Back to Journals » Nature and Science of Sleep » Volume 13
Snoring Sound Characteristics are Associated with Common Carotid Artery Profiles in Patients with Obstructive Sleep Apnea
Authors Chuang HH, Liu CH, Wang CY, Lo YL, Lee GS, Chao YP ![]() , Li HY
, Li HY ![]() , Kuo TBJ, Yang CCH
, Kuo TBJ, Yang CCH ![]() , Shyu LY, Lee LA
, Shyu LY, Lee LA ![]()
Received 15 March 2021
Accepted for publication 12 July 2021
Published 24 July 2021 Volume 2021:13 Pages 1243—1255
DOI https://doi.org/10.2147/NSS.S311125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Hai-Hua Chuang, 1– 3 Chi-Hung Liu, 4 Chao-Yung Wang, 5 Yu-Lun Lo, 6 Guo-She Lee, 7, 8 Yi-Ping Chao, 4, 9 Hsueh-Yu Li, 10 Terry BJ Kuo, 11 Cheryl CH Yang, 11 Liang-Yu Shyu, 12 Li-Ang Lee 10, 11
1Department of Family Medicine, Chang Gung Memorial Hospital, Taipei Branch and Linkou Main Branch, Chang Gung University, Taoyuan, Taiwan; 2Department of Industrial Engineering and Management, National Taipei University of Technology, Taipei, Taiwan; 3Genomic Medicine Institute & Obesity Institute, Geisinger Medical, Danville, PA, USA; 4Department of Neurology, Chang Gung Memorial Hospital, Linkou Main Branch, Chang Gung University, Taoyuan, Taiwan; 5Department of Cardiology, Chang Gung Memorial Hospital, Linkou Main Branch, Chang Gung University, Taoyuan, Taiwan; 6Department of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, Linkou Main Branch, Chang Gung University, Taoyuan, Taiwan; 7Faculty of Medicine, National Yang-Ming University, Taipei, Taiwan; 8Department of Otolaryngology, Taipei City Hospital, Ren-Ai Branch, Taipei, Taiwan; 9Department of Computer Science and Information Engineering, Chang Gung University, Taoyuan, Taiwan; 10Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou Main Branch, Chang Gung University, Taoyuan, Taiwan; 11Institute of Brain Science, National Yang-Ming University, Taipei, Taiwan; 12Department of Biomedical Engineering, Chung Yuan Christian University, Taoyuan, Taiwan
Correspondence: Li-Ang Lee
Departments of Otorhinolaryngology-Head and Neck Surgery, Sleep Center, Chang Gung Memorial Hospital, Linkou Main Branch, No. 5, Fu-Hsing Street, Guishan District, Taoyuan, 33305, Taiwan
Tel +886 33281200 ext. 3972
Fax +886 33979361
Email [email protected]
Background: Obstructive sleep apnea (OSA) and snoring have been reported to be modifiable risk factors for thick carotid intima-media thickness (CIMT) and carotid atherosclerosis, which are closely linked to cardiovascular disease.
Methods: This cross-sectional study prospectively recruited 70 participants with OSA and without a history of carotid artery disorder, who primarily sought surgical Intervention. OSA and snoring were assessed with the Epworth Sleepiness Scale, Snore Outcomes Survey, polysomnography, and snoring sound recording. The carotid arteries were evaluated with ultrasonography and divided into three types of carotid artery profiles (normal carotid artery, thick CIMT, or significant carotid atherosclerosis). Multivariate linear/logistic/categorical regressions were performed with the forward selection approaches/logistic least absolute shrinkage and selection operator, as appropriate.
Results: Normalized snoring sound energy (301– 850 Hz) was independently associated with the carotid intima-media thickness (regression coefficient [β] = 0.01, standard error [SE] = 0.004, P = 0.03; R 2 = 0.067) and type of carotid profile (β = 0.40, SE = 0.09, P < 0.001; R 2 = 0.156). Normalized snoring sound energy (4– 300 Hz) (β = − 0.10, SE = 0.04, P = 0.01) and female sex (β = 1.90, SE = 0.94, P = 0.04) were independently related to the presence of carotid stenosis (R 2 = 0.159). The optimal regression model of the type of carotid artery profile included normalized snoring sound energy (301– 850 Hz) (β = 0.33, SE = 0.14, P = 0.03), snoring time (β = 0.26, SE = 0.13, P = 0.047), female sex (β = 0.26, SE = 0.13, P = 0.047), and increased age (β = 0.20, SE = 0.10, P = 0.04) under the control of the Snore Outcomes Survey score, 3% oxygen desaturation index, snoring sound energy (4– 1500 Hz), normalized snoring sound energy (851– 1500 Hz), cigarette smoking, and hyperlipidemia (R 2 = 0.427).
Conclusion: Our findings suggested that snoring sound characteristics are associated with carotid artery profiles among early OSA patients who cannot be noticed by ultrasound because organic changes of the carotid artery have not yet started. Future studies are warranted to verify the clinical significance of the results.
Keywords: atherosclerosis, common carotid artery, categorical regression, obstructive sleep apnea, snoring, ultrasound
Corrigendum for this paper has been published
Introduction
Atherosclerotic cardiovascular disease (CVD), mainly comprising coronary heart disease and cerebrovascular disease, is one of the most important causes of morbidity and premature death worldwide.1–3 Thick carotid intima-media thickness (CIMT) and carotid atherosclerosis are well-documented risk factors for CVD, along with hypertension, diabetes mellitus (DM), cigarette smoking, and hyperlipidemia.4
Epidemiological studies indicate that patients with obstructive sleep apnea (OSA) have increased CIMT and subclinical atherosclerosis.5–8 OSA is associated with an increased incidence and progression of CVD.9,10 From a meta-analysis, long-term continuous positive airway pressure (CPAP) therapy significantly reduced CIMT in patients with severe OSA.11 However, an investigation by McEvoy et al did not support that CPAP prevented cardiovascular events in patients with moderate-to-severe OSA and established CVD.12 Identification and early intervention for OSA patients who are at-risk of future atherosclerotic CVD remain an important yet challenging clinical issue.
Snoring is a cardinal and probably also the most notable symptom of OSA. It negatively affects the quality of life of the patients. Previous studies suggest that snoring sound energy (SSE) is associated with structural pathogenic factors, disease severity, and treatment response.13–15 Snoring-associated vibration energy can be transmitted from the upper airway lumen to the peri-pharyngeal tissues and then across the carotid artery wall to the lumen.16,17 In animal models, snoring vibration of the peri-carotid tissue induced endothelial dysfunction18 and resulted in a depression of baroreflex sensitivity.19 Both endothelial and autonomic dysfunctions promote carotid atherosclerosis in humans.20,21
Kim et al reported an independent association between snoring and increased CIMT.15 Lee et al further demonstrated that CIMT was correlated with SSE at some specific frequencies.22 Notably, features of snoring sounds differ largely within individuals. Therefore, normalization of SSEs is essential to ensure comparability between different subjects regardless of pre-existing heterogeneity. SSE-based technology may be beneficial to risk stratification for carotid artery disorders among patients with OSA. However, investigations on the field are rare, evidence scarce, and conclusions unclear.
