Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Social Inferences as Mediators of Wellbeing in Depression
Authors Giurgi-Oncu C ![]() , Bredicean C, Frandeș M
, Bredicean C, Frandeș M ![]() , Enătescu V
, Enătescu V ![]() , Papavă I
, Papavă I ![]() , Riviș I, Ursoniu S
, Riviș I, Ursoniu S ![]()
Received 1 March 2021
Accepted for publication 29 April 2021
Published 27 May 2021 Volume 2021:17 Pages 1679—1687
DOI https://doi.org/10.2147/NDT.S309009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Cătălina Giurgi-Oncu,1,2 Cristina Bredicean,1,3 Mirela Frandeș,4 Virgil Enătescu,1,2 Ion Papavă,1,2 Ioana Riviș,5 Sorin Ursoniu6
1Department of Neuroscience, Discipline of Psychiatry, “Victor Babeș” University of Medicine and Pharmacy, Timișoara, Romania; 2“Pius Brînzeu” County Emergency Clinical Hospital, Timișoara, Romania; 3“Dr. Victor Popescu” Military Clinical Emergency Hospital, Timișoara, Romania; 4Department of Functional Sciences, Discipline of Medical Informatics and Biostatistics, “Victor Babeș” University of Medicine and Pharmacy, Timișoara, Romania; 5“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; 6Department of Functional Sciences, Discipline of Public Health, Center for Translational Research and Systems Medicine, “Victor Babeș” University of Medicine and Pharmacy, Timișoara, Romania
Correspondence: Cristina Bredicean
Department of Neuroscience, Discipline of Psychiatry, “Victor Babeș” University of Medicine and Pharmacy, No. 2 Eftimie Murgu Square, Timișoara, 300041, Romania
Tel +40722424301
Email [email protected]
Background: Depression is an increasingly prevalent chronic mental health condition that involves a range of potentially negative implications, in the long term. Theory of Mind (ToM) serves to form and maintain social relationships, by accurately identifying thoughts and emotions in others. Defective ToM abilities have been noted in people with a history of clinical depression.
Purpose: To identify whether impairments of emotion recognition are correlated with a lower subjective feeling of wellbeing in people diagnosed with a chronic depressive illness.
Patients and Methods: In a cross-sectional analysis of a recurrent depressive disorder (RDD, as per WHO ICD-10 nosology) cohort (n=57), the BECK depression scale and the “Reading the mind in the eyes” test were employed for the diagnosis of clinical symptoms, and for the evaluation of individual ToM skills, respectively. Wellbeing was quantified using the FANLCT scale.
Results: The wellbeing of service-users decreased significantly, in correlation with their defective emotion recognition abilities. Additionally, a low capacity for the correct perception of emotions in other people appears to significantly influence the social relationships status, with scores of 14.00 (10.00– 18.50) at low capacity vs 23.00 (17.58– 24.75) at normal capacity (Mann–Whitney U-test, p < 0.001). Our study findings indicate that a normal ability for a correct recognition of emotions in others is significantly and strongly correlated with adequate social relationships (Spearman r = 0.757, p < 0.05).
Conclusion: Wellbeing is significantly correlated with the individual ability for a correct recognition of emotions in others.
Keywords: theory of mind, wellbeing, depressive disorder, emotion recognition, social functioning
Introduction
In the evolution of a depressive illness, one of the main therapeutic goals is to reduce its negative impact, while focusing on resuming or enhancing the quality of life of service-users. Health comprises several essential dimensions, ie, the physical, mental, and social aspects that, each, contribute to our wellbeing. In an effort to maintain the status of wellbeing, one must strike a correct balance between these dimensions, and to focus, not merely on living a longer life but, more importantly, on enjoying a healthy and valuable existence.
The quality of our mental health is reflected by our emotions, such as positive/negative self-regard, feelings about day-to-day situations and about others. Emotional health implies an ability to understand emotions, and the proficiency of dealing with routine problems or stress, as well as the ability to study, work, or perform effectively, while maintaining a positive affect, throughout. Emotions are an intricate part of being human, influencing our physical health and global functioning. The literature on this topic considers that facial expressions are an indicator of emotional experience, starting from the assumption that each primary emotion is associated with a unique facial expression pattern.1
The emotional state of wellbeing includes indicators, such as happiness, positive affect, a healthy self-esteem, a complex spiritual life, feelings of safety, and being guarded from excessive stress.2 An awareness and the recognition of our own and others` emotions are essential for the management of the manner that we employ, when seeking to express our own experiences, in the context of social interactions. To be emotionally competent requires an ability to recognize that an emotion is, first and foremost, an experience.3
It has been shown that the cerebellum, together with the frontal lobe and basal ganglia, play an important role in the mechanisms of depression.4 Studies that analyze the different emotional states that people experience have shown that a depressive mood is correlated with the activation of the limbic system and cerebellar hemispheres.5 Other authors have also noted that a depressed mood causes an increase in the anterior region of the vermis.6 In patients with depression, a significant decrease in cerebral and thalamus haemocirculation has been noted, alongside an increase of the haemocirculation in the vermis.7
Depressive disorders are accompanied by a poor affect recognition, namely, a reduction of the abilities that serve to interpret emotional stimuli or infer what others think. These changes lead to a decline in social interactions and psychosocial functioning, generally giving way to isolation, which, in turn, determines a possible relapse or the maintenance of depression.8
The social human being has thoughts, desires, and emotions, which may not be palpable, but are essential in negotiating relationships, and when trying to make sense of what those around us might feel or experience.9 The ability to understand what others think and feel, which, ultimately, translates into the ability “to read the mind” of those around us, is recognized as Theory of Mind (ToM). ToM is a part of social cognition and plays an important role in social functioning and maintaining interpersonal relationships.10 Furthermore, ToM is thought to have two components: an affective and a cognitive one, or, metaphorically speaking, a warm and a cold component. The affective factor is responsible for understanding other people’s emotions, while the cognitive component helps understand others’ cognitive states, beliefs, thoughts, and intentions.
