multiple cystic-solid masses in the tail of the pancreas, the lesser curvature and greater curvature of the stomach, the intrahepatic and hilar regions, the upper pole of the left kidney, and the left subphrenic space, consistent with changes indicative of a solid pseudopapillary tumor of the pancreas. The patient subsequently underwent exploratory laparotomy and omentectomy at the local hospital. Intraoperative findings demonstrated extensive metastatic tumors in the omentum, the largest measuring approximately 10 cm × 4 cm × 3 cm, with a hard texture. Additionally, multiple hard nodules were palpated in the pelvic cavity, around the stomach, and the liver, rendering radical resection impossible. Thus, only the metastatic tumor in the omentum was excised and sent for pathological examination to clarify the nature of the tumor. The postoperative pathological result (from the abdominal omentum) indicated a solid pseudopapillary tumor of the pancreas. Immunohistochemical results showed: CD56(+), syn(+), CK broad(+), vimentin(+), CD10(+), Ki-67 (approximately 1% positive), P53 (approximately 10% positive), NSE (±), CgA(−). The patient underwent two cycles of postoperative chemotherapy, with details of the regimen unspecified. Follow-up abdominal MRIs were conducted at six-month intervals postoperatively, with no significant changes in tumor size observed.
Obstetric history: G6P1, with five instances of adverse obstetric outcomes (Table 1). Following her fifth miscarriage, the patient sought consultation from our obstetrics department for a comprehensive evaluation of recurrent miscarriage causes. This assessment revealed a lupus anticoagulant ratio of 2.62%, anti-β2 glycoprotein I antibody levels exceeding 300 AU/mL, and anti-cardiolipin antibody levels also greater than 300 AU/mL, with persistent positivity observed at the 12-week follow-up. These findings established a diagnosis of obstetric antiphospholipid syndrome (OAPS).6 The patient was subsequently initiated on a treatment regimen consisting of oral tacrolimus (0.5 mg, qd), hydroxychloroquine sulfate (0.2 g, bid), and prednisone acetate (10 mg, qd). Two years later, the patient’s condition remained stable, and she expressed a desire to conceive once more.
 |
Table 1 Adverse Obstetric History |
The patient conceived naturally. The last menstrual period was on September 6, 2023. After natural ovulation, subcutaneous injection therapy with Fondaparinux (2.5 mg, qd) was started, and oral medications were adjusted: Tacrolimus (0.5 mg, bid), Hydroxychloroquine Sulfate (0.2 g, bid), and Prednisone Acetate (10 mg, qd). Oral Aspirin (75 mg, qn) was started at 11 weeks of pregnancy and continued until 35 weeks. At 17 weeks of pregnancy, a follow-up abdominal MRI (Figure 1) revealed multiple cystic-solid mass shadows in the tail of the pancreas, left adrenal region, liver parenchyma, hepatic hilum, along the greater curvature of the stomach, and in the left subphrenic space, with the largest mass measuring approximately 9.2×8.5 cm. The antiphospholipid antibodies (aPLs) profile indicated: anticardiolipin antibody IgG at 60.6 U/mL, anti-β2 glycoprotein I antibody at 38.5 U/mL, and a lupus anticoagulant ratio of 1.63%. The low molecular weight heparin regimen was adjusted to Fondaparinux (2.5 mg, Q36h) and Enoxaparin Calcium (4100 U, qd). Routine monitoring of fetal growth and development throughout the pregnancy has shown normal trends (Figure 2). At 34 weeks of gestation, blood pressure increased, reaching a maximum of 150/102 mmHg, with urine protein monitored as negative. Labetalol (100 mg, qid) was added until delivery, and low molecular weight heparin calcium (4100 U, qd) and fondaparinux sodium (2.5 mg, qd) were adjusted until 24 hours before delivery. At 36 weeks, a male infant was delivered by cesarean section, with a birth weight of 3250g and an Apgar score of 10. Postpartum, prednisone, hydroxychloroquine sulfate, and low molecular weight heparin calcium were continued for 42 days. A follow-up abdominal MRI at 42 days postpartum (Figure 3) showed the size and shape of the pancreatic head to be normal,the body and tail were unclear.Multiple heterogeneous lesions with variable signal intensity and restricted diffusion were seen in the retroperitoneum and bilateral adrenal regions. The largest mass (9.8 × 8.0 × 8.6 cm) was in the left adrenal area, compressing the left kidney.