We hypothesized that OSA severity and SSE were associated with an abnormal carotid artery profile. In this study, the first aim was to investigate differences in polysomnographic parameters and frequency-specific SSE between patients with normal carotid arteries, thick CIMT, or carotid atherosclerosis. The second aim was to identify independent factors predicting the carotid artery profile among patients with OSA.
Materials and Methods
Data Availability Statements
The data underlying this article cannot be shared publicly due to the privacy of individuals that participated in the study. The data can be shared at reasonable request to the corresponding author.
Study Design and Subjects
This prospective cross-sectional study was approved by the Institutional Review Board at the Chang Gung Medical Foundation (No. 201700902A3; date of approval: 26 July 2017), and all procedures were conducted in compliance with the Declaration of Helsinki 1975. Written informed consent was obtained from all participants. Consecutive patients who sought surgical intervention at the clinics of Department of Otorhinolaryngology, Head and Neck Surgery, Chang Gung Memorial Hospital, Taoyuan, Taiwan because of typical OSA symptoms (habitual snoring, witnessed sleep apnea, or excessive daytime sleepiness) were recruited between May 2018 and October 2020. The inclusion criteria were: (1) age between 20 and 59 years; (2) body mass index (BMI) between 18 and 35 kg/m2; and (3) willingness to participate in this study after it had been explained in detail. The exclusion criteria were (1) history of upper airway surgery such as uvulopalatopharyngoplasty; (2) contraindications for OSA surgery, such as established CVD with or without medication and psychiatric disorders; and (3) history of abnormal carotid artery profile such as thick IMT, carotid plaque, or carotid atherosclerosis. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were followed.23
Clinical Variables and Traditional Atherosclerotic CVD Risk Factors
Sex, age, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), and the duration of OSA were recorded. The Epworth Sleepiness Scale (ESS) questionnaire was used to assess daytime sleepiness,24 and the Snore Outcomes Survey (SOS) questionnaire was used to assess snoring-related health status.25 Furthermore, traditional atherosclerotic CVD risk factors, including increased age (men, ≥45 years; women, ≥55 years), overweight or obesity (BMI ≥24 kg/m2), cigarette smoking (previous or current), hypertension, diabetes mellitus (DM), and hyperlipidemia, were also collected.26–28
OSA Severity Parameters from Polysomnography
All patients underwent in-laboratory polysomnography (Alice 5, Philips Respironics, MA, USA) in a silent environment.29 An apnea event was defined as a drop in the peak thermal sensor excursion by ≥90% of the baseline for at least 10 s. Hypopnea was defined as a decrease in the nasal pressure signal excursion by ≥30% for at least 10 s, accompanied by desaturation of 4% or more from the pre-event baseline or an arousal from sleep.30 Apnea–hypopnea index (AHI), 3% oxygen desaturation index (ODI3), mean pulse oxygen saturation (SpO2), and minimal SpO2 were recorded. OSA was defined as obstructive AHI ≥5 events/h.
Snoring Sound Detection and Analysis
In this study, snoring sound detection and polysomnography were performed simultaneously in a well-controlled sleep laboratory setting to ensure a high quality of the data. A portable digital sound recorder with linear pulse-code modulation (PCM-D50, Sony Electronics Inc., Tokyo, Japan) was positioned 100 cm above the participant’s head to record snoring sounds. The methodologies of snoring sound detection and analysis have been described in detail in previous studies.22,29 At least 4 h of snoring sounds were recorded at a sampling rate of 44,100 Hz with a 16-bit analog-to-digital converter for each participant.14 The frequency power spectrum was created by fast Fourier transformation (range, 4–1500 Hz) with a frequency resolution of 4 Hz. We further analyzed snoring sounds throughout each recording using a 0.25-s time window with no overlapping data. Net snore power was obtained by subtracting the long-term spectrum average of noise from that of each snoring frequency. The snoring index (SI) and snore time ratio (ratio of total snoring time to total sleep time) were analyzed. SSE levels (J/m3) of various frequency domains were acquired using a specially developed software program (Figure 1A). There were four frequency bands (total, 4–1500 Hz; B1, 4–300 Hz; B2, 301–850 Hz; and B3, 851–1500 Hz).13,29,31–33 Notably, differences in the total SSE and specific frequency-domain SSEs of between individuals were very heterogeneous. Although snoring intensity was similar in both sexes and seemed not to be affected by AHI, SI was higher in men and in slow wave sleep in adults.34 As inter-individual comparisons were potentially affected by lack of SSE normalization, the specific frequency-domain normalized SSE (SSE%) was further quantified as the ratio of the frequency-domain SSE to the sum of all frequency-domain SSEs (Figure 1B).
 |
Figure 1 Distribution of long-term energy spectrum of the snoring sounds before and after normalization in 70 adults with obstructive sleep apnea. (A), Before normalization, the distributions of all frequency-domains of snoring sound energies were very heterogenous between different subjects. (B) After normalization, heterogeneity of all frequency-domains of snoring sound energies had been reduced to evaluate both the amount and characteristics of energy conveyed by snoring. Frequency domain: B1, 4–300 Hz; B2: 301–850 Hz; B3: 851–1500 Hz. |
Carotid Artery Evaluation with Ultrasonography
To minimize observer bias, the investigation team members who performed carotid ultrasonography were blinded to the patients’ clinical information. With the patient placed in the supine position, images of bilateral common, internal, and bifurcation sites of the carotid arteries were obtained using a B-mode ultrasound system (Philips HDI 5000 System, ATL-Philips, Bothell, USA) and a 5- to 13-MHz vascular probe. In this study, far-wall CIMT in the distal portion of each common carotid artery (CCA) was measured in the proximal 1 to 2 cm of the carotid bulb in plaque-free areas.35 The CIMT of the right and left CCAs were measured six times, and all results were averaged for statistical analysis. The American Society of Echography task force recommends that CIMT ≥75th percentile (according to sex and age subgroups for right and left CCAs) was considered “thick CIMT” because of an increased CVD risk.26,36 The presence of plaque was defined by focal structures infringing into the arterial lumen by at least 1.5 mm or focal narrowing of the vessel wall of >50% relative to adjacent segments.26,37,38 The degree of carotid stenosis (normal: 0% stenosis of the CCA luminal diameter; mild: <50% stenosis; moderate: 50–69% stenosis; severe: 70–99% stenosis) were measured.37,38 Herein, thick CIMT indicated subclinical carotid atherosclerosis while significant carotid atherosclerosis was defined if there was the presence of plaque or carotid stenosis, which could be a potential source of embolic strokes. Therefore, participants were further categorized into three carotid artery profiles: ‘normal carotid arteries (ie, none of thick CIMT or carotid plaque), “thick CIMT” (ie, solitary thick CIMT without carotid plaque or stenosis), or ‘significant carotid atherosclerosis’ (ie, having carotid plaque or stenosis).
