Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Socioeconomic Inequality in Knowledge About HIV and Its Contributing Factors Among Women of Reproductive Age in Sub-Saharan Africa: A Multicountry and Decomposition Analysis
Authors Teshale AB ![]() , Tesema GA
, Tesema GA ![]()
Received 20 November 2022
Accepted for publication 24 February 2023
Published 1 March 2023 Volume 2023:15 Pages 53—62
DOI https://doi.org/10.2147/HIV.S392548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Achamyeleh Birhanu Teshale, Getayeneh Antehunegn Tesema
Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Achamyeleh Birhanu Teshale, Email [email protected]
Aim: To examine the socioeconomic inequality in knowledge about HIV and its contributing factors among women of reproductive age in sub-Saharan Africa.
Methods: We have used the most recent demographic and health survey data of the 15 sub-Saharan African countries. 204,495 women of reproductive age made up the entire weighted sample. Erreygers normalized concentration index (ECI) was utilized to evaluate socioeconomic inequality in knowledge about HIV. The variables that contributed to the observed socioeconomic inequality were determined using decomposition analysis.
Results: We found the pro-rich inequality in knowledge about HIV (the weighted ECI was 0.16 with a Standard error = 0.007 and P value< 0.001). The decomposition analysis indicated that educational status (46.10%), wealth status (30.85%), listening to the radio (21.73%), and reading newspapers (7.05%) were among the contributors to the pro-rich socioeconomic inequalities in knowledge about HIV.
Conclusion: Having knowledge about HIV is concentrated among rich reproductive-age women. Educational status, wealth status, and media exposure were the major contributors and should be a priority for interventions to reduce the inequality in knowledge about HIV.
Keywords: socioeconomic inequality, concentration index, decomposition analysis, comprehensive knowledge, HIV/AIDS, sub-Saharan Africa
Background
Until now, 74.9 million people are living with the human immunodeficiency virus (HIV) and 32 million people have died of AIDS-related illnesses.1 In 2021, over 1.5 million individuals acquired HIV, and 650000 people died from HIV-related causes, making HIV an ongoing and serious public health issue.2 The majority of people who have HIV are in low- and middle-income nations, with 68% of them thought to be in sub-Saharan Africa.1,3
Unprotected sexual intercourse is the main source of HIV infection and women are vulnerable because they may be afraid to say no to sex or to insist that their partner use a condom. Besides, during heterosexual intercourse, women are usually more exposed to bodily fluids than their male partners. Therefore HIV infection is a concern for women of reproductive age everywhere, and only 30% of these women are fully informed about HIV.4 Besides, a potential obstacle to the achievement of the 2030 Sustainable Development Goal 3, which is promoting well-being and ensuring healthy lives for everyone, regardless of age, is the HIV pandemic.5–9
Lower knowledge about HIV is associated with an alarming increase in new infections, and intervening this is pivotal in combating the epidemic.10–12 According to findings from different studies, education, wealth status, residence, sex of the family’s head, and media exposure are some of the factors that are associated with knowledge about HIV.10,13–17 Our previous study also identified different individual and community level factors that affect knowledge about HIV and, of these, wealth is one of the individual level factors.17 In addition, studies in Malawi revealed that knowledge about HIV is concentrated among individuals with good socioeconomic status.18,19
However, except for the above-mentioned research in Malawi, we are unaware of any study that has been done in Africa that assess the socioeconomic inequality (SEI) using concentration index (CI) and the contributing factors involved using a decomposition analysis at the Sub-Saharan African level. Therefore, we aimed to investigate the SEI in knowledge about HIV among women of reproductive age in sub-Saharan Africa. The finding will help policymakers to set appropriate interventions since it quantifies both the extent of SEI in knowledge about HIV and the factors involved for such socioeconomic inequality.