The cerebral structures supporting ToM are represented by a set of brain regions, including the medial prefrontal cortex (mPFC), the area around the posterior superior temporal sulcus (pSTS), the precuneus, and amygdala/temporopolar cortex.11 More specifically, evidence supports the suggestion that dorsal areas are recruited for the understanding of cognitive mental states, while ventral regions are involved in affective state comprehension.12
Although it is a well-known theory that ToM deficits represent a key feature of bipolar disorder,13 anorexia nervosa,14 emotionally-unstable personality disorder,15 antisocial personality disorder,16 schizophrenia and autism spectrum disorders,17,18 the evidence available to date provides contradictory data on the relationship between ToM and depression, with some research reporting that there was no evidence of significant ToM deficits in people with depression.19,20
An adequate ToM, alongside neurocognition, ensures a good social functioning and adequate interpersonal relationships.10 Recurrent depressive episodes are known to have an overabundance of critical negative consequences, not only impacting the physical health in various ways,21 but also progressively leading to cognitive dysfunctions, which are detrimental to social functioning.22 Certain clinical trials involving patients with chronic depressive disorders have shown an impairment in cognitive functioning, as well as emotional processing deficits/empathy that include ToM.23
The present study aims to analyze the relationship between ToM (the affective component) and wellbeing in participants with depressive symptomatology of mild and moderate intensity. We hypothesized that the ability to “read the mind in the eyes” of others would be impaired and that personal wellbeing would be decreased.
Study Design and Participants
The study was conducted on a sample of 57 individuals, selected from the outpatient clinic or the inpatient register of the University Psychiatry Clinic of the “Pius Brinzeu” County Emergency Clinical Hospital of Timisoara, with an existing diagnosis of recurrent depressive disorder (RDD), according to the International Classification of Diseases 10 (ICD-10) criteria,24 aged between 18 and 65 years. All patients had a mental illness history of over two years at the time of the study, and reported, at least, one previous admission in the Timisoara University Psychiatry Clinic. The evaluation was carried out between October-December 2018. The study was conducted as per the Declaration of Helsinki, and an approval was issued by the Local Ethics Committee of the “Pius Brinzeu” County Emergency Clinical Hospital (No. 127/24.08.2017). All patients included in the study provided written informed consents for acquiring, analyzing, and publishing the anonymized data collected either during their hospital admission or from their individual outpatient medical records.
The selection of subjects was based on inclusion/exclusion criteria without using statistical methodology.
Inclusion Criteria
- Subjects diagnosed with a chronic depressive illness, namely, a depressive episode in the context of a Recurrent Depressive Disorder (RDD), according to WHO ICD-10 nosology of mild or moderate intensity (F33.0, F33.1)
- Aged between 18 and 65 years
- Personal history of chronic mental health difficulties (unipolar depression or Recurrent Depressive Disorder) for a minimum of two years
- Subjects who agreed to participate in the study
Exclusion Criteria
- Current severe depressive episode in the context of a Recurrent Depressive Disorder (F33.2 and F33.3) that might distort results, due to the complications associated with the potential co-occurrence of psychotic features
- Comorbid maladaptive personality traits or intellectual difficulties
- Comorbid drug-induced illness
- Underlying organic disorder
Data collection was performed directly, by way of a thorough anamnesis, and by applying standardized psychometric scales and diagnostic tools, as well as from the analysis of individual medical records. At the time of our evaluation, all subjects were diagnosed with a recurrent depressive episode of mild or moderate intensity that required mental health care, either as inpatients in the University Psychiatry Clinic, or as secondary care outpatients in the affiliated Community Mental Health Center.
We collected biographical and sociodemographic data, such as: gender, age, educational level, marital status, professional status, information about personal background, family history of mental health difficulties, previous and current psychotropic/psychotherapeutic treatment, misuse of toxic substances (alcohol, tobacco, psychoactive drugs). For the self-evaluation of the severity of current depressive symptoms, we employed the Beck Depression Scale; ToM was evaluated using the “Reading the mind in the eyes” test; the state of wellbeing was evaluated with the FANLTC scale.