Statistical Analysis
The main outcome measure was the type of the carotid artery profile. Using the D’Agostino and Pearson normality test, most of the variables were not normally distributed. Therefore, those non-normally distributed continuous variables were transformed to normal using a two-step approach: the fractional rank and inverse-normal transformation.39 Thereafter, continuous data are presented as means and standard deviations for normally distributed variables or medians and interquartile ranges (IQR) for skewed variables and were compared using the oneway analysis of variance test followed by Tukey post hoc test for independent samples, as appropriate. Categorical data are presented as numbers and percentages and were compared using X2 test. The associations between continuous and continuous variables or between continuous and binary variables were investigated using the Pearson correlation test or Point-Biserial correlation test, as appropriate. Spearman correlation test was performed to examine the associations between multi-categorical variables and continuous/binary variables.
The associations between the CIMT/presence of carotid stenosis were further investigated using multivariate linear/logistic regression models. Besides, the variables associated with the type of the carotid artery profile were analyzed using multivariate categorical regression models. Incorporation of external information and the sign of regression coefficients with full models, including important variables with significance levels of 0.50 in univariate analyses, were further assessed using multivariate linear/logistic/categorical regression models.40 Regression coefficients were optimally reduced with the forward selection approaches for the multivariate linear/logistic regression models or the logistic least absolute shrinkage and selection operator (LASSO) for multivariate categorical regression models.41 The standard errors (SE) of the regression coefficients (β) were obtained using the bootstrap resampling (n of samples = 50; 1000 runs). Two-tailed P-values <0.05 were considered to be statistically significant. All statistical analyses were performed using SPSS software (version 25.0; International Business Machines Corp., Armonk, NY, USA) and Graph Pad Prism 9.0 for Windows (Graph Pad Software Inc., San Diego, CA, USA).
Results
Clinical Characteristics of Patients with OSA
There were 167 consecutive adults who primarily sought surgical intervention due to habitual snoring, witnessed sleep apnea, or excessive daytime sleepiness during the study period (Figure 2). Fifty-three patients did not meet the inclusion criteria. Furthermore, 17 patients were excluded due to a history of upper airway surgery (n = 6), contraindications for OSA surgery (n = 7), or a history of abnormal carotid artery profile (n = 4). Moreover, two patients with simple snoring (obstructive AHI <5 events/h), 20 patients with inadequate quality of snoring sound data, and five patients with lack of ultrasonography were not included for further statistical analysis.
 |
Figure 2 Flow diagram of study participants. Abbreviations: BMI, body mass index; OSA, obstructive sleep apnea. |
Therefore, a total of 62 (89%) men and eight (11%) women with a median age of 39 (IQR, 33–48) years and a median BMI of 27.3 (IQR, 25.6–29.8) kg/m2 were recruited (Table 1). The median SBP was 124 (IQR, 116–134) mmHg and mean DBP was 75.0 ± 11 mmHg. The median ESS scale was 13 (IQR, 10–18), and the mean SOS score was 36.9 ± 10.0.
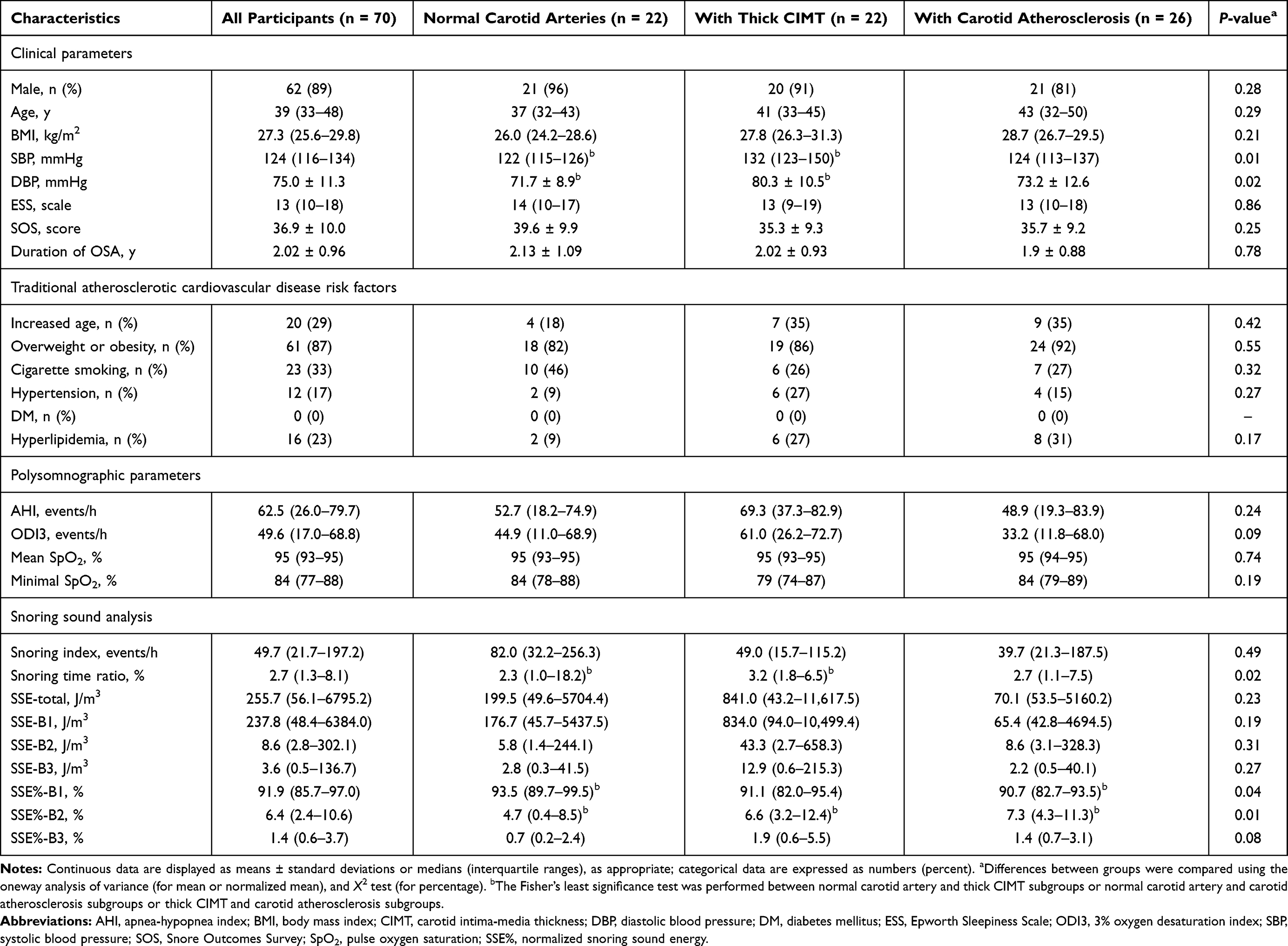 |
Table 1 Characteristics of the Study Population and Comparisons Among Participants with Different Carotid Artery Profile |
Twenty (29%) patients had an increased age; 61 (87%) had overweight or obesity; 23 (33%) were previous or current smokers; 12 (17%) had hypertension; 16 (23%) had hyperlipidemia. None had a known diagnosis of DM.
The average AHI, ODI, mean SpO2, and minimal SpO2 were 62.5 (IQR, 26.0–79.7) events/h, 49.6 (IQR, 17.0–68.8) events/h, 95% (IQR, 93–95%), and 84% (IQR, 77–88%), respectively.
