Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Social-Emotional Development and Associated Risk Factors in Chinese Toddlers with Cerebral Palsy
Authors Wu Y, Tang J, Chen Y, Huang Y ![]()
Received 24 February 2021
Accepted for publication 12 July 2021
Published 24 July 2021 Volume 2021:17 Pages 2451—2463
DOI https://doi.org/10.2147/NDT.S308138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yu-Ping Ning
You Wu,1,* Jianyong Tang,2,* Yanni Chen,3 Yanxia Huang4
1Department of Neurology, Xi’an Children’s Hospital, The Affiliated Children’s Hospital of Xi’an Jiaotong University, Xi’an, 710003, Shaanxi, People’s Republic of China; 2Department of Laboratory Medicine, Xi’an Children’s Hospital, The Affiliated Children’s Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 3Department of Children’s Health Care, Xi’an Children’s Hospital, The Affiliated Children’s Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 4Department of Rehabilitation, Xi’an Children’s Hospital, The Affiliated Children’s Hospital of Xi’an Jiaotong University, Xi’an, 710003, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanxia Huang Email [email protected]
Objective: This study aimed to analyze the social-emotional behaviors of Chinese toddlers with cerebral palsy and to identify the risk factors associated with these behaviors.
Methods: A total of 300 Chinese toddlers and their parents were recruited in this study. A Chinese version of the Infant-Toddler Social-Emotional Assessment was used to assess the children and basic information and clinical data were collected using an author-designed questionnaire. The patients were also assessed using a coping style questionnaire and the hospital anxiety and depression scale. Multiple logistic regression analysis was performed to identify risk factors.
Results: The scores of the externalizing and competence domains for Chinese toddlers with cerebral palsy at different ages were lower compared to healthy children of the same age and gender (p< 0.05). For the boys with cerebral palsy aged between 12– 17 and 18– 23 months, the scores of the internalizing and dysregulation domains were significantly lower compared to the national normal (p< 0.01). The effect of perinatal factors on the externalizing and competence domains was more significant compared to other domains, whilst the coping style of the parents significantly affected the dysregulation domain (p=0.001). Multivariate analysis showed that the parental emotional state, education level, coping style and perinatal factors were closely associated with the social-emotional problems of children with cerebral palsy.
Conclusion: Children with cerebral palsy are more likely to have behavioral, emotional, and psychiatric issues that are mostly ignored. These children may benefit from early screening and intervention for risk factors to improve rehabilitation and long-term prognosis.
Keywords: cerebral palsy, social-emotional development, Chinese children, cross-sectional study
Introduction
Cerebral palsy (CP) describes a group of lifelong conditions that are characterized by abnormal tone, posture and movements. CP occurs in two to three infants per 1,000 live births and is clinically classified based on the predominant motor syndrome including spastic hemiplegia, spastic diplegia, spastic quadriplegia, and extrapyramidal or dyskinetic.1,2 The prevalence of cerebral palsy in China is 2.07‰, and the prevalence of CP is higher in males compared to females and is also higher in rural areas compared with urban areas.3 The disability rate caused by CP is 42–45%. Severe disabilities in children have huge economic and social impacts on patients, families and caregivers.4 Many previous reports have focused on identifying risk factors for CP and developing approaches for early diagnosis, and rehabilitation of motor functions.5,6 Recently, the abnormal psychological and behavioral problems displayed by children with CP have attracted significant research attention.7
Up to one in four children with CP have behavioral or emotional issues.8 Many children also meet the criteria for comorbid psychiatric diagnoses such as attention-deficit/hyperactivity disorder, conduct disorders, anxiety, and depression, which can lead to decreased well-being in children and can compromise the quality of life for family members.9 In these children, the disease itself is a particularly important factor that affects and limits the social development of their emotions. Physical activity dysfunction and associated cognitive decline, audio-visual disorders, logopathy, and perceptual disorders may impede the normal development of emotional sociality in children with CP.10 Unfortunately, most social-emotional problems in children with CP during childhood are neglected.11 Also, when social-emotional problems occur earlier, children often have more significant problems that directly affect the efficacy of clinical rehabilitation therapy. Therefore, the early evaluation of these conditions is recommended to assure early access to resources and associated treatments.
Previously it has been shown that more than 40% of preschool children with CP have significant psychological and behavioral issues at a frequency of three times the rate of normal children.12 However, there is a lack of detailed, comprehensive and scientific evidence on the emotional problems in toddlers with CP in China and around the world. This study aimed to provide comprehensive theoretical support to understand the current situation and factors affecting toddlers with CP in China. Moreover, we aimed to develop a novel strategy to detect the early warning signs of emotional problems in children with CP and to inform the implementation of targeted interventions and treatments.
Materials and Methods
Study Participants
This cross-sectional study was conducted in the Neurology and Rehabilitation Department of the Xi’an Children’s Hospital from June 2015 to December 2018 using a convenience sampling method. Children with CP aged between 1–3 years and their parents were enrolled in this study. The inclusion criteria for children with CP were: i) compliance with the diagnostic criteria for CP discussed and approved in the 2014 China National Conference on Rehabilitation of Children with CP and illustrated in the China CP Rehabilitation Guidelines (2015): Part I;2 ii) Children with a Developmental Quotient >55 evaluated using the Gesell scale; iii) Children without serious genetic or metabolic diseases; iv) Children without organic lesions in important organs such as heart, liver, or kidneys; v) Children without serious limb deformities and other serious organic diseases such as visual impairment or hearing disorders; vi) Parents who can read and independently complete questionnaires; vii) Parents signed informed consent and volunteered to participate in the study. The exclusion criteria for the subjects were: i) Children whose parents refused to cooperate during the study; ii) Children with other complications who could not participate in the survey; iii) Children whose family suffered from other serious incidents resulting in the inability to complete the questionnaire.
Before the questionnaire survey, the parents were fully informed of the purpose and significance of this study and written informed consent was obtained. To reduce the bias resulting from the differences in understanding of the questionnaire content due to differences in the education levels of parents, the survey contents were explained in detail before completion. All data were anonymized before analysis. This study was conducted in accordance with the Declaration of Helsinki, and the study design and the proposal implementation were approved by the Medical Ethics Committee of the Children’s Hospital of Xi’an Jiaotong University (approval number: 201503).
