Back to Journals » Advances in Medical Education and Practice » Volume 16
Social Accountability in Clinical Education: A Scoping Review
Authors Abdalla MN ![]() , Osman A, Mahmoud N, Harney SC, Abdalla ME
, Osman A, Mahmoud N, Harney SC, Abdalla ME
Received 28 June 2025
Accepted for publication 30 September 2025
Published 17 October 2025 Volume 2025:16 Pages 1897—1916
DOI https://doi.org/10.2147/AMEP.S550053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mohamed Nazar Abdalla,1 Amani Osman,2 Nazar Mahmoud,3 Sarah C Harney,1 Mohamed Elhassan Abdalla1
1School of Medicine, University of Limerick, Limerick, Ireland; 2Department of Family and Community Medicine, King Khalid University, Abha, Saudi Arabia; 3College of Medicine, Mashreq University, Khartoum, Sudan
Correspondence: Mohamed Nazar Abdalla, School of Medicine, University of Limerick, Limerick, V94 T9PX, Ireland, Email [email protected]; [email protected]
Background and Purpose: Clinical education serves as a vital bridge between theoretical knowledge and practical application, preparing healthcare professionals to meet societal health needs. Social accountability, as defined by the World Health Organization, obliges educational institutions to align education, research, and service activities with community health priorities. Although widely recognized, the integration of social accountability into clinical education remains underexplored, with notable gaps in evaluation, curriculum alignment, and implementation strategies. This scoping review’s purpose is to bridge the existing knowledge gap by synthesizing current evidence, analysing various implementation methods, identifying barriers and evaluation frameworks, and outlining opportunities for advancing socially accountable clinical training.
Methods: This scoping review synthesizes current evidence on embedding social accountability within clinical education. Guided by the Population–Concept–Context (PCC) framework, the review asked: How is social accountability integrated into clinical education for healthcare professionals, students, and educators across clinical training settings? Studies involving healthcare students, professionals, and educators in hospitals, community clinics, and rural placements were included. A comprehensive search of six databases (PubMed, CINAHL, Scopus, Web of Science, PsycINFO, and ERIC) was conducted from inception up to February 28, 2025. Only English-language publications were included. Data extraction followed Joanna Briggs Institute and PRISMA-ScR guidelines, with thematic analysis conducted using Braun and Clarke’s approach.
Results: From 893 identified records, 58 studies met the inclusion criteria. Key themes emerged, including curricular integration, faculty engagement, barriers to implementation, community engagement, practical applications, Educational Outcomes and evaluation strategies.
Conclusion: Integrating social accountability into clinical education promotes equity in healthcare and prepares graduates to address systemic health challenges. However, persistent obstacles related to implementation and assessment remain. Future research should focus on identifying effective strategies for integrating social accountability into clinical training, considering diverse regional and cultural contexts, and exploring innovative approaches to evaluation and stakeholder collaboration.
Keywords: social accountability, health advocacy, curriculum integration, implementation barriers, evaluation frameworks, service learning
Introduction
Clinical education serves as the bridge between theoretical knowledge and medical practice, playing a pivotal role in developing competent healthcare professionals equipped to meet societal health needs. It is the formal, supervised, experiential phase of health-professional training in which students apply classroom learning in real-world settings, such as hospitals, clinics, and community environments, while working alongside clinical faculty.1–3 Clinical education integrates theory and practice across areas such as patient assessment, treatment, management, quality improvement, research, teaching, and teamwork, using clear objectives and reflection to build the competence and professionalism needed for independent practice.1–3 Originating from the structured, science-driven reforms introduced by Abraham Flexner in 1910, clinical education has evolved into a multifaceted training system encompassing diverse settings, such as hospitals, community health centres, and rural placements.4,5 This progression reflects a shift in educational focus beyond technical competencies to incorporate a broader accountability framework aimed at addressing societal health challenges.6 Today, clinical education presents a unique context for embedding social accountability, a principle gaining recognition as essential for achieving equity in healthcare systems.
This broader orientation within education emerged alongside global movements aimed at reshaping health systems, notably The Alma-Ata Declaration of 1978, which established health as a fundamental human right and underscored the importance of equity, community participation, and primary healthcare as the foundation of healthcare systems.7 While the declaration did not explicitly reference “social accountability”, it articulated principles that align with the concept by advocating for healthcare that is responsive to societal needs.
Building on this foundation, the World Health Organization (WHO) later defined social accountability as the obligation of educational institutions to align their education, research, and service activities with the priority health concerns of the communities they serve.8 At its core, this definition underscores that the primary aim of social accountability is to address the priority health needs of society. It also highlights the necessity for medical education to integrate social, economic, and cultural determinants of health to enhance equity, relevance, and effectiveness in healthcare delivery.9
The Global Consensus on Social Accountability for Medical Schools reinforced this paradigm by urging institutions to integrate their missions with societal health needs.10 Despite these efforts, the operationalization of social accountability in medical education, particularly within clinical training, remains incomplete, particularly in terms of standardized evaluation metrics and curricular integration.11–13 Embedding social accountability in clinical education fosters healthcare professionals adept at addressing systemic inequities, cultural competencies, and the specific needs of diverse populations.14,15
Globally, integrating social accountability into clinical education varies significantly due to differences in healthcare systems and educational frameworks.16 Tailored strategies, such as community-based education and competency-based medical education (CBME), are essential for ensuring that clinical training addresses local and regional health priorities17–19 However, many medical education curricula including those focused on clinical training lack comprehensive approaches to address these needs, underscoring the necessity of systematic evaluation and framework development.20
Clinical education provides an unparalleled opportunity to operationalize social accountability principles through experiential learning. By engaging learners in real-world healthcare settings, such as rural placements and community clinics, clinical education facilitates direct interaction with underserved populations.21,22 These experiences promote a nuanced understanding of systemic barriers to healthcare access, fostering empathy, communication skills, and critical thinking.23 Additionally, interprofessional collaboration in clinical education enhances cultural competence and prepares learners to address health disparities effectively.24
Despite the recognized importance of social accountability and its potential to transform healthcare outcomes, the integration of this concept into clinical education remains insufficiently developed, particularly in relation to curricular design, assessment methods, and institutional alignment with community health needs.22,25 While research has begun to examine social accountability in pre-clinical settings, particularly through problem-based learning (PBL), this work remains relatively isolated. For example, Ghaly et al (2023) assessed the alignment of PBL scenarios with social accountability values in undergraduate curricula, while Kelly et al (2022) and Dash et al (2022) applied a validated inventory to map social and health system issues in pre-clinical medical education.26–28 However, the overlap between social accountability and clinical education remains insufficiently explored. This lack of exploration overlooks the potential to uncover how integrating social accountability principles can enrich clinical education and support the development of socially accountable healthcare practitioners. Further research is needed to explore the integration of social accountability within clinical education by examining specific strategies and programs and identifying associated barriers. This scoping review aimed to address this gap by synthesizing existing evidence, analysing implementation approaches, barriers, and evaluation strategies, and highlighting opportunities to enhance socially accountable clinical training. Uniquely, this review synthesizes evidence on social accountability specifically within clinical education, distinguishing it from prior reviews that have largely focused on pre-clinical contexts. In doing so, it offers a comprehensive foundation for curriculum design, faculty development, and evaluation strategies tailored to clinical training settings.
Materials and Methods
Study Design
The methodology adhered to the Joanna Briggs Institute (JBI) guidelines for scoping reviews.29 The reporting of this review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR)30 to ensure transparency and reproducibility. The research question was guided by the Population–Concept–Context (PCC) framework and formulated as follows: How is social accountability integrated into clinical education for clinical educators, healthcare professionals, and students across diverse clinical training environments such as hospitals, community clinics, and rural placements?
Eligibility Criteria
Eligibility criteria were established based on the Population-Concept-Context (PCC) framework.29 Studies were included if they involved healthcare professionals, students, or faculty engaged in clinical education. The concept focused on research examining the definition, implementation, impact, curricular integration, or educational outcomes of social accountability. The context encompassed clinical education environments, including hospitals, ambulatory care, and other healthcare settings.
Eligible sources included diverse methodologies and designs, encompassing peer-reviewed articles, non-peer-reviewed literature, reviews, text, and opinion papers. No publication date restrictions were applied, to capture the evolution and historical significance of social accountability in clinical education.
Exclusion Criteria
Studies were excluded if they did not focus explicitly on the concept of social accountability. Additionally, studies addressing social accountability unrelated to clinical education, such as purely theoretical discussions or studies from non-healthcare domains, were excluded. Incomplete studies, non-English publications, and sources deemed irrelevant to the specific objectives of this review were also excluded.
Information Sources
To identify potentially relevant sources, the literature search covered six bibliographic databases: PubMed, CINAHL, Scopus, Web of Science, PsycINFO, and ERIC. The search spanned all years up to February 28, 2025. A preliminary exploratory search was conducted in MEDLINE and CINAHL to identify keywords and index terms and further refined through team discussion. The finalized strategy combined the MeSH term “Social Responsibility” with keywords including “social accountability”, “accountability in healthcare”, “healthcare responsibility”, “social responsiveness”, and terms related to clinical training such as “clinical education”, “clinical training”, “clinical teaching”, “placement”, and “clerkship”, using Boolean operators (AND/OR) as appropriate. The final search results were exported into EndNote. Complete search strings for all databases are provided in Table 1.