Methods
Data Source and Variable Measurement
We used the most recent Demographic and Health Surveys (DHS) data gathered in Sub-Saharan African nations between 2015 and 2020. The detailed information such as the data source, population, and sampling technique are found in our previous publication.17 Besides, Further information about DHS data is found elsewhere.20 For this study, there were 19 countries with their most recent DHS conducted in the study period (2015 to 2020). However, the DHS data of the four nations; Angola, Tanzania, South Africa, and Senegal, did not have information about the outcome variable. Therefore, for this study, we used the 15 countries DHS data (Table 1). Knowledge about HIV was the outcome variable (binary outcome variable; Yes/No). How the outcome was measured is found in our previous publication.17
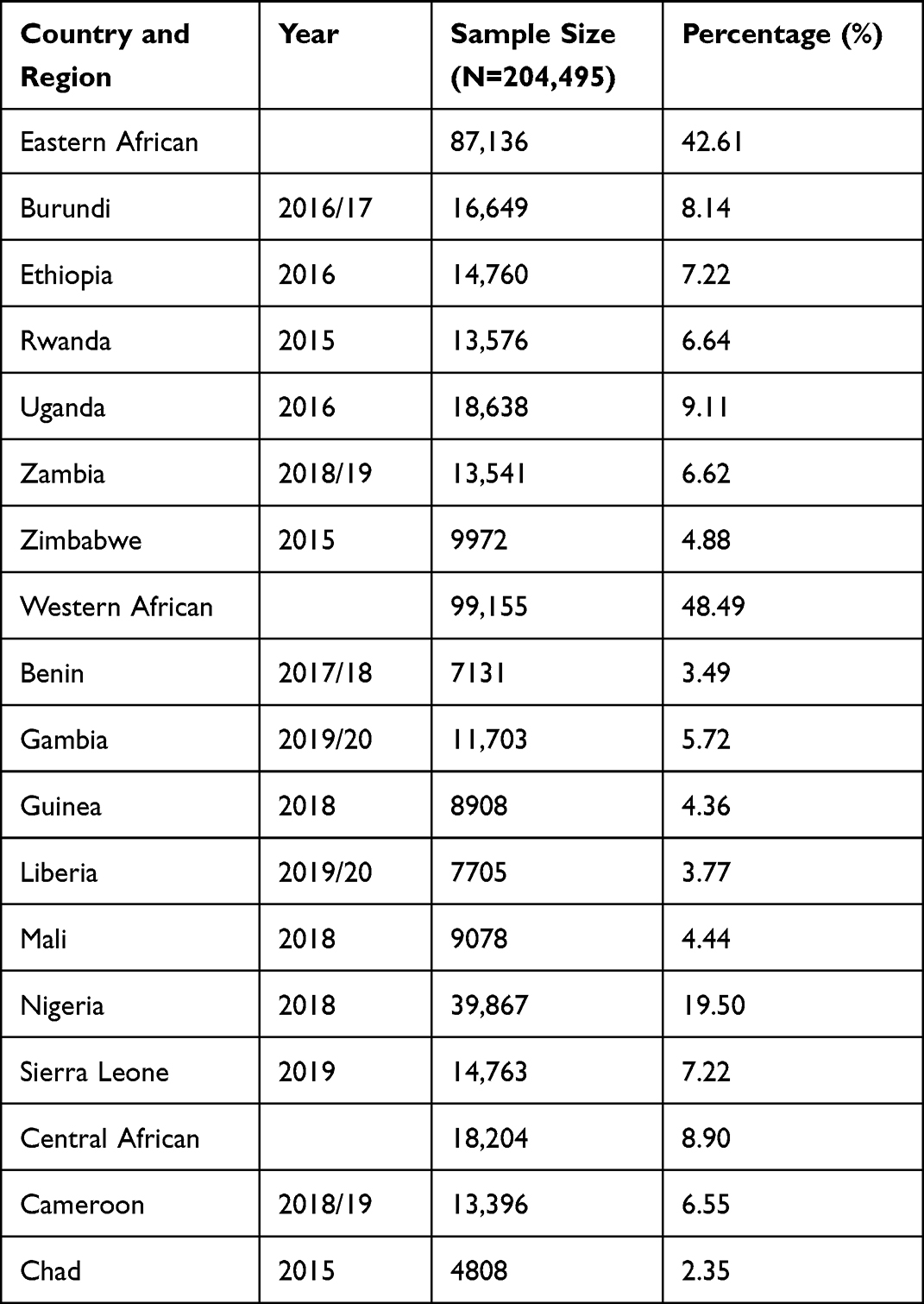 |
Table 1 Sample Size and Years When the DHS Surveys Were Conducted |
Regarding explanatory variables, we searched different literatures including using our previous work13–17,21 and considering their availability in the DHS data; age of the women, marital status, level of educational, wealth index, sex of household head, contraceptive utilization, exposure to media (whether a woman listens to the radio, watches television, and reads a newspaper or magazine at least once a week or not), and place of residence were incorporated as explanatory variables.
The wealth index is used in this study to quantify household socioeconomic status and is also used as a measure of permanent income in DHS data sets. The wealth index is created from the DHS data using principal component methods and is used as a socioeconomic status indicator for international comparison.22–25
Data Management and Statistical Analysis
Extracting, recoding, and analyzing of the data were conducted using Stata version 16 software. The study was based on weighting and since it is a pooled data analysis, the standard weighting variable v005 was rescaled by dividing total reproductive age women in each country by total interviewed reproductive age women.26
SEI in Knowledge About HIV
We computed the SEI in knowledge about HIV using a CI. The CI, which is a relative measure of inequality, is calculated as two times the area of the concentration curve and the 45-degree line (the line of equality). Additionally, CI can be defined as the covariance between the rank of the living standards variable (in our case, wealth index) and the health variable (in our case, knowledge about HIV).24 That means:

Where CI is the concentration index, μ is the mean of the health variable (proportion of knowledge about HIV), h is the health variable (knowledge about HIV), and r is the cumulative percentage that each woman represents over the total population after ranking knowledge about HIV by the wealth index.