Measures
The General Information Survey was used as a measurement tool for child subjects in this study that was designed by our investigators for this study. This was mainly used to collect data on the demographics (eg, age, sex, whether the only child, parent’s age, parent’s education level, provider payment, parental rearing style, caregiver, entertainment activity) and clinical medical characteristics (general condition of gestation period, birth status, type of cerebral palsy, concomitant symptom, auxiliary examination, rehabilitation therapy) of the subjects. The standardized Chinese Version of Infant Toddler Social-Emotional Assessment (CITSEA) based on the version from Yale University and standardized for Chinese children was used to assess a broad range of social-emotional and behavioral problems and competencies from 12 to 36 months of age.13 The CITSEA social-emotional items addressed four behavioral domains (subdomains in parentheses), specifically, Externalizing (activity-impulsivity, aggression/defiance, and peer aggression), Internalizing (depression/withdrawal, separation distress, general anxiety, and inhibition to novelty), Dysregulation (sleep, eating, negative emotionality, and sensory sensitivity), and Competence (compliance, attention, imitation/play, empathy, prosocial peer interactions, and mastery motivation). Primary caregivers rated 166 items according to the degree to which their children exhibited certain behavior and emotional characteristics during the last month, using a three-point scale ranging from 0 = Not true/rarely, 1 = Somewhat true/sometimes, to 2 = Very true/often. Also, nine items had a N = No opportunity code to account for instances when the primary caregiver had no opportunity to observe the particular behavior. A three-level scoring method was used in the scale to calculate the initial total score of each dimension which was then converted to the average raw score of each domain into a normal standard T-score where the mean was 50 and the standard deviation is 10. Each domain of the social-emotional development score was classified as negative and positive according to the critical value of the T-score. For the problem domain (externalizing behavior, internalizing behavior and dysregulation domains), a T-score > 63 was determined as positive, where the higher T-score indicated the worse problem. A T-score < 37 for the competence domain is positive and lower scores indicated worse problems.
The coping style questionnaire was used as a self-reported behavioral assessment scale that is based on the existing theory and scale of foreign countries. This was combined with the cultural and social background to capture the actual situation in China.14 The coping style questionnaire assessed 6 factors, specifically i) Problem solving, ii) Self-blame, iii) Seeking help, iv) Fantasy, v) Retreat, and vi) Rationalization. According to the score for each factor, the coping style was divided into three types; mature (Problem-solving – Seeking help), immature (Self-blame – Fantasy - Retreat) and mixed (Rationalization).
The hospital anxiety and depression scale (HADS) is a tool that was originally proposed by Zigmond and Snaith in 1983 for the rapid screening of emotional disorders such as anxiety and depression in patients displaying symptoms of physical illness.15 In this study, anxiety and depression were measured in parents using a Chinese version of the HADS (C-HADS) that has become widely used in China.16,17 The scale is divided into an anxiety subscale (C-HADS-A) and a depression subscale (C-HADS-D), each of which contains 7 sub-items and a total of 14 items. The items are presented in the form on a 4-point Likert scale ranging from 0 to 3. The recommended cutoff score is ≥8 and the scores are classified as follows: 0–7 was considered asymptomatic, 8–10 indicated suspicious symptoms and 11–21 indicated confirmed symptoms.
Data Collection and Statistical Analysis
The procedures used in this study under strict quality control as shown in Additional File 1. EpiData Software 3.0 was used for data entry and management. Trained investigators were responsible for collecting and inputting all of the questionnaire data. Statistical analysis was performed using IBM SPSS Statistics for Windows software, version 21.0 (IBM Corp, Armonk, NY). Data are expressed as the means with standard deviations, medians with interquartile ranges, or frequency with percentages, depending on the distribution of the data. The statistical differences between the sample and the normal data were compared using a one-sample t-test and the differences between two subject groups were compared using an unpaired t-test. Statistical comparisons across multiple groups were conducted using a one-way analysis of variance followed by an LSD t-test for pairwise comparisons. The measurement data were analyzed using a chi-square test or Fisher exact test. The univariate analysis indicators with significant differences were included as independent variables in the multiple logistic regression model. Three methods (enter model, backward elimination method, and forward elimination method) were used to screen the risk factors associated with the positive results of each domain. At each step of the selection process, the variables with p<0.05 were included in the equation and the variables with p>0.10 were excluded until all of the included variables conformed to the demand for model establishment. Then, the model was evaluated for goodness of fit. Statistical significance was defined as p-values of <0.05.