Assessment of Depressive Symptoms
The Beck Depression Inventory (BDI) is a self-evaluation questionnaire that can provide valuable information on the existence of depressive symptoms and their severity. The survey consists of 21 questions. For each question, there are four possible responses, ranging from the absence of the symptom, to an intense level of the same item, chosen depending on the relevance to one’s current mental health status over the course of the previous week.25
Assessment of the Emotion Recognition Capacity
The ability to “read” someone’s mind in their eyes signifies one’s ability to recognize the intentions, the mood, and the beliefs of another person, just by the expression in their gaze. The test was developed by S. Baron-Cohen and included 36 black-and-white images of people’s eyes, each of them suggesting a certain state of mind. Each image corresponds to four possible answers, namely, four emotions.26 The person being tested is asked to look at the images, one by one, to read the four options, and to choose one of these. In case of difficulties understanding any of the words, there is a short definition available for each statement. A score of over 30 points reveals an increased ability to understand what another person thinks; scores between 22 and 30 points show a normal ability to “read” a person’s state of mind by looking into his/her eyes; a score of under 22 points shows a low ability.
The emotions identified by using this test were later regrouped into six fundamental emotions, following psychologist W. Gerrod Parrott’s criticisms, which enabled the more precise assessment of the type of emotion recognized. According to Gerrod Parrott, the six fundamental emotions are love, joy, surprise, anger, sadness, and fear.27
Assessment of Wellbeing
Wellbeing was gauged using the Romanian version of the Functional Assessment of Non-Life-Threatening Conditions (FANLTC) questionnaire, which is a 5-point Likert scale consisting of 26 items, divided into four subscales, with possible responses ranging from 0 (“not at all”) to 4 (“very much”). The four subscales comprise the following: the patient’s physical health level, their psycho-emotional state; their social/family relationships; and functional status. Certain scores require reverse calculating. Higher scores correlate with a higher state of wellbeing.28
Statistical Analysis