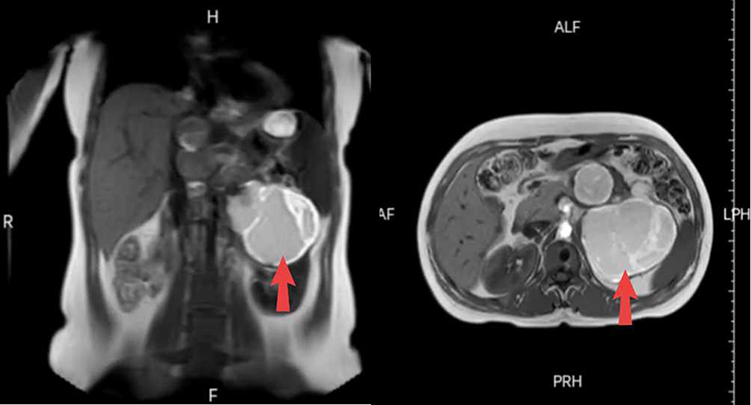 |
Figure 1 Abdominal Magnetic Resonance Imaging (Mid-Pregnancy): Multiple cystic-solid mass shadows are observed in the tail of the pancreas, the left adrenal region, within the liver parenchyma, at the hepatic hilum, along the greater curvature of the stomach, and in the left subphrenic space, with the largest mass measuring approximately 9.2×8.5 cm. The red arrow indicates the location of the largest mass. |
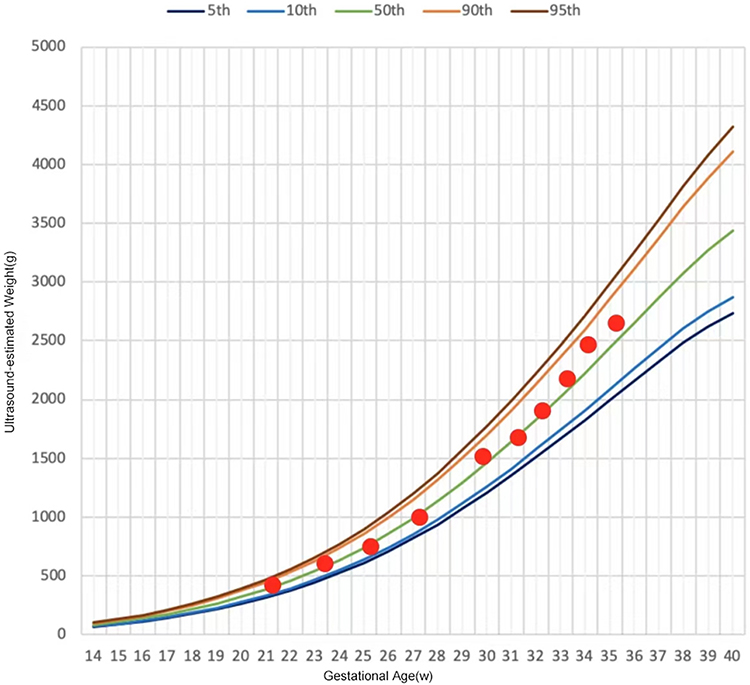 |
Figure 2 Estimated fetal weight growth trend throughout pregnancy as assessed by ultrasound, generated using the Yunsuan application. |
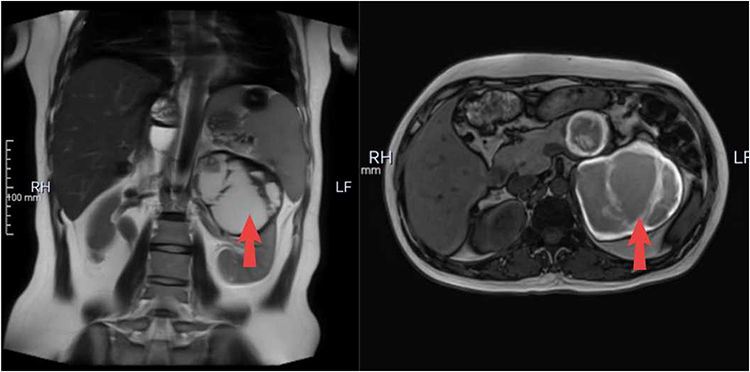 |
Figure 3 Abdominal MRI (Postpartum): The body and tail of the pancreas are poorly visualized. Multiple mixed signals of varying sizes are observed in the local, retroperitoneal, and bilateral adrenal regions, with heterogeneous signals and partial diffusion restriction. The largest lesion is located in the left adrenal region (measuring approximately 9.8 × 8.0×8.6 cm, marked by a red arrow), exhibiting well-defined margins. The left kidney is significantly compressed. |
Discussion
Solid pseudopapillary neoplasm (SPN) of the pancreas accounts for 1% to 2% of all exocrine pancreatic tumors. These lesions are commonly found in young females, with a male-to-female ratio of 1:10, predominantly occurring in individuals in their 20s and 30s.8–10 Due to their malignant potential, with metastasis or local invasion occurring in 10% to 15% of cases, the World Health Organization classifies them as borderline tumors of the exocrine pancreas.3 Furthermore, tumor tissue expresses progesterone receptors, and elevated serum progesterone levels (such as during pregnancy) may stimulate rapid tumor growth11 and increase the risk of tumor rupture during pregnancy.12 Currently, the literature reports that SPN is often discovered during pregnancy, with no cases of planned pregnancies after diagnosis leading to successful deliveries. Surgical resection is the preferred treatment for SPN.13 However, surgical intervention during the first or third trimester may increase the risks of early miscarriage and preterm delivery, respectively. Some experts recommend elective surgical resection during the second trimester to prevent spontaneous tumor rupture and hemorrhage secondary to rapid gestational tumor growth.14 Notably, some case reports demonstrate that SPN may remain stable throughout full-term pregnancy, underscoring the importance of close tumor surveillance combined with