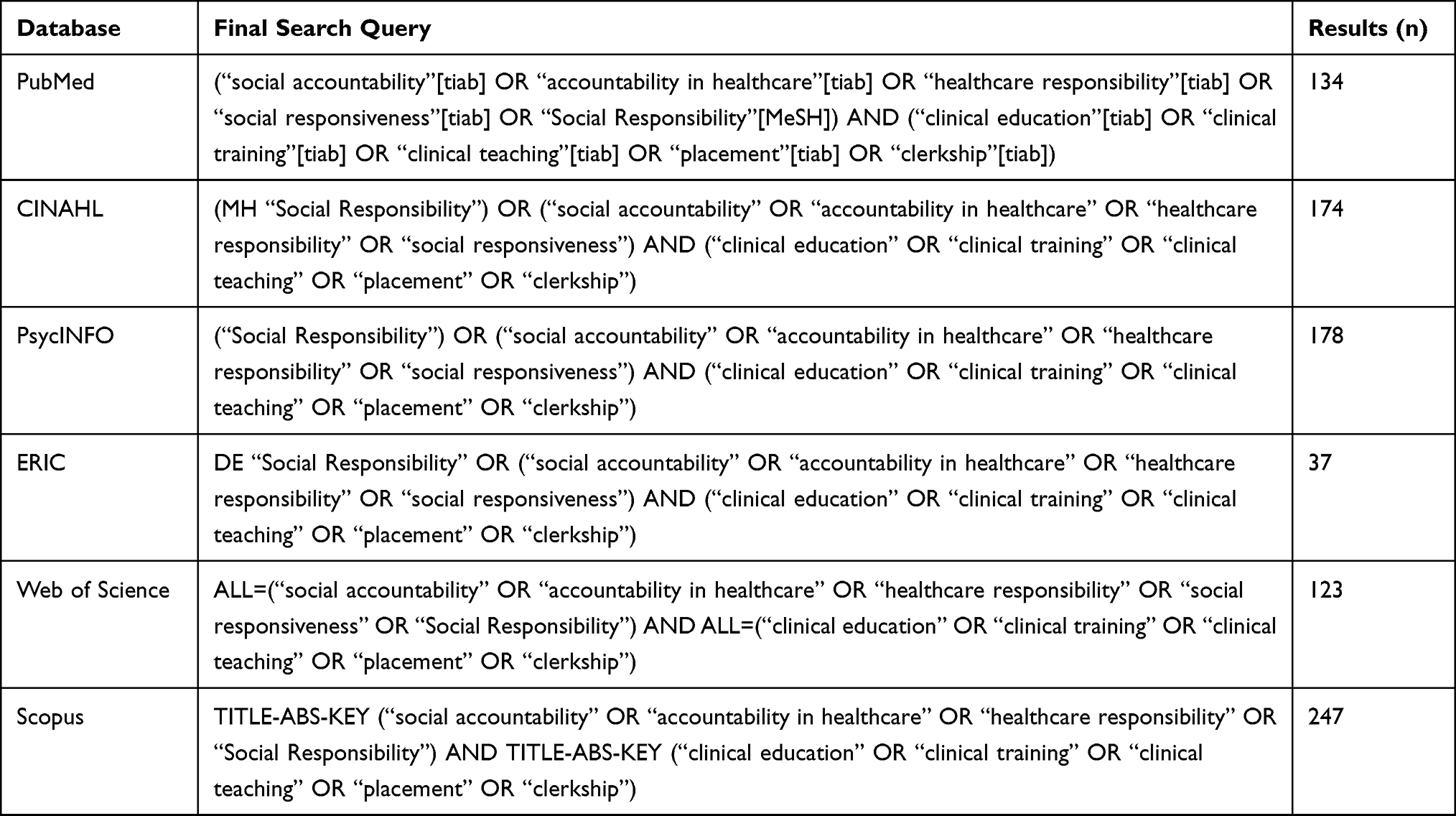 |
Table 1 Final Search Strategies and Results Across Databases (From Inception to February 28, 2025) |
Selection of Sources of Evidence
Citations retrieved from the search were collated using EndNote version 21, which facilitated the removal of duplicates. The screening process was conducted independently by two reviewers (N.M and A.O). Titles and abstracts were screened against the eligibility criteria, followed by full-text assessments of the articles that satisfied the inclusion criteria. Discrepancies were resolved through discussion or consultation with the main author. A calibration exercise was performed using a subset of studies to ensure consistency in applying the eligibility criteria.
Data Charting Process
A data charting form was developed iteratively by the research team to extract relevant data. Two independent reviewers piloted the form using a random sample of three studies to ensure its clarity and applicability. Data extraction was conducted by the primary reviewer (M.N.A)., and all entries were subsequently verified by a second independent reviewer (A.O.) to ensure accuracy. These roles were not rotated. Any discrepancies identified during verification were discussed and resolved through consensus, with input from a third reviewer if needed.
Data Items
The data extracted from the included studies were aligned with the review objectives and comprised study characteristics such as publication year, geographical location, and clinical education setting; methodological details including research design and participant type and specialty; implementation strategies and evaluation methods; educational outcomes and impacts on healthcare or the community; and barriers to implementation.
Quality Assessment of Included Studies
A quality assessment was not conducted in this review, as it is not mandatory for scoping reviews.
Data Analysis
Descriptive statistics were used to provide a quantitative overview of study characteristics and contextual distribution. Thematic analysis was conducted following Braun and Clarke’s six-step framework, involving data familiarization, systematic coding, theme identification, coherence review, definition, and synthesis into a structured narrative.31 To ensure analytical rigor and relevance, the coding and thematic development were collaboratively reviewed and refined by members of the author team with expertise in social accountability in medical education. The final themes were presented in a narrative format to illustrate key patterns across the dataset.
Results
Study Selection
The PRISMA diagram (Figure 1) shows that 893 records were identified; after removing 159 duplicates, 734 records underwent title/abstract screening, with 588 excluded for not meeting inclusion criteria. 146 full-text articles were then assessed, of which 88 were excluded (53 for irrelevant context, 35 for irrelevant conceptual focus), yielding 58 studies in the final analysis.
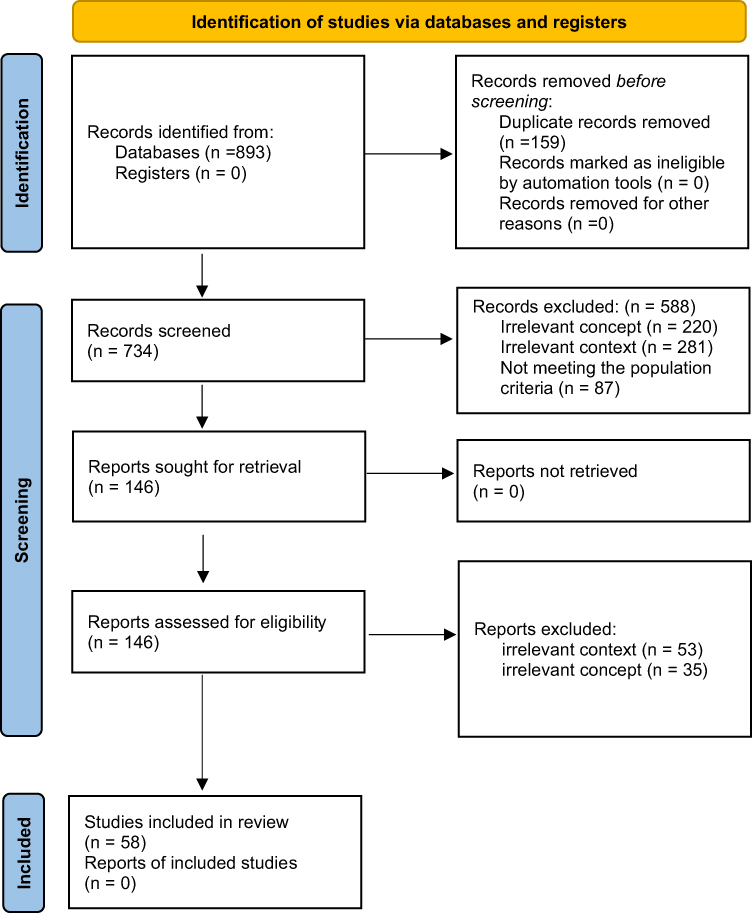 |
Figure 1 PRISMA flow diagram showing the study selection process. |
Characteristics of Source Evidence
The characteristics of the included studies, summarized in Table 2, highlight variations in study design, geographical distribution, learner populations, specialties, and clinical education settings. The studies employed diverse research designs to explore the integration of social accountability (SA) in clinical education. Qualitative methods were the most common, appearing in 13 studies (22.4%), followed by mixed methods approaches (12 studies, 20.7%), narrative reviews and reflective commentaries (10 studies, 17.2%), program evaluations (8 studies, 13.8%), quantitative studies (6 studies, 10.3%), and descriptive analyses (6 studies, 10.3%). The geographical distribution varied, with the majority conducted in Canada (22 studies, 37.9%), followed by the United States (17 studies, 29.3%), Australia (7 studies, 12.1%), the United Kingdom (3 studies, 5.2%), and Iran (2 studies, 3.4%). Additional contributions came from Israel, Italy, South Korea, the Philippines (each 1 study, 1.7%), along with two multi-country studies: one involving Spain, Belgium, Turkey, and Portugal, and another involving Sudan, Saudi Arabia, and Egypt.