The median SI, snoring time ratio, SSE-total, SSE-B1, SSE-B2, SSE-B3, SSE%-B1, SSE%-B2, and SSE%-B3 were 49.7 (IQR, 21.7–197.2) events/h, 2.7% (IQR, 1.3–8.1%), 255.7 (IQR, 56.1–6795.2) J/m3, 237.8 (IQR, 48.4–6384.0) J/m3, 8.6 (IQR, 2.8–302.1) J/m3, 3.6 (IQR, 0.5–136.7) J/m3, 91.9% (IQR, 85.7–97.0%), 6.4% (IQR, 2.4–10.6%), and 1.4% (IQR, 0.6–3.7%), respectively.
The median CIMT of the overall cohort was 0.60 (IQR, 0.51–0.77) mm. Twenty-two (31%) participants had normal carotid artery, 22 (31%) patients had solitary thick CIMT (ie, subclinical carotid atherosclerosis), and 26 (37%) patients had significant carotid atherosclerosis (solitary carotid plaque [n = 2], thick CIMT with carotid plaque [n = 3], and solitary carotid stenosis [n = 21]). The median CIMTs of these three subgroups were 0.50 (IQR, 0.43–0.53) mm, 0.61 (IQR, 0.55–0.75) mm, and 0.78 (IQR, 0.71–0.91 mm), respectively. Among the patients with significant carotid atherosclerosis, eleven (42%) had mild carotid stenosis, 14 (54%) had moderate stenosis, and one (4%) had severe carotid stenosis.
The mean duration of OSA was 2.02 ± 0.96 years. The mean time interval between carotid ultrasound and polysomnography was 22.3 ± 14.6 days.
Differences in Clinical Characteristics Across Three Subgroups
Differences in SBP, DBP, snoring time ratio, SSE%-B1, and SSE%-B2 were significant across three subgroups (Table 1). Notably, the thick CIMT subgroup had significantly higher SBP, DBP, and snoring time ratio than the normal carotid artery subgroup. Furthermore, the significant carotid atherosclerosis subgroup had a significantly lower SSE%-B1 and a significantly higher SSE%-B2 than the normal carotid artery subgroup. Differences in sex, age, BMI, cigarette smoking, hypertension, hyperlipidemia, DM, ESS, SOS, AHI, ODI3, mean SpO2, minimal SpO2, and other six snoring sound analysis parameters across the three subgroups were not statistically significant.
Associations Between CIMT and Variables of Interest
The CIMT was significantly and weakly associated with the SSE%-B2 (r = 0.26, P = 0.03) using the Pearson correlation test. For reducing the likelihood of overfitting, the variables with P <0.50 such as age (r = 0.15, P = 0.23), BMI (r = 0.18, P = 0.15), SBP (r = 0.12, P = 0.34), DBP (r = 0.11, P = 0.38), SOS score (r = −0.19, P = 0.12), the duration of OSA (r = 0.10, P = 0.42), AHI (r = 0.11, P = 0.36), SI (r = −0.11, P = 0.38), snoring time ratio (r = 0.18, P = 0.24), SSE-total (r = −0.13, P = 0.28), SSE-B1 (r = −0.13, P = 0.30), SSE%-B1 (r = −0.20, P = 0.10), and SSE%-B3 (r = 0.19, P = 0.12), using the Pearson correlation test, and female sex (r = 0.18, P = 0.13), using the Point-Biserial correlation test, were included for multivariate linear analysis.41 Using the forward selection methods, the SSE%-B2 was the independent variables related to CIMT (β = 0.01, SE = 0.004, P = 0.03) (R2 = 0.067). The relationship between the SSE%-B2 and CIMT remained to be significant (β = 0.01, SE = 0.004, P = 0.04) after adjustment for increased age (β = 0.09, SE = 0.05, P = 0.07), overweight or obesity (β = 0.04, SE = 0.07, P = 0.60), cigarette smoking (β = −0.01, SE = 0.05, P = 0.78), hypertension (β = 0.04, SE = 0.06, P = 0.53), and hyperlipidemia (β = 0.04, SE = 0.05, P = 0.46) (R2 = 0.156).
Associations Between the Presence of Carotid Stenosis and Variables of Interest
The presence of carotid stenosis was significantly related to SSE%-B2 (r = 0.26, P = 0.03) using the Point-Biserial correlation test. Herein, female sex (r = 0.20, P = 0.10), age (r = 0.16, P = 0.20), SBP (r = −0.09, P = 0.48), DBP (r = −0.10, P = 0.40), SOS (r = −0.09, P = 0.48), ODI3 (r = −0.17, P = 0.18), minimal SpO2 (r = 0.10, P = 0.41), the duration of OSA (r = −0.09, P = 0.46), SSE-total (r = −0.16, P = 0.20), SSE-B1 (r = −0.18, P = 0.15), SSE%-B1 (r = −0.23, P = 0.06), and SSE%-B3 (r = 0.18, P = 0.13) were additionally included for multivariate logistic regression analysis. Using the forward selection methods, female sex (β = 1.81, SE = 0.85, P = 0.03) and SSE%-B1 (β = −0.08, SE = 0.03, P = 0.02) were the independent variables related to the presence of carotid stenosis (R2 = 0.159). The significant relationships of the presence of carotid stenosis with female sex (β = 1.90, SE = 0.94, P = 0.044) and SSE%-B2 (β = −0.10, SE = 0.04, P = 0.01) persisted after adjustment for increased age (β = 0.85, SE = 0.66, P = 0.20), overweight or obesity (β = 1.40, SE = 1.04, P = 0.18), cigarette smoking (β = 0.01, SE = 0.63, P = 0.99), hypertension (β = −0.60, SE = 0.83, P = 0.47), and hyperlipidemia (β = 0.68, SE = 0.66, P = 0.30) (R2 = 0.234).
Associations of the Type of the Carotid Artery Profile with Variables of Interest
The carotid artery profiles were further quantified as type 1 (normal carotid artery), type 2 (thick CIMT), and type 3 (significant carotid atherosclerosis) according to the potential of future CVD.4 The type of the carotid artery profile was significantly and weakly associated with the SSE%-B1 (r = −0.28, P = 0.02), SSE%-B2 (r = 0.34, P = 0.004), and SSE%-B3 (r = 0.25, P = 0.04) using the Spearman correlation test. For avoiding overfitting, the variables with P <0.50 and traditional atherosclerotic CVD risk factors were additionally included for multivariate categorical analysis. Therefore, female sex (r = 0.19, P = 0.11), age (r = 0.19, P = 0.12), BMI (r = 0.11, P = 0.37), SOS score (r = −0.21, P = 0.09), ODI3 (r = −0.09, P = 0.47), SI (r = −0.12, P = 0.34), snoring time ratio (r = 0.17, P = 0.25), SSE-total (r = −0.12, P = 0.33), and SSE-B1 (r = −0.13, P = 0.28), increased age (r = 0.15, P = 0.22), overweight or obesity (r = 0.13, P = 0.28), cigarette smoking (r = −0.16, P = 0.19), hypertension (r = 0.06, P = 0.62), and hyperlipidemia (r = 0.21, P = 0.08) were further selected for regression models. Moreover, overlapping information (age, BMI) was removed from regression analysis.40
Table 2 shows data adjusted for all the selected variables including specific variables and traditional atherosclerotic CVD risk factors. Using the LASSO methods for actively selecting from a potentially multicollinear set of variables in the regression,41 the optimal categorical regression model of the type of the carotid artery profile included female sex, SOS score, ODI3, snoring time ratio, SSE-total, SSE%-B2, SSE%-B3, increased age, cigarette smoking, and hyperlipidemia (R2 = 0.427) (Figure 3). Among them, the female sex (β = 0.26, SE = 0.13, P = 0.047), increased age (β = 0.20, SE = 0.10, P = 0.04), snoring time ratio (β = 0.26, SE = 0.13, P = 0.047), and SSE%-B2 (β = 0.33, SE = 0.14, P = 0.03) were significantly and independently related to the type of the carotid artery profile. The most parsimonious model within one standardized error included only the SSE%-B2 (β = 0.40, SE = 0.09, P < 0.001; R2 = 0.156).
