Back to Journals » Journal of Hepatocellular Carcinoma » Volume 6
Socioeconomic And Survival Differences Among Minorities With Hepatocellular Carcinoma In Florida
Authors Jones PD ![]() , Scheinberg AR, Muenyi V
, Scheinberg AR, Muenyi V ![]() , Gonzalez-Diaz J, Martin PM, Kobetz E
, Gonzalez-Diaz J, Martin PM, Kobetz E
Received 16 April 2019
Accepted for publication 10 October 2019
Published 15 November 2019 Volume 2019:6 Pages 167—181
DOI https://doi.org/10.2147/JHC.S212401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Patricia D Jones,1,2 Andrew R Scheinberg,3 Valery Muenyi,3 Joselin Gonzalez-Diaz,1 Paul M Martin,1,2 Erin Kobetz2,4
1Department of Medicine, Division of Gastroenterology and Hepatology, University of Miami Miller School of Medicine, Miami, Florida, USA; 2Sylvester Comprehensive Cancer Center, University of Miami Miller School of Medicine, Miami, Florida, USA; 3Department of Medicine, University of Miami Miller School of Medicine, Miami, Florida, USA; 4Department of Medicine, Division of Computational Medicine and Population Health, University of Miami Miller School of Medicine, Miami, Florida, USA
Correspondence: Patricia D Jones
Department of Medicine, Division of Gastroenterology and Hepatology, University of Miami Miller School of Medicine, 1120 NW 14 th Street, Miami, FL 33136, USA
Tel +1 305 243-0779
Email [email protected]
Background: Disparities in hepatocellular carcinoma (HCC) have been partly attributed to low socioeconomic status among minorities. We investigated associations between race, socioeconomic characteristics, geographic characteristics and survival in HCC patients in Florida.
Methods: Using the Florida Cancer Data System (FCDS), we analyzed HCC cases diagnosed between 1/1/2004 and 12/31/2013. To ascertain population-level socioeconomic characteristics, we linked FCDS to the 2010–2014 US Census American Community Survey and the 2013 Florida Behavioral Risk Factor Surveillance System. We also estimated patient distance to liver transplant and academic cancer centers. Using Cox proportional hazards, we modeled the association between race and survival.
Results: Of 10,852 patients, 13.1% were Black, 67.1% White, 15.7% Hispanic, and 3.2% Asian. At diagnosis, Blacks were younger with more extensive disease, p <0.001. Transplants were performed in 9.3% of Hispanics, 7.5% of Whites, 5.8% of Asians and 4.2% of Blacks, p <0.001. Median survival was longest in Hispanics and shortest in Blacks, p<0.001 When adjusted for gender, age, payer, SEER stage, surgery type, and receipt of treatment, Blacks had a 17% increased risk of death [hazard ratio (HR) 1.17, 95% confidence interval (CI) 1.07–1.29] and Whites a 9% increased risk of death [HR 1.09, 95% CI 1.02–1.17] compared to Hispanics. As a group, Hispanics lived closest to any transplant or academic cancer center, p <0.001. Neighborhood poverty level was highest where Hispanic patients lived, p <0.001.
Conclusion: Though socioeconomic differences may contribute to disparities, Hispanics survived longer than Blacks and Whites in Florida despite living in the most socioeconomically depressed neighborhoods. Increased access to transplant likely contributed to improved survival. Additional research is needed to identify which individual socioeconomic and geographic determinants contribute most to disparities.
Keywords: racial disparities, hepatocellular carcinoma, geographic disparities
Introduction
Over the past three decades, the incidence of hepatocellular carcinoma (HCC) has risen dramatically in the United States (US).1 In 2012, nearly 25,000 new cases were diagnosed.2 The Surveillance, Epidemiology, and End Results (SEER) Program estimates that over 42,000 persons will be diagnosed with liver cancer/intrahepatic bile duct cancer in 2019;3 approximately 75% of those cases represent HCC.4 Although HCC ranks 13th in the number of new cancers each year in the US, it is the 5th leading cause of cancer death3 and the fastest-growing cause of cancer-related death among men.5
Increases in HCC incidence vary by race; incidence rose faster among Blacks and Hispanics than non-Hispanic Whites2,6 with HCC risk highest in Hispanics.2,7 Significant racial disparities in HCC surveillance8 may contribute to the observation that Blacks more often present with late-stage cancer compared to other races.9–11 Adjusted for stage at presentation and severity of liver disease, Blacks are least likely to receive treatment for HCC and have the lowest survival.9,10,12,13 The etiology of chronic liver disease (CLD) causing HCC differs by race, which may confer increased risk for HCC.14,15 However, there is little evidence that HCC survival differences are driven primarily by race as a biological factor. Rather, sociodemographic implications of race such as area socioeconomic deprivation, lack of insurance and/or access to specialized care, including transplant, are major determinants of survival.13,16
Geographic differences in disease etiology and practice patterns may influence HCC incidence and survival.2,16,17 Through retrospective analysis of our local registry combined with chart review, we identified significant racial differences in HCC survival.9 In the study described herein, we aimed to evaluate whether the same trends observed locally would be present throughout the state. Florida is the third-most populous state with the fourth-highest number of HCC cases.2 The rich diversity of Florida’s population, enhanced by a large immigrant population, allows for the evaluation of multiple determinants of survival. Few studies have investigated how geography18 or neighborhood socioeconomic status (SES), which vary significantly by race, influence HCC survival on a population level. This study explores the association between race, geography, individual- and neighborhood-level socioeconomic factors and in that context, evaluates how race impacts HCC survival.
Materials And Methods
Study Cohort
We analyzed the Florida Cancer Data System (FCDS) for incident HCC cases diagnosed from 1/1/2004 to 12/31/2013. Cancers of the liver and intrahepatic bile ducts are combined in FCDS using International Classification of Disease Code-10, C22.0, n=14,017. We included only HCC cases, defined by International Classification of Diseases for Oncology ICD-O-3 codes 8170–8179, n=10,891. After removing duplicates, the sample size was 10,852 (Figure 1).