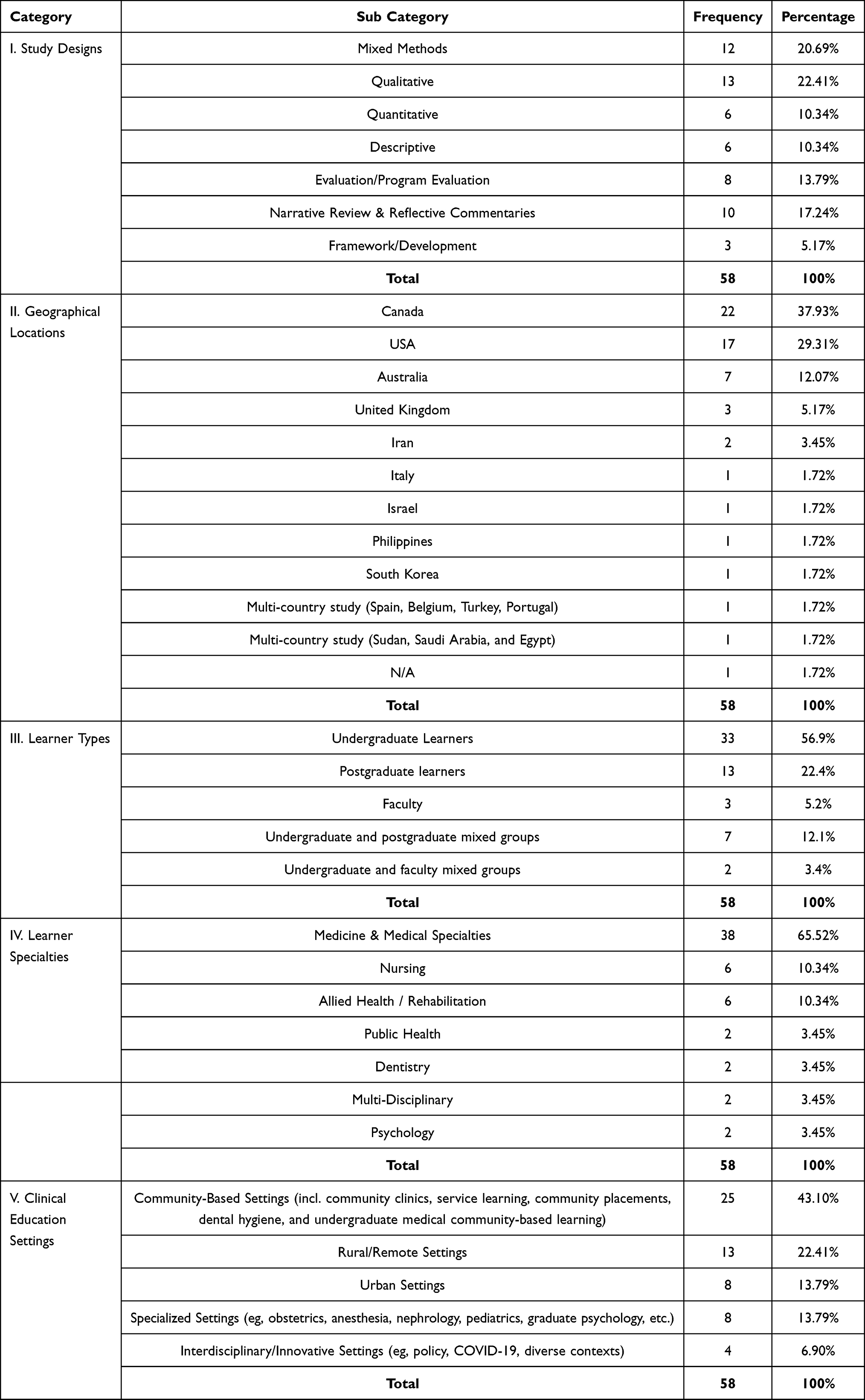 |
Table 2 Characteristics of Included Studies |
Regarding targeted learner populations and specialties, undergraduate learners were the most frequently studied group, appearing in 33 studies (58.9%), followed by postgraduate learners, including residents (13 studies, 23.2%), faculty (3 studies, 5.4%), undergraduate and postgraduate mixed groups (7 studies, 12.5%), and undergraduate and faculty mixed groups (2 studies, 3.6%). Most studies focused on medicine and medical specialties (38 studies, 65.52%), followed by nursing and allied health/rehabilitation disciplines (6 studies each, 10.34%). Studies targeting dentistry, psychology, public health, and multidisciplinary populations each accounted for 2 study respectively (3.45% each).The clinical education settings examined included community-based environments (25 studies, 43.1%), rural or remote settings (13 studies, 22.4%), urban and specialized settings (every 8 studies, 13.8%), and interdisciplinary or innovative settings (4 studies, 6.9%), with examples such as community health programs, rural clinics, urban hospitals, and specialized centres.
Thematic Analysis
This section outlines the results of our thematic analysis, which identifies key components of social accountability within clinical education learning environment. The emerging themes provide a comprehensive examination of the fundamental aspects that support and implement social accountability in clinical training.
Theme 1: Integration of Social Accountability Into Curricula and Educational Frameworks
This theme refers to the deliberate incorporation of social accountability principles into educational and clinical curricula, emphasizing the adoption of competency-based frameworks, the use of spiral curricula, and the incorporation of interprofessional education (IPE) to ensure that training aligns with societal and patient needs. In this review, 13 studies provided evidence supporting this theme, demonstrating a strong emphasis on curriculum design that integrates community focus and clinical frameworks to meet broader social accountability goals.
A prominent manifestation of this integration was the design of curricula grounded in community needs and values, reflecting how educational objectives were shaped by local health priorities and cultural contexts. Curriculum design with a community focus was prominently featured, with programs integrating cultural competence, local engagement, and community health needs into educational objectives.19,32–43
A key strategy identified within this theme is the use of Competency-Based Medical Education (CBME), which was described by Caccia et al (2015) as “fundamentally oriented to graduate outcome abilities and organized around competencies derived from an analysis of societal and patient needs”.35
Additionally, the literature revealed gaps in the explicit teaching of social accountability within clinical curricula. For example, Ponka et al (2017) observed that
Participants identified that the concept of social accountability wasn’t necessarily formally taught in the curriculum, making it difficult for residents to recognize it as an important competency.44
Innovative curricular models, such as spiral curricula, were also discussed as effective mechanisms for reinforcing these principles of social accountability and health advocacy. Fung and Ying (2022) described the spiral curriculum as one that allows for iterative, progressively complex learning, stating that this approach “highlights the importance and relevance of social accountability and advocacy in health management”.42 Finally, interprofessional education (IPE) emerged as another strategic approach. Moeller and Salas (2023) emphasized the need to integrate “health disparities, social determinants of health, and social responsibility” into core clinical training to better prepare students for interdisciplinary collaboration.45
Taken together, these findings underscore the importance of curricular scaffolding, through competency frameworks, iterative designs, and interprofessional training, in embedding social accountability into clinical education.
Theme 2: Faculty Engagement and Development for Advancing Social Accountability in Clinical Education
Beyond curriculum design, faculty engagement and professional development emerged as another critical factor in advancing social accountability within clinical training. Faculty engagement and development for advancing social accountability in clinical education refers to the involvement and professional growth of faculty in integrating socially accountable practices into clinical education. This theme is supported by evidence from 8 unique studies:.33,41,46–51
Findings indicate that faculty workload and competing responsibilities present challenges to the development and implementation of socially accountable initiatives. For instance, Asgary and Smith (2013) reported, “Most practitioners, however, do not have experience or training in broader advocacy, nor do they have interest or time”,46 while Turner and Farquhar (2008) noted that the development and implementation of socially accountable curriculum initiatives through initiatives such as the “Contract for Social Commitment” slowed when faculty members’ attention was diverted by other professional obligations.33
Evidence also shows that effective mentorship and supervision can bridge the gap between theory and practice in advocacy and social collaboration. Hashmi et al (2020) noted that having different mentorship relationships helps students engage with the “real-world context, realities of health and social collaboration and advocacy” while also learning to maintain healthy professional boundaries.41
Faculty fatigue and burnout, related to excessive workload, further limit the capacity for supervision. Courtney-Pratt et al (2015) highlighted that “reasonable concerns that individual capacity and motivation is impacted by fatigue or burnout” can adversely affect faculty supervision. To mitigate these challenges, Demers et al (2021) suggested that peer-assisted learning in challenging placements allows students to “work as a team, support each other, and reflect together in these new environments”.
In addition to workload challenges, hesitancy to delegate responsibilities stems from ambiguity in expectations regarding Entrustable Professional Activities (EPAs). Fisk et al (2024) noted that faculty are “hesitant to entrust residents to perform EPAs with less supervision” because of such ambiguity. This, in turn, undermines social accountability because residents are prevented from practicing and being assessed on the community-responsive tasks that socially accountable training aims to instil.
Finally, targeted faculty development (FD) programs are identified as essential for building the confidence and skills needed to teach social accountability. Brown et al (2016) stated, “There is an increasing need for FD in areas where current participation is lowest, namely research and social accountability”.
In summary, the evidence shows that faculty engagement is central to advancing social accountability through mentorship, supervision, and training initiatives; however, these efforts are constrained by competing responsibilities, fatigue, hesitancy to delegate, limited institutional support, and the absence of structured faculty development opportunities.
Theme 3: Barriers to Implementing Social Accountability in Clinical Education
Building on faculty-related challenges, this theme captures the multifaceted obstacles that impede the implementation of socially accountable practices into clinical education. It encompasses several subthemes: institutional resistance, time constraints, logistical and resource limitations, technological shortcomings, ethical dilemmas, and communication barriers. A substantial body of literature cited in over 27 studies provided evidence supporting these barriers.
