Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Soft Tissue Cephalometric Norms in Emirati Population: A Cross-Sectional Study
Authors Abutayyem H ![]() , Alshamsi A, Quadri MFA
, Alshamsi A, Quadri MFA ![]()
Received 19 August 2021
Accepted for publication 30 September 2021
Published 13 October 2021 Volume 2021:14 Pages 2863—2869
DOI https://doi.org/10.2147/JMDH.S334971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Huda Abutayyem,1 Amna Alshamsi,2 Mir Faeq Ali Quadri3
1Department of Orthodontics, College of Dental Sciences, Ras Al Khaimah University, Ras Al Khaimah, United Arab Emirates; 2Al Qassimi Hospital, Ministry of Health, Ras Al Khaimah, United Arab Emirates; 3Department of Preventive Dental Sciences, College of Dentistry, Jazan University, Jazan City, Kingdom of Saudi Arabia
Correspondence: Mir Faeq Ali Quadri
Department of Preventive Dental Sciences, College of Dentistry, Jazan University, PO Box: 114, Jazan City, Kingdom of Saudi Arabia
Email [email protected]
Introduction: The current study is the first to present the cephalometric norms in Emirati adults and aimed to investigate the differences in the angular and linear soft tissue cephalometric measures between male and female Emirati adults.
Methods: A group of 176 individuals (91 males and 85 females) with normal occlusion, proportional facial profiles were chosen, and lateral cephalograms were obtained. Standard values of 16 soft-tissue measurements were determined. Descriptive statistics were first carried out for each parameter. The Student’s t-test was then performed to determine significant differences between male and female measurement means. Significant differences were determined at the 95% probability level.
Results: Soft tissue measurements showed that men had a greater soft tissue profile and H-angle than women. A significant difference between the genders was observed for all linear soft tissue measurements except for the lower lip to E-plane, N’-Sn’ and Sn’-Stomion/Sn-Me ratio measurements. The lengths and thicknesses of the upper and lower lips independently, protrusion of both upper and lower lips, Sn’-Me’ (mm) and N’-Sn’/Sn’-Me’ (%) were found to be significantly different (p < 0.001) and so were the upper lip to E-plane (mm) and the soft tissue thickness of the chin measurements (p < 0.05). Except for upper and lower lip protrusion dimensions and the N’-Sn’/Sn’-Me’ (%), men presented with greater linear measurements.
Conclusion: The differences in soft-tissue cephalometric norms between men and women were established, suggesting that the orthodontist must individualize therapy using local norms as the reference.
Keywords: linear and angular measures, cephalometry, cephalometric measures, Emirates, Arab, orthodontic treatment
Introduction
Facial attractiveness is an inadequately defined perception, difficult to enumerate and linked to cultural preferences. Structural and other aspects of human facial appearance such as facial harmony, synchronization, and balance or equilibrium are best determined by the facial skeleton and its overlying soft tissue framework.1 In orthodontic treatment, harmonious facial esthetics and functional occlusion have long been recognized as two of the most important goals. Broadbent2 and Hofrath3 from the United States and Germany, respectively, were the first to present cephalometry in 1931, and since then, it has become one of the most reliable and reproducible diagnostic modalities in orthodontic practice.4 Standardized cephalometric analysis is used to obtain realistic guiding principles in orthodontic diagnosis and therapeutic scheduling, in addition to the evaluation of the patients’ skeletal, dental and soft tissue patterns linked to their ethnic groups.5,6
Orthodontists need to become more aware of cephalometric norms of each ethnic group before starting with any type of orthodontic treatment, as it has been reported that norms specific to one group cannot always be applied to another group. Therefore, many research studies have been carried out to set up standardized cephalometric values for patients belonging to different ethnicities including but not limited to the Caucasians, European-Americans,6,7 African-Americans,8,9 Mexican & Puerto-Rican Americans,10,11 the Japanese,12,13 the Chinese,14 the Turkish15,16 and the Indians.17
Bishara et al18 reported that most Egyptian adolescent measurements were similar to North American norms, while Sarhan et al,19 Hassan et al20 and Al-Jasser et al21 reported that Saudis preferred greater proclination and protrusion of incisors in contrast to a group of North Americans and Caucasians, respectively. In addition, Sarhan and Hassan found Saudi adult men to exhibit more prognathism with bimaxillary skeletal retrusion when compared to Saudi adult women.19 Hamdan and Rock22 found a difference in the cephalometric norms between Jordanian and the Caucasians in relation to the Eastman standards, where Jordanian subjects were reported to be present with incisor protrusion.