 |
Table 2 The Estimated Coefficients for Logistic Least Absolute Shrinkage and Selection Operator (LASSO) Regression Between Studied Variables and Traditional Atherosclerotic Cardiovascular Disease Risk Factors with the Type of the Carotid Artery Profile |
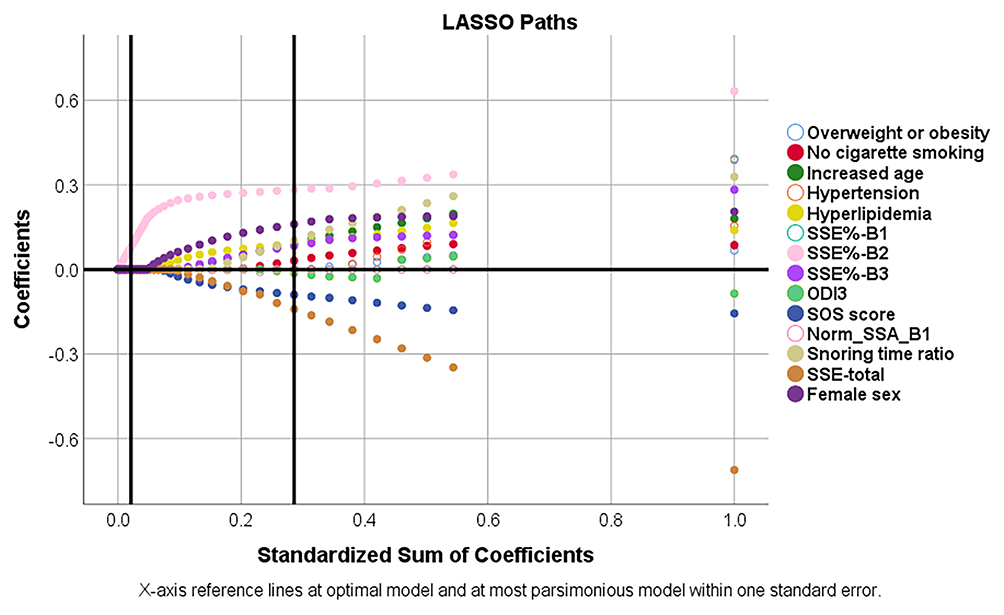 |
Figure 3 Logistic least absolute shrinkage and selection operator (LASSO) paths for the type of the carotid artery profiles. Fifteen variables, including studied variables and traditional atherosclerotic cardiovascular disease risk factors, were analyzed using the multivariate categorical regression models. X-axis reference lines indicate the optimal model (ten variables) and the most parsimonious model (one variable) within one standard error. Abbreviations: ODI3, 3% oxygen desaturation index; SOS, Snore Outcomes Survey; SSE, snoring sound energy; SSE%, normalized snoring sound energy. |
Discussion
The present study conducted a detailed investigation on the relationships between OSA severity, snoring sound characteristic, and carotid artery profile based on a hospital-based sample. We discovered that the SSE%-B2 was associated with CIMT, independently of traditional atherosclerotic CVD risk factors (Figure 4). In contrast, SSE%-B1 and female sex were related to the presence of carotid stenosis with or without adjustment for traditional atherosclerotic CVD risk factors. Furthermore, the increased SSE%-B2, snoring time ratio, female sex, and increased age were independent risk factors for the abnormal carotid artery profile after adjustment for the other six covariances with the optimal performance. Interestingly, polysomnographic parameters, including AHI, mean SpO2, and minimal SpO2, were not related to carotid sonographic parameters in patients with OSA. In most clinical settings, carotid sonography is not a routine exam for patients with early OSA with subclinical carotid artery disease. Our findings suggest that this non-invasive snoring sound analysis has the potential to help the risk stratification of carotid artery disease for this population.
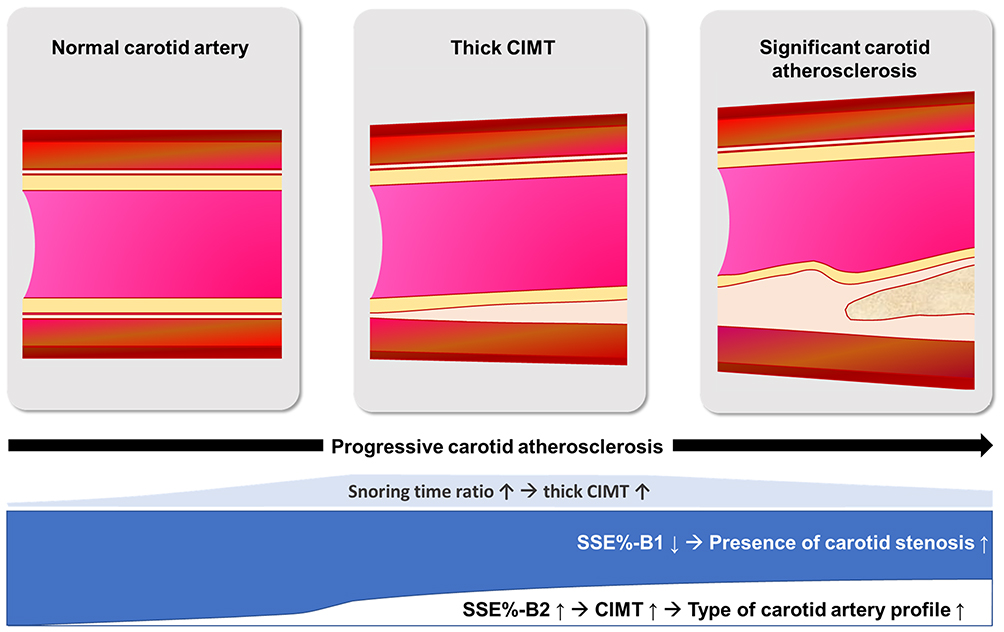 |
Figure 4 Snoring sound characteristics and carotid atherosclerosis in patients with obstructive sleep apnea. Abbreviations: B1, 4–300 Hz; B2, 301–850 Hz; CIMT, carotid intima-media thickness; SSE%, normalized snoring sound energy. |
An increasing number of studies have investigated the relationships between OSA and carotid arteries because of their clinical importance and shared risk factors. Previous studies reported that traditional CVD risk factors seemed less accurate in estimating atherosclerosis for patients with OSA.42,43 The current study had a few strengths, which enabled us to provide several novel and unique perspectives to the topic and overcame some limitations of the previous works.15,44,45
First, the profile of carotid arteries was carefully evaluated and defined. Increased CIMT and carotid atherosclerosis are both well-known risk factors for ischemic stroke.4,46 Besides, CIMT nonlinearly predicts the risk of CVD events.47 However, both CIMT and atherosclerosis progress with age, and age-related CIMT growth is not necessarily connected with atherosclerosis.46,48,49 In this study, we defined “thick CIMT” according to the American Society of Echography Task Force recommendations, which is considered to perform better in predicting cardiovascular events.26,36 We found that both female sex and increased age were independently related to the high type of the carotid artery profile in patients with OSA.