Besides, while assessing the socioeconomic inequality, a health variable can be bounded or unbounded. The CI ranges between − 1 and 1 for unbounded variable and from μ − 1 to 1 − μ for bounded variables.27 For knowledge about HIV, which is a bounded variable, an Erreygers CI (ECI), a modified version of the normal CI, was used to measure its SEI.27,28 ECI can be mathematically defined as:28

Where CI (y) is the generalized CI that is explained in the previous formula and μ is the mean knowledge about HIV.
Finally, the concentration curve that demonstrates the cumulative percentage of knowledge about HIV and women ranked by the wealth index on the y-axis and x-axis, respectively, was reported. In the assessment of SEI of knowledge about HIV, if ECI is zero then there is no SEI. This means, regardless of wealth status, everyone has the same value of knowledge about HIV, and its concentration curve lies at a 45-degree line (that is the line of equality). However, when it is above the line of equality (meaning when the ECI takes a negative value) having knowledge about HIV is favoring the poor (pro-poor). If the ECI is positive, the curve lie below the line of equality and this means having knowledge about HIV is favoring the rich (pro-rich).24,29 Generally, the further the concentration curve is from the diagonal line, the greater the degree of inequality in knowledge about HIV.29 We have also tested the statistically significance of the pro-rich or the pro-poor concentration of knowledge about HIV.
Decomposing of the SEI in Knowledge About HIV
Individual contributing factors for the SEI can be assessed based on the Wag staff et al decomposition analyses technique.24,27,29,30 That is, for any linear additive regression model of health outcome (y).24
Where “y” is the SEI of knowledge about HIV,  is its socioeconomic determinants, α represents the intercept,
is its socioeconomic determinants, α represents the intercept,  is the coefficient of
is the coefficient of  , µ is the mean of y,
, µ is the mean of y,  is the mean of
is the mean of  ,
,  is the CI for
is the CI for  ,
,  is the generalized CI for the error term (
is the generalized CI for the error term ( ),
),  is the elasticity of y with respect to
is the elasticity of y with respect to  . The residual (
. The residual ( ) depicts the inequality in knowledge about HIV that cannot be accounted for by systematic differences in income levels in the
) depicts the inequality in knowledge about HIV that cannot be accounted for by systematic differences in income levels in the  , which should be close to zero for a well-defined model.27,30 However, the above equation is a Wagstaff’s equation for decomposing a continuous health outcome using ordinary least square (OLS) regression and there are two methods for the decomposition of a binary health outcome. The first method is based on van Doorslaer’s modification of the above equation using marginal effects from probit analysis.24,31 The second method is the use of the Generalized Linear Model (GLM), which is an extension of the above equation.32 Since GLM preserves both the distribution and the link between the independent and dependent variables and estimates are not depending on the choice of reference groups, it is appropriate for this study.33 Therefore, we have conducted a decomposition analysis using the GLM method, which is a modification of the mathematics above (equation of CI) with binomial family and identity link.
, which should be close to zero for a well-defined model.27,30 However, the above equation is a Wagstaff’s equation for decomposing a continuous health outcome using ordinary least square (OLS) regression and there are two methods for the decomposition of a binary health outcome. The first method is based on van Doorslaer’s modification of the above equation using marginal effects from probit analysis.24,31 The second method is the use of the Generalized Linear Model (GLM), which is an extension of the above equation.32 Since GLM preserves both the distribution and the link between the independent and dependent variables and estimates are not depending on the choice of reference groups, it is appropriate for this study.33 Therefore, we have conducted a decomposition analysis using the GLM method, which is a modification of the mathematics above (equation of CI) with binomial family and identity link.
In the decomposition analysis, for each determinant variable, the coefficient and its significant level, elasticity, ECI, and percent contribution were calculated and reported. Besides, the portion of the inequality in knowledge about HIV that cannot be explained by systematic variation in the explanatory variables was found small.
Results
Study Participant’s General Characteristics
A total of 204, 495 women of reproductive age (weighted sample) were used (Table 1). The overall proportion of having knowledge about HIV in the 15 sub-Saharan Africa countries was 38.54% (95% CI: 38.32, 38.75). As shown in Table 2, a large proportion (around one-half) of women with knowledge about HIV were from the richest households and 63.90% of women with knowledge about HIV had higher education (Table 2).