When comparing soft tissue cephalometric norms of distinct ethnic groups, differences in clinical implication have been revealed, predominantly in size and position of the nose, prominence and curvature of the lips, thicknesses of soft tissues covering the chin and the length of the lips among other parameters. Using the Holdaway soft tissue analysis, Al-Gunaid et al23 and Mafi et al24 reported that most Yemeni and Iranian adult measurements were different from white norms, whereas Basciftci et al16 reported similar soft-tissue cephalometric norms between the Turkish and the white.
At present, a great number of young Emirati adults are seeking orthodontic treatment. Very few and inadequate research studies have been conducted focusing on soft tissue cephalometric norms in adults from the United Arab Emirates, necessitating the need to carry out precise and comprehensive research studies on these standards for the population in question. Therefore, the current study is the first to present the cephalometric norms in Emirati adults and to investigate if there are differences in the angular and linear soft tissue cephalometric measures between male and female Emirati adults.
Materials and Methods
Ethical Considerations
The research proposal was reviewed, and ethical approval was granted by the Al Qassimi Hospital Research Ethics Committee, Ministry of Health, the United Arab Emirates (UAE). Written and signed consent was obtained from the study participants before carrying out clinical examinations and data collections. All participants were informed about the purpose of the study, in accordance with the Declaration of Helsinki.
Sample Selection Criteria
Inclusion criteria comprise UAE nationals, age range between 19 and 25 years, having balanced soft-tissue profiles, having Class I molar relationships, presence of permanent dentition only and no history of any previous trauma, any orthodontic or prosthodontic treatment, any maxillofacial or plastic surgery, any congenital facial anomalies, and any systemic diseases affecting dentofacial growth.
Those subjects with facial asymmetry or deformity, presence of deciduous/retained teeth, severe crowding, previous or current orthodontic treatment, evidence of previous trauma or surgery, obvious periodontal disease, or presence of any other pathological conditions were excluded.
Sampling Procedure and Sample Size
The study subjects were recruited using a convenience sampling technique. Patients visiting the Department of Orthodontics, Sharjah Dental Centre, Ministry of Health, Sharjah, UAE, during the study period of January to November 2019 were subjected to the selection criteria. A sample of 176 adult Emiratis (91 males and 85 females) from health centers, high schools and colleges from different areas of the UAE fulfilled the selection criteria and agreed to participate in the study.
The power of the study was calculated using the OpenEpi software to check if the sample size of 176 adult Emiratis (91 males and 85 females) was adequate. With 5% precision and 30% prevalence in the exposed group, and a prevalence coverage ratio of 3, the power was estimated at 91.58%, which is satisfactory for presenting a conclusive finding.
Study Variables
Soft Tissue Cephalometric Study
Lateral cephalometric radiographs were taken for each subject according to the Broadbent method using the Planmeca proline XC system at the Ibn Sina Medical Centre, UAE. For consistency purposes, all the radiographs were taken by the same person, with the same machine, and employing the same method. Dolphin imaging system software package version 10.5 was utilized to perform the digital cephalometric analysis comprising 7 angular and 9 linear measurements (Table 1).