Institutional resistance is a prominent barrier, driven by conflicting priorities and a reluctance to change traditional practices. This subtheme is supported by 11 studies.33,35,36,42,45,51–56 For example, Fung and Ying (2022) observed a lack of “institutional support for students to translate social accountability and advocacy from theory into practical applications throughout clinical training”,42 while Biswas et al (2020) noted that “the amount of work involved in running a practical curriculum inevitably invites institutional reluctance”.57
Time constraints further exacerbate these challenges.58–60 Schneider and Snell (2000) highlighted that “time constraints, negative attitudes among residents, logistical problems, scheduling demands on teachers, and lack of reinforcement” affected the integration process.
Logistical and resource constraints present another layer of difficulty.20,38,46,47,57,61–69 Biswas et al (2020) described the organizational and logistical challenges associated with community-based placements as “numerous and complex”, while Demers et al (2021) pointed “limited accommodation availability, funding” as barriers to Indigenous fieldwork placements. Similar challenges were echoed by Anton-Solanas et al (2021), who reported that issues like “workload, communication, and language barriers, gender issues, lack of resources” further complicated socially accountable clinical placements.
Technological limitations add further complexity, particularly in the context of rural and Indigenous placements. Hudson and Maar (2014) detailed issues with “distance, communication, technologies, student and cultural safety” in Aboriginal community settings.60 Meanwhile, Moeller and Salas (2023) highlighted uncertainties surrounding the integration of innovative technologies such as telehealth into clinical education, questioning “how and whether telehealth will be implemented into curricula”.45
Ethical challenges also emerge as a significant concern. Rivkin-Fish (2011) warned that inadequately structured clinical experiences might inadvertently reinforce “stigmatizing stereotypes”,56 while Anderson and Irwin (2013) identified ethical dilemmas arising from “unclear expectations of professional behaviors”34 and the lack of robust guidelines to address “these negative behaviors”.34 Thereby compromising social accountability by graduating clinicians ill-equipped to meet their communities’ priority health needs.
Lastly, communication barriers were identified as impeding effective integration. Biswas et al (2020) pointed out that linguistic challenges noting, “ensuring that all students were placed with patients they could travel to easily and communicate with through a shared language was a challenge for course organizers”,57 and Fisk et al (2024) noted that faculty hesitated to entrust learners with responsibilities to perform entrustable professional activities (EPAs) “wording is ambiguously broad”.50 This subtheme is supported by four studies.50,57,67,68
In summary, the evidence demonstrates that institutional resistance, time pressures, logistical and resource limitations, technological gaps, ethical concerns, and communication barriers collectively restrict the integration of social accountability into clinical education.
Theme 4: Community Engaged Clinical Education
In response to the institutional and systemic barriers outlined in Theme 3, several studies highlighted community engagement as a means of strengthening socially accountable clinical training. This theme describes an approach in which community members and organizations actively co-design, participate in, and benefit from clinical training programs, ensuring that learners’ training is grounded in locally identified health priorities and that education and service are mutually reinforcing. This theme is supported by evidence from 18 unique studies.
One subtheme, Service Learning as a Bridge, is documented in 9 studies.48,49,55,59,64–66,70,71 Hansen et al (2007) emphasized its potential by describing it as,
An approach that can help. graduate entry-level practitioners to understand and enact a social vision developed through thoughtfully planned educational experiences of community engagement.
A second subtheme, Long-term Professional Values, is reported in 3 studies.40,72,73 Integrating community engagement into clinical education cultivates lasting professional values, such as students’ social responsibility, justice awareness, and lifelong dedication to service, by rooting their learning in actual community needs. Thornton and Persaud (2018) observed that “social responsibility, awareness, and understanding of social justice among students increases after participation in a service learning experience”, further noting that students are more likely to engage in similar activities once they enter professional practice.40 One study stated, “Service-learning experiences move the issue of teaching social accountability beyond well-meaning rhetoric to measurable achievement”.73 The same study further noted that
Educational strategies giving medical students clinical and service-learning experience in rural/remote, urban underserved, and international communities may be an effective way to increase social awareness and practice in these settings.73
A third subtheme, Collaboration with Community Stakeholders, is supported by 3 studies.20,50,74 Strasser (2010) reported that
Active participation of communities through community engagement has the potential not only to enhance rural clinical education but also to provide substantial benefits for the communities themselves.
The final subtheme, structural and partnership challenges in community engaged clinical education, is evidenced in 3 studies.67,68,75 Maar et al (2018) emphasized the importance of aligning university schedules with community-defined benefits by stating, “Making time not only to develop the relationships but also ongoing community involvement in decision making and data analysis” is essential for sustained success. Wasylenki et al (1997) stressed that “Good working relationships between community and university representatives are vital if such collaborative ventures are to work”, and further observed that responsibilities must be delegated beyond central planning committees, “making the community agencies feel like true partners”.
Overall, the findings indicate that community-engaged clinical education employs service-learning to connect classroom and community practice, fosters long-term professional values such as social responsibility and justice awareness, promotes co-design and collaboration with community stakeholders, and encounters structural and partnership challenges that can limit sustainability.
Theme 5: Practical Applications of Social Accountability in Clinical Education
Expanding from community engagement, Practical Applications of Social Accountability in Clinical Education refer to the operational strategies used to embed social accountability within clinical training. This theme is supported by evidence from nine articles that emphasized strategies including cultural brokerage, addressing social determinants of health (SDOH), and health advocacy.42,43,46,50,52,54,58,68,76
The first subtheme, Cultural Brokerage, focuses on fostering meaningful connections between learners and diverse patient populations. It bridges cultural divides, enabling learners to engage empathetically with patients while addressing barriers to effective care. Abbott et al (2007) reported that
Cultural mentors support the learning and day-to-day work of non-Indigenous health professionals, usually nurses and doctors, in their efforts to effectively communicate and work with Aboriginal people.68
In addition, involving Aboriginal Health Workers (AHWs) further exemplifies the practical application of cultural brokerage in clinical settings. Abbott et al (2007) noted that
The AHW advising the nurse or GP that the reason a client does not want to go to hospital is due to a previous bad experience, or that they will not purchase the recommended medication because they cannot afford it this week.68
The second subtheme, Addressing Social Determinants of Health (SDOH), documents the use of immersive experiences that contextualize health within broader social structures and encourage multidisciplinary approaches partnerships to tackle systemic issues. Konkin and Myhre (2018) stated that
Students need to be in learning environments where they form authentic, therapeutic, longitudinal relationships with patients, particularly those from underserved populations.76
Fung and Ying (2022) emphasized that “Social work and medicine intersect in addressing the social determinants of health” and further proposed that patient partners roles in clinical training “should be expanded to be lecturers, moderators, facilitators, and assessors of students’ clinical skills in addressing the social determinants of health”.42
The third subtheme, Health Advocacy, encompasses training in clinical, paraclinical, and supraclinical advocacy with an emphasis on reflective practices, hands-on initiatives, and Interprofessional Collaboration. Hubinette et al (2014) documented the inclusion of “clinical, paraclinical, and supraclinical” dimensions in advocacy training.52 Hubinette et al (2014) noted inconsistent conceptualizations of advocacy and suggested that
Medical educators can use these preceptor conceptualizations … to elaborate on what they mean by advocacy, and to integrate these various constructs in a way that is consistent and compatible with clinical practice.52
Furthermore, they described hands-on activities to promote paraclinical advocacy including engaging learners in “navigating systems such as social services, filling out forms for special services, and connecting patients with community resources”.52 Reflective practices were also highlighted by Fung and Ying (2022), who mentioned activities such as “case seminars, intention/reflection practices, and clinical post-conference” to emphasize the interplay between “social changes, advocacy, and medical management”.42 Finally, the authors emphasize building partnerships to support patient-centred advocacy and preparing trainees to address structural inequities through Interprofessional Collaboration. For instance, Fisk et al (2024) argued that clinical educators should encourage “trainees to collaborate with other professionals when it would optimize patient care… preparing trainees to advocate for their patients’ health”.50
Taken together, the studies demonstrate that practical applications of social accountability in clinical trainings are enacted through cultural brokerage to strengthen learner–patient connections, immersive experiences targeting social determinants of health, and advocacy training that combines reflective practices, hands-on initiatives, and interprofessional collaboration.
Theme 6: Educational Outcomes and Competencies
The implementation of socially accountable practices also translates into measurable educational outcomes and competencies in clinical skills, professional identity, and practice behaviours that arise from socially accountable clinical placements. This theme is supported by evidence from 36 unique articles.14,33–35,37–39,41–43,45,46,49,50,53–57,59–62,64,65,67,69,70,72–80
Within this theme, several subthemes emerge. One such subtheme is the development of cultural competence and empathy to enhance understanding of diverse cultural contexts. Evidence from this subtheme shows that, for example, Anton-Solanas et al (2021) reported that students identified “respect, active listening, and empathy” as critical values for providing equitable care to culturally diverse populations, while Asgary and Smith (2013) noted, “For trainees, this opportunity is an eye opener and provides them with an early training in cultural competencies”.
Another subtheme is bias awareness and resilience, defined as the process by which learners recognize personal biases and build resilience through direct exposure to diverse clinical settings, thereby addressing issues of racism and prejudice. Supporting evidence includes Bentley and Ellison (2005), who reported that “service learning made them more aware of some of their own biases and prejudices”, and Alzeera and Ward (2022), who stated,
Breaking down bias, fear, racism, and xenophobia while providing a healthcare service to a vulnerable patient group is a way to increase the social accountability of medical schools.
Additionally, Anton-Solanas et al (2021) observed that clinical placements enabled learners to confront “some important issues including witnessing unequal care, racism, prejudice and conflict”.