Collected data were presented as mean and standard deviations for continuous variables with Gaussian distribution, median and interquartile range (IQR) for continuous variables without Gaussian distribution, or percentage (absolute frequency) for categorical variables. Continuous variable distributions were tested for normality using Shapiro–Wilk’s test and equality of variances using Levene’s test.
The significance of the differences between groups was assessed by applying the Student’s t-test (means, Gaussian populations). The correlation between the measured variables was evaluated using the Spearman rank sum correlation coefficient.
Data were analyzed using the Statistica v7.0 software. A p-value of 0.05 was considered the threshold for statistical significance, and a confidence level of 0.95 was adopted for estimating intervals.
Results
The sociodemographic characteristics are presented in Table 1; they generally comply with the embedded features of depressive disorder. We observed that most of the patients were women (77.5%). The mean age of onset for the first episode of depression was 43.74 (± 9.38) years. Most of the patients were retired (76.5%) and married (70.6%). Also, half of the patients had a basic education level (55.9%), and most of the patients (73.5%) lived in an urban setting. The descriptive statistics for the data related to mental illness are delineated in Table 2; all the results obtained using the assessment scales are presented in Table 3.
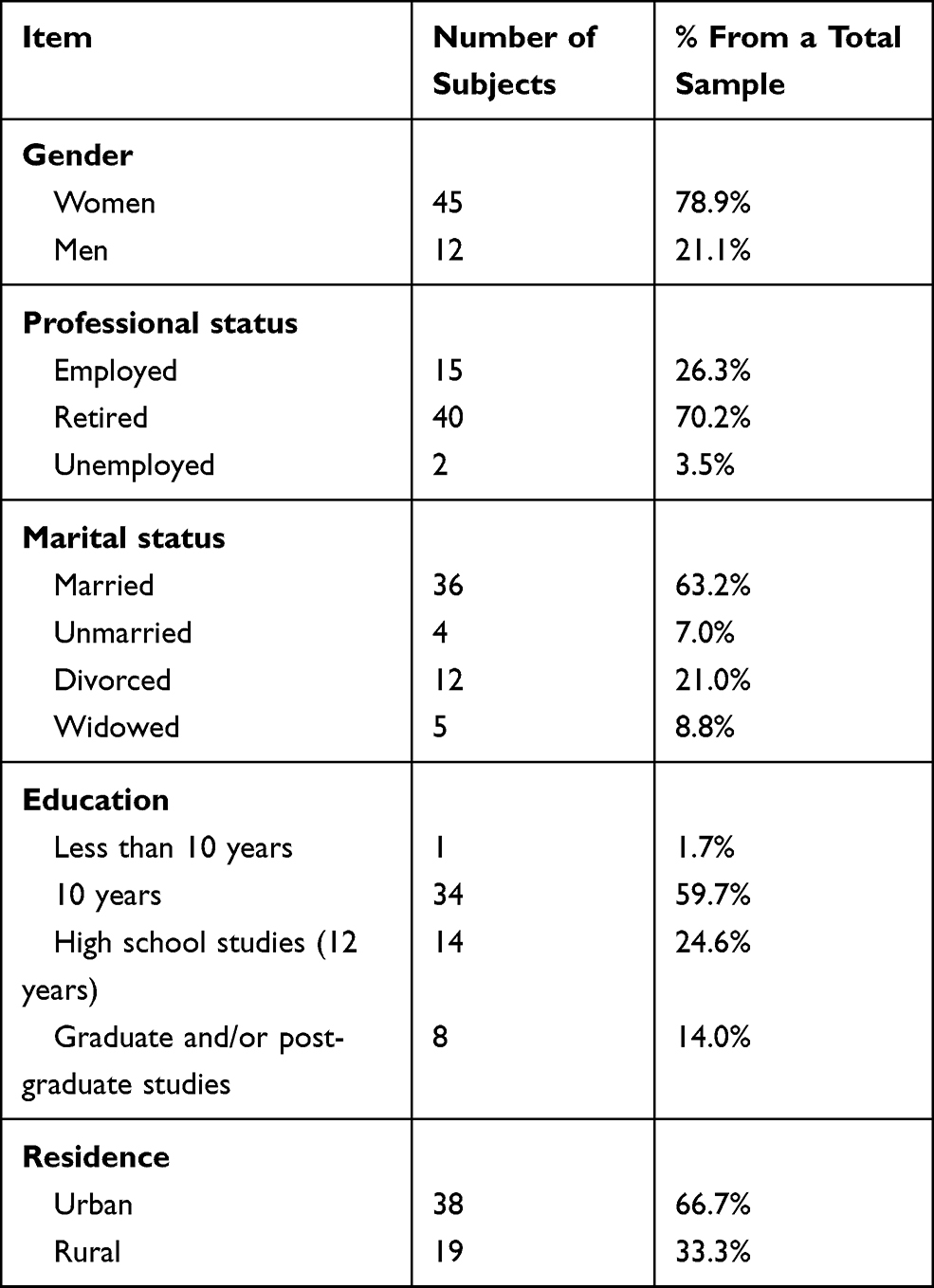 |
Table 1 Characteristics of the Studied Sample |
 |
Table 2 Descriptive Statistics for Data Related to the Mental Illness |
 |
Table 3 Descriptive Statistics Related to the Results Obtained Using the Assessment Scales |
We evaluated the affective component of ToM, noting that 84.21% (48 subjects) of the cohort scored low, in terms of abilities, while the rest maintained normal capacities for emotion recognition. The emotions identified by using the “Reading the mind in the eyes” test were regrouped into the six fundamental emotions, as described by W. Gerrod Parrott, with the most recognizable being “Love” and the least recognizable being “Fear” (Table 4).
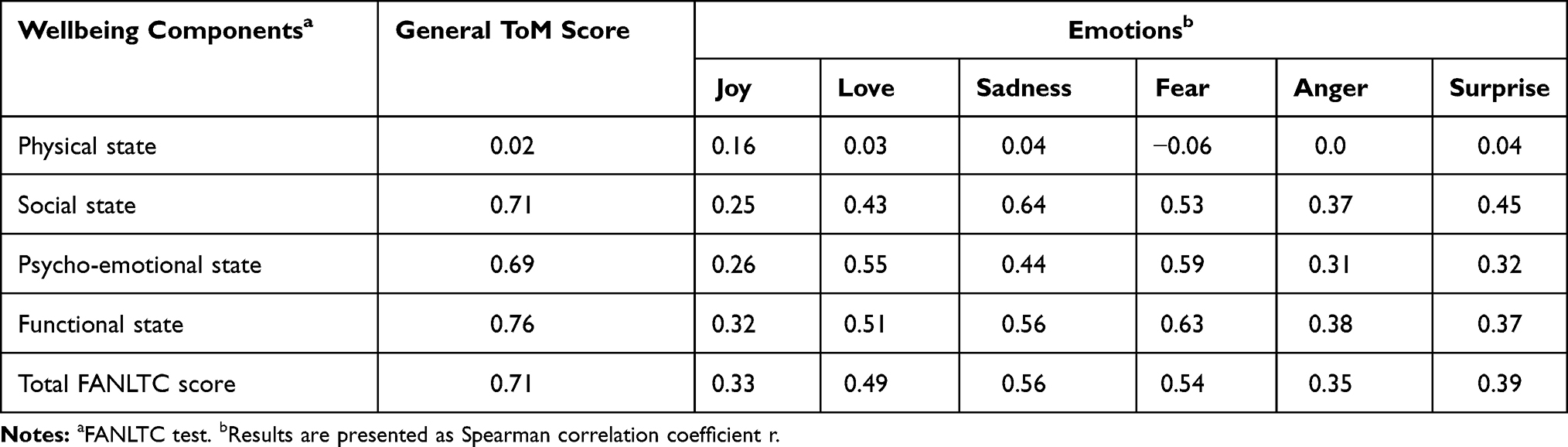 |
Table 4 The Relationship Between the Capacity for Reading Emotions and the Various Wellbeing Components |
Regarding the dimension of wellbeing, the maximum score that could be obtained, showing the highest level of wellbeing, is 104 points. Our study shows that only 17.6% of subjects have scored above 80 points. The average score was 59.4 (standard deviation = 14.9). The FANLCT score is directly proportional to the individual quality of life and wellbeing (Table 4).