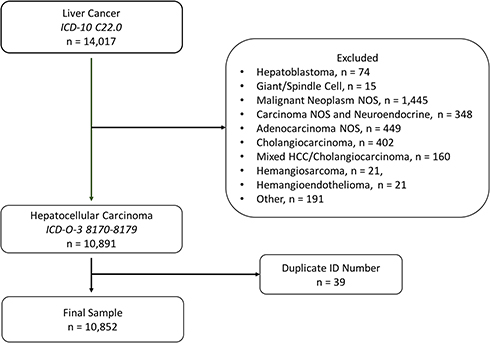 |
Figure 1 Study flow diagram. Abbreviations: ICD-10, International Classification of Disease; ICD-O-3, International Classification of Diseases for Oncology; NOS, not otherwise specified. |
Variables And Data Source
The FCDS is a statewide, population-based cancer incidence registry created in 1978 by the State of Florida Department of Health (DOH) and is operated by Sylvester Comprehensive Cancer Center (SCCC) at the University of Miami Miller School of Medicine (UMMSM) with support from the Florida DOH, the Centers for Disease Control and Prevention (CDC) and the National Program for Cancer Registries. The FCDS collects over 98% of all incident cancers in Florida and performs passive follow-up of patient status annually through a series of linkages with the State of Florida Bureau of Vital Statistics and the National Death Index.19 The registry contains demographics, tumor and treatment characteristics. Race and ethnicity are defined by North American Association of Central Cancer Registries criteria. In the FCDS, nearly 98% of hepatocellular carcinoma (HCC) cases were reported by hospitals or managed care plans with comprehensive-unified medical records. Other sources were radiation treatment centers, medical oncology centers, laboratory centers, private physician offices, nursing homes, hospice facilities, autopsy (<0.1%) and outpatient hospital settings or ambulatory surgery centers. In <1%, the diagnosis was made on clinical grounds alone; for <1%, the death certificate was the only confirmation of diagnosis. Diagnosis was confirmed by histology in 78.9%, cytology in 2.2%, laboratory test in 3.5%, and imaging without microscopic confirmation in 13.7%. The FCDS also contains geographic variables, e.g. zip code, county and census tract. Zip code was missing in 10 persons (<0.1%).
US Census American Community Survey (ACS) – Selected Economic Characteristics
To evaluate racial differences in neighborhood SES, we linked FCDS to the 2010–2014 US Census American Community Survey (ACS) – Selected Economic Characteristics database using 2010 census tracts. Census tract was missing in only 137 (1.3%). Response rates for ACS ranged from 90.8% to 98.9% during the years 2010 through 2014.20 The ACS, an ongoing survey administered by the US Census Bureau, collects information on economic characteristics and aggregates data by geographic units of varying size, ranging from national data (largest unit) to census block (smallest unit). To ascertain neighborhood-level socioeconomic characteristics, we linked FCDS to ACS by census tract, an established geographic unit designed to be “as homogeneous as possible with respect to population characteristics, economic status, and living conditions.”21 Therefore, the socioeconomic characteristics of the individual should closely resemble that of the group. Although ACS data is also aggregated by zip code and county, these geographic units cover larger, more heterogeneous populations and can present a skewed assessment of socioeconomic characteristics.22,23 We used 5-year estimates as these are most reliable.24 The coverage rate of ACS in Florida during 2010–2014 period ranged from 97.6% in 2010 to 98.9% in 2013. For ACS variables reported as the percentage of respondents, we report the median percentage and interquartile range. We included those variables which reflect the economic health of a community, such as the percentage of families living below the poverty level and the percentage of those uninsured or unemployed.
Behavioral Risk Factor Surveillance System (BRFSS)
To approximate access to cancer-specific preventative services on a county level, we linked FCDS to the 2013 CDC Florida Behavioral Risk Factor Surveillance System (BRFSS),25 a telephone survey which collects self-reported data regarding health-related behaviors, chronic health conditions, use of preventative services, access to care and health-related quality of life.26,27 Of those eligible respondents who were contacted, 57.1% (landline) and 65% (cell phone) cooperated with the survey, consistent with participation rates for other national telephone surveys. Approximately 34,000 persons completed interviews. Florida has participated in BRFSS since 1986 and periodically publishes county-level reports. The response rate is the number of respondents who completed the survey as a proportion of all eligible and likely-eligible persons. The median survey response rate for all states, territories and Washington, DC, in 2013 was 46.4%, and ranged from 20.9% to 60.3%. The combined response rate for Florida BRFSS in 2013 was 35.2%. For detailed information, see the BRFSS Summary Data Quality Report.28
Disparities are not mediated by individual-level determinants alone; therefore, assessment of population-level characteristics may provide insight that informs future interventions. Most variables in BRFSS are reported as the percentage of adults who have a chronic condition, e.g. high cholesterol, or the percentage of adults who have received a screening test for cancer, e.g. adults 50 years of age or older with a stool blood test in the past year. For BRFSS variables, we report the median with interquartile range. To evaluate for population differences in the burden of common chronic diseases, we included variables reporting the percentage of persons with high cholesterol, diabetes or obesity. Prevalence rates are adjusted or “weighted” by the Centers for Disease Control and Prevention (CDC).25 Health behaviors, such as current or heavy alcohol use, may influence HCC incidence and survival. Thus, we included variables for smoking and binge or heavy alcohol use. We report the median percentage of adults who report poor health and the median number of days per month where health interferes with regular activity as proxies for health-related quality of life.29,30 Finally, we report on receipt of age-appropriate cancer screening (pap smear, stool test, colonoscopy, and mammogram), which may approximate access to care and screening, the latter of which is critically important for early diagnosis of HCC.
Distance To Academic Cancer Centers And Liver Transplant Centers
We used CDXZipStream™ to calculate straight-line distance between zip code at diagnosis and the three Florida academic cancer centers: SCCC (Miami), University of Florida Health Cancer Center (Gainesville), and Moffitt Cancer Center (Tampa). Similarly, we also estimated distance to the seven active liver transplant programs in Florida.31 We estimated Euclidean (straight-line) distance in miles rather than travel distance, which is affected by variables not included in FCDS, such as access to personal transportation and rurality.32 Straight-line distance correlates significantly with travel distance and travel time.33,34 Zip code centroids were used to calculate distance rather than census tract centroids, a smaller geographic unit, due to ease of calculation using zip code compared to census tract with commercially available programs such as CDXZipStream™, ArcGIS, and Google Maps. Additionally, both census tracts and zip codes may cover non-contiguous geographic areas and thus may be prone to similar distance calculation errors.
Outcomes
The primary outcome variable was survival after HCC diagnosis, measured as the difference in days between diagnosis date and date of death or last follow-up, if alive. Participating institutions perform chart review to determine the date of last follow-up or death. This data is reported to FCDS and is supplemented by the FCDS mortality file, which is linked with incidence data and is based on data from the State of Florida Bureau of Vital Statistics and the National Death Index.
Statistical Analysis
Categorical variables were expressed using proportions and continuous variables using median and interquartile range (IQR). We identified associations between baseline characteristics, race and vital status using Wilcoxon rank-sum and Kruskal–Wallis tests for continuous and Pearson’s chi-square for categorical variables. We assessed interaction with multiple degree-of-freedom likelihood ratio tests. A priori, we included age at diagnosis, gender and tumor stage in the multivariate model as confounders based on clinical reasoning and published data.5 We included potential confounders in the multivariate model, if p <0.10 in bivariate analysis and eliminated confounders via hierarchical backwards elimination strategy using a change in estimate approach (<10%). We determined crude and adjusted hazard ratios (HR) for mortality using Cox proportional hazards modeling with a robust standard error correction to adjust for geographic clustering. Receipt of multiple procedures is common in HCC care. Although FCDS provides information about the date of surgery; the chronology of surgical procedures in persons who have received more than one surgical procedure cannot be established through analysis of the cancer registry. Therefore, patients who received transplant were not censored at the time of transplant.