shared decision-making regarding surgical timing based on patient preference.15 In this case, the patient was diagnosed at the age of 27 and underwent omentectomy due to extensive metastasis, followed by two cycles of postoperative chemotherapy. She was then followed up every six months, and the disease did not progress post-surgery. The decision regarding the patient’s ability to conceive and the timing of pregnancy was made through multiple multidisciplinary consultations (obstetrics, rheumatology, hepatobiliary surgery, and neonatology) and involved abdominal MRI follow-ups for tumor changes during the pre-pregnancy, mid-pregnancy, and postpartum periods.
In addition to having an SPN, this patient was found to be positive for aPLs during the screening for causes of recurrent miscarriage. Since the relevant tests were conducted for the first time seven years after the discovery of the tumor, it is impossible to determine whether there is a correlation between the occurrence of SPN and APS. However, the relationship between tumors and aPLs has been studied for many years, with numerous studies reporting elevated aPLs levels and the occurrence of APS in various malignancies.16–18 A hypothesis proposes that aPLs (antiphospholipid antibodies) are produced by the immune system as a normal response to tumor antigens.19 A prospective cohort study of cancer patients in Brazil (n=95; 79% solid tumors and 21% hematological malignancies) detected lupus anticoagulant (LA) and anti-β2-GPI in 61% and 32% of patients, respectively.20 A meta-analysis indicates that solid tumors are associated with an elevated risk of producing antiphospholipid antibodies (aPLs), with gastrointestinal tumors, breast cancer, and lung cancer exhibiting the highest risk. Simultaneously, these aPLs may exacerbate pre-existing thrombosis risks in cancer patients.21 However, no reported cases exist of patients with solid pseudopapillary tumors of the pancreas exhibiting elevated aPLs levels.
The presence of aPLs in the patient can promote thrombosis, induce inflammatory responses, activate complement, and affect placental function through abnormal immune reactions and a hypercoagulable state, thereby impacting the development of the embryo and leading to pregnancy loss and complications such as preeclampsia, placental abruption, and fetal growth restriction.22 Although the first five pregnancy losses in this patient were not subjected to etiological screening, clinical manifestations strongly suggest that they were recurrent miscarriages caused by APS.