Functional wellbeing is negatively influenced (inverse correlation, R= −0.35, p < 0.05) by the number of illness episodes: the higher the number of episodes experienced by a subject, the lower the score of functional wellbeing. The level of depression also inversely correlates with physical wellbeing: the better one feels (subjective physical wellbeing), the lower their level of depression is.
There is no statistically significant correlation between the level of depression (as assessed by the BDI) and the ability to recognize emotions, generally (R = 0.07) or specifically, for the six emotions, as defined by Gerrod Parrott (joy R= 0.01, hate R = −0.05, sadness R = −0.05, fear R = 0.08, surprise R = 0.2, love R = −0.05).
There is a reverse statistically significant correlation (R = −0.35, p< 0.05) between the number of episodes and functional wellbeing: the higher the number of episodes experienced by an individual, the lower his functional wellbeing state will be. This is to be expected; however, the number of years of illness evolution does not correlate significantly with any of the wellbeing scores on these subscales. Also, the illness evolution (in terms of duration and/or the number of episodes) does not seem to correlate with the ability to “read the mind in the eyes” of others.
The ability to correctly identify emotions (ToM) seems to relate to the subjective feeling of wellbeing, as shown by the direct correlation between the “Reading the Mind in the Eye” scale scores and the wellbeing scale scores (R = 0.71, p < 0.05).
The physical wellbeing score is not correlated with the ToM score; therefore, it seems that the ability to “read the mind in the eyes” is not related to the physical state of the subject, but with the social, emotional, and functional state: the higher the scores of these items, the better the scores on the ToM scale.
The correlation between ToM and wellbeing indicates that a low ability to “read the mind in the eyes” corresponds to a low level of wellbeing. However, the strongest correlation that we found was between the functional wellbeing and the ToM scores (R = 0.76, p<0.05), followed by those regarding social wellbeing (R = 0.71, p<0.05). The ability to recognize emotions strongly correlates to the functional and social wellbeing of our study participants. A low ability to recognize emotions impacts negatively upon the functional and social wellbeing of a person. It is interesting to note that the ability to recognize “Fear” has the strongest correlation with the functional wellbeing state of a person (R = 0.63, p<0.05), as well as with the psycho-emotional wellbeing (R = 0.59), while the ability to recognize “Sadness” is strongly related to social wellbeing (R = 0.64, p<0.05).
The t-test (Student) was used for assessing differences between gender groups. No statistically significant differences were found between genders concerning scores on the BDI, FANLTC, and ToM scales.
In conclusion, our results seem to indicate that the ability to correctly discern emotions in others impacts upon personal wellbeing, especially regarding the functional and social subcomponents, with certain emotions (“fear” and “sadness”) making the greatest impact. The current intensity of depressive symptoms does not seem to impact the ability of participants to identify emotions.
Discussion
According to the World Health Organization (WHO), depressive disorders are, currently, the sixth cause of disability, worldwide, in the 24–49 year age group. However, since 1990–2019, depressive disorders have been included in the top ten drivers of increased disease burden, commonly affecting people from teenage years into old age. Moreover, according to the same records, depressive and anxiety disorders were among the top three causes of Disability Adjusted Life Years (DALYs) among females.29 Depressive illness is a recurrent mental health condition that involves significant personal, social, and familial consequences, and is often associated with an unfavorable evolution and prognosis. Since young and middle-aged adults are the most impacted by the onset of depression during their productive years, and beyond the negative impact that depression has on their wellbeing, this also affects their wider social functioning, especially when it comes to the ability to establish or maintain valuable relationships. The state of wellbeing determines our interconnectedness, and our abilities to fulfill our various social, familial, and professional roles. A decrease of our capacities for social engagement and functioning leads to social withdrawal, a reduction in wellbeing, and, possibly, the (re)occurrence of clinical elements of depression, which may, in turn, accentuate the decline in social functioning, therefore creating a vicious cycle.
Our study evaluated the relationship between emotion recognition and wellbeing, the latter being gauged depending on its composing parts, specifically, the physical, social/familial, emotional, and functional areas, in subjects with mild or moderate depressive episodes, starting from the theory that our ability to correctly interpret the emotions of others plays an essential role in achieving and maintaining a state of wellbeing.
The demographic characteristics of the study group showed that most of the subjects were women (76.5%), with an average age of 55.59 years, which is consistent with findings in other studies,30 regarding a higher prevalence and burden of depression in older women. Regarding educational levels, 55.9% of study participants benefitted from an average of 10 years of continuous education, while the rest of the sample reported higher educational achievements (more than 12 years of continuous education). We also noted that most participants (76.5%) were retired at the time of our study, which is reflective of the Romanian social system that is still suffering from a pervasive lack of opportunities for supported employment for people with a chronic mental health diagnosis. In terms of socio-familial functioning, most patients (70.6%) in our study group were married.