We addressed missing data by categorizing continuous variables and adding a category for unknown data. We compared these results to those obtained from multivariate models with multiple imputation. Kaplan-Meier survival curves were generated and the log-rank test was used to compare groups. For multivariate analyses, two-sided p-values ≤0.05 were considered statistically significant. Analyses were performed using Stata version 14.2 (College Station, TX). The data accessed are not freely available, but can be requested through The Florida Cancer Data System. (https://fcds.med.miami.edu/inc/datarequest.shtml). This project was approved by the University of Miami Miller School of Medicine Institutional Review Board (IRB # 2014-08-UM).
Results
Overall Sample
The sample was predominantly male, 77.4%. Median age at diagnosis was 63 years. Median size of the largest tumor was 49 mm and cancer stage, defined by SEER Summary Tumor Stage 2000, was localized in 44.1%, regional with direct extension and/or lymph node involvement in 26%, distant in 14.9%, and unstaged in 15%. Metastases were present at diagnosis in 14.3%. Alpha-fetoprotein (AFP) was borderline or elevated in 81.1% of patients for whom it was reported, ~30% of the sample. Ishak fibrosis score was reported in 4.8% of the sample; 67.9% had severe fibrosis or cirrhosis (Ishak 5–6). See Table 1.
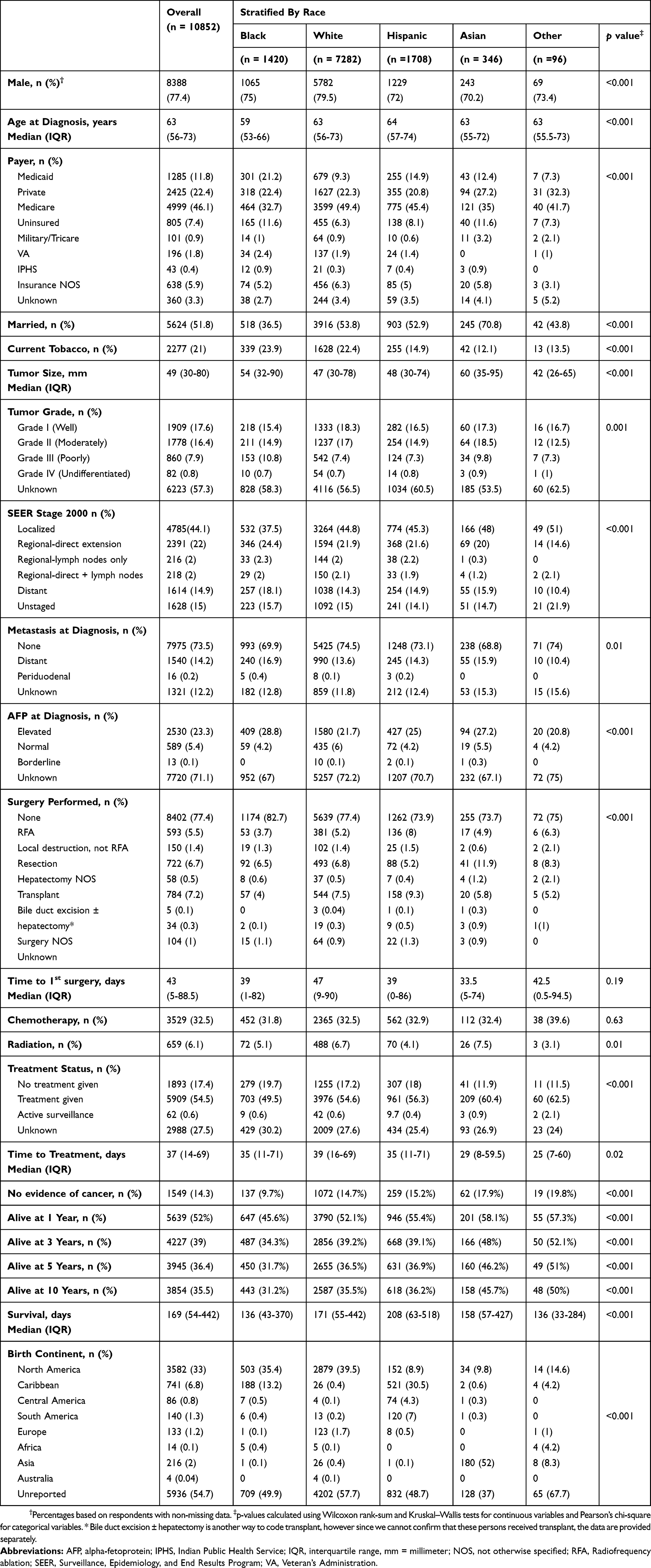 |
Table 1 Baseline Characteristics Of The Overall Sample And The Sample Stratified By Race |
Surgery and/or local destruction was performed in 21.7% of patients; 593 patients had radiofrequency ablation (RFA), 150 patients had non-RFA local destruction. Transplant was performed in 784 patients, 7.2%, and 722 patients, 6.7%, had resection. While radiotherapy (external beam radiation, implants and isotopes) was utilized infrequently, chemotherapy was administered to 32.5%. As in other cancer registries, e.g. SEER,35 chemoembolization is coded as chemotherapy in FCDS.36 Median time to first treatment was 37 days. In 14.3% of the sample, “No Evidence of Disease” (NED) was achieved. In those alive at follow-up, mean time followed was 233 days (Range 0–3805 days). In those deceased, median time followed was 132 days (Range 0–3354 days). Median survival was 169 days; 52% of the sample was alive at 1 year, 39% was alive at 3 years, and 36.4% was alive at 5 years.
Baseline Characteristics Stratified By Race
Blacks were youngest at diagnosis, median age was 59 years, compared to 63 years in Whites, Asians, and others, and 64 years in Hispanics, p <0.001. More Blacks and Asians, 11.6%, were uninsured compared to Whites, Hispanics, and others, p <0.001. Asians and Blacks had significantly larger tumors; median size of the largest tumor was 60 mm in Asians, 54 mm in Blacks, 48 mm in Hispanics, 47 mm in Whites and 42 mm in others, p <0.001. More Blacks had distant disease; only 37.5% of Blacks presented with localized disease, compared to 44.8% of Whites, 45.3% of Hispanics, 48% of Asians, and 51% of others, p <0.001.
There were no significant racial differences in receipt of chemotherapy or radiotherapy. Transplant was performed in 9.3% of Hispanics, 7.5% of Whites, 5.8% of Asians, 5.2% of others and 4% of Blacks, p <0.001. Resection was performed more frequently in Asians and RFA more frequently in Hispanics. Median survival was 136 days in Blacks, 158 days in Asians, 171 days in Whites and 208 days in Hispanics, p <0.001. One-year survival was 45.6% in Blacks, 52% in Whites, 55.4% in Hispanics, 57.3% in others, and 58.1% in Asians, p <0.001. Five-year survival was 31.7% in Blacks, 36.5% in Whites, 36.9% in Hispanics, 46.2% in Asians and 51% in others, p <0.001.