A further subtheme is the enhancement of patient-centred care competencies, which refers to improving communication, ethical care, all of which are rooted in fostering patient-centred care. Newbronner et al (2017) highlighted that primary care placements “support the development of a holistic, patient-centred approach, awareness of the social context of ill-health, and increased empathy for patients”. In addition, Fisk et al (2022) noted that socially accountable entrustable professional activities (EPAs) “ultimately produce … physicians that offer more holistic patient-centred care”, and Hashmi et al (2020) described patient-centred competencies as the provision of “high quality, patient-centred, compassionate care that is built on trust and cultural safety”.
The subtheme of professional identity formation (PIF), defined as integrating experiences of social justice, advocacy, and leadership to build self-awareness and professional motivation, has been documented in several studies. Littlewood et al (2005) observed that early clinical experiences
Fostered self-awareness, empathetic attitudes towards ill people, boosted students’ confidence, motivated them, gave them satisfaction, and helped them develop a professional identity.
Similarly, Konkin and Myhre (2018) stated that “students’ PIF is informed by health equity and social justice” when they are in environments supporting “authentic, therapeutic, longitudinal relationships with patients, particularly those from underserved populations”. Biswas et al (2020) further noted that learners “demonstrated empathy, compassion, motivation, advocacy, and leadership in their field journal entries”, while Hashmi et al (2020) emphasized, “Being a leader … requires constant contributions to the improvement of healthcare in teams, organizations, and systems”.
Moreover, the subtheme clinical decision-making and procedural competence focuses on enhancing decision-making skills and procedural abilities through practical, hands-on experience. For instance, at the Northern Ontario School of Medicine (NOSM), the Distributed Community Engaged Learning program incorporates a longitudinal integrated clerkship, across more than 70 rural and underserved clinical settings. Strasser et al (2013) reported that
In the Medical Council of Canada (MCC) Part I examination, NOSM students have performed consistently above the national average, with very high scores in the section on clinical decision making.
Moreover, Strasser (2010) observed that community engagement on rural clinical education
Provides more hands-on experience for students, with the result that they are exposed to a wide range of common health problems and develop greater procedural competence.
The integration of multiple core skills is encapsulated in the subtheme Integrated Core Competencies, which involves combining communication, advocacy, leadership, and teamwork into everyday clinical practice. Hansen et al (2007) observed that Service-learning approaches embedded in socially accountable training programs
Enhance students’ communication and decision-making skills, understanding of the community context, advocacy, professional ethics, teamwork and develop leadership abilities.
while Reilly et al (2024) noted that such training improves clinical learning environments “by enhancing interprofessional teamwork to reduce errors”.
Collectively, the studies indicate that socially accountable clinical placements strengthen a wide range of learner outcomes, including cultural competence, bias awareness, patient-centred care, professional identity formation, decision-making, procedural skills, and integrated core competencies.
Theme 7: Evaluation and Assessment of Social Accountability in Clinical Education
Alongside the competencies developed through socially accountable placements, considerable attention has been directed toward how these outcomes, and their broader community impacts, are systematically evaluated. Evaluation and Assessment of Social Accountability in Clinical Education refers to the systematic measurement of learner development, community impact, and program alignment with societal needs within clinical training settings. This theme is supported by evidence from 32 unique studies.14,20,32,33,35,38,42–45,49,51,53–55,57,59–62,64,67,69–71,73,74,77–81
The area of assessing learners participating in socially accountable clinical education requires methods that extend beyond knowledge to include attitudes, skills, and the practical application of social accountability principles. Articles indicate that traditional assessment methods are insufficient for capturing the full scope of learners’ development. Caccia et al (2015) observed,
Our current assessment systems rely heavily on traditional limited methods, such as examinations, ward assessments, and in-training evaluation reports, with minimal direct observation in the clinical setting and little assessment that is formative.
Moeller and Salas (2023) noted the potential of structured assessment strategies, stating that these methods “standardize the experience and reduce bias and because this allows for much more direct comparison between learners”.
Assessing competencies such as professionalism remains particularly challenging. Carenzo et al (2021) highlighted that professionalism assessments have traditionally “been implicit, unstandardized”, and “subjective” (61). Carenzo et al (2021) assessed professionalism, including “health advocacy” and “humanistic characteristics”, which are central to social accountability. Accordingly, challenges in assessing professionalism also affect efforts to evaluate social accountability, especially when relying on conventional methods.63
Reflective practices also play a significant role in evaluation. Evidence indicates that journaling and self-assessment are used to capture personal growth and transitions. Hansen et al (2007) stated,
Reflective activities and documentation are used to assess achievement of process-oriented objectives and to document a student’s transitions and insight into a situation.
In addition, Fung and Ying (2022) claimed that “(OSCEs) provide an assessment structure ‘designed to test clinical skill performance and competence in a range of skills’” and further asserted that
OSCE stations must increasingly engage with more complex sociocultural issues and become more intricate with expectations of diagnosis and management… allows for a more consistent evaluation of social accountability.
Evaluating the impact on target communities is documented through the incorporation of community feedback and stakeholder involvement. Sen Gupta et al (2018) stated,
Meaningful impacts on rural and remote workforce and positive outcomes for underserved communities. Reports need to describe absolute numbers not proportions, as that is the outcome that communities and funders want.
Similarly, Hyde et al (2021) described a rural placement program where “Community stakeholders have direct input into the evaluation, and additional parameters are included as needed on a case-by-case basis”, including measures such as
Student engagement and confidence in working with vulnerable population groups and with other discipline areas, sense of social accountability, degree of meeting a service need, connectedness to community.
The overall evaluation of clinical programs encompasses multiple dimensions. Fung and Ying (2022) stated, “The dynamic, multifaceted nature of social accountability and health advocacy requires a reliable and valid assessment approach”. Examples of frameworks used to assess program accountability include the framework of Competency-Based Medical Education (CBME), which Caccia et al (2015) reported “allows standardization of assessment, enabling the potential for portability of training”. The CARE model is also employed; Emadzadeh et al (2016) described that the model identifies four important areas for social accountability measures “including clinical activities, advocacy, research and education”. One study acknowledged, “albeit imperfect, of whether social accountability is truly being integrated into all of the college’s activities” and noted, “Although the CARE model serves to assess ongoing activities, a more comprehensive assessment is needed”.81
Findings across these studies suggest that while diverse tools, ranging from reflective practices and OSCEs to community feedback and structured frameworks like CBME and CARE, have been applied to evaluate social accountability, existing approaches remain fragmented and often insufficient to capture its full complexity.
Discussion
This scoping review examined how social accountability is integrated into clinical education and identified key areas for improvement. The emphasis on qualitative and mixed-methods research reflects a focus on the complex nature of socially accountable education. Early professional development emerged as a critical stage for embedding social accountability, yet most studies centred on medicine, with limited inclusion of other health professions and interprofessional education (IPE). The concentration of studies in North America also points to a gap in global representation, especially from low- and middle-income countries, which agrees with a recent bibliometric analysis confirming that collaboration networks remain concentrated in high-income countries and highlighting the need to strengthen research networks with developing regions.25 The themes identified offer a basis for understanding current practices and informing future development.
Efforts to embed social accountability in clinical curricula often incorporate Competency-Based Medical Education (CBME), spiral curricula, and Interprofessional Education (IPE). CBME provides a structured framework to align graduate competencies with patient and community expectations.35 These findings align the broader literature emphasizing the importance of outcome-based education tailored to societal needs.82 Additionally, CBME’s potential for enhancing social accountability is recognized, though its success relies on active community stakeholder involvement in design and evaluation.83 The spiral curriculum reinforces progressively complex social accountability learning, allowing students to build on prior knowledge.42 IPE further strengthens this approach by integrating health disparities, social determinants of health, and social responsibility into core training, thereby enhancing interdisciplinary collaboration.45 However, social accountability remains largely implicit rather than a core curricular component, limiting its full integration.44 Addressing this gap requires explicit curricular strategies and overcoming key implementation barriers discussed in Theme 3 to ensure its effective incorporation into clinical education. Overall, the evidence highlights that while CBME, spiral curricula, and IPE offer promising frameworks for embedding social accountability, their impact depends on intentional design, explicit integration, and strong stakeholder engagement.
This study reviewed Faculty role and professional growth in advancing social accountability in clinical training. Nevertheless, heavy workloads, competing demands, and limited advocacy training often contribute to fatigue, burnout and reduced supervision capacity.46,49 Reducing faculty burden while ensuring quality supervision requires peer-assisted learning, where students collaborate, support each other, and reflect in demanding placements.47 Mentorship bridges theory and practice, fostering a real-world understanding of health systems, social collaboration, and professional boundaries.41 However, without faculty development programs to build confidence and teaching skills, the overall impact remains limited.51 Aligning with the Association for Medical Education in Europe’s guidance, which emphasizes the importance of equipping faculty with the necessary tools and training to deliver socially accountable education,84 Abdalla et al (2018) found that an online social accountability faculty development program markedly improved and transformed faculty understanding and teaching confidence, but also highlighted the need for protected time and reliable technical support.85 Without active faculty engagement, these efforts risk being superficial creating a gap between intended values and learner experiences. Overcoming institutional resistance and resource constraints is essential to embedding social accountability into training. Taken together, the literature underscores that sustainable integration of social accountability depends not only on reducing faculty workload but also on providing structured development opportunities and institutional support.