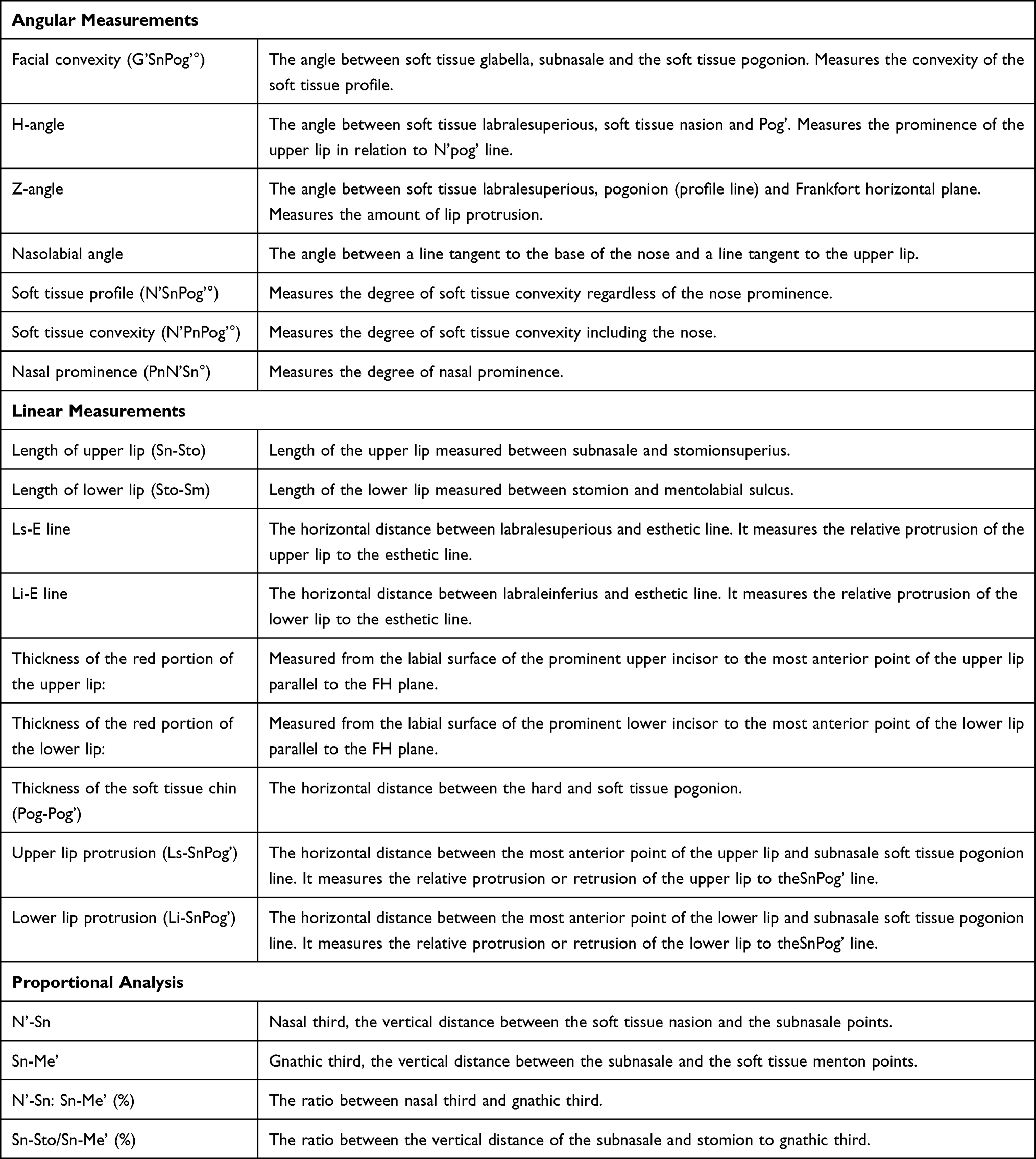 |
Table 1 Soft Tissue Cephalometric Measurements Used in the Study |
All the measurements were performed by one orthodontist (HM) and reviewed twice by two different investigators, and no discrepancies were reported. The analysis was repeated on forty randomly selected cephalometric radiographs after three weeks, and the results were statistically compared using the Dahlberg formula. The intra-operator error ranged from 0.35° to 0.44° for angular measurements and 0.15° to 0.48° for linear measurements. No differences were determined, and intra-operator reliability was deemed satisfactory.