Sociodemographic And Behavioral Characteristics
Using the 2010–2014 US Census ACS – Selected Economic Characteristics, we investigated neighborhood economic characteristics. Neighborhood poverty, defined as the percentage of families and people whose income in the past 12 months was below poverty level, was highest in the census tracts where Hispanic HCC patients lived, 11.9%, followed by Blacks, 11.1%, Asians, 10.7%, and Whites, 10.4%, p <0.001. Similarly, Hispanics lived in neighborhoods with the most uninsured persons. Mean household income was lowest where Hispanics lived compared to other races, p <0.001. Unemployment was similar regardless of race. Although most lived in urban areas, this varied by race.
We linked FCDS to the 2013 CDC Florida BRFSS25 to obtain county-level data on use of preventative services, community burden of chronic disease, and aggregate health behaviors, which could influence HCC risk. There were no significant differences in self-report of heavy or binge alcohol use. Receipt of age-appropriate cancer screening may approximate access to care on a population level. In the counties where Hispanic HCC patients lived, more women reported mammograms in the past year, 64%, compared to 58.5% of women where Blacks lived, 57.4% where Whites lived, and 56.9% in where Asians lived, p <0.001. The counties where Whites lived had the lowest percentage of women reporting Papanicolau tests in the past year, 51.7%. Although Hispanics lived in counties with the highest rates of stool testing for colorectal cancer screening, Whites lived in counties with the highest colonoscopy rates, p <0.001. The percentage of persons reporting cancer screening via Pap smear, mammogram and colonoscopy in Florida was consistent with national averages.37 See Table 2 for details.
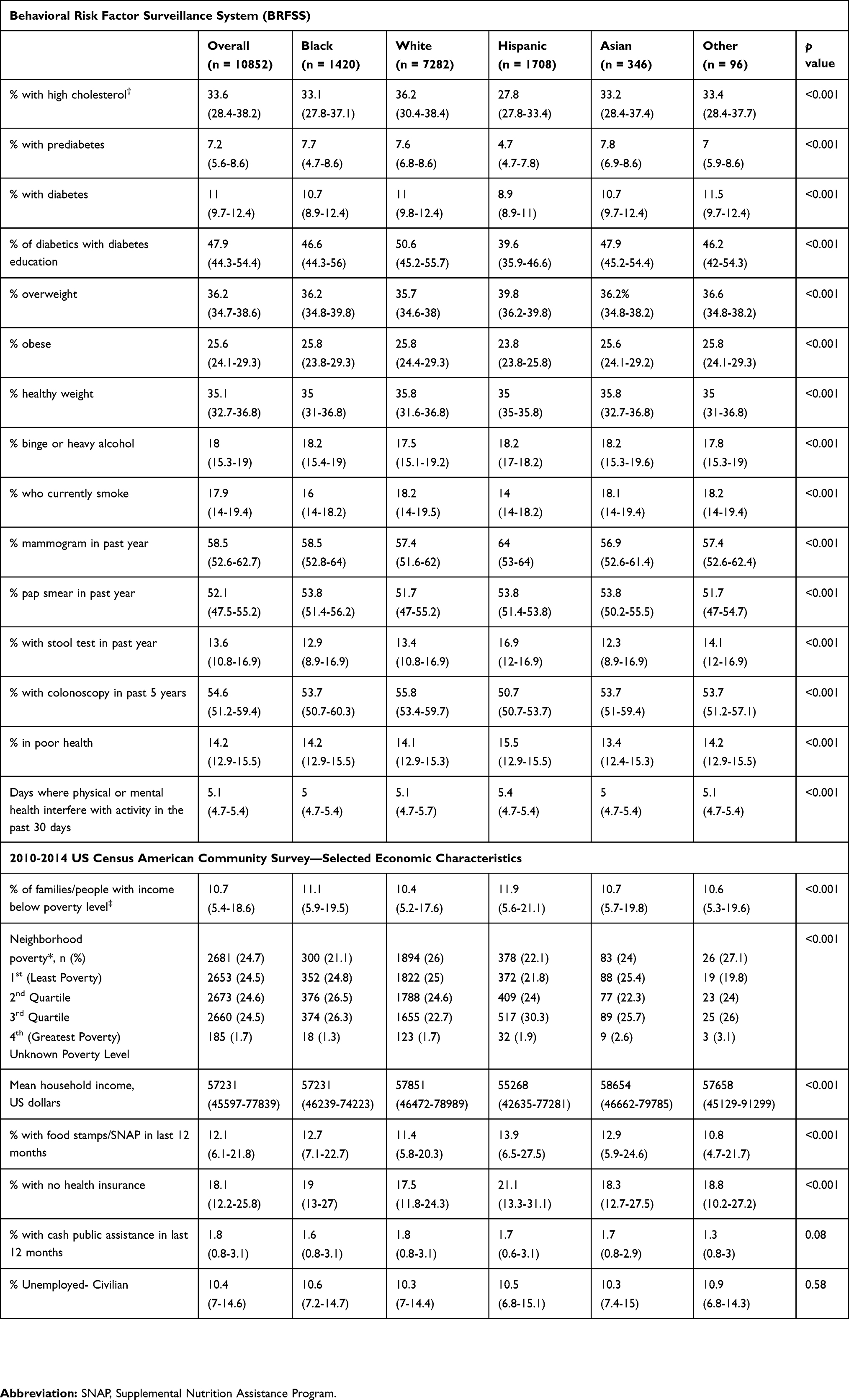 |
Table 2 Selected Population Characteristics Of The Overall Sample And The Sample Stratified By Race |
Geographic Access To Specialty Care
Having noted significant racial differences in receipt of transplant, we calculated the distance between zip code at diagnosis and the seven liver transplant programs in Florida. Hispanics lived closest to any liver transplant program, 10.6 miles, compared to 14.3 miles in Blacks, 15.2 miles in Asians, 18.3 miles in others, and 29.7 miles in Whites, p <0.001. Over 80% of the sample lived within 60 miles of a liver transplant program (Supplementary Table 1). Distance from a transplant center was not significantly different when stratified by mortality. Hispanics also lived closest to an academic cancer center, 16.3 miles, compared to 35.9 in others, 39.4 in Blacks, 54.3 in Asians and 56.9 in Whites, p <0.001. Over 50% lived within 60 miles of an academic cancer center. See Figure 2 for a graphical representation of HCC burden within Florida.