This review explored the barriers to implementing social accountability in clinical learning environment, revealing how institutional resistance, resource limitations, and time constraints hinder progress, particularly in environments with entrenched practices or limited infrastructure, such as rural and underserved population settings where logistical, technological, and resource shortages further restrict implementation.42,57,58,60 Ethical concerns also arise when poorly structured clinical experiences reinforce stereotypes and stigmatization.56 Language barriers and unclear competency expectations complicate communication and assessment, while faculty hesitation to entrust students with responsibilities due to vague definitions of professional competencies weakens learning opportunities and creates uncertainty in clinical roles.50 These barriers are interconnected, as institutional resistance often limits resource allocation, exacerbating time constraints and ethical dilemmas, ultimately weakening efforts to integrate social accountability. This reflects broader challenges in healthcare systems, where resistance to change and resource scarcity continue to hinder reforms.86 Addressing these obstacles is essential for embedding social accountability into clinical education and fostering authentic community engagement in training noted in Theme 4. The literature therefore portrays these barriers not as isolated hurdles but as overlapping constraints that collectively weaken the integration of social accountability into clinical education, underscoring the need for coordinated solutions that address institutional, structural, and ethical dimensions simultaneously.
This review examined how community engagement and service learning integrate social accountability into clinical education by connecting theoretical learning with real community health needs. The high representation of studies in community-based settings (43.1%) reinforces their critical role in socially accountable clinical training, as such environments offer authentic exposure to underserved populations, fostering professional responsibility and long-term commitment to equity-driven healthcare. Service learning strengthens reciprocal relationships between medical institutions and communities, enhancing students’ ability to navigate social determinants of health while developing culturally responsive, patient-centred care.40,55 However, misaligned institutional and community priorities, scheduling conflicts, and resource limitations can restrict access to these experiences, limiting their intended impact on learners and communities.75 Ensuring long-term sustainability requires shifting from institution-driven initiatives to shared governance, where community stakeholders actively shape decision-making and program evaluation.67,75 These insights agree with a recent critical review, which, while recognizing the transformative potential of service learning, emphasizes the need to address logistical and ethical challenges to ensure community-driven learning fosters long-term engagement in socially accountable practice.87 Together, these findings highlight community engagement and service learning as pivotal strategies for embedding social accountability, provided that partnerships are genuinely collaborative, adequately resourced, and ethically sustained.
This review explored strategies for embedding social accountability in clinical training, highlighting cultural brokerage, immersive SDOH experiences, and health advocacy training as key approaches. Cultural brokerage enhances learner-patient connections, fostering cultural competence and trust in diverse clinical settings.68 Immersive SDOH experiences provide real-world exposure to systemic health inequities, reinforcing students’ ability to navigate social determinants and build long-term, therapeutic relationships with underserved populations.76 Expanding patient partner roles as lecturers, facilitators, and assessors further integrates social accountability into training.42 Advocacy training strengthens clinical, paraclinical, and supraclinical competencies, equipping students to engage in health justice efforts, navigate social services, and connect patients with essential resources.52 Reflective practices, such as case seminars and intention/reflection exercises, deepen students’ critical engagement with social inequities, reinforcing long-term commitment to advocacy.42 Interprofessional collaboration further enhances advocacy training by preparing students to work across disciplines, ensuring holistic, patient-centred care.50 These findings align closely with what we see in the wider literature. The WHO report highlights the importance of social justice and health equity in effectively addressing social determinants of health.88 Building on this, Abdalla et al (2024) translated these principles into practical recommendations, advocating for clear curricular frameworks that embed experiential, community-based modules, such as service-learning partnerships, consistently across undergraduate and postgraduate training.89 Recent scoping reviews further support this approach, showing that programmes which combine classroom learning with extended, immersive experiences in communities are particularly successful in boosting learners’ abilities, confidence, and readiness to tackle health inequities.90,91 Additionally, involving patients directly as teachers has been proven to deepen learners’ empathy and strengthen their patient-centred approach to care.92 These practical applications are most effective when faculty are actively engaged and supported (Theme 2) and when barriers to implementation are addressed (Theme 3). In essence, the literature demonstrates that strategies such as cultural brokerage, immersive SDOH learning, and advocacy training can meaningfully embed social accountability into clinical education, but their success depends on patient involvement, faculty support, and the removal of structural barriers.
This article studied how socially accountable clinical placements foster measurable improvements in clinical skills, professional identity, and practice behaviours. Exposure to socially accountable practices in diverse clinical settings addressing racism, prejudice, and health inequities enhances learners’ bias awareness, cultural competence, empathy, and resilience.59,69 Authentic, long-term relationships with underserved patients further strengthen learners’ professional identity formation, promoting leadership and motivation toward social justice, health equity, and advocacy.76 These placements support patient-centred, ethical communication and holistic care, leading to high-quality, culturally safe clinical practice.37 Hands-on community experiences also advance learners’ clinical decision-making and procedural competencies. These findings agree with a recent review, which highlights the potential of integrating social accountability frameworks into medical education to enhance educational outcomes and expand the profession’s broader societal impact,93 further reinforcing the role of socially accountable clinical placements in shaping competent, equity-driven healthcare professionals However, the multifaceted and complex nature of these competencies poses challenges for objectively evaluating the overall impact of socially accountable clinical placements on learner development. The evidence therefore points to socially accountable placements as powerful drivers of professional growth, though their full educational value is difficult to measure given the complexity and interdependence of the competencies they cultivate.
This review underscores the need for comprehensive, multidimensional evaluation strategies of social accountability in clinical education, as traditional assessments fail to capture attitudes, practical skills, and real-world application.35 While structured methods, such as standardized evaluations, enhance consistency and reduce bias, assessing subjective competencies like professionalism remains challenging due to reliance on implicit and unstructured judgments.45,63 Reflective practices, including journaling and self-assessment, offer deeper insight into personal and professional growth, while OSCEs enhance structured evaluation, but their design must evolve to assess sociocultural competencies and real-world advocacy in clinical practice.42,55 Beyond individual performance, evaluating the broader impact of clinical programs requires direct stakeholder engagement and absolute community outcome measures, ensuring tangible benefits for underserved populations.20,62 Existing frameworks, such as CBME and the CARE model, provide standardization but fail to fully capture social accountability, necessitating refinement and integration of diverse assessment approaches.35,54,81 Ultimately, the review calls for a shift toward holistic, structured, and community-informed assessment strategies that that move beyond knowledge testing by integrating reflective practices, sociocultural competencies, and community-driven outcomes to more effectively capture the societal impact of clinical education while addressing the limitations of existing methods.
This scoping review underscores the integration of social accountability in clinical education, highlighting the role of curricular design, faculty engagement, and community partnerships in shaping socially accountable healthcare professionals. Our findings contribute a clinically grounded perspective to the broader discourse in medical education, reinforcing the need for structured frameworks that connect education to societal needs, and reinforce the necessity of learning health systems (LHS), which emphasize data-driven, community-partnered approaches to improving health outcomes.94,95 However, institutional resistance and resource limitations continue to hinder implementation, mirroring global challenges in operationalizing social accountability.96,97 While medical schools express commitment to social accountability, traditional assessment models prioritize accreditation over real-world impact, creating a gap in evidence-based evaluation frameworks.96,98 Extending beyond existing approaches, our findings advocate for a multidimensional evaluation framework that integrates learner development, community impact, and program effectiveness to align clinical education with societal needs, agreeing with LHS principles.95 Yet, stakeholder-driven assessments remain scarce, limiting efforts to track long-term trainee contributions to community outcomes.94,98 To move beyond symbolic commitments, a holistic assessment of clinical education’s societal impact, requiring interdisciplinary collaboration, faculty engagement, and community-centred placements to transform medical education into a measurable driver of health equity.16 In summary, achieving this transformation depends on aligning curricular design, community partnerships, and robust evaluation frameworks to ensure training translates into tangible health outcomes.
Limitations
Following the JBI and PRISMA frameworks and using Braun and Clarke’s thematic analysis framework as methodological strengths, our review benefits from a rigorous and systematic approach; however, it is subject to several limitations. We restricted our inclusion to English-language publications, which may have excluded valuable insights from non-English sources and narrowed the diversity of perspectives. Our reliance on select electronic databases and published studies raises the possibility of publication bias, as innovative programs reported in gray literature may have been missed. The heterogeneity of study designs and the absence of a formal quality appraisal further limit the generalizability of our findings. Additionally, the inherent subjectivity of thematic analysis, illustrated by our decision to separate “Practical Applications” from “Community Engagement”, despite their potential overlap, means that alternative interpretations of the data are possible.
Future Directions
Further research is needed to identify the most effective approaches for integrating social accountability into clinical education and to better understand its broader impacts. It will also be important to explore how clinical training can continue to evolve in response to changing societal needs and expectations.
Conclusion
This scoping review synthesized evidence on the integration and assessment of social accountability in clinical education, identifying seven core themes that reflect its complexity and necessity. Findings confirm that innovative curricula, faculty development, and community partnerships are essential for cultivating clinicians committed to health equity. Clinical education must extend beyond technical proficiency to actively contribute to a more equitable healthcare system.
Despite progress, a critical need remains for robust assessment tools that capture the societal impact of clinical programs and trainees’ contributions to community health. Standardizing evaluation practices and ensuring institutional support remain challenges. Future research should focus on developing stakeholder-driven, multidimensional evaluation frameworks using quantitative and qualitative measures. Addressing implementation barriers will require interdisciplinary collaboration, faculty engagement, and sustained investment in community-centred placements. Advancing these efforts is key to fully realizing the transformative potential of social accountability in clinical education.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report there are no competing interests to declare.
References
1. Delany C, Bragge P. A study of physiotherapy students’ and clinical educators’ perceptions of learning and teaching. Med Teach. 2009;31(9):e402–e411. doi:10.1080/01421590902832970
2. Moore ML, Perry JF. Clinical education in physical therapy: present status/future needs. final report of the project on clinical education in physical therapy; 1976.