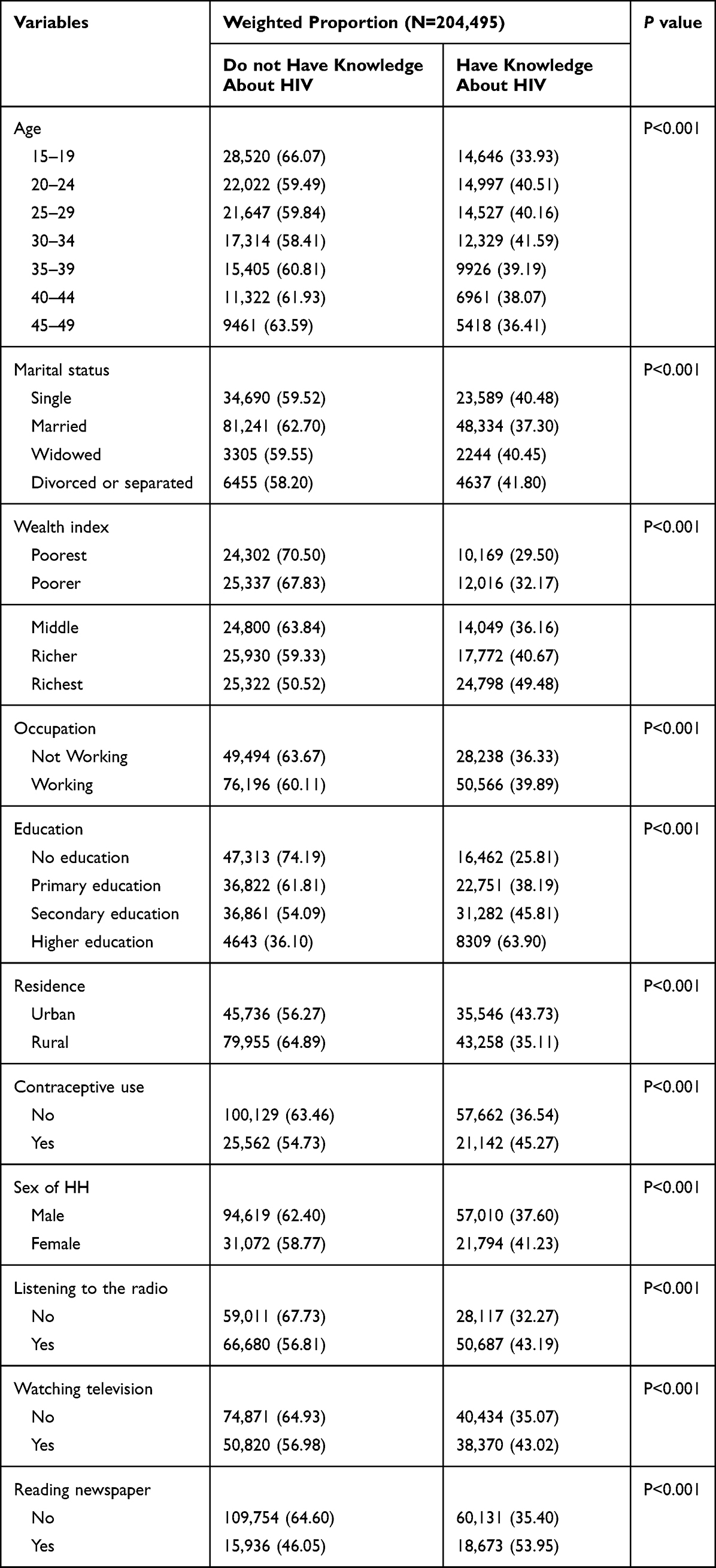 |
Table 2 The Weighted Proportion of Knowledge About HIV per Characteristics of the Study Participants |
SEI of Knowledge About HIV
The weighted ECI for knowledge about HIV was 0.16 with Standard error = 0.007 and P< 0.001 (Figure 1). This revealed that knowledge about HIV favors the rich, pro-rich inequality.
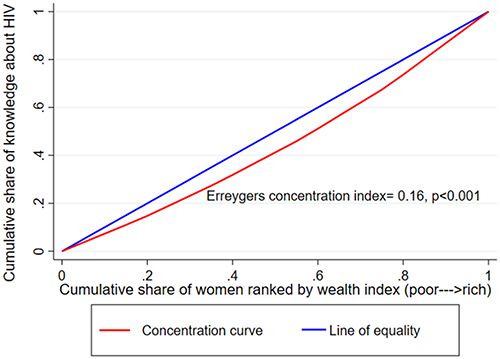 |
Figure 1 Concentration curve for Knowledge about HIV in sub-Saharan Africa. |
Decomposing the SEI in Knowledge About HIV
Table 3 presents findings from the decomposition analysis that showed the contributions of individual determinants to the overall SEI of knowledge about HIV.