The intensity of the current depressive episode was evaluated by calculating the Beck Index, which showed that subjects reported a distress level consistent with, either, a mild or a moderate clinical intensity of symptoms.
Theory of Mind (ToM) has two components: a cognitive section, which is evaluated through the ability to infer other people’s thoughts and, even, to predict their next actions (“mind-reading”), alongside an affective component that evaluates the ability to identify other people’s emotions by analyzing their gaze (“reading the mind in the eyes”).12,31 The two components may exhibit different dynamics within the same mental disorder, namely, one may be modified, while the other remains unchanged, thus allowing us to compare different mental illnesses. The evaluation of individual ToM abilities continues to be of interest in current mental health research, since its deficits impact people suffering with schizophrenia,32 bipolar affective disorder,33 addictive pathologies,34 and depressive disorders,35 alongside other general medical conditions, such as Parkinson’s disease.36 Recent studies have shown that in people suffering with a chronic depressive illness, both, the cognitive and the affective components, are deficient,37 and that a flawed individual ToM might be the culprit for the psychosocial and functional deficits associated with a poor mental health.17,38
In our study, alongside the evaluation of current depressive symptoms, we also sought to analyze the affective component of ToM, which was poor for most of the participants.
Although included in the World Health Organization’s definition of health since 1948,39 in recent years, clinicians and researchers alike have shown an even stronger interest in the concept of physical and mental wellbeing, rather than on merely the treatment of ill health.40 Wellbeing represents a central aspect of mental health, which reflects our clinical goals, in terms of an optimum treatment strategy. This is a complex and multidimensional concept, comprising various emotional, psychological, and social dimensions,41 which can be restored or maintained stable through specific evidence-based psychotherapeutic and medical interventions.42
The results that we obtained by applying the FANLTC questionnaire revealed that most study participants reported a low subjective wellbeing, which should be interpreted considering their current clinical depressive features.
The correct or erroneous recognition of emotions in others determines how we feel, react, and behave towards them, thereby influencing the quality of our relationships and, overall, our social functioning. An adequate social engagement, alongside the ability of correctly identifying emotions in others, helps to achieve a state of wellbeing.43
After compounding all the various emotions that the study sample were asked to analyze into a positive and a negative group, we were able to conclude that the most accurately perceived emotion was “Love”, and the least recognized was “Fear.” “Love” is a complex and, somewhat, problematic emotion, since it can be considered either self-contained or encompassing all other basic emotions. It should also be noted that our group included more women than men, with the former sex potentially situated at an advantage, across the lifespan, in terms of overall “social thinking”,44 and, especially, when faced with having to recognize a positive affect or display subtleties.45 This might also be explained by the fact that most of the study participants were married, which is consistent with findings in literature suggesting that a greater intimate-life satisfaction correlates with a greater expertise in recognizing positive, but not negative, emotions.46 Although “Fear” is a negative emotion that can be regarded as a motivational force, with an important role in interpersonal relationships and when deciding on how to act in a certain situation, current literature on this topic harmonizes with our findings, namely, that this emotion is poorly recognized in major depressive disorders, alongside most other basic emotions, except sadness.47
The severity of depressive symptoms has also been correlated with ToM impairments; the emotion identification deficits increase as the severity of depression increases.35 In this study, no statistically significant correlations have been established between these parameters; this was probably because the subjects included in this study reported mild or moderate depressive symptoms. Also, we did not find the severity of depression as being linked to a differentiation in recognizing the different types of emotions.
Starting from the idea that the presence of depressive elements influences the ability to identify emotions, this study showed a direct correlation between ToM and wellbeing: the higher the capacity of identifying emotions, the higher the wellbeing, including social wellbeing, which is achieved through healthy relationships with family and friends.
Some clinical studies suggest that remitted depression may be related to improved performance in recognizing basic negative emotions, such as “Fear” or “Anger”.48,49 An adequate ability to recognize negative emotions can be correlated with a decrease in the intensity of depression. In this study, subjects who performed best at recognizing the emotion “Sadness” reported an adequate level of social wellbeing and a satisfactory social support system.
All participants were undergoing psychotropic treatment with various types of antidepressants, of which only a few were prescribed a combination of medication and psychological counselling/cognitive behavioural psychotherapy, at the time of inclusion in this study. The number of patients receiving talk therapies was limited, as a direct consequence of the poor provision of such therapies in the public health system, which leaves service-users in the unhelpful and, sometimes, impossible position of having to pay for this privately.
We suggest that future longitudinal studies are required, to compare the ToM abilities/subjective wellbeing correlations found in participants during an acute depressive episode versus when they are in remission.
The methodological limitations of this study are represented by the low number of participants, with a predominance of the female gender, an older average age, and an almost uniform employment status (ie, retired due to age or for health-related reasons - a chronic mental health condition). We would also like to note the absence of a comparison group of service-users with a diagnosis of severe depressive episode (that might have skewed results due to the complications associated with the co-occurrence of psychotic features) or a matched control group.