Results
Participants and Demographic Characteristics
Based on the inclusion and exclusion criteria, a total of 322 children with CP were investigated in this study and 22 invalid questionnaires were excluded. The final study included 300 children aged 1–3 years, amongst whom 192 were male (64.0%) and 108 were female (36.0%). Among these children, 148 (49.3%) were aged 12–17 months, 68 (22.7%) were aged 18–23 months, 64 (21.3%) were aged 24–29 months and the remaining 20 (6.7%) children were aged 30–36 months. The birth weight of the children ranged from 1.10 kg to 5.30 kg with a mean of (3.15±0.66) kg. There were 68 premature infants (22.7%) and 28 infants born with asphyxia (48.8%). Spastic tetraplegia was the main type of clinical classification observed in 45.3% of the children. 196 (65.3%) children had complications of which 168 (56.0%) had dysfluency. 36 cases (12.0%) presented with EEG abnormalities. Also, 10.7% of the children had visual and auditory evoked potential abnormalities. The demographic characteristics of the subjects recruited in this study are shown in Table 1.
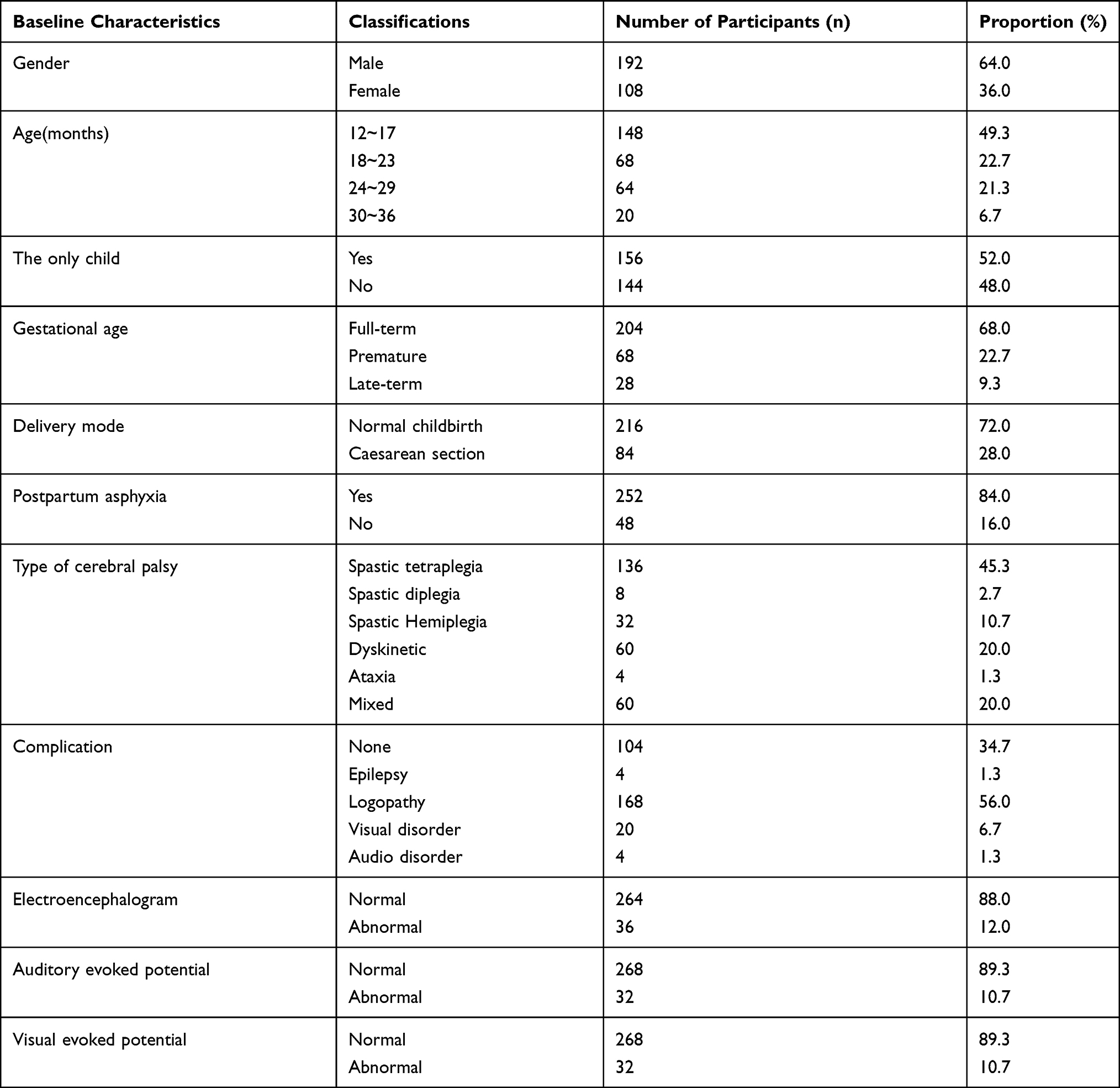 |
Table 1 Basic Information on Children with Cerebral Palsy (n=300) |
Comparison of the Scores of Social-Emotional Development in Children with CP Compared to the National Normal
The scores from the CITSEA showed that amongst the 300 subjects, the positive rate in the externalizing behavior domain was 16.0% (48 cases), the rate in the internalizing behavior domain was 8.0% (24 cases), the rate in the dysregulation domain was 10.7% (32 cases) and the rate in the competence domain was 13.3% (40 cases). Our results showed that the scores of the externalizing behavior and the competence domains for the boys and girls with CP in different age groups were significantly lower compared to healthy children of the same age and gender. For the scores in the internalizing and dysregulation domains, no significant difference was observed in the girls with CP in all age groups based on the national normal. Furthermore, the scores of the boys with CP aged 12 and 23 months were significantly lower than the normal which was not found in those aged 24–36 months (Figure 1).
 |
Figure 1 Comparison of the scores of each dimension of social-emotional development in children with cerebral palsy (CP) and the national normal. (A1–A4) Scores of externalizing, internalizing, dysregulation, and competence domains for boys with CP and the national normal, respectively. (B1–B4) Scores for the externalizing, internalizing, dysregulation, and competence domain for girls with CP and the national normal, respectively. All data are represented by mean ± SD values. *Indicates p < 0.05 and **p < 0.01. |
Analysis of the Clinical Features Affecting the Social-Emotional Development of the Children with CP
The t-test or the one-way analysis of variance showed that the gender difference in the children with CP affected the scores in the internalizing and dysregulation domains, ie the scores for the girls were significantly higher compared to boys (p<0.001 and p=0.011, respectively). Also, a trend of increasing scores was observed in older children. The clinical classification and the birth gestational age significantly affected the four domains of the social-emotional development in children with CP. Preterm infants with CP had higher scores in the problem domain and lower scores in the competence domain compared to full-term and late-term infants. The children with CP who suffered from postpartum asphyxia had lower scores in the externalizing and competence domains. Amongst the children with CP, those with abnormal electroencephalograms had significantly higher scores in the dysregulation domain compared to children with normal electroencephalograms (t=−5.14, p<0.001) (Table 2).
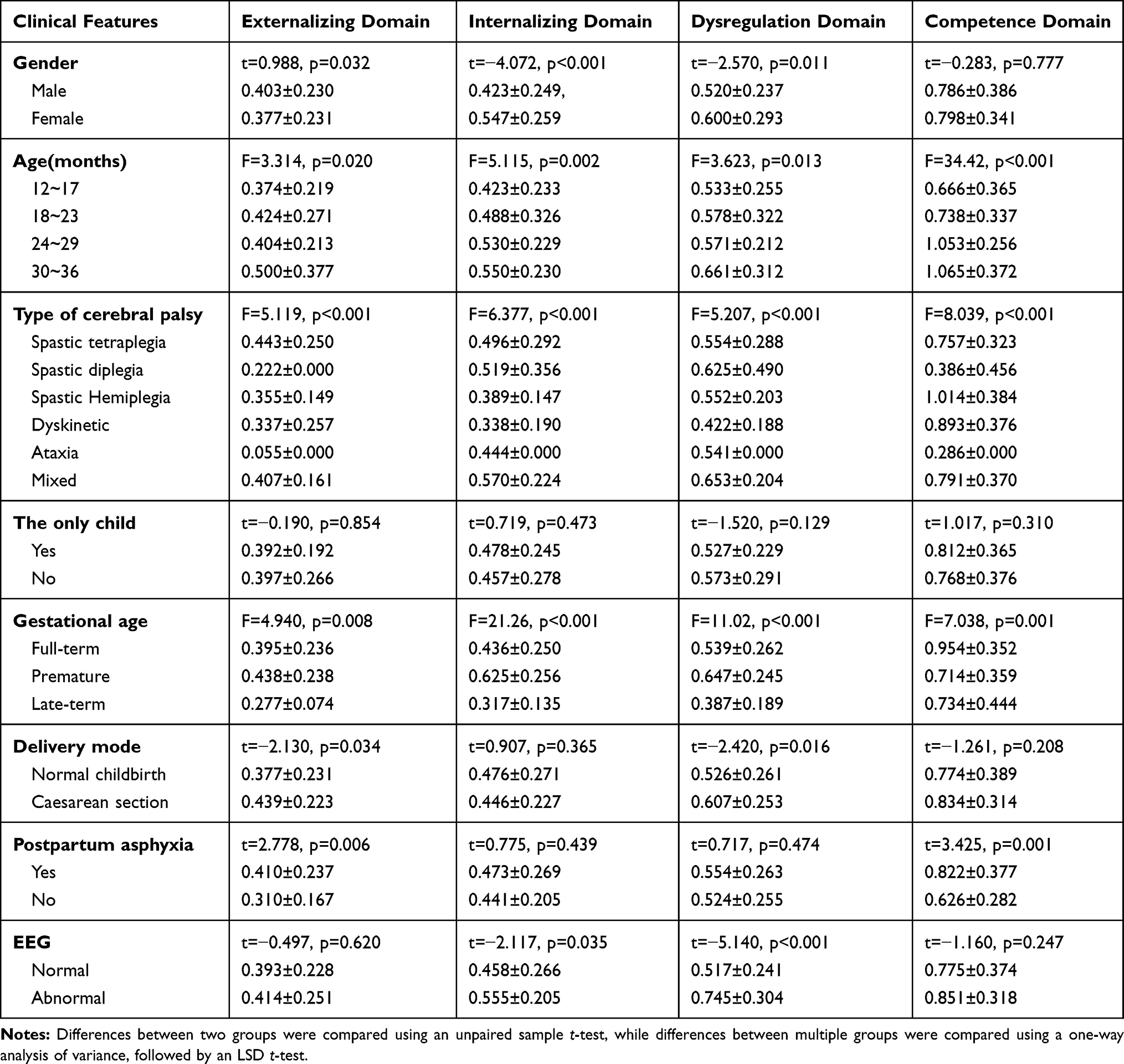 |
Table 2 The Effect of General Clinical Features of Children with Cerebral Palsy on the Score of the Social-Emotional Development Scale |
The Effect of the Family-Social Demographic Characteristics on the Social-Emotional Development of the Children with CP
In this study, a one-way analysis of variance followed by an LSD t-test was used to evaluate the effect of the family-social demographic characteristics on the social-emotional development scale for children with CP. Our results showed that parental age and education level, parenting style, recreational activity, and the caregiver of the children could significantly affect the scores in the externalizing domain of the child subjects. Statistically significant differences in the scores of the internalizing domain were observed amongst the groups of caregivers, maternal age and paternal educational level. A significant difference was found in the scores of the dysregulation domain between each group for the maternal education level. The parental coping style and the frequency of children’s participation in social entertainment activities could significantly affect the scores in the competence domain (Table 3).