After identifying the causes of recurrent miscarriage, we implemented targeted treatment. First, we conducted immunotherapy in conjunction with the rheumatology and immunology department. Following stable control of aPLs, ovulation monitoring was performed, and anticoagulant therapy with fondaparinux sodium was initiated immediately after ovulation, with the addition of aspirin for antiplatelet therapy at 11 weeks of gestation. Anticoagulation therapy is the cornerstone of management during pregnancy and the postpartum period for patients with APS. Patients must be closely monitored and receive effective prevention and treatment to reduce the risk of venous thromboembolism. The combination of low molecular weight heparin (LMWH) and low-dose aspirin (LDA) is currently the most commonly used treatment regimen during pregnancy for APS,7 effectively reducing the risk of pregnancy loss and improving pregnancy outcomes.5 However, considering the risks of tumor rupture and bleeding during pregnancy, we initially chose fondaparinux sodium for anticoagulation therapy. Simultaneously, given the potential risk of preterm birth, we administered two rounds of fetal lung maturity treatment at appropriate gestational weeks. Despite aggressive treatment, the patient experienced elevated blood pressure at 34 weeks of gestation; fortunately, blood pressure remained stable without affecting other organs. After comprehensive consideration, a cesarean section was performed to terminate the pregnancy at 36 weeks.
In summary, patients with solid pseudopapillary neoplasm of the pancreas may consider pregnancy during periods of disease stability, with attention needed on the tumor’s growth rate during pregnancy. For patients with high-titer refractory conditions, immunosuppressive therapy should be initiated before pregnancy, and conception should be planned after controlling antiphospholipid antibody levels. The combination of LDA and LMWH is a key measure to improve pregnancy outcomes in patients with OAPS, and during pregnancy, it is crucial to balance the risks of anticoagulation and tumor bleeding.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Weifang People’s Hospital (Approval No.: KYLL20250724-1). All data were collected from the electronic medical record system in the department of Obstetrics Medicine Center. Data were anonymized and de-identified before analysis. In accordance with Weifang People’s Hospital policy, additional ethical approval was not required for publishing anonymized case details. Informed consent was obtained from the patient for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the 2025 project of Weifang Municipal Health Commission, Shandong Province, China (WFWSJK-2025-045).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Law JK, Ahmed A, Singh VK, et al. A systematic review of solid-pseudopapillary neoplasms: are these rare lesions? Pancreas. 2014;43(3):331–337. doi:10.1097/MPA.0000000000000061
2. Yepuri N, Naous R, Meier AH, et al. A systematic review and meta-analysis of predictors of recurrence in patients with solid pseudopapillary tumors of the pancreas. HPB. 2020;22(1):12–19. doi:10.1016/j.hpb.2019.06.005
3. Liu Q, Dai M, Guo J, et al. Long-term survival, quality of life, and molecular features of the patients with solid pseudopapillary neoplasm of the pancreas: a retrospective study of 454 cases. Ann Surg. 2023;278(6):1009–1017. doi:10.1097/SLA.0000000000005842
4. Naik RKH, Amudhan A, Ashokkumar A, et al. Solid pseudopapillary epithelial neoplasm of pancreas in pregnancy: a case report and review of literature. Ann Hepatobiliary Pancreat Surg. 2024;28(1):92–98. doi:10.14701/ahbps.23-083
5. Knight JS, Branch DW, Ortel TL. Antiphospholipid syndrome: advances in diagnosis, pathogenesis, and management. BMJ. 2023;380:e069717. doi:10.1136/bmj-2021-069717
6. Barbhaiya M, Zuily S, Naden R, et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheumatic Dis. 2023;82(10):1258–1270. doi:10.1136/ard-2023-224609