Conclusions
This study showed that the ability to perceive and correctly identify emotions in other people is impaired for service-users suffering with a mild/moderate depressive episode in the context of a chronic depressive illness. The correlation between ToM abilities and all four FANLTC wellbeing components was also noteworthy, meaning that the state of wellbeing was better, if the person showed an adequate ability to “mind-read” by analyzing the gaze of another. Moreover, our results indicated that, during a depressive episode, existing ToM disabilities impacted the person mostly in terms of aspects relating to the social/familial wellbeing. This suggests the need for more recovery-focused approaches in the provision of mental health care, where, besides the widely available psychotropic treatment, service-users may also potentially benefit from social skills training that may, subsequently, enhance their trust of engaging and persisting in more meaningful and adequate social relationships.
Data Sharing Statement
Data are available upon reasonable request.
Acknowledgments
We thank all the service-users who agreed to participate in this study.
Disclosure
The authors report no conflicts of interest in this work. No funding was received for this research study.
References
1. Keltner D, Sauter D, Tracy J, Cowen A. Emotional expression: advances in basic emotion theory. J Nonverbal Behav. 2019;7:1–28. doi:10.1007/s10919-019-00293-3
2. Grühn D, Kotter-Grühn D, Röcke C. Discrete affects across the adult lifespan: evidence for multidimensionality and multidirectionality of affective experiences in young, middle-aged and older adults. J Res Pers. 2010;44(4):492–500.
3. Garner PW. Emotional competence and its influences on teaching and learning. Educ Psychol Rev. 2010;22(3):297–321.
4. Baron-Cohen S. Theory of mind and autism: a fifteen-year review. Understanding Other Minds. 2000;2:3–20.
5. Fodor JA. The Modularity of Mind. MIT Press; 1983.
6. Corcoran R. Theory of mind in other clinical conditions: is a selective ‘theory of mind’ deficit exclusive to autism. In: Understanding Other Minds: Perspectives from Developmental Cognitive Neuroscience. New York: Oxford Univ. Press. 2000:391–421.
7. Brüne M, Brüne-Cohrs U. Theory of mind—evolution, ontogeny, brain mechanisms and psychopathology. Neurosci Biobehav Rev. 2006;30(4):437–455.
8. Knight MJ, Baune BT. The direct and indirect relationship between social cognition and psychosocial dysfunction in Major Depressive disorder. Front Psychiatry. 2019;17(10):347.
9. Hilbe C, Chatterjee K, Nowak MA. Partners and rivals in direct reciprocity. Nat Human Behav. 2018;2(7):469–477.
10. Tomasello M, Carpenter M, Call J, Behne T, Moll H. Understanding and sharing intentions: the origins of cultural cognition. Behav Brain Sci. 2005;28(5):675–691.
11. Gallagher HL, Frith CD. Functional imaging of ‘theory of mind ’. Trends Cognitive Sci. 2003;7(2):77–83.
12. Shamay-Tsoory SG, Tomer R, Berger BD, Goldsher D, Aharon-Peretz J. Impaired “affective theory of mind” is associated with right ventromedial prefrontal damage. Cognitive Behav Neurol. 2005;18(1):55–67.
13. Kerr N, Dunbar RI, Bentall RP. Theory of mind deficits in bipolar affective disorder. J Affect Disord. 2003;73(3):253–259.
14. Gál Z, Egyed K, Pászthy B, Németh D. Impaired theory of mind in anorexia nervosa. Psychiatria Hungarica. 2011;26(1):12–25.
15. Fonagy P, Leigh T, Steele M, et al. The relation of attachment status, psychiatric classification, and response to psychotherapy. J Consult Clin Psychol. 1996;64(1):22.
16. Dolan M, Fullam R. Theory of mind and mentalizing ability in antisocial personality disorders with and without psychopathy.
17. Bora E, Eryavuz A, Kayahan B, Sungu G, Veznedaroglu B. Social functioning, theory of mind and neurocognition in outpatients with schizophrenia; mental state decoding may be a better predictor of social functioning than mental state reasoning. Psychiatry Res. 2006;145(2–3):95–103.
18. Irani F, Seligman S, Kamath V, Kohler C, Gur RC. A meta-analysis of emotion perception and functional outcomes in schizophrenia. Schizophr Res. 2012;137(1–3):203–211.
19. Bertoux M, Delavest M, de Souza LC, et al. Social cognition and emotional assessment differentiates frontotemporal dementia from depression. J Neurol Neurosurg Psychiatry. 2012;83(4):411–416.
20. Wilbertz G, Brakemeier EL, Zobel I, Härter M, Schramm E. Exploring preoperational features in chronic depression. J Affect Disord. 2010;124(3):262–269.
21. Tudoran M, Tudoran C, Ciocarlie T, Giurgi-Oncu C. Aspects of diastolic dysfunction in patients with new and recurrent depression. PLoS One. 2020;15(1):e0228449.