Second, the effect of snoring was investigated with an intricate and in-depth method. Snoring is an easily recognizable symptom but not easily described and quantified as a parameter. It is usually screened with self-reported questionnaires such as Berlin Questionnaire, STOP-Bang questionnaire, and SOS questionnaire. These tools are convenient and highly accessible, but the data collected are mostly subjective and not ideal for an objective and quantitative evaluation. Previous investigations on the associations between snoring and carotid artery disorder had inconsistent conclusions. Self-reported snoring was demonstrated to be related to subclinical atherosclerosis,7 high-risk carotid plaque features,50 or bilateral carotid artery stenosis.51 However, some research suggested differently. In a larger cohort study, habitual snoring (≥3 nights/week) was not a risk factor of carotid atherosclerosis.8 From our results, no significant correlation was found on carotid artery status with SOS, SI, or the duration of OSA.
Based on the hypothesis that the long-term acoustic or vibratory energy of snoring is a possible driving force of endothelial damage of adjacent vessels, a spectrum that demonstrates the energy of snoring sound (either in SSE or SSE%) and snoring time ratio can serve as better parameters for assessing the dose–response effect of snoring on CIMT and carotid atherosclerosis compared to all the other currently used approaches. This has formed the rationale for a series of previous studies.13–15 In an earlier investigation, we found that full-night SSE-0–20 Hz and SSE-652–1500 Hz, as their snoring sounds recorded in the home environment, were positively associated with CIMT in 15 patients with OSA.22 In this study, the SSE%-B2 was positively associated with CIMT, the SSE%-B1 was inversely related to the presence of carotid stenosis under the control of the other two covariances, and the SSE%-B2 and snoring time ratio were positively correlated with the type of the carotid artery profile under the control of the other eight covariances. These findings suggested that the SSE might play a less important role than the SSE% and snoring time ratio in a specific population. Noteworthy, the snoring time ratio and type of carotid artery profile were inverted U-shape relationship and SEE%-B1 and SEE%-B2 were a reciprocal relationship (Figure 4). Apparently, these indexes might account for some unexplained causes of the traditional atherosclerotic model. Our results suggested that snoring plays an important role in the thickening wall of the carotid artery, and traditional atherosclerotic risk factors continuously contributed to the formation of atheroma and plaque of the carotid artery in patients with OSA.
Notably, the SSE%-B2 seems to be a novel independent marker for CIMT and type of carotid artery profile. More studies are warranted to prove its effects on the carotid artery wall. The snoring sounds with a peak frequency between 301 Hz and 850 Hz (B2) were linked to epiglottic snores (peak frequency, 490 Hz).52 Because the epiglottis is anatomically located nearby the CCA, our finding suggested that epiglottic snores might transmit to the CCA and then involve in the development of thick CIMT and carotid atherosclerosis. Furthermore, SSE-B2 has been correlated with oropharyngeal lateral wall collapse, epiglottis obstruction,29 or tonsil/tongue base obstruction.53,54 Notably, a high SSE%-B2 does not necessarily mean a high SSE-B2, especially when the SSE-total is small. Therefore, future studies are warranted to investigate whether SSE%-B2 is a possible pathogenic or exacerbating factor effected on the damage of carotid arteries through the lateral wall of the pharynx, either by structural compression, which could disturb blood flow, or repetitive vibrating motions, which could lead to microdamage to the endothelium of the vessels, or both.
The literature has had inconsistent conclusions on whether the clinical presentation or disease severity of OSA is associated with CIMT.45,55,56 Ghofraniha et al reported a correlation between ESS and CIMT.57 Zhou et al elucidated that OSA was an independent risk factor for CIMT after adjusting for confounders.58 However, some other studies found no evidence to support AHI as an independent predictor of CIMT.59,60 From our data, the ODI3 was partially associated with the type of carotid artery profile, but there were no associations of the carotid artery profile with ESS, AHI, mean SpO2, or minimal SpO2.
There were some limitations to this study. First, it was cross-sectional and unable to confirm causal relationships. Longitudinal studies are warranted to examine the long-term effects of OSA severity and snoring on carotid atherosclerosis and CVD events. Second, the subjects of this study were patients in need of surgical treatment for OSA, and this might limit the generalizability of our findings. Although this study was a biased sample towards males, younger age, more severe OSA, and absence of morbid obesity, diabetes, and clinical carotid atherosclerosis because we used convenience sampling, it reflected the truth of an academic otolaryngology center in Taiwan. Noteworthily, CPAP is the first-line treatment for moderate-to-severe OSA;61 surgical intervention is an alternative treatment for patients who are incompliant or unwilling to CPAP therapy.62 Third, the sample size was relatively small for multivariate regression models with a lot of variables. In this study, qualitative external information for selection and estimation was used to reduce overfit models in small data sets.40 Furthermore, the forward selection approach and LASSO regression analysis was performed to select optimal variables, reduce the variability in the estimates of regression coefficient, improve the prediction error of the model, and increase interpretability.41 However, further studies with a larger sample size are warranted to thoroughly investigate the role of snoring in the pathogenesis of carotid atherosclerosis among OSA patients at different disease stages and with various treatment plans.
Conclusion
In summary, approximately two-third of early OSA patients had abnormal carotid artery profiles, highlighting the importance of carotid artery examinations. Notably, the SSE%-B2 was independently associated with CIMT; the SSE%-B1 was independently related to the presence of carotid stenosis; the SSE%-B2 and snoring time ratio were independently correlated with the type of carotid artery profile. In contrast, traditional CVD risk factors and OSA parameters were partially related to carotid sonographic measurements in patients with OSA who primarily thought to surgical intervention. Therefore, this non-invasive snoring sound analysis may be a rational approach to stratify the risk of subclinical carotid atherosclerosis and help to prevent possible atherosclerotic CVD events in patients with OSA. Particularly, snoring sound analysis is effective in screening at-risk OSA patients for carotid artery diseases, who are not yet identified by ultrasound because of their relatively early stage of organic damages in the carotid arteries. Further studies are warranted to confirm the clinical significance of the results.