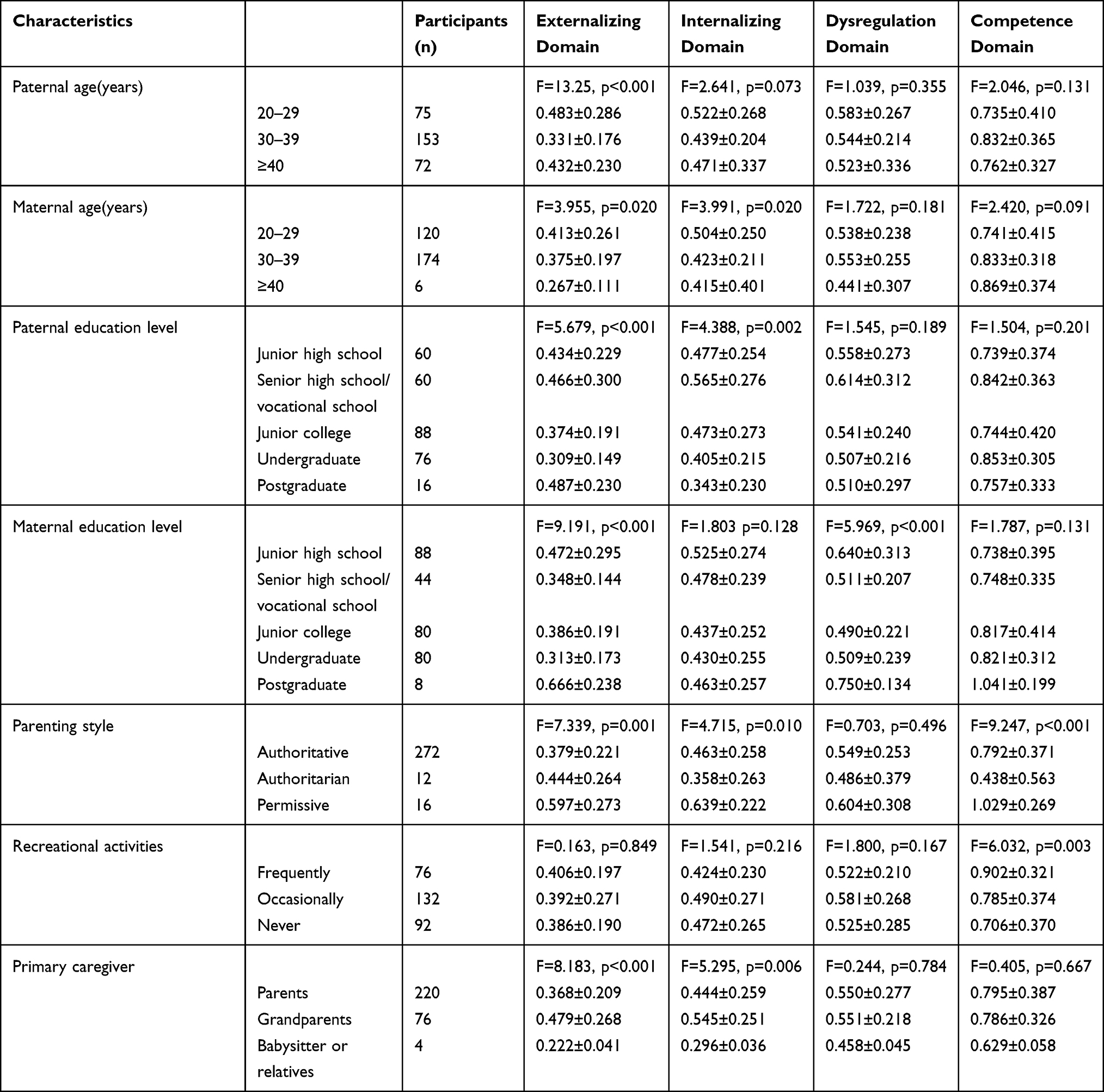 |
Table 3 The Effect of Family Social Demographic Characteristics on the Score of Social Emotional Development for Children with Cerebral Palsy |
Correlation analysis between the scores of the parental coping style and the four domains of social-emotional development in the subjects was performed using a chi-square test. The coping styles were mature in 76 (25.3%) parents, immature in 168 (56.0%) parents and mixed in 56 (18.7%) parents. Data analysis showed that the parental coping style significantly affected the positive detection rate in the dysregulation domain (p=0.001). The rate for parents who showed a mixed coping style was significantly higher than the other two groups whilst the effect on the rates of the other domains was not statistically significant (Table 4).