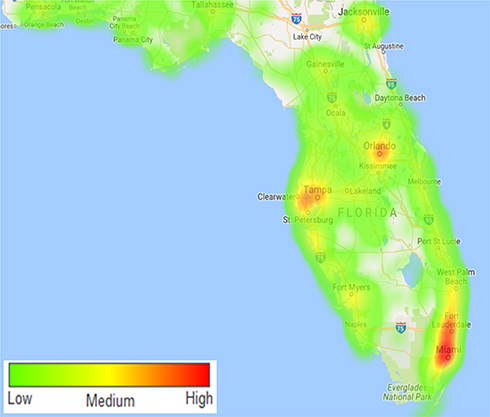 |
Figure 2 Geographic distribution of HCC cases throughout Florida, unadjusted for population density. Regions in red have the highest raw number of HCC cases. |
Factors Associated With HCC Survival
At study end, 6999 were deceased, median survival 169 days, and 3853 were alive, median survival 233 days, p <0.001. Deceased subjects were older at diagnosis, median age 64 years, compared to 62 years in those alive. They also presented at more advanced cancer stage; tumor stage was localized in 57.7% of those alive compared to 36.6% of those deceased, p <0.001. Distant metastases were present in 17.7% of those deceased vs 7.8% of those alive, p <0.001. Liver transplant was performed in 15.2% of those alive, compared to 2.8% of those who died, p <0.001.
Using Cox modeling, we found that older age at diagnosis, male gender, lack of insurance, current tobacco use, larger tumor size, and advanced SEER tumor stage were negatively associated with survival. Hispanic ethnicity, receipt of surgery or other treatment was protective. As Hispanics had the longest survival, they were used as the referent group in univariate and multivariate modeling. Compared to Hispanics, Whites had a 7% increased rate of death, hazard ratio (HR) 1.07, 95% confidence interval (CI) 1–1.14, p 0.04, and Blacks had a 29% increased rate of death, HR 1.29, 95% CI 1.18–1.4, p <0.001. When adjusted for gender, age, payer, SEER stage, surgery type, and receipt of treatment, Whites had 9% increased rate of death, HR 1.09, 95% CI 1.02–1.17, p 0.02 and Blacks had 17% increased rate of death, HR 1.17, 95% CI 1.07–1.29, p <0.001 compared to Hispanics. Neither neighborhood poverty, distance to transplant nor distance to cancer center significantly changed the multivariate model and were removed without consequence. See Table 3 and Figure 3 for HR, CI, p values and Kaplan-Meier survival curves.
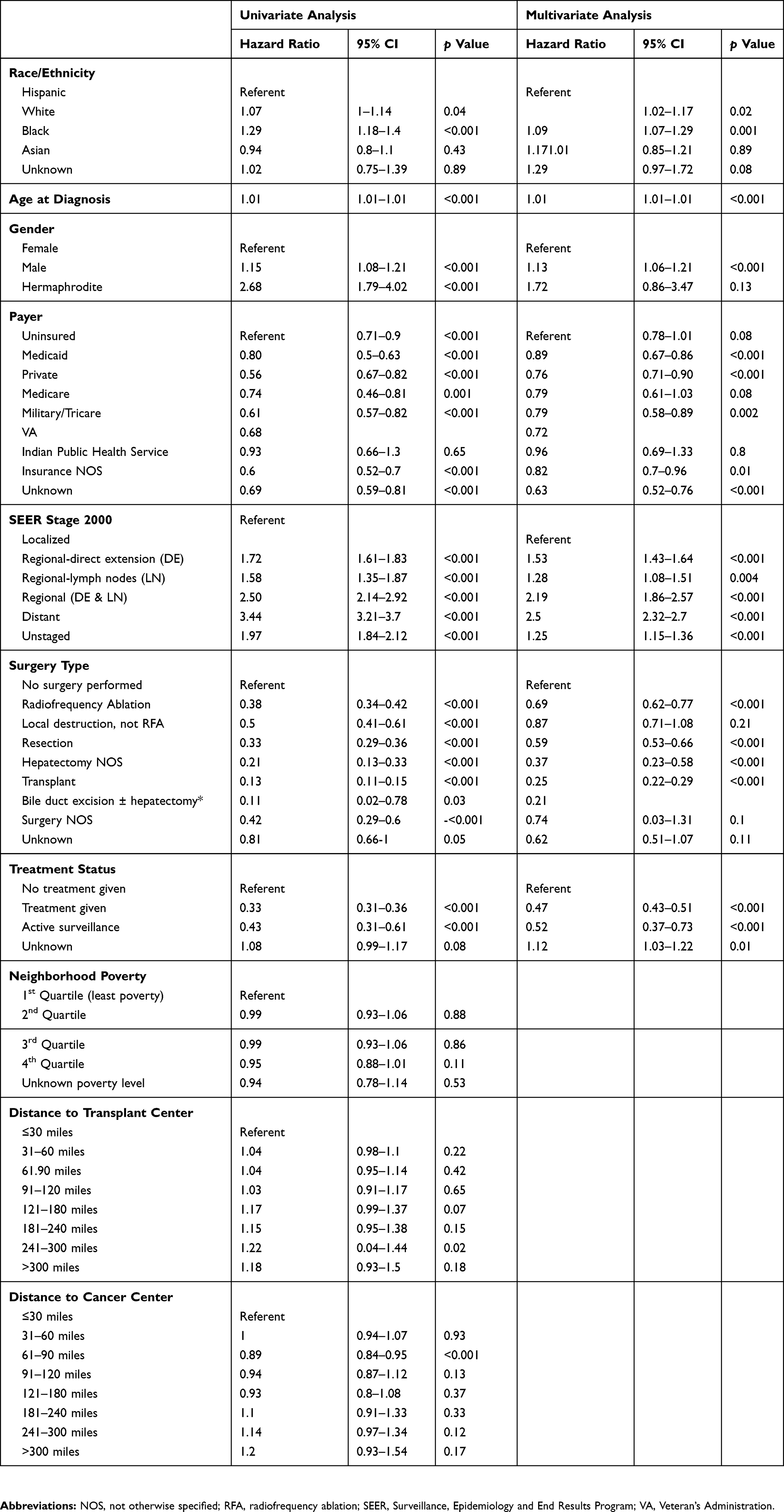 |
Table 3 Factors Associated With Survival On Univariate And Multivariate Analysis |
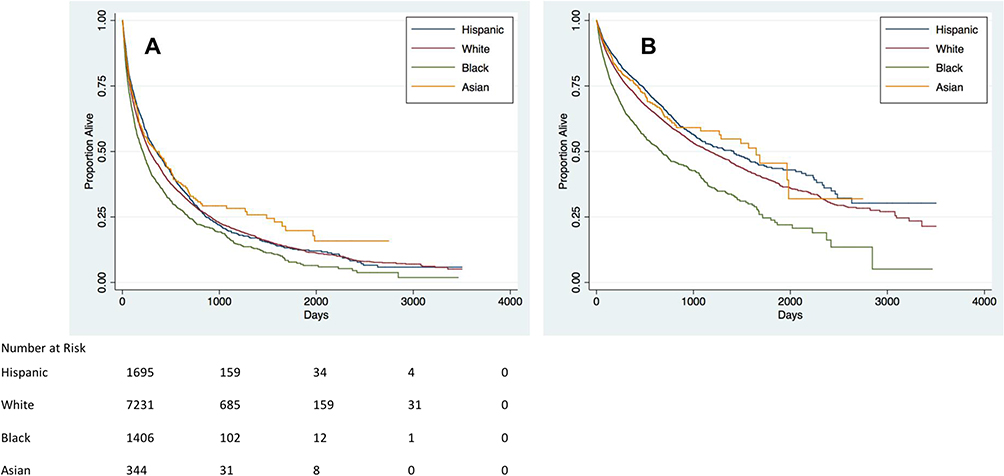 |
Figure 3 Kaplan–Meier curves (A) stratified by race/ethnicity and (B) stratified by race/ethnicity and adjusted for gender, age at diagnosis, insurance type, SEER Summary Tumor Stage, surgery type, and treatment status. |
Discussion
There are clear racial differences in HCC incidence,1,2,6 survival,9,10,38 and mortality.39 In this retrospective study evaluating over 10,000 persons diagnosed with HCC from 2004 to 2013 in Florida, we found that Hispanics lived longest, 208 days, and had liver transplant and/or RFA more often. Blacks had more extensive disease at diagnosis, were least likely to receive liver transplant and had the shortest survival, 136 days. Compared to Hispanics, Blacks had 17% and Whites had 9% increased risk of death. The strongest predictors of survival were cancer stage at presentation and treatment, especially surgical treatment, which varied significantly by race.