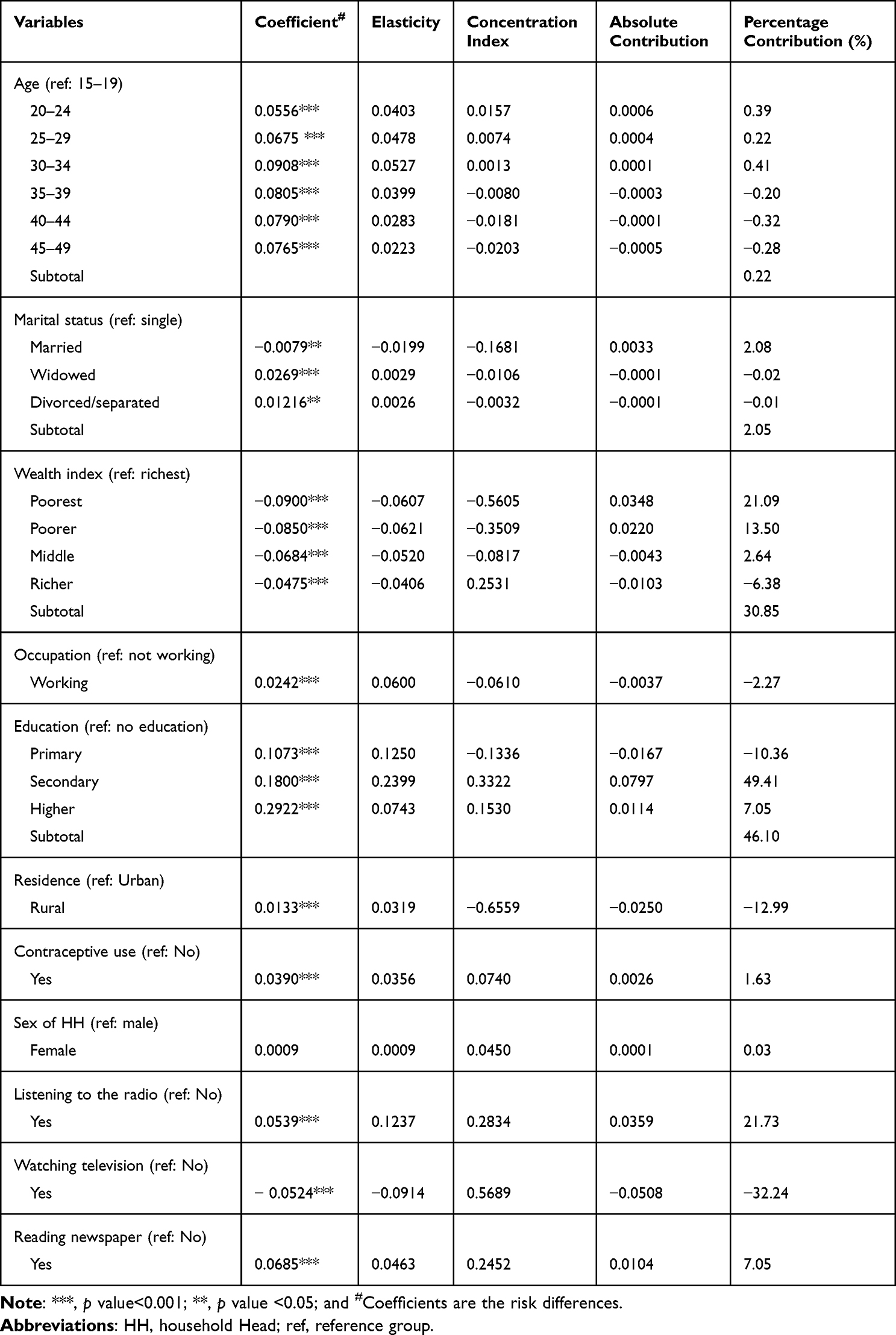 |
Table 3 Determinants of Inequality in Knowledge About HIV in Sub-Saharan Africa |
The coefficients are presented and their level of significance is indicated to show whether knowledge about HIV may increase or decrease per each independent variable. Elasticity was mentioned in this study. It’s a unitless partial association measure that shows the change in SEI that corresponds to a one-unit change in the independent variables. It shows how sensitive SEI is to changes in the explanatory variable. The sign of elasticity, which can be either positive or negative, indicates whether the SEI is expanding or reducing in response to a positive change in the determinant.30,34,35 For instance, a positive sign in elasticity for the variable age indicates a 1% change in women’s age from 15–19 years to an older age will result in an increment of the SEI in knowledge about HIV. A negative sign in elasticity for the variable wealth status revealed that a 1.00% change in women’s wealth status from richest to poorest, poorer, middle, and richer will result in a 6.07%, 6.21%, 5.20%, and 4.06% reduction of the SEI in knowledge about HIV, respectively. Regarding occupational status, a 1.00% change in women working status from not working to working results in a 6.00% increment in socioeconomic inequality. Looking at educational status, a 1.00% change in women’s education from no formal education to primary education, secondary education, and higher education increase SEI in knowledge about HIV by 12.50%, 23.99%, and 7.43%, respectively. A 1.00% change in women’s listening of radio from being listening to not listening increases SEI in knowledge about HIV by 12.37%.
The ECI was calculated for each determinant, and a positive or negative value implies that the determinants of inequality are concentrated among rich or poor households, respectively. For instance, in this study, worker women, women who had primary education, and women who did not watch television had negative ECI and this means these groups of women were more likely to be concentrated among the poor households. In contrast, those who listens to the radio, who used contraceptives, women who had secondary and above education, and who were from female-headed households were more likely to be concentrated in the upper tail of the wealth distribution.