Acknowledgments
This study was supported by the Chang Gung Medical Foundation, Taiwan, grant numbers CMRPG3F1091-3 (LAL), and CORPG1I0021, CMRPG1J0041 (HHC). We are grateful to all of the volunteers in the study cohort for their participation. We thank Chung-Fang Hsiao for her excellent technical assistance and case management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ellulu MS, Patimah I, Khaza’ai H, Rahmat A, Abed Y, Ali F. Atherosclerotic cardiovascular disease: a review of initiators and protective factors. Inflammopharmacology. 2016;24(1):1–10. doi:10.1007/s10787-015-0255-y
2. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
3. Thrift AG, Howard G, Cadilhac DA, et al. Global stroke statistics: an update of mortality data from countries using a broad code of “cerebrovascular diseases”. Int J Stroke. 2017;12(8):796–801. doi:10.1177/1747493017730782
4. Ravikanth R. Relevance of carotid intima-media thickness and plaque morphology in the risk assessment of patients with acute ischemic cerebral infarcts: a case-control study of large series from a single center. J Med Ultrasound. 2020;28(1):29–34.
5. Nadeem R, Harvey M, Singh M, et al. Patients with obstructive sleep apnea display increased carotid intima media: a meta-analysis. Int J Vasc Med. 2013;2013:839582.
6. Somuncu MU, Karakurt ST, Karakurt H, Serbest NG, Cetin MS, Bulut U. The additive effects of OSA and nondipping status on early markers of subclinical atherosclerosis in normotensive patients: a cross-sectional study. Hypertens Res. 2019;42(2):195–203. doi:10.1038/s41440-018-0143-0
7. Deol R, Lee KA, Kanaya AM, Kandula NR. Obstructive sleep apnea risk and subclinical atherosclerosis in South Asians living in the United States. Sleep Health. 2020;6(1):124–130. doi:10.1016/j.sleh.2019.09.007
8. Zhao YY, Javaheri S, Wang R, et al. Associations between sleep apnea and subclinical carotid atherosclerosis: the multi-ethnic study of atherosclerosis. Stroke. 2019;50(12):3340–3346. doi:10.1161/STROKEAHA.118.022184
9. Geovanini GR, Wang R, Weng J, et al. Association between obstructive sleep apnea and cardiovascular risk factors: variation by age, sex, and race. the multi-ethnic study of atherosclerosis. Ann Am Thorac Soc. 2018;15(8):970–977. doi:10.1513/AnnalsATS.201802-121OC
10. Aurora RN, Crainiceanu C, Gottlieb DJ, Kim JS, Punjabi NM. Obstructive sleep apnea during REM sleep and cardiovascular disease. Am J Respir Crit Care Med. 2018;197(5):653–660. doi:10.1164/rccm.201706-1112OC
11. Chen LD, Lin L, Lin XJ, et al. Effect of continuous positive airway pressure on carotid intima-media thickness in patients with obstructive sleep apnea: a meta-analysis. PLoS One. 2017;12(9):e0184293. doi:10.1371/journal.pone.0184293
12. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919–931. doi:10.1056/NEJMoa1606599
13. Lee LA, Yu JF, Lo YL, et al. Energy types of snoring sounds in patients with obstructive sleep apnea syndrome: a preliminary observation. PLoS One. 2012;7(12):e53481. doi:10.1371/journal.pone.0053481
14. Lu CT, Li HY, Lee GS, et al. Snoring sound energy as a potential biomarker for disease severity and surgical response in childhood obstructive sleep apnoea: a pilot study. Clin Otolaryngol. 2019;44(1):47–52. doi:10.1111/coa.13231
15. Kim J, Pack A, Maislin G, Lee SK, Kim SH, Shin C. Prospective observation on the association of snoring with subclinical changes in carotid atherosclerosis over four years. Sleep Med. 2014;15(7):769–775. doi:10.1016/j.sleep.2014.03.009
16. Amatoury J, Howitt L, Wheatley JR, Avolio AP, Amis TC. Snoring-related energy transmission to the carotid artery in rabbits. J Appl Physiol (1985). 2006;100(5):1547–1553. doi:10.1152/japplphysiol.01439.2005
17. Howitt L, Kairaitis K, Kirkness JP, et al. Oscillatory pressure wave transmission from the upper airway to the carotid artery. J Appl Physiol (1985). 2007;103(5):1622–1627. doi:10.1152/japplphysiol.01413.2006
18. Cho JG, Witting PK, Verma M, et al. Tissue vibration induces carotid artery endothelial dysfunction: a mechanism linking snoring and carotid atherosclerosis? Sleep. 2011;34(6):751–757. doi:10.5665/SLEEP.1042
19. Narayan J, Amatoury J, Cho JG, et al. Snoring effects on the baroreflex: an animal model. Respir Physiol Neurobiol. 2012;180(2–3):342–351. doi:10.1016/j.resp.2011.12.012
20. Perticone F, Ceravolo R, Pujia A, et al. Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation. 2001;104(2):191–196. doi:10.1161/01.CIR.104.2.191
21. Ulleryd MA, Prahl U, Borsbo J, et al. The association between autonomic dysfunction, inflammation and atherosclerosis in men under investigation for carotid plaques. PLoS One. 2017;12(4):e0174974. doi:10.1371/journal.pone.0174974
22. Lee GS, Lee LA, Wang CY, et al. The frequency and energy of snoring sounds are associated with common carotid artery intima-media thickness in obstructive sleep apnea patients. Sci Rep. 2016;6:30559. doi:10.1038/srep30559
23. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
24. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
25. Gliklich RE, Wang PC. Validation of the snore outcomes survey for patients with sleep-disordered breathing. Arch Otolaryngol Head Neck Surg. 2002;128(7):819–824. doi:10.1001/archotol.128.7.819
26. Stein JH, Korcarz CE, Hurst RT, et al. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr. 2008;21(2):
27. Santos-Neto PJ, Sena-Santos EH, Meireles DP, et al. Association of carotid plaques and common carotid intima-media thickness with modifiable cardiovascular risk factors. J Stroke Cerebrovasc Dis. 2021;30(5):105671. doi:10.1016/j.jstrokecerebrovasdis.2021.105671
28. Sun Y, Lin C-H, Lu C-J, Yip P-K, Chen R-C. Carotid atherosclerosis, intima media thickness and risk factors—an analysis of 1781 asymptomatic subjects in Taiwan. Atherosclerosis. 2002;164(1):89–94. doi:10.1016/S0021-9150(02)00017-5
29. Lee LA, Lo YL, Yu JF, et al. Snoring sounds predict obstruction sites and surgical response in patients with obstructive sleep apnea hypopnea syndrome. Sci Rep. 2016;6:30629. doi:10.1038/srep30629
30. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. deliberations of the sleep apnea definitions task force of the American academy of sleep medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
31. Lee LA, Yu JF, Lo YL, et al. Comparative effects of snoring sound between two minimally invasive surgeries in the treatment of snoring: a randomized controlled trial. PLoS One. 2014;9(5):e97186. doi:10.1371/journal.pone.0097186
32. Chen WC, Lee LA, Chen NH, et al. Treatment of snoring with positional therapy in patients with positional obstructive sleep apnea syndrome. Sci Rep. 2015;5:18188. doi:10.1038/srep18188
33. Li HY, Lee LA, Yu JF, et al. Changes of snoring sound after relocation pharyngoplasty for obstructive sleep apnoea: the surgery reduces mean intensity in snoring which correlates well with apnoea-hypopnoea index. Clin Otolaryngol. 2015;40(2):98–105. doi:10.1111/coa.12325
34. Levartovsky A, Dafna E, Zigel Y, Tarasiuk A. Breathing and snoring sound characteristics during sleep in adults. J Clin Sleep Med. 2016;12(3):375–384. doi:10.5664/jcsm.5588
35. Rosvall M, Janzon L, Berglund G, Engstrom G, Hedblad B. Incident coronary events and case fatality in relation to common carotid intima-media thickness. J Intern Med. 2005;257(5):430–437. doi:10.1111/j.1365-2796.2005.01485.x
36. Nambi V, Chambless L, Folsom AR, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol. 2010;55(15):1600–1607. doi:10.1016/j.jacc.2009.11.075
37. Zhai FF, Yang M, Wei Y, et al. Carotid atherosclerosis, dilation, and stiffness relate to cerebral small vessel disease. Neurology. 2020;94(17):e1811–e1819. doi:10.1212/WNL.0000000000009319
38. Topakian R, King A, Kwon SU, Schaafsma A, Shipley M, Markus HS. Ultrasonic plaque echolucency and emboli signals predict stroke in asymptomatic carotid stenosis. Neurology. 2011;77(8):751–758. doi:10.1212/WNL.0b013e31822b00a6
39. Templeton GF. A two-step approach for transforming continuous variables to normal: implications and recommendations for IS research. Commun Assoc Info Syst. 2011;28:4. doi:10.17705/1CAIS.02804
40. Steyerberg EW, Eijkemans MJC, Harrell FE, Habbema JDF. Prognostic modelling with logistic regression analysis: a comparison of selection and estimation methods in small data sets. Stat Med. 2000;19(8):1059–1079. doi:10.1002/(SICI)1097-0258(20000430)19:8<1059::AID-SIM412>3.0.CO;2-0