Much of the data regarding disparities in HCC is derived from analysis of administrative databases, like SEER-Medicare, which lack clinical information regarding liver function. Consequently, some hypothesize that survival differences are attributable to racial differences in liver function, which does affect treatment eligibility. However, three large retrospective analyses challenge this hypothesis. Previously, we reported that Blacks with HCC had lower model for end stage liver (MELD) score, as well as lower rates of ascites, hepatic encephalopathy and varices compared to Whites and Hispanics.9 In studies by Rich et al10 and Estevez et al,38 Blacks with HCC had higher rates of compensated cirrhosis (Child Pugh Class A) and lower rates of ascites and hepatic encephalopathy compared to other races. Except in specific scenarios, e.g. chronic hepatitis C,14,15 there is little evidence that HCC risk or its biological behavior is mediated by race. Therefore, other important factors must be contributing to adverse outcomes.
Other investigators have postulated that existing disparities are attributable mostly to socioeconomic barriers disproportionately affecting minorities, such as lack of health insurance.13,16 Inadequate access to healthcare leads to missed opportunities to diagnose underlying liver disease and perform HCC surveillance. This may explain why Blacks consistently present with more advanced HCC, as noted in this study and others.9,10,12 Even when surveillance is consistent and Blacks and Hispanics present with early stage HCC, they are less likely than Whites to receive invasive treatment according to Mathur et al.12 Blacks with HCC have considerably lower transplant rates,9,10,12,40 and our study confirms this finding. Although this may be due to medical ineligibility for transplant, such as advanced cancer exceeding the Milan criteria, socioeconomic and/or geographic barriers likely play important roles. Within FCDS, the only direct measure of individual SES is insurance status. Blacks and Asians were most often uninsured, which limits access to treatment and influences the quality of care. Uninsured patients are ineligible for transplant. We found that uninsured patients had significantly shorter survival than insured patients.
In our study, Hispanics lived closest to transplant and academic cancer centers and had the highest transplant rates, which likely contributed to improved survival. These findings suggest that geographic proximity to multidisciplinary care, e.g. liver transplant, significantly influences treatment decisions/outcomes and potentially mitigates the adverse effects of low individual or neighborhood socioeconomic status. This study is the first to explore neighborhood-level socioeconomic factors in the context of HCC survival using census tract, a geographic unit designed to be “as homogeneous as possible with respect to population characteristics, economic status, and living conditions” such that individual characteristics are well reflected by the group.21 Despite living in relatively disadvantaged neighborhoods with the lowest mean household income and more persons living below poverty level, Hispanics had the best survival after HCC diagnosis. Our study demonstrates that adverse socioeconomic conditions alone are insufficient to explain disparate HCC outcomes. Although not previously reported for HCC, these findings may reflect the “Hispanic paradox”, whereby Hispanics have better cancer outcomes compared to other US populations despite poorer socioeconomic conditions.41,42 Rich et al also found that Hispanics had increased adjusted survival compared to Whites.10 We noted that Hispanics living in neighborhoods with the lowest percentage of persons below the poverty line had prolonged survival compared to Hispanics living in neighborhoods with higher degrees of poverty. Prospective studies are needed to assess how individual socioeconomic status interacts with neighborhood poverty to influence HCC survival in diverse populations. As country of birth was missing in 48.7% of Hispanics, which precluded a full assessment of the impact of nativity on survival in Hispanics.
Retrospective analyses of cancer incidence registries, including FCDS, are fraught with challenges, mainly incomplete clinical information and potentially inaccurate dates. The most widely used staging system for HCC in clinical practice is the Barcelona Clinic Liver Cancer (BCLC) Staging System. Despite its widespread use, current cancer registries such as SEER and the US Cancer Statistics registry,2 do not contain sufficient clinical information to classify patients according to BCLC. For consistency with other registries, the FCDS also relies on the SEER staging system. Though this is less granular than BCLC, we found that SEER stage correlated with survival, p <0.001. Another limitation of this study is the lack of information pertaining to the etiology of chronic liver disease leading to HCC. Although disease etiology may vary substantially by race,9,10 there is no significant evidence that survival differs by disease etiology. Fibrosis stage and liver function can affect treatment options and may influence survival; however, registries do not reliably provide this information.
Despite the aforementioned limitations of cancer registries, they enable assessment of much larger sample sizes than can be analyzed at a single center and also highlight variations in clinical practice over large geographic areas. For example, liver biopsy is not required for HCC diagnosis in the presence of characteristic imaging features.43 However, nearly 80% of our sample was diagnosed by histology and approximately 14% by radiological imaging alone during the study period. Though large academic medical centers may have confidence in the ability of radiologic imaging to diagnose HCC, smaller centers or community hospitals may opt to confirm the diagnosis with biopsy. Sherman et al reported that 62.9% of patients in a managed care population received liver biopsy during their diagnostic workup for HCC.44
A strength of FCDS is that it can be linked to other publicly available databases to characterize community characteristics, which is of importance as we seek to understand the determinants contributing to disparities in HCC. Through Census data, we ascertained that neighborhood-level SES has minimal impact on survival. Using BRFSS, we found population-level variations in the percentage of adults who reported cancer screening for other common cancers by race. On an individual level, we know that risk factors for inconsistent HCC surveillance include Black race, uninsured status, and failure to identify the cancer-predisposing disease, i.e. cirrhosis.8 Future studies regarding access to HCC surveillance services on a community level are needed in order to intervene and ensure equitable access to vulnerable populations.