Furthermore, the percentage contribution denotes the relative contribution of each predictor in the model to the overall SEI in knowledge about HIV. A positive percentage contribution suggests a factor that causes the observed SEI to increase, whereas a negative percentage contribution indicates a factor that causes the observed SEI to decrease. In this study, educational status is the major driver of the SEI in knowledge about HIV. Whereas primary education reduces inequality as shown by the negative sign, secondary and higher education contribute positively to the inequality in possession of knowledge about HIV with an overall percent contribution of 46.10%. Wealth status had also a great contribution to the SEI in knowledge about HIV (percentage contribution= 30.85%). The lower wealth quintiles increase the inequality as shown by the positive sign and the upper quintile contributes negatively to the inequality. Listening to radio also contributed to the socioeconomic inequalities in knowledge about HIV, explaining 21.73% of the overall inequality. Factors such as reading newspapers (7.05%), marital status (2.05%), and contraceptive use (1.63%) were also responsible for the observed SEI. The major contributing factor for the reduction of SEI was watching television, 32.24% of the reduction of inequality was explained by being not watching television. Rural residence (−12.99%) and working occupational status (−2.27%) also contribute to the reduction of SEI in knowledge about HIV (Table 3).
Discussion
This study examined the SEI in Knowledge about HIV in Sub-Saharan Africa. In this study, Knowledge about HIV is in favor of women from rich households. This revealed that higher knowledge about HIV is concentrated among the rich. This is in line with a study conducted in Malawi, which revealed that knowledge about HIV is concentrated among wealthier individuals.18,19,36 This could be attributed to socioeconomically disadvantaged women’s inability to access health information, such as HIV/AIDS, and their lack of autonomy in making healthcare decisions. As a result, programs aimed at improving the socioeconomic status of disadvantaged women must be strengthened.
In the decomposition analysis, women’s education, wealth status, media exposure (listening to radio and reading newspaper), marital status, age, and contraceptive use contributes to an increment of the overall SEI in Knowledge about HIV. While watching television, occupation, and residence contributes to the reduction of the overall SEI in Knowledge about HIV.
Consistent with a study in Malawi,19 in this study, educational status had a positive contribution to the overall SEI with an overall percent contribution of 46.10%. Primary education had a negative effect to the SEI. This may be attributed to the fact that primary education is mainly concentrated among the poor (see the negative ECI in Table 3). To put it another way, providing elementary education is critical for closing gaps in comprehensive HIV/AIDS knowledge. Conversely, in this study, secondary education contributes positively to inequality. One possible explanation is that a higher level of education and appropriate knowledge about HIV/AIDS is concentrated among the wealthier.37 The positive ECI in the current study also revealed that secondary and higher education is concentrated among the rich (see Table 3).
Wealth status was also an important determinant of the overall SEI in Knowledge about HIV. It increases the overall SEI by 30.85%. Different studies also found wealth as the single most significant factor influencing disparities in maternal healthcare utilization,38–42 which in turn affect the accessibility of information for sexually transmitted infections such as HIV/AIDS.
The current study also demonstrated that listening radio and reading newspaper are among the contributors to the SEI in Knowledge about HIV. They increase the overall SEI by 21.73% and 7.05%, respectively. This is since watching television and reading newspaper are concentrated among the rich, as indicated by positive ECI (see Table 3). This implies the need to enhance strategies of exposing people to the media to reduce media exposure-related inequalities in terms of knowledge about HIV/AIDS. Watching television was another factor responsible for SEI. Not watching television reduces the overall SEI by 32.24%. This is supported by the negative coefficient, which revealed that being not watching television was associated with a reduction of the Knowledge about HIV.
The study at hand also revealed that working occupation status contributes to the reduction (−2.27%, respectively) of SEI in Knowledge about HIV. This implies occupation should be considered to reduce the SEI in knowledge about HIV/AIDS.
The data used in this study were from 15 sub-Saharan Africa countries (a large sample of population-based surveys) (Table 1). Another strength is the use of a more rigorous decomposition analysis to pinpoint the factors that contribute to SEI in Knowledge about HIV. However, the study has limitations in that it relies on cross-sectional data, which makes it difficult to prove causation. Besides, the selection of variables as key indicators, as well as the assumption that they occur in parallel with no chance of interaction, can be problematic. Wealthier households, for example, may have more access to televisions and radios, and hence may have greater access to knowledge. Furthermore, since the 15 sub-Saharan African countries were used in the pooled data analysis and it was not possible to conduct a distinct analysis for each country, caution should be used when applying the study’s findings.
Conclusion
In this study, knowledge about HIV was concentrated among wealthier reproductive age women (pro-rich inequality of knowledge about HIV) in Sub-Saharan Africa, as revealed by the positive ECI. The decomposition analysis shows that women’s education, wealth status, listening to the radio, and reading newspaper are the main contributors for the inequality.
These identified factors for the SEI should be a priority for interventions to reduce the SEI in Knowledge about HIV. This means, accelerating poverty alleviation programs and generating work opportunities could be one of the most effective ways to lift disadvantaged women out of poverty and reduce SEI. Besides, equal access to education and the media can aid in the reduction of the observed inequality. Moreover, the author recommends the application of low-cost technology to spread messages across all groups with different socioeconomic characteristics.