3. O’Brien B, Teherani A. Using workplace learning to improve patient care. Acad Med. 2011;86(11):e12. doi:10.1097/ACM.0b013e3182320ce6
4. Flexner A. Medical Education in The United States and Canada. Carnegie Foundation for the Advancement of Teaching; 1910.
5. Ash JK, Walters LK, Prideaux DJ, Wilson IG. The context of clinical teaching and learning in Australia. Med j Aust. 2012;196(7):475. doi:10.5694/mja10.11488
6. Murray E, Gruppen L, Catton P, Hays R, Woolliscroft JO. The accountability of clinical education: its definition and assessment. Med Educ. 2000;34(10):871–879. doi:10.1046/j.1365-2923.2000.00757.x
7. Organization WH. Declaration of alma-ata; 1978.
8. Boelen C, Heck JE, Organization WH. Defining and measuring the social accountability of medical schools. Geneva: World Health Organization. 1995.
9. Boelen C, Woollard B. Social accountability and accreditation: a new frontier for educational institutions. Med Educ. 2009;43(9):887–894. doi:10.1111/j.1365-2923.2009.03413.x
10. Boelen C. Global consensus on social accountability of medical schools. Sante Publique. 2011;23(3):247–250. doi:10.3917/spub.113.0247
11. Bates J, Schrewe B, Ellaway RH, Teunissen PW, Watling C. Embracing standardisation and contextualisation in medical education. Med Educ. 2019;53(1):15–24. doi:10.1111/medu.13740
12. Boydell V, McMullen H, Cordero J, Steyn P, Kiare J. Studying social accountability in the context of health system strengthening: innovations and considerations for future work. Health Res Policy Syst. 2019;17:1–6. doi:10.1186/s12961-019-0438-x
13. Wood B, Attema G, Ross B, Cameron E. A conceptual framework to describe and evaluate a socially accountable learning health system: development and application in a northern, rural, and remote setting. Int J Health Plann Manag. 2022;37:59–78. doi:10.1002/hpm.3555
14. Ross BM, Cameron E, Greenwood D. Remote and rural placements occurring during early medical training as a multidimensional place-based medical education experience. Educ Res Rev. 2020;15(3):150–158. doi:10.5897/ERR2019.3873
15. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
16. Preston R, Larkins S, Taylor J, Judd J. Building blocks for social accountability: a conceptual framework to guide medical schools. BMC Med Educ. 2016;16:1–10. doi:10.1186/s12909-016-0741-y
17. Mennin S, Petroni-Mennin R. Community-based medical education. Clinl Teacher. 2006;3(2):90–96. doi:10.1111/j.1743-498X.2006.00093.x
18. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
19. Abdalla M, Taha M, Wadi M, Khalafalla H. What makes a medical school socially accountable? A qualitative thematic review of the evaluation of social accountability of medical schools in the Eastern Mediterranean Region. East Mediterr Health J. 2022;28(5):381–389. doi:10.26719/emhj.22.016
20. Hyde S, Smith B, Lawrence J, Barry R, Carey A, Rogers C. Co-designing community-focused rural placements for collaborative practice. Aust J Rural Health. 2021;29(2):284–290. doi:10.1111/ajr.12718
21. Yardley S, Teunissen PW, Dornan T. Experiential learning: transforming theory into practice. Med Teach. 2012;34(2):161–164. doi:10.3109/0142159X.2012.643264
22. Cooke M, Irby DM, O’Brien BC. Educating Physicians: A Call for Reform of Medical School and Residency. Vol. 16. John Wiley & Sons; 2010.
23. Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287(2):226–235. doi:10.1001/jama.287.2.226
24. Kumagai AK, Lypson ML. Beyond cultural competence: critical consciousness, social justice, and multicultural education. Acad Med. 2009;84(6):782–787. doi:10.1097/ACM.0b013e3181a42398
25. Abdalla M, Onchonga D, Taha MH. Social accountability in medical education: a bibliometric analysis; 2024.
26. Kelly D, Hyde S, Abdalla ME. Mapping health, social and health system issues and applying a social accountability inventory to a problem based learning medical curriculum. Med Educ Online. 2022;27(1):2016243. doi:10.1080/10872981.2021.2016243
27. Ghaly M, Taha MH, Abdalla M, Hosny S. Assessment of the compliance of problem-based learning case scenarios with the social accountability values in undergraduate medical education curriculum; 2023.
28. Dash NR, Taha MH, Shorbagi S, Abdalla ME. Evaluation of the integration of social accountability values into medical education using a problem-based learning curriculum. BMC Med Educ. 2022;22(1):181. doi:10.1186/s12909-022-03245-6
29. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z. JBI manual for evidence synthesis. JBI. 2024;2024:
30. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
31. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
32. Starr RA, Wagstaff NV. Implementing a surgical skills training program. Obstet Gynecol Clin North Am. 2006;33(2):247–58,viii. doi:10.1016/j.ogc.2006.01.006
33. Turner JL, Farquhar L. One medical school’s effort to ready the workforce for the future: preparing medical students to care for populations who are publicly insured. Acad Med. 2008;83(7):632–638. doi:10.1097/ACM.0b013e31817836af
34. Anderson DK, Irwin KE. Self-assessment of professionalism in physical therapy education. Work. 2013;44(3):275–281. doi:10.3233/WOR-121504
35. Caccia N, Nakajima A, Kent N. Competency-based medical education: the wave of the future. J Obstet Gynaecol Can. 2015;37(4):349–353. doi:10.1016/S1701-2163(15)30286-3
36. Eva KW, Bordage G, Campbell C, et al. Towards a program of assessment for health professionals: from training into practice. Adv Health Sci Educ Theory Pract. 2016;21(4):897–913. doi:10.1007/s10459-015-9653-6
37. Newbronner E, Borthwick R, Finn G, Scales M, Pearson D. Creating better doctors: exploring the value of learning medicine in primary care. Educ Prim Care. 2017;28(4):201–209. doi:10.1080/14739879.2016.1277789
38. Labarda CE, Pilar Labarda MD. A community-based strategy in medical education of the university of the Philippines Manila-school of health sciences - Lessons from innovations in human resources for health development in a developing country. Educ Health. 2018;31(3):168–173. doi:10.4103/efh.EfH_366_13
39. Pinsk M, Karpinski J, Carlisle E. Introduction of competence by design to canadian nephrology postgraduate training. Can J Kidney Health Dis. 2018;5:2054358118786972. doi:10.1177/2054358118786972
40. Thornton M, Persaud S. Preparing today’s nurses: social determinants of health and nursing education. OJIN. 2018;23(3). doi:10.3912/OJIN.Vol23No03Man05
41. Hashmi SS, Saad A, Leps C, et al. A student-led curriculum framework for homeless and vulnerably housed populations. BMC Med Educ. 2020;20(1):232. doi:10.1186/s12909-020-02143-z
42. Fung OW, Ying Y. Twelve tips to center social accountability in undergraduate medical education. Med Teach. 2022;44(11):1214–1220. doi:10.1080/0142159X.2021.1948983
43. Reilly JB, Kim JG, Cooney R, et al. Breaking down silos between medical education and health systems: creating an integrated multilevel data model to advance the systems-based practice competency. Acad Med. 2024;99(2):146–152. doi:10.1097/ACM.0000000000005294
44. Ponka D, Archibald D, Ngan J, Wong B, Johnston S. Attitudes towards sub-domains of professionalism in medical education: defining social accountability in the globalizing world. Can Med Educ J. 2017;8(2):e37. doi:10.36834/cmej.36867
45. Moeller J, Salas RME. Neurology education in 2035: the neurology future forecasting series. Neurology. 2023;100(12):579–586. doi:10.1212/WNL.0000000000201669
46. Asgary R, Smith CL. Ethical and professional considerations providing medical evaluation and care to refugee asylum seekers. Am J Bioeth. 2013;13(7):3–12. doi:10.1080/15265161.2013.794876
47. Demers M, Phenix A, Schmitz C, Storr C. Socially accountable Canadian Occupational Therapy fieldwork with indigenous peoples: where are we at? Occup Ther Health Care. 2021;35(2):182–197. doi:10.1080/07380577.2021.1919953
48. Barraclough FL, Pit S. Preparing the future workforce to address the health needs of small rural Australian towns through non-traditional allied health student placements. Intl J Integrated Care. 2018;18(s2):65. doi:10.5334/ijic.s2065
49. Courtney-Pratt H, Ford K, Marlow A. Evaluating, understanding and improving the quality of clinical placements for undergraduate nurses: a practice development approach. Nurse Educ Pract. 2015;15(6):512–516. doi:10.1016/j.nepr.2015.07.002
50. Fisk D, Clendenning B, St John P, Francois J. Multi-stakeholder validation of entrustable professional activities for a family medicine care of the elderly residency program: a focus group study. Gerontol Geriatr Educ. 2024;45(1):12–25. doi:10.1080/02701960.2022.2130913
51. Brown GM, Lang E, Patel K, et al. A national faculty development needs assessment in emergency medicine. CJEM. 2016;18(3):161–182. doi:10.1017/cem.2015.77
52. Hubinette MM, Ajjawi R, Dharamsi S. Family physician preceptors’ conceptualizations of health advocacy: implications for medical education. Acad Med. 2014;89(11):1502–1509. doi:10.1097/ACM.0000000000000479
53. Balch P, McWilliams SA. Community-based program evaluation through a graduate practicum in community psychology. Professional Psychol. 1975;6(3):331. doi:10.1037/0735-7028.6.3.331
54. Emadzadeh A, Karimi Moonaghi H, Bazzaz MM, Karimi S. An investigation on social accountability of general medicine curriculum. Electron Physician. 2016;8(7):2663–2669. doi:10.19082/2663
55. Hansen AM, Munoz J, Crist PA, et al. Service learning: meaningful, community-centered professional skill development for occupational therapy students. Occup Ther Health Care. 2007;21(1–2):25–49. doi:10.1080/J003v21n01_03
56. Rivkin-Fish M. Learning the moral economy of commodified health care: “community education”, failed consumers, and the shaping of ethical clinician-citizens. Cult Med Psychiatry. 2011;35(2):183–208. doi:10.1007/s11013-011-9208-0
57. Biswas S, Douthit NT, Mazuz K, et al. Implementing a practical global health curriculum: the benefits and challenges of patient-based learning in the community. Front Public Health. 2020;8:283. doi:10.3389/fpubh.2020.00283
58. Schneider GW, Snell L. CARE: an approach for teaching ethics in medicine. Soc Sci Med. 2000;10(51):1563–1567. doi:10.1016/S0277-9536(00)00054-X
59. Bentley R, Ellison KJ. Impact of a service-learning project on nursing students. Nurs Educ Perspect. 2005;26(5):287–290.