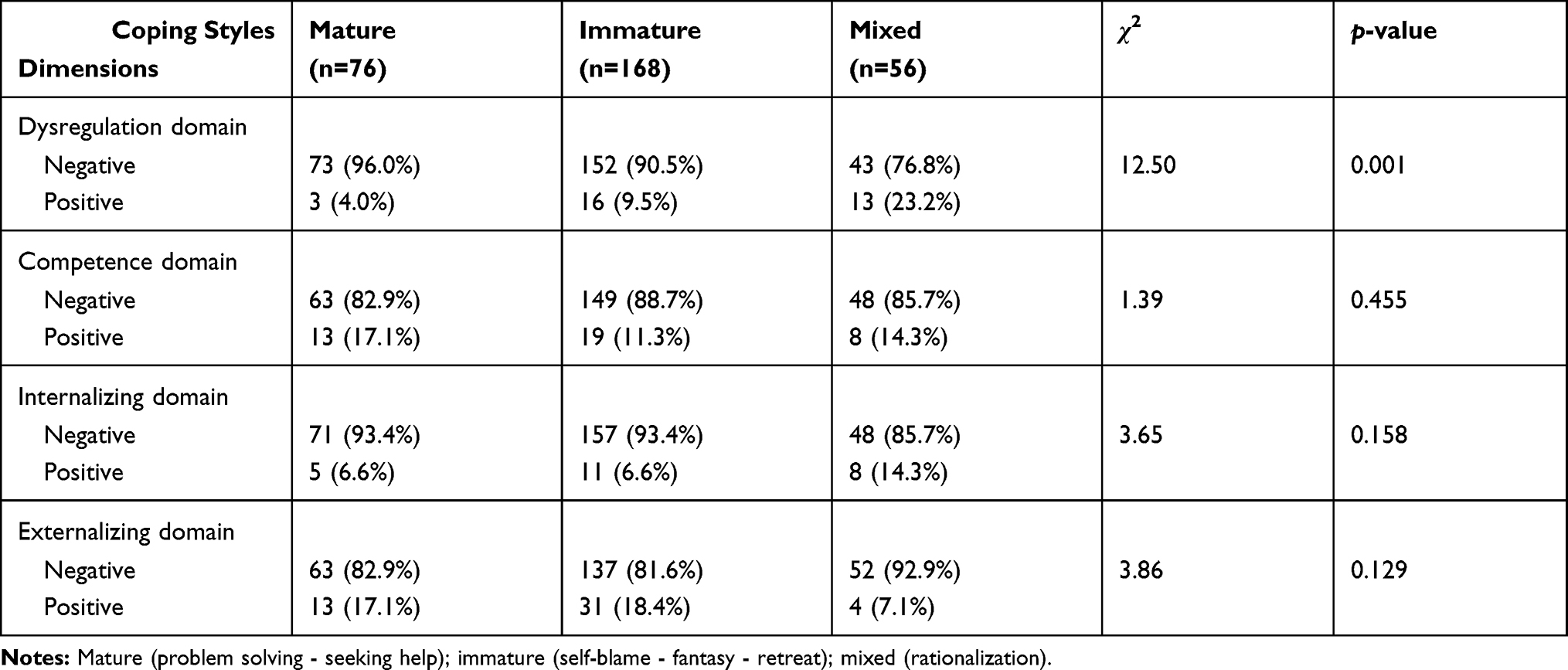 |
Table 4 The Relationship Between Parental Coping Styles and Positive Detection Rates |
The Effect of Parental Anxiety and Depression on the Positive Detection Rate of Social-Emotional Development in the Children with CP
For 48 children with CP, the externalizing domain was positive and in all cases the parents showed positive symptoms of anxiety and depression. When the mothers had anxiety, the positive detection rate in the internalizing, dysregulation and competence domains for the child subjects were 33.3% (8/24), 50.0% (16/32) and 50.0% (20/40), respectively. The corresponding rates of maternal depression were 66.6% (16/24), 68.8% (22/32) and 50.0% (20/40), respectively. When the fathers had psychological disturbances, the positive detection rates in each domain were 33% (8/24), 25% (8/32) and 50% (20/40) for paternal anxiety, respectively. The rates of paternal depression were 50% (12/24), 50% (16/32) and 50% (20/40), respectively (Figure 2).
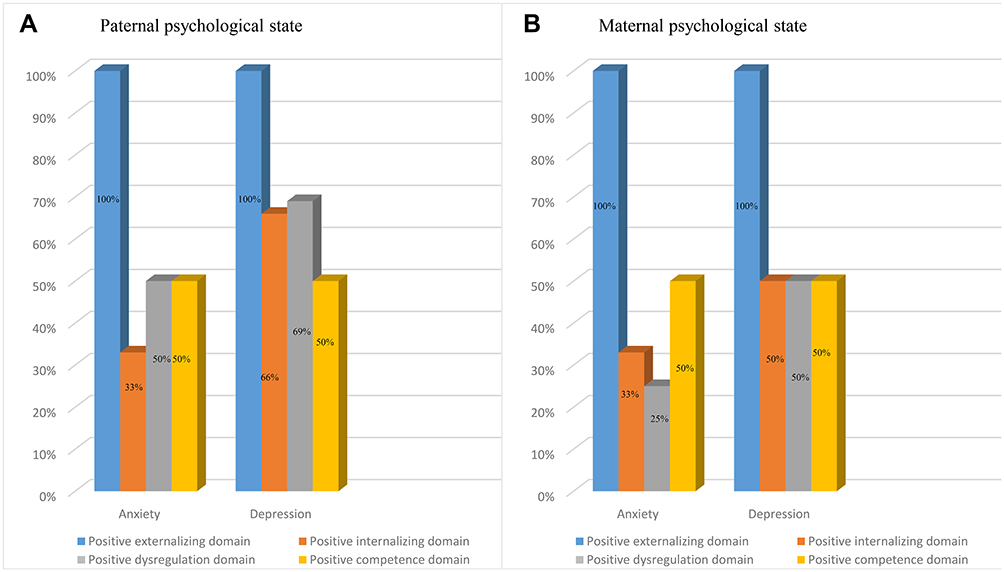 |
Figure 2 The effect of parental anxiety and depression on the positive detection rate of social emotional development in children with cerebral palsy (CP). (A) Correlations between paternal psychological state (anxiety and depression) and the positive detection rate of each domain for social emotional development in children with CP. (B) Correlations between the maternal psychological state (anxiety and depression) and the positive detection rate of each domain for social emotional development in children with CP. |
Multivariate Logistic Regression Analysis of the Influencing Factors of Social-Emotional Development
As shown in Table 5, amongst the independent variables, the risk of externalizing behavior in children delivered by caesarean section was 2.5 times higher compared to naturally delivered children (OR=0.501, 95% CI:1.225~5.107). Concerning the influence of caregivers, children who were looked after by their grandparents, babysitters or relatives showed a doubled risk of positive externalizing behavior compared to other subjects (OR = 1.893, 95% CI: 0.977~3.667). Birth weight, gestational age, and maternal education level were identified as protective factors for the occurrence of externalizing behavior.