Abbreviations
DHS, Demographic and Health Survey; ECI, Erreygers Concentration Index; GLM, Generalized Linear Model; HIV, Human Immunodeficiency Virus; OLS, Ordinary Least Square; SEI, Socio Economic Inequality.
Data Sharing Statement
All result-based data are contained within the manuscript. However, everyone can access the data set from the measure DHS Program using the link https://dhsprogram.com.
Ethics Approval and Consent to Participate
The Declaration of Helsinki was considered during the conduct of this study. By logging in and making an online request, we were able to access the data set from the DHS website (https://dhsprogram.com). Additionally, no individual Identifiers were discovered in the data set. Furthermore, because we used openly available data, the Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Ethiopia, Ethical Evaluation Committee decided not to conduct an ethical review of this study.
Acknowledgment
We would like to express our profound gratitude and appreciation to the MEASURE DHS PROGRAM for making the data sets available to us.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Mahy M, Marsh K, Sabin K, Wanyeki I, Daher J, Ghys PD. HIV estimates through 2018: data for decision-making. AIDS. 2019;33(Suppl 3):S203. doi:10.1097/QAD.0000000000002321
2. World Health Organzation. HIV. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
3. Avert. Global hiv and aids statistics; 2019.
4. HIV/AIDS JUNPo. 2008 report on the global AIDS epidemic. Unaids; 2008.
5. Warren CE, Hopkins J, Narasimhan M, Collins L, Askew I, Mayhew SH. Health systems and the SDGs: lessons from a joint HIV and sexual and reproductive health and rights response. Health Policy Plan. 2017;32(Suppl 4):iv102.
6. Assembly G. Sustainable development goals. In: SDGs Transform Our World 2030. UN General Assembly; 2015.
7. Zeng W, Shepard DS, Avila-Figueroa C, Ahn H. Resource needs and gap analysis in achieving universal access to HIV/AIDS services: a data envelopment analysis of 45 countries. Health Policy Plan. 2016;31(5):624–633.
8. McRobie E, Matovu F, Nanyiti A, et al. National responses to global health targets: exploring policy transfer in the context of the UNAIDS ‘90–90–90’treatment targets in Ghana and Uganda. Health Policy Plan. 2018;33(1):17–33.
9. World Health Organisation. 10 facts on HIV/AIDS. Available from: https://www.who.int/features/factfiles/hiv/facts/en/index3.html.
10. Teshome R, Youjie W, Habte E, Kasm N. Comparison and association of comprehensive HIV/AIDS knowledge and attitude towards people living with HIV/AIDS among women aged 15–49 in three east African countries: Burundi, Ethiopia and Kenya. J AIDS Clin Res. 2016;7(4):1–8. doi:10.4172/2155-6113.1000559
11. Oljira L, Berhane Y, Worku A. Assessment of comprehensive HIV/AIDS knowledge level among in‐school adolescents in eastern Ethiopia. J Int AIDS Soc. 2013;16(1):17349. doi:10.7448/IAS.16.1.17349
12. Sohn A, Park S. HIV/AIDS knowledge, stigmatizing attitudes, and related behaviors and factors that affect stigmatizing attitudes against HIV/AIDS among Korean adolescents. Osong Public Health Res Perspect. 2012;3(1):24–30. doi:10.1016/j.phrp.2012.01.004
13. Agegnehu CD, Geremew BM, Sisay MM, et al. Determinants of comprehensive knowledge of HIV/AIDS among reproductive age (15–49 years) women in Ethiopia: further analysis of 2016 Ethiopian demographic and health survey. AIDS Res Ther. 2020;17(1):1–9. doi:10.1186/s12981-020-00305-z
14. Gebremedhin S, Wang Y, Tesfamariam E. Predictors of HIV/AIDS knowledge and attitude among young women of Nigeria and Democratic Republic of Congo: cross-sectional study. J AIDS Clin Res. 2017;8(3):677. doi:10.4172/2155-6113.1000677
15. Fenny AP, Crentsil AO, Asuman D. Determinants and distribution of comprehensive HIV/AIDS knowledge in Ghana. Glob J Health Sci. 2017;9(12):1–32. doi:10.5539/gjhs.v9n12p32
16. Sheikh MT, Uddin MN, Khan JR. A comprehensive analysis of trends and determinants of HIV/AIDS knowledge among the Bangladeshi women based on Bangladesh demographic and health surveys, 2007–2014. Arch Public Health. 2017;75(1):1–11. doi:10.1186/s13690-017-0228-2
17. Teshale AB, Yeshaw Y, Alem AZ, et al. Comprehensive knowledge about HIV/AIDS and associated factors among women of reproductive age in sub-Saharan Africa: a multilevel analysis using the most recent demographic and health survey of each country. BMC Infect Dis. 2022;22(1):130. doi:10.1186/s12879-022-07124-9
18. Chirwa GC. Socio-economic inequality in comprehensive knowledge about HIV in Malawi. Malawi Med J. 2019;31(2):104–111. doi:10.4314/mmj.v31i2.1
19. Chirwa GC. “Who knows more, and why?” Explaining socioeconomic-related inequality in knowledge about HIV in Malawi. Sci Afr. 2020;7:e00213. doi:10.1016/j.sciaf.2019.e00213
20. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
21. Ochako R, Ulwodi D, Njagi P, Kimetu S, Onyango A. Trends and determinants of Comprehensive HIV and AIDS knowledge among urban young women in Kenya. AIDS Res Ther. 2011;8:11. doi:10.1186/1742-6405-8-11
22. Filmer D, Pritchett LH. Estimating wealth effects without expenditure data—or tears: an application to educational enrollments in states of India. Demography. 2001;38(1):115–132. doi:10.1353/dem.2001.0003
23. Vyass S, Kumaranayake L. Constructing socioeconomic status indexes: how to use principal component analysis. Health Policy Plan. 2006;21(6):459–468. doi:10.1093/heapol/czl029
24. Wagstaff A, O’Donnell O, Van Doorslaer E, Lindelow M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation. World Bank Publications; 2007.