41. Tibshirani R. Regression shrinkage and selection via the lasso. J Royal Stat Soc Series B. 1996;58(1):267–288.
42. Kavousi M, Leening MJ, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, ADULT TREATMENT PANEL III guidelines, and European Society of Cardiology guidelines for cardiovascular disease prevention in a European cohort. JAMA. 2014;311(14):1416–1423. doi:10.1001/jama.2014.2632
43. Papageorgiou N, Briasoulis A, Androulakis E, Tousoulis D. Imaging subclinical atherosclerosis: where do we stand? Curr Cardiol Rev. 2017;13(1):47–55. doi:10.2174/1573403X12666160803095855
44. Deeb R, Judge P, Peterson E, Lin JC, Yaremchuk K. Snoring and carotid artery intima-media thickness. Laryngoscope. 2014;124(6):1486–1491. doi:10.1002/lary.24527
45. Salepci B, Fidan A, Ketenci SC, et al. The effect of obstructive sleep apnea syndrome and snoring severity to intima-media thickening of carotid artery. Sleep Breath. 2015;19(1):239–246. doi:10.1007/s11325-014-1002-0
46. Waje-Andreassen U, Naess H, Thomassen L, Eide GE, Meijer R, Vedeler CA. Ultrasound, atherosclerosis and stroke at a young age: a cross-sectional long-term follow-up in western Norway. Eur J Neurol. 2008;15(5):512–519. doi:10.1111/j.1468-1331.2008.02118.x
47. Simonetto C, Heier M, Rospleszcz S, et al. Risk for cardiovascular events responds nonlinearly to carotid intima-media thickness in the KORA F4 study. Atherosclerosis. 2020;296:32–39. doi:10.1016/j.atherosclerosis.2020.01.013
48. Roldan PC, Greene ER, Qualls CR, Sibbitt WL, Roldan CA. Progression of atherosclerosis versus arterial stiffness with age within and between arteries in systemic lupus erythematosus. Rheumatol Int. 2019;39(6):1027–1036. doi:10.1007/s00296-019-04267-y
49. Dinenno FA, Jones PP, Seals DR, Tanaka H. Age-associated arterial wall thickening is related to elevations in sympathetic activity in healthy humans. Am J Physiol Heart Circ Physiol. 2000;278(4):H1205–H1210. doi:10.1152/ajpheart.2000.278.4.H1205
50. Kirkham EM, Hatsukami TS, Heckbert SR, et al. Association between snoring and high-risk carotid plaque features. Otolaryngol Head Neck Surg. 2017;157(2):336–344. doi:10.1177/0194599817715634
51. Deeb R, Smeds MR, Bath J, et al. Snoring and carotid artery disease: a new risk factor emerges. Laryngoscope. 2019;129(1):265–268. doi:10.1002/lary.27314
52. Agrawal S, Stone P, McGuinness K, Morris J, Camilleri AE. Sound frequency analysis and the site of snoring in natural and induced sleep. Clin Otolaryngol Allied Sci. 2002;27(3):162–166. doi:10.1046/j.1365-2273.2002.00554.x
53. Gurpinar B, Salturk Z, Kumral TL, Civelek S, Izel O, Uyar Y. Analysis of snoring to determine the site of obstruction in obstructive sleep apnea syndrome. Sleep Breath. 2020;1–6. doi:10.1007/s11325-020-02252-5
54. Miyazaki S, Itasaka Y, Ishikawa K, Togawa K. Acoustic analysis of snoring and the site of airway obstruction in sleep related respiratory disorders. Acta Otolaryngol Suppl. 1998;537:47–51. doi:10.1080/00016489850182350
55. Bozkus F, Dikmen N, Gungor G, Samur A. The effect of obstructive sleep apnea syndrome and hypothyroidism to intima-media thickness of carotid artery. Sleep Breath. 2017;21(1):31–36. doi:10.1007/s11325-016-1384-2
56. Çetin N, Güneş Tatar İ, Yüceege M, Ergun O, Hekimoğlu B. Ultrasonographic evaluation of abdominal wall fat index, carotid intima-media thickness and plaque score in obstructive sleep apnea syndrome. Med Ultrason. 2019;21(4):422–426. doi:10.11152/mu-1949
57. Ghofraniha L, Amini M, Davoudi Y, et al. The relation of carotid arteries’ intima-media thickness with snoring and obstructive sleep apnea in type 2 diabetes patients. Acta Med Iran. 2017;55(12):765–771.
58. Zhou M, Guo B, Wang Y, Yan D, Lin C, Shi Z. The association between obstructive sleep apnea and carotid intima-media thickness: a systematic review and meta-analysis. Angiology. 2017;68(7):575–583. doi:10.1177/0003319716665985
59. Gorzewska A, Specjalski K, Drozdowski J, et al. Intima-media thickness in patients with obstructive sleep apnea without comorbidities. Lung. 2013;191(4):397–404. doi:10.1007/s00408-013-9471-7
60. Song F, Zou J, Song Z, et al. Association of adipocytokines with carotid intima media thickness and arterial stiffness in obstructive sleep apnea patients. Front Endocrinol (Lausanne). 2020;11:177. doi:10.3389/fendo.2020.00177
61. Sullivan C, Berthon-Jones M, Issa F, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;317(8225):862–865. doi:10.1016/S0140-6736(81)92140-1
62. Li HY, Lee LA, Hsin LJ, et al. Intrapharyngeal surgery with integrated treatment for obstructive sleep apnea. Biomed J. 2019;42(2):84–92. doi:10.1016/j.bj.2019.02.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.