Although Florida has the 4th highest number of HCC cases nationally,2 there is only one National Cancer Institute (NCI) designated cancer center in Florida and many patients reside at great distances from comprehensive multidisciplinary cancer care. Those receiving transplant lived closer to transplant centers than those not receiving transplant. Although straight-line distance correlates strongly with more meaningful measures, such as travel distance,34 it is somewhat limited. In order to enhance our understanding of the geographic factors contributing to racial disparities in HCC, future studies should incorporate complete geographic information, including full address at diagnosis and primary mode of transportation.32 In addition to exploring how known determinants of racial disparities impact HCC survival on an individual level, future studies should investigate the impact of environmental factors and community resources on survival in diverse individuals with HCC.
Conclusions
Our study evaluating over 10,000 HCC patients during a 10-year period confirms significant survival differences by race in Florida. Hispanics survived longer than Blacks and Whites despite living in the neighborhoods with the highest rates of poverty and uninsured persons. Hispanics also lived closest to liver transplant and academic cancer centers which potentially mitigated negative consequences of low SES and contributed to increased survival. Additional study is needed to identify the most influential determinants of racial disparities in minority populations that are disproportionately affected by HCC.
Abbreviations
ACS, American Community Survey; AFP, alpha-fetoprotein; BRFSS, Behavioral Risk Factor Surveillance System; CDC, Centers for Disease Control and Prevention; CI, confidence interval; CLD, chronic liver disease; DOH, Department of Health; HR, hazard ratio; HCC, hepatocellular carcinoma; IQR, interquartile range; FCDS, Florida Cancer data System; MELD, Model for End Stage Liver Disease; NCI, National Cancer Institute; NED, no evidence of disease; RFA, radiofrequency ablation; SEER, Surveillance, Epidemiology, and End Results; SES, socioeconomic status; SCCC, Sylvester Comprehensive Cancer Center; UMMSM, University of Miami Miller School of Medicine; US, United States.
Acknowledgements
We acknowledge the CDC and Florida Department of Health (DOH) for support of the FCDS, and the publication and distribution of the Florida Annual Cancer Report under cooperative agreement U58DP003872-04. The findings and conclusions in this manuscript are those of the authors and do not represent the official position of the CDC, DOH or National Institutes of Health. This research was conducted in collaboration with the Biostatistics and Bioinformatics Shared Resource of the Sylvester Comprehensive Cancer Center, University of Miami. The salary of the corresponding author is partially supported by a Diversity Supplement awarded by the National Institutes of Health (NIH) National Institute on Minority Health and Health Disparities (U01MD010614-01S1). The NIH was not involved in study design or in the collection, analysis or interpretation of data. Furthermore, the NIH did not contribute to the writing of this manuscript or decision to submit for publication. An earlier version of the abstract of this paper was presented at the 9th Annual Meeting, American Association for Cancer Research Science of Cancer Health Disparities in Racial/Ethnic Minorities & the Medically Underserved as a poster presentation with interim findings. The poster’s abstract was published in “Abstracts” in Cancer Epidemiol Biomarkers Prev 2017;26(2 Suppl):Abstract nr A01. DOI: 10.1158/1538-7755.DISP16-A01. A revised version of the abstract for this paper was presented at the 67th Annual Meeting of the American Association for the Study of Liver Diseases: The Liver Meeting 2016 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Session IV” in Hepatology: https://doi.org/10.1002/hep.28800.
Author Contributions
- Jones – Project conception and design, methodology development, data acquisition, data analysis and interpretation, manuscript drafting, critical revision. I approved the final draft submitted.
- Scheinberg – Data acquisition, data analysis and interpretation, manuscript drafting, critical revision. I approved the final draft submitted.
- Muenyi – Data acquisition of data, data analysis and interpretation, manuscript drafting, critical revision. I approved the final draft submitted.
- Diaz – Data acquisition of data, data analysis and interpretation, manuscript drafting, critical revision. I approved the final draft submitted.
- Martin – Project conception and design, data analysis and interpretation, manuscript drafting, critical revision. I approved the final draft submitted.
- Kobetz –- Project conception and design, methodology development, data acquisition, data interpretation, manuscript drafting, critical revision. I approved the final draft submitted. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Dr Paul M Martin reports grants from AbbVie, grants from Gilead, grants from BMS, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Njei B, Rotman Y, Ditah I, Lim JK. Emerging trends in hepatocellular carcinoma incidence and mortality. Hepatology. 2015;61(1):191–199. doi:10.1002/hep.27388
2. White DL, Thrift AP, Kanwal F, Davila J, El-Serag HB. Incidence of hepatocellular carcinoma in all 50 United States, from 2000 through 2012. Gastroenterology. 2017;152(4):812–820 e815. doi:10.1053/j.gastro.2016.11.020
3. https://seer.cancer.gov/statfacts/html/livibd.html
4. Altekruse SF, Devesa SS, Dickie LA, McGlynn KA, Kleiner DE. Histological classification of liver and intrahepatic bile duct cancers in SEER registries. J Registry Manag. 2011;38(4):201–205.
5. El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132(7):2557–2576. doi:10.1053/j.gastro.2007.04.061
6. Ha J, Yan M, Aguilar M, et al. Race/ethnicity-specific disparities in cancer incidence, burden of disease, and overall survival among patients with hepatocellular carcinoma in the United States. Cancer. 2016;122(16):2512–2523. doi:10.1002/cncr.v122.16
7. Setiawan VW, Hernandez BY, Lu SC, et al. Diabetes and racial/ethnic differences in hepatocellular carcinoma risk: the multiethnic cohort. J Natl Cancer Inst. 2014;106:12. doi:10.1093/jnci/dju326
8. Singal AG, Li X, Tiro J, et al. Racial, social, and clinical determinants of hepatocellular carcinoma surveillance. Am J Med. 2015;128(1):90e91–97. doi:10.1016/j.amjmed.2014.07.027
9. Jones PD, Diaz C, Wang D, Gonzalez-Diaz J, Martin P, Kobetz E. The impact of race on survival after hepatocellular carcinoma in a diverse American population. Dig Dis Sci. 2018;63(2):515–528. doi:10.1007/s10620-017-4869-3
10. Rich NE, Hester C, Odewole M, et al. Racial and ethnic differences in presentation and outcomes of hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2018.
11. Sloane D, Chen H, Howell C. Racial disparity in primary hepatocellular carcinoma: tumor stage at presentation, surgical treatment and survival. J Natl Med Assoc. 2006;98(12):1934–1939.