7. Alijotas-Reig J, Esteve-Valverde E, Anunciación-Llunell A, et al. Pathogenesis, diagnosis and management of obstetric antiphospholipid syndrome: a comprehensive review. J Clin Med. 2022;11(3):675. doi:10.3390/jcm11030675
8. Burk KS, Knipp D, Sahani DV. Cystic pancreatic tumors. Magn Reson Imaging Clin N Am. 2018;26(3):405–420. doi:10.1016/j.mric.2018.03.006
9. Kumar NAN, Bhandare MS, Chaudhari V, et al. Analysis of 50 cases of solid pseudopapillary tumor of pancreas: aggressive surgical resection provides excellent outcomes. Eur J Surg Oncol. 2019;45(2):187–191. doi:10.1016/j.ejso.2018.08.027
10. Tan HL, Syn N, Goh BKP. Systematic review and meta-analysis of minimally invasive pancreatectomies for solid pseudopapillary neoplasms of the pancreas. Pancreas. 2019;48(10):1334–1342. doi:10.1097/MPA.0000000000001426
11. Fu C, Li X, Wang Y, et al. Solid pseudopapillary neoplasm of the pancreas: a retrospective study of 195 cases. Front Oncol. 2024;14:1349282. doi:10.3389/fonc.2024.1349282
12. Huang SC, Wu TH, Chen CC, et al. Spontaneous rupture of solid pseudopapillary neoplasm of the pancreas during pregnancy. Obstetrics Gynecol. 2013;121(2 Pt 2 Suppl 1):486–488. doi:10.1097/AOG.0b013e31826d292f
13. Lubezky N, Papoulas M, Lessing Y, et al. Solid pseudopapillary neoplasm of the pancreas: management and long-term outcome. Eur J Surg Oncol. 2017;43(6):1056–1060. doi:10.1016/j.ejso.2017.02.001
14. Huang TT, Zhu J, Zhou H, et al. Solid pseudopapillary neoplasm of pancreas in pregnancy treated with tumor enucleation: case report and review of the literature. Niger J Clin Pract. 2018;21(9):1234–1237. doi:10.4103/njcp.njcp_39_18
15. Yu Y, Teng L, Liu J, et al. Pregnancy complicated with a giant pancreatic tumor and decompensation of liver cirrhosis: a case report and literature review. Matern Fetal Med. 2024;6(1):50–53. doi:10.1097/FM9.0000000000000168
16. Bairey O, Blickstein D, Monselise Y, et al. Antiphospholipid antibodies may be a new prognostic parameter in aggressive non-hodgkin’s lymphoma. Eur J Haematol. 2006;76(5):384–391. doi:10.1111/j.1600-0609.2005.00620.x
17. Gómez-Puerta JA, Cervera R, Espinosa G, et al. Antiphospholipid antibodies associated with malignancies: clinical and pathological characteristics of 120 patients. Semin Arthritis Rheumatism. 2006;35(5):322–332. doi:10.1016/j.semarthrit.2005.07.003
18. Pugliese L, Bernardini I, Pacifico E, et al. Antiphospholipid antibodies in patients with cancer. Inter J Immuno Pharmacol. 2006;19(4):879–888. doi:10.1177/039463200601900417
19. Miesbach W. Antiphospholipid antibodies and antiphospholipid syndrome in patients with malignancies: features, incidence, identification, and treatment. Semin Thromb Hemost. 2008;34(3):282–285. doi:10.1055/s-0028-1082272
20. Vassalo J, Spector N, de Meis E, et al. Antiphospholipid antibodies in critically ill patients with cancer: a prospective cohort study. J Crit Care. 2014;29(4):533–538. doi:10.1016/j.jcrc.2014.02.005
21. Abdel-Wahab N, Tayar JH, Fa’ak F, et al. Systematic review of observational studies reporting antiphospholipid antibodies in patients with solid tumors. Blood Adv. 2020;4(8):1746–1755. doi:10.1182/bloodadvances.2020001557
22. Killian M, van Mens TE. Risk of thrombosis, pregnancy morbidity or death in antiphospholipid syndrome. Front Cardiovasc Med. 2022;9:852777. doi:10.3389/fcvm.2022.852777
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Coexistence of Congenital Dysfibrinogenemia and Antiphospholipid Syndrome in Pregnancy: A Case Report
Wang Z, Mao S, Wang S, Zhang W, Jia C, Zhu T
International Journal of Women's Health 2025, 17:2885-2890
Published Date: 4 September 2025
Solid Pseudopapillary Neoplasms of the Pancreas with Delayed Ovarian Metastasis During Pregnancy: A Case Report and Literature Review
Jie R, Dai X, Lei H, Peng F
International Journal of Women's Health 2026, 18:575652
Published Date: 11 April 2026