60. Hudson GL, Maar M. Faculty analysis of distributed medical education in Northern Canadian Aboriginal communities. Rural Remote Health. 2014;4(14):101–108.
61. Biggs JS, Wells RW. The social mission of Australian medical schools in a time of expansion. Aust Health Rev. 2011;35(4):424–429. doi:10.1071/AH10970
62. Sen Gupta T, Johnson P, Rasalam R, Hays R. Growth of the James Cook University Medical Program: maintaining quality, continuing the vision, developing postgraduate pathways. Med Teach. 2018;40(5):495–500. doi:10.1080/0142159X.2018.1435859
63. Carenzo L, Cena T, Carfagna F, et al. Assessing anaesthesiology and intensive care specialty physicians: an Italian language multisource feedback system. PLoS One. 2021;16(4):e0250404. doi:10.1371/journal.pone.0250404
64. Shannon CK, Baker H, Jackson J, Roy A, Heady H, Gunel E. Evaluation of a required statewide interdisciplinary rural health education program: student attitudes, career intents and perceived quality. Educ Health. 2005;18(3):395–404. doi:10.1080/13576280500289710
65. Alzeera M, Ward A. Involving medical students in the planning and delivery of a vaccination and health screening outreach clinic. Educ Prim Care. 2022;33(2):113–119. doi:10.1080/14739879.2021.1983732
66. Dela Cruz FA, Brehm C, Harris J. Transformation in family nurse practitioner students’ attitudes toward homeless individuals after participation in a homeless outreach clinic. J Am Acad Nurse Pract. 2004;16(12):547–554. doi:10.1111/j.1745-7599.2004.tb00434.x
67. Wasylenki DA, Cohen CA, McRobb BR. Creating community agency placements for undergraduate medical education: a program description. CMAJ. 1997;156(3):379–383.
68. Abbott P, Gordon E, Davison J. Expanding roles of Aboriginal health workers in the primary care setting: seeking recognition. Contemporary Nurse. 2007;26(1):66–73. doi:10.5172/conu.2007.26.1.66
69. Anton-Solanas I, Tambo-Lizalde E, Hamam-Alcober N, et al. Nursing students’ experience of learning cultural competence. PLoS One. 2021;16(12):e0259802. doi:10.1371/journal.pone.0259802
70. Callister LC, Hobbins-Garbett D. “Enter to learn, go forth to serve”: service learning in nursing education. J Prof Nurs. 2000;16(3):177–183. doi:10.1053/PN.2000.6177
71. Hong J, Jung I, Park M, et al. Attitude of medical students about their role and social accountability in the COVID-19 pandemic. Front Psychiatry. 2021;12:645340. doi:10.3389/fpsyt.2021.645340
72. Littlewood S, Ypinazar V, Margolis SA, Scherpbier A, Spencer J, Dornan T. Early practical experience and the social responsiveness of clinical education: systematic review. BMJ. 2005;331(7513):387–391. doi:10.1136/bmj.331.7513.387
73. Meili R, Fuller D, Lydiate J. Teaching social accountability by making the links: qualitative evaluation of student experiences in a service-learning project. Med Teach. 2011;33(8):659–666. doi:10.3109/0142159X.2010.530308
74. Strasser RP. Community engagement: a key to successful rural clinical education. Rural Remote Health. 2010;10(3):1–7.
75. Maar M, Boesch L, Tobe S. Enhancing Indigenous health research capacity in northern Ontario through distributed community engaged medical education at NOSM: a qualitative evaluation of the community engagement through research pilot program. Can Med Educ J. 2018;9(1):e21. doi:10.36834/cmej.42187
76. Konkin DJ, Myhre D. Attending to relationships: a necessary evolution in the clerkship. Med Educ. 2018;52(8):780–782. doi:10.1111/medu.13641
77. Strasser R, Hogenbirk JC, Minore B, et al. Transforming health professional education through social accountability: Canada’s Northern Ontario School of Medicine. Med Teach. 2013;35(6):490–496. doi:10.3109/0142159x.2013.774334
78. Asarnow JR, Hoagwood KE, Stancin T, et al. Psychological science and innovative strategies for informing health care redesign: a policy brief. J Clin Child Adolesc Psychol. 2015;44(6):923–932. doi:10.1080/15374416.2015.1077451
79. Mahoney S, Boileau L, Floridis J, Abi-Abdallah C, Lee B. How social accountability can be incorporated into an urban community-based medical education program: an Australian initiative. Educ Health. 2014;27(2):148–151. doi:10.4103/1357-6283.143746
80. Rourke J, Asghari S, Hurley O, et al. From pipelines to pathways: the Memorial experience in educating doctors for rural generalist practice. Rural Remote Health. 2018;18(1):4427. doi:10.22605/RRH4427
81. Meili R, Ganem-Cuenca A, Leung JW, Zaleschuk D. The CARE model of social accountability: promoting cultural change. Acad Med. 2011;86(9):1114–1119. doi:10.1097/ACM.0b013e318226adf6
82. Harden RM. Outcome-based education: the future is today. Med Teach. 2007;29(7):625–629. doi:10.1080/01421590701729930
83. Nabin AR, Hamza YS, Kenya M. IFMSA policy document social accountability of medical schools; 2021.
84. Abdalla ME, Taha MH, Onchonga D, et al. Instilling social accountability into the health professions education curriculum with international case studies: AMEE Guide No. 175. Med Teach. 2024;1–14.
85. Abdalla ME, Boelen C, Osman WN. Development and evaluation of an online course about the social accountability of medical schools. J Taibah Univ Sci. 2019;14(3):241–245. doi:10.1016/j.jtumed.2019.03.004
86. Ferlie EB, Shortell SM. Improving the quality of health care in the United Kingdom and the United States: a framework for change. Milbank Q. 2001;79(2):281–315. doi:10.1111/1468-0009.00206
87. Ratnayake A, Lederer A. Service learning in public health: a critical assessment of potential benefits and unintended consequences. Pedagogy Health Promotion. 2024;10(1):11–15. doi:10.1177/23733799231177043
88. WHO Commission on Social Determinants of Health, World Health Organization. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health: Commission on Social Determinants of Health Final Report. World Health Organization; 2008.
89. Abdalla ME, Taha MH, Onchonga D, et al. Integrating the social determinants of health into curriculum: AMEE Guide No. 162. Med Teach. 2024;46(3):304–316. doi:10.1080/0142159X.2023.2254920
90. Nour N, Onchonga D, Neville S, O’Donnell P, Abdalla ME. Integrating the social determinants of health into graduate medical education training: a scoping review. BMC Med Educ. 2024;24(1):565. doi:10.1186/s12909-024-05394-2
91. Nour N, Stuckler D, Ajayi O, Abdalla ME. Effectiveness of alternative approaches to integrating SDOH into medical education: a scoping review. BMC Med Educ. 2023;23(1):18. doi:10.1186/s12909-022-03899-2
92. Wykurz G, Kelly D. Developing the role of patients as teachers: literature review. BMJ. 2002;325(7368):818–821. doi:10.1136/bmj.325.7368.818
93. Barber C, Van der Vleuten C, Leppink J, Chahine S. Social accountability frameworks and their implications for medical education and program evaluation: a narrative review. Acad Med. 2020;95(12):1945–1954. doi:10.1097/ACM.0000000000003731
94. Boelen C. Building a socially accountable health professions school: towards unity for health. Educ Health. 2004;17(2):223–231. doi:10.1080/13576280410001711049
95. Wood B, Fitzgerald M, Kendall C, Cameron E. Integrating socially accountable health professional education and learning health systems to transform community health and health systems. Learn Health Syst. 2021;5(3):e10277. doi:10.1002/lrh2.10277
96. Ventres W, Boelen C, Haq C. Time for action: key considerations for implementing social accountability in the education of health professionals. Adv Health Sci Educ. 2018;23:853–862. doi:10.1007/s10459-017-9792-z
97. Shrivastava SR, Shrivastava PS, Wanjari M. Adoption of a comprehensive approach to overcome the challenges involved in the implementation of social accountability in medical education: a brief review. J Pharm Bioallied Sci. 2024;16(Suppl 3):S1916–S1919. doi:10.4103/jpbs.jpbs_1253_23
98. Taha MH, Abdalla ME, Wadi MMS, Khalafalla HE, Akbarilakeh M. The implementation of social accountability in medical schools in Eastern Mediterranean region: a scoping review. J Taibah Univ Sci. 2023;18(1):84–97. doi:10.1016/j.jtumed.2022.08.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.