22. Evans VC, Iverson GL, Yatham LN, Lam RW. The relationship between neurocognitive and psychosocial functioning in major depressive disorder: a systematic review. J Clin Psychiatry. 2014;75(12):1359–1370.
23. Bailey PE, Henry JD. Growing less empathic with age: disinhibition of the self-perspective. J Gerontol B Psychol Sci Soc Sci. 2008;63(4):P219–26.
24. World Health Organization. International Classification of Diseases ICD10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. World Health Organisation; 1993.
25. Beck AT, Steer RA, Brown G. Beck depression inventory–II. Psychol Assess. 1996.
26. Baron-Cohen S, O’riordan M, Stone V, Jones R, Plaisted K. Recognition of faux pas by normally developing children and children with Asperger syndrome or high-functioning autism. J Autism Dev Disord. 1999;29(5):407–418.
27. Parrott WG, editor. Emotions in Social Psychology: Essential Readings. Psychology Press; 2001.
28. Cella D, Nowinski CJ. Measuring quality of life in chronic illness: the functional assessment of chronic illness therapy measurement system. Arch Phys Med Rehabil. 2002;1(83):S10–7.
29. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
30. Barry LC, Allore HG, Guo Z, Bruce ML, Gill TM. Higher burden of depression among older women: the effect of onset, persistence, and mortality over time. Arch General Psychiatry. 2008;65(2):172–178.
31. Shamay-Tsoory SG, Shur S, Barcai-Goodman L, Medlovich S, Harari H, Levkovitz Y. Dissociation of cognitive from affective components of theory of mind in schizophrenia. Psychiatry Res. 2007;149(1–3):11–23.
32. Bora E, Pantelis C. Theory of mind impairments in first-episode psychosis, individuals at ultra-high risk for psychosis and in first-degree relatives of schizophrenia: systematic review and meta-analysis. Schizophr Res. 2013;144(1–3):31–36.
33. Bora E, Bartholomeusz C, Pantelis C. Meta-analysis of Theory of Mind (ToM) impairment in bipolar disorder. Psychol Med. 2016;46(2):253–264.
34. Bosco FM, Capozzi F, Colle L, Marostica P, Tirassa M. Theory of mind deficit in subjects with alcohol use disorder: an analysis of mindreading processes. Alcohol Alcoholism. 2014;49(3):299–307.
35. Bora E, Berk M. Theory of mind in major depressive disorder: a meta-analysis. J Affect Disord. 2016;1(191):49–55.
36. Romosan AM, Dehelean L, Romosan RS, Andor M, Bredicean AC, Simu MA. Affective theory of mind in Parkinson’s disease: the effect of cognitive performance. Neuropsychiatr Dis Treat. 2019;15:2521.
37. Wang YY, Wang Y, Zou YM, et al. Theory of mind impairment and its clinical correlates in patients with schizophrenia, major depressive disorder and bipolar disorder. Schizophr Res. 2018;1(197):349–356.
38. Bora E, Veznedaroğlu B, Vahip S. Theory of mind and executive functions in schizophrenia and bipolar disorder: a cross-diagnostic latent class analysis for identification of neuropsychological subtypes. Schizophr Res. 2016;176(2–3):500505.
39. Huber M, Knottnerus JA, Green L, et al. How should we define health? BMJ. 2011;26:343.
40. Prince M, Patel V, Saxena S, et al. No health without mental health. The Lancet. 2007;370(9590):859–877.
41. Seligman ME. Flourish: a visionary new understanding of happiness and well-being. Policy. 2011;27(3):60–61.
42. Slade M, Oades L, Jarden A, editors. Wellbeing, Recovery and Mental Health. Cambridge University Press; 2017.
43. Brackett MA, Rivers SE, Shiffman S, Lerner N, Salovey P. Relating emotional abilities to social functioning: a comparison of self-report and performance measures of emotional intelligence. J Pers Soc Psychol. 2006;91(4):780.
44. Turkstra LS, Mutlu B, Ryan CW, et al. Sex and gender differences in emotion recognition and theory of mind after TBI: a narrative review and directions for future research. Front Neurol. 2020;4(11):59.
45. Donges US, Kersting A, Suslow T. Women’s greater ability to perceive happy facial emotion automatically: gender differences in affective priming. PLoS One. 2012;7(7):e41745.
46. Petrican R, Moscovitch M, Grady C. Proficiency in positive vs. negative emotion identification and subjective well-being among long-term married elderly couples. Front Psychol. 2014;28(5):338.
47. Dalili MN, Penton-Voak IS, Harmer CJ, Munafò MR. Meta-analysis of emotion recognition deficits in major depressive disorder. Psychol Med. 2015;45(6):1135–1144.
48. Anderson IM, Shippen C, Juhasz G, et al. State-dependent alteration in face emotion recognition in depression. Br J Psychiatry. 2011;198(4):302–308.
49. LeMoult J, Joormann J, Sherdell L, Wright Y, Gotlib IH. Identification of emotional facial expressions following recovery from depression. J Abnorm Psychol. 2009;118(4):828.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.