Statistical Analysis
Descriptive statistics were first carried out for each parameter. The Student’s t-test was then performed to determine significant differences between male and female measurement means. Significant differences were determined at the 95% probability level. All statistical analyses were carried out using the Statistical Package for the Social Sciences (SPSS; IBM; USA) version 24.0.
Results
The lateral cephalometric radiographs of the study participants with Class I malocclusion were analyzed to establish a normative database. Descriptive statistics (mean, standard deviation and standard error) of the angular and linear soft tissue measurements in the male and female study participants are shown in Table 2. The significance of the difference between the male and female samples was tested with the Student’s t-test (Table 3). Statistical analysis showed that there were significant differences with all angular soft tissue measurements, by sex except in the nasolabial angle and nose prominence dimensions.
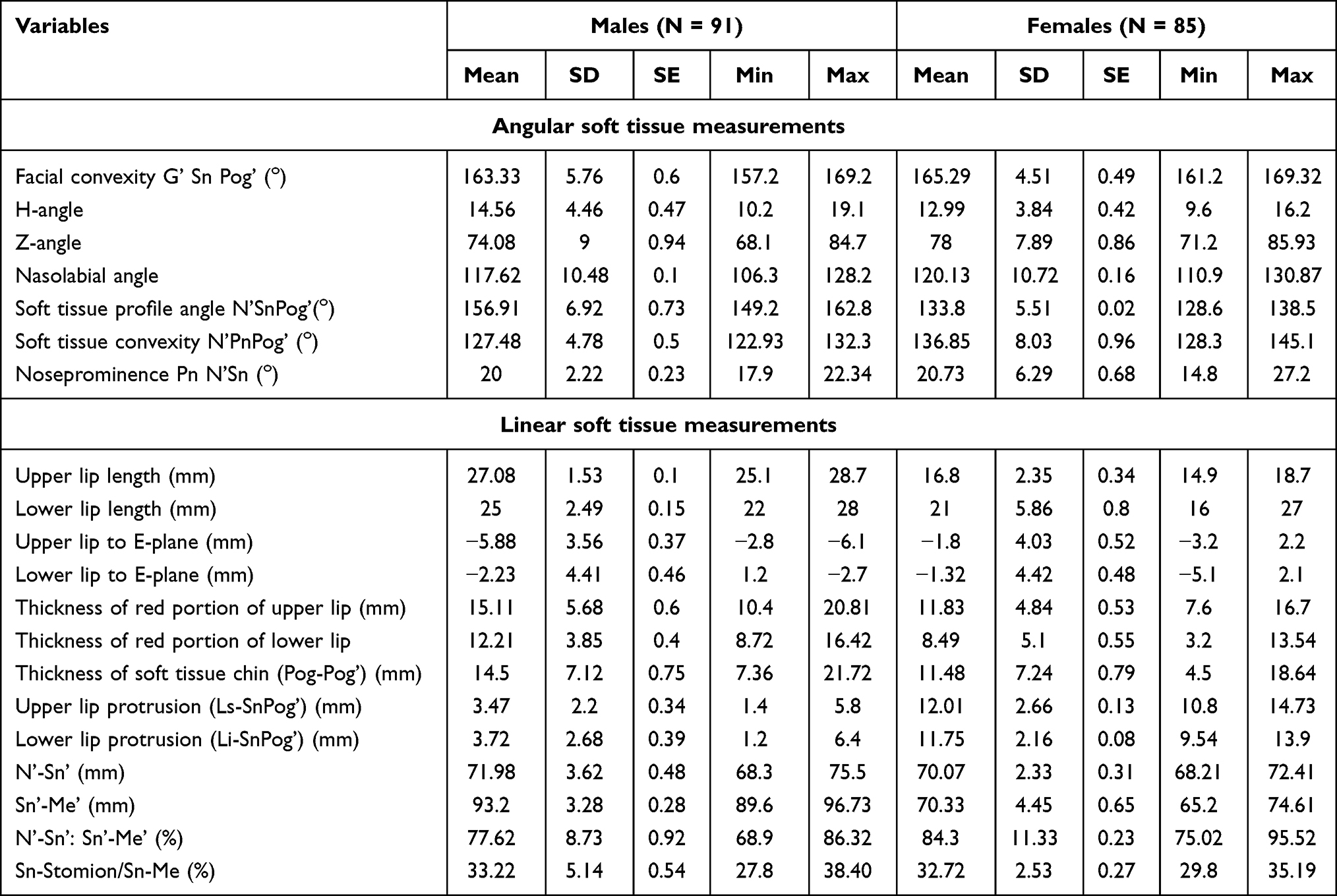 |
Table 2 Descriptive Statistics of Angular and Linear Soft Tissue Measurements in Male and Female Study Participants |
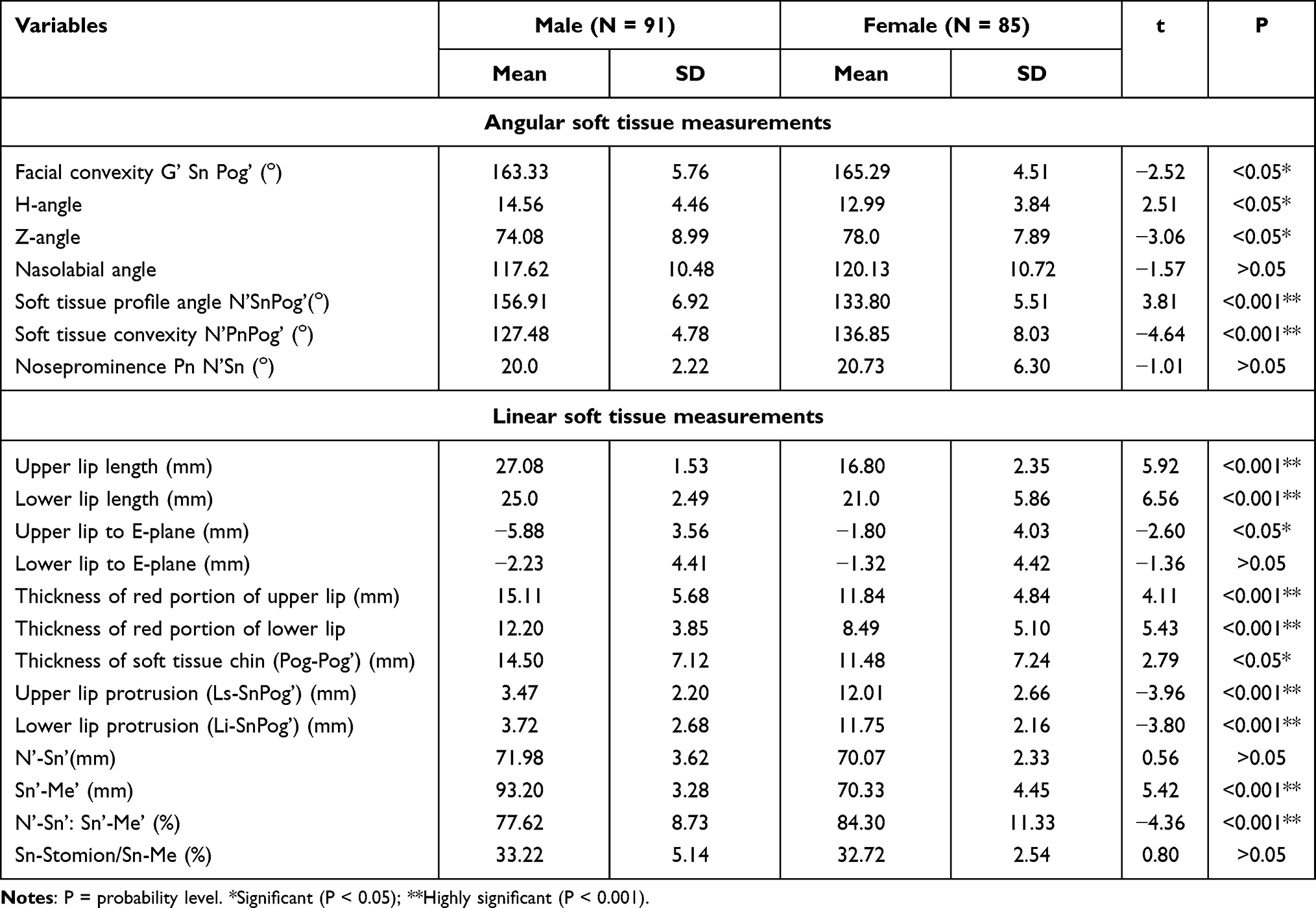 |
Table 3 Comparison of Soft Tissue Cephalometric Angular and Linear Measurements Between Males and Females |
Soft tissue measurements showed that men had a greater soft tissue profile and H-angle than women. The significance of the difference for linear soft tissue measurements between the male and female samples was tested with the Student’s t-test (Table 3). A significant difference by sex was observed for all linear soft tissue measurements except for the lower lip to E-plane, N’-Sn’ and Sn’-Stomion/Sn-Me ratio measurements. The lengths and thicknesses of the upper and lower lips independently, protrusion of both upper and lower lips, Sn’-Me’ (mm) and N’-Sn’/Sn’-Me’ (%) were noted to be statistically significantly different (p < 0.001) and so were the upper lip to E-plane (mm) and the soft tissue thickness of the chin measurements (p < 0.05), except for the upper and lower lip protrusion dimensions and the N’-Sn’/Sn’-Me’ (%).