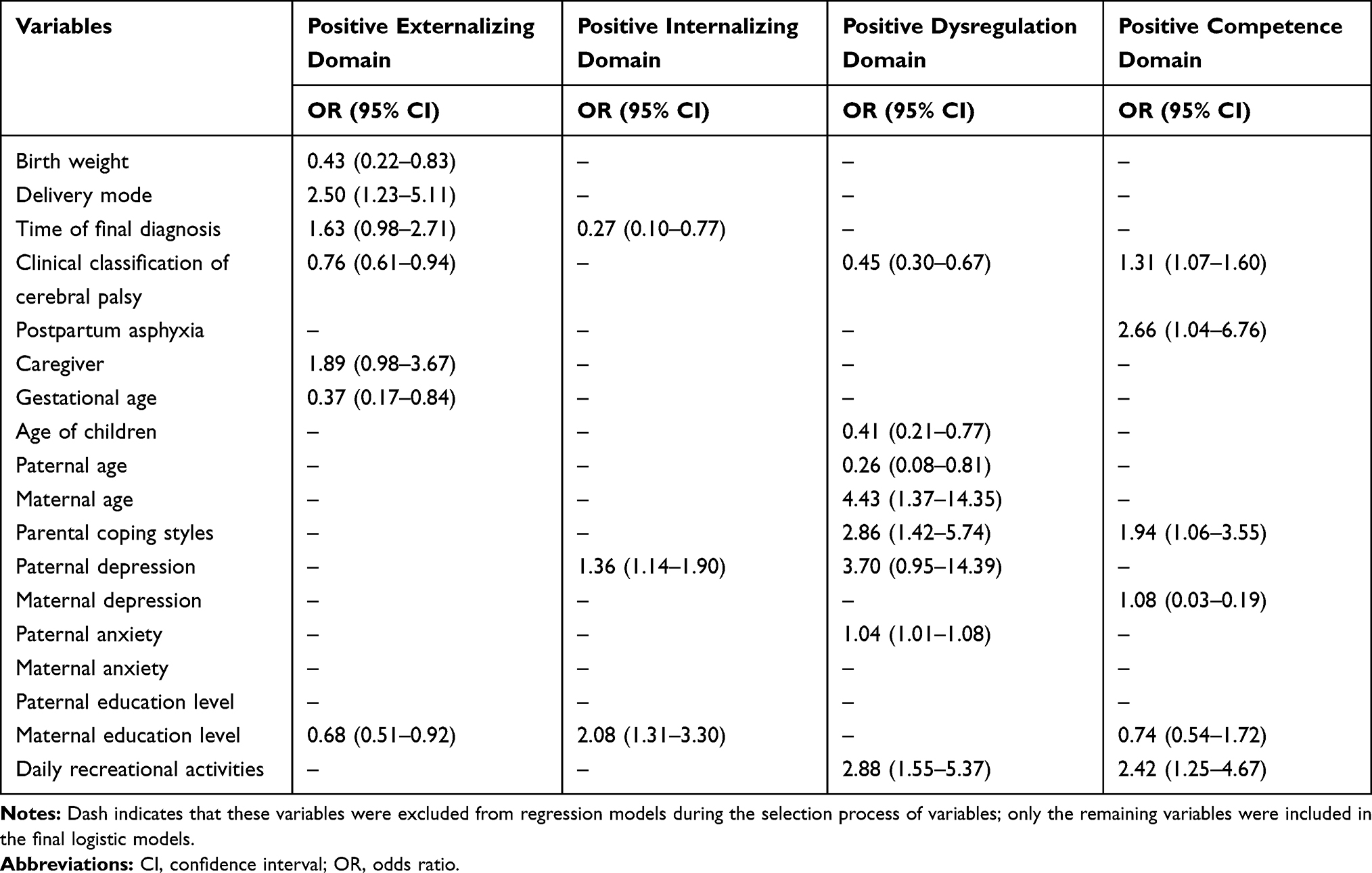 |
Table 5 Multivariate Logistic Regression Analysis of Independent Risk Factors for the Positive Domains of Children with Cerebral Palsy |
In the positive internalizing domain, the OR for the time of final diagnosis was < 1 if other variables were maintained under control. Earlier diagnosis had a lower positive rate. Maternal education level is also an independent risk factor affecting the ability of children to internalize emotions. Children whose mothers were educated to high-school level or below had a one-fold increase in the prevalence of the positive internalizing domain compared to those with college degrees or above (OR=2.083, 95% CI: 1.315~3.301). Paternal depression is another independent variable related to the positive internalizing domain that was responsible for a 1.37-fold higher risk compared to children whose fathers had no signs of depression.
With increasing age, the risk of detection in the dysregulation domain was reduced (OR=0.406, 95% CI: 0.214~0.772) (p=0.006). Compared to children with spastic quadriplegia, the prevalence of the positive dysregulation domain in children with other types of CP was relatively low (OR=0.447, 95% CI: 0.297~0.673). Interestingly, we found that maternal age was positively correlated with the risk of detection, whilst an increase in paternal age led to a relative reduction in risk. Also, paternal anxiety and depression lead to a 0.04-fold and 2.7-fold increase in the positive rate of dysregulation domain in the children, respectively.
Lastly, children with CP who experienced postnatal asphyxia had a 2.6 times risk of disability compared to those with no asphyxia. Compared to children who regularly participate in social recreational activities, those with occasionally or not involved in recreational activities had a higher risk in the positive competence domain (OR = 2.418, 95% CI: 1.253~4.665). Moreover, maternal depression was positively related to children’s disabilities.
Discussion
In this study, we investigated the clinical features and the related factors that may influence the social-emotional behavior in children with CP. Our results showed that the scores of externalizing behaviors and competence domains in the children with CP were significantly lower compared to healthy children of the same age and gender. These data suggest that children with CP have low activity, weak impulses and lower levels of aggression. The clinical classification of CP and the gestational age of the children significantly affected the scores in the four domains of social-emotional development.