25. Macro ICF. The DHS program Wealth index construction; 2018. Availiable from: https://www.dhsprogram.com/topics/wealth-index/Wealth-Index-Construction.cfm.
26. ICF International. Demographic and health survey sampling and household listing manual. In: Measure DHS. Calverton, Maryland, U.S.A: ICF International; 2012.
27. Wagstaff A. The bounds of the concentration index when the variable of interest is binary, with an application to immunization inequality. Health Econ. 2005;14(4):429–432. doi:10.1002/hec.953
28. Erreygers G. Correcting the concentration index. J Health Econ. 2009;28(2):504–515. doi:10.1016/j.jhealeco.2008.02.003
29. Wagstaff A, Paci P, Van Doorslaer E. On the measurement of inequalities in health. Soc Sci Med. 1991;33(5):545–557. doi:10.1016/0277-9536(91)90212-U
30. Wagstaff A, Van Doorslaer E, Watanabe N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J Econom. 2003;112(1):207–223. doi:10.1016/S0304-4076(02)00161-6
31. Doorslaer E, Koolman X, Jones AM. Explaining income‐related inequalities in doctor utilisation in Europe. Health Econ. 2004;13(7):629–647. doi:10.1002/hec.919
32. McCullagh P, Nelder JA. Generalized Linear Models. Routledge; 2019.
33. Yiengprugsawan V, Lim LL, Carmichael GA, Dear KB, Sleigh AC. Decomposing socioeconomic inequality for binary health outcomes: an improved estimation that does not vary by choice of reference group. BMC Res Notes. 2010;3(1):1–5. doi:10.1186/1756-0500-3-57
34. Jain K, Goli S, Arokiasamy P. Are self reported morbidities deceptive in measuring socio-economic inequalities. Indian J Med Res. 2012;136(5):750.
35. Hosseinpoor AR, Van Doorslaer E, Speybroeck N, et al. Decomposing socioeconomic inequality in infant mortality in Iran. Int J Epidemiol. 2006;35(5):1211–1219. doi:10.1093/ije/dyl164
36. Hamidouche M, Ante-Testard PA, Baggaley R, Temime L, Jean K. Monitoring socioeconomic inequalities across HIV knowledge, attitudes, behaviours and prevention in 18 sub-Saharan African countries. AIDS. 2022;2022:1. doi:10.1097/qad.0000000000003191
37. NSO, ICF International, International ICF, ONS, International ICF. Malawi demographic and health survey 2015–16: key indicators report. Zomba, Malawi, and Rockville, Maryland, USA; 2016. Available from: http://dhsprogram.com/pubs/pdf/PR73/PR73.pdf.
38. Amporfu E, Grépin KA. Measuring and explaining changing patterns of inequality in institutional deliveries between urban and rural women in Ghana: a decomposition analysis. Int J Equity Health. 2019;18(1):1–12. doi:10.1186/s12939-019-1025-z
39. Bonfrer I, Van de Poel E, Grimm M, Van Doorslaer E. Does the distribution of healthcare utilization match needs in Africa? Health Policy Plan. 2014;29(7):921–937. doi:10.1093/heapol/czt074
40. Gebre E, Worku A, Bukola F. Inequities in maternal health services utilization in Ethiopia 2000–2016: magnitude, trends, and determinants. Reprod Health. 2018;15(1):1–9.
41. Mezmur M, Navaneetham K, Letamo G, Bariagaber H. Socioeconomic inequalities in the uptake of maternal healthcare services in Ethiopia. BMC Health Serv Res. 2017;17(1):1–11.
42. Faust L, Yaya S, Ekholuenetale M. Wealth inequality as a predictor of HIV-related knowledge in Nigeria. BMJ Glob Health. 2017;2(4):e000461.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.