Discussion
One need was to consider differences in the cephalometric norms between racial and ethnic groups of different populations. Therefore, norms of a definite population may not apply to other ethnic groups necessitating the conduct of studies specific to each ethnicity/group.25,26 Besides, with the increasing number of Emiratis seeking specialized treatment from orthodontists, maxillofacial surgeons, or plastic and reconstructive surgeons, it would be useful to settle on what constitutes a pleasing and esthetic face for this population. The present study aimed to develop cephalometric soft-tissue norms that can assist in orthodontic diagnosis and treatment schedules for young Emirati adult males and females. Facial harmony and esthetics are principally associated with racial preferences. The available norms pertinent to Caucasians/Americans cannot be standardized and applied to other races unless personalized. Comparative research studies have been conducted for different races in various countries. For instance, in East Asia, craniofacial norms are characterized by oblong eyes and small nose, whilst these features may not be acknowledged as norms in other ethnic groups.25,26 Studies carried out on Egyptians,18 Yemenis23 and Indians27 established greater facial convexity in these populations in comparison with the Caucasians. Normative data of normal samples of different ethnic groups is a helpful guide, and identifying the normal range of cephalometric values for a given population is necessary to diagnose abnormalities effortlessly.13
Our findings of soft tissue measurements showed noteworthy differences between the sexes; the mean soft tissue facial angle of men was superior to that of women, suggesting that women have more convex facial profiles. However, Legan and Burstone,28 Scheideman7 and others presented contrasting findings with no significant difference between the sexes. Stark and Epker defined the nasal profile parameters of American men and women on traced cephalograms to establish the normal value of nasal parameters.29 The nose prominence of women (20.73–6.30 mm) in this study was found to be higher than that of men (20–2.29 mm). These findings are not in concurrence with those of Abdel Mageed et al30 and Mohamed et al.31
In our study, males had extra protrusive lips and chin when compared to females. It may be due to the thicker soft-tissue structures in males. This was assured by a p-value <0.05, increased G,Sn’Pog’ as well as H-angle and decreased Z-angle in men. Similar results were reported by Kalha et al32 and Sachan et al33 in the south and north Indian ethnic populations, correspondingly. Using the E-plane as a reference, however, the lips appeared more retrusive in Emirati adult males owing more to the soft tissue chin protrusion rather than the actual procumbence of the lips. Upper and lower lip lengths were significantly higher in men attributing to a greater lower facial height. These findings align with those reported by Abdel Mageed et al,30 Mohamed et al31 and Scheideman et al.7
The differences in soft tissue parameters between different races highlight the importance of defining what is normal for a specific ethnic group. The differences further signify the need for developing distinct sets of values between the sexes. The main benefit of this study is giving standard lateral soft-tissue cephalometric measurements for Emirati adults of both genders helping in diagnosis and treatment planning for orthodontic and surgical decisions and improving post-treatment outcomes.