Social-emotional development establishes the basis for young children to form healthy personality characteristics and good social adaptability behaviors. The occurrence of psychological behavior problems in children is related to factors such as the home environment, the level of parental education, parental mental disorders, and mental status during pregnancy. The results from this study showed that the gestational age significantly affected the four domains of social-emotional development in the children with CP. Preterm infants had higher scores in the problem domains (including the externalizing, internalizing and dysregulation domains) and lower scores in the ability domain, compared TO healthy and post-term children. Spittle et al18 reported that the scores of the internalizing and dysregulation domains in the preterm infants were significantly lower compared to healthy children but were not significantly different in the externalizing domain. Similarly, Cheong et al19 found that the social ability scores of the preterm children were significantly lower compared to healthy children. These observations may be related to the low birth weight of preterm infants. A previous multicenter study revealed that the risk of CP was ten times higher in low birth-weight infants or fetal macrosomia, compared to children with normal birth weights.20 Compared to healthy newborns, preterm infants are vulnerable to impaired white and gray matter in the brain, periventricular leukomalacia, overactivated microglial cells and opened astrocyte channels. These changes in the brain result in the release of ATP and the activation of purinergic receptors as well as the proliferation of pro-inflammatory microglial cells associated with early damage.21,22 Moreover, significant differences in externalizing, internalizing, and competence domain scores were observed in different types of CP with no significant differences in the dysregulation domain. Each domain consists of different dimensions and the behavior related to each dimension is controlled by different areas of the brain. The classification of CP is related to the location of brain injury. Children with hemiplegic CP are more likely to have mixed gray matter and white matter abnormalities, whilst children with spastic diplegia or ataxia CP are more likely to have white matter abnormalities.23 Children with left-sided brain injury show significant delays in speech and language functions whilst the children with right-sided brain injury developed poor visual and spatial skills as well as somatesthesia functions.24
We further screened the risk factors associated with the positive domains for the social-emotional development scale using a multivariate logistic regression method. Our data showed that the parental emotional state and education level were closely related to problems arising in multiple dimensions of the children’s social emotions. The effect of perinatal factors on the externalizing and competence domains in children were more significant than on other domains. Parental emotion and coping styles had more significant effects on the internalizing and dysregulation domains. As the primary guardians of their children, parents impart their own experiences, knowledge and feelings to their children either consciously or unconsciously in the interactive process of communication.25 A family raising a child with CP is always faced with heavy mental burdens and huge economic pressures and so family relationships are fragile. If the parents cannot effectively release and dredge the long-term psychological stress resulting from a gap between reality and ideals, they are highly likely to struggle with anxiety and depression.26 Previous studies have shown that maternal anxiety and depression during pregnancy negatively impact the intelligence and personality development of children. Children who grown up in families with parental psychological problems have a higher risk of social-emotional behavior problems, even if parental psychological problems are within the subclinical range.27–29 Parental education level is related to a variety of social family factors such as parenting style, family atmosphere and economic conditions. These factors may have a greater impact on the emotional issues of children. In this context, we advocate an overall parenting model that helps to create a positive family environment and atmosphere for the children. Also, it is important to pay attention to children and give appropriate language and information stimulation as well as necessary guidance and assistance. This approach can highly beneficial to children’s emotional management and social development.
The externalizing and competence domains reflect the ability of individuals to regulate and control emotions. In this study, we found that the effects of perinatal factors on the children’s positive problems of the externalizing and competence domains were more prominent than on other domains. The biological basis of emotional regulation in children is the level of development of brain nerves in which the excitation and inhibition of the parasympathetic nerve play an important role in the perception and control of emotions. The low-level inhibition of the vagus nerve is a risk factor for emotional health and poor mood regulation, whilst high-level inhibition is generally beneficial.30 Brain damage in children with CP caused by perinatal risk factors makes it difficult for them to regulate their emotions through biological processes. This leads to many problems in emotional management making the children susceptible to stimulation and impulsivity.31 Also, parental emotional state and coping style have significant effects on the internalizing and dysregulate domains. Stress management in parenthood can be challenging, particularly for the parents of children with CP. Previous studies have shown that the long-term development of the children’s psychology and sociality is closely related to the participation of paternal parenting activities and the secretion of hormones such as prolactin and oxytocin which correlate with maternal care.32 In families with children who have CP, the father’s family and social roles are particularly important. Paternal anxiety and depression directly affect family and social participation as well as the family atmosphere and so influences the children’s emotional state, mentality and behaviors.33,34 Therefore, in the parenting activities for the children with CP, special attention should be paid to the adjustment and intervention of the paternal psychological state to help fathers cope with the difficulties in the children’s growth. Also, the treatment of limb function recovery should be coordinated with psychological counseling for the children and their parents.35,36
Whilst this study provides sound observations, it had several limitations. Firstly, this was a single-center study that had a relatively small sample size. All of the subjects were from Northwestern China and so our data may not be valid for other regions of China or other countries and so further studies conducted in a larger multi-center cohort are needed to validate our results. Secondly, information was collected from parents only which limits the understanding of children’s mental health status. However, we consider parents to have the best understanding of a child’s mental health status particularly when communication is limited, however, a more objective assessment should also be considered. Thirdly, the entire cohort was included regardless of functional levels. The clinical population based on the study design resulted in non-uniform assessment methods of the cognitive levels of half the population which reduces the strength of the study. Fourthly, small numbers were used in this study which also lacked a control group. Finally, we only screened the independent risk factors that affected the social-emotional development of children with CP, while the effect of early interventions for each factor requires further research.
Conclusions
This is the first study to investigate the clinical features and risk factors associated with the positive domains for social-emotional development in children with CP in China. To our knowledge, children with CP are more likely to have behavioral, emotional, and psychiatric issues and most of these issues are ignored. The parental emotional state, education level, coping style and perinatal factors are closely associated with the social-emotional issues of Chinese toddlers with CP. Our data have possible implications for the management of CP during childhood and suggest the need to avoid exclusive focus on motor function goals. There is an urgent need to develop a strategy for the early screening, diagnosis and treatment of social-emotional issues in children with CP that will be beneficial to their rehabilitation and long-term prognosis.
Consent for Publication
All authors have given consent for publication.
Acknowledgments
The authors thank all of the participants and their families for their collaboration. We also thank the Neurology and Rehabilitation Department of the Affiliated Children’s Hospital of Xi’an Jiaotong University, for their collaboration during the enrollment process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the General Program of the National Natural Science Foundation of China (Grant NO. 81371900).
Disclosure
We wish to confirm that all of the authors report no conflicts of interest.
References
1. Patel DR, Neelakantan M, Pandher K, Merrick J. Cerebral palsy in children: a clinical overview. Transl Pediatr. 2020;9(S1):S125–S135. doi:10.21037/tp.2020.01.01
2. China Rehabilitation Association Children’s Rehabilitation Professional Committee. Chinese cerebral palsy rehabilitation guide: part I. Chin J Rehabil Med. 2015;30:747–754.
3. Yang S, Xia J, Gao J, Wang L. Increasing prevalence of cerebral palsy among children and adolescents in China 1988–2020: a systematic review and meta-analysis. J Rehabil Med. 2021. doi:10.2340/16501977-2841
4. Frslev-Friis C, Dunkhase-Heinl U, Andersen J, Stausbl-Grn B, Garne E. Epidemiology of cerebral palsy in Southern Denmark. Dan Med J. 2015;62(1):A4990.