12. Mathur AK, Osborne NH, Lynch RJ, Ghaferi AA, Dimick JB, Sonnenday CJ. Racial/ethnic disparities in access to care and survival for patients with early-stage hepatocellular carcinoma. Arch Surg. 2010;145(12):1158–1163. doi:10.1001/archsurg.2010.272
13. Artinyan A, Mailey B, Sanchez-Luege N, et al. Race, ethnicity, and socioeconomic status influence the survival of patients with hepatocellular carcinoma in the United States. Cancer. 2010;116(5):1367–1377. doi:10.1002/cncr.v116:5
14. Dillon ST, Bhasin MK, Feng X, Koh DW, Daoud SS. Quantitative proteomic analysis in HCV-induced HCC reveals sets of proteins with potential significance for racial disparity. J Transl Med. 2013;11:239. doi:10.1186/1479-5876-11-239
15. Di Poto C, He S, Varghese RS, et al. Identification of race-associated metabolite biomarkers for hepatocellular carcinoma in patients with liver cirrhosis and hepatitis C virus infection. PLoS One. 2018;13(3):e0192748. doi:10.1371/journal.pone.0192748
16. Major JM, Sargent JD, Graubard BI, et al. Local geographic variation in chronic liver disease and hepatocellular carcinoma: contributions of socioeconomic deprivation, alcohol retail outlets, and lifestyle. Ann Epidemiol. 2014;24(2):104–110. doi:10.1016/j.annepidem.2013.11.006
17. Davila JA, Petersena NJ, Nelson HA, El-Serag HB. Geographic variation within the United States in the incidence of hepatocellular carcinoma. J Clin Epidemiol. 2003;56(5):487–493. doi:10.1016/S0895-4356(02)00605-4
18. Sonnenday CJ, Dimick JB, Schulick RD, Choti MA. Racial and geographic disparities in the utilization of surgical therapy for hepatocellular carcinoma. J Gastrointest Surg. 2007;11(12):1636–1646. [discussion 1646]. doi:10.1007/s11605-007-0315-8
19. https://fcds.med.miami.edu/inc/welcome.shtml#.
20. https://www.census.gov/acs/www/methodology/sample-size-and-data-quality/response-rates/.
21. https://www2.census.gov/geo/pdfs/reference/GARM/Ch10GARM.pdf.
22. Krieger N, Waterman P, Chen JT, Soobader MJ, Subramanian SV, Carson R. Zip code caveat: bias due to spatiotemporal mismatches between zip codes and US census-defined geographic areas – the Public Health Disparities Geocoding Project. Am J Public Health. 2002;92(7):1100–1102. doi:10.2105/AJPH.92.7.1100
23. Krieger N, Chen JT, Waterman PD, Soobader MJ, Subramanian SV, Carson R. Geocoding and monitoring of US socioeconomic inequalities in mortality and cancer incidence: does the choice of area-based measure and geographic level matter?: the Public Health Disparities Geocoding Project. Am J Epidemiol. 2002;156(5):471–482. doi:10.1093/aje/kwf068
24. Spielman SE, Folch D, Nagle N. Patterns and causes of uncertainty in the American Community Survey. Appl Geogr. 2014;46:147–157. doi:10.1016/j.apgeog.2013.11.002
25. http://www.floridahealth.gov/statistics-and-data/survey-data/behavioral-risk-factor-surveillance-system/reports/_documents/2013county/_documents/2013_summary.pdf.
26. Li C, Balluz LS, Okoro CA, et al. Surveillance of certain health behaviors and conditions among states and selected local areas – behavioral Risk Factor Surveillance System, United States, 2009. MMWR Surveill Summ. 2011;60(9):1–250.
27. Pierannunzi C, Xu F, Wallace RC, et al. A methodological approach to small area estimation for the behavioral risk factor surveillance system. Prev Chronic Dis. 2016;13:E91. doi:10.5888/pcd13.150480
28. https://www.cdc.gov/brfss/annual_data/2013/pdf/2013_dqr.pdf.
29. https://chronicdata.cdc.gov/browse?category=Health-Related+Quality+of+Life.
30. https://www.cdc.gov/hrqol/pdfs/mhd.pdf.
31. https://www.srtr.org/transplant-centers/?query=&distance=50&location=&state=FL&recipientType=adult&organ=liver&sort=rating.
32. Wong MS, Grande DT, Mitra N, et al. Racial differences in geographic access to medical care as measured by patient report and geographic information systems. Med Care. 2017;55(9):817–822. doi:10.1097/MLR.0000000000000774
33. Boscoe FP, Henry KA, Zdeb MS. A Nationwide comparison of driving distance versus straight-line distance to hospitals. Prof Geogr. 2012;64:2. doi:10.1080/00330124.2011.583586
34. Apparicio P, Gelb J, Dube AS, Kingham S, Gauvin L, Robitaille E. The approaches to measuring the potential spatial access to urban health services revisited: distance types and aggregation-error issues. Int J Health Geogr. 2017;16(1):32. doi:10.1186/s12942-017-0105-9
35. https://seer.cancer.gov/registrars/data-collection.html.
36. Sanoff HK, Chang Y, Stavas JM, Sturmer T, Lund J. Effectiveness of initial transarterial chemoembolization for hepatocellular carcinoma among medicare beneficiaries. J Natl Compr Canc Netw. 2015;13(9):1102–1110. doi:10.6004/jnccn.2015.0135
37. https://www.cdc.gov/brfss/annual_data/2013/pdf/codebook13_llcp.pdf.
38. Estevez J, Yang JD, Leong J, et al. Clinical features associated with survival outcome in African-American patients with hepatocellular carcinoma. Am J Gastroenterol. 2018.
39. Kim D, Li AA, Perumpail BJ, et al. Changing trends in etiology-based and ethnicity-based annual mortality rates of cirrhosis and hepatocellular carcinoma in the United States. Hepatology. 2019;69(3):1064–1074. doi:10.1002/hep.v69.3
40. Yu JC, Neugut AI, Wang S, et al. Racial and insurance disparities in the receipt of transplant among patients with hepatocellular carcinoma. Cancer. 2010;116(7):1801–1809. doi:10.1002/cncr.v116:7
41. Pinheiro PS, Williams M, Miller EA, Easterday S, Moonie S, Trapido EJ. Cancer survival among Latinos and the Hispanic Paradox. Cancer Causes Control. 2011;22(4):553–561. doi:10.1007/s10552-011-9727-6
42. Pruitt SL, Tiro JA, Xuan L, Lee SJ. Hispanic and immigrant paradoxes in U.S. breast cancer mortality: impact of neighborhood poverty and hispanic density. Int J Environ Res Public Health. 2016;13:12. doi:10.3390/ijerph13121238
43. Roberts LR, Sirlin CB, Zaiem F, et al. Imaging for the diagnosis of hepatocellular carcinoma: a systematic review and meta-analysis. Hepatology. 2018;67(1):401–421. doi:10.1002/hep.29487
44. Sherman CB, Zhao W, Corley DA, Guy J. Utilization and accuracy of biopsy in patients with hepatocellular carcinoma in a community based setting. J Clin Gastroenterol Treat. 2016;2(2):026. doi:10.23937/2469-584X/1510026
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.