The above-mentioned differences between diverse races or ethnicities are accredited to genetics, epigenetic and residing in diverse geographical locations. The obtained data in this study emphasize the further need for defining group-specific norms for each population/ethnic population to augment the achievement of orthodontic treatment and attain higher patient satisfaction. Further studies including more assessors of facial profile attractiveness and more subjects, in general, are desirable to explicate the topic.
Conclusion
The present study developed normative soft-tissue cephalometric data for the nationals of the United Arab Emirates, which will assist in diagnosis and management planning. From the findings of the present study, it has been concluded that females possess a more convex facial soft-tissue profile when compared to males, females have more nasal prominence in contrast to males, and males have thicker soft tissue structures than females. The present study is of the view that orthodontic treatment must be individualized with the help of local norms according to sex as the reference rather than using norms established for other ethnic groups.
Data Sharing Statement
The data is available with Huda Abutayyem and will be released on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no conflicts of interest for this work, financial or otherwise.
References
1. AlMansoub YAM, Jubari M, Li A, Jun L, Tang S. Patient’s facial soft tissue changes following the orthodontics treatment. IOSR J Dent Med Sci. 2019;18:69–78.
2. Broadbent BH. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931;1:45–66.
3. Hofrath H. Die bedeutung der roentgenfern der kieferanomalien. Fortschr Orthod. 1931;1:232–248.
4. Athanasiou A. Orthodontic Cephalometry. London: Mosby-Wolfe; 1997.
5. Bishara SE, Jacobsen JR, Hession TJ, Treder JE. Soft tissue profile changes from 5 to 45 years of age. Am J Orthod Dentofacial Orthop. 1998;114(6):698–706. doi:10.1016/S0889-5406(98)70203-3
6. Bishara SE, Fernandez AG. Cephalometric comparisons of the dentofacial relationships of two adolescent populations from Iowa and Northern Mexico. Am J Orthod. 1985;88(4):314–322. doi:10.1016/0002-9416(85)90131-9
7. Scheideman GB, Bell WH, Legan HL, Finn RA, Reisch JS. Cephalometric analysis of dento-facial normals. Am J Orthod. 1980;78(4):404–420. doi:10.1016/0002-9416(80)90021-4
8. Drummond RA. A determination of cephalometric norms for the Negro race. Am J Orthod. 1968;54(9):670–682. doi:10.1016/0002-9416(68)90018-3
9. Fonseca RJ, Klein WD. A cephalometric evaluation of American Negro women. Am J Orthod. 1978;73(2):152–160. doi:10.1016/0002-9416(78)90185-9
10. Swierenga D, Oesterle LG, Messersmith ML. Cephalometric values for adult Mexican Americans. Am J Orthod Dentofacial Orthop. 1994;106(2):146–155. doi:10.1016/S0889-5406(94)70032-X
11. Evanko AM, Freeman K, Cisneros GJ. Mesh diagram analysis: developing a norm for Puerto Rican Americans. Angle Orthod. 1997;67:381–388.