5. Sadowska M, Sarecka-Hujar B, Kopyta I. Cerebral palsy: current opinions on definition, epidemiology, risk factors, classification and treatment options. Neuropsychiatr Dis Treat. 2020;16:1505–1518. doi:10.2147/NDT.S235165
6. Ritzmann R, Stark C, Krause A. Vibration therapy in patients with cerebral palsy: a systematic review. Neuropsychiatr Dis Treat. 2018;14:1607–1625. doi:10.2147/NDT.S152543
7. Vitrikas K, Dalton H, Breish D. Cerebral palsy: an overview. Am Fam Physician. 2020;101(4):213–220.
8. Parkes J, White-Koning M, Dickinson HO, Thyen U, Colver A. Psychological problems in children with cerebral palsy: a cross-sectional European study. J Child Psychol Psychiatry. 2010;49(4):405–413. doi:10.1111/j.1469-7610.2007.01845.x
9. Weber P, Bolli P, Heimgartner N, Merlo P, Ktterer C. Behavioral and emotional problems in children and adults with cerebral palsy. Eur J Paediatr Neurol. 2016;20(2):270–274. doi:10.1016/j.ejpn.2015.12.003
10. Dickinson HO, Parkinson KN, Ravens-Sieberer U, Schirripa G, Colver AF. Self-reported quality of life of 8–12-year-old children with cerebral palsy: a cross-sectional European study. Lancet. 2007;369(9580):2171–2178. doi:10.1016/S0140-6736(07)61013-7
11. Chorna O, Heathcock J, Key A, et al. Early childhood constraint therapy for sensory/motor impairment in cerebral palsy: a randomised clinical trial protocol. BMJ Open. 2015;5(12):e010212. doi:10.1136/bmjopen-2015-010212
12. Sigurdardottir S, Indredavik MS, Eiriksdottir A, et al. Behavioural and emotional symptoms of preschool children with cerebral palsy: a population-based study. Dev Med Child Neurol. 2010;52(11):
13. Jianduan Z, Huishan W, Shuhua S, Xiaonan H, Guoyan L, Guangli L, Junxin S. Reliability and validity of standardized Chinese version of Urban Infant-Toddler Social and Emotional Assessment. Early Hum Dev. 2009;85(5):331–336. doi:10.1016/j.earlhumdev.2008.12.012.
14. Xiao J, Xu X. The reliability and validity of coping style questionnaire. Chin Mental Health J. 1996;9(4):164–168.
15. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361. doi:10.1111/j.1600-0447.1983.tb09716.x
16. Leung CM, Ho S, Kan CS, Hung CH, Chen CN. Evaluation of the Chinese version of the hospital anxiety and depression scale. A cross-cultural perspective. Int J Psychosom. 1993;40(1–4):29.
17. Xia NG, Ding SQ, Lin JH, Dong FR, Xu HQ. Comparison of the performance of two depression rating scales in patients with epilepsy in southern China. Epilepsy Behav. 2020;106:107025. doi:10.1016/j.yebeh.2020.107025
18. Spittle AJ, Treyvaud K, Doyle LW, Roberts G, Anderson PJ. Early emergence of behavior and social-emotional problems in very preterm infants. J Am Acad Child Adolesc Psychiatry. 2009;48(9):909–918. doi:10.1097/CHI.0b013e3181af8235
19. Cheong JL, Doyle LW, Burnett AC, et al. Association between moderate and late preterm birth and neurodevelopment and social-emotional development at age 2 years. JAMA Pediatr. 2017;171(4):e164805. doi:10.1001/jamapediatrics.2016.4805
20. Platt MJ, Cans C, Johnson A, et al. Trends in cerebral palsy among infants of very low birthweight. Lancet. 2007;369(9555):43–50. doi:10.1016/S0140-6736(07)60030-0
21. Inder TE, Huppi PS, Warfield S, et al. Periventricular white matter injury in the premature infant is followed by reduced cerebral cortical gray matter volume at term. Ann Neurol. 1999;46(5):755. doi:10.1002/1531-8249(199911)46:5<755::AID-ANA11>3.0.CO;2-0
22. Mallard C, Davidson JO, Tan S, et al. Astrocytes and microglia in acute cerebral injury underlying cerebral palsy associated with preterm birth. Pediatr Res. 2014;75(1–2):234. doi:10.1038/pr.2013.188
23. Korzeniewski SJ, Birbeck G, Delano MC, Potchen MJ, Paneth N. A systematic review of neuroimaging for cerebral palsy. J Child Neurol. 2008;23(2):216–227. doi:10.1177/0883073807307983
24. Kolk A, Talvik T. Cognitive outcome of children with early-onset hemiparesis. J Child Neurol. 2000;15(9):581–587. doi:10.1177/088307380001500903
25. Filce HG, Lavergne L. Absenteeism, educational plans, and anxiety among children with incontinence and their parents. J Sch Health. 2015;85(4):241–250. doi:10.1111/josh.12245
26. Basaran A, Karadavut KI, Uneri SO, Balbaloglu O, Atasoy N. The effect of having a children with cerebral palsy on quality of life, burn-out, depression and anxiety scores: a comparative study. Eur J Phys Rehabil Med. 2013;49(6):815–822.
27. Snyder J, Gewirtz A, Schrepferman L, et al. Parent-child relationship quality and family transmission of parent posttraumatic stress disorder symptoms and child externalizing and internalizing symptoms following fathers’ exposure to combat trauma. Dev Psychopathol. 2016;28(4pt1):947–969. doi:10.1017/S095457941600064X
28. Pol L, Groeneveld MG, Endendijk JJ, et al. Associations between fathers’ and mothers’ psychopathology symptoms, parental emotion socialization, and preschoolers’ social-emotional development. J Child Fam Stud. 2016.
29. Michelsen SI, Flachs EM, Madsen M, Uldall P. Parental social consequences of having a child with cerebral palsy in Denmark. Dev Med Child Neurol. 2015;57(8):768–775. doi:10.1111/dmcn.12719
30. Izard C. Basic emotions, natural kinds, emotion schemas, and a new paradigm. Perspect Psychol Sci. 2007;2(3):260. doi:10.1111/j.1745-6916.2007.00044.x
31. Tsoi W, Zhang LA, Wang WY, Tsang KL, Lo SK. Improving quality of life of children with cerebral palsy: a systematic review of clinical trials. Child Care Health Dev. 2012;38(1):21–31.
32. Abraham E, Hendler T, Shapira-Lichter I, Kanat-Maymon Y, Zagoory-Sharon O, Feldman R. Father’s brain is sensitive to childcare experiences. Proc Natl Acad Sci USA. 2014;111(27):9792–9797. doi:10.1073/pnas.1402569111
33. Esposito G, Valenzi S, Islam T, Bornstein MH. Three physiological responses in fathers and non-fathers’ to vocalizations of typically developing infants and infants with autism spectrum disorder. Res Dev Disabil. 2015;43:43–50. doi:10.1016/j.ridd.2015.06.007
34. Baker JK, Fenning RM, Crnic KA. Emotion socialization by mothers and fathers: coherence among behaviors and associations with parent attitudes and children’s social competence. Soc Dev. 2011;20(2):412–430. doi:10.1111/j.1467-9507.2010.00585.x
35. Sanders W, Zeman J, Poon J, Miller R. Child regulation of negative emotions and depressive symptoms: the moderating role of parental emotion socialization. J Child Fam Stud. 2015;24(2):402–415. doi:10.1007/s10826-013-9850-y
36. Barlow JH, Ellard DR. Psycho-educational interventions for children with chronic disease, parents and siblings: an overview of the research evidence base. Child Care Health Dev. 2010;30(6):637–645. doi:10.1111/j.1365-2214.2004.00474.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.