12. Miyajima K, McNamara JA
13. Alcalde RE, Jinno T, Pogrel MA, Matsumura T. Cephalometric norms in Japanese adults. J Oral Maxillofac Surg. 1998;56(2):129–134. doi:10.1016/S0278-2391(98)90849-7
14. Yen PKJ. The facial configuration in a sample of Chinese males. Angle Orthod. 1973;43:301–304.
15. Erbay EF, Canikliog ̆lu CM, Erbay SK. Soft tissue profile in Anatolian Turkish adults: part I. Evaluating of horizontal lip position using different soft tissue analyses. Am J Orthod Dentofacial Orthop. 2002;121(1):57–64. doi:10.1067/mod.2002.119780
16. Basciftci FA, Uysal T, Buyukerkmen A. Determination of Holdaway soft tissue norms in Anatolian Turkish adults. Am J Orthod Dentofacial Orthop. 2003;123(4):395–400. doi:10.1067/mod.2003.139
17. Nanda R, Nanda RS. Cephalometric study of the dentofacial complex of North Indians. Angle Orthod. 1969;39:22–28.
18. Bishara SE, Abdullah EM, Hoppens BJ. Cephalometric comparisons of dentofacial parameters between Egyptian and North American adolescents. Am J Orthod Dent Orthop. 1990;97(5):413–421. doi:10.1016/0889-5406(90)70113-Q
19. Sarhan OA, Nashashibi IA. A comparative study between two randomly selected samples from which to derive standards for craniofacial measurements. J Oral Rehabil. 1988;15(3):251–255. doi:10.1111/j.1365-2842.1988.tb00154.x
20. Hassan AH. Cephalometric norms for the Saudi children living in the western region of Saudi Arabia: a research report. Head Face Med. 2005;24:1–5.
21. Al-Jasser NM. Cephalometric evaluation of craniofacial variation in normal Saudi population according to Steiner analysis. Saudi Med J. 2000;21:746–750.
22. Hamdan AM, Rock WP. Cephalometric norms in an Arabic population. J Orthod. 2001;28(4):297–300. doi:10.1093/ortho/28.4.297
23. Al-Gunaid T, Yamada K, Yamaki M, Saito I. Soft tissue cephalometric norms in Yemeni men. Am J Orthod Dent Orthop. 2007;132:e7–14.
24. Mafi P, Ghazisaeidi MR, Mafi A. Ideal soft tissue facial profile in Iranian females. J Craniofac Surg. 2005;16(3):508–511. doi:10.1097/01.scs.0000171971.21808.d1
25. Azarbayejani S, Omrani A, Kalaantar- Motamedi A, Abdellahi M, Taalebi V, Teimoori F. Cephalometric norms for 6–17 year-old Iranians with normal occlusion and well-balanced faces. Dent Res J. 2014;11:327–335.
26. Jacobson A, Jacobson R. Radiographic Cephalometry from Basic to 3-D Imaging. Quintessence Pub Co; 2006:205–216.
27. Jain P, Kalra JP. Soft tissue cephalometric norms for a North Indian population group using Legan and Burstone analysis. Int J Oral Maxillofac Surg. 2011;40(3):255–259. doi:10.1016/j.ijom.2010.09.011
28. Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg. 1980;38:744–751.
29. Stark A, Epker BN. Cephalometric analysis of profile nasal aesthetics. Part 1: methods and normative data. Int J Adult Orthodon Orthognath Surg. 1996;11:91–103.
30. Abdelmageed HA. A cephalometric study of soft tissue profile in relation to the hard tissue in a group of Egyptian adults. Egypt: Faculty of oral and dental medicine, Cairo University; 1989.
31. Mohammad AMQ. Lateral cephalometric norms for a sample of Jordanian adults. Egypt: Cairo University; 2003.
32. Kalha AS, Latif A, Govardhan SN. Soft-tissue cephalometric norms in a South Indian ethnic population. Am J Orthod Dentofacial Orthop. 2008;133(6):876–881. doi:10.1016/j.ajodo.2006.05.043
33. Sachan A, Srivastav A, Chaturvedi TP. Soft-tissue cephalometric norms in a north Indian ethnic population. J Orthod Sci. 2012;1(4):92–97. doi:10.4103/2278-